Embed Size (px)
Citation preview

British Heart Journal, I975, 37, I27-135.
Problems concerning assessment ofanatomical site of accessory pathway inWolff-Parkinson-White syndrome
R. A. J. Spurrell,' D. M. Krikler,2 and E. SowtonFrom The Cardiac Department, Guy's Hospital, London
Two patients with type B WPW syndrome and reciprocal tachycardias have been studied using intracardiacelectrograms andprogrammed electrical stimulation of the heart. One patient, who had a right-sided accessorypathway giving the surface electrocardiographic appearances of type B WPW syndrome, was shown to havean additional left-sided accessory pathway as occurs in type A WPW syndrome. This concealed left-sidedatrioventricular connexion formed the retrograde pathway during reciprocal tachycardia. In the secondpatient the appearances of type B WPW syndrome were shown to be caused by an accessory pathway be-tween the atrial septum and the right side of the interventricular septum rather than an accessory pathway inthe right atrioventricular groove. The significance of thesefindings when considering surgical interruption ofanaccessory atrioventricular conduction pathway is discussed.
In the Wolff-Parkinson-White (WPW) syndromethe surface electrocardiogram shows a short PRinterval and a wide bizarre QRS complex and thereis a tendency to paroxysmal tachycardia (Wolff,Parkinson, and White, I930); the onset of QRS isdeformed by a delta wave (Segers, Lequime, andDenolin, I944). It is now thought that this abnormalcomplex is caused by fusion between activation ofthe ventricles via the normal atrioventricular nodeHis pathway and an accessory atrioventricular path-way (Wolferth and Wood, 1933; Butterworth andPoindexter, I942). The WPW syndrome has beendivided into types A and B depending upon theQRS configuration in the right praecordial leads(Rosenbaum et al., I945): in type A, the QRS com-plex is dominantly positive in Vi and V2, whereasin type B it is dominantly negative. Histologicalexamination of hearts from patients with the WPWsyndrome has shown that in many instances thelocation of the accessory pathway can be deducedfrom the surface electrocardiogram, the accessorypathway classically being in the right atrioventric-ular groove in type B (Lev, Gibson, and Miller,
Received 5 July I974.'Present address: Cardiac Department St. Batholomew'sHospital, London ECi.2Present address: Cardiovascular Division, Royal Post-graduate Medical School, Hammersmith Hospital, LondonW12.
I955) and in the left atrioventricular groove in typeA (Mann et al., I973; Ohnell, I944).We now describe two patients with the surface
electrocardiographic appearances of type B WPWsyndrome: an electrophysiological study revealedthat one patient had an additional accessory path-way on the left side of the heart (as well as one onthe right side) and that in the other case the acces-sory pathway was not in the right atrioventriculargroove but that it connected the right atrium directlywith the right side of the interventricular septum.
Patients and methodsThe clinical details of the two patients studied are shownin the Table. Both patients had long-standing historiesof paroxysmal supraventricular tachycardia. Informedconsent was obtained from both patients and an electro-physiological study was then carried out in the post-absorptive, non-sedated state.Three bipolar catheter electrodes with an inter-
electrode distance of i cm were introduced percu-taneously via one or both femoral veins. One catheterwas positioned high in the right atrium to record a highright atrial electrogram; one catheter was positionedacross the tricuspid valve and a His bundle electrogramrecorded using the technique described by Scherlaget al. (I969). A third catheter was used for atrial or ven-tricular pacing and for introducing atrial or ventricularpremature beats. In Case I a fourth bipolar electroedcatheter was passed to the left atrium via a patentforamen ovale and positioned in the region of the left
I28 Spurrell, Krikler, and Sowton
TABLE
Case Age Sex Electro- Clinical detailsNo. (yr) cardiogram
I 26 M Type B WPW Recurrent bouts ofsupraventriculartachycardia; mitralstenosis and aorticincompetence
2 28 F Type B WPW Recurrent bouts ofsupraventriculartachycardia
superior pulmonary vein to record a high left atrialelectrogram.
All recordings were made on an eight channel ElemaMingograf 8i. The His bundle electrogram was re-corded with the frequency response set at 45-500cycles/s. Leads I, III, Vi, and V6 of the surface electro-cardiogram were recorded simultaneously with the intra-cardiac recordings. All recordings were taken at a paperspeed of ioo mm/s.A Devices' 4270 stimulator was used for atrial and
ventricular pacing. The heart was driven at a constantfrequency, thus preventing any changes in excitabilityor refractoriness caused by irregularities in rhythm.Single or double atrial or ventricular premature beatswere delivered after every eighth beat of the basic drivenrhythm. A variable delay circuit triggered by either theR wave of the surface electrocardiogram, or an atrialelectrogram was used so that the premature beats couldbe delivered in the cardiac cycle at a preset delay fol-lowing the preceding driven beat. In each patient themode of initiation and termination of tachycardia wasstudied as was the effect of premature beats on the basicrhythm during tachycardia. Pacing of the His bundlewas carried out in both patients using the catheter elec-trode that recorded the His bundle electrogram.
Results
Case i
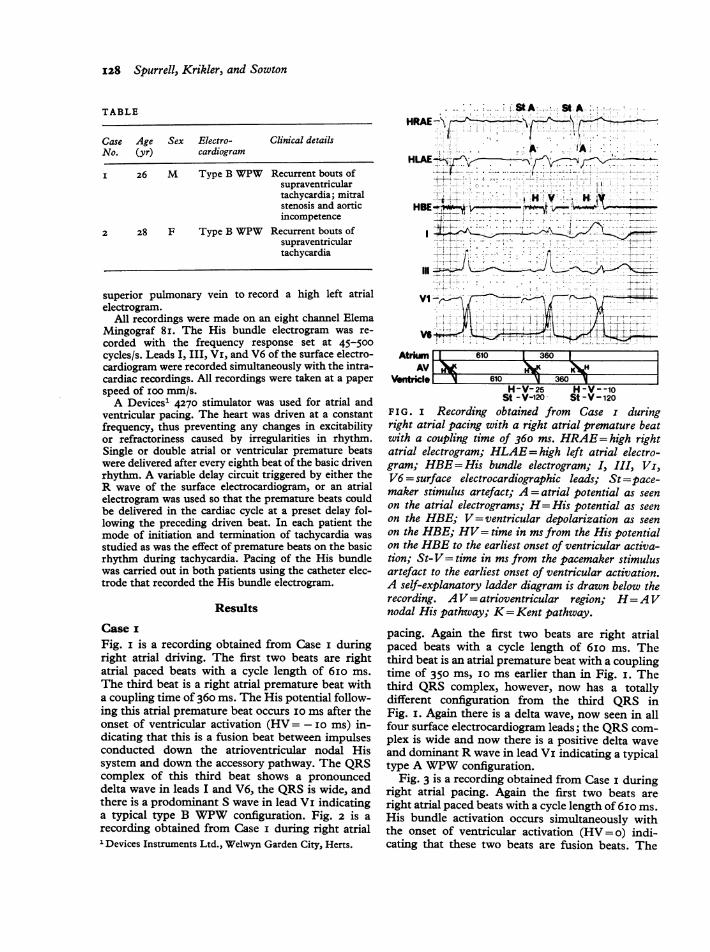
Fig. i is a recording obtained from Case i duringright atrial driving. The first two beats are rightatrial paced beats with a cycle length of 6ioims.The third beat is a right atrial premature beat witha coupling time of 360 ms. The His potential follow-ing this atrial premature beat occurs i0 ms after theonset of ventricular activation (HV= -i0 ims) in-dicating that this is a fusion beat between impulsesconducted down the atrioventricular nodal Hissystem and down the accessory pathway. The QRScomplex of this third beat shows a pronounceddelta wave in leads I and V6, the QRS is wide, andthere is a prodominant S wave in lead Vi indicatinga typical type B WPW configuration. Fig. 2 is arecording obtained from Case i during right atrial'Devices Instruments Ltd., Welwyn Garden City, Herts.
HRAE-\7-
HLAE-,-a A*t~ ~+ :
_ - i >
,,,. L-='-VI
Vs -4- z -(i-Vl~~~~VAtrim 610 1 360 1I
AVI) )~XK *LHVentricle 610 360 l
H-V-25 H-V--loSt - V-120 St -V-120
FIG. i Recording obtained from Case i duringright atrial pacing with a right atrial premature beatwith a coupling time of 360 ms. HRAE= high rightatrial electrogram; HLAE= high left atrial electro-gram; HBE= His bundle electrogram; I, III, Vi,V6 = surface electrocardiographic leads; St =pace-maker stimulus artefact; A = atrial potential as seenon the atrial electrograms; H= His potential as seenon the HBE; V= ventricular depolarization as seenon the HBE; HV= time in ms from the His potentialon the HBE to the earliest onset of ventricular activa-tion; St-V= time in ms from the pacemaker stimulusartefact to the earliest onset of ventricular activation.A self-explanatory ladder diagram is drawn below therecording. AV= atrioventricular region; H=AVnodal His pathway; K=Kent pathway.
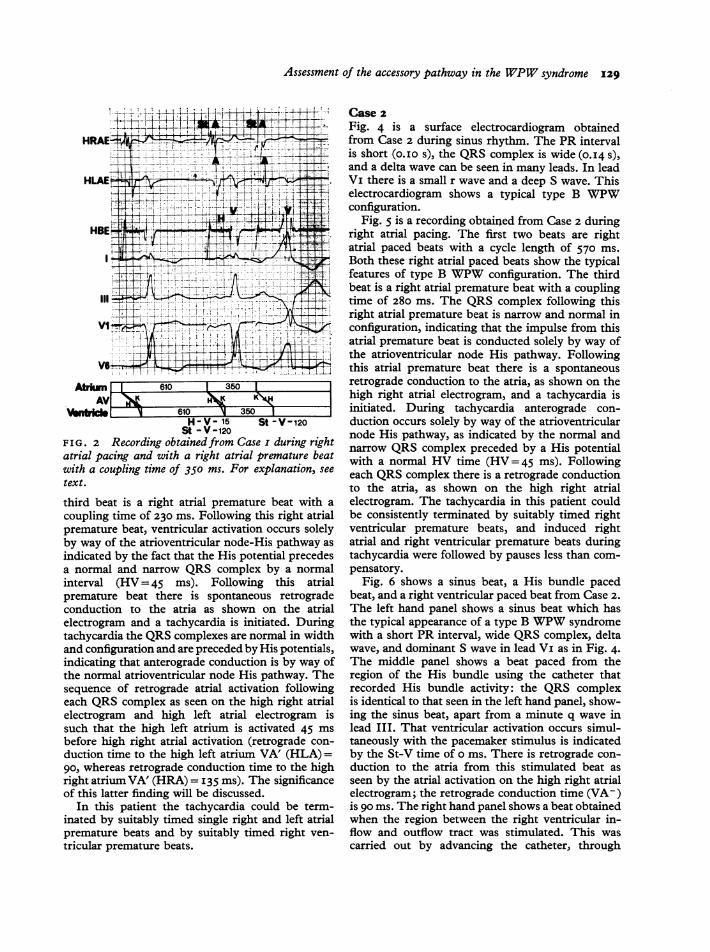
pacing. Again the first two beats are right atrialpaced beats with a cycle length of 6io ms. Thethird beat is an atrial premature beat with a couplingtime of 350 ms, i0 ms earlier than in Fig. I. Thethird QRS complex, however, now has a totallydifferent configuration from the third QRS inFig. I. Again there is a delta wave, now seen in allfour surface electrocardiogram leads; the QRS com-plex is wide and now there is a positive delta waveand dominant R wave in lead Vi indicating a typicaltype A WPW configuration.
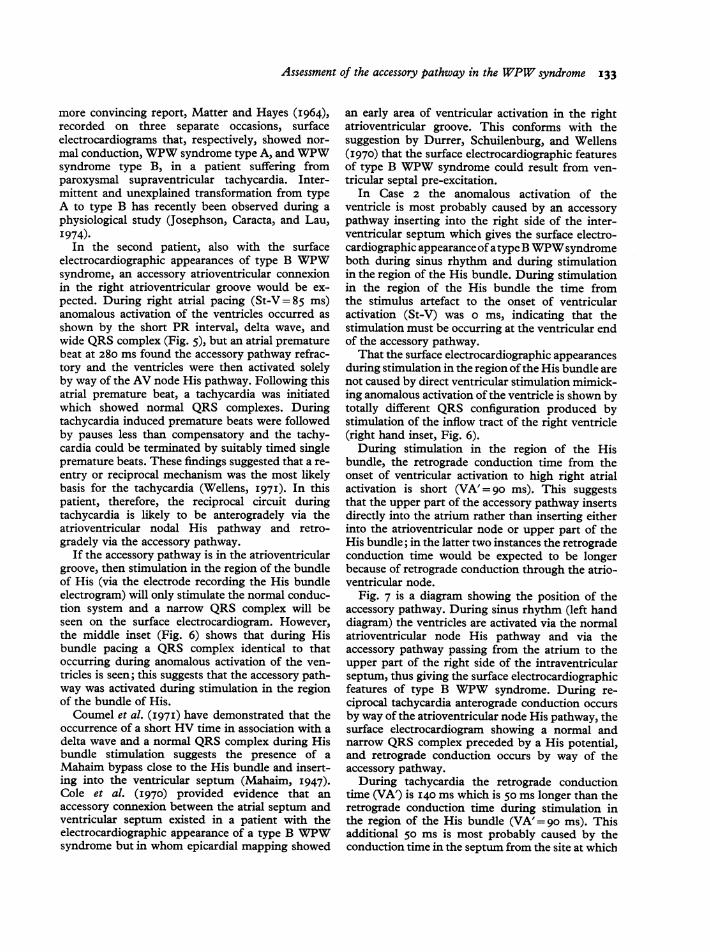
Fig. 3 is a recording obtained from Case i duringright atrial pacing. Again the first two beats areright atrial paced beats with a cycle length of 6io ms.His bundle activation occurs simultaneously withthe onset of ventricular activation (HV = o) indi-cating that these two beats are fusion beats. The
Assessment of the accessory pathway in the WPW syndrome 129
itf d , M -if N
...T- -.1i.- - .-r ---L
I.W- -01
.-I jf -4--
VI
V1r_4
4V4
Atrk 610 1 350 1
H-V- 15 St-St -V-120
F I G. 2 Recording obtained from Case i c
atrial pacing and with a right atrial prerwith a coupling time of 350 ms. For explktext.
third beat is a right atrial premature bcoupling time of 230 ms. Following thispremature beat, ventricular activation oc
by way of the atrioventricular node-Hisindicated by the fact that the His potentia normal and narrow QRS complex bzinterval (HV = 45 ms). Followingpremature beat there is spontaneousconduction to the atria as shown on
electrogram and a tachycardia is initiatetachycardia the QRS complexes are norm
and configuration and are preceded by Hisindicating that anterograde conduction isthe normal atrioventricular node His patsequence of retrograde atrial activationeach QRS complex as seen on the highelectrogram and high left atrial electsuch that the high left atrium is activabefore high right atrial activation (retroduction time to the high left atrium VAgo, whereas retrograde conduction time*right atrium VA' (HRA) = I35 ms). The sof this latter finding will be discussed.
In this patient the tachycardia coulcinated by suitably timed single right an(
premature beats and by suitably timedtricular premature beats.
Case 2Fig. 4 is a surface electrocardiogram obtainedfrom Case 2 during sinus rhythm. The PR intervalis short (o.io s), the QRS complex is wide (0.14 s),and a delta wave can be seen in many leads. In leadVi there is a small r wave and a deep S wave. This
7 electrocardiogram shows a typical type B WPW-V= X + Lconfiguration.
A V.--t;N t Fig. 5 is a recording obtained from Case 2 during;,C-L- .right atrial pacing. The first two beats are right
atrial paced beats with a cycle length of 570 ms.Both these right atrial paced beats show the typicalfeatures of type B WPW configuration. The thirdbeat is a right atrial premature beat with a couplingtime of 280 ms. The QRS complex following this
X+- right atrial premature beat is narrow and normal in- r configuration, indicating that the impulse from this
i44j2i'_ ,atrial premature beat is conducted solely by way of
ZziL~~< the atrioventricular node His pathway. Following4,FX- this atrial premature beat there is a spontaneousretrograde conduction to the atria, as shown on thehigh right atrial electrogram, and a tachycardia isinitiated. During tachycardia anterograde con-
V-120 duction occurs solely by way of the atrioventricularnode His pathway, as indicated by the normal and
,uring right narrow QRS complex preceded by a His potentialanatue beat with a normal HV time (HV=45 ms). Followingination, see each QRS complex there is a retrograde conduction
to the atria, as shown on the high right atrial)eat with a electrogram. The tachycardia in this patient couldright atrial be consistently terminated by suitably timed rightcurs solely ventricular premature beats, and induced rightpathway as atrial and right ventricular premature beats duringal precedes tachycardia were followed by pauses less than com-y a normal pensatory.this atrial Fig. 6 shows a sinus beat, a His bundle pacedretrograde beat, and a right ventricular paced beat from Case 2.the atrial The left hand panel shows a sinus beat which has
ed. During the typical appearance of a type B WPW syndromeLal in width with a short PR interval, wide QRS complex, deltapotentials, wave, and dominant S wave in lead Vi as in Fig. 4.
3 by way of The middle panel shows a beat paced from thehway. The region of the His bundle using the catheter that1 following recorded His bundle activity: the QRS complexright atrial is identical to that seen in the left hand panel, show-trogram is ing the sinus beat, apart from a minute q wave inLted 45 ms lead III. That ventricular activation occurs simul-ograde con- taneously with the pacemaker stimulus is indicated.' (HLA) = by the St-V time of o ms. There is retrograde con-to the high duction to the atria from this stimulated beat assignificance seen by the atrial activation on the high right atrial
electrogram; the retrograde conduction time (VA-)I be term- is go ms. The right hand panel shows a beat obtainedd left atrial when the region between the right ventricular in-right ven- flow and outflow tract was stimulated. This was
carried out by advancing the catheter, through
4-.j '-,-i --- ----4--4,, C t--l I 1 .-.: -1.1 I - i4-4--;-.-, I'l "'
0-14 -1
HLAE .-.11A?-
4.4., LHBE4,11m-.A'm T-
HRAEi- I'::
. !..4
i^ I-'4in-;
AV610 1 350 1

130 Spurrell, Krikler, and Sowton
HRAEiL
*~~~ HV 1{', ''HLAE----
HBE- v 9
4- ~ ~
VI
Antridm 610 23 650 43 40 1
H-V-o H-V-45 V- (HLA)-oFIG. 3 Recording obtained from Case i showing the onset of a supraventricular tachycardiafollowing an atrial premnature beat with a coupling tiMe Of 230 ins. A' =retrograde atrialpotentials as seen on the atrial electrograms; St-H= time in milliseconds from the pacemaherstimulus artefact to the His potential on the HBE; VA' (HRA) = retrograde conduction time inms from the onset of ventricular activation to the retrograde atrial potential on the HRAE;VA' (HLA) = retrograde conduction time in ms from the onset of ventricular activation to theretrograde atrial potential on the high left atrial electrogram.
AVR AVL AVF .iI
VIK V31 V5tb
V2>+ V4, e4 V6.L
FIG. 4 Surface electrocardiogram obtained duringsinus rhythm from Case 2.
which the region of the His bundle had been stimu-lated, I to 2 cm into the right ventricle. The QRScomplex is now seen to be quite different from thatof the sinus beat and from the QRS complex re-sulting from pacing in the region of the His bundle.The QRS complex in the right hand inset nowshows a left bundle-branch block pattem with rightaxis deviation, as may occur with pacing in thisregion. Following this ventricular paced beat, thereis retrograde conduction to the atria as indicated byretrograde atrial activation on the high right atrialelectrogram. The retrograde conduction time isconsiderably longer than when pacing from theregion of the His bundle was undertaken (VA'=I70 ms as opposed to VA'=0go ms).
DiscussionPatients with intractable tachycardias associatedwith the WPW syndrome can now be treated bysurgical section of the accessory pathway. Duringepicardial mapping studies in a patient with type BWPW syndrome, Cobb et al. (I968) found an areaof ventricular pre-excitation in the right atrioven-tricular groove; when this area was divided

Assessment of the accessory pathway in the WPW syndrome 131
St-v- &-Vs= v-k-rnF I G . 5 Recording obtainedfrom Case 2 showing the initiation ofa supraventricular tachycardiaby a right atrial premature beat with a coupling time of 280 ms. VA' = retrograde conductiontime in ms from the earliest onset of ventricular activation to the retrograde atrial potential onthe high right atrial electrogram.
B.G. Si
HRAE 4HHRAE- HRAE
HB76 ¶yf HETWF HBE~Iw
III~ ~ ~ I
SinusR?ithm Hilpjjndlo V ircuar
st-v=o V-K 170FIG. 6 Recordings obtained from Case 2 showing asinus beat in the left hand panel, a His bundle pacedbeat in the centre panel, and a beat obtained fromstimulation of the right ventricular inflow tract in theright hand panel.
Sinus Rhythm TachycardiaFIG. 7 Diagram of the normal conduction systemand the accessory atrioventricular connexion in Case 2showing the conduction sequence (interrupted line)during sinus rhythm in the left hand panel and duringtachycardia in the right hand panel. SI= sinusimpulse.
1 570 1 28D 1 495 1 m 380 300
r \-
1 570 1 575 f 340 I' 390 1 300
lwi-AV
Vlwddd*

132 Spurrell, Krikler, and Sowton
surgically the pre-excitation and episodes of tachy-cardia were abolished. Since then other workershave had similar success in patients with type BWPW. More recently, Wallace et al. (I974) havereported two patients with type A WPW syndromein whom epicardial mapping studies showed an areaof ventricular pre-excitation posteriorly in the leftatrioventricular groove; appropriate atrial incisionswere made, and the pre-excitation and episodes oftachycardia were abolished.
This form of therapy depends upon the accurateassessment of the site and function of the accessorypathway. In the first patient described in this paperthe resting surface electrocardiogram showed a typeB WPW configuration and classically the accessorypathway would be expected to occur in the rightatrioventricular groove. It would have been reason-able to expect that the circus movement tachycardiaoccurring in this patient involved retrograde con-duction by way of this right-sided accessory path-way. Had epicardial mapping been carried out inthis patient, an early area of ventricular activationmay well have been found in the right atrioven-tricular groove and surgery carried out in thisregion. Initially the electrophysiological studydemonstrated that during sinus rhythm and withatrial premature beats down to a coupling time of360 ms the ventricles were activated via a right-sided accessory pathway giving the appearance of atype B WPW syndrome. However, with atrial pre-mature beats occurring at coupling times of 350 msand less (Fig. 2), this right-sided accessory pathwaybecame refractory and the ventricles were thenactivated via a left-sided accessory pathway, nowwith the surface electrocardiographic appearancesof type A WPW syndrome. This latter configura-tion of type A WPW syndrome was never seen onresting electrocardiograms. An unusual feature,however, concerns the stimulus to delta interval(St-V) of the beats showing a type B WPW con-figuration and those showing a type A configura-tion. In both instances this interval is the same(St-V= 120 ms). In the presence of a left-sidedaccessory pathway it would be expected that theconduction time from a right atrial stimulus to theatrial insertion of a left-sided accessory pathwaywould be longer than the conduction time to a right-sided accessory pathway. The lack of prolongationof the St-V time in this patient when left-sidedaccessory pathway activation occurs may be causedby the atrial end of both pathways being insertedrelatively close together, possibly posteriorly, oneinto the right atrium and the other into the left.At an atrial premature beat coupling time of 230 msthis left-sided accessory pathway also became re-fractory and the ventricles were activated solely by
way of the atrioventricular node His pathway, and are-entry tachycardia was initiated. During tachy-cardia it is conceivable that retrograde conductionwould occur by way of either the left- or right-sided accessory pathway, or the re-entry circuitcould be intra-atrioventricular nodal with neitheraccessory pathway involved. However, the retro-grade activation sequence of the atria during tachy-cardia was such that the high left atrium was acti-vated 45 ms in advance of the high right atrium (seeFig. 3), suggesting that the retrograde pathway in-serted into the left atrium. In addition, this patienthad mitral valve disease with an enlarged leftatrium. Under these circumstances, one wouldexpect retrograde atrial activation in the region ofthe left superior pulmonary vein (the site of theleft atrial recording electrode) to be delayed. Inthis patient, the high left atrium was still activatedin advance of the right and in the presence of anormal left atrial size the high left atrial activationwould occur even earlier still, thereby emphasizingfurther the abnormal retrograde atrial activationsequence with high left atrial activation occurringbefore the right. A similar retrograde atrial activa-tion sequence during tachycardia was found byWallace et al. (I974) in two patients with type AWPW syndrome. It has been found in our labora-tory that during re-entry tachycardia in type BWPW syndrome retrograde right atrial activationinvariably precedes left atrial activation and inatrioventricular nodal re-entry tachycardia activa-tion of the high right and high left atria occurs eithersimultaneously or the right atrium is activated inadvance of the left. These findings accord well withthose of Massumi et al. (I969) who found thatduring right ventricular pacing in patients withnormal conduction systems retrograde activation ofthe atria by way of the atrioventricular node Hispathway led to simultaneous right and left atrialactivation, or right atrial activation occurred up to30 ms before left atrial activation. It appears, there-fore, that Case I has two accessory pathways, onegiving the appearance of type B WPW syndrome onthe resting electrocardiogram; the other whichprobably lies in the left atrioventricular groove isonly apparent following early right atrial pre-mature beats. However, it is this concealed left-sided accessory pathway which provides the retro-grade pathway for the reciprocal circuit duringtachycardia.
Mulptiple anomalous atrioventricular connexionshave been identified in the rabbit (Sano, Suzuki,and Tsuchihasi, I970) and squirrel monkey (Boin-eau et al., I973). Appearances may be seen in mansuggestive, at different times, of WPW syndrometypes A and B (Ramachandran, 1972); but in a
Assessment of the accessory pathway in the WPW syndrome 133
more convincing report, Matter and Hayes (I964),recorded on three separate occasions, surfaceelectrocardiograms that, respectively, showed nor-mal conduction, WPW syndrome type A, and WPWsyndrome type B, in a patient suffering fromparoxysmal supraventricular tachycardia. Inter-mittent and unexplained transformation from typeA to type B has recently been observed during aphysiological study (Josephson, Caracta, and Lau,I974).
In the second patient, also with the surfaceelectrocardiographic appearances of type B WPWsyndrome, an accessory atrioventricular connexionin the right atrioventricular groove would be ex-pected. During right atrial pacing (St-V=85 ms)anomalous activation of the ventricles occurred asshown by the short PR interval, delta wave, andwide QRS complex (Fig. 5), but an atrial prematurebeat at 280 ms found the accessory pathway refrac-tory and the ventricles were then activated solelyby way of the AV node His pathway. Following thisatrial premature beat, a tachycardia was initiatedwhich showed normal QRS complexes. Duringtachycardia induced premature beats were followedby pauses less than compensatory and the tachy-cardia could be terminated by suitably timed singlepremature beats. These findings suggested that a re-entry or reciprocal mechanism was the most likelybasis for the tachycardia (Wellens, I971). In thispatient, therefore, the reciprocal circuit duringtachycardia is likely to be anterogradely via theatrioventricular nodal His pathway and retro-gradely via the accessory pathway.
If the accessory pathway is in the atrioventriculargroove, then stimulation in the region of the bundleof His (via the electrode recording the His bundleelectrogram) will only stimulate the normal conduc-tion system and a narrow QRS complex will beseen on the surface electrocardiogram. However,the middle inset (Fig. 6) shows that during Hisbundle pacing a QRS complex identical to thatoccurring during anomalous activation of the ven-tricles is seen; this suggests that the accessory path-way was activated during stimulation in the regionof the bundle of His.Coumel et al. (I97I) have demonstrated that the
occurrence of a short HV time in association with adelta wave and a normal QRS complex during Hisbundle stimulation suggests the presence of aMahaim bypass close to the His bundle and insert-ing into the ventricular septum (Mahaim, I947).Cole et al. (I970) provided evidence that anaccessory connexion between the atrial septum andventricular septum existed in a patient with theelectrocardiographic appearance of a type B WPWsyndrome but in whom epicardial mapping showed
an early area of ventricular activation in the rightatrioventricular groove. This conforms with thesuggestion by Durrer, Schuilenburg, and Wellens(I970) that the surface electrocardiographic featuresof type B WPW syndrome could result from ven-tricular septal pre-excitation.
In Case 2 the anomalous activation of theventricle is most probably caused by an accessorypathway inserting into the right side of the inter-ventricular septum which gives the surface electro-cardiographic appearanceofatypeB WPWsyndromeboth during sinus rhythm and during stimulationin the region of the His bundle. During stimulationin the region of the His bundle the time fromthe stimulus artefact to the onset of ventricularactivation (St-V) was o ms, indicating that thestimulation must be occurring at the ventricular endof the accessory pathway.That the surface electrocardiographic appearances
during stimulation in the region ofthe His bundle arenot caused by direct ventricular stimulation mimick-ing anomalous activation of the ventricle is shown bytotally different QRS configuration produced bystimulation of the inflow tract of the right ventricle(right hand inset, Fig. 6).During stimulation in the region of the His
bundle, the retrograde conduction time from theonset of ventricular activation to high right atrialactivation is short (VA'=9go ms). This suggeststhat the upper part of the accessory pathway insertsdirectly into the atrium rather than inserting eitherinto the atrioventricular node or upper part of theHis bundle; in the latter two instances the retrogradeconduction time would be expected to be longerbecause of retrograde conduction through the atrio-ventricular node.
Fig. 7 is a diagram showing the position of theaccessory pathway. During sinus rhythm (left handdiagram) the ventricles are activated via the normalatrioventricular node His pathway and via theaccessory pathway passing from the atrium to theupper part of the right side of the intraventricularseptum, thus giving the surface electrocardiographicfeatures of type B WPW syndrome. During re-ciprocal tachycardia anterograde conduction occursby way of the atrioventricular node His pathway, thesurface electrocardiogram showing a normal andnarrow QRS complex preceded by a His potential,and retrograde conduction occurs by way of theaccessory pathway.During tachycardia the retrograde conduction
time (VA') is 140 ms which is 50 ms longer than theretrograde conduction time during stimulation inthe region of the His bundle (VA'=go ms). Thisadditional 50 ms is most probably caused by theconduction time in the septum from the site at which

134 Spurrell, Krikler, and Sowton
the activation impulse leaves the right bundle-branch to the ventricular insertion of the accessorypathway (see Fig. 7).
Atrioseptal accessory pathways were described byPaladino in I914 and more recently by Schumann,Jansen, and Anschutz (1970). It appears that anatrioseptal accessory pathway of the type postulatedin this patient may be similar to that found by Coleet al. (I970), as described earlier in the discussion.The findings in these two patients, therefore,
indicate the importance of an adequate electro-physiological study in patients with the WPW syn-drome who are under consideration for surgicaldivision of the accessory pathway. In the firstpatient an accessory pathway in the right atrioven-tricular groove may have been found and dividedat surgery, but an attempt to divide the additionalconcealed left-sided accessory pathway, the oneresponsible for the reciprocal tachycardia, would nothave been made unless it had been demonstratedbefore operation; thus attacks of tachycardia mayhave persisted. In the second patient the accessorypathway was not in the classical site of a Kent path-way in the atrioventricular groove but was adjacentto the normal specialized conduction system insert-ing into the upper part of the ventricular septum.If this situation had not been assessed adequatelybefore operation then an unsuccessful attempt todivide an accessory pathway in the right atrioven-tricular groove may have been made, especially ifepicardial mapping had shown an early area ofventricular excitation in the right atrioventriculargroove, as was the case in the patient described byCole et al. (1970), and discussed earlier. In thispatient, a possible surgical approach would be toattempt to divide the accessory pathway betweenthe atrium and the upper part of the right side ofthe interventricular septum, but such an approachwould be extremely difficult without causing addi-tional damage to the normal specialized conductionsystem in this region, thereby possibly necessitatingthe implantation of a pacemaker.As has been indicated previously (Spurrell,
Krikler, and Sowton, I973), even in the presence ofan anomalous pathway, paroxysmal tachycardiamay depend exclusively on pathways within theatrioventricular node. Before surgery is contem-plated for the treatment of refractory tachycardia,it is essential not only to identify such pathways asmay be present, but also to demonstrate that theyare implicated in the tachycardia circuit. Unless thisis done, what appears to be a justifiable surgicalprocedure may fail, not because of poor surgicaltechnique, but because the mechanism of the tachy-cardia has not been completely defined by rigorouselectrophysiological study.
ReferencesBoineau, J. P., Moore, E. N., Spear, J. F., and Sealy, W. C.
(I973). Basis of static and dynamic electrocardiographicvariations in Wolff-Parkinson-White syndrome. AmericanJournal of Cardiology, 32, 32.
Butterworth, J. S., and Poindexter, C. A. (I942). Short PRinterval associated with a prolonged QRS complex.Archives of Internal Medicine, 69, 437.
Cobb, F. R., Blumenschein, S. D., Sealy, W. C., Boineau,J. P., Wagner, G. S., and Wallace, A. G. (I968). Success-ful surgical interruption of the bundle of Kent in a patientwith Wolff-Parkinson-White syndrome. Circulation, 38,Ioi8.
Cole, J. S., Wills, R. E., Winterscheid, L. C., Reichenbach,D. D., and Blackmon, J. R. (I970). The Wolff-Parkinson-White syndrome; problems in evaluation and surgicaltherapy. Circulation, 42, III.
Coumel, P., Waynberger, M., Slama, R., and Bouvrain, Y.(197I). Interet de l'enregistrement des potentiels Hisiensau coeurs du syndrome de Wolff-Parkinson-White apropos de six observations. Acta Cardiologica, 26, i88.
Durrer, D., Schuilenburg, R. M., and Wellens, H. J. J.(I970). Pre-excitation revisited. American Journal ofCardiology, 25, 690.
Josephson, M. E., Caracta, A. R., and Lau, S. H. (I974).Alternating type A and type B Wolff-Parkinson-Whitesyndrome. American Heart,Journal, 87, 363.
Lev, M., Gibson, S., and Miller, R. A. (I955). Ebsteinsdisease with Wolff-Parkinson-White syndrome. AmericanHeart Journal, 49, 724.
Mahaim, I. (1947). Kent's fibers and the AV paraspecificconduction through the upper connections of the bundleof His-Tawara. American Heart journal, 33, 65I.
Mann, R. B., Fisher, R. S., Scherlis, S., and Hutchins, G. M.(I973). Accessory left atrioventricular connection in typeA Wolff-Parkinson-White syndrome. Johns HopkinsMedical,Journal, 132, 242.
Massumi, R. A., Sarin, R. K., Tawakkol, A. A., Rios, J. C.,and Jackson, H. (I969). Time sequence of right and leftatrial depolarization as a guide to the origin of the P waves.American Journal of Cardiology, 24, 28.
Matter, B. J., and Hayes, W. L. (I964). Wolff-Parkinson-White syndrome. Report of a case with both type A andtype B pre-excitation. American Journal of Cardiology, 13,284.
Ohnell, R. F. (i944). Pre-excitation. A cardiac abnormality.Acta Medica Scandinavica, Suppl. 152, 77.
Paladino, G. (I914). Ancora per una questione di priorita aproposito del fascio atrio-ventricolare del cuore. Anatom-ischer Anzeiger, 46, go.
Ramachandran, S. (I972). Wolff-Parkinson-White syndrome.Conversion of type A to type B electrocardiographicchanges. Circulation, 45, 529.
Rosenbaum, F. F., Hecht, H. H., Wilson, F. N., and Johnston,F. D. (I945). The potential variations of the thorax andthe esophagus in anomalous atrioventricular excitation(Wolff-Parkinson-White syndrome). American Heartjournal, 29, 28I.
Sano, T., Suzuki, F., and Tsuchihashi, H. (I970). Functionof potential bypass tracts for atrioventricular conduction.Circulation, 41, 413.
Scherlag, B. J., Lau, S. H., Helfant, R. H., Berkowitz, W. D.,Stein, E., and Damato, A. N. (I969). Catheter techniquefor recording His bundle activity in man. Circulation, 39,13.

Assessment of the accessory pathway in the WPW syndrome 135
Schumann, G., Jansen, H. H., and Anschutz, F. (I970).Zur pathogenese des WPW syndroms. Virchows Archivfiir pathologische Anatomie und Physiologie, 349, 48.
Segers, M., Lequime, J., and Denolin, H. (I944). L'activa-tion ventriculaire precoce de certains coeurs hyperexcit-ables. Etude de l'onde delta de l'electrocardiogramme.Cardiologia, 8, II 3.
Spurrell, R. A. J., Krikler, D., and Sowton, E. (I973). Two ormore intra AV nodal pathways in association with eithera James or Kent extranodal bypass in 3 patients withparoxysmal supraventricular tachycardia. British HeartJournal, 35, II3.
Wallace, A. G., Sealy, W. C., Gallagher, J. J., Svenson, R. H.,Strauss, H. C., and Kasell, J. (I974). Surgical correctionof anomalous left ventricular pre-excitation: Wolff-Parkinson-White (Type A). Circulation, 49, 206.
Wellens, H. J. J. (I97I). Electrical Stimulation of the Heart inthe Study and Treatment of Tachycardia. H. E. StenfertKroese NV, Leiden.
Wolferth, C. C., and Wood, F. C. (I933). The mechanism ofproduction of short PR intervals and prolonged QRScomplexes in patients with presumably undamaged hearts:hypothesis of an accessory pathway of auriculo-ventric-ular conduction (bundle of Kent). American Heartjournal, 8, 297.
Wolff, L., Parkinson, J., and White, P. D. (I930). Bundle-branch block with short PR interval in healthy youngpeople prone to paroxysmal tachycardia. American Heartj3ournal, 5, 685.
Requests for reprints to Dr. R. A. J. Spurrell, CardiacDepartment, St. Bartholomew's Hospital, London E.C.i.





























