Embed Size (px)
Citation preview

Alessandro Follador
NSCLC EGFR mutato: quali opzioni terapeutiche?
Profilo di tossicita degli inibitori
di EGFR
Padova 17 settembre 2105
Dipartimento di Oncologia direttore dr. Gianpiero Fasola

Erlotinib, Gefitinib
1st generation, reversible, targeted to EGFR, small molecules, quinazolinamine class.
They inhibit the tyrosine kinase activity of the epidermal growth factor receptor (EGFR) by competing with ATP
for the ATP-binding site.
TKis in NSCLC IIIb/IV EGFR mut+ve
AZD9291, Dacomitinib, Rociletinib… 3rd generation and beyond
Afatinib
2nd generation, selectively and irreversibly binds and inhibits EGFR, HER2, HER4

No EGFR monoclonal antibodies
No combination therapy: biological, chemotherapy, radiotherapy
No EGFR wild type setting
TKis in NSCLC IIIb/IV EGFR mut+ve

TKis in NSCLC IIIb/IV EGFR mut+ve
Standard of care, proved benefit over doublets platinum
based chemotherapy -1st line setting - in terms of
PFS
ORR
Toxicity/tolerability
QoL, symptoms improvement, PROs
Masters, JCO 2015 ASCO guidelines
Randomized phase 3 clinical trial

TKis in NSCLC IIIb/IV EGFR mut+ve / Main toxicities
Gastrointestinal Diarrhea
Stomatitis/mucositis
Nausea
Anorexia
Dermatological Rash
Pruritus
Dry skin
Paronychia
Systemic Fatigue
Hepatic Hypertransaminasemia
Respiratory Interstitial lung disease and ILD-like events

TKis in NSCLC IIIb/IV EGFR mut+ve / Main toxicities
New toxicity (3rd generation) Hypeglicemia
QTc prolongation
Hypertricosis
Different toxicity profile compared to standard CT No myelosuppression, vomiting and neurotoxicity

TKis in NSCLC IIIb/IV EGFR mut+ve / Main toxicities
Usually mild/moderate, manageable, not life threatening
Reversible, even to complete resolution
Potentially affecting QOL due to long lasting treatment period
Difficult to asses (lack of accurate and standardized definition and
scales, subjective evaluation, underestimated by the treating
physicians..)
Discrepancy in perception between pts and clinicians
Possibly related to case by case decisions on treatment stop or
dose reduction.

Silvia Novello, Transl Lung Cancer Res 2014
Different perception of skin toxicity and relative toxicity
grades
TKis in NSCLC IIIb/IV EGFR mut+ve / Perception
G2 Rash acneiform: Papules and/or pustules covering 10-30% BSA, which may or may not be associated with
symptoms of pruritus or tenderness; associated with psychosocial impact; limiting instrumental ADL.
CTCAE v.4 NCI

Silvia Novello, Transl Lung Cancer Res 2014
Different perception of astenia toxicity grades
TKis in NSCLC IIIb/IV EGFR mut+ve / Perception

No direct comparison yet, different trials
Methodological issues Inclusion criteria, stratification factors, selected vs unselected population
EGFR test
Type of chemotherapy
Main study objective
Assessment scales and timing
Reporting bias
Items to be considered
Tolerability: dose reduction, treatment discontinuation
Toxicity: grading and management adverse events
Treatment-related grade ≥ 3 event
Treatment-related event leading to discontinuation
Treatment-related event leading to death
Quality of Life
Patient Report Outcomes
Economic evaluation
TKis in NSCLC IIIb/IV EGFR mut+ve / Methodological issues

Drug reduction, modification and discontinuation
Raffaele Califano, Drugs 2015
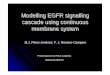
TKis in NSCLC IIIb/IV EGFR mut+ve / Main toxicities

Alon Scope, JCO 2010
Kinetic of appareance
Wk of EGFR-Targeted Therapy
Acne-like rash Postinflammatory effects
Dry skin
Fissure
Paronychia
1 2 3 4 5 6 7 8 9
Pruritus
TKis in NSCLC IIIb/IV EGFR mut+ve / Dermatological toxicities

TKis in NSCLC IIIb/IV EGFR mut+ve / Gastrointestinal
Gefitinib,
BJC 2014
EURTAC,
Lancet Oncology
2012
LUX-lung3,
JCO 2013
Grade Any 3 4 Any 3 4 Any 3 4
Diarrhoea 30,8 3,7 57 5 0 95.2 14.4 0
Stomatitis NR NR NR NR NR 72,1 8,7
Nausea 10,3 0 NR NR NR 17,9 0,9
Vomiting 13,1 0 NR NR NR 17 3,1

TKis in NSCLC IIIb/IV EGFR mut+ve / Dermatological
Gefitinib,
BJC 2014
EURTAC,
Lancet Oncology
2012
LUX-lung3,
JCO 2013
Grade Any 3 4 Any 3 4 Any 3 4
Rash 44,9 0 80 13 0 70,3 14 0
Rash/acne NR NR NR
NR NR 89,1 16,2
Dermatitis
acneiform 6,5 0 NR NR NR 34,9 2,6 0
Dry skin 11,2 0 NR NR NR 29,3 0,4 0
Pruritus NR NR NR NR NR 18,8 0,4 0
Cheilitis NR NR NR NR NR 12,2 0 NA
Paronychia NR NR NR NR NR 56,8 11,4

TKis in NSCLC IIIb/IV EGFR mut+ve / Miscellaneous
Gefitinib,
BJC 2014
EURTAC,
Lancet Oncology
2012
LUX-lung3,
JCO 2013
Grade Any 3 4 Any 3 4 Any 3 4
Decreased
appetite 9,3 0 31 0 0 20,5 3,1 0
Fatigue 11,2 0 56 6 NA 7,5 1,3 NA
Alopecia NR NA 14 NA NA NR NA NA
Aspartate
aminotransferase 8,4 0,9 NR NR NR NR NR NR
Arthralgia NR NR 11 1 0 NR NR NR

TKis in NSCLC IIIb/IV EGFR mut+ve / Interstitial lung disease
Onset: 3-7 weeks [?]
1/3 fatal
Incidence ~ 1-3% [?]
Pre existing lung disease
Supportive therapy (ICU assistance)
High dose corticosteroids
Treatment discontinuation

TKis in NSCLC IIIb/IV EGFR mut+ve / Conclusion 1/2
Pay attention and consider
Education
Prophylactic measures
Early assessment
Early treatment
Dose delay/interruption
Dose reduction (if appropriate
EGFR-TKi >> platinum based doublets for IIIb/IV
NSCLC EGFR mut+ve, 1st line.

TKis in NSCLC IIIb/IV EGFR mut+ve / Conclusion 2/2
Head to head trial in EGFR Mut+
Prospective interventional trial to manage toxicity
Physiopathology of EGFR induced toxicity
Correlation between response / pharmacodynamic /
pharmacokinetics / toxicity
Confirmatory data for subset (i.e. exon 19 and rare
mutation subgroups…)










![New Trends In Internal Medicine2009hocc.medicine.psu.ac.th/files/acadamic/New_Trends... · cytopenia EGF-R profile EGFR FISH EGFR FISH docetaxel gefitinib ñu EGFR FISH Lf-]utnn EGF-R](https://img.pdfslide.us/doc/110x75/60098f15be7b15544f1b652e/new-trends-in-internal-cytopenia-egf-r-profile-egfr-fish-egfr-fish-docetaxel-gefitinib.jpg)