Embed Size (px)
Citation preview
14th HKKI CONFERENCE
DRIVING IMPACTS IN LABORATORY MEDICINE
PROCEEDING BOOK
UDAYANA UNIVERSITY PRESS

Complete electrolyte profileNa, K, Cl, iCa, iMg
Whole blood, plasma, serum,urine, and CSF samples
1-minute stat testing
Optional 10-position autosampler
Exceptional Simplicity in a New Generation Electrolyte Analyser
Introducing an advanced technology electrolyteanalyser that has all sensors combined in a single, replaceable, no maintenance card for a simpler, easier analyser.
Easy to Use and MaintainNova’s advanced technology analyser consists of a nomaintenance MicroSensor card that contains all sensors and a ready-to-use, snap-in calibrator cartridge thatcontains all reagents and a waste container.
Nova MicroSensor cards and calibration cartridges offer a true nomaintenance solution for electrolyte testing.
Indonesia Exxcluusive DistribuutorPT. Tamara Overseas Corpporindo
Jl. Pinangsia Timur no : 49, Jakarta 11110 . FAX : 021-6251689, 6901932 email : [email protected]

14th Himpunan Kimia Klinik Indonesia (HKKI)
Conference
Driving Impacts in Laboratory Medicine
Proceeding Book
Himpunan Kimia Klinik Indonesia (HKKI)
2018
14th HKKI CONFERENCE “ Driving Impacts in Laboratory
Medicine
Editor:
dr. I Putu Yuda Prabawa, S.Ked
Reviewer:
Dr. dr. Sianny Herawati, SpPK
Dr. dr. I Nyoman Wande, SpPK
30 + viii hal
ISBN 978-602-294-294-8
Hak Cipta Dilindungi Undang-Undang
Dilarang memperbanyak, mencetak, dan menerbitkan sebagian atau
seluruh isi buku ini dengan cara dan dalam entuk apapun juga tanpa
seizing penulis dan penerbit
Diterbitkan pertama kali oleh
Udayana University Press, Juli 2018
SAMBUTAN KETUA PENGURUS PUSAT HIMPUNAN KIMIA
KLINIK INDONESIA
Himpunan Kimia Klinik Indonesia (HKKI) yang
sudah terbentuk sejak tahun 1980 menjadi suatu
wadah tempat berkumpul semua stakeholder yang
berkecimpung dalam dunia kimia klinik di
Indonesia, mulai dari para peneliti, praktisi,
industri, maupun pemasok.
Misi dari HKKI antara lain menjadi sarana untuk berbagi ilmu,
keterampilan, dan pengalaman di bidang kimia klinik yang mencakup
semua uji laboratorium maupun penelitian yang didasari reaksi kimia
yang terkait dengan kesehatan manusia.
Kegiatan ilmiah sehubungan dengan Konferensi Kerja keempatbelas
HKKI di Sanur, Bali yang diadakan pada tanggal 19-21 Juli 2018
merupakan salah satu acara untuk mencapai misi tersebut. Selain
dalam bentuk simposia, terdapat juga berbagai lokakarya (workshop),
termasuk manajemen laboratorium.
Semoga berbagai kegiatan ilmiah dalam Konker ke-14 tersebut
bermanfaat untuk pengembangan diri maupun institusi¸ termasuk
bidang industri.
Selamat mengikuti.
Salam sejahtera,
July Kumalawati
Ketua Pengurus Pusat HKKI 2016-2019
Ii
WELCOME ADDRESS FROM THE CHAIRMAN OF 14TH
HKKI CONFERENCE
Dear Colleagues and Friends,
On behalf of the organizing committee of 14th HKKI
Conference, I would like to extend our welcome to
Bali, Indonesia. It is with great pleasure that we
welcome you to the conference. It is a honor for HKKI
Bali to once again become host of the conference.
The theme of 14th HKKI conference is Driving Impacts in Laboratory
Medicine. This conference will cover the interesting subjects, including
infertility, women’s health, oncology, infections, geriatry, and kidney
disease. The programs include exciting and informative plenary lecturer,
symposia, education workshops, poster presentations, and exhibition.
We extend our great appreciation to the member of HKKI, and board of
PDS PatKLIn, IDI, and PATELKI from sabang to merauke. I as
chairman, would like to thanks to the members of the organizing
committee for the work in the preparation of this conference.
Since Bali is famous for its rich culture and beautiful mature, we hope all
of you enjoy at Bali.
DAFTAR ISI
A. A. Wiradewi Lestari
Chairman of 14th HKKI Conference 2018
Iii

DAFTAR ISI
Kata Sambutan ketua HKKI ....................................................... i
Kata Sambutan ketua Panitia ...................................................... ii
Daftar Isi ................................................................................... iii
Susunan Panitia.......................................................................... iv
Susunan Acara ........................................................................... vi
Abstrak Pembicara Simposium ................................................... 1
Abstrak Presentasi Poster ........................................................... 25
Ucapan Terimakasih .................................................................. 30
Iiii
SUSUNAN PANITIA
Penasihat : dr. July Kumalawati, SpPK, DMM
Ketua : Dr. dr. A.A. Wiradewi Lestari, SpPK
Wakil Ketua : Dr. dr. Nyoman Wande, SpPK
Sekretaris : Dr. dr. Sianny Herawati, SpPK
Wakil Sekretaris : Made Putra Semadhi, S.Si, M.Farm
Bendahara : Sri Paulani, S.Si, Apt., MSM.
Wakil Bendahara : dr. Ni Kadek Mulyantari, SpPK(K)
Dr. Ni Ketut Puspasari
Seksi Acara : dr. I.A. Putri Wirawati SpPK(K)
dr. Ni Komang Ayu Parmawati
dr. Made Minarti Witarini Dewi
Luh Putu Bintang Utami, Amd.A.K
Ni Luh Candra Wati, Amd.A.K
Seksi Penggalangan : Dr. dra. Ellis Susanti, MM., M.Pd, M.Si., Apt
Dana Dr. Theresia Roesli, SpPK
Seksi Ilmiah : Prof. Dr. Rahajuningsih D. Setiabudi, SpPK
Dr. Tjan Sian Hwa, SpPK
Dr. Dewi Muliaty, M.Si
Dr. dr. I Wayan Putu Sutirta Yasa, M.Si
dr. I Putu Sidhi rastu Karyana
dr. Ni Komang Krisnawati
D.G.D Dharmasanti, S.Si., M.Kes., Apt.
Dewita Narolita, S.Farm, Apt.
Iiv
Febriyanti, Amd. A.K
Seksi Akomodasi : Dr. dr. A.A.N. Subawa, M.Si
dan perlengkapan dr. A.A.A. Lydia Prawita
dr. Ivan Master Worung
Seksi Dokumentasi : dr. I Made Dharma Pramana
dan publikasi
Seksi Konsumsi : dr. Ni Nyoman Mahartini, SpPK(K)
Ni Wayan Meni
Seksi Sekretariat : dr. Komang Juwita Endrawati
Pendaftaran Ketut Adi Santika, Amd.A.K.
A.A. Wira Santhi Gayatri, Amd. A.K.
Kadek Desy Kartika, S.Si
Iv
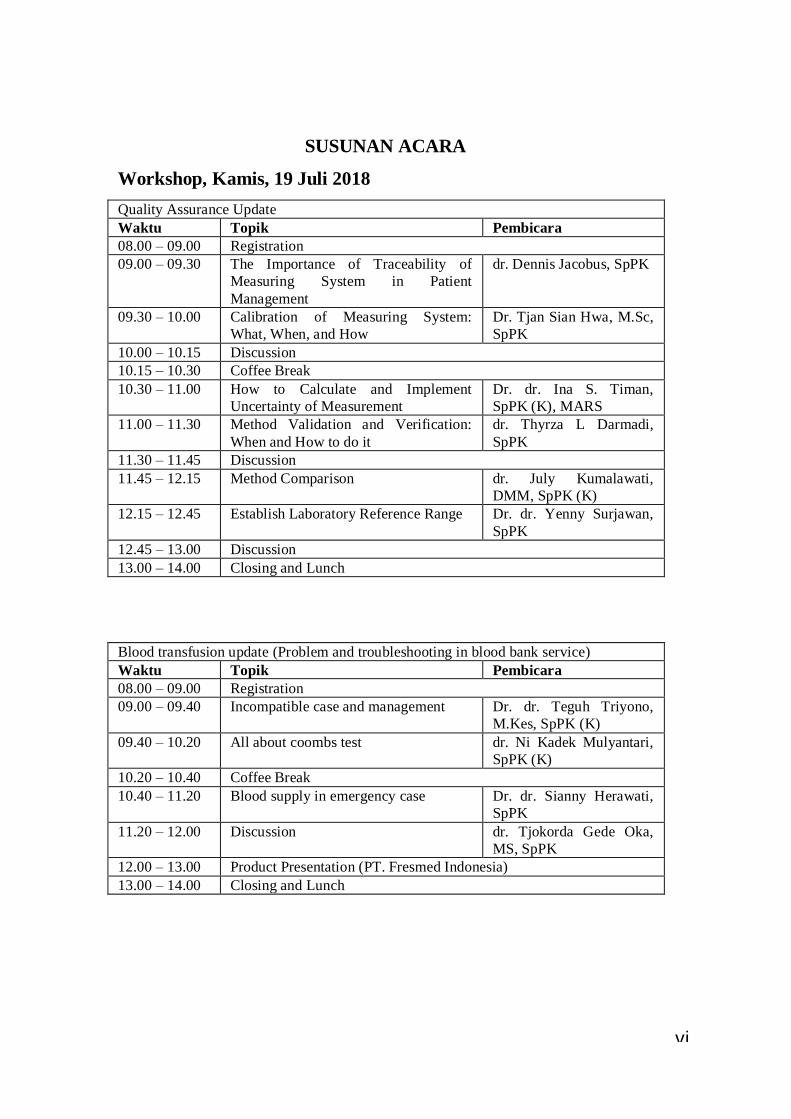
SUSUNAN ACARA
Workshop, Kamis, 19 Juli 2018
Quality Assurance Update
Waktu Topik Pembicara
08.00 – 09.00 Registration
09.00 – 09.30 The Importance of Traceability of
Measuring System in Patient
Management
dr. Dennis Jacobus, SpPK
09.30 – 10.00 Calibration of Measuring System:
What, When, and How
Dr. Tjan Sian Hwa, M.Sc,
SpPK
10.00 – 10.15 Discussion
10.15 – 10.30 Coffee Break
10.30 – 11.00 How to Calculate and Implement
Uncertainty of Measurement
Dr. dr. Ina S. Timan,
SpPK (K), MARS
11.00 – 11.30 Method Validation and Verification:
When and How to do it
dr. Thyrza L Darmadi,
SpPK
11.30 – 11.45 Discussion
11.45 – 12.15 Method Comparison dr. July Kumalawati,
DMM, SpPK (K)
12.15 – 12.45 Establish Laboratory Reference Range Dr. dr. Yenny Surjawan,
SpPK
12.45 – 13.00 Discussion
13.00 – 14.00 Closing and Lunch
Blood transfusion update (Problem and troubleshooting in blood bank service)
Waktu Topik Pembicara
08.00 – 09.00 Registration
09.00 – 09.40 Incompatible case and management Dr. dr. Teguh Triyono,
M.Kes, SpPK (K)
09.40 – 10.20 All about coombs test dr. Ni Kadek Mulyantari,
SpPK (K)
10.20 – 10.40 Coffee Break
10.40 – 11.20 Blood supply in emergency case Dr. dr. Sianny Herawati,
SpPK
11.20 – 12.00 Discussion dr. Tjokorda Gede Oka,
MS, SpPK
12.00 – 13.00 Product Presentation (PT. Fresmed Indonesia)
13.00 – 14.00 Closing and Lunch
Ivi
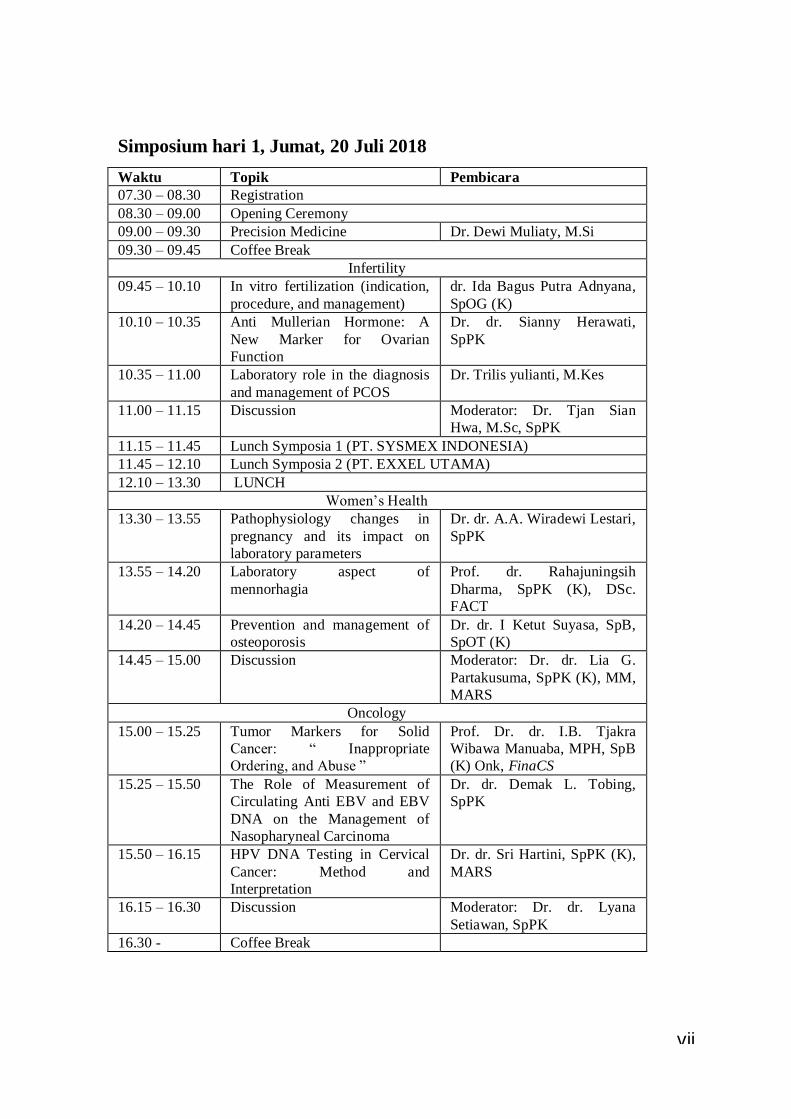
Simposium hari 1, Jumat, 20 Juli 2018
Waktu Topik Pembicara
07.30 – 08.30 Registration
08.30 – 09.00 Opening Ceremony
09.00 – 09.30 Precision Medicine Dr. Dewi Muliaty, M.Si
09.30 – 09.45 Coffee Break
Infertility
09.45 – 10.10 In vitro fertilization (indication,
procedure, and management)
dr. Ida Bagus Putra Adnyana,
SpOG (K)
10.10 – 10.35 Anti Mullerian Hormone: A
New Marker for Ovarian
Function
Dr. dr. Sianny Herawati,
SpPK
10.35 – 11.00 Laboratory role in the diagnosis
and management of PCOS
Dr. Trilis yulianti, M.Kes
11.00 – 11.15 Discussion Moderator: Dr. Tjan Sian
Hwa, M.Sc, SpPK
11.15 – 11.45 Lunch Symposia 1 (PT. SYSMEX INDONESIA)
11.45 – 12.10 Lunch Symposia 2 (PT. EXXEL UTAMA)
12.10 – 13.30 LUNCH
Women’s Health
13.30 – 13.55 Pathophysiology changes in
pregnancy and its impact on
laboratory parameters
Dr. dr. A.A. Wiradewi Lestari,
SpPK
13.55 – 14.20 Laboratory aspect of
mennorhagia
Prof. dr. Rahajuningsih
Dharma, SpPK (K), DSc.
FACT
14.20 – 14.45 Prevention and management of
osteoporosis
Dr. dr. I Ketut Suyasa, SpB,
SpOT (K)
14.45 – 15.00 Discussion Moderator: Dr. dr. Lia G.
Partakusuma, SpPK (K), MM,
MARS
Oncology
15.00 – 15.25 Tumor Markers for Solid
Cancer: “ Inappropriate
Ordering, and Abuse ”
Prof. Dr. dr. I.B. Tjakra
Wibawa Manuaba, MPH, SpB
(K) Onk, FinaCS
15.25 – 15.50 The Role of Measurement of
Circulating Anti EBV and EBV
DNA on the Management of
Nasopharyneal Carcinoma
Dr. dr. Demak L. Tobing,
SpPK
15.50 – 16.15 HPV DNA Testing in Cervical
Cancer: Method and
Interpretation
Dr. dr. Sri Hartini, SpPK (K),
MARS
16.15 – 16.30 Discussion Moderator: Dr. dr. Lyana
Setiawan, SpPK
16.30 - Coffee Break
Ivii

Simposium hari 2, Sabtu, 21 Juli 2018
Waktu Topik Pembicara
09.00 – 09.30 Methodology and technology for
therapeutic drug monitoring and
drug of abuse testing
Dr. Raja Elina Raja Aziddin
09.30 – 09.45 Coffee Break
Infections
09.45 – 10.10 Updates on MoH policy in
tuberculosis, hepatitis, and HIV
infection
Dr. dr. Lia G Partakusuma,
SpPK (K), MM, MARS
10.10 – 10.35 Reporting viral load of HIV:
result comparability of different
tests
dr. July Kumalawati, DMM,
SpPK (K)
10.35 – 11.00 Pitfalls in serology test methods Prof. Dr. Jusak Nugraha, dr,
MS, SpPK (K)
11.00 – 11.15 Discussion Moderator: dr. Anugrah Sitta
Latumahina, SpPK
11.15 – 12.45 ISHOMA
Geriatry
12.45 – 13.10 The impact of ageing on
laboratory parameters
Prof. dr. Suzanna Imanuel,
SpPK (K)
13.10 – 13.35 Laboratory Diagnosis of
Alzheimer’s Disease
Dr. dr. I Nyoman Wande,
SpPK
13.35 – 14.00 Laboratory investigations in
stroke
Dr. dr. Yenny Surjawan,
SpPK
14.00 – 14.15 Discussion Moderator: Dr. Dewi Muliaty,
M.Si
Kidney Disease
14.15 – 14.40 Update on glomerular filtration
rate markers: Cystatin C,
Creatinin clearance, and eGFR
Dr. dr. Indranila K.S., SpPK
(K)
14.40 – 15.05 Novel biomarker for Kidney
Diseases: Liver-fatty Acid
Binding Protein (L-FABP)
Prof. Dr. Marzuki
Suryaatmadja, SpPK (K)
15.05 – 15.30 Therapeutic drug monitoring in
renal transplant patients
Dr. Raja Elina Raja Aziddin
15.30 – 15.55 Discussion Moderator: Dr. Tjan Sian
Hwa, SpPK, MSc
15.55 – 16.30 Closing ceremony and coffee break
Iviii
1
ABSTRAK PEMBICARA SIMPOSIUM

2
PRECISION MEDICINE
Dewi Muliaty
PT Prodia Widyahusada Tbk
(Clinical Labs and Clinics)
Precision medicine (PM) mulai dikenal ketika Presiden Obama meluncurkan Precision
Medicine Initiative pada tahun 2015 di Amerika Serikat. PM Initiative merupakan suatu
upaya riset jangka panjang yang melibatkan National Institutes of Health (NIH) dan
berbagai pusat penelitian lainnya, dengan tujuan untuk memahami bagaimana peran gen,
lingkungan, dan gaya hidup dapat membantu menetapkan pendekatan terbaik untuk
mencegah dan mengobati penyakit pada setiap individu. Pendekatan ini diharapkan
dapat digunakan untuk memprediksi strategi pengobatan dan pencegahan penyakit
tertentu yang lebih akurat pada sekelompok orang tertentu. Hal ini bertolak belakang
dengan pendekatan “one-size-fits-all” dengan strategi pengobatan dan pencegahan yang
berlaku sama bagi semua orang, kurang mempertimbangkan adanya perbedaan diantara
individu. Para peneliti berharap pendekatan ini akan meluas ke banyak bidang kesehatan
dan pelayanan kesehatan di masa yang akan datang. Sebelumnya dikenal pula istilah
“personalized medicine” yang mengaitkan pengobatan dan pencegahan unik untuk
setiap individu. Belakangan istilah Precision Medicine digunakan untuk pendekatan
yang berorientasi pada faktor genetik, lingkungan, dan gaya hidup.
“Pharmacogenomics” merupakan bagian dari PM yang mempelajari bagaimana gen
dapat mempengaruhi respon obat secara individual. Tujuan jangka pendek PM Initiative
ini adalah meningkatkan pengetahuan tentang genetik dan biologi kanker untuk
menemukan pengobatan baru yang lebih efektif; sedangkan tujuan jangka panjang PM
Initiative adalah menyebarkan PM kepada semua bidang kesehatan dan pelayanan
kesehatan dalam skala yang besar. Jika pendekatan PM menjadi bagian dari pelayanan
kesehatan rutin, maka dokter dan pelayan kesehatan lainnya perlu mengetahui lebih
dalam tentang genetika molekuler, yang akan meningkatkan kemampuan interpretasi
hasil tes genetik, memahami bagaimana menyampaikan informasi yang relevan untuk
pendekatan pengobatan dan pencegahan bagi pasien.

3
IN VITRO FERTILIZATION: INDICATION, PROCEDURE AND
MANAGEMENT
Ida Bagus Putra Adnyana1,2
1Obstetrics and Gynecology Dept.- Reproductive endocrinology and Fertility
subdivision, Medical Faculty of Udayana University/ Sanglah Hospital 2Royal IVF Clinic - Bali Royal Hospital (BROS)
Infertility is a disease of the reproductive system defined by the failure to achieve
a clinical pregnancy after 12 months or more of regular unprotected sexual
intercourse. Worldwide, infertility affects approximately 10–15% of couples. The
major causes of female infertility include ovulatory dysfunction (20–40%), tubal and
peritoneal pathology (30–40%), and male factors (30–40%); and the rest were
unexplained.
IVF consisting a sequence of steps that start with controlled ovarian hyper-
stimulation, followed by oocytes retrieval, fertilization in the laboratory, trans-
cervical transfer of embryos into the uterus followed by luteal support. Indication for
IVF including primary or secondary infertility caused by female or male factors,
recurrence failure of IUI, and immunology related infertility.
Initial procedure for IVF consist of routine infertility tests, medical condition
assessment, infectious diseases screening and treatment. For male, Sperm analysis,
and anti-sperm antibody testwere done commonly. Pelvic organ examination with
physical examination, SIS, hysteroscopy and laparoscopy. Ovarian reserve
assessment with FSH, E2, inhibin B and the AMH is recommended.
The management of IVF patients were depended on their responses to
stimulation, whether its poor, sub-optimal, normal or hyper-responder.
Keywords: In Vitro Fertilization (IVF), infertility, IVF management

4
ANTI-MULLERIAN HORMONE (AMH): A NEW MARKER FOR OVARIAN
FUNCTION
Sianny Herawati
Departemen Patologi Klinik Fakultas Kedokteran Universitas Udayana /
RSUP Sanglah Denpasar
Anti-Mullerian Hormone (AMH) is a homodimeric glycoprotein linked by disulfide
bonds, belongs to the Transforming Growth Factor (TGF) beta superfamily. AMH is
produced by gonadal tissue namely testicular Sertoli cells and ovarian granulosa cells
especially pre-antral and antral follicles. AMH involved in sexual differentiation of male
embryo, inducing regression of Mullerian duct, embryological precursor of female
reproductive tract. In females, AMH has an inhibitory effect on primordial follicle
recruitment and on the responsiveness of the growing follicles to FSH.
There are multiple roles of AMH in females and males, AMH reflect ovarian
follicular reserve in variety of clinical situation such as infertility treatment (assisted
reproductive technology), sensitive marker for ovarian aging, valuable tool in diagnosis
and recognition of recurrence granulosa cell tumors, marker of ovarian dysfunction
especially polycystic ovary syndrome, impact obesity in AMH level, AMH could be
used as tumor inhibitor and role of AMH in male infertility.
Keyword: Anti-Mullerian Hormone

5
PATHOPHYSIOLOGY CHANGES IN PREGNANCY AND ITS IMPACT ON
LABORATORY PARAMETERS
A.A.Wiradewi Lestari
Departemen Patologi Klinik Fakultas Kedokteran Universitas Udayana /
RSUP Sanglah Denpasar
Numerous physiological changes occur during pregnancy to accommodate the maternal
and fetal needs. Most of these changes begin soon after conception and continue until
late gestation. Not surprisingly, these physiologic adaptations of pregnancy result in
many significant changes in laboratory test values. Some of these changes are well-
known, such as the reduction in hematocrit and hemoglobin levels, which is termed
physiological or dilutional anemia of pregnancy. Similarly, the renal changes leading to
lower creatinine values in pregnancy are well-described. Pregnancy is known to be a
state of “physiologic anemia” due to the disproportionate increase in plasma volume
relative to red blood cell volume. This increase in blood volume is necessary to supply
the fetus and placenta and begins very early in pregnancy. The red cell volume
increaseprompted by a higher level of erythropoietin. Thus, despite a higher red cell
volume, the hematocrit will fall during pregnancy. Other hematologic changes in
pregnancy include an increase in white blood cells, particularly neutrophils, and a slight
decrease in platelet count.. Platelets, on the other hand, remain in the normal non-
pregnant range but mean platelet counts may be slightly lower than in healthy non-
pregnant women. There are also many changes in blood chemistries during pregnancy as
well, mostly by the same dilutional mechanism as the hematocrit. Important among
these are albumin, total protein and creatinine. Both albumin and total protein decrease
by about 1g/dL by mid-pregnancy and creatinine decreases by about 0.3mg/dL. Alkaline
phosphatase levels, continue to rise during normal pregnancy. Similarly, the upper limit
of normal for D-dimer nearly doubles from the first to the third trimester. Several
hormones and coagulation factors all increase markedly.
Keywords : Pathophysiology, Pregnancy, Laboratory parameters

6
LABORATORY ASPECT OF MENORRHAGIA
Rahajuningsih Dharma Setiabudy
Prodia PRN
Menorrhagia is menstruation at regular cycle interval but with excessive blood flow
(>80 ml) and duration. Generally menorrhagia is associated with gynecological
disorder such as uterine fibroid or myoma, hormonal imbalance or iatrogenic such as
IUD or warfarin therapy. In the past decade, hemostasis disorders have been
recognized as underlying of menorrhagia. The most common hemostasis disorders
associated with menorrhagia is von Willebrand’s disease (vWd), while other platelet
function disorders, idiopathic thrombocytopenic purpura, and acquired hemophilia
are relatively rare. Von Willebrand factor is a large glycoprotein (MW 230 – 20.000
kD), which function in platelet adhesion and carrier of factor VIII. Von Willebrand’s
disease is a hereditary disorder that can be classified as type 1, type 2 which is
subclassified as 2A, 2B, 2M, and 2N, and type 3. In addition, acquired vWd, platelet
type vWdwere also recognized. Laboratory diagnosis in vWd consist of bleeding
time, platelet count, ristocetin induced platelet aggregation (RIPA), von Willebrand
factor antigen (vWF:Ag), vWFRistocetin cofactor (vWF:RCof), factor VIII, and
multimer analysis.
Key words: menorrhagia, von Willebrand’s disease, platelet function disorders,
acquired hemophilia, ITP

7
PREVENTION AND MANAGEMENT OF OSTEOPOROSIS
I Ketut Suyasa
Faculty of Medicine Universitas Udayana
Osteoporosis as a skeletal disorder characterized by compromised bone strength
predisposing to an increase risk of fracture. Osteoporosis can affected quality of life due
to fracture and postural change. This condition is due to imbalance between bone
formation and bone resorption. It is common in postmenopausal women and the men
over the age 60. The gold standard diagnosis is by measurement of bone mineral density
(BMD) at the hip and lumbar spine. Osteoporosis, defined by BMD less than or equal to
2.5 standard deviations below the mean BMD of a young-adult reference population.
Prevention programmeand treatment is needed to combat the disease. Prevention
strategies include lifestyle changes, addressing secondary factors and pharmacological
therapy. Lifestyle changes programmeare good nutrition, physical activities, eliminate
alcohol, eliminate tobacco, and fall prevention. The secondary factor must be addressing
to know the drugs and the condition that can caused osteoporosis. The two principal
pharmacological type of osteoporosis are antiresorptive agent and anabolic agent.
Antiresorptive agents reduce the bone loss by prevent the action of osteoclast are
biphosphonate, estrogen, selective estrogen receptor modulators (SERMs), and
calcitonin. The anabolic agent that increase formation of the bone are synthetic
parathyroid hormones. If the osteoporotic fracture occur bracing and surgery is the
choice of management.
keywords : Osteoporosis, prevention and management

8
TUMOR MARKERS FOR SOLID CANCER:
“INAPPROPRIATE ORDERING, AND ABUSE”
Tjakra Wibawa Manuaba
Definition of tumor marker is traditionally referred to substances manly protein
(hormones, enzymes, cancer antigens, metabolites, normal protein, oncofetal antigens,
receptors, genetic changes or translocation), that Is produced by tumor cells, or by other
cells that is influenced by malignancy growth (Holdenrieder, et al., 2016; Wu, 2013).
Tumor markers can be associated to specific cancers such as: Prostatic cancer (PSA) or
for Differentiated Thyroid Cancer/ DTC such as thyroglobulin. There were tumor
makers that were not specific to only one type cancer, but they were positive to a couple
of cancers. For example CA19-9 was positive in pancreatic cancer, Hepato-biliair cancer
and gastric adenocarcinoma, or on contrary they would not always positive in certain
cancer such as AFP in HCC (hepatocellular cancer) or CEA in Colo-Rectal Cancer.
Looking at this lack of specificity, Oncologist should aware the present status and the
role of tumor markers in cancer management, to avoid under or over treatment of
cancer patients.
Majority of Surgeons and Surgical Oncologist order “tumor markers” for different
reasons and purposes. Unfortunately, many of the ordering of tumor markers was not
appropriate, or skewing from their purposes.
The ideal tumor markers, should have the capacity for:
- Cancer Screening
- Cancer Diagnosis
- Differential Diagnosis
- Prognosis
- Specific Treatment or directing specific treatment
- Recurrences after treatment
-
Majority tumor markers available, was not able to fulfill the above ideal criteria. Certain
tumor markers could be used for screening, while others were not.
9
For tumor marker to fulfill the criteria for screening, was usually lack of acceptable
sensitivity or specificity. PSA (Prostatic Specific Antigen) was probably the most
commonly used for screening of prostatic cancer. Panel of Tumor Markers, not only
useless for screening, but they also quite expensive.
The over use of tumor markers for diagnosis purposes, was actually abusing the standard
steps for solid cancer diagnosis. Although, tumor markers might help sharpening the
diagnosis and to overcome differential diagnosis by directing the most possible
diagnosis, for example for “unknown primary cancer (CUP)”, for example for
“metastatic of adenocarcinoma of unknown origin” on the neck/ supraclavicular, a
couple of tumor markers such as AFP, HCG (testicular cancer/ non-seminoma) , CA-
125 (ovarial cancer), PSA (prostat), CA19-9 (pancreatic or gastric cancer). The use of
tumor markers for CUP becoming less with the availability of CT, MRI and PET-Scan,
to find the primary location of the cancer.
Tumor markers were often used for advancing cancer/ stage, prognosis and relapsing
cancer were CA19-9, CA13-3, and PSA. Tumor marker was also used to monitoring
recurrences cancer after treatment finished such as PSA for pancreatic cancer, CA125
for ovarial cancer, and CEA for Colo-Rectal Cancer, thyroglobulin or ATA for well
differentiated thyroid cancer post total thyroidectomy.
Other molecular tumor markers could be used to direct to a specific treatment, such as
KRAS and BRAF for CRC; ER, PR, and HER2 for Breast Cancer (for hormonal therapy
and anti Her2 (Trastuzumab, Lapatinib, and Pertuzumab) , and the presence of EGFR
mutation in NSCLC. There was a specific tumor marker for GIST or EGIST, such as C-
Kit Protein/ CD 117 or PDGFR mutation, which can be used as specific and sensitive
marker to “imatinib or Sunitinib and recently Dasatinib”.
The future direction of tumor markers test can be very important especially the most
commonly used CA125, CEA, AFP, CA15-3, CA19-9 et cetera, but with the expanding
evidence based medicine, the education about the appropriate use for tumor markers
among health professional, and Cohort Prospective Trial or RCT should be started,
although, it is going to be very difficult to apply.

10
The availability of standard laboratory or reference lab., will be very important for
quality assurance and control for the tests themselves.
The expanding test as tumor markers is not only testing for protein in blood circulation
but also protein being expressed in the cancer cells, to understand the subtype, clinical
behavior, prognosis and what targeted drug can be used effectively.

11
THE ROLE OF MEASUREMENT OF CIRCULATING ANTI EBV AND EBV
DNA ON THE MANAGEMENT OF NASOPHARYNGEAL CARCINOMA
DL Tobing and NPC Multi Discipline Team
Dharmais Cancer Hospital
Nasopharyngeal carcinoma is cancer that occurs in the nasopharynx, which is
located behind the nose and above the back of the throat and is a tumor arising from the
epithelium of the nasopharynx
In the western world, the incidence rate is 1 patients / 100.000 population (Petgel et
al ,2005; Chan, 2002; Cho , 2007; Korcum , 2006). In the Southern China (Guangdong),
the incidence rate is 50 patients/100.000 population. In China and Taiwan , the case
reached 20% of all malignancy, In indonesia (Globocan 2012), the incidence rate of
male is 8 patients/ 100.000 population per year and of women is 3 patients/100.000
population per year. In Dharmais Cancer Hospital, the incidence rate in the year 2000 to
2005, there are 235 patients of NPC that consist of 169 males and 66 women.
The NPC risk can increase in line with age and it can be occur at any age, including
children. Based on the data in the United State shows that a half of NPC is at younger
age of 55 years
Nasopharyngeal carcinoma (NPC) Cancer is malignancy found in the nasopharynx
where cancer started from epithelial cells lining the regions the nasopharynx .
Epstein-Barr virus (EBV) is a double stranded DNA γ-herpesvirus with widespread
distribution in all human populations. EBV is associated with a variety of diseases
including infectious mononucleosis, hairy leukoplakia, inflammatory pseudotumors,
nasopharyngeal carcinoma (NPC), Burkitt's lymphoma, Hodgkin lymphoma, post-
transplants lymphoproliferative disorders, HIV-associated B-cell lymphomas, some T-
cell lymphomas particularly extranodal NK/T cell lymphomas of the nasal-type, and
recently a subset of gastric and breast carcinomas. Epstein Barr Virus (EBV)
preferentially infects B-lymphocytes through the binding of the major envelop
glycoprotein gp350 to the CD21 receptor on the surface of B-cells and through the

12
binding of a second glycoprotein, gp42, to human leukocyte antigen (HLA) class II
molecules as a co-receptor. EBV has the capacity to transform resting B-cells into
permanent latently infected lymphoblastoid cell lines.
EBV-transformed lymphoblastoid cell lines express a set of viral gene products
referred to as latent proteins which include six EBV nuclear antigens (EBNAs 1,2, 3A,
3B, 3C, -LP) and three latent membrane proteins (LMPs 1, 2A, and 2B). Transformed
lymphoblastoid cells also show abundant expression of small, non-polyadenylated, non-
coding RNAs (EBER1 and EBER2), which are expressed in all forms of latent EBV
infection. Transcripts from the BamHI-A viral genome known as BAR-transcripts are
also detected in lymphoblastoid cells. EBNA2, EBNA3C and LMP1 are key in the
transformation of EBV-infected cells. LMP1 is the main transforming protein of EBV
and functions as a classic oncogene in fibroblast transformation assay, LMP1 function as
an activated member of the tumor receptor (TNFR) superfamily, and activates several
signaling pathways.
Anti EBV (EA, VCA and EBNA) and expression EBV latent DNA (EBER 1 to 2;
EBNA1; BARTs and LMP 1-2 ) are markers currently used to support the diagnosis and
monitoring of NPC

13
HPV DNA TESTING IN CERVICAL CANCER : METHOD AND
INTERPRETATION
Sri Hartini
Clinical Pathology Department, Dharmais National Cancer Center, Jakarta , Indonesia
Human Papilloma Virus (HPV) is member of papovavirus family. All
papillomaviruses share a number of characteristics and contain double-stranded circular
DNA within an icosahedral capsid, it typically contains around 8000 bphas. Persisten
HR-HPV infection has been found to be associated with several human cancers such as
head & neck,skin, breast and cervic. Epidemiology studies show that the major type of
HR-HPV in Cervical malignancy are 16 and 18. On average, it takes 12–15 years before
a persistent HR-HPV infection may ultimately, via consecutive premalignant stages (ie
CIN lesions), lead to an overt cervical carcinoma. This argues that HPV-induced
cervical carcinogenesis is multi-step in nature. The Early-7 (E7) protein of HPV binds to
the underphosphorelated form of the tumor suppressor protein – pRb and displaces the
E2F transcription factor that is normally bound by pRb. Overexpression of E2F
transcription factor with upregulation of cell cycle genes resulting in DNA replication,
in the transition of the cell from the G1 to the S phase, and in increased cell proliferation
The Early-6 protein of HPV binds to and facilitates the degradation of the p53 gene
product. Therefore, inactivation of pRb and degradation of the p53 gene , both are tumor
suppressor genes, may dysregulate its functions resulting in increased cell proliferation,
in accumulation of damaged DNA, in growth of cells harbouring DNA errors, and in
prolonged cell survival.
Diagnosis of HPV infection can be established by detecting the presence of viral
nucleic acid in a patient sample or known as HPV DNA testing to determine whether
there is HR or HPV LR or HPV Genotyping examination for more detailed genotypes of
HPV. Laboratory methods for HPV DNA testing can be classified as PCR (Polymerase
Chain Reaction) method and non PCR method. The PCR method has several advantages
such as improving accuracy, reproducibility, requiring the same sample as the Liqiud
Pap test in small quantities so that it can be done simultaneously with Pap test
examination as well as having an internal Quality Control with β globin. According to
the experience of Dharmais Cancer Hospital, from 117 cervical swab and biopsy sample,

14
the result showed the main type of HPV were 16, 18, and 52 consecutively. Percentage
of HR-HPV+ increase in comformity with the increase of CIN (Cervical Intra
Neoplasia) stage.
Interpretation of HPV DNA testing not only knows the presence of infection but
rather the determination of the risk of getting cancer in persistent infections. Especially
in cervical cancer screening, Pap testing combined with HPV DNA examination in
women over the age of 30 can identify more high risk women than just by Pap test
examination In addition, HPV DNA testing can help clarify the results of Pap tests are
dubious, to monitor persistent HR-HPV infections as well as monitor the success of
treatment of pre-cancerous lesions
Given the relative risk of cervical cancer is determined by HPV type infection then
HPV DNA testing should be used on early routine tests, combine with Pap smear test or
as primary tool screening.
Key Word : HPV DNA testing, Cervical Cancer and PCR Method

15
METHODOLOGIES AND TECHNOLOGIES FOR THERAPEUTIC DRUG
MONITORING AND DRUGS OF ABUSE TESTING
Raja Elina Raja Aziddin, PhD
President, Malaysian Association of Clinical Biochemists
Immunoassay is the most common methodology used for therapeutic drug monitoring
and drugs of abuse testing. Although this technique has the advantage of simple
analytical procedures with minimum sample preparation, the present assays have limited
specificity. This has resulted in overestimates of the drug concentrations in clinical
samples especially in TDM of immunosuppresants and may also give a false positive
result for a drug test. The high sensitivity and selectivity of liquid chromatography with
MS detection (LC/MS/MS) has made it increasingly popular in the analysis of TDM
samples. It allows simultaneous measurement of several co-prescribed drugs with low
sample volume requirements thereby reducing cost and time of analysis.
Toxicology screening to detect drugs of abuse in various biological specimens may use
immunoassays or chromatography assays, the choice depending on the application of the
test method. The immunoassay screen is sufficiently sensitive to detect classes of drugs
or drug metabolites in symptomatic patients in the clinical setting. However in the
penalty setting, a positive immunoassay result needs to be confirmed by a different
analytical technique that has greater than or equal sensitivity to the immunoassay test.
Gas chromatography-mass spectrometry (GC/MS) has been the gold standard for
confirming initial immunoassay results. In recent years the LC/MS or LC/MS/MS has
increasingly become a more popular method for drugs of abuse testing, as it does not
require time-consuming derivatization or excessive sample clean-up necessary in
GC/MS analysis.
The various methods available, their application as well as factors affecting the
interpretation of the test result will be discussed.

16
LAPORAN HASIL PEMERIKSAAN VIRAL LOAD HUMAN
IMMUNODEFICIENCY VIRUS:
APAKAH DAPAT DIBANDINGKAN?
July Kumalawati
Departemen Patologi Klinik
Fakultas Kedokteran Universitas Indonesia
Rumah Sakit dr. Cipto Mangunkusumo
Jakarta
Viral load HIV dibutuhkan dalam penentuan awal dan pemantauan pengobatan anti-
retroviral. Saat ini terdapat beberapa reagen komersial yang tersedia untuk pemeriksaan
tersebut. Terdapat perbedaan dalam prinsip pemeriksaan, cara pelaporan atau konversi
hasil pemeriksaan, regio target yang mengalami amplifikasi, serta subtipe HIV yang
dapat dideteksi. Perbedaan tersebut dapat mempengaruhi keputusan klinisi dalam
penatalaksanaan pasien, terutama pemantauan respon pengobatan anti-retroviral, karena
arti hasil yang dilaporkan belum tentu sama bila menggunakan reagen berbeda.

17
PITFALLS IN SEROLOGIC TESTING
Jusak Nugraha
Dep. Patologi Klinik FK Unair / RSUD Dr. Soetomo
Surabaya
PENDAHULUAN
Metode pengukuran atas dasar ELISA dan uji serologis berlabel lain telah dipakai secara
luas untuk berbagai pengujian antibodi dan antigen. Ada banyak faktor yang dapat
mempengaruhi hasil pengujian serologi, dan semua tes serologi mempunyai
kemungkinan untuk memberikan hasil yang positif palsu maupun negatif palsu, dan
sebenarnya tidak mudah untuk membuat tes serologis yang benar2 handal dan
terpercaya, itu memiliki beberapa persyaratan teknis saat pelaksanaan. Dari berbagai
faktor yang dapat mempengaruhi hasil tersebut, faktor yang paling penting adalah
antibodi yang dipakai. Dasar dari reaksi antigen dan antibodi-lah yang merupakan topik
kajian yang terutama dipilih untuk dibahas lebih mendetail. Nanti akan dibahas tentang
dasar kimiawi reaksi berbasis antibodi, bagaimana memilih antibodi yang baik dan
bagaimana untuk mengurangi reaksi yang non-spesifik.
FAKTOR2 YANG BEPENGARUH
Interpretasi hasil uji serologis untuk mendeteksi penyakit infeksi dipengaruhi juga oleh
prevalensi penyakit di daerah tersebut. Kemungkinan bahwa sesorang menderita suatu
penyakit infeksi bila hasil tesnya positif , lebih besar sensitivitas dan spesifisitasnya bila
prevalensi penyakit tersebut tinggi atau endemis. Sebaliknya bila prevalensinya rendah
maka kemungkinan hasil tersebut false positif menjadi lebih besar.
Error pra-analitik dapat berasal dari hemolisis, komponen dari tabung vacutainer
(sumbat, pelumas, surfaktan dan gel pemisah) dapat melebur ke dalam spesimen atau
mengadsorbsi analit, aditif khusus juga dapat mempengaruhi stabilitas analit, aglutinasi
tak sempurna, keterlambatan pemrosesan dan penyimpanan yang salah.
Kesalahan analitik dapat disebabkan interferens yang analyte-dependent dan analyte-
independent. Termasuk yang analyte-dependent antara lain bahan serupa yang
memberikan reaksi silang, dan endogenous antibody seperti faktor rematoid, antibody
18
heterofil, antibodi anti-mouse, otoantibodi, dan adanya antibodi polispesifik dengan
affinitas rendah.
SIFAT DASAR ANTIBODI
Walaupun antigen merupakan makromolekul, tetapi epitope atau bagian yang berikatan
dengan antibodi terdiri hanya dari 12 - 30 asam amino saja dan dapat berupa epitope
linier seperti pada western blot atau epitope yang konformasional (3 dimensi).
Antibodi yang berasal dari germ-line pada suhu 37o C menunjukkan reaksi silang yang
tinggi tetapi pada suhu 4oC tetap spesifik; sebaliknya antibody yang berasal dari sel yang
mature tidak menunjukkan reaksi silang baik pada suhu 37oC maupun pada suhu 4oC.
Hal ini disebabkan antibodi germ-line masih menyesuaikan bentuk
MEMILIH ANTIBODI YANG BERKUALITAS
Antibodi yang berkualitas diproduksi oleh sel yang mature, strukturnya lebih rigid,
mempunyai afinitas yang tinggi, dan reaksi ikatannya menghasilkan energi
termodinamis (entrophy driven), serta sedikit reaksi silang.
MEMINIMALKAN REAKSI NON SPESIFIK
Reaktivitas antibodi yang non-spesifik dan tidak diinginkan dapat terjadinya karena
polispesifisitas / multispesifisitas atau reaksi silang. Pada multispesifisitas terjadi ikatan
yang tidak ada hubungannya dengan jenis antibodinya, ini disebabkan karena jenis
ikatan yang lain.
Reaksi silang (molecular mimicry) dapat terjadi karena struktur yang mirip misal strain
wild type yang memiliki residu utama yang hampir sama.
Solusi untuk mengatasi reaktivitas non spesifik yaitu dengan pemilihan antibodi yang
berkualitas, melakukan optimalisasi pengenceran antibody, memakai alat/system
deteksi sederhana namun sensitive dan melakukan opitimisasi buffer (konsentrasi ion /
blocking agent)
Terakhir yang penting yaitu harus selalu ada kontrol positif dan kontrol negatif untuk
semua imunoassai.

19
PENGARUH AGING TERHADAP PARAMETER LABORATORIUM
Suzanna Immanuel Departemen Patologi Klinik, Fakultas Kedokteran Universitas Indonesia, Jakarta
Penuaan adalah proses fisiologis yang akan dialami oleh seluruh makhluk hidup bila
berumur panjang, terjadinya berbeda dan kecepatan usia mulai proses juga berbeda.
Proses penuaan dikaitkan dengan faktor genetik, radikal bebas, pemendekan telomer,
reaksi Mailard, perubahan neuroendokrin dan perubahan lainnya. Penuaan ditandai
dengan banyak perubahan pada seluruh sistem tubuh, terutama pada sistem endokrin.
Pada usia lanjut terjadi perubahan kadar banyak hormon, diantaranya penurunan hormon
dehydroepiandrosterone (DHEA), melatonin, tiroksin (T4), triiodotironin (T3), growth
hormone (GH), testosteron, estrogen, kortisol, aldosteron. Peningkatan
antidiuretichormone (ADH), thyroid stimulating hormone (TSH), katekolamin
(epinefrin dan norepinefrin) dan follicle stimulating hormone (FSH) dan luteinizing
hormone (LH). Pada penuaan tidak terdapat perubahan yang berarti pada prolaktin dan
adrenocorticotrophic hormone (ACTH). Pemeriksaan laboratorium untuk pemantauan
antiaging saat ini umumnya berupa panel pemeriksaan hormonal. Pada pemeriksaan
hormon perlu diperhatikan tahap praanalitik yang dapat mempengaruhi hasil
pemeriksaan, adanya variasi diurnal, pada wanita adanya irama siklik (siklus haid).
Pemeriksaan hormon dapat menggunakan sampel saliva, darah dan urin. Faktor lain
yang harus dipertimbangkan dalam pemeriksaan hormon adalah dalam bentuk apa
hormon tersebut diukur, bisa dalam bentuk bebas atau terikat dengan protein.

20
LABORATORY DIAGNOSIS OF ALZHEIMER’S DISEASE
I NyomanWande
Clinical Pathology Department, School of Medicine
Udayana University/Sanglah Hospital
Alzheimer’s disease is 60 to 70% the most common cause of dementia in old age.
It is characterized by progressive and irreversible deterioration of cognitive abilities. The
disease generally starts with mild symptoms and ends with severe damage of the brain.
In the brain of a patient with Alzheimer’s disease, protein deposits form within and
outside the nerve cells, which lead to destruction of the nerve cells.
Suspected diagnosis of Alzhaimer’s disease primarily based on the identification
of clinical symptoms. Imaging technique and biomarkers analysis for to support the
diagnosis. Clinical symptoms of Alzheimer’s disease amongst other things memory loss
that disrupts daily life, problems understanding visual and spatial relationships, trouble
in finding words, withdrawal from social activities, changes in personality and up to
depression. Imaging techniques such as MRT or CT should be performed in order to
identify typical atrophy patterns and to exclude other causes for cognitive impairment.
PET imaging can help to detect and quantify amyloid deposits in the brain.
Laboratory examinations to the support diagnosis of Alzheimer’s disease amongst
other things, Beta-amyloid, Tau protein and APOE. Cerebrospinal fluid (CSF) of
patients who are developing Alzheimer’s diseases showed significantly decreased
concentrations of Beta-amylod (Aβ1-42 isoform) or decreased ratio of Aβ1-42 to Aβ1-40
even before the onset of cognitive changes. The concentrations of unphosphorylated
(total Tau) and phosphorylated Tau (P-tau) increase in CSF patients with progressing
neurodegeration and cognitive impairement. The gene codes for the lipoprotein ApoE,
which plays role in the breakdown of beta-amyloid.
Conclutions. Diagnosis of Alzheimer’s disease based on clinical sign, imaging
technique and biomarkers such as Beta-amyloid, Tau and APOE.
Keywords: Alzheimer’s disease, Beta-amyolid, Tau protein and APOE.

21
LABORATORY INVESTIGATION IN STROKE
dr. Yenny Surjawan, SpPK
Demographic transisition data indicates that the incidence of stroke will increase in
the future. Currently, the role of laboratories in stroke management Is to provide
testing to identify stroke's Risk factor,differentiate between stroke and stroke-mimics,
and monitor anticoagulant therapy. Despite many attempts to reduce stroke-related
morbidity and mortality, the incidence of stroke Had not decreased, and stroke is still
the leading cause of disability and mortality worldwide. Many studies aimed to
search for ideal biomarkers based on stroke pathophysiology, including The –omics
approach, but it is still very challenging and their clinical application need to be
validated.
Keywords: stroke, laboratory's role, stroke biomarker

22
UPDATE ON GLOMERULAR FILTRATION RATE MARKERS : CYSTATIN
C, CREATININ CLEARANCE AND eGFR
Dr.dr.Indranila KS. SpPK(K)
Department of Clinical Pathology, Medical Faculty of Diponegoro University
Glomerular filtration rate (GFR) is a measure of the function of the kidneys. This
measures the level of creatinine in the blood and uses the result in a formula to calculate
a number that reflects how well the kidneys are functioning, called the estimated GFR or
e GFR. Estimated Glomerular Filtration Rate (e GFR): is a number based on blood
test for creatinine, a waste product in your blood. It tells how well your kidneys are
working. Now GFR is commonly reported by clinical laboratories. Creatinine and
Cystatin C performance based on equation estimation are also used as their guidance in
clinical practice and public health. Low of GFR level are associated with some poor
outcome, including acute renal failure .Equation CKD-EPI improves its performance
and predicts risk compared to the equation of MDRD study and Cockcroft-Gault.
Estimation GFR reporting has been used more as a reference by the nephrologist, using
MDRD Study or Cockcroft – Gault. Urea and creatinine biomarkers each have their
limitations and strengths for the diagnosis of chronic renal failure. A creatinine
clearance test can be performed endogenous substances to measure GFR (mGFR) and
“estimated” equation GFR (eGFR).Understand each has its own advantages and
limitations, it is necessary to look for such more sensitive and more specific biomarkers.
More sensitive and specific biomarkers for renal functional biomarkers are Cystatin C.
Currently based on inaccurate equation in all populations, even with reduced muscle
mass or in chronic disease, Cystatin C is expected to replace creatinine. The exogenous
and endogenous filtration markers, alone or in combination can be a determinant of
screening markers and are required to predict for a more accurate estimates of GFR.
Key words :Glomerular filtration rate (GFR), estimate GFR (e GFR) , creatinine,
clearance creatinine and Cystatin-C

23
NOVEL BIOMARKER FOR KIDNEY DISEASES:
Liver- Fatty Acid Binding Protein (L-FABP)
Marzuki Suryaatmadja
HKKI, Mayapada Hospital Jakarta Selatan
Two kinds of Kidney diseases with high morbidity and mortality are Acute Kidney
Injury (AKI) and Chronic Kidney Disease (CKD). AKI is the condition marked by
abrupt (within hours) of kidney function, which encompasses injury (structural damage)
and impairment (loss of function). This term has recently replaced the old term Acute
Renal failure. Based on the etiologies AKI can be differentiated as pre renal, renal and
post renal. CKD is condition with gradual loss of renal function over the courses of
months or years or decades. There is strong interrelationship between AKI and CKD;
CKD can develop from AKI and CKD can also cause AKI.
AKI should be well managed fast to gain best outcome, therefore demand for the
presence of parameter with high sensitivity for early detection. The available parameters
e.g. creatinine, cystatin-C and even albumin excretion are considered too late. One
novel biomarker is L-FABP, a 14 kDa protein, found in the proximal tubules of kidney.
Analysis of L-FABP by latex turbidimetric immunoassay (LTIA) method can give
results within relatively short time. The reference interval of urinary L-FABP is ≤8.4
ug/gCr. Urinary L-FABP increases before the albumin excretion in cases of AKI, CKD,
and diabetic nephropathy.
In conclusion, the L-FABP biomarker is promising as diagnostic for several kidney
diseases.
Key words: acute kidney injury, chronic kidney disease, biomarker, liver type fatty acid
binding protein.

24
THERAPEUTIC DRUG MONITORING IN RENAL TRANSPLANT PATIENTS
Raja Elina Raja Aziddin, PhD
President, Malaysian Association of Clinical Biochemists
Kidney transplant is an established treatment for many end-stage renal failure patients
and is the only alternative to dialysis. Patients who undergo renal transplant are required
to receive treatment with immunosuppressive drugs. Survival of renal organ transplant
has improved with the introduction of drugs such as cyclosporine, tacrolimus, sirolimus,
everolimus and other drugs. However these drugs have a narrow therapeutic window.
Over dosing will increase the toxicity risk and under dosing may result in organ
rejection. The target therapeutic level depends on the time after transplantation and the
co-medication.
The variable pharmacokinetics of immunosuprressants within and between patients as a
result of variations in absorption, distribution and or elimination makes it impossible to
reliably predict the best dose for each patient. Therapeutic drug monitoring (TDM)
therefore plays an important role in the optimal use of immunosuppressants in transplant
patients.The aim is to achieve therapeutic efficacy and to minimize the occurrence of
adverse effects.However assay sensitivity, specificity and linearity may pose a challenge
in meeting the needs of an effective TDM.
An efficient and effective TDM service therefore requires the understanding of the renal
transplant patient management, pharmacokinetic and pharmacodynamic of each
immunosuppressive drug and the analytical methods.
25
ABSTRAK PRESENTASI POSTER

26
PROFILE AND COMPARISON OF ERITROSIT INDEX ON
NORMAL LABOR AND SECTIO CAESAREA
Ellis Susanti¹, Fuja Fathonah¹, Siti Jumhati¹
¹University of MH Thamrin
According to the World Health Organization (WHO) the prevalence of anemia in
pregnant women worldwide is 41.8% and 48.2% in Asia. Based on the results of
Research Basic Health in 2013, the prevalence of anemia in pregnant women in
Indonesia is at 37.1%, for women who undergone caesarean surgery, the number is at
9.8% of a total of 49,603 births, the highest proportion in DKI Jakarta (19.9%). Anemia
in pregnant women may lead to harmful impacts on pregnancy, childbirth and the fetus
itself. The index values of erythrocytes categories anemia morphologically, so it is
hoped to assist in the management of anemia. The purpose of this research is to identify
the profile and comparison of the Erythrocyte Index in normal delivery and caesarean
section surgery as well as classifying anemia morphologically to categories different
types of anemia in order to improve the management of anemia. The design of this study
is a cross sectional observation of 60 respondents, . The results of the study on normal
delivery obtained the MCV values of 86,36 (73-97)fl, 3,33% (microcytic), 96,66%
(normocytic); MCH 27,86 (23-33)pg, 13,33% (hypochromic), 83,33% (normochromic),
3.33% (hyperchrom); MCHC 32,23 (30-34)%, 23,33% (microcytic), 76.66%
(normocytic). In caesarean delivery the study found MCV values of 86.08 (74-99)fl,
20% (microcytic), 76.66% (normocytic), 3.33% (macrocytic); MCH 27,74 (23-33)pg,
26,66% (hypochromic), 70% (normochromic), 3,33% (hyperchrom); MCHC 32.2 (30-
34)%, 23.33% (microcytic), 76.66% (normochromic). The significance value of normal
labor and caesarean delivery did not substantially differ (p value MCV = 0.624, MCH =
0.573 and MCHC = 0.385). Summary is most of the abnormalities identified are
normocytic anemia caused by acute blood loss, especially in caesarean delivery.
Suggestions for more research are proposed by adding the Ferritin test and the
Erythrocyte imaging.
Keywords: Erythrocyte index, anemia, normal delivery, sectio caesarea

27
COMPARING THE EFFECTIVENESS OF EXAMINATIONS OF NON-HDL
CHOLESTEROL AND SMALL DENSE LDL CHOLESTEROL TO
ESTABLISHING THE DIAGNOSIS OF CARDIOVASCULAR DISEASE
Gilang Nugraha, S.Si., M.Si.1, Prof. Subagijo Poegoeh Edijanto, dr., Sp. PK (K)2
1Study Program of Medical Laboratory Technology, faculty of health University of
Nahdlatul Ulama Surabaya 2Study Program of Medicine, Faculty of Medicine, University of Nahdlatul Ulama
Surabaya
Kolesterol non-HDL dan estimasi kolesterol sdLDL formula Srisawasdi menjadi
predikator yang baik untuk menegakan diagnosis penyakit Kardiovaskular dengan
menggunakan hasil pemeriksaan profil lipid sehingga tidak memerlukan biaya
tambahan. Akan tetapi predikator yang unggul dalam menegakan diagnosis penyakit
kardiovaskular belum pernah dilaporkan pada sampel orang Indonesia. Tujuan penelitian
ini adalah menentukan validitas diagnostik non-HDL-C dan sdLDL-C formula
Srisawasdi pada trigliserida kurang dari 400 mg/dL. Sebanyak 88 sampel dilakukan
pemeriksaan profil lipid dan perhitungan non-HDL-C serta sdLDL-C formula
Srisawasdi. Pemeriksaan direk sdLDL-C digunakan sebagai metode referen. Hasil uji
regresi linier dan ROC terhadap direk sdLDL-C didapat non-HDL-C R2 : 64,86% dan
AUC : 93% sedangkan sdLDL-C Srisawasdi R2 : 65,41% dan AUC : 91%. Nilai
Diagnostik non-HDL-C dan sdLDL-C Srisawasdi berturut-turut meiliki nilai sensitivitas
8,3% dan 43,8%; spesifisitas 100% dan 95,8%; Akurasi 37,5% dan 86,2%; Tingkat
positif palsu 0% dan 4,2%; Nilai ramal positif 100% dan 70,0%; Nilai ramal negatif
33,7% dan 88,3%. Dapat disimpulkan bahwa pemeriksaan sdLDL-C Srisawasdi lebih
menjanjikan dalam menegakan diagnosis penyakit kardiovaskular dibandingkan non-
HDL-C.
Kata kunci : sdLDL-C, non-HDL-C dan Penyakit Kardiovaskular

28
CORRELATION OF WAIST CIRCUMFERENCE WITH FRAMINGHAM RISK
SCORE IN RURAL ADULTS IN BONJOROYO VILLAGE, KULONPROGO,
YOGYAKARTA
Fenty 1,2 Yunita Linawati1, Aris Widayati1
Fakultas Farmasi Universitas Sanata Dharma Yogyakarta1
RS. BETHESDA YOGYAKARTA2
Email korespondensi : [email protected]
Introduction : Cardiovascular disease (CVD) is the leading cause of death in most
countries worldwide. The prevalence of overweight and obesity continued to increase in
developing countries. Central obesity prevalence tends to increase in rural areas in
Indonesia. It increased correlates with increased cardiovascular risk. Framingham Risk
Score FRS) is a used to estimate the 10-year cardiovascular risk of an individual.
Method :This is an analytic observational study with cross-sectional design. Research
subjects were rural community in Bonjoroyo village, Kulonprogo Regency, DIY which
fulfilled inclusion criteria. The data obtained are obesity index data (Body Mass Index /
BMI, Waist Circumference (WC) and fasting blood glucose levels, and FRS –BMI
based, which are then analized statistically with normality test and continued with
correlation test Spearman with 95% confidence level.
Results & Discussion : There were 122 subjects (42 men and 80 women), ages 30-75
years old. This study showed 56% low risk, 26% medium risk and 18% high risk in
10-year CVD event prediction in rural adults. The results showed that WC
measurements were positive correlated with FRS (r: 0,166, p: 0.294) in men and (r:
0,21 p: 0.62) in women, but were not statistically significant.
Conclusion :Although weak and no statistically significant, this study adds evidence
that there is a correlation between WC (as central obesity) and 10-year CVD event
prediction by FRS.
Keywords: Waist Circumference, Framingham Risk Score, rural

29
A VERY HIGH LEVEL OF CREATININE KINASE IN EXERCISE-INDUCED
RHADBOMYOLYSIS
Martha Riestiana, Tandry Meriyanti
Laboratorium Department of Siloam Hospitals Lippo Village
Introduction
Rhabdomyolysis is defined as medical condition, exhibited by a triad symtoms: muscle
weekness, myalgia, and elevation in serum CK. Missing diagnosis can cause life-
threatening condition and complication. We report the case of a 21 year-old-woman who
has a very high level of CK.
Case
21 year-old woman came to orthopedic clinic, with complain weakness affecting lower
body since a week ago after completing highly intense training. She denied use of
streroids, statins, and other supplements. There was no specific abnormalities on
physical examination.
Laboratory findings were very high level of CK(>215262 U/L), normal level of ureum
and creatinine. There was occult blood+3 and erytrocyte only 2 cells/uL on urinalysis
test and positive myoglobinuria. There was increasing ALT(1996 U/L) and
AST(546U/L), LDH(7170 U/L). The patient did not developed any significant
electrolyte and bilirubin abnormalities.
Discussion
The diagnosis of exercise-induce rhabdomyolysis is based on muscle pain responses,
and laboratory test high level of CK and LDH, and myoglobinuria. Increased CK and
LDH are associated with muscle damage. A very high CK level(> 5000 IU/L) is
associated with kidney failure, but at present it still shows normal function.
IncreasedALT/ASTis closely related to the enzyme release from muscle, not related to
liver disease.
Conclusion
Based on clinical picture, physical examination, and laboratory test, the patient was
diagnosed as exercise-induced rhabdomyolisis.
Keyword: CK, Rhabdomyolysis, LDH

UCAPAN TERIMA KASIH
PT PRIMACO