Embed Size (px)
Citation preview

renovascular hypertension have been published and include thefollowing:
. Abruptor severehypertension.
. Hypertensionresistantto medicaltherapy.
. Abdominalor flankbruits.
. Unexplainedazotemia.
. Worseningrenalfunctionduringtherapywith ACEIs.
. Grade3 or 4 hypertensiveretinopathy.
. Occlusivediseasein othervascularbeds.
. Onsetof hypertensionbeforeage30or afterage55.
PARTIV:PROCEDUREA. Patient Preparation
The patient should be well hydrated before testing. Ifan oral ACEI is used, the patient should drink onlywater and should not eat a solid meal within 4 hr of thestudy. One suggested protocol is 7 ml water/kg bodyweight 30—60mm before the study. Hydration shouldcontinue between studies if two studies are performedon the same day. An intravenous line should be placedfor normal saline infusion in high-risk patients and forthose receiving intravenous enalaprilat (see SectionIV.C, Precautions, below). Ideally, ACEIs should bewithheld for 2—5days (depending on half-life) beforethe study. Captopril and enalapril/lisinopril probablyshould be withheld for 48 hr and 96 hr, respectively.Some patients will present for the test on a therapeuticACEI. In such a patient, it is reasonable to give theACEI and perform captopril or enalaprilat renography,although the referring physician should understand thatthere may be a slight loss of sensitivity.
Chronic administration of diuretics may also decrease the sensitivity of the procedure, and chronicdiuretic administration should be stopped several daysbefore the study, ifpossible. In a well-hydrated patient,however, chronic diuretic administration probably willnot affect test results. The effect of other hypertensivemedications on ACEI renography is not completelyunderstood, but it appears small. If hypertension issevere, it is not necessary to discontinue all antihypertensive medications before the procedure.
B. Information Pertinent to Performing the ProcedureRelevant history, physical findings, patient medica
Key Words: renovascular hypertension, procedure guideline
J Nuci Med 1998;39'.1297-1302
PARTI: PURPOSEThe purpose of this guideline is to assist nuclear medicine
practitioners in recommending, performing, interpreting andreporting the results of renal procedures for diagnosis ofrenovascular hypertension.
PART II:BACKGROUND INFORMATION ANDDEFINITIONS
Renovascular hypertension is estimated to affect PVo—3%ofthe unselected hypertension population and up to lS%—3O%ofpatients referred to a subspecialty center because of refractoryhypertension. Clinical features should indicate which patientshave moderate or high risk of renovascular hypertension. Cluesinclude abrupt or severe hypertension, hypertension resistant tomedical therapy, bruits in the abdomen or flank, unexplainedazotemia or worsening renal function during therapy withangiotensin-converting enzyme inhibitors (ACEIs). It is important to distinguish between renovascular hypertension andstenosis of the renal artery. Stenosis of the renal artery iscommon in nonhypertensive elderly persons and is an associated but nonetiologic finding in a number of hypertensivepatients. Renovascular hypertension is defined as an elevatedblood pressure caused by renal hypoperfusion, usually due toanatomic stenosis of the renal artery and activation of therenin-angiotensin system. The goals of a screening test are todetect those patients who have renal artery stenosis as the causeof hypertension and, to predict curability of hypertensionfollowing intervention.
PART III: COMMON INDICATiONSThe test is most cost-effective if used primarily in patients
who have moderate to high risk of renovascular hypertension.Clinical features associated with moderate to high risk of
For correspondence or reprints contact: Wendy J.M. Smith, Director of Health CarePolk@y,Society of Nuclear Med,cine, 1850 Samuel Morse Dr., Reston, ‘/A20190-5316,[email protected].
Note: 1@JI26SNM-approved procedureguidelines are available on the Society's homepage. We encourage you to downloadthese documents via the Internetat www.snm.org. If you would like information on the development of this guideline@ to ordera compendium of all 26 procedure guidelines for $20.00, contact Marie Davis, Societyof NuclearMedicine,at (703)708-9000,ext 250,orbye-mailat [email protected].
PROCEDURE GUIDELINE FOR DIAGNOSIS OF RENOVASCULAR HYPERTENSION •Taylor et al. 1297
Procedure Guideline for Diagnosis of RenovascularHypertensionAndrew T. Taylor, Jr., James W. Fletcher, Joseph V. Nally, Jr., M. Donald Blaufox, Eva V. Dubovsky, Eugene J. Fine,Daniel Kahn, Kathryn A. Morton, Charles D. Russell, George N. Sfakianakis, Mattias Aurell, Maurizio Dondi, Enza Fommei,Gijsbert Geyskes, Goran Granerus and Hong-Yoe OeiEmory University School ofMedicine, Atlanta, Georgia; St. Louis University School ofMedicine, St. Louis, Missouri;Cleveland Clinic, Cleveland, Ohio; Albert Einstein College ofMedicine and Montefiore Medical Center, Bronx, New York;University ofAlabama Hospital, Birmingham, Alabama; Jacobi Medical Center, Bronx, New York; Veterans AdministrationMedical Center, University oflowa College ofMedicine, Iowa City, Iowa; Veterans Administration Medical Center, Portland,Oregon; University ofMiami School ofMedicine, Miami, Florida; Department ofNephrology, Shalgrenska Hospital,Goteborg, Sweden; Servizio de Medicina Nucleare, Ospedale per gli Inftrmi, Faenza, Italy; Institute of Clinical Physiology,University ofPisa, Pisa, Italy; Hospital New Nickerie, Suriname; Department of Clinical Physiology, University Hospital,Linkoping, Sweden; and Department ofNuclear Medicine, University Hospital D@/kzigt, Rotterdam, The Netherlands
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from

Organrece@ngAdministeredactMty the largest radiationdoses Effectivedose@MBq
mGymSvRadiopharrnaceutical(mQ) (rad)(rem)@Tc@DWAt
37-370 0.0650.0063Bladderwail(1—10)
(024)(0.023)@Tc@MAG3*37—370 0.110.0073Bladderwall(1—10)
(0.41)(0.027)*per
MBq(permCi).tICAP53,page188.*ICRP,62, page17.tions,
when ACEIs were stopped, patient's serum cre- raphy should be done on the first day. If the ACEIatinine and patient's resting blood pressure while sitting renogram is normal, the chance that the patienthasand
standing. . renovascular hypertension is low, and there is no needtoC.Precautions have the patient return on the second day for abaselineACEIs
can cause significant hypotension. Therefore, study. When the study result is abnormal, specificitycanbloodpressure and pulse should be monitored and be improved by obtaining a baselinestudy.recorded
before administration and at least every 10—15 When the i-day protocol is performed,baselinemmthereafter. An intravenous line should be estab- renography should be performed first with only 37 MBq
lished in high-risk patients (e.g., history of carotid (1 mCi) of 9@Tc-DTPA or @Tc-MAG3.The admindisease, stroke, transient ischemic attack, angina and istered activity for the ACE! renogram should be200—recent
myocardial infarction) and in patients who re- 400 MBq (5—10mCi) to overwhelm any counts fromtheceiveintravenous enalaprilat. A patient should not be baselinestudy.sent
home unless his or her standing blood pressure is at Instrumentation, Positioning and Timing ofImages:least70% of baseline and he or she is asymptomatic The study should be acquired with the gammacamerawhenstanding. facing the lower back of the supine patient. A large
D. Radiopharmaceuticals (See Tables 1 and 2.) field-of-view camera is preferred so that the heart,The optimal radiopharmaceutical remains to be de- kidneys and bladder can all be included in the field of
termined. However, @Tc-mercaptoacetylthglycine view. If only two organs can be imaged, the kidney and(MAG3) and 99mTcdiethylenethaminepen@cetic acid bladder should be visualized. For @Tcagents and(DTPA) are most commonly used. Radioiodinated hip- 123-orthoiodohippurate (OIH), a low-energy or highpuran has also been used. Technetium-99m-MAG3 is resolution, all-purpose collimator should be used. Mapreferred over 9@Tc-DTPA in patients with elevated trix resolution is preferably 128 X 128, although 64Xcreatinine
because of its higher extraction. 64 is acceptable. When a dynamic flow study is obE. Image Acquisition tamed, the time per frame should be 1—3sec for thefirstStudy
Protocol: Both I-day and 2-day protocols are 60 sec and 10—30sec per frame for the remainder oftheacceptable.If there is a relatively low likelihood of study. The total acquisition time should be 20—30mm.renovascular
disease, the 2-day protocol is preferred Patients should void before beginning the study, andaoverthe 1-day protocol. The i-day protocol requires postvoid image isrecommended.that
the patient remain in the department for a longer F.Interventionstime,but the entire study is completed in I day. Although captopril has been most widely used, cap
When the 2-day protocol is performed, ACE! renog- topril and enalaprilat are both acceptable forACE!TABLE
2RadiationDoelmetry for Children w@i Notmal Renal Function*(5.y@J)Organ
recalvingAdministeredactMty the largest radiation @j@t Effective@j@tMBq/kg
mGymSvAadiopharmaceutical(mCi/kg) (red)(rem)@Tc-DTPA
3.7 0.0860.012Bladderwall(0.1)
(0.32)(0.044)@‘Tc-MAG33.7 0.180.015Bladderwall(0.1)
(0.67)(0.055)Treves
ST, Pediatric Nuclear Medicine, 2nd ad., New Yoric Springer-Verlag;1995.tperMBq (permCi).
TABLE IRadiatiOn Dosimetry for Adults with Normal Renal Function
1298 THEJOURNALOFNUCLEARMEDICINE•Vol. 39 •No. 7 . July 1998
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from

renography. The recommended dose of captopril is25—50mg by mouth. Crushing the tablets and dissolvingthem in 150—250 ml water may enhance absorption.Unless the patient has delayed gastric emptying or poorabsorption from the gastrointestinal tract, 25 mg issufficient. Patients should not eat a solid meal within4 hr of the study, as food in the gastrointestinal tractdecreases captopril absorption. Radiopharmaceutical administration should be delayed for at least 60 mm aftercaptopril administration, as peak blood levels occurapproximately 60 mm after oral ingestion. Enalaprilat(Vasotec) can also be used, with 40 ug/kg administeredintravenously over 3—5mm. A total dose of 2.5 mgshould not be exceeded. Because the radiopharmaceutical can be given I 5 mm after enalaprilat administration,procedure time is shorter and potential problems withgastrointestinal tract absorption are also avoided. It isrecommended that the radiopharmaceutical not be administered until at least 15 mm after intravenous enalaprilat administration.
Option: Administration of furosemide with captopril orenalaprilat is not considered to be an essential componentofACEI renography. Since furosemide is a loop diuretic, itcan wash the radiopharmaceutical out of the calyces andpelvis and improve evaluation of cortical retention oftubular agents MAG3 and OIH. It also can cause volumedepletion and increase the risk of hypotension.
G. ProcessingBackground subtraction is recommended using a
ring, elliptical or perirenal region of interest (ROl). Therenal uptake of MAG3 and OIH should be measured ineach kidney in the 1—2-or 1—2.5-mm interval afterinjection of the radiopharmaceutical. After 2.5 mm aportion of these tracers may have already left the renalROI, thus leading to incorrect estimates of relativefunction. The relative renal uptake of DTPA should bemeasured from 2—3mm postinjection. Renogram curvesshould be generated from ROIs that are selectivelyassigned to the renal cortices or the whole kidney.Exclusion of the pelvis and calyces is important if thereis retention of activity in these structures. The time tomaximum activity (Tmax) should be determined. A 20mm/peak mm (20 mm/maximum) activity ratio shouldbe calculated for MAG3 and OIH. Measurement ofrenal parenchymal transit time is recommended using aparenchymal ROI if the software algorithm is available.
H. Interpretation/ReportingThe most specific diagnostic criterion for renovascu
lar hypertension is an ACEI-induced change in therenogram. Overall, ACE! renography has a sensitivityand specificity of about 90% for diagnosis of renalartery stenosis. Most importantly, ACEI-induced renographic findings ofrenovascular hypertension indicate ahigh probability that blood pressure will be reducedafter intervention.
The post-test probability for disease cannot be determined solely based on the test results. The test resultsmust be combined with the pretest probability. In thediscussion of probability that follows, a pretest probability of lO%—30%is assumed for high-risk patients inwhom ACEI renography should be performed. Whenthis test is performed in lower-risk patients, the post-testprobability will be lesser than the numbers cited below.Test results should be interpreted as consistent withhigh, low or intermediate probability of disease.
Low Probability: Normal findings on ACE! renography indicate a low probability (<10%) for renovascularhypertension. Abnormal baseline findings that improveafter ACE inhibition also indicate low probability forrenovascular hypertension.
Intermediate Probability: Patients with intermediateprobability of disease have abnormal baseline findingsbut the renogram is unchanged after ACE inhibition.This group includes some azotemic patients and hypertensive patients who have a small, poorly functioningkidney. The sensitivity of abnormal baseline findingsthat are unchanged after ACE inhibition is quite high(>90%), but the specificity is poor, probably in therange of 50%—75%.
High Probability: The probability is considered high(>90%) when marked change of the renogram curveoccurs after ACE inhibition compared to baseline findings. For DTPA, this change can be quantitated bymeasuring the change in relative function or absoluteindividual kidney function. For tubular agents, the changecan be best quantitated by a change in the 20 mm/peakcount ratio or a prolongation of the Tmax. In subjectswith normal renal function and in the absence of pelvicor caliceal retention, a normal 20 mm/peak ratio forOIH or MAG3 is <0.3. A 0.15 change (i.e., 0.3—0.45)after ACE inhibition usually is considered to be significant. A 0. 1—0.15 change is considered to be borderline.
General Interpretive Criteria:
. A normal ACE! renogram indicates a low probability (< 10%) of renovascular hypertension.
. Criteria associated with renovascular hypertension include worsening of the renogram curve,reduction in relative uptake, prolongation of therenal and parenchymal transit time, increase inthe 20 mm/peak ratio and prolongation of the
Tmax@. A small,poorlyfunctioningkidney(<30% up
take with a Tmax 2 mm) that shows no changeafter ACE! renography and bilateral symmetrical change (cortical retention with tubular agentsand decrease of DTPA uptake) are indicative ofintermediate probability for renovascular hypertension.
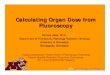
Spec@flc Interpretive Criteria for MAG3 and OIH:Unilateral parenchymal retention after ACE! administration is the most important criterion for MAG3 andOIH and represents high probability (>90%) forrenovascular hypertension. This can be measured bya change in the 20 mm/peak ratio of 0. 15 or greater,a significantly prolonged transit time or a change inthe renogram grade (Fig. 1). It also can be detected asa delay in the excretion of the tracer into the renalpelvis >2 mm after ACEI administration or anincrease in the Tmax of at least 2 mm or 40%. Achange in relative uptake of MAG3 or 0tH >10%after ACE! administration is uncommon, but it represents a high probability for renovascular hypertension when present.
Spec@fIcInterpretive Criteriafor DTPA: Reductionin relative uptake greater than 10% after ACE!administration indicates high probability for renovascular hypertension; S%—9%indicates intermediateresponse. High probability is also associated with a
PROCEDURE GUIDELINE FOR DIAGNoSIs OF RENOVASCULAR HYPERTENSION •Taylor et al. 1299
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from

B. The following sources of error should be discussed: (1)retained activity within the collecting system and (2)RO! selection, hepatic uptake of MAG3. The locationof the right kidney background RO! may significantlyaffect the calculated relative uptake in patients withseverely impaired renal function.
C. The reference test or “goldstandard―in future studiesshould be the outcome, the response to successfulrevascularization, not angiographic evidence of renalartery stenosis. Future studies also need to clearlydefine patient subgroups and the results of ACE!administration in these subgroups, (e.g., azotemic versus nonazotemic patients; results in patients takingdiuretics, beta-blockers and ACEIs versus patients nottaking these medications; and results in patients withnormal baseline studies versus results in patients withabnormal baseline studies). The utility of 1—3-secdynamic images in detection of renovascular hypertension is uncertain. Further information is needed correlating bilateral symmetrical changes in the renogramcurve with angiography and with results of revascularization. Additional studies are needed in patients withsolitary kidneys or renal transplants. Additional dataare needed regarding the effect of chronic drug administration (diuretics, beta-blockers, ACEIs) on test sensitivity and specificity; regarding the utility of ACE!renography in assessing functional significance of stenosis of the least-affected kidney in patients withbilateral renal artery stenosis; on the effects of saltloading and the state of hydration; and on bettercharacterization of the baseline abnormality in patientsin whom the abnormal baseline does not change afterACEI administration.
PART VII: CONCISE BIBLIOGRAPHY
1. Black HR, Bourgoignie JJ, Pickering T, et al. Report of theworking party group for patient selection and preparation.Am J Hypertens 1991;4:7455—7465.
2. Black HR. Captopril renal scintigraphy—a way to distinguish functional from anatomic renal artery stenosis [Editorial; Comment]. J Nuci Med 1992;33:2045—2046.
3. Blaufox MD, Dubovsky EV, Hilson AJ, et al. Report of theworking party group on determining the radionuclide ofchoice. Am J Hypertens 1991;4:7475—7485.
4. Blaufox MD. Captopril renography: considerations in theselection of radiopharmaceuticals, provocative agents, andhypertensive subjects. Am J Hypertens 1991;4:6755—6775.
5. Clorius JH, Hupp T, Schmidlin P, et al. The diagnosis ofrenovascular hypertension: the role of captopril renal scmtigraphy and related issues [Letter; Comment]. Eur J NuclMed 1994;21:264—267.
6. Derkx FH, van den Meiracker AH, Jaarsveld BC, et al.Captopril in the diagnostic work-up ofhypertensive patientswith suspected renal artery stenosis. Net/i J Med 1993;43:S12—S19.
7. Dey HM, Hoffer PB, Lerner E, et al. Quantitative analysisof the technetium-99m-DTPA captopril renogram: contribution ofwashout parameters to the diagnosis ofrenal arterystenosis.JNucl Med l993;34:1416—1419.
8. Dondi M. Captopril renal scintigraphy with 9@Tc-mercap
Time(minutes)
FIGURE 1. Patterns of renographic curves from normal to blood background-typecurve.0 = normal;1 = minorabnormalities,but withT@ >5mmand (forOIHand MAG3)20 mirt/maxratio >0.3; 2 = marked delayedexcretion rate with preserved washout phase; 3 = delayed excretionrate@Añthoutwashout phase (accumulation curve); 4 = renal failure pattern w@imeasurable kidney uptake; 5 = renal failurepattern without measurablekidney uptake (blood background-type curve).
10% decrease in calculated glomerular filtration rateof the ipsilateral kidney after ACE! administration.Marked unilateral parenchymal retention after ACE!administration compared to baseline study also represents high probability for renovascular hypertension.
I. Quality ControlGamma camera and image displays as described in the
Society of Nuclear Medicine Procedure Guideline forGeneral Imaging. Images should be reviewed in adynamic format to evaluate for presence of patientmotion.
J. Sources of ErrorExisting clinical and renographic results must be
interpreted with some caution because the protocols arecomplex and the diagnostic criteria are not well standardized.
PART V: DISCLAIMERThe Society of Nuclear Medicine has written and approved
guidelines to promote the cost-effective use of high-qualitynuclear medicine procedures. These generic recommendationscannot be applied to all patients in all practice settings. Theguidelines should not be deemed inclusive of all proper procedures or exclusive of other procedures reasonably directed toobtaining the same results. The spectrum of patients seen in aspecialized practice setting may be quite different than thespectrum ofpatients seen in a more general practice setting. Theappropriateness of a procedure will depend in part on theprevalence of disease in the patient population. In addition, theresources available to care for patients may vary greatly fromone medical facility to another. For these reasons, guidelinescannot be rigidly applied.
Advances in medicine occur at a rapid rate. The date of aguideline should always be considered in determining itscurrent applicability.
PART VI: ISSUES REQUIRING FURThERCLARIFiCATiON
A. It would be useful to know how high a patient's serumcreatinine can be without significantly compromisingtest accuracy.
1300 THEJoui@i. OFNUCLEARMEDICINE•Vol. 39 •No. 7 . July 1998
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from

toacetyltriglycine (99mTc@MAG3)for detecting renal arterystenosis. Am J Hypertens 1991;4:7375—7405.
9. Dondi M, Fanti 5, Fabritiis AD, et al. Prognostic value ofcaptopril renal scintigraphy in renovascular hypertension[see comments]. J Nucl Med l992;33:2040—2044.
10. Dondi M, Fanti 5, Monetti N. Captopril renal scintigraphy:a viewpoint.J NuclBiolMed l993;37:259—263.
11. Dubovsky EV, Russell CD. Diagnosis of renovascularhypertension after renal transplantation. Am J Hypertens1991;4:7245—7305.
12. Erley CM, Duda SH, Wakat JP, et al. Noninvasive procedures for diagnosis of renovascular hypertension in renaltransplant recipients—a prospective analysis. Transplantation 1992;54:863—867.
13. Fanti 5, Dondi M, Barozzi L, et al. Detection of renal arterystenosis by means of captopril renal scintigraphy in patientswith multiple renal arteries. Clin Nucl Med 1992; 17:849—852.
14. Fine EJ. Captopril scintirenography: a protocol to assessefficacy and methodology. A collaborative study. ContribNephrol l990;79:2l1—218.
15. Fine EJ, Blaufox MD. The Einstein/Cornell collaborativeprotocol to assess efficacy and methodology in captoprilscintirenography: early results in patients with essentialhypertension. Report of the Einstein/Cornell CollaborativeHypertension Group [published erratum appears in Am JHypertens1992;5:49].Am J Hypertens1991;4:7165—7205.
16. Fine EJ. Nuclear medicine evaluation of hypertension. UrolRadio!l992;l4:85—95.
17. Fleishman MJ, Greenspan RL, Heertum RV. The additionalvalue of visual findings in captopril-enhanced renal scintigraphy with Tc-99m MAG3. Clin Nucl Med 1993; 18:382—386.
18. Fommei E, Mezzasalma L, Ghione S. Captopril radionuclide test in renovascular hypertension: a European multicenter study. Contrib Nephro! 1990;79:205—210.
19. Fommei E, Mezzasalma L, Ghione S, et al. Europeancaptopnl radionuclide test multicenter study: preliminaryresults. Inspective renographic analysis. The European Captopril Radionuclide Test Multicenter Study Group. Am JHypertens1991;4:6905—6975.
20. Gale B, Zhang C, Lee HB, et al. The effect of captopril onglucoheptonate uptake in experimental renal artery stenosis.Nucl Med Commun 1992;13:110—113.
21. Geyskes GG, Bruyn A. Captopril renography and the effectof percutaneous transluminal angioplasty on blood pressurein 94 patients with renal artery stenosis. Am J Hypertens1991;4:6855—6895.
22. Hillman BJ. The imaging diagnosis of renovascular hypertension.UrolRadio!l990;l2:130—131.
23. Itoh K, Tsukamoto E, Nagao K, et al. Captopril renoscintigraphy with Tc-99m DTPA in patients with suspectedrenovascular hypertension: prospective and retrospectiveevaluation.CliiiNuc!Med l993;l8:463—47l.
24. Jensen G, Moonen M, Aurell M, et al. Reliability of ACEinhibitor-enhanced 99mTc@DTPAgamma camera renography in the detection of renovascular hypertension. Nuci MedCommun 1993;14:169—175.
25. Kang Z, Chen F, Wang Z. Evaluation of captopril renography with 99mTc@(@G3 in the diagnosis of renovascularhypertension [published erratum appears in Chin Med Sci Jl994;9:2l4].ChinMed SciJ 1994;9:49—5l.
26. Kletter K, Mostbeck G, Duczak R. Captopril renographyand duplex sonography: comparison of two noninvasive
methods for the diagnosis and follow-up in renovascularhypertension. Contrib Nephrol 1990;79:l90—l95.
27. Lee HB, Blaufox MD. Renal functional response to captopril during diuretic therapy. J Nuc! Med l992;33:739—743.
28. Lu ZW, Liu LS. The value ofthe captopril test and the effectof captopril on renal function. J Hum Hypertens l990;4:138—140.
29. McLean AG, Hilson AJ, Scoble JE, et al. Screening forrenovascular disease with captopril-enhanced renography.NephrolDial Transplantl992;7:211—215.
30. Meholic Al, Saddler MC, Hallin GW, et al. The captoprilrenogram in percutaneous transluminal angioplasty of therenal arteries. Am J Physiol Imaging 1992;7:36—41.
31. Meier GH, Sumpio B, Setaro iF, et al. Captopril renalscintigraphy: a new standard for predicting outcome afterrenal revascularization. J Vasc Surg l993;l7:280—285.
32. Miralles M, Santiso A, Gimenez A, et al. Renal duplexscanning: correlation with angiography and isotopic renography.EurJ VascSurg1993;7:188—194.
33. Nally JV Jr, Bedoya LA, Park CH, et al. Captoprilstimulated renography versus renal vein renins in twokidney, two-clip hypertension. Contrib Nephrol 1990;79:176—180.
34. Nally iv Jr, Chen C, Fine E, et al. Diagnostic criteria ofrenovascular hypertension with captopril renography: aconsensus statement. Am J Hypertens 199 l;4:7495—7525.
35. Nally JV Jr, Black HR. State-of-the-art review: captoprilrenography—pathophysiological considerations and clinicalobservations. Semin Nucl Med 1992;22:85—97.
36. Nally Pt Jr. Provocative captopril testing in the diagnosis ofrenovascular hypertension. Urol Clin North Am l994;2l:227—234.
37. Nortier J, Wautrecht JC, Delcour C, et al. Role of thecaptopril test in renovascular hypertension: a case report.Angiology 1992;43:939—945.
38. Oei HY. Captopril renography: early observations anddiagnostic criteria. Am J Hypertens 199 l;4:6785—6845.
39. Pedersen EB. Angiotensin-converting enzyme inhibitorrenography: pathophysiological, diagnostic and therapeuticaspects in renal artery stenosis. Nephrol Dial Transplant1994;9:482—492.
40. Pelsang RE, Rezai K. Abnormal captopril renogram in apatient without renovascular hypertension. Clin Nuci Med1992;17:303—305.
41 . Piccoli A, Pillon L. Reasonable positive predictive values ofcaptopril renography in renovascular hypertension [Letter;Comment]. Am J Nephro! l993;13:298—299.
42. Pickering TG. Diagnosis and evaluation of renovascularhypertension: indications for therapy. Circulation l991;8l(suppl2):!147—I154.
43. Roccatello D, Picciotto G, Rabbia C, et al. Prospective studyon captopril renography in hypertensive patients [see comments]. Am J Nephrol 1992; 12:406—411.
44. Sfakianakis GN, Sfakianaki E, Bourgoignie J. Lasix captopril renography in the diagnosis of renovascular hypertension. Contrib Nephrol 1990;79:2 19—227.
45. Sheps SG, Blaufox MD, Nally JV Jr, et al. Radionuclidescintirenography in the evaluation of patients with hypertension: American College of Cardiology position statement. J Am Coil Cardiol l993;21 :838—839.
46. Stansby GP, Hilson AJ, Hamilton G. Renovascular hypertension secondary to renal artery aneurysm detected bycaptopril-renography. Eur J Vasc Surg 1991;5:343—346.
47. Stansby GP, Scoble J, Hilson A, et al. Captopril renalscintigraphy—an advance in the detection and treatment of
PROCEDURE GUIDELINE FOR DIAGNOSIS OF RENOVASCULAR HYPERTENSION •Taylor et al. 1301
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from

renovascular hypertension [Letter; Comment]. J Vasc Surgl99l;l3:765—766.
48. Svetkey LP, Wilkinson R Jr, Dunnick NR, et al. Captoprilrenography in the diagnosis of renovascular disease. Am JHypertensl99l;4:7l15—7155.
49. Takata M, Yoshida K, Tomoda F, et al. Diagnostic value ofcaptopril test in hypertensive patients with renal arterystenosis. Angio!ogy 1994;45: 181—186.
50. Taylor A Jr, Martin LG. The utility of 99mTc@mercapto@acetyltriglycine in captopril renography. Am J Hypertens1991;4:7315—7365.
51. Trepashko DW, Warner D, Amida J, et al. Positive captoprilrenal scintigraphy in a patient with extensive bilateral renalinterlobar arterial disease. Clin NuclMed 1994;l9:727—730.
52. Wilcox CS. ACE inhibitors in the diagnosis of renovascularhypertension.Hosp Pract(OffEd)1992;27:117—121.
region ofthe body (e.g., probable lung carcinoma, evaluation ofhilar lymph node involvement).
Dynamic Tomographic Images: Consist of multiple sequential three-dimensional images in a limited field. This typeof acquisition often is used when quantitation of regionalmetabolic rates is needed.
Whole-Body Tomographic Images: Usually performed tosurvey the entire body to search for areas of abnormal FDGaccumulation.
Attenuation Correction: The method for correcting emission photon attenuation by either:
Transmission Imaging: A set of corresponding imagesare acquired with an external source of radiation. Typically,these images are acquired with PET.
Mathematical Attenuation Correction: Typically used inbrain imaging, where an estimated attenuation correction basedon the emission data may be used instead of actually acquiringtransmission data.
PART III: COMMON INDICATIONSA. Differentiation of benign from malignant lesions
(2,3,6, 7).B. Staging of malignant disease (7,10,11).C. Grading of malignant brain lesions (2,3).D. Differentiation of recurrent malignant disease from ther
apy-induced changes (4,9,12).E. Monitoring response to therapy for breast cancer (13).
PART IV: PROCEDUREA. Patient Preparation
1.PrearrivalPatients fast for at least 4 hr to diminish physiologic
Key Words tumor imaging; fluorodeoxyglucose; PET; procedureguideline; positron imaging
J Nuci Med I998 39I302-1305
PART I: PURPOSEThe purpose of this guideline is to assist nuclear medicine
practitioners in recommending, performing, interpreting andreporting the results of 18-fluoro-2-deoxyglucose (FDG) imaging in the evaluation of patients with suspected malignantdisease, for staging malignant disease or for monitoring ther
apy.
PART II: BACKGROUND INFORMATION ANDDEF1N@ONS
There is a growing body of evidence for the use of FDG indifferentiating malignant from benign disease, staging andgrading malignant disease, differentiating recurrent diseasefrom therapy-induced changes and monitoring response totherapy.
Depending on the clinical question and type of equipmentavailable, the FDG imaging procedure may include the following:
Limited-Field Tomographic Images: Usually performedwhen critical abnormalities are likely to be localized in a known
For correspondence or reprints, contact: Wendy J.M. Smith, Director of Health CarePolicy, Society of Nuclear Medicine, 1850 Samuel Morse Dr., Reston, VA20190-5316,orby [email protected].
Note: aM26 SNM-approved procedureguidelines areavadabison the Society's homepage. We encourage you to download these documents via the Internet at www.snm.org. If you would I@e @iformationon the development of this guideline or to ordera compendium of all 26 precedure guidelines for $20.00, contact Marie Davis@SocietyofNuclearMedicine,at(703)708-9000,ext250,[email protected].
1302 THEJOURNALOFNUCLEARMEDICINE•Vol. 39 . No. 7 •July 1998
PART VIIP@LAST HOUSE OF DELEGATES APPROVAL DATEJanuary 14, 1996
PART IX: NEXT ANTiCIPATED APPROVAL DATE1998
ACKNOWLEDGMENTSHenry D. Royal, MD, immediate past-chair of the Guidelines
and Communications Committee, Commission on Health CarePolicy and Practice, for overall coordination and oversight of theSociety of Nuclear Medicine Guideline Development Project;Wendy J.M. Smith, MPH, Director of Health Care Policy, Societyof Nuclear Medicine, for project coordination, data collection andediting; and members of the Guideline Development Subcommittee, who contributed their time and expertise to the development ofthisinformation.
Procedure Guideline for Tumor Imaging UsingFluorine- 18-FDGHeinrich R. Schelbert, Carl K. Hoh, Henry D. Royal, Manuel Brown, Magnus N. Dahlbom, Farrokh Dehdashti andRichard L. WahlUniversity of Ca4fornia Los Angeles School ofMedicine, Los Angeles, California; Mallinckrodt Institute of Radiology,St. Louis, Missouri; University ofPittsburgh Medical Center, Pittsburgh, Pennsylvania; andUniversity ofMichigan Medical Center, Ann Arbor, Michigan
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from

1998;39:1297-1302.J Nucl Med. Fommei, Gijsbert Geyskes, Goran Granerus and Hong-Yoe OeiDaniel Kahn, Kathryn A. Morton, Charles D. Russell, George N. Sfakianakis, Mattias Aurell, Maurizio Dondi, Enza Andrew T. Taylor, Jr., James W. Fletcher, Joseph V. Nally, Jr., M. Donald Blaufox, Eva V. Dubovsky, Eugene J. Fine, Procedure Guideline for Diagnosis of Renovascular Hypertension
http://jnm.snmjournals.org/content/39/7/1297.citationThis article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1998 SNMMI; all rights reserved.
by on April 4, 2020. For personal use only. jnm.snmjournals.org Downloaded from











![Volume 2389, II-1297 - UN PeacemakerSecure Site YE_340… · Volume 2389, II-1297 [TRANSLATION - TRADUCTION]1 1. Translation supplied by the Government of Saudi Arabia - Traduction](https://img.pdfslide.us/doc/110x75/6078a1866e8032000475b8e4/volume-2389-ii-1297-un-peacemakersecure-site-ye340-volume-2389-ii-1297-translation.jpg)




![Volume 2389, II-1297 - UN Peacemakerpeacemaker.un.org/sites/peacemaker.un.org/files/SA YE... · 2018. 12. 20. · 315 Volume 2389, II-1297 [TRANSLATION - TRADUCTION]1 1. Translation](https://img.pdfslide.us/doc/110x75/6078a2e15c8fea1898347d95/volume-2389-ii-1297-un-ye-2018-12-20-315-volume-2389-ii-1297-translation.jpg)










