Embed Size (px)
Citation preview

POSTGRAD. MED. J. (I961), 37, 259
PROBLEMS RAISED BY THE TREATMENTOF STEATORRHOEA WITHANTIBACTERIAL DRUGS
J. M. FRENCH, M.D., M.R.C.P., Ph.D., D.T.M. & H.WVelicome Research Wing, Department of Medicine, University of Birmingham and Queen Elizabeth Hospital, Birmingham
CELIAC disease in children, with its counterpartidiopathic steatorrhaea in adults, is one of thecommonest and, perhaps, the most important ofthe malabsorption syndromes. Serious searchfor a bacterial origin for these conditions more orless ceased over 40 years ago. and for a long timethey were relegated to the group of deficiencydiseases. During the last decade the discovery thatremoval of wheat and rye gluten from the diets ofill coeliacs resulted in recovery in almost allinstances has revolutionized not only the treat-ment and prognosis of the condition but alsotheoretical consideration of the mechanism ofdefective absorption in these patients. Develop-ments in biopsy techniques in the last five yearshave allowed histological study of fresh smallintestinal mucosa, and it has become apparentthat in most of these cases there are abnor-malities of the villi and intestinal epithelium,which might account in some measure for themalabsorption. As it is quite an easy matter toproduce a malabsorptive state in a caliac childwho has recovered on a gluten-free regime simplyby re-introducing gluten into the diet, consider-able thought and experimental work has goneinto efforts to link together malabsorption, thealtered epithelial appearance and the deleteriouseffects of gluten.The mechanism of the gluten effect in cceliac
disease is still quite obscure; several investigatorshave concentrated on isolating toxic factors fromwheat gluten and gliadin. Weijers and van deKamer (I960) showed high blood glutaminevalues after a loading dose of gliadin; as glutamineitself was not harmful, they concluded that aglutamine-containing peptide was the injuriousagent, and they thought it reached the blood froman enzymatic defect in the mucosal cells of thesmall intestine affecting peptide digestion. Frazer(1956) and Krainick (1958) took into account thepossibility that the peptides also contained proline,and postulated a prolinase or prolidase deficiency.These suggestions are difficult to reconcile with
the fact that many other proteins, casein forexample, contain almost as great a proportion ofglutamine and proline as gluten, yet they can befed to cceliac children in much greater amountsthan gliadin without causing trouble. Schneider,Bishop and Shaw (I960) have drawn attention tosubstances derived from the digestion of glutenwhich inhibit a peristaltic reflex of the smallintestine of the rat but they found substanceswith a similar action in muscle and casein also.Although interesting, the relevance of thesefindings to cceliac disease awaits clarification. Allreports on small intestinal biopsy findings inceliac disease and idiopathic steatorrhcea drawattention to the lack of correlation between themucosal appearance and the absorptive state, asjudged by the fat excretion. It is not clear,therefore, whether the 'toxic factors', epithelial,changes and malabsorption are closely related, orindeed, whether there is any direct relationship, soadditional factors must still be given considerationin the production of malabsorption in theseconditions. Those most deserving of study areexcessive production of mucus, defective smallbowel motility, defective mucosal enzymes (Daw-son and Isselbacher, I960), and abnormal gutflora. This paper is concerned only with evidencefor and against the last consideration.
It is often evident in both child and adultpatients with caliac disease and tropical spruethat there is excessive fermentation in the stools.Many patients complain of excessive borboryg-miasis and evil-smelling flatus, which indicatethat abnormal fermentation and putrefaction aretaking place within the intestinal canal. If radio-graphs are taken of the abdomen of such patientsin the upright position, it is common to see manyfluid levels with gas over them in the small intes-tine as well as in the colon. This excess of gascould be due to aerophagy or to a circulatorydisturbance of the gut rendering it unable toremove gases, as believed by de Langen (1953).Gas production could be due to excessive fer-
copyright. on A
pril 9, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.259 on 1 M
ay 1961. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
mentation of carbohydrate by intestinal bacteria.This explanation would fit in with the frothycharacter of the stools which is so often seen.Observations of this nature, though crude, aresuggestive, in florid cases at least, that some typeof abnormal bacterial fermentation within thelumen of the gut is worthy of consideration.Unfortunately the inaccessibility of the bowel,especially the small intestine, and the rapidalterations of its contents during digestion, dueto changes in rates of secretion, absorption andgut motility, have made it extraordinarily difficultto characterize exactly what is taking place. Inaddition, there are great practical difficulties inculturing intestinal juice to obtain a true quantita-tive picture of the organisms in a single sample,and culturing numerous samples from differentlevels in the intestine at various stages of digestionpresents at the moment an almost insuperableproblem. Multiple examinations, however, areessential for proper evaluation, as it is wellrecognized that the flora varies enormously atdifferent levels in the small and large bowel evenin normal subjects. It is not surprising, therefore,that in spite of many and varied studies of thesubject, no clear picture has emerged in patho-logical conditions. Although the direct bacterio-logical approach of culture of intestinal contentshas tended to show that the flora in malabsorptionis not different from normal, approaches to theproblem from other angles, especially by the use ofantibiotics, suggest that an entirely different viewmay eventually have to be taken. The mainquestions at issue are: firstly, has any substantialevidence of an abnormal gut flora in malabsorptivestates ever been established, and if so, secondly,should such a floral change be regarded as primaryor secondary?As the mechanisms underlying the absorptive
defect in quite a number of malabsorption syn-dromes are not well understood, it may serve auseful purpose to compare evidence from a con-dition such as cceliac disease, with what is knownabout tropical sprue, gastro-jejuno-colic fistula,diverticulosis of the small intestine, blind loopsyndromes, Whipple's disease and even gas-trectomy. What may be learnt from the study ofone may be applicable in some degree to all,despite what appear to be different origins for themalabsorption.
Total Weight of Bacteria in the StoolSome 25% or more of the dried weight of a
normal stool is due to bacteria (Spencer, I960)most of which have developed within the gut. Noattempts appear to have been made to assess theweight of bacteria in malabsorption, though thedried weight of stool is greater than normal, the
increase being more than would be accounted forby the excess fat alone (Comfort, Wollaeger,Taylor and Power, 1953, Cooke, Thomas,Mangall and Cross, 1953, Hendry, I960). Itmight be possible to decide if there was an increasein numbers of bacteria by dilution, centrifugationand nephelometry against standard bacterialsuspension (Goiffon, 1946).
Specific OrganismsAfter careful bacteriological study of many
frcal samples from coeliac children, Herter (I908)concluded that the condition was caused bypersistence through childhood of a bacillus whichwas normally present only in babyhood. Thiswas a gram positive rod-like organism predomi-nant in the feces of his cceliac children, which hecalled B. infantilis. It is no longer known by thisname. It is probable that he was describingLactobacillus acidophilus, which is often presentin large numbers in the stools of patients withmalabsorption of various origins together withanother aciduric group, Cl. actobutylicum (iodophilbacteria, Goiffon, I949). In tropical sprue, on theother hand, Ashford (19I7) held the view formany years that a yeast (Monilia psilosis) wasresponsible. Although his conclusions supportedthose of Kohlbrugge (I9OI), they have never metwith general acceptance. It is commonly believedthat excessive yeasts and lactobacilli are due tothe presence of unabsorbed fermentable carbo-hydrate and that they are therefore secondaryinvaders. The fermentation products of theseorganisms could conceivably add to the sympto-matology by exacerbating diarrhcea for instance,but this aspect has not been studied satisfactorily.Later investigations of feecal flora have shown noconsistent picture (Mackie, Gore, and Wadia,1928) and although it is now generally believedthat neither sprue nor coeliac disease is due to aspecific organism, the idea dies hard and it hasrecently been suggested on general grounds thattropical sprue is primarily due to a virus infection(Manson-Bahr, I953).
Bacteriological Studies of the Upper IntestineAn obvious approach to the study of the
bacterial population of the gut is by peroral intuba-tion (Kendall, Day, Walker and Haner, 1927).Using this technique, Olleros (1942) noted aninvasion of the stomach in tropical sprue by gram-positive and gram-negative organisms, the majorityof the latter being coliforms, but no significantchange from normal was found in the smallintestine in patients with tropical sprue (Milanes,Curbelo, Rodriguez, Kouri and Spies, 1946,Nadel and Gardner, 1956), or in idiopathicsteatorrhaea (French, Peeney and Thompson,
May I96I'26ocopyright.
on April 9, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.427.259 on 1 May 1961. D
ownloaded from

May I96I FRENCH: Problems Raised by the Treatment of Steatorrhcea with Antibacterial Drugs 26i
BACTERIOLOGY OF INTUBATION STUDIES
IN IDIOPATHIC STEATORRHOEA (NON TROPICAL SPRUE)
VIABLE COUNTS c . DILUTION IN WHICH COLIFORMSCt*d%sento WERE PRESENT
COLONIPER ML STOMACH DUODENUM ML. STOMACH DUODENUMOF JUw 7
0 0
o0 0 0
id
0
0.0.
00 0
0 * i
NTo 00 00 CB o
NORMAL' N.T.SPRUJE NORMALS NTSPRUE NO TLS1SPRU- NORMALS N.T SPRUESUIBJECTSIII
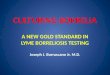
FIG. i.-Comparison of cultures ofthe contents of the stomachand duodenum in normal sub-jects and patients with idio-pathic steatorrhea. Viablecounts of four main groupsonly were determined, viz.coliforms, lactobacilli, entero-cocci, and clostridia. Theresults suggested that there wasno significant difference be-tween the two groups ofindividuals either in stomach orduodenum. No sterile cultureswere encountered using anintubation technique. Thepatient with the highest bac-terial count in stomach andduodenum (1o01 and io9 respec-tively) had bronchiectasis,with E. coli in the sputum.(French, Peeney and Thomp-son, 1949.)
I949) (Fig. i) or in coeliac disease (Anderson andLangford, 1958).One of the main difficulties with intubation
studies is contamination of the tube by mouthorganisms. This has been overcome to someextent by occluding the distal holes with latex,sterilising the tube, and disrupting the latex witha syringe full of air when the tube is in position inthe intestine (French, Peeney and Thompson,1949). An alternative technique adopted by othersdisregards organisms which can also be culturedfrom the mouth as 'transient' intestinal flora andtherefore of no significance. Whether this is avalid assumption in the presence of malabsorptionis another matter. Baker and Achaya (I96I)adopting the method of Cregan and Hayward(I953) needled the intestine at laparotomy inthree cases of tropical sprue; cultures of the fluidobtained were sterile. In general it may be saidthat as far as the present experimental work hasgone, no gross and possibly no significant con-tamination of the upper small intestine with fecalorganisms has been demonstrated in these mal-absorptive states. One important omission in theexperimental work to date must be noted however.All the studies mentioned here dealt with patientsin a fasting state, when the cleansing effects ofgastric acidity, peristaltic movements of the guttowards the colon and the absence of food wouldgive the least favourable conditions for retention orsurvival of any colonies of bacteria within thelumen of the small intestine; but conditionsduring feeding may be quite different. Coliforms,in ideal conditions, divide once every 15 minutesor so. If the nutrient medium is absorbed in
normal subjects, say, for the sake of argument, inhalf an hour, one coliform might divide to becomefour, but if the same absorption process took 4hours, as it might well do in malabsorption (Craneand Neuberger, I960) then one coliform mightdivide to become 6o,ooo organisms. The reallysignificant experiments might well lie in a series ofstudies designed to elucidate what happens to thegrowth of bacterial flora throughout a 24-hoursperiod. The complexity of such a procedure isformidable but an interesting finding has beenrecorded by Anderson and Langford (1958), whoobserved gross contamination by fiecal flora if thetube was allowed to lie within the intestine for24 hours, after fasting studies had shown a normalflora. They were uncertain whether this repre-sented growth within the tube or within the gut.Until some studies of this nature have been carriedout, it would be unwise to conclude that the smallintestinal flora after feeding in the presence ofmalabsorption is necessarily normal, since atpresent the only available evidence has beenderived from subjects in a fasting state.
Influence of Antibiotics on Diarrhoea andSteatorrhoea
If intestinal bacteria play some part in themalabsorption syndromes, their influence couldbe studied retrospectively by an examination ofthe effect of their elimination by antibiotic drugs.Unfortunately, even with the large array of anti-biotics effective in suppressing intestinal organ-isms, no single drug, or combination of drugshas been shown to eliminate all organisms (Kirsner,Levin and Palmer, 1952). The removal of a
copyright. on A
pril 9, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.259 on 1 M
ay 1961. Dow
nloaded from

262 POSTGRADUATE MEDICAL JOURNAL May I96I
sensitive species quickly results in an overgrowthof insensitive bacteria and yeasts. The complexbacterial changes which take place in the intestinaltract during antibiotic therapy have not yet beenstudied extensively in malabsorption states.Nevertheless, several studies already indicate thatantibiotics may have a great influence on thebacterial population and that malabsorption hasbeen cured and induced by antibacterial drugs.
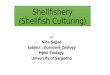
In tropical sprue, seven patients were cured aftera course of combined drugs (French, Gaddie andSmith, 1956), and this effect was confirmed byCaroli, Le Quintrec and Reboul (1957). Similarcourses of antibiotics were used by Baker (1957) ina few patients with sprue in India. Some appearedto show lasting improvement but in others littleor no improvement was noted. A third groupimproved as judged by the fat balance during thecourse of chemotherapy, but they relapsed later.The cure of a case of 'indigenous' sprue withchloromycetin followed by aureomycin was de-scribed by Renner (1952). In I5 patients withidiopathic steatorrhoea resistant to a gluten-freediet we have tried chemotherapy in addition to thediet (Crane and French, I96I). In six of these, nochange took place in the absorptive state, asjudged by the fat excretion. In four, fat absorptionbecame normal within a few days, though in oneof them steatorrhcea returned a week after stoppingthe drugs (Fig. 2); one made a striking clinicalimprovement but no fat studies were done; in fourthe diarrhera and steatorrhoea were greatlyincreased. In two of the latter group, diarrheeaincreased almost to choleraic proportions and thedrugs had to be stopped. Bacteriological studiesprovided no evidence that the increase in diarrhcrawas staphylococcal in origin. Wirts and Goldstein(I960) reported a patient cured with neomycin.In caliac disease, we have seen no significantchanges in fat absorption in several childrentreated with antibiotics. In Whipple's disease,the abatement or disappearance of diarrheea andsteatorrhaea has been noted after chloramphenicol(Paulley, I952), chlortetracycline (Schaffner andScherbel, I955), sulphasalazine (Haex and vanBeek, 1955, Kooreman, I957), and tetracycline(England, French and Rawson, I960). In diverti-culosis of the small intestine, diarrhiea disappearedafter therapy with one or other of the tetra-cyclines (Dick, I955, Badenoch, Bedford andEvans, I955, Blachford and Dawson, 1956,Gellman, I956). Although steatorrhcea wasproved to be present in these patients, no observa-tions were made of the effect of the antibiotics onfat absorption, but Watkinson, Feather, Marsonand Dossett (I959) showed that steatorrhoeadisappeared with tetracycline therapy in theirpatient, and we have observed the same in one
IDIOPATHIC STEATORRHOEA(70 gm. fat diet)
EFFECT OF ANTIBIOTICS
WT 60Kg.
55.
3-DAY MEAN EXCRETION OF FATTY ACID
GM. >A!AEAAi!
40 ot
40 60 80B.W. DAYS
FIG. 2.-Fat excretion during antibiotic therapy in apatient with idiopathic steatorrhcea of thirty yearsduration, who had been having a gluten-free diet fora year previously with only slight improvement.During the course of antibiotics (aureomycin anderythromycin) fat excretion became normal, butincreased again some days after stopping the drugs.
patient (French and Hawkins, I96I). In severalpatients with malabsorption after partial gas-trectomy, in whom there was afferent loop stasis,oral antibiotics cured the steatorrhcea (Kinsella,Hennessy and George, I960, Goldstein, Wirtsand Kramer, I96I). In gastro-colic fistula, fewnow believe that the steatorrhcea is due to a by-passing of the small intestine, as assumed byBennett and Hardwick (1940) in their concept ofileo-jejunal insufficiency. It seems most likely thatthe seepage of fiecal bacteria from the colon intothe upper small intestine results in a 'jejuno-ileitis', a mild inflammatory process from un-specified toxic products of bacterial metabolism.There is no suggestion that any specific bacteriaare involved, yet the steatorrhcea is always a severeone, and patients usually go downhill very rapidly.Mere diversion of the faccal stream by colostomymay improve their nutrition enormously beforerepair of the fistula is undertaken. In two patientswith gastro-colic fistula, we have noted a short-lived improvement of fat absorption with anti-biotic therapy; the benefit derived from treatmentwith intestinal antibiotics is now regarded as oneof the mainstays of pre-operative preparation(Kay, I960). In a patient with blind-loop syn-drome, neomycin cured the steatorrhaea, though
copyright. on A
pril 9, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.259 on 1 M
ay 1961. Dow
nloaded from

May I96I FRENCH: Problems Raised by the Treatment of Steatorrhca with Antibacterial Drugs
it returned gradually afterwards (Kay, I960). Itmay well be that the rare cases of post-gastrectomysteatorrhkea which respond to antibiotics areinstances of blind-loop syndrome analagous tothose in the lower gut (Goldstein et al, I96I).Apart from our own group of four patients withadult celiac disease whose steatorrhcea was mademuch worse, all these studies record improvementof absorption with antibiotics.On the other hand, there is evidence that anti-
biotics can induce steatorrhcra. It is well recog-nized that when given orally they may causediarrhea. This is loosely attributed to the irritanteffect of the drug, changes in intestinal bacteria orgrowth of yeasts. Sometimes the intestinal upsetspersist for weeks or months after withdrawal ofthe drugs. Little attempt has been made to definethis common disorder, but Merliss and Hoffman(195I) described several patients with a steatorr-hea syndrome which developed after antibiotictherapy. Recently, there have been several reportsof a more clearly defined malabsorptive state,including changes in the intestinal villi, inducedby large doses of neomycin (Jacobson, Chodosand Faloon, I960). Although in the disorderdescribed by Merliss and Hoffman, a floralchange within the intestine seems the most likelyexplanation, in the neomycin-induced syndromethe doses used were so large (12 gm. daily) that adirect toxic effect upon the intestinal epithelium orenzyme systems must also be considered.
It is clear from this survey that antibiotics mayeither ameliorate or worsen malabsorption; itmay also actually induce it in previously normalsubjects. Although there are few supportingbacteriological studies, it is likely that the changesare related closely to alterations in the intestinalflora. In all the pathological states described, theintestine is altered in such a way that bacteriamight be expected to proliferate in abnormalnumbers, though it is not yet proved that they infact do so. The range of antibacterial drugs is sowide that it seems most unlikely that the changescould be due wholly to specific metabolic effectsof the drugs themselves but this cannot yet bedisregarded. One of the most instructive reportsas to the role of bacteria is provided by the work ofWatkinson et al (I959) in a patient with diverti-culosis of the small intestine. Antibiotic therapycured the steatorrhoea so long as the drug wasgiven. The bacteria cultured from the diverticulawere normal intestinal inhabitants. When theworst-affected area was resected, steatorrhceadisappeared, despite shortening of the intestinefrom the removal of 70 cm. of jejunum. Thisstrongly suggests that the steatorrhcea was due toseeding of the upper intestinal contents with bac-teria from areas of stasis in the diverticula. A
similar idea would explain the disorders en-countered in gastro-colic fistula, blind loops andsome cases of post-gastrectomy steatorrhaea. Ingastrectomy patients, Goldstein et al (I96I) wereable to show that the good response to antibioticswas in those with an abnormally high bacterialcount in the afferent loop juice. The anastomoseswere antiperistaltic, the loops were long, andthere was achlorhydria, all conditions favouringthe growth of organisms naturally occurring inthe gut. Where there is no isolated source ofseeding, as in sprue, adult cceliac disease and otherconditions such as Whipple's disease and systemicsclerosis, delay in absorption with poor motilityof the small intestine might result in an analagoussituation, in which the presence of only a fewnormal bacteria would suffice, but they wouldhave an unusually long period in a mediumenriched by the unabsorbed products of digestion,in which they could grow readily. Their role in allthese states could be regarded as secondary inthe sense that some other condition was necessarybefore they could cause steatorrhcea. One remark-able feature that needs consideration is that in allthose instances in which a source of bacterialseeding of the intestine could be identified, onlynormal intestinal organisms were grown onculture, and the same would, no doubt, apply inthe case of gastro-colic fistula, one of the mostsevere forms of malabsorption. How does itcome about that normal organisms in their usualhabitat can give rise to such a severe upset? Itdoes not seem likely that their mere presencewould cause malabsorption, as might Giardialamblia, for instance, applied to the duodenal andjejunal walls. It seems more reasonable to supposethat the malabsorption is due to some effect oftheir products of metabolism, or dissolution, andalthough these might be complex toxins, theycould equally be quite simple substances, such asamines, or organic acids. It is possible that the keyto this situation is their rapid growth in thepresence of food, and that there is no heavybacterial contamination until food is actually pre-sent. In this respect, an interesting analogy inveterinary medicine is worth recounting; entero-toxamia of sheep is a highly fatal condition causedsimply by abruptly feeding wheat to animals usedto a hay diet (Bullen and Scarisbrick, I957). Theunusual flow of starch into the small intestine isfollowed by an intense fermentation by Strepto-coccus bovis and the animals die in acute acidosis,with blood pH as low as 6.6, from the absorptionof large amounts of organic acids; if they survivethis, they may succumb from toxamia from thedevelopment of enormous numbers of clostridiawithin the intestine. The organic acids may playa further part by making the mucosal walls more
263copyright.
on April 9, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.427.259 on 1 May 1961. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
permeable to toxic materials ordinarily retained inthe lumen. The amount of wheat fed is critical.If it is introduced into the diet gradually, notoxwemia ensues, as the bacteria of the rumen, anorgan tolerant of acid fermentation, t'hen havetime to change slowly to amylolytic types. Theacids, streptococci, clostridia and their toxins arepresent normally in the sheep, but in smallerquantities, and the toxamia from fermentationwithin the small intestine appears to be due notso much to the type of flora as to its rapidlygrowing nature, a conception well borne out bythe work of Jenkin and Rowley (1959).From the report of Merliss and Hoffman (I95 I),
it still seems possible that bacteria could also be aprimary cause of malabsorption. If it is assumedthat their patients had normal small intestinesprior to the course of antibiotics, steatorrheamust have resulted simply from a change of flora,provided it can also be assumed that injury to themucosa was not part of the antibiotic action.Malabsorption persisting for some months follow-ing acute infective enteritis has recently beennoted by King and Joske (I960) and Crismer,Dreze and Demelenne-Jaminon (1959) reportedsteatorrhcea from enteritis due to Proteus hausericured by neomycin. These observations mighthave a bearing on the etiology of tropical sprue. Itis fully recognized that the types of bacteriapredominating in the intestine depend almostentirely on the kind of food ingested and residuesat various levels. It might well be that in someareas of the tropics, the type of diet or presence ofsome special dietary constituent is all-importantfor the initiation of tropical sprue, in that it leadsto the establishment of a type of flora whichgradually injures the mucosa. Once malabsorptionhas begun it is easily maintained by normalintestinal organisms. There seems no goodreason to believe that tropical sprue is primarilydue to vitamin deficiencies as it is well recognizedthat many sprue patients have had an excellentdiet at the time of onset of their illness (French,Gaddie and Smith, I956).The anomaly of malabsorption being both
created and cured by antibiotics need not be takenas evidence against the general thesis that thealterations are due to floral changes. At present,the impossibility of sterilizing the intestinal tractby any drug and the difficulties involved intracing bacterial changes during such therapy haveprevented a proper day-to-day evaluation whichmight explain these apparent inconsistencies.
Influence of Antibiotilcs on the Absorptionand Excretion of Materials Other than Fatand WaterThe prominence of the fatty nature of the
stools of patients with malabsorption, and theease with which fat is recovered and measuredchemically have tended to obscure the importanceof measuring other excreted products. Someattention has been paid to nitrogen, but noreports have been made of the influence of anti-biotics on nitrogen excretion in these conditions.The pallor of the stools is mainly due to altera-
tions in the type of bile pigment in the faces.When antibiotics are given, the stools undergochanges in colour which differ according to theantibiotic used. In tropical sprue stercobilin andstercobilinogen are reduced in amount andbilirubin and biliverdin are increased (French,Gaddie and Smith, 1956). There is little doubtthat these changes are the result of alterations inflora induced by the drugs, and parallel thoseseen in normal subjects (Sborov, Jay and Watson,195 I, Goiffon and Goiffon, I954). After cessationof tetracycline therapy, stercobilin (tetrahydro-mesobilene, b) returns to colour the faces, buturobilin (mesobilene, b) returns largely as d-uro-bilin, instead of the normal i-urobilin (Sborovet al, I95I, Gray and Nicholson, 1958). D-uro-bilin, which tautomerizes readily to a mesobili-violin, may be excreted for months after with-drawal of tetracycline. This explains the deep-violet colour of processed stool extracts sometimesseen after tetracycline has been used, and indicatesthat long after the immediate influence of thedrug has gone, some floral change persists, thenature of which is quite unknown. Increasedfiecal porphyrins have been reported in 'sprue' byVanotti (I954) and in a man with Whipple'sdisease (England, French and Rawson, I960).During treatment of this patient with chlor-tetracycline for his steatorrhiea, the amounts offacal porphyrins were strikingly reduced, indicat-ing that they were probably largely of bacterialorigin. At the same time, a chronic sunlight-sensitive dermatitis faded rapidly, having failed torespond to nicotinic acid given during a two-month period beforehand. This observationsuggests that the pellagroid dermatitis sometimesseen in malabsorption is due to the presence ofabnormal amounts of porphyrins and not tonicotinic acid deficiency as usually thought.It also re-opens the question of the origin of thesunlight dermatitis in true pellagra. In a numberof patients with steatorrhea of the adult celiactype, fical porphyrins were found to be greatlyincreased, both copro- and protoporphyrin beingin excess; frequently other porphyrins (deutero-and meso-) were present in the fxces in abnormalquantities also, but total daily excretion in theurine was normal (England and French, I96I).Indican, indigoid pigments and other indole andskatole derivatives may be found in excess in the
264 May I96Icopyright.
on April 9, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.427.259 on 1 May 1961. D
ownloaded from

May I96I FRENCH: Problems Raised by the Treatment of Steatorrhcea with Antibacterial Drugs 265
URINARY INDICANEFFECT OF ANTIBIOTICS
Mg. DAILY lU I CHL |
40
20
0 M10 20 30
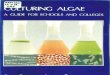
DAYSFIG. 3.-Urinary indican in a patient with idiopathic
steatorrhcea, during treatment with aureomycin andchloromycetin. There was a striking decrease withaureomycin followed by an increase with the seconddrug.
urine (Rimington, 1946, Horning and Dalgliesh,1958). The amounts may be reduced by anti-biotics (Fig. 3), denoting their bacterial origin, andthey are therefore probably to be found in excessin the faeces. Important pharmacological effectsin sprue have been attributed to the porphyrins(Vanotti, 1954) and to the skatoles (Horning andDalgliesh, 1958). In a study of patients with idio-pathic steatorrhcea, Boscott and Cooke (I954)reported an excess of p-hydroxyphenylacetic acidin the urine and attributed this to an upset in thetyrosine metabolism due to a lack of ascorbic acid.Attention was first drawn to this excessive excre-tion (as oxyphenylacetic acid) by Herter (I908) incceliac disease, and attributed by him to excessivebacterial action in the gut. Study of the excretionbefore and during antibiotic therapy would settlewhich of these views is correct.
VitaminsPatients with severe malabsorption may show
manifestations of vitamin deficiency of almost anytype. This may be due to simple malabsorption ofthe vitamin concerned, as seems likely in the case
of folic acid and the fat soluble vitamins, forinstance, or to some more subtle form of mal-absorption, as in the destruction, deviation, orfailure to synthesize by intestinal organisms. Onlyin the case of vitamin B12 so far has there beenevidence offered on these points. A rise of reti-culocyte count with subsequent heematologicalimprovement after antibiotic courses in a patientwith a cul-de-sac of the small intestine was notedby Naish and Capper (1953) and similar observa-tions have been reported since in other steatorr-heas. This has suggested that bacteria take upvitamin B12 to the detriment of the host and thisinterpretation has been confirmed in a number ofinstances by improved absorption of radioactivecyanocobalamin after antibiotics in diverticulosis,blind loop syndromes and tropical sprue (Badenochet al, I955, Gellman, I956, Halsted, Swendseid,Lewis and Gasster, I956, Mollin, Booth andBaker, 1957, Scudamore, Hagedorn, Wollaegerand Owen, 1958, Badenoch, I960, Doig andGirdwood, I960) though there is little or noimprovement in idiopathic steatorrhcea. Thechoice of antibiotic was important; tetracyclineswere effective whilst neomycin was not (Halstedet al, 1956).
It has been suggested by Badenoch (i960) thatvitamin K deficiency might be precipitated byantibiotic therapy. In 195I, we studied a patientwith idiopathic steatorrhra who was given a sixweeks' course of succinylsulphathiazole in normaldaily therapeutic dosage. Within a few days ofstopping the drug, she developed bixmorrhagiceffusions in skin, muscles and joints, and herh2emoglobin fell from go% to 40%. She had notpreviously shown any hlemorrhagic tendency,though this has been described in steatorrhcea in anumber of instances. Her prothrombin activity atthe time of the onset of her hamorrhagic conditionwas estimated as nearly zero. Twenty-four hoursafter administration of vitamin K intramuscularly,it was 67% and the following day ioo%. Thisseemed clearly a case where the sulphonamidedrug had interfered with bacterial synthesis ofvitamin K in the gut.
SummaryI. It may be concluded that ovex the past few
years evidence has steadily accumulatedwhich indicates that bacteria play animportant part in the symptomatology ofmany of the malabsorption syndromes.Owing to the technical difficulties of thebacteriological approach to the problem,their role up till now has largely beenregarded as secondary.
2. Many bacterial metabolites are present inexcess in the urine and fmces of patients
copyright. on A
pril 9, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.259 on 1 M
ay 1961. Dow
nloaded from

266 POSTGRADUATE MEDICAL JOURNAL May I96I
with these conditions, and, apart from theppssibility of cure, antibiotics offer anexcellent weapon for attacking problemsconnected with their formation, excretionand pharmacological importance.
3. They may also be used to study the forma-tion, absorption or destruction of vitaminsand other materials by intestinal bacteria.
4. Study of patients with malabsorption byantibiotics has produced increasing evidencethat bacteria play more than just a secondaryrole in the production of symptoms, and insome cases they appear to play an integralpart in the mechanism by which mal-absorption is maintained. It may in time be
shown that intestinal bacteria play a primaryrole in the causation of some of the syn-dromes.
5. From the therapeutic point of view anti-biotics have curative value in some instances,but cause deterioration in others. Moreextensive study of their action shoulddisclose the reasons underlying this dis-crepancy.
I wish to acknowledge the unstinted support and helpof Professor W. Melville Arnott. I am grateful to theUnited Birmingham Hospitals Endowment Fund, theStag Charitable Trust (Watney Mann Ltd.) and theMedical Research Council for financial assistance.
REFERENCESANDERSON, C. M. and LANGFORD, R. F. (1958): Bacterial Content of Small Intestine of Children in Health, in Celiac
Disease, and in Fibrocystic Disease of the Pancreas, Brit. med. J., i, 803.ASHFORD, B. K. (1917): The Etiology of Sprue, Amer. J. med. Sci., IS4 I57.BADENOCH, J. (I960): Steatorrhcea in the Adult, Brit. med. J., ii, 879.
, BEDFORD, P. D., and EvANS, J. R. (1955): Massive Diverticulosis of the Small Intestine with Steatorrhea andMegaloblastic Aniemia, Quart. J. Med., 24, 321.
BAKER, S. J. (1957): Idiopathic Tropical Steatorrhcea, Indian J. med. Sci., iI, 687.and AcHAYA, K. (I96I): To be published.
BENNErT, T. I. and HARDwICK, C. (I940): Chronic Jejuno-ileal Insufficiency, Lancet, ii, 38I.BLACHFORD, R. D. and DAWSON, D. W. (1956): Association of Jejunal Diverticulosis with Macrocytic Aniemia, Brit.
med. J., i, 1407.BOSCOTT, R. J. and COOKE, W. T. (1954): Ascorbic Acid Requirements and Urinary Excretion of p-Hydroxyphenylacetic
Acid in Steatorrh.ea and Macrocytic Anemia, Quart. J. Med., 23, 307.BULLEN, J. J. and SCARISBRICK, R. (I957): Enterotoxwmia of Sheep. Experimental Reproduction of the Disease, J. Path.
Bact., 73, 495.CAROLI, J., LE QUINTREC and REBOUL (1957): Le Traitement des Steatorrhees Eventuellement Compliques de Steatose
Massive du Foie par les Antibiotiques, Arch. Mal. Appar. dig., 46, 613.COMFORT, M. W., WOLLAEGER, E. E., TAYLOR, A. B., and POWER, M. H. (1953): Non-tropical Sprue: Observations on
Absorption and Metabolism, Gastroenterology, 23, I55.COOKE, W. T., THOMAS, G., MANGALL, D., and CROSS, H. (I953): Observations on the Fecal Excretion of Total Solids,
Nitrogen, Sodium, Potassium, Water and Fat in the Steatorrhcea Syndrome, Clin. Sci., 12, 223.CRANE, C. W. and FRENCH, J. M. (I961): To be published.
and NEUBERGER, A. (I960): Absorption of 15N Labelled Yeast Protein in Adult Coeliac Disease, Brit. med. 7., ii, 8i 5.CREGAN, J. and HAYWARD, N. J. (1953): The Bacterial Content of the Healthy Human Small Intestine, Brit. med. 37.,
i, 1356.CRISMER, R., DRtZE, C., and DEMELENNE-JAMINON, G. (1959): Gu6rison par la Neomycine d'une Steatorrhee Associee
a une Enterite i Proteus Hauseri: Relation des Steatorrhees Infectieuses avec la Sprue Nostras, Acta gastroent.beig., 22, 47.
DAWSON, A. M. and ISSELBACHER, K. J. (I960): The Esterification of Palmitate -i-C14 by Homogenates of IntestinalMucosa, Y. clin. Invest., 39, I50.
DE LANGEN, C. D. (I953): Steatorrhcea and the Intestinal Circulation, Acta med. scand., x46, 7.DICK, A. P. (I955): Association of Jejunal Diverticulosis and Steatorrhcea, Brit. med. Y., i, 145.DOIG, A., and GIRDWOOD, R. H. (I960): The Absorption of Folic Acid and Labelled Cyanocobalamin in Intestinal
Malabsorption, Quart. 7. Med., 29, 333.ENGLAND, M. T. and FRmCH, J. M. (I96I): To be published.
I , , and RAWSON, A. B. (I960): Antibiotic Control of Diarrhcea in Whipple's Disease, Gastroenterology, 39, 219.FRAZER, A. C. (1956): On the Growth Defect in Cceliac Disease, Proc. Roy. soc. Med., 49, IOO9.FRECH, J. M., GADDIE, R., and SMITH, N. M. (I956): Tropical Sprue. A Study of Seven Cases and their Response to
Combined Chemotherapy, Quart. 7. Med., 25, 333.and HAWKINS, C. F. (I96I): Unpublished data.PEENEY, A. L. P., and THOMPSON, M. D. (1949): Unpublished data.
GELLMAN, D. D. (1956): Diverticulosis of the Small Intestine with Steatorrhcea and Megaloblastic Aniemia, Lancet, ii,873.
GoIoN, R. (I946): Appreciation de la Quantite de Microbes Contenus dans les Selles, Arch. Mal. Appar. dig., 35, 462.(I949): Manuel de Coprologie Clinique, 5th Edn. Paris: Masson.and GOIFFON, B. (I954): Signes Coprologiques des Diarrhees par Antibiotiques, Presse mid., 23, 488.
GOLDSTEIN, R., WIRTS, C. W., and KRAMER, S. (I96I): The Relation of Afferent Limb Stasis and Bacterial Flora to theProduction of Post-gastrectomy Steatorrhcea, Gastroenterology, 40, 47.
copyright. on A
pril 9, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.259 on 1 M
ay 1961. Dow
nloaded from

May I96I FRENCH: Problems Raised by the Treatment of Steatorrhcea with Antibacterial Drugs 267
GRAY, C. H. and NICHOLSON. D. C. (1958): The Chemistry of the Bile Pigments. The Structures of Stercobilin andd-Urobilin, J7. chem. SOc., 3, 3085.
HA$X, A. J. C. and VAN BEEK, C. (1955): Behandeling van de Ziekte van Whipple met Chemotherapie en Antibiotica,Ned. T. Geneesk. 99, 2770.
HALSTED, J. A., SWENDSEID, M. E., LEwIs P. M., and GASSTER, M., (I956): Mechanisms Involved in the Development ofVitamin B12 Deficiency, Gastroenterology, 30, 2I.
HENDRY, E. B. (I960): The Chemical Diagnosis of Steatorrhoea, Brit. med. Y., ii, 975.HERTER, C. A. (I908): On Infantilism from Chronic Intestinal Infection. New York: Macmillan.HORNING, E. C. and DALGLIESH, C. E. (I958): The Association of Skatole-forming Bacteria in the Small Intestine with
Malabsorption Syndrome and Certain Aneemias, Biochem. J., 70, 13P.JACOBSON, E. D., CHODOS, R. B., and FALOON, W. W. (I960): An Experimental Malabsorption Syndrome Induced by
Neomycin, Amer. Jt. Med., 28, 524.JENKIN, C. R. and ROWLEY, D. (1959): Possible Factors in the Pathogenesis of Cholera, Brit. J. exp. Path., 40, 474.KAY, A. W. (I960): Surgical Aspects of the Malabsorption Syndrome, Brit. med. 7., i, I291.KENDALL, A. I., DAY, A. A., WALKER, A. W., and HANER, R. C. (1927): The Bacteriology and Chemistry of Adult
Duodenal Contents, J. infect. Dis., 40, 677.KING, M. J. and JOSKE, R. A. (I960): Acute Enteritis with Temporary Intestinal Malabsorption, Brit. med. J., i, 1324.KINSELLA, V. J., HENNESSY, W. B., and GEORGE, E. P. (I960): A Study on Post-gastrectomy Malabsorption, Gut, I, 372.KIRSNER, J. B., LEVIN, E., and PALMER, W. (1952): Use of Antibiotics in Gastrointestinal Diseases, A.M.A. Arch.
intern. Med., 90, 677.KOHLBRUGGE, J. H. F. (I90I): Een Bijdrage tot de Aetiologie der Indische Spruw (Psilosis), Ned. T. Geneesk., 37 ii, 88i.KOOREMAN, P. J. (1957): De Ziekte van Whipple (discussion), Ned. T. Geneesk., 101, 2254.KRAINICK, H. G. (1958): Weitere Untersuchungen uiber den Schadlichen Weizenmehleffekt bei der Coliakie I, Helv.
pa-diat. Acta, 13, 432.MACKIE, F. P., GoRE, S. N., and WADIA, J. H. (1928): The Bacteriology of Sprue, IndianY. med. Res., z6, 95.MANSON-BAHR, P. (1953): The Causation of Tropical Sprue, Lancet, ii, 389.MERLISs, R. H. and HOFFMAN, A. (I95 ): Steatorrhoea following the Use of Antibiotics, New Engl. J7. Med., 245, 328.MILANES, F., CURBELO, A., RODRIGUEZ, A., KOURI, P., and SPIES, T. D. (1946): A Note on Bacteriological and Parasitic
Studies of the Intestinal Contents of Patients with Sprue, Gastroenterology, 7, 306.MOLLIN, D. L., BOOTH, C. C., and BAKER, S. J. (1957): The Absorption of Vitamin B12 in Control Subjects in Addisonian
Pemicious Anamia and in the Malabsorption Syndrome, Brit. J. Hatmat., 3, 412.NADEL, H. and GARDNER, F. H. (1956): Bacteriological Assay of Small Bowel Secretion in Tropical Sprue, Amer. 7.
trop. Med., 5, 686.NAISH, J. and CAPPER, W. M. (I953): Intestinal cul-de-sac Phenomena in Man Lancet, ii, 597.OLLEROS, A. R. (1942): Gastric Similarities and Differences between Tropical Sprue and Pemicious Anlemia, Amer.
J. dig. Dis., 9, 26I.PAULLEY, J. W. (1952): A Case of Whipple's Disease (Intestinal Lipodystrophy), Gastroenterology, 22, 128.RENNER, VON DIETER (1952): Erfolgreiche Aureomycin Behandlung bei Einheimischer Sprue, Med. Klin., 47, 1659.RIMINGTON, C. (1946): Indigoid Pigments derived from a Pathological Urine, Biochem, J., 40, 669.SBOROV, V. M., JAY, A. R., and WATSON, C. J. (I95*): The Effect of Aureomycin on Urobilinogen Formation and the
Fecal Flora, J. Lab. clin. Med., 37, 52.SCHAFFNER, F. and SCHERBEL, A. L. (1955): Whipple's Disease, Gastroenterology 29, I09.SCHNEIDER, R., BISHOP, H., and SHAW, B. (I960): The Inhibition of the Peristaltic Reflex by Substances from Protein
Sources, Brit. J. Pharmacol., X5, 219.SCUDAMORE, H. H., HAGEDORN, A. B., WOLLAEGER, E. E., and Owen, C. A. (1958): Diverticulosis of the Small Intestine
and Macrocytic Anamia: Absorption of Radioactive B12, Gastroenterolkgy 34, 66.SPENCER, R. P. (I960): The Intestinal Tract. Springfield, Illinois: Charles Thomas.VANOTTI, A. (1954): Porphyrins. London: Hilger and Watts.WATKINSON, G., FEATHER, D. B., MARSON, F. G. W., and DOSSETT, J. A. (1959): Massive Jejunal Diverticulosis with
Steatorrhcea and Megaloblastic Anaemia Improved by Excision of Diverticula, Brit. med. .7. ii, 58.WEIJERS, A. A. and KAMER, J. H. VAN DE (I960): Celiac Disease and Wheat Sensitivity, Pediatrics, 25, 127.WIRTS, C. W. and GOLDSTEIN, F. (1960): Effect of Antibiotic Therapy in a Probable Case of Non-tropi"al Sprue.
Gastroenterolry, 39, 628.
copyright. on A
pril 9, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.259 on 1 M
ay 1961. Dow
nloaded from