Embed Size (px)
Citation preview

Professional Practice Meeting February 2018
Hepatitis C

Hepatitis C Overview

Hepatitis C Virus
Enveloped, single-stranded RNA virus
6 main genotypes: Rapidly mutating virus makes vaccination design difficult
Type 1a and 1b most common in the US
Type 1 most aggressive
Types 2 and 3 most likely to respond to Interferon
Mixed genotype infections in IVDU population
Type, Dose, Duration of treatment depends on genotype

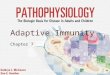
Genotypes 1-6
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC100152/
1a/1b- worldwide (more in US, Europe, Japan) 2: Europe, Japan 3: Asia, India, South America 4: N. Africa (Egypt) 5-6: E. Asia, S. Africa 7-9: E. Asia

Transmission
Via blood products: IV drugs use
Blood transfusions prior to 1992
Clotting factors prior to 1987
Chronic hemodialysis
Needle sticks in hospital settings
Rarely during sexual encounters

Hep C Natural History
30,000 new infections every year in U.S. Acute Phase
This stage lasts up to 6 months approximately 65-75% of people experience no symptoms Symptoms may include fatigue, loss of appetite, jaundice,
nausea, and abdominal pain Symptoms usually clear within several weeks 15-20% undergo spontaneous resolution during this period
(clear all viral RNA)
Chronic Phase 75-80% progress to chronic Hepatitis C Patients likely to be asymptomatic in chronic phase for 20+
years Slow, progressive damage to the liver occurs

Hep C Natural History


Chronic Carriers
Up to 60% develop some liver fibrosis
20% develop cirrhosis within 20-25 years Nausea, loss of appetite, weight loss
Ascites, peripheral edema
Jaundice
Excessive bleeding
Spider veins
Darkening of palms/hands
Mental confusion
Testicular atrophy and/or breast enlargement in men http://www.medpractitioners.com/liver-cirrhosis/

Who to Screen
Universal Screening One time screening for adults born between 1945-1965 75% of those who screen positive were born in this time frame
Selective screening (+1 of the following) Have ever injected illegal drugs Received blood or organs before July 1992 Have received blood products from a donor who later tested positive
for HCV Ever been on chronic hemodialysis Have persistently high ALT Were born to HCV-positive mother Has HIV infection Had needle stick injury or mucosal exposure to HCV infected blood
No recommendation on frequency of selective screening

Hepatitis C Screening Tests
Serum analysis for anti-HCV antibodies Sensitivity >97% AND Specificity of 100% Positive test indicates prior exposure (not necessarily chronic
disease) 3 to 12 weeks for Abs to develop after exposure
If Ab positive, continue with HCV RNA screening Indicates ongoing infection Skip Ab screening and use RNA if suspected recent infection If RNA negative, repeat several months later to confirm
If RNA positive, continue with tests for hepatic fibrosis LFTs, abdominal ultrasound Biochemical markers including APRI
AST/Platelet Ratio Index for information on level of liver fibrosis

To Biopsy or NOT to Biopsy That is the question…

Pre-Treatment Considerations
Vaccination against Hepatitis A+B and Pneumovax23 if not already immunized
Published algorithms to determine type of treatment and duration Based on genotype, cirrhosis status and prior treatments
Additional considerations History of Alcohol Use
Renal impairment
Drug-Drug interactions in those with HIV and HepC co-infection

Hepatitis C Protocol

Pharmacological Treatment Options First Line
Harvoni (ledipasvir/sofosbuvir)
Epclusa (sofosbuvir/velpatasvir)
Zepatier (elbasvir/grazoprevir)
Mavyret (glecaprevir/pibrentasvir)
Alternatives Ribavirin
Peginterferon Alfa-2a
Simeprevir
Daclatasvir
Telaprevir
Viekira Pak (ombitasvir/paritaprevir/ritonavir/dasabuvir)
Technivie (ombitasvir, paritaprevir, ritonavir)
Vosevi (sofosbuvir, velpatasvir, voxilaprevir)

Harvoni
Ledipasvir 90 mg and Sofosbuvir 400 mg
Genotype 1a, 1b, 4, 5, 6
Warnings/Precautions Black Box Warning: Hepatitis B Reactivation
Adverse Reactions Headache; Fatigue; Weakness; Irritability; Nausea
Drug Interactions Amiodarone; Carbamazepine; Rosuvastatin; Proton Pump Inhibitors
Monitoring CBC, INR, LFTs, calculated GFR, HCV genotype and subtype and HCV
viral load at baseline, 4 weeks, and 12 weeks of therapy
Pricing 90-400 mg: $75600 - $113400

Epclusa
Sofosbuvir 400 mg and Velpatasvir 100 mg
Genotype 1a, 1b, 2, 3, 4, 5, 6
Warnings/Precautions Black Box Warning: Hepatitis B Reactivation
Adverse Reactions Headache; Fatigue; Nausea
Drug Interactions Amiodarone; Carbamazepine; Proton Pump Inhibitors; Rosuvastatin;
Atorvastatin
Monitoring CBC, INR, LFTs, calculated GFR, HCV genotype and subtype and HCV
viral load at baseline, 4 weeks, and 12 weeks of therapy
Pricing 400-100 mg: $59808 - $89712

Zepatier Elbasvir 50 mg and Grazoprevir 100 mg
Genotype 1a, 1b, 4
Warnings/Precautions Black Box Warning: Hepatitis B Reactivation
ALT elevations; Hepatic impairment
Adverse Events Fatigue; Headache; Nausea; Insomnia
Drug Interactions Ketoconazole; Rifampin; St John’s Wort; Atazanavir; Cobicistat
Monitoring CBC, INR, LFTs, calculated GFR, HCV genotype and subtype and HCV
viral load at baseline, 4 weeks, and 12 weeks of therapy
Pricing 50-100 mg: $43680 - $54600

Mavyret Glecaprevir 100 mg and Pibrentasvir 40 mg
Genotype 1a, 1b, 2, 3, 4, 5, 6
Warnings/Precautions Black Box Warning: Hepatitis B Reactivation
Hepatic Impairment
Adverse Events Headache; Fatigue; Nausea; Diarrhea
Drug Interactions HMG-CoA reductase inhibitors; Carbamazepine; St John’s Wort
Monitoring CBC, INR, LFTs, calculated GFR, HCV genotype and subtype and HCV
viral load at baseline, 4 weeks, and 12 weeks of therapy
Pricing 100-40 mg: $31680 - $47520

AASLD/IDSA 2017 Guideline Recommendations for Genotype 1 HCV infection
Treatment Naïve Treatment Experienced
Without Cirrhosis With Cirrhosis Without Cirrhosis With Cirrhosis
Harvoni 1 tablet for 8-12 weeks
1 tablet for 12 weeks
1 tablet for 12 weeks
1 tablet + ribavirin for
12 weeks
Epclusa 1 tablet for 12 weeks
1 tablet + ribavirin for 12
weeks Same as naïve
Zepatier 1 tablet for 12 weeks 1 tablet + ribavirin for 16 weeks
Mavyret 3 tablets for 8 weeks
3 tablets for 12 weeks 3 tablets for 12-16 weeks

Limitations to Therapy
Cost
Adherence Patients need to take these medications for 8-12 weeks
Additional Labs/Tests/Monitoring Some drugs require additional steps or therapy modification for
specific genetic make up
Concurrent hepatic impairment
Adverse Reactions
Drug-drug Interactions

Alternatives Drug Name Limitations
Ribavirin Adjunct; Teratogenic; Hemolytic anemia
Peginterferon Alfa-2a “Flu-like” ADR; Several Black Box Warnings
Simeprevir Only treats type 1; No combination; Cannot be used in decompensated cirrhosis
Viekira Pak (ombitasvir/ paritaprevir/ritonavir/dasabuvir)
Cost ($33k/month); Excessive Therapy; Dosage Frequency
Daclatasvir Long Treatment Duration; No combination
Telaprevir Steven-Johnson syndrome; Cannot treat type 1 Technivie (ombitasvir, paritaprevir, ritonavir)
Only for type 4
Vosevi (sofosbuvir/ velpatasvir/ voxilaprevir)
Epclusa showing efficacy without the exposure to voxilaprevir (limiting for hepatic impairment)

Treat Hep C Treat! On the Road to Health Again! Treat Hep C Treat! Because the Meds Really Work this Time!
Get a genotype! A viral load! And no more liver biopsy! Treat, Hep C, Treat! Now at C V I M!

Blood Borne Pathogen Exposure Protocol

CVIM Case Study
“MC” a 25 year old father and patient had a recent exposure.
A friend had been staying at his townhome and MC was cleaning the living room. He went to quickly pick up a hat and felt a sharp prick. That is when he found he had been pricked by a used needle. He then found out his friend had been using drugs at his house. His friend did not know his HIV/Hepatitis
status.
CVIM realized we needed a standard protocol for patients exposed to Blood Borne Pathogens.

Assessing an Exposure
For transmission of a Blood Borne Pathogen (HIV-0.3%, HBV 30%, HCV 1.8%) to occur an exposure must include both of the following: 1. Infectious Body Fluid 2. Portal of Entry

Infectious Body Fluid
Blood, semen, vaginal fluids, amniotic fluids, breast milk, CSF, pericardial fluid, peritoneal fluid, pleural fluid and synovial fluid can transmit HIV, HBV and HCV.
Saliva, urine, feces, sweat, tears, non–bloody emesis and respiratory secretions do not transmit HIV.

Portal of Entry Percutaneous
Increased risk if: hollow bore needles, visibly bloody device, deep injury device used in artery/vein
Mucous membrane Increased risk if large volume exposure
Cutaneous with non intact skin
*you need an infectious body fluid & portal of entry for a risk of transmission to exist

CDC PEP recommendations for Non-occupational Exposures
PEP is Post Exposure Prophylaxis for HIV exposure
CDC recommends prompt initiation of PEP <72 hours after exposure if source is known to be HIV infected and exposure has adequate risk
If exposure <72 hours but source HIV status unknown health care works should assess need for PEP on case by case basis
When patient seeks care >72 hours after exposure PEP is not recommended since window for prevention of transmission has closed

Post Exposure Baseline Labs
Source Person
HIV Ab rapid or HIV Ag/Ab
HCV Ab or HCV RNA
HBS S Ag
RPR
Exposed Person
HIV Ab rapid or HIV Ag/Ab
HCV Ab or HCV RNA
HBV panel
RPR

Follow Up Labs – Exposed Person
Six Weeks (4 weeks in PEP)
HIV 4th gen Ag/Ab
HCV RNA
Four Months
HIV 4th gen Ag/Ab
Anti HCV
**Anti HBV titer if vaccine series was given

Treatment
If a risk of HIV transmission exists patient should receive PEP
If patient has not been vaccinated against HBV they should receive Hep B vaccine and immune globulin, regardless of source status
There is no prophylaxis treatment for HCV Patients should be evaluated the need for
tetanus treatment

Resource
UCSF Needlestick and Exposure Hotline Phone number: 425-353-7842 Hours: 8am-8pm EST

HIV Post Exposure Prophylaxis
For 28 days

Truvada
Tenofovir DF 300 mg and Emtricitabine 200 mg
Warnings/Precautions Black Box Warning: Post-treatment acute exacerbation of Hepatitis B
Decreased bone mineral density; Renal impairment
Adverse Events Headache; Nausea; Dizziness; Insomnia; Weakness; Skin rash
Drug Interactions NSAIDs; Acyclovir; Valacyclovir; Aminoglycosides
Monitoring CBC, renal and hepatic function at baseline and 2 weeks after exposure;
Documented HIV test at baseline and 6 weeks, 12 weeks and 6 months after exposure
Pricing 200-300 mg (30): $2010.95

Raltegravir
Brand Name: Isentress
Warnings/Precautions Myopathy; Skin and hypersensitivity reactions
Adverse Events Headache; Insomnia; Elevations in creatine kinase; Increase serum ALT
Drug Interactions Rifampin
Monitoring CBC, renal and hepatic function at baseline and 2 weeks after exposure;
Documented HIV test at baseline and 6 weeks, 12 weeks and 6 months after exposure
Pricing 400 mg (60): $1800.00

Dolutegravir
Brand Name: Tivicay
Warnings/Precautions Hepatotoxicity; Hypersensitivity reactions
Adverse Events Hyperglycemia; Increase serum ALT; Insomnia; Nausea; Depression
Drug Interactions Carbamazepine; Dofetilide; Phenytoin; Phenobarbital; St. John’s Wort
Monitoring CBC, renal and hepatic function at baseline and 2 weeks after exposure;
Documented HIV test at baseline and 6 weeks, 12 weeks and 6 months after exposure
Pricing 50 mg (30): $1989.13

References
Joshi, SN. Hepatitis C Screening. The Ochsner Journal. 2014; 14(4):664-668. Zein NN. Clinical Significance of Hepatitis C Virus Genotypes. Clinical
Microbiology Reviews. 2000;13(2):223-235. Vercauteren K, de Jong YP, Meuleman P. Animal models for the study of HCV.
Current Opinions in Virology. 2015;13:67-74. Zhao Y-J, Ju Q, Li G-C. Tumor markers for hepatocellular carcinoma. Molecular
and Clinical Oncology. 2013;1(4):593-598. https://www.cdc.gov/hepatitis/hcv/guidelinesc.htm https://www.aafp.org/afp/2014/0915/od1.html http://www.hepctrust.org.uk/information/impact-hepatitis-c-liver/progression-
hepatitis-c/acute-phase-hepatitis-c http://www.hepatitiscentral.com/hepatitis-c/ https://www.uptodate.com/contents/overview-of-the-management-of-chronic-
hepatitis-c-virus-infection?search=hepatitis%20c&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
http://nvhr.org/sites/default/files/.users/u32/HCV%20Initiating%20Treatment%20Guide.pdf