Embed Size (px)
Citation preview
Profile of Medical Student Teaching in Radiology: Teaching Methods, Staff Participation, and Rewards 1
Sal im Samuel , MD, Kitt Shaffer, MD, PhD
Rationale and Objectives. The purpose of this study was to collect demographic information about radiology departments and rewards for teaching activities, as well as the impact of new digital imaging methods on teaching.
Materials and Methods. Two surveys were conducted of directors of medical school clerkships in radiology. The,initial survey focused on numbers of staff and students, courses taught, and perception of rewards for teaching. The follow-up sur- vey more specifically addressed teaching methods.
Results. Sixty-nine (50%) of the initial surveys sent to 139 departments and 46 (39% of a total of 119) of the follow-up surveys were returned. Clerkship directors spent an average of 9 hours per week teaching and performing administrative tasks, with most given no additional time off. Eighty-four percent of departments provide either no or insignificant rewards for teaching. Many departments have integrated the use of computers in teaching, and most have computers that students use during the radiology course. At the same time, digital imaging and picture archiving and communication systems (PACS) are used, or will be used within 1 year, in most departments.
Conclusion. Clerkship directors receive little compensation in terms of time and rewards for medical student teaching. Teaching methods are evolving in response to the increasing use of computers, digital imaging, and PACS for at least part of the workload in most radiology departments.
Key Words. Education; radiology; medical student education.
ReLent changes in health care, particularly the decreasing funds available for teaching hospitals, threaten to constrain medical education programs. The current emphasis on clinical productivity has the potential to overshadow and diminish interest in teaching. The lack of an ordered struc- ture for acknowledging teaching efforts either financially
or academically may discourage participation by faculty overall and will certainly have a negative impact on recruit-
ment of new faculty. In radiology, these changes have been compounded by a
revolution in information technology. Film-oriented radiol-
Acad Radiol 2000; 7:868-874
1 From the Department of Radiology, Brigham and Women's Hospital, Bos- ton, Mass (S.S.), and the Department of Radiology, Dana-Farber Cancer Institute, Harvard Medical School, 44 Bmney St, Boston, MA 02115 (K.S.) Recewed March 1,2000; revision requested April 19; revision received May 23; accepted May 25. Address correspondence to K.S.
© AUR, 2000
ogy departments are now becoming filmless with digital im- aging and picture archiving and communication systems (PACS). The transitional period requires money, time, and
patience, thus putting additional stress on faculty, who may already feel pressure to increase clinical output.
A final issue is the disappearance of anatomy as a spe- cialty, with the subsequent need for medical schools to dis- cover other resources for teaching this essential subject. Ra-
diology departments have been involved in teaching anato- my for many years (1), but increasing the radiologist's role
in this endeavor requires a considerable time commitment. To define the current atmosphere of radiology teaching
in medical schools, a survey was designed for directors of medical student education in radiology. The demographics
of programs, the rewards for teaching activities, and the
participation of radiologists in teaching anatomy were ex- amine& A follow-up survey was used to assess the impact of PACS and technologic changes on methods of medical
student education.
8 6 8
Name
Address
problems
[ ] yes
MEDICAL STUDENT RADIOLOGY EDUCATION SURVEY-- TIME OFF CLINICAL SCHEDULE AND OTHER DEPARTMENTAL SUPPORT
PLEASE DISREGARD ANY DUPLICATE FORMS
Name(s) of med stu course you teach
e-mail address
Telephone I
FAX I
zip code
Are you director of course?
Number of % tad staff students How often do you who teach per course teach this course? in course
Oyes Oyes Oyes Oyes
Number radiology faculty in your Number med students department at your entire school
I I I I How much time do YOU have off for teaching med students per week? (excluding academic time)
I f Format of most teaching sessions
I-]interactive "hot seat" r-lformal slide presentation r-lobservation of actuaJ clinical work Nether: specify-
For clerkship directors, Estimated time YOU estimated time YOU spend on spend teaching med administration for med
students/wk students/wk
[ 1 r 1 For clerkship directors, how much time do YOU have off
other duties for administration for students per wk?
[ 1 What type of final exam do students take? r-lmultiple choice
Dotal case discussion r-lpractical film review r-lno exam given I-Iother: specify-
Flother: specify- When do YOU do most of your medical student teaching?
I-Iduring regular clinical work hours I-Iduring specified teaching time I-Iduring academic time Doff-hours
Rate how high a priority medical student teaching is in your department overall
Over,/high Ohigh Omoderate Olow Overy low
How are you rewarded for teaching?
How important is quality or quantity of medical student teaching in academic promotion in your
department, to your knowledge? Overy important Osomewhat important Onot important Odon't know
For clerkship directors, how are you rewarded for administration related to medical students?
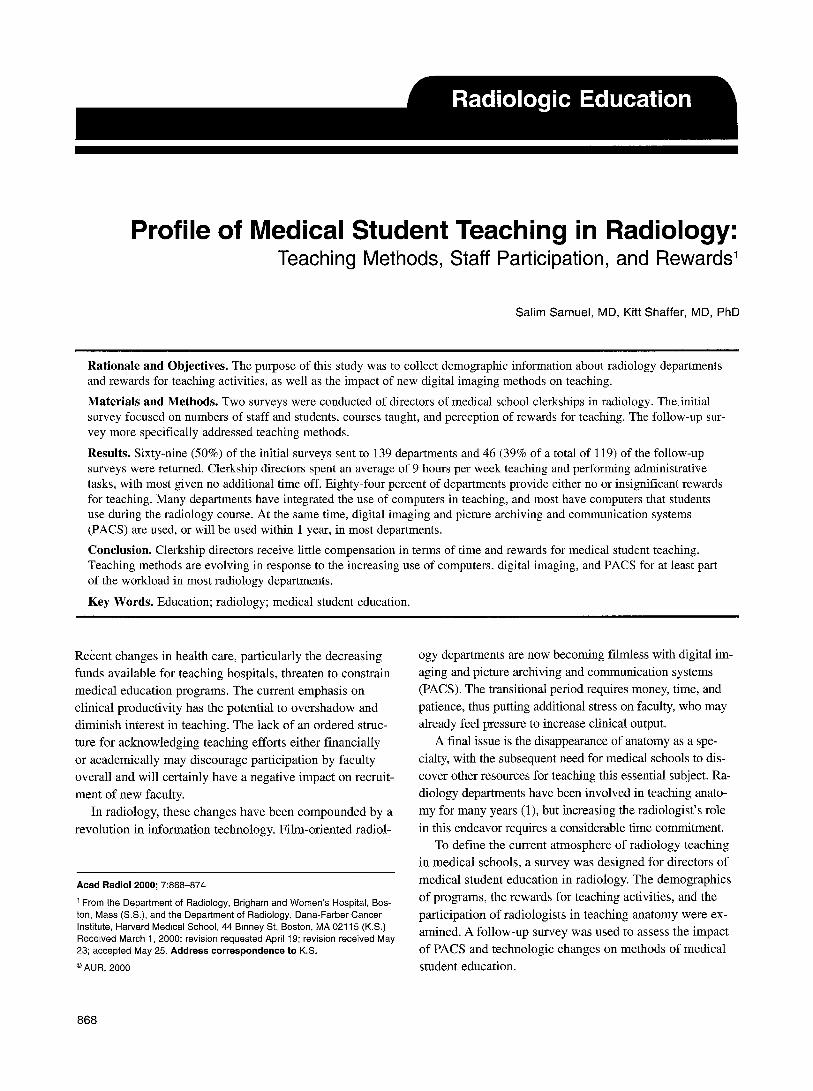
Figure 1. Initial survey.
The initial survey (Fig 1) was sent to all 61 members of American Medical Student Educators in Radiology (AMSER)
and all academic radiology chairmen as identified from the Association of University Radiologists (AUR) mailing list. A
total of 200 surveys were mailed. Since many programs were
sent duplicate surveys, the total number of departments was
used for determination of response rate, rather than the total number of surveys sent. The initial mailing was followed 1 month later by a repeat mailing to all nonresponders. The follow-up survey (Fig 2) was sent out 6 months after the
869
F O L L O W U P Q U E S T I O N N A I R E O N M E D I C A L S T U D E N T E D U C A T I O N IN R A D I O L O G Y Impac t of T e c h n o l o g y on T e a c h i n g M e t h o d s
name I med school I
e'mai l I I hosp ital
Background info on your medical school teaching activities: med school courses you teach required? what year?
01st r 02nd r 03rd r 04th r 01st r 02nd r 03rd r 04th r 01st r 02nd r 03rd r 04th r
] Orequired Oelective 01st yr 02nd yr 03rd yr 04th yr Orequired Oelective 01st yr 02nd yr 03rd yr 04th yr
Background info on your department: PACS chest imaging
Oall modalities on PACS Ocompletely digital Oall but mammo on PACS Osome digital OCT and/or MR only on PACS Oplanned digital within lyr Oconverting to PACS within lyr Onot digital Ono PACS OOther...
general radiography mammography Ocompletely digital Ocompletely digital Osome digital Osome digital Oplanned digital within lyr Oplanned digital within lyr Onot digital Onot digital
use of film in your department Ototally filmless-no films printed OOther... Ooccasional films printed, almost all workstation interpretation Ofilms printed, some workstation interpretation Ofilms printed and used for ALL interpretation
Impact of new technology on your medical student teaching: primary teaching methods please describe " . . . . . . . . - i" ,~ ~.--'.:~,,--'%~:~::~?- ~.,-~ ~~:4°~~ ° - . , , . , ~,, ; ,.~-~-~. ,.,~"o~~:::~, , :~
035 mm slides teaching methods Ovideo you use . . . . . : ' o'- ~--.-: , ; . . :~ . ;2 : , : , : , /o< . , : . , ? Oprojected computer images ; .. - Oindividual computer use by students , ~'k,, -"~ ~:~';~:~ 'J.:.,i-~':'::-,/..: ; ' : ~ "' ' "~: Osimultaneous computer use by groups of students = :/,. : - . 7 ~ f ~~r : , % ~ :-_ ~ -~
Department computer resources used for teaching: do students have computers number of
in your department that Oyes computers are these computers shared? they use during courses? Mac OS ~ Owith residents/fellows Ostudent use only
(If not, skip to next section) Windows OS~_,. ~ : | Owith residents/fellows Ostudent use only other I I Owith residents/fellows Ostudent use only
Department space resources used for teaching: do students have space space for students designated for their use Oyes Ocom uter learnin lab
during courses in your department? Ostud area
(if not, skip this section) Oconference room Oother
Owith
is this space shared? Owith residents/fellows Ostudent use only.._
esidents/fellows Ostudent use o n l y _ ~ Owith residents/fellows Ostudent use only__ Owith residents/fellows Ostudent use only__ Owith residents/fellows Ostudent use only
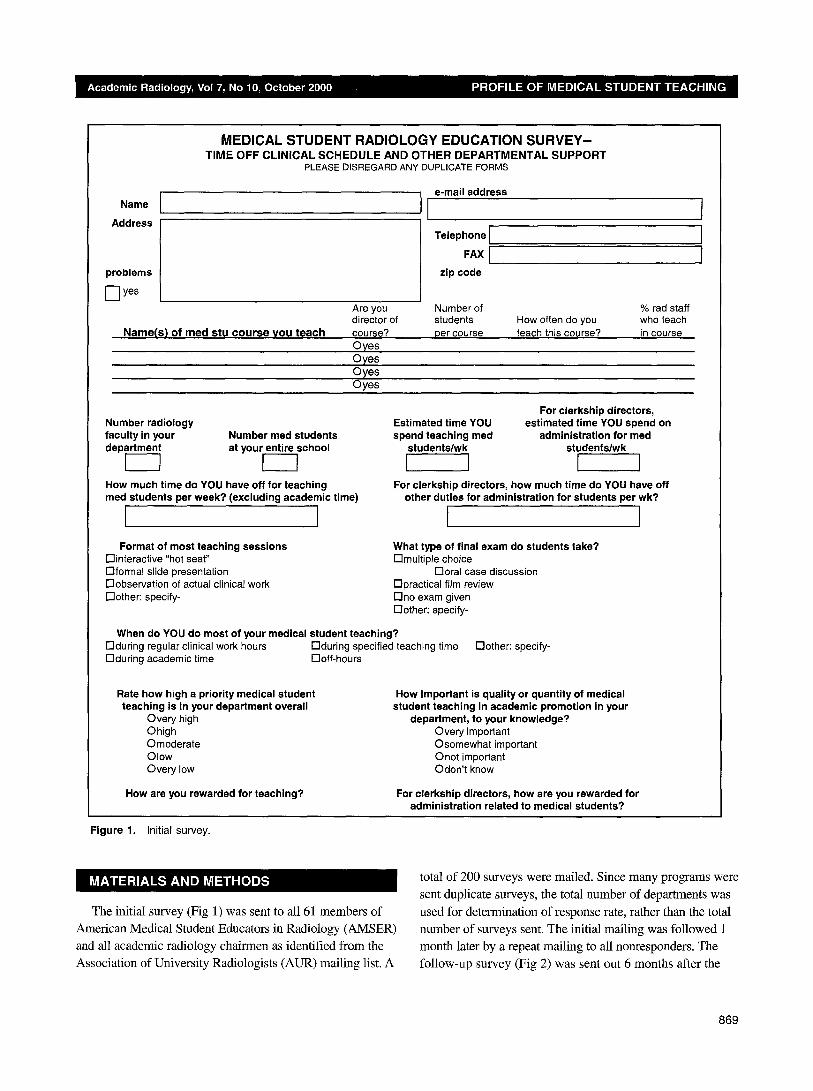
Figure 2. Follow-up survey.
initial survey to a total of 119 sites by using $he mailing list of responders from the initial survey and the AMSER roster and the AUR mailing list. After 6 weeks, all nonresponders
received a 2nd mailing.
Responses were tabulated and examined with a
spreadsheet (Excel, version 8; Microsoft, Redmond,
Wash). Statistical analysis was performed with the Z 2
test.
870
60
50
v 4 0
E "~ 3O Q_
2O
10
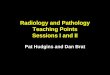
O Very High High Moderate Low Very Low Very frnportant Somewhat Not Irnportent Don't Know
Important Priority of Teaching Importance for Promotion
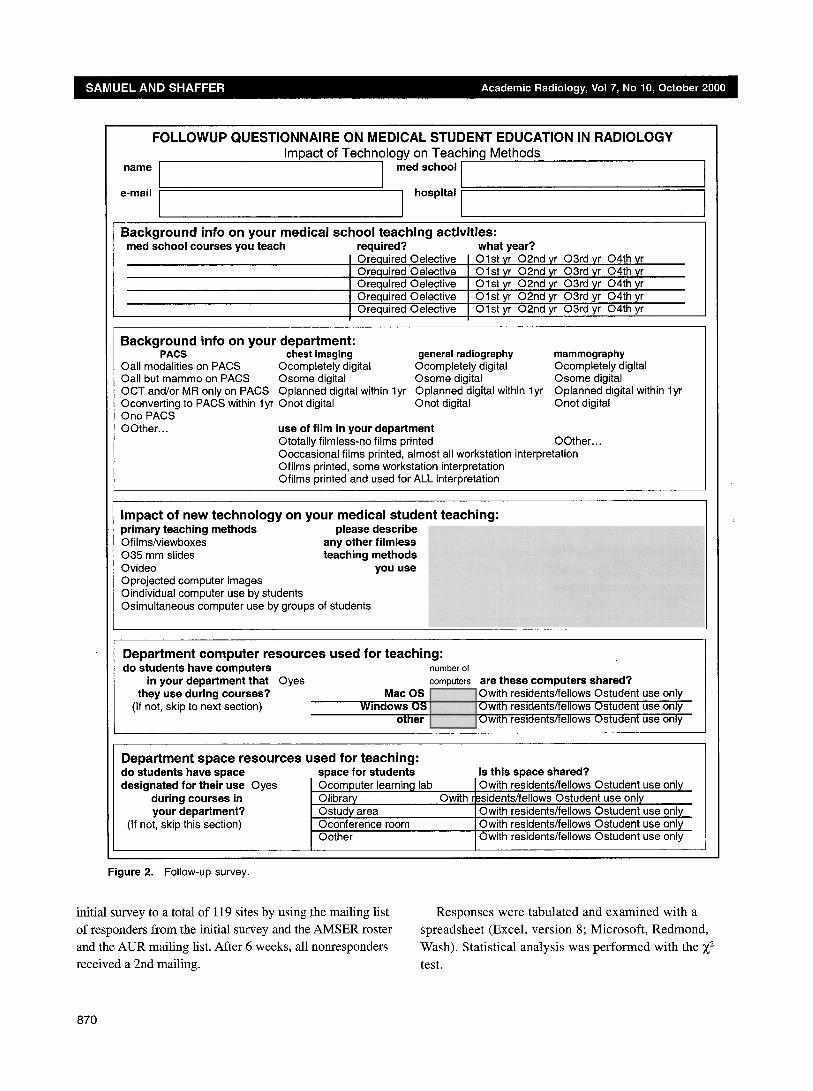
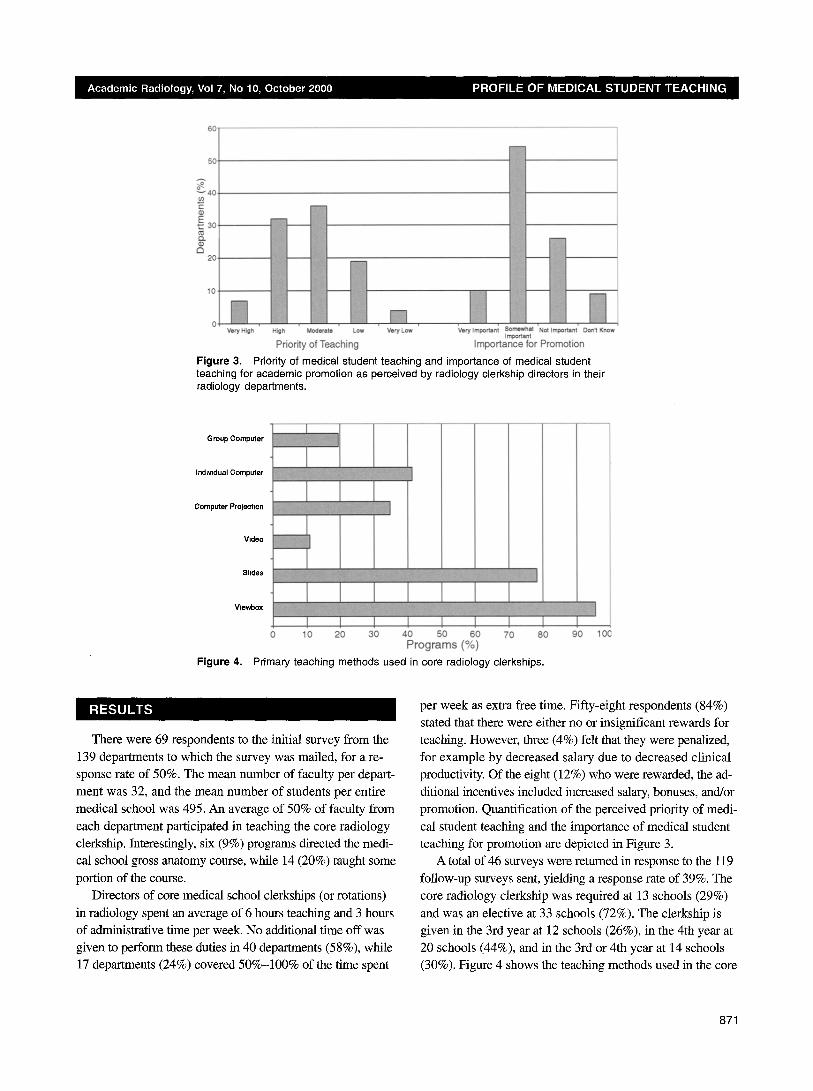
Figure 3. Priority of medical student teaching and importance of medical student teaching for academic promotion as perceived by radiology clerkship directors in their radiology departments.
Group Computer [ I Indiv,dual Computer ~ _ ~
I I
Computer Proj,~t,on ~ ~ i ~N
Video ~
Vlewbox
Figure 4.
I I I I I I I 0 to 20 ao 40 so 60 70 so
Programs (%)
Primary teaching methods used in core radiology clerkships.
I I
i
90 100
There were 69 respondents to the initial survey from the 139 departments to which the survey was mailed, for a re- sponse rate of 50%. The mean number of faculty per depart- ment was 32, and the mean number of students per entire medical school was 495. An average of 50% of faculty from
each department participated in teaching the core radiology clerkship. Interestingly, six (9%) programs directed the medi- cal school gross anatomy course, while 14 (20%) taught some portion of the course.
Directors of core medical school clerkships (or rotations)
in radiology spent an average of 6 hours teaching and 3 hours of administrative time per week. No additional time off was given to perform these duties in 40 departments (58%), while 17 departments (24%) covered 50%-100% of the time spent
per week as extra free time. Fifty-eight respondents (84%) stated that there were either no or insignificant rewards for teaching. However, three (4%) felt that they were penalized,
for example by decreased salary due to decreased clinical productivity. Of the eight (12%) who were rewarded, the ad- ditional incentives included increased salary, bonuses, and/or promotion. Quantification of the perceived priority of medi-
cal student teaching and the importance of medical student teaching for promotion are depicted in Figure 3.
A total of 46 surveys were returned in response to the 119
follow-up surveys sent, yielding a response rate of 39%. The core radiology clerkship was required at 13 schools (29%)
and was an elective at 33 schools (72%). The clerkship is given in the 3rd year at 12 schools (26%), in the 4th year at 20 schools (44%), and in the 3rd or 4th year at 14 schools (30%). Figure 4 shows the teaching methods used in the core
871
==o
60
w E
£ Q.
D
Figure 5,
• Shared with residents
Computer Laboratory Library Study Area Conference Room
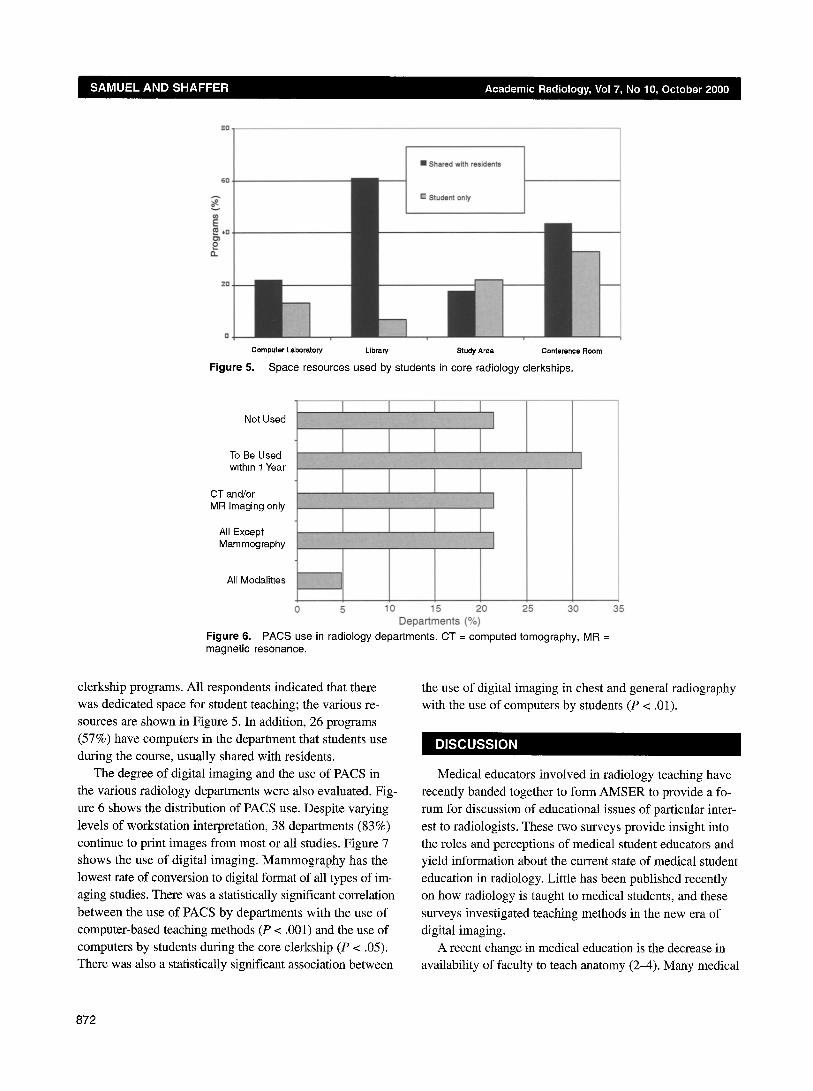
Space resources used by students in core radiology clerkships.
Not Used
To Be Used within 1 Year
CT and/or MR Imaging only
All Except Mammography
All Modalitles
0 5 10 15 20 Departments (%)
Figure 6. PACS use in radiology departments. CT = computed tomography, MR = magnetic resonance.
25 30 35
clerkship programs. All respondents indicated that there was dedicated space for student teaching; the various re- sources are shown in Figure 5. In addition, 26 programs
(57%) have computers in the department that students use during the course, usually shared with residents.
The degree of digital imaging and the use of PACS in the various radiology departments were also evaluated. Fig- ure 6 shows the distribution of PACS use. Despite varying
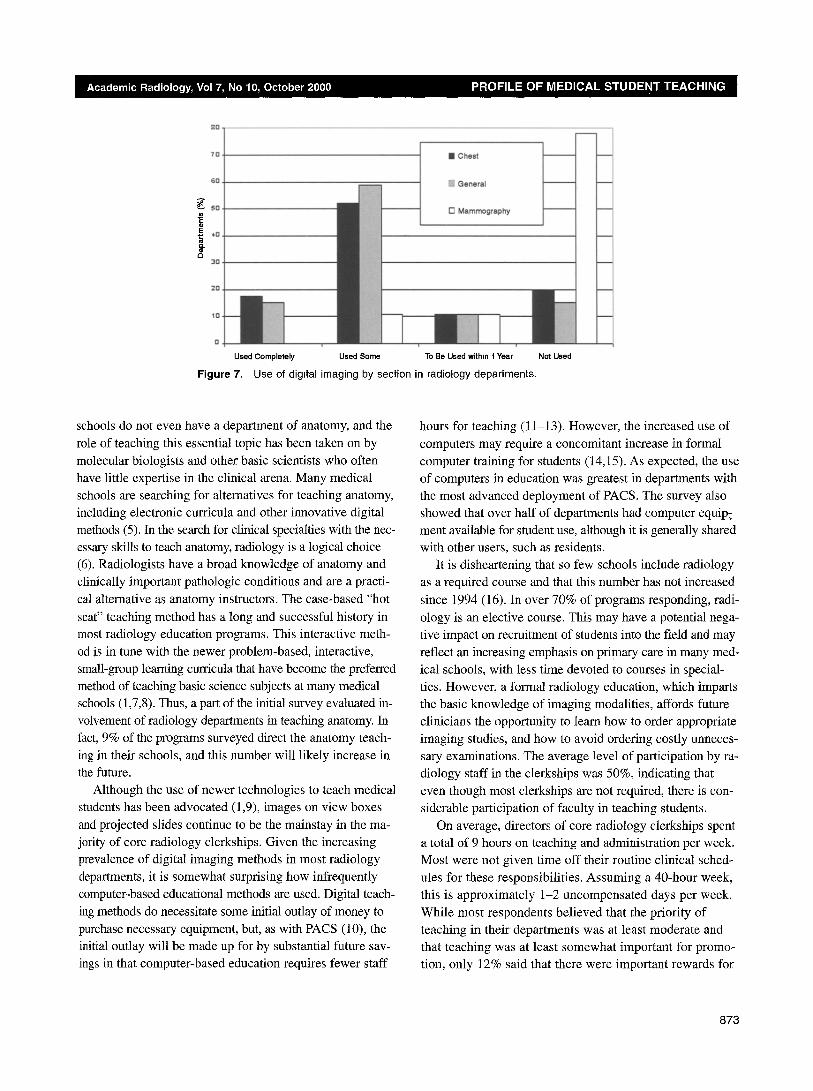
levels of workstation interpretation, 38 departments (83%) continue to print images from most or all studies. Figure 7 shows the use of digital imaging. Mammography has the
lowest rate of conversion to digital format of all types of im- aging studies. There was a statistically significant correlation
between the use of PACS by departments with the use of computer-based teaching methods (P < .001) and the use of
computers by students during the core clerkship (P < .05). There was also a statistically significant association between
the use of digital imaging in chest and general radiography with the use of computers by students (P < .01).
Medical educators involved in radiology teaching have recently banded together to form AMSER to provide a fo-
rum for discussion of educational issues of particular inter-
est to radiologists. These two surveys provide insight into the roles and perceptions of medical student educators and yield information about the current state of medical student
education in radiology. Little has been published recently on how radiology is taught to medical students, and these
surveys investigated teaching methods in the new era of digital imaging.
A recent change in medical education is the decrease in availability of faculty to teach anatomy (2-4). Many medical
872
"ta
40
=o
0
;ZO.
10.
• Chest
t l
Used Completely Used Some To Be Used within t Year
Figure 7. Use of digital imaging by section in radiology departments.
Not Used
_._J
__j
. - . d
schools do not even have a department of anatomy, and the role of teaching this essential topic has been taken on by molecular biologists and other basic scientists who often have little expertise in the clinical arena. Many medical schools are searching for alternatives for teaching anatomy, including electronic curricula and other innovative digital methods (5). In the search for clinical specialties with the nec- essary skills to teach anatomy, radiology is a logical choice (6). Radiologists have a broad knowledge of anatomy and clinically important pathologic conditions and are a practi- cal alternative as anatomy instructors. The case-based "hot
seat" teaching method has a long and successful history in most radiology education programs. This interactive meth- od is in tune with the newer problem-based, interactive, small-group learning curricula that have become the preferred method of teaching basic science subjects at many medical schools (1,7,8). Thus, a part of the initial sttrvey evaluated in- volvement of radiology departments in teaching anatomy. In fact, 9% of the programs surveyed direct the anatomy teach- ing in their schools, and this number will likely increase in the future.
Although the use of newer technologies to teach medical students has been advocated (1,9), images on view boxes
and projected slides continue to be the mainstay in the ma- jority of core radiology clerkships. Given the increasing prevalence of digital imaging methods in most radiology departments, it is somewhat surprising how infrequently computer-based educational methods are used. Digital teach- ing methods do necessitate some initial outlay of money to purchase necessary equipment, but, as with PACS (10), the initial outlay will be made up for by substantial future sav- ings in that computer-based education requires fewer staff
hours for teaching (11-13). However, the increased use of computers may require a concomitant increase in formal computer training for students (14,15). As expected, the use of computers in education was greatest in departments with the most advanced deployment of PACS. The survey also showed that over half of departments had computer equip: ment available for student use, although it is generally shared with other users, such as residents.
It is disheartening that so few schools include radiology as a required course and that this number has not increased
since 1994 (16). In over 70% of programs responding, radi- ology is an elective course. This may have a potential nega- tive impact on recruitment of students into the field and may reflect an increasing emphasis on primary care in many med- ical schools, with less time devoted to courses in special- ties. However, a formal radiology education, which imparts the basic knowledge of imaging modalities, affords future clinicians the opportunity to learn how to order appropriate imaging studies, and how to avoid ordering costly unneces- sary examinations. The average level of participation by ra- diology staff in the clerkships was 50%, indicating that even though most clerkships are not required, there is con- siderable participation of faculty in teaching students.
On average, directors of core radiology clerkships spent a total of 9 hours on teaching and administration per week. Most were not given time off their routine clinical sched- ules for these responsibilities. Assuming a 40-hour week, this is approximately 1-2 uncompensated days per week. While most respondents believed that the priority of teaching in their departments was at least moderate and that teaching was at least somewhat important for promo- tion, only 12% said that there were important rewards for
873

teaching. Intangible rewards such as "appreciation by stu-
dents," "personal satisfaction," "service to medicine," and "pat on the back" were much more common. This lack of
remuneration is exacerbated by the deficiency of methods to accurately account for teaching effort, which is harder
to quantify than clinical productivity or grant support. In the past, when workloads were lower and compensation higher, it was relatively easy to make the time to teach
during a regular work week. Now, however, with mark- edly increasing demands on radiologists' time, this is no
longer feasible. This may be a blessing in disguise, as it may force departments and medical schools to devise ways to quantify, and adequately compensate, teaching ef- fort in a more rational fashion (17-19). Many schools are developing "teaching tracks" for promotion, reflecting a new emphasis on teaching as a scholarly effort worthy of academic recognition in a manner similar to basic re- search (20). Inquiry into how many departments have a
separate teaching promotion track would be interesting to
correlate with the perception of the importance of teach- ing overall.
The response rate for the initial survey was 50%. Be- cause the survey was not anonymous, the results may be biased. However, the number of specifically detailed com- plaints indicates that the lack of anonymity did not pre- vent many clerkship directors from answering candidly.
Future surveys could be done anonymously. However,
part of the purpose of the survey was to obtain a more
complete mailing and e-mail list of clerkship directors to facilitate future interactions. The response rate for the ini- tial survey was somewhat higher than for the follow-up survey, possibly because of their proximity in time. Clerk- ship directors might have believed that the two surveys covered such similar ground that they were reluctant to complete the follow-up survey. The surveys were designed to be relatively simple to complete, but some effort was required to return them by fax. Future surveys might bet- ter be performed through the Internet or with e-mail be-
cause this would save time for responders compared with the methods used here. Nonetheless, the response rates
overall are reasonable for a survey of this type, which is generally in the 40%-60% range (7,14-16).
The two surveys highlight several important issues con- cerning medical student education in radiology. Changing medical student curricula are giving many radiology de-
partments the opportunity to take a greater role in teaching
anatomy and to become increasingly involved in the pre- clinical years. Rapidly changing technology has started to
translate into increasing computer-based teaching. Radiol- ogy departments need to concentrate on improving the
compensation for the important scholarly pursuit of medi- cal student teaching so that the potential improvements in
medical student education afforded by improved technol- ogy and changing times can be fully realized.
:IEFERENCE
1. Squire LF. On teaching radtology to medical students: challenges for the nineties. A JR Am J Roentgeno11989, 152"457-461.
2. Cottam WW. Adequacy of medical school gross anatomy education as perceived by certain postgraduate residency programs and anatomy course directors. Clin Anat 1999; 12.55-65.
3. Fasel JH, Bader C, Gail]oud P. Anatomy teachtng for medical under- graduates: general practice as a guideline ? the brain. Clin Anat 1999; 12:115-119.
4. Jones DG, Harris RJ. Curriculum developments in Australaslan anatomy departments. Clin Anat 1998; 11:401-409
5. Marks SJ. Information technology, medical educatton, and anatomy for the twenty-first century. Clin Anat 1996; 9:343-348.
6 Teichgraber UK, Meyer JM, Rautenfeld DB. Teaching apphed anatomy to senior medical students with an emphasis on surgery and radiology. Surg Radiol Anat 1996; 18:141-142.
7. Zehr CL, Butler RG, Richardson RJ Students' use of anatomy modules in problem-based medtcal education at McMaster University. Acad Med 1996; 71:1015-1017.
8. Mennm S, Kalishman S, Friedman M, Pathak D, Snyder J. A survey of graduates in practtce from the University of New Mexico's conventional and community-oriented, problem-based tracks. Acad Med 1996; 71: 1079-1089.
9. Moore TE, Kathol MH, Zollo SA, Albanese MA. Comparison of a video- disc system with a conventional film file for medical student teaching. In- vest Radio11993; 28:969-973.
10. Protopapas Z, Siegel EL, Remer BI, et al. Picture archiving and commu- nication system training for physictans' lessons learned at the Baltimore VA Medical Center. J Digit Imaging 1996; 9:131-136.
11. Downie AC. Teaching radiology on the internet. Clin Radio11997; 52:4-7. 12. Jaffe CC, Lynch PJ. Educational challenges. Radiol Clin North Am 1996;
34:629-646. 13. Pastore G, Valentini V, Campioni P, Mareno P. Telecommunications and
multimedia systems in education: what developments for radiology? Rays 1996; 21:290-301.
14. Hollanders Assessing and enhancmg medical students' computer skills. a two-year experience. Bull Med Libr Assoc 1999; 87:67-73.
15. Asgari-Jirhandeh N, Haywood J. Computer awareness among medical students: a survey. Med Educ 1997; 31:225-229.
16 Barley DM, Lautin EM, Amis ES Jr, Lerner ME. A survey of radiology clerkships at teaching hospitals in the United States. Invest Radiol 1994; 29:105-108
17. Milad MP, Henddcks SK, Williford LE. Plan for compensating full-time physicians involved in medical education. Obstet Gyneco11999; 93:614- 618.
18. Olmesdahl PJ. Rewards for teachmg excellence: practtce m South Afri- can medical schools. Med Educ 1997; 31:27-32.
19. Nieman LZ, Donoghue GD, Ross LL, Morahan PS. Implementing a com- prehensive approach to managing faculty roles, rewards, and develop- ment in an era of change. Acad Med 1997; 72:496-504
20. Cruess RL, Cruess SR. Teaching medlcme as a profession rn the service of healing. Acad Med 1997; 72:941-952.
8 7 4