Embed Size (px)
Citation preview

Program made possible by an unrestricted educational grant provided by
The Dannon Company, Inc and Yakult Honsha Co., Ltd
Practical Applications
of Probiotics in Health and Disease
Proceedings of the Symposium
American College of Nutrition49th Annual Meeting

Table of Contents
a note fromDr. W. Allan WalkerW. Allan Walker, MD 2
Frequently Asked Questions 3
The Potential Use for Probiotics in HealthMary Ellen Sanders, PhD 4
Probiotics and PediatricsW. Allan Walker, MD 6
Probiotics and Inflammatory Bowel DiseaseStefano Guandalini, MD 8
Can Probiotics Help the Elderly?Simin Meydani, DVM, PhD 10
a note fromDr. W. Allan Walker
Probiotics are a diverse group of live microbes defined by FAO/WHO as “live microorganisms which when administered in sufficient quantities can confer a health benefit.” The field of probiotics is an evolving field. Used historically around the world for health promotion and therapeutic purposes, probiotics have now become mainstream in the United States and are part of a huge food and supplement market.
Research continues to emerge, supporting the use of different probiotic strains in a variety of conditions. The research now suggests that these “healthy” bacteria have beneficial effects on gastrointestinal dysfunctions, including diarrhea, as well as the immune system and conditions such as allergy, in children, adults, and the elderly.
Recently, at the 49th Annual Meeting of the American College of Nutrition, experts in the field of probiotics shared new data and insights on the “Practical Applications of Probiotics in Health and Disease.”
The potential use for probiotics in maintaining health, improving health, and in the treatment of conditions such as Inflammatory Bowel Disease were discussed throughout the lifespan.
Please enjoy highlights from the program in this executive summary. You are also invited to view the webcast at, http://nutrition.med.harvard.edu, and http://www.usprobiotics.org.
Sincerely,
W. Allan Walker, MD
Division of Nutrition Harvard Medical School
Practical Applications of Probiotics in Health and Disease2
Frequently Asked Questions
What is the origin of probiotics?
Typically, probiotics are isolated from a number of different sources. Some are isolated from fermented dairy products; others are isolated from human fecal samples, mucosal samples, and breast milk. Others, such as Saccharomyces boulardii is a yeast isolated from animals, which is not a native colonizer. In addition, currently there are no genetically modified probiotics on the market.
Are probiotics regulated by FDA?
In the FDA, probiotics fall under DSHEA as the regulatory category. Claims on products under DSHEA are required to be truthful and not misleading. It is therefore not an unregulated category. One can argue if it is regulated less than it should be, but the framework of DSHEA was to allow a fairly less difficult path to market for products that are considered to be safe. When products are used to cure disease then they should be considered drugs and regulated differently.
Since these organisms are not normally found in our GI systems, is there a way to alter the diet to encourage them to remain in the intestine longer?
There are substances in the diet that can affect the stimulus of endogenous bacteria, but there is no evidence of a nutritional way of maintaining or enhancing a probiotic. The only way to maintain a probiotic, is to continually provide it.
QA
QA
Q
A
Are probiotics “generally recognized as safe” (GRAS)?
Probiotics are a diverse group of organisms and therefore would not be called GRAS across the board as a group. It is important to look at who a probiotic is being administered to, at what levels, and to know what the safety parameters are of the specific genus and species that is being administered. Products that are on the market today have supposedly been through appropriate safety assessments.
What are appropriate levels of probiotics?
It is best to look to the literature to see what has been clinically tested as effective. There is a broad range of levels that have been utilized for different strains of probiotics and that have shown efficacy in clinical trials. There is not a standardized recommendation at this time. Some probiotics have shown efficacy at 100 million per day, whereas others have been effective at trillions per day.
QA
QA
ProbioticsWeb Cast
available athttp://nutrition.med.harvard.edu & www.usprobiotics.org/webcast.asp
Practical Applications of Probiotics in Health and Disease3

What are Probiotics?Probiotics were defined in 2001 by a group convened by FAO/WHO Expert Consultation as live microorganisms, which when administered in adequate amounts confer a health benefit on the host. The important characteristics of this definition are that the organisms need to be alive and must have been shown in a controlled, human study to confer a health benefit; otherwise they are not probiotics. Some studies have also documented health effects with cellular components of microorganisms, but these are not considered probiotics, because they are not alive. Not all live organisms or “live cultures” are probiotics because not all have been shown to have a health benefit. Additionally, probiotics are a diverse group of microorganisms. The most familiar ones in the United States are Lactobacillus, Bifidobacterium, Saccharomyces, a yeast, and Bacillus.
It is also important to recognize that not all probiotics are the same. Probiotics are identified by genus, such as Lactobacillus or Bifidobacterium, and then by species of each genus. The genus Lactobacillus, for example, has dozens of species including Lactobacillus acidophilus or Lactobacillus casei. Furthermore, within each species, there are different strains, such as Lactobacillus acidophilus NCFM or Lactobacillus acidophilus La-1. Different strains
of the same species can have different characteristics, strengths and weaknesses. It is important to recognize that the clinical support to substantiate claims must be specifically based on each probiotic strain or blend of strains that are used.
A clinical illustration of this was shown in a study conducted in Israel with children 4-10 months of age in childcare centers. This study compared two different probiotic organisms, Lactobacillus reuteri ATCC 55730 and Bifidobacterium lactis Bb-
12. Different characteristics of the health of the children were observed over a 12-week period. The Bifidobacterium lactis Bb-12 strain showed improvements in episodes of fever and diarrhea and days of diarrhea, but the Lactobacillus reuteri ATCC 55730 strain was more broadly effective.
The Potential Use for Probiotics in Health Mary Ellen Sanders, PhD
Mary Ellen Sanders, PhD
is an internationally recognized
consultant in the area of probiotic
microbiology, and owner of Dairy
and Food Culture Technologies.
She consults on all aspects of
probiotic applications in the food and
supplement industries. Dr. Sanders
also serves on the newly created
Product Quality Working Group of
the NIH National Advisory Council
for Complementary and Alternative
Medicine.
Are Live Cultures the Same as Probiotics?Live cultures are microbes that are used to make fermented foods such as cheese, cultured cottage cheese, yogurt, kefir, fermented milks, vegetables, fermented meats, bread, beer, and wine. In some cases, cultures stay alive in foods prior to consumption, especially in dairy products, and these foods are, therefore, a source of live cultures. But not all live cultures are probiotics, because not all live cultures have undergone the evaluation to show that they impart health effects. They may have health effects, but in terms of making a strong recommendation, just because something has live cultures does not mean it will have a particular physiological effect in humans.
Dose of Probiotics is ImportantAnother important consideration in looking at the field of probiotics is dose. Unfortunately one number cannot be given as a “minimum dose” across the board for all probiotics. This is because the effective dose will differ depending on the strain, the consumer and the health endpoint being tested. In addition, oftentimes the dose-dependency of effects for products has not been established, so if results are beneficial at one tested level, a lower level may not have the same effect. Thus, the minimum level of individual probiotics used in products must be based on levels found to be efficacious in human studies.
To illustrate the broad range of effective doses for different probiotics, Lactobacillus reuteri ATCC 55730 and Bifidobacterium infantis 35264 have both been shown in clinical studies to be effective at 1x108 (100 million)/day, whereas VSL#3, a probiotic used in the recurrence of pouchitits, is used at 1.8x1012 (1.8 trillion)/day.
Role of Colonizing Microbiota in Health Human bodies are highly colonized. There are 1014 microbial cells associated with the human body, which are in the mouth, intestine, vagina, and on the skin. This is about 10-fold higher than the human cells that comprise our bodies. The organisms are also quite diverse with 1000’s of different bacterial species that have been identified in the intestine. In addition, the metabolic capacity of the combined microbiota is estimated to be about 100 times greater than what human genes encode.
In 2004, Bäckhed, et al. captured the significance of this saying, ‘the microbiota can be viewed as a metabolic “organ” exquisitely tuned to our physiology that performs functions that we have not had to evolve on our own.’ Scientists are realizing that this symbiotic evolution of microbes along with man is a very important one for human physiology.
Physiologically, these native, colonizing bacteria have different
Executive Director, International Scientific Association for Probiotics and Prebiotics (ISAPP), Consultant, Dairy and Food Culture Technologies
Practical Applications of Probiotics in Health and Disease4

functions, including protective functions, structural functions, and metabolic functions. The protective functions have also been referred to as colonization resistance since properly colonized animals are more resistant to infection. Protective functions include displacing pathogens, competing for receptor sites with pathogens, competing for nutrients, and production of antimicrobial substances.
The structural functions include impact on immune system development, reinforcement of intestinal barrier effects, and effects on intestinal cell health and development. Metabolically, microbes can aid in digestion. Fibers, which are non-digestible foods that make it through the small intestine and into the colon, can be substrates for growth for the colonizing microbes, and can contribute to overall energy humans extract from foods. Preliminary studies have identified a distinct microbiota that is associated with obese people, which is different from what has been associated with lean people. Colonizing microbes also produce organic acids, such as short chain fatty acids, which inhibit pathogens. In addition, they synthesize vitamins, increase mineral absorption, increase or decrease pH, detoxify carcinogens, and can salvage energy. Probiotic bacteria can use some of these same mechanisms to impact human physiology.
“Maintaining Health” in Healthy People with ProbioticsSome studies suggest that probiotics can have a role in keeping people healthy. As an example, one randomized, double-blind, placebo-controlled study looked at healthy adult workers in Sweden. Subjects were fed the probiotic Lactobacillus reuteri or a placebo and the number of workplace absences was recorded. Those fed probiotics were statistically less likely to report sick to work.
Another study that was done in healthy subjects looked at the effects of a mixture of probiotic strains on episodes of colds in adults. The results showed that compared to the control, the probiotic consumers had reduced number of days of illness, of total bronchial symptoms, and of days with fever. Another study, with infants with colic, who were otherwise healthy, were fed the probiotic Lactobacillus reuteri ATCC 55730 for 28 days and showed significant reduction in crying time.
Probiotics in the Marketplace In the marketplace, an underlying fact is that not all products that are called “probiotic” are probiotic. There are numerous probiotic foods and supplements currently available. Some are
more substantiated by scientific evidence than others. Regular yogurt, for example, might not have adequate levels of probiotics to provide any probiotic benefit. It can be difficult for consumers to sort through which of these are validated probiotic products and which are not. In general, the best recommendation for choosing a product is to buy from a trusted company that readily shares information with consumers and health care professionals on the content and efficacy substantiation for its products. Additional
recommendations can be found at www.isapp.net.
ConclusionsProbiotics are a diverse group of live microbes that have been tested in humans and shown to have health effects. It must be recognized that these effects are strain-specific as well as dose-specific. The strongest recommendations are for products that have been tested in humans and shown to have the desired benefit. Colonizing microbiota are important to health in a variety of ways and probiotics may bolster some of their effects. Research on the horizon will develop a better understanding of the concepts of how colonizing microbes and probiotics can influence health.
Practical Applications of Probiotics in Health and Disease5

Probiotics and PediatricsW. Allan Walker, MD
W. Allan Walker, MD is the Conrad
Taff Professor of Nutrition and Pediatrics
at Harvard Medical School (HMS) and
Professor of Nutrition at the Harvard School
of Public Health. He is the Chairman of the
Division of Nutrition, Principal Investigator
of an NIH-funded Clinical Nutrition Research
Center at HMS and Director of the Mucosal
Immunology Laboratory at Massachusetts
General Hospital for Children (MGHfC).
His research interests include defining the
role of initial bacterial colonization in the
development of intestinal host defense
and determining the protective effects of
breastfeeding in the prevention of disease
in neonates.
Initial Bacterial ColonizationThe initial bacterial colonization of the intestinal tract is important to health. In utero, the epithelium is very immature and turns over slowly, with a lack of lymphoid elements. In contrast, once an infant has entered the extra-uterine environment, there is a mature, actively turning over epithelium with all the subclasses of epithelial cells and an abundance of lymphoid elements. This underscores the importance of the initial colonization of the development of the gastrointestinal tract in the infant.
Under normal circumstances, the fetus leaves a germ-free environment and naturally delivers through the birth canal where it picks up a healthy bolus of bacteria from the mother’s colonic and vaginal cavities. With the introduction of feeding, these bacteria are stimulated and proliferate. They then change slightly with weaning when breast or formula feeding is transitioned to solid foods, so that by 18 months to 2 years of age, the intestine is completely colonized and remains with the infant
for life.
The number of bacteria that have been identified within the intestine ranges between 400 and 1000 different strains. This is 10-fold greater than the total number of cells in the body, which is why the intestine is sometimes considered a separate organ of the body. Under normal colonized conditions, the large diverse intestinal flora exists in a balanced ecosystem where health-promoting bacteria balance potential pathogens and there is no expression of disease.
Development of Host DefenseAs a function of gestation, the various immune components of the intestine develop differently. For example, a specific form of epithelium, the microfold cell is formed, which facilitates antigens and bacteria from crossing into aggregates of lymphoid elements and Peyer’s patches. Interstitial and interepithelial lymphocytes are also formed. These cells are all developed at
birth, but they do not function until they are stimulated initially by colonizing bacteria. The colonizing bacteria stimulate the lymphoid elements, so that they mature, produce both protective and regulatory cytokines and secretory IgA.
IgA is a protective immunoglobulin that coats mucosal surfaces and balances T-helper cell response. Healthy full-term newborns are deficient at birth and it takes a finite amount of time for protective levels to be produced, which requires that the first two stages of bacterial colonization occur.
Another factor in the development of host defense is oral tolerance. Oral tolerance is defined as the down regulation of systemic immunity after oral exposure to “harmless” bacteria and antigens. It is one of the most important mature mechanisms of the intestinal tract because it discerns between potential hazardous antigens and organisms, which require an acute inflammatory response to contain and innocuous antigens and bacteria, which should not cause an immunologic response.
Clinical Consequences of Inadequate ColonizationIn 2002, the New England Journal of Medicine published a review article that compared the disease burden over the last half century with regard to infections versus immune disorders. The epidemiological evidence showed that in developed countries there has been a striking decrease in infectious diseases, such as hepatitis, tuberculosis, measles, and mumps. Unfortunately, this has been substituted by a shifting paradigm in disease, where there is an increase in immune mediated diseases, such as allergy and autoimmune diseases like Type 1 Diabetes and Crohn’s Disease.
This observation has been explained by the “Hygiene Hypothesis,” which states that due to a decreased exposure to microorganisms during infancy, the mucosal immune system fails to develop properly resulting in aberrant responses to allergens and autoantigens leading to an increase in disease burden.
One large study looked at infants who were born in a sterile, urban environment without pets or siblings and who had very little exposure to microorganisms compared to infants who were born in a rural farm setting, with animals and lots of exposure to microorganisms. Symptoms of allergy, including wheezing, hay fever, and positive responses to outdoor and indoor antigens were considerably higher in those who were born in an urban setting, strongly suggesting that lack of exposure to organisms in infancy is a factor in the development of disease.
In the past decades, additional factors have contributed to
Conrad Taff Professor of Nutrition and Pediatrics, Harvard Medical School, Director, the Mucosal Immunology Laboratory, Massachusetts General Hospital for Children, Boston, MA
Practical Applications of Probiotics in Health and Disease6

inadequate initial colonization. These include premature delivery, cesarean section, and an inappropriate use of perinatal antibiotics. One study in animals, which provided the broad-spectrum antibiotic, kanamycin, during the perinatal period, showed that there is a much higher development of IgE antibodies, the basis for allergic disease, than those not given antibiotics.
In another study, mothers without a family or self history of allergy, who delivered naturally, were compared to, 1) mothers who had allergy or a family history of allergy and delivered naturally, and 2) mothers who had allergy or a family history of allergy and delivered by cesarean section. The mothers in the first group were found to have two and a half times the risk of having allergy, while the mothers in the second group had almost an 8-fold increase in risk of allergy. This illustrates the importance of initial colonization in the development of disease.
Probiotics as “Surrogates” for Colonization Under circumstances, such as incomplete colonization or excessive use of antibiotics, there can be a shift in the ecologic balance of bacteria in the intestine, which makes one much more susceptible to disease. When incomplete colonization occurs, however, it has been suggested that probiotics can act as a surrogate for colonization. With the addition of probiotics, a balanced system can be restored as long as the probiotics are continuously used as their effects are transient. The bacteria that have been used most commonly as probiotics in pediatrics and studied the most are Bifidobacterium lactis Bb12 and Lactobacillus rhamnosus GG.
All babies are born with an imbalanced immune response to protect them from rejection in utero, so they have an imbalanced Th2-helper cell system, which favors the development of allergy. With colonization and stimulus of other immune cells, there is a balance and no expression of disease. A number of studies have shown that when there is a persistent Th2 response, using probiotics can stimulate Th1 response and cause a balance, helping to prevent allergy.
Probiotics in Treatment and Prevention of Pediatric DiseaseOral probiotics have also been shown to reduce the incidence and severity of necrotizing enterocolitis (NEC) in very low birth weight infants. NEC is a condition in which there is a very high inflammatory response with a low ability to break down inflammatory cytokines with appropriate enzymes. A number of studies have looked at the effectiveness of probiotics in helping to ameliorate and reduce this condition. A study published in Pediatrics showed that when Bifidobacteria and Lactobacillus were used in 1500 gram or smaller infants, they had decreased mortality and morbidity compared to the control group. In addition, when exposed to human fetal enterocytes in culture, these same probiotics modulated the inflammatory response, making it more similar to a mature intestine.
In one study the introduction of Lactobacillus GG in the latter stages of pregnancy, continued though lactation, produced a striking reduction in expression of atopic dermatitis even at two and four years. This suggests when probiotics are introduced early, in a situation where there might be inadequate colonization, the process may be reversed. Additional studies suggest that probiotics may be effective in the treatment of allergy.
Many studies have also shown that probiotics are effective
in reducing the duration and the severity of acute diarrhea. The use of antibiotics can produce symptoms of diarrhea in many children and adults causing a condition called antibiotic-associated diarrhea (AAD). When Saccharomyces boulardii was provided to children, there was a significant decrease in the side effects of antibiotic therapy.
ConclusionsThe field of probiotics is an evolving field so we do not yet have all of the answers. Probiotics have been shown to be very effective in the field of pediatrics. It is important, however, to be aware of the specific strain of probiotic, the dose of probiotic, and the condition for which the probiotic has been shown to be clinically effective. When these factors are taken into consideration, probiotics may be helpful in the prevention and treatment of different conditions, including allergy and NEC.
Practical Applications of Probiotics in Health and Disease7

Probiotics and Inf lammatory Bowel Disease Stefano Guandalini, MD
Stefano Guandalini, MD is
Professor of Pediatrics, Chief, Division
of Gastroenterology, Hepatology and
Nutrition, University of Chicago Comer
Children’s Hospital. Dr. Guandalini is
an internationally recognized expert on
celiac disease and is also known for his
expertise in the research and treatment of
other diarrheal diseases in children. His
clinical and research efforts have greatly
influenced the way celiac disease is
diagnosed and treated today. Dr. Guandalini
created the University of Chicago Celiac
Disease Center in response to the low rate
of celiac disease detection in the United
States. Selected from a worldwide pool of
candidates, Dr. Guandalini is the first and
currently past President of FISPGHAN (The
Federation of International Societies for
Pediatric Gastroenterology, Hepatology,
and Nutrition).
Inf lammatory Bowel DiseaseInflammatory Bowel Disease (IBD) is an uncurable disease of unknown pathogenisis that leads to one in 10,000 being newly diagnosed every year in the United States. It contributes to morbidity, but mortality is not as extensive. The main diseases that are grouped under Inflammatory Bowel Disease include Crohn’s disease and Ulcerative Colitis. Crohn’s disease may involve any part of the gastrointestinal tract from the mouth to the anus and inflammation is defined as transmural, which means that it penetrates across the bowel wall and beyond. Ulcerative Colitis (UC) is by definition limited to the colon and inflammation is limited to the mucosal layer with a different appearance and histology.
In the pathogenesis of IBD, several factors come together. Presence of disease susceptibility genes are better characterized for Crohn’s disease, but they are also known for UC, and depending on their combination, you can have a predisposition to just IBD genetically, or more specifically to UC or Crohn’s disease. The interplay of environmental factors, including smoking and luminal bacteria can also be present. Germ-free animals have shown that unless there are bacteria in the gut, IBD models cannot be developed. There are also some genes that determine the phenotype of the
disease, for instance the response to treatment and the location of disease.
Why Would Probiotics be Effective in Inf lammatory Bowel Disease?Probiotics induce several beneficial host responses. They
are known to regulate host homeostasis by interfering with bacterial pathogens, producing antibacterial substances, and even competing for receptor sites. They also enhance innate immunity by decreasing the production of pro-inflammatory cytokines and increasing the production of anti-inflammatory cytokines. They improve the enterocyte health by increasing the barrier integrity and preventing cytokine-induced apoptosis. Research has given a lot of support to the theory that probiotics may have a role in balancing all the inflammation in Crohn’s disease and in UC.
Evidence from Animal Models in Inf lammatory Bowel DiseaseEvidence from animal models of Ulcerative Colitis have shown effectiveness. For example, orally administered culture media from Bifidobacterium infantis acutely reduced colonic permeability in mice. Long-term treatment in interleukin-10 deficient mice attenuated inflammation, normalized colonic permeability, and decreased colonic and splenic interferon-gamma secretion. The oral administration of lactic acid bacteria (8 strains) to mice inhibited colon shortening and inflammatory activities in models of colitis.
Human Data and Inf lammatory Bowel DiseaseThere is only one placebo-controlled study in adults (n=11) that used Lactobacillus GG looking at Crohn’s disease. It showed no statistical difference in the number and severity of relapses. In children, an open label study was performed using Lactobacillus GG for six months in four subjects. Intestinal permeability was looked at over time because studies have shown that children with Crohn’s disease do have a baseline increase, especially paralleling disease severity. A progressive decline in permeability was initially seen, but it reverted after six months despite continuing administration of Lactobacillus GG. All four children in the study, however, experienced a dramatic improvement in disease activity as was measured by PCDAI score.
In a larger population of children (n=79), remission of Crohn’s disease was then studied in a randomized, double-blind trial of Lactobacillus GG versus placebo in addition to standard maintenance therapy. The probability of not relapsing was not improved with probiotics. A recent meta-analysis that appeared
Professor of Pediatrics, Section Chief, Pediatric Gastroenterology, Hepatology, and Nutrition,Director, University of Chicago Celiac Disease Center
Practical Applications of Probiotics in Health and Disease8

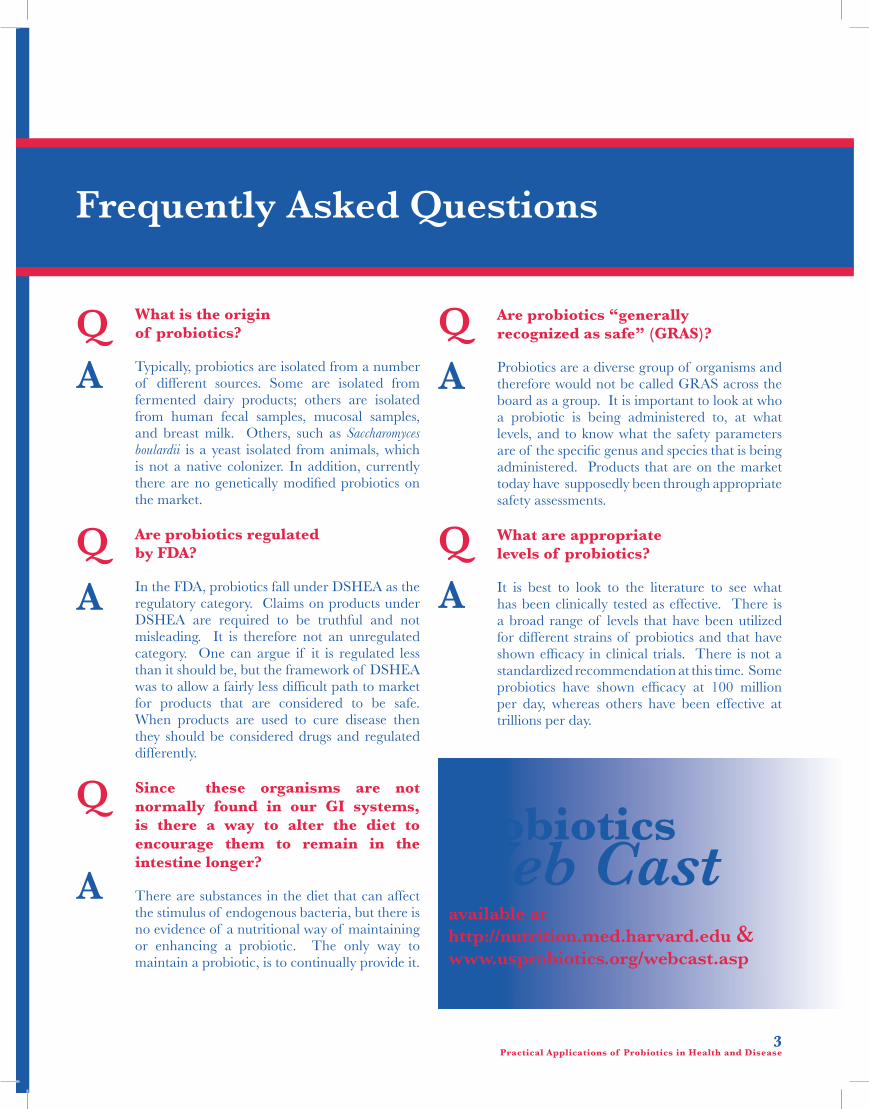
Probiotic Administration in Patients with Ileal Pouch for Ulcerative Colitis is Associated with Expansion of Mucosal Regulatory Cells
0 3 6 120.0
0.5
1.0
1.5
2.0
2.5
VSL#3 Control
Pou
chit
is D
isea
se A
ctiv
ity
Ind
ex
Time(Months)
in the Cochrane Library on the use of probiotics in Crohn’s disease also showed no significant difference.
There are more data published looking at maintenance of remission in Crohn’s disease using various strains, such as Escherichia coli Nissle, Lactobacillus GG, as well as VSL#3, in which subjects were looked at endoscopically. Again, all studies showed no change in remission. Remission in Crohn’s disease after surgery was also studied and did not show any differences.
The induction of remission in Ulcerative Colitis, however, may be affected by the use of probiotics. One study out of Italy using VSL#3 and another out of Japan using a mixture of Lactobacillus and Bifidobacterium showed that the UC index and histology were significantly improved in these studies. Most studies looking at maintenance of remission in UC did not show effectiveness, while one using a mixture of Lactobacillus and Bifidobacterium did show a significantly better outcome, but it was an open-label study.
Pouchitis and ProbioticsPouchitis is the most common of complications in patients with UC after surgery. If UC becomes out of control, the total colon must be removed. The colon is resected in the anus and the ileum is pulled down to create a “J-pouch,” which is attached to the remaining muscles in the rectum. The idea is to create a container for stools, thereby improving general well being and
causing less frequent defecation and the need for an ostomy bag. This has been the treatment of choice for patients in the past 15 years. There is a problem, however, because the pouch can get inflamed often. It’s been thought that this is an inflammatory condition, but it probably originates from the disarray of microbes as the ileum was probably not meant to deal with massive amounts of microbes. Prevention, induction of remission, and maintenance of remission of pouchitis have all been studied using VSL#3. All studies showed statistically significant improvement compared to placebo. A recent study from Italy also showed positive results using VSL#3 as there was expansion of mucosal regulatory cells, which correlated very well with clinical outcomes.
Conclusions on Probiotics in IBDThere is a robust pathophysiological basis for potential use of probiotics and data in animal models supports this. With Crohn’s disease, however, it is possible that the right probiotic may not have been found, because the results thus far have been disappointing. On the other hand, in Ulcerative Colitis there is marginal but significant evidence of efficacy of some strains in inducing or maintaining remission in adults. There is strong evidence of efficacy in pouchitis especially with the use of VSL#3 in adults, and there is an emerging possibility of promising efficacy in children.
Practical Applications of Probiotics in Health and Disease9

Can Probiotics Help the Elderly? Simin Meydani, DVM, PhD
Simin Meydani, DVM, PhD is
Associate Director and Senior Scientist
at the Jean Mayer USDA Human Nutrition
Research Center on Aging at Tufts
University. She is also a Professor of
Nutrition at Tufts School of Nutrition and
Immunology at the Sackler Graduate School
of Biomedical Sciences. Her specific area
of research examines changes that occur
in the immune system in response to aging
and various nutrients. Dr. Meydani has
coauthored several influential studies that
have appeared in key medical journals.
Probiotics, Immune Response and Infection in the Elderly The number of people over the age of 60 is increasing worldwide. One of the major problems that the elderly face is a dysregulation of the immune response, which predisposes them to infectious diseases as well as to cancer. The type of infections that are critical to the elderly include respiratory infections such as tuberculosis, pneumonia and influenza, gastrointestinal infections, urinary tract infections, and Herpes zoster, which all contribute to higher morbidity and mortality in the aged. There is also an increase in incidence and mortality from cancer and other immune related diseases.
Elderly are More Susceptible to Infectious DiseaseThere have been many studies that have shown a consistent increased susceptibility to infectious diseases among the aged, across all species, and there are many reasons that contribute to this. Chief among them is impaired immune response, particularly in T cell-mediated function, increased pathogen virulence in the aged host, and perhaps a change in gut microflora.
With aging, the immune response changes and there is evidence that all cells of the immune system show some age related change. The major changes occur in T cell mediated function, which is a key factor in predisposition to infectious disease and cancer. The indices of T cell mediated function have been shown to be good indicators of morbidity and mortality in the elderly. One study administered a test of the T cell mediated function, delayed type hypersensitivity skin response, in a group of healthy elderly and then followed them for ten years. They found that the people who were anergic, or did
not have a good immune response, had twice as much mortality compared to those who did have a functioning immune response. A similar relationship was also seen when death due to sepsis was studied.
About 25% of lymphoid tissue in the body is found in the gut and it
accounts for over 50% of the body’s immune function. Not much is known about the age related changes in the gut-associated immunity in humans. Gut biopsies from healthy, young subjects were studied and showed that the interepithelial lymphoid cells did not show age-related changes, but the lamina propria lymphocytes showed a significant reduction in production of the cytokine, IL-2 and in the proliferative ability of T cells. This suggests that the gut-associated immune response also shows age-related changes similar to what is seen in the peripheral response.
Increased pathogen virulence in the elderly is another reason why they may be more susceptible to infectious disease. It has been shown that the benign species of CVB3/0 virus put into a vitamin E or selenium deficient host has nucleotide changes and mutates to a virulent type. Since selenium and vitamin E deficiency are conditions which are associated with increases in oxidative stress, which is also observed in the elderly, the possibility of viral mutation occurring in an aged host was studied.
A series of experiments by our laboratory showed that avirulent CVB3/0 placed into a young or old host, separated, and then put back into a young host, resulted in different outcomes in the young host depending on whether they had been put in the old or young host. The virus that had originally been placed in the young host did not cause any disease, whereas the virus originally passed into the old host, resulted in significantly increased viral titer, high pathology and mortality in the young host. Sequencing showed that the virus passed from the young host did not show any changes in viral genome nucleotides sequence compared to the avirulent virus, whereas the virus that was passed through an old host showed several nucleotide changes that made it look similar to the nucleotide sequence of the virulent type. This suggested that by passing the virus through an old host, there was a mutation occurring in the virus which made it more virulent. These results provide a new paradigm by which the elderly are more susceptible to infectious diseases.
Additionally, there is the possibility that the elderly experience changes in gut microflora, which could make them more susceptible to infectious diseases. There is not much data available, but some studies suggest that with aging, there is a decrease in the number and diversity of beneficial bacteria, such as Bifdobacteria, whereas there is an increase in the number and species of harmful bacteria. It is not clear if this contributes to more susceptibility of disease. Gut Microf lora, Aging, and ProbioticsThe mechanism by which the gut microflora changes with age is not known, but it could be due to: 1) changes in mucin composition in the elderly; 2) a decline in immune response, which would allow for more of the harmful bacteria to proliferate; 3) excessive use of antibiotics; 4) dietary changes; and 5) other factors such as gut bacterial mutations similar to what is seen with viral mutations.
Associate Director, Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University, Boston, MA
Practical Applications of Probiotics in Health and Disease10

Probiotics, Immune Response and Infection in ElderlyThe theories by which probiotics could increase resistance to infectious diseases include improvement in the immune response, particularly that of the T cell-mediated function in the aged, decreased virulence of pathogens in the aged host, or by changing the gut microflora. Most of the research, thus far, has focused on the effect of probiotics on improving the immune response. However, little is known about the effects of probiotics on the immune response of elderly.
One double-blind, placebo-controlled study, which supplemented with Lactobacillus rhamnosus HN001 (5x1010 CFUs/day) or Bifidobacterium lactis HN109 (5X 109 CFUs/day) for 3 weeks, showed that daily ingestion of probiotics improved innate defense capacity in healthy middle-aged people. The cytotoxicity of natural killer (NK) cells significantly increased with both strains during the 3-week supplementation and declined after the probiotic supplementation was stopped, indicating the necessity for continued use of probiotics for the effect to be maintained. The percentage of NK cells also increased, more so with the Bifidobacterium lactis HN109, and the phagocytic ability of both mononuclear cells and polymorphic mononuclear cells was significantly increased. In addition, the probiotics showed more of an effect as age increased.
Another study looked at 3 cups per day of fermented milk that contained Lactobacillus casei DN114001 (108cfu/ml) on the innate defense capacity in healthy middle-aged people (45, 51-58 years old) in a double-blind, placebo-controlled study for 8 weeks. Similarly, an increase in NK cytotoxicity was seen, as well as an increase in monocyte oxidative burst.
The effect of Lactobacillus casei DN114-001 on all types of winter infection was studied in 180 subjects over 60 years old. Over 3 weeks, 100 mL of Actimel was provided twice daily. There was no effect seen on the incidence of winter infection, but the duration of infection was shorter. A study in adults (n=479) using a mixture of probiotics over three months during the winter looked at the duration and severity of common colds. They found similar results in that there was a reduced duration of colds by two days and a decrease in fever, which was associated with an increase in percent cytotoxic T cells.
Probiotics and Antibiotic Associated DiarrheaAntibiotic associated diarrhea (AAD) is diarrhea associated with antibiotic use caused by Clostridium difficile that is common in
hospitalized patients with broad spectrum antibiotic use. Symptoms include diarrhea for at least 48 hours occurring within two months of antibiotic use. Antibiotics cause a disruption of the normal intestinal microbiota, which act as barriers to colonization of pathogenic bacteria. The incidence and mortality of this condition is high in the elderly. It prolongs hospitalization stay and costs as well as the risk of other infections.
Several studies have looked at the effect of probiotics on AAD.
In 2006, in a meta-analysis of probiotic use in AAD, over half of the 25 randomized controlled studies (52%) showed significant decrease of AAD. It was also found that 44% of the studies showed efficacy in adults, whereas 67% showed efficacy in children. In addition, when AAD due to Clostridium difficile was looked at, two of six studies were effective. Various probiotics and doses were utilized in each study included in the meta-analysis.
A later study looking at supplementation of probiotics and AAD found about an 80% risk reduction in occurrence, while in 2007, Hickson, et al. provided a probiotic yogurt drink (100ml x 2/d) containing 4 probiotics for one week longer than antibiotic therapy and found a significant reduction in diarrhea as well as Clostridium difficile infection in 135 elderly subjects.
ConclusionsThe elderly have an impaired immune response which predisposes them to high incidence of morbidity and mortality from infectious diseases. Few studies have evaluated the effect of probiotics on the immune response of the elderly, but those conducted thus far suggest that they could be beneficial. Longer-term randomized, double-blind, placebo-controlled human trials with adequate numbers of elderly subjects and clinically relevant outcomes as well as studies in animal models will help to confirm these data.
Practical Applications of Probiotics in Health and Disease11

Akobeng AK. Review article: the evidence base for interventions used to maintain remission in Crohn’s disease. Aliment Pharmacol Ther. 2008 Jan 1;27(1):11-18. Epub 2007 Oct 5.
Bach JF. The effect of infections on susceptibility to autoimmune and allergic diseases.N Engl J Med. 2002 Sep 19;347(12):911-920.
Bäckhed, et al. The gut microbiota as an environmental factor that regulates fat storage. PNAS 2004 101:15718-15723.
Blaut, et al. Probiotics and the Intestinal Microflora: What Impact on the Immune System, Infections and Aging? Current Nutrition and Food Science. Vol. 2, No. 1, February 2006, pp. 79-95(17).
Braat H, et al. Lactobacillus rhamnosus induces peripheral hyporesponsiveness in stimulated CD4+ T cells via modulation of dendritic cell function. Am J Clin Nutr. 2004 Dec;80(6):1618-1625.
Braun-Fahrlander, et al. Prevalence of hay fever and allergic sensitization in farmer’s children and their peers living in the same rural community. Clinical & Experimental Allergy, 1999, Volume 29, Number 1, January, pp. 28-34(7).
Christou et al. Estimating mortality risk in preoperative patients using immunologic, nutritional, and acute-phase response variables. Annals of Surgery. 1989 Jul; 210(1): 69-77.
Claud EC and Walker WA. Hypothesis: inappropriate colonization of the premature intestine can cause neonatal necrotizing enterocolitis. FASEB J. 2001 Jun;15(8):1398-1403.
De Vrese M. et al. Effect of Lactobacillus gasseri PA 16/8, Bifidobacterium longum SP 07/3, B. bifidum MF 20/5 on common cold episodes: a double blind, randomized, controlled trial. Clinical Nutrition. 2005 Aug; 24(4): 481-491.
Douglas LC and Sanders ME. Probiotics and prebiotics in dietetics practice. J Am Diet Assoc. 2008 Mar;108(3):510-521. Review. Erratum in: J Am Diet Assoc. 2008 Aug;108(8):1381.
Eggesbø M. Is delivery by cesarean section a risk factor for food allergy? J Allergy Clin Immunol. 2003 Aug;112(2):420-426.
Ewaschuk JB, et al. Secreted bioactive factors from Bifidobacterium infantis enhance epithelial cell barrier function. Am J Physiol Gastrointest Liver Physiol. 2008 Nov;295(5):G1025-1034.
Fedorak RN and Dieleman LA. Probiotics in the treatment of human inflammatory bowel diseases: update 2008. J Clin Gastroenterol. 2008 Jul;42 Suppl 2:S97-103. Review.
Gaya DR. New genes in inflammatory bowel disease: lessons for complex diseases? Lancet. 2006 Apr 15;367(9518):1271-1284.
Gay et al. An aged host promotes the evolution of avirulent coxsackievirus into a virulent strain. PNAS, USA. 2006; Sep. 12; 103(37): 13825-13830.
Gill et al. Dietary probiotic supplementation enhances natural killer cell activity in the elderly: an investigation of age-related immunological changes. Journal of Clinical Immunology. 2001 Jul; 21(4): 264-271.
Gill et al. Enhancement of immunity in the elderly by dietary supplementation with the probiotic Bifidobacterium lactis HN019. American Journal of Clinical Nutrition. 2001 Dec; 74(6): 833-839.
Gupta P, et al. Is lactobacillus GG helpful in children with Crohn’s disease? Results of a preliminary, open-label study. J Pediatr Gastroenterol Nutr. 2000 Oct;31(4):453-457.
Hickson M, et al. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomised double blind placebo controlled trial. BMJ. 2007 Jul 14;335(7610):80.
Hopkins, MJ and Macfarlane, GT. Changes in predominant bacterial populations in human faeces with age and with Clostridium difficile infection. Journal of Medical Microbiology. 2002 May; 51(5): 448-454.
Indrio, et al. The Effects of Probiotics on Feeding Tolerance, Bowel Habits, and Gastrointestinal Motility in Preterm Newborns. The Journal of Pediatrics , Vol. 152 , Issue 6 , Pp. 801-806.
Isaacs K and Herfarth H. Role of probiotic therapy in IBD. Inflamm Bowel Dis. 2008 Nov;14(11):1597-1605.
Ishikawa H, et al. Randomized controlled trial of the effect of bifidobacteria-fermented milk on ulcerative colitis. J. Am. Coll. Nutr. 2003; 22: 56-63.
Kalliomaki M, et al. Probiotics in primary prevention of atopic disease: a randomised placebo-controlled trial. Lancet. 2001 Apr 7; 357(9262): 1076-1079.
Kalliomaki M, et al. Probiotics and prevention of atopic disease: 4-year follow-up of a randomised placebo-controlled trial. Lancet. 2003 May 31; 361(9372): 1869-1871.
Kato K, et al. Randomized placebo-controlled trial assessing the effect of bifidobacteria-fermented milk on active ulcerative colitis. Aliment. Pharmacol. Ther. 2004; 20: 1133-1141.
Kotowska M, et al. Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea in children: a randomized double-blind placebo-controlled trial. Aliment Pharmacol Ther. 2005 Mar 1;21(5):583-590.
Lee HS, et al. Lactic acid bacteria inhibit proinflammatory cytokine expression and bacterial glycosaminoglycan degradation activity in dextran sulfate sodium-induced colitic mice. Int Immunopharmacol. 2008 Apr;8(4):574-580.
Lin HC, et al. Oral probiotics reduce the incidence and severity of necrotizing enterocolitis in very low birth weight infants. Pediatrics. 2005 Jan;115(1):1-4.
McFarland LV. Meta-analysis of probiotics for the prevention of antibiotic associated diarrhea and the treatment of Clostridium difficile disease. Am J Gastroenterol. 2006 Apr;101(4):812-822.
Murosaki S, et al. Heat-killed Lactobacillus plantarum L-137 suppresses naturally fed antigen-specific IgE production by stimulation of IL-12 production in mice. J Allergy Clin Immunol. 1998 Jul;102(1):57-64.
O’Hara AM and Shanahan F. Gut microbiota: mining for therapeutic potential. Clin Gastroenterol Hepatol. 2007 Mar;5(3):274-284. Review.
O’Hara and Shanahan. The gut flora as a forgotten organ. EMBO reports. 2006. 7: 688-693.
Parra MD, et al. Daily ingestion of fermented milk containing Lactobacillus casei DN114001 improves innate-defense capacity in healthy middle-aged people. Journal of Physiology and Biochemistry. 2004 Jun; 60(2): 85-91.
Prescott SL, et al. Development of allergen-specific T-cell memory in atopic and normal children. Lancet. 1999 Jan 16;353(9148):196-200.
Pronio A, et al. Probiotic administration in patients with ileal pouch-anal anastomosis for ulcerative colitis is associated with expansion of mucosal regulatory cells. Inflamm Bowel Dis. 2008 May;14(5):662-668.
Sanders ME. Probiotics: definition, sources, selection, and uses. Clin Infect Dis. 2008 Feb 1;46 Suppl 2:S58-61; discussion S144-151.
Schultz M, et al. Lactobacillus GG in inducing and maintaining remission of Crohn’s disease. BMC Gastroenterol. 2004 Mar 15;4: 5.
Selner, JC et al. Salivary immunoglobulin and albumin: development during the newborn period. Journal of Pediatrics. 1968 May; 72(5): 685-689.
Turchet P, et al. Effect of fermented milk containing the probiotic Lactobacillus casei DN-114001 on winter infections in free-living elderly subjects: a randomised, controlled pilot study. Journal of Nutrition, Health, and Aging. 2003; 7(2): 75-77.
Tubelius P, et al. Increasing work-place healthiness with the probiotic Lactobacillus reuteri: a randomised, double-blind placebo-controlled study. Environmental Health. 2005 Nov 7; 4: 25.
Vanderpool C, et al. Mechanisms of probiotic action: Implications for therapeutic applications in inflammatory bowel diseases. Inflamm Bowel Dis. 2008 Nov;14(11):1585-1596.
Van Niel CW, et al. Lactobacillus therapy for acute infectious diarrhea in children: a meta-analysis. Pediatrics. 2002 Apr;109(4):678-684.
Wayne SJ, et al. Cell-mediated immunity as a predictor of morbidity and mortality in subjects over 60. J Gerontol. 1990 Mar;45(2):M45-48.
Weizman Z, et al. Effect of a probiotic infant formula on infections in child care centers: comparison of two probiotic agents. Pediatrics. 2005 Jan;115(1): 5-9.
Wenus C, et al. Prevention of antibiotic-associated diarrhoea by a fermented probiotic milk drink. Eur J Clin Nutr. 2008 Feb;62(2):299-301. Epub 2007 Mar 14.
Zoumpopoulou G, et al. Lactobacillus fermentum ACA-DC 179 displays probiotic potential in vitro and protects against trinitrobenzene sulfonic acid (TNBS)-induced colitis and Salmonella infection in murine models. Int J Food Microbiol. 2008 Jan 15;121(1):18-26. Epub 2007 Nov 6.
ProbioticsWeb Cast
available at:http://nutrition.med.harvard.edu & www.usprobiotics.org/webcast.asp
Suggested Reading