Embed Size (px)
Citation preview

Prof JH van Zyl 2010
01. Central role of liver in drug metabolism
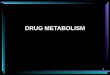
02. Principal reactions in drug metabolism
03. Electron flow pathway in the microsomal drug-oxidizing system
04. Orphan nuclear receptors and drug metabolism
05. Genetic polymorphism of cytochrome P450 and acetylation
06. Consequences of drug biotransformation
07. Drug-drug interactions
08. Effect of cirrhosis on the plasma clearance of diazepam
09. Factors leading to decreased drug metabolism in aging
10. Primary mechanisms of impaired drug metabolism
11. Secondary mechanisms of impaired drug reactions
12. One of the outcomes of drug metabolism is the induction of liver injury
13. Drug-induced liver disease
14. Pathogenesis of drug-induced liver diseases
15. Mechanisms of acetaminophen toxicity
16. Mechanisms of isoniazid hepatotoxicity
17. Halothane hepatitis
18. Drug-induced fatty liver
19. Herbal preparations implicated in hepatotoxicity
20. Diagnosis of drug-induced liver disease
Drugs and liver

1. Isoniazid hepatitis incidence
2. Drug-induced fatty liver
3. Mechanisms of cholestasis
4. Herbal preparations implicated in hepatotoxicity
5. Antecedent liver injury and the use of potentially
hepatotoxic drugs
6. Diagnosis of drug-induced liver disease
7. Management of drug-induced liver disease
Management

Learning Outcomes
1. Know what the liver does to drugs
2. Know how drugs affect the liver
3. Distinguish between the 2 types of drug induced liver disease:
Drug induced hepatitis vs Liver toxins
4. Know what the levels are for “safe” alcohol usage
5. Know the effects of alcohol on the liver
6. Know how to recognise alcohol induced liver disease

Central role of liver in drug metabolism

Principal reactions in drug metabolism

Electron flow pathway in the microsomal drug-oxidizing system

How does the liver affect drugs?
• Change from lipid-soluble to water-soluble
• Takes place in the intracellular space

FACTORS INFLUENCING HEPATIC UPTAKE OF DRUGS
• Protein binding
• Blood flow
• Specific receptor or transport protein

FACTORS INFLUENCING HEPATIC UPTAKE OF DRUGS
• Protein binding
• Weakly or strongly bound to protein

FACTORS INFLUENCING HEPATIC UPTAKE OF DRUGS
• Blood flow
• Normal portal flow in man
= 1000-1200ml/min
• Reduced in cirrhosis
• 100% of blood in portal vein recovered from hepatic vein in
health and only 13% in cirrhosis( 87% via collaterals)

FACTORS INFLUENCING HEPATIC UPTAKE OF DRUGS
• Specific receptor or transport protein

FACTORS INFLUENCING THE ACTIVITY OF DRUG METABOLIZING ENZYMES
• Genetic
• Age
• Drugs
• Disease

FACTORS INFLUENCING THE ACTIVITY OF DRUG METABOLIZING ENZYMES
• Genetic
• Slow and fast acetylation of INH

FACTORS INFLUENCING THE ACTIVITY OF DRUG METABOLIZING ENZYMES
• Age
Table 6-18. Factors Leading to Decreased Drug Metabolism in Aging
Decreased liver blood flow
Decreased liver mass
Pseudo-capillarization
Decline in hepatic oxygenation?

FACTORS INFLUENCING THE ACTIVITY OF DRUG METABOLIZING ENZYMES
• Drugs
• Warfarin and Phenytoin

FACTORS INFLUENCING THE ACTIVITY OF DRUG METABOLIZING ENZYMES
• Disease
• In the metabolizing of the drug –
- Weaker?
- Stonger?

HOW DO DRUGS AFFECT THE LIVER?
• Increased load – Sulphonamides• Disordered metabolism- Anabolic Steroids• Hepatotoxins – C Cl4• Sensitivity
- Hepatitis - INH, Halothane
- Cholestatic – Phenothiazine

HEPATOTOXINS
• Exhibit a distinctive histological pattern for any given hepatotoxin
• Is dose related• Can be elicited in all individuals• Are reproducible in laboratory animals.• Appear after a predictable and brief exposure

HEPATOTOXINS
• Carbon tetrachloride
• Tetracycline
• Aminita phalloides
• Cytotoxic drugs
• Methotrexate
• Paracetamol
• Arsenic

HEPATOTOXINS : PATHOLOGY
• Necrosis
• Fatty infiltration
• Little inflammation

HEPATOTOXINS : CLINICAL FEATURES
• Short latent period
• Symptom of hepatitis without pre-icteric fever
• Anorexia, nausea and vomiting
• Jaundice
• Hepatomegaly

SEVERE TOXIC HEPATITIS
• Intense abdominal pain
• Haematemesis
• Rapid decrease in liver size
• Ascites, oedema
• Bleeding tendency
• Coma
• Uraemia +/-

TOXIC HEPATITIS
• Treatment
- Gastric lavage
- Antidotes
Cysteamine for paracetamol

DRUG INDUCED HEPATITIS
• They cannot be produced in animals
• Only some individuals are at risk
• Severity or occurrence bears no relation to amount consumed
• No relationship to the institution of therapy
• Histology varies
• Often fever, arthralgia, rash and eosinophilia

DRUG INDUCED HEPATITIS: TREATMENT
• Stop offending drug
• Do not rechallenge
• Value of corticosteroids uncertain

DRUG INDUCED HEPATITIS
• Patients with atopic allergy and a history of antecedent reactions to other drugs are at risk
• A drug with other hypersensitivity reactions will sooner or later produce hepatitis in others.

Orphan nuclear receptors and drug metabolism

Genetic polymorphism of cytochrome P450 and acetylation
Table 6-9. Genetic Polymorphism of Cytochrome P450 and Acetylation
Enzyme P450IID6 P450IIC N-Acetyltransferase (NAT)
Designation Debrisoquine/sparteine polymorphism
Mephenytoin polymorphism
Acetylation (INH) polymorphism
Antidepressants Mephobarbital Hydralazine
(Other drugs involved) Antiarrhythmics Hexobarbital Phenelzine
β blockers Omeprazole Procainamide
Codeine, neuroleptics Dapsone
Sulfamethazine
Sulfapyride
Poor metabolism (incidence)
Japanese 5%-10% 18%-23% 40%-70%
Chinese 0%-2% 15%-20% 10%-20%
Whites 5%-10% 2%-5%

Consequences of drug biotransformation

Drug-drug interactions

Effect of cirrhosis on the plasma clearance of diazepam

Factors leading to decreased drug metabolism in aging
Table 6-18. Factors Leading to Decreased Drug Metabolism in Aging
Decreased liver blood flow
Decreased liver mass
Pseudo-capillarization
Decline in hepatic oxygenation?

Primary mechanisms of impaired drug metabolism

Secondary mechanisms of impaired drug reactions

One of the outcomes of drug metabolism is the induction of liver injury

Drug-induced liver disease
Table 6-4. Drug-induced Liver Disease: General Characteristics
Hepatotoxicity
Predictable Unpredictable*
Incidence High Low
Reproducible in animals Usually No
Dose-dependent Yes Rarely
Example Acetaminophen Diphyenylhydantoin
*Metabolic idiosyncrasy, presumably related to formation of toxic metabolite(s) under genetic control.
Hypersensitivity idiosyncrasy, presumably related to immune reaction, ? to metabolite.

Pathogenesis of drug-induced liver diseases

Mechanisms of acetaminophen toxicity

Mechanisms of isoniazid hepatotoxicity

Halothane hepatitis

Drug-induced fatty liver
Table 6-32. Agents Producing Drug-induced Fatty Liver
Macrovesicular
Methotrexate
Allopurinol
Halothane
Isoniazid
α-Methyldopa
Microvesicular
Tetracycline
Valproic acid
Ibuprofen
Pirprofen
Amineptine
Tianeptine
Salicyclic acid
Tamoxifen

Herbal preparations implicated in hepatotoxicity
Table 6-41. Herbal Preparations Implicated as Possible Hepatotoxins *
Common names
Scientific names Folk uses
Possible toxic component Hepatic disorder
Chaparral Larrea tridentata
Cancer, arthritis, bruises, diarrhea, eczema, colds, bronchitis, menstrual cramps, amenorrhea, venereal disease, "blood purifier", emetic, antiseptic, diuretic
Nordihydroguaiaretic acid (DNGA) and other related compounds
Acute and subacute hepatitis
(Creosote bush, greasewood, governadora)
Larrea divaricata
Chinese herbs Coptis senesia Tonic, to remove "toxic products of pregnancy" in neonates
Unknown Unconjugated hyperbilirubinemia
Chuen-Lin (Huang-Lien, Ma Huang)
Coptis japonicum
Yin-Chen Antemesia scoparia
Neonatal jaundice Unknown Potential kernicterus
Comfrey Symphytum officinate
Fatigue, abdominal pain, allergy
Pyrrolizidine alkaloids Venoocclusive disease
Germander Teucrium chamaedrys
Weight control, bitter tonic, appetizer, choleretic, antiseptic
Furano neoclerodane deterpenoids
Reversible acute hepatitis, fatal massive hepatic necrosis
Gordolobo
Verbascum thaprus, senecio longilobus, gnaphalium macounii
Pyrrolizidine alkaloids Potential for venoocclusive disease
Mistletoe Viscum album, phoradendron flavescens
Infertility, asthma, epilepsy, aphrodisiac
β-Phenylethylamine, tyramine, acetylcholine, propionylcholine
Hepatitis with piecemeal necrosis and distortion of lobular architechture
Senna Cassia angustifolia, cassia acutifolia
Laxative or cathartic Senosides, rhein anthron Hepatitis
Skullcap Scuttelaria galericulata
Sedative, anticonvulsant
Hepatitis with centrilobular and bridging necrosis
Valerian (garden heliotrope)
Valerian officinalis
Sedative, hypnotic, spasmolytic, hypotensive
Hepatitis with piecemeal necrosis, chronic aggressive hepatitis with fibrosis
*Herbal teas vary widely in composition and may contain several potential toxins often containing pyrrolizidine alkaloids from Senecio, Symphytum, Crotalaria, or Heliotropum. Intrauterine damage may also result from maternal consumption of these concoctions. Babies may develop toxic liver disease from consuming herbal beverages or milk from mothers taking toxin-containing herbal drinks.

Isoniazid hepatitis incidence

Mechanisms of cholestasis

Antecedent liver injury and the use of potentially hepatotoxic drugs
Table 6-9. Antecedent Liver Injury and the Use of Potentially Hepatotoxic Drugs
Lower dose in hepatically metabolized dose-dependent hepatotoxins
Consider drug binding in plasma and drug-drug interactions
Consider pharmacodynamic effects ie, sedatives and NSAIDs in cirrhotics)
No basis for avoiding unpredictable hepatotoxins, ie, no increased frequency of drug-induced liver disease*
However, greater risk of increased severity of combined liver disease
Thus, need for good baseline liver tests, monitoring of early therapy, and vigilance
*In patients with chronic hepatitis C, there may be a higher incidence of hepatotoxicity to antituberculous and antiretroviral (ritonavir) medications, as well as chemotherapy regimens.

Diagnosis of drug-induced liver disease
Table 6-45. Diagnosis of Drug-induced Liver Disease
High index of suspicion
Careful history of drug intake
Compatible temporal sequence
Short duration of drug use
Clinical/laboratory profile consistent with known pattern (ie, hepatocellular, cholestatic) of drug injury
Use of drug combinations (ie, isoniazid/rifampin/alcohol/acetaminophen) known to predispose to drug toxicity
Age compatible with particular drug toxicity (ie, > 40 for isoniazid; < 20 for valproic acid)
Systemic manifestations (ie, fever, rash, eosinophilia, multisystem involvement)
Liver biopsy consistent with drug-induced injury (not necessarily specific and not always needed)
Exclusion of other causes
Improvement (clinical/laboratory) after cessation of drug use; usually significant fall in transaminases in 2-4 wk for hepatocellular injury, slower with cholestasis
Rechallenge (almost never indicated)

Management of drug-induced liver disease
Table 6-11. Management of Drug-induced Liver Disease
Prompt cessation of suspected drug use*
Specific antidote (ie, N-acetylcysteine for acetaminophen
Supportive therapy for liver disease (ie, management of complications/transplant)
Corticosteroids offer no proven benefit but may be tried in patients with hypersensitivity (vasculitis) not responding to drug withdrawal
Liver transplantation for fulminant hepatic failure (acute liver failure)
*Clinical and b iochemical monitoring may permit early discontinuation of drug use. The frequency and cost/benefit of biochemical monitoring is presently under discussion and requires more study.