Embed Size (px)
Citation preview

This article was downloaded by: [UQ Library]On: 05 November 2014, At: 16:11Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Journal of Social Service ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/wssr20
Problem-Solving Processes in Task-Centered Treatmentwith Adults and ChildrenAnne E. Fortune aa Assistant Professor, George Warren Brown School of Social Work, Washington University, St.Louis, MO 63130Published online: 18 Oct 2008.
To cite this article: Anne E. Fortune (1979) Problem-Solving Processes in Task-Centered Treatment with Adults and Children,Journal of Social Service Research, 2:4, 357-371, DOI: 10.1300/J079v02n04_02
To link to this article: http://dx.doi.org/10.1300/J079v02n04_02
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

PROBLEM-SOLVING PROCESSES IN TASK-CENTERED TREATMENT WITH ADULTS AND CHILDREN
Anne E. Fortune
ABSTRACT. This study concept'icolizes treatment communication as a set of joint practitioner-client, problem-solving activities. Patterns o f activities within and across six interviews o f inlensive task-centered practice are compared for twelve adult and twelve child cases. Although both adults' and children's cases implemented a general task-centered model, there were differences in proportionate utilization and temporal pat- terns of problem-solving activities which suggest that children's cases adhered t o a logical problem.solving process more closely than adults'cascs.
Many treatment models ostensibly offer prescrip- tions about how clients should be diagnosed and treated, but at- tempts t o verify the actual treatment process in social work are rela- tively rare (e.g., Hollis, 1972; Reid & Shyne, 1969). This paper fo- cuses on two issues related t o individual treatment process. The first is the extent t o which normative prescriptions for treatment process are carried out in actual practice. The second issue is the differences in application of the same treatment model with adults and children. The prescriptive model examined is task-centered casework, a form of psychosocial treatment that emphasizes time-limited, goal-orient- ed problem resolution through a series of specific problem-solving steps (Reid & Epstein, 1972).
Task-centered treatment is organized around specific problems-in- living defined by the client and around actions (tasks) t o alleviate those problems within a short period of time, usually two t o three months. Tasks are normally developed within interviews and carried out by client o r practitioner between interview sessions. The task- centered practitioner's primary responsibility within interviews is
Dr. Fortune is Assistmt Professor, George Warren Brown School o f Social Work, Washington University, St. Louis, MO 63130. This research was funded in part by SRS Grant No. 18-P-5777415-03. The author is indebted t o the project directors, William J. Reid and Laura Epstein.
sournalofSoeialScrviccR~earch.Vol.2(4). Summer 1979 OL919byTheHaworth Ress.AUrightareserved. 357
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

358 JOURNAL OF SOClAL SERVICE RESEARCH
to maintain an empathic goal orientation and t o assist the client t o develop and implement tasks likely t o resolve the identified pro- blems. These practitioner responsibilities may be conceptualized as guiding the client through problem-solving steps: (1) orientation toward problem recognition; (2) problem definition; (3) generation of alternatives; (4) decision making; and (5) verification (D'Zurilla & Goldfried, 197 1 ; Heppner, 1978).
The general problem-solving steps are operationalized in the task- centered model as a set of intervention strategies including problem specification (problem definition); generating alternatives, task plan- ning, analyzing obstacles t o task accomplishment, task agreement, practice of skills related t o tasks (generation of alternatives and decision-making), and review of task progress in relation to problem change (verification). There is some empirical evidence that clients who receive the problem-solving interventions d o better than clients who d o not receive them (Reid, 1975, 1977). However, these studies did not determine if there were temporal patterns indicating pro- blem-solving stages. In general, numerous studies have found shifts in other types of communication over therapy time (Gurman, 1973; Hollis, 1968, 1972; Lennard & Bernstein, 1960, 1969; Mullen, 1969; Proctor, 1978), but relatively few have used typologies related t o problem-solving (Cunningham, 1977; Sucato, 1978).
The patterns to be expected if the task-centered cases were follow- ing problem-solving stages were not entirely clear, since as a thera- peutic model task-centered practice emphasizes empathy and respon- siveness t o the client's immediate concerns as much as problem-solv- ing structure. However, it was anticipated that interviews would be dominated by task planning activities. Within each individual inter- view, attention was expected t o focus initially on task review (veri- fication of previous problem-resolution actions) and problem speci- fication (to assess the impact of tasks on the problem) and then shift t o planning of future tasks (generation of alternatives and decision- making). Over time in treatment, that is, across a sequence of inter- views, an increase in task planning was expected as client and practi- tioner clarified the parameters and obstacles to problem-change and were free t o devote more time t o task-actions.
The second question, whether the real-life patterns would be dif- ferent for .adults and children, stemmed from the developmental aspect of task-centered practice. The model was initially seen as appropriate only for adult individuals (Reid & Epstein, 1972), but i t
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

Anne E. Fortune 359
has been extended t o work with families and groups as well as child- ren (Reid & Epstein, 1977). Roberts and Northen (1976) note the thrust in social work t o develop generic models applicable t o various systems, but relatively few investigators have questioned if a theoreti- cal approach is implemented in the same manner with different sys- tems or populations (Lish, 1973; Barrett, Hampe, & Miller, 1978). The task-centered model now includes several adaptations for child- ren, for example, preliminary interviews t o familiarize the child t o the practitioner (Epstein, 1977). However, none of the adaptations directly affected the verbal problem-solving activities in the middle phase of treatment. Consequently, it was anticipated that the utili- zation of problem-solving activities and patterns among children would be similar t o patterns among adults.
The two questions-patterns of actual use of prescribed problem- solving activities in task-centered practice, and differences in patterns between adult and child cases-are addressed by applying a typology of task-centered problem-solving activities t o audio tape recordings of treatment sessions from the middle phase of treatment.
THE SAMPLE
The sample was 24 practitioner-client pairs who engaged in intensive task-centered treatment in the Task-Centered Service Project (Reid, 1977.)' In half the cases, the client was a child offered service in a school or youth guidance setting. The twelve adult cases were clients a t a psychiatric outpatient clinic. The practitioners were (24) white first-year graduate students in the task- centered treatment sequence at the School of Social Service Admin- istration, University of Chicago, who carried tape-recorded cases as part of their clinical and research field experience. Most had had paid o r voluntary social work experience prior t o entering the program, but were relatively inexperienced in the task-centered approach and new t o their assigned practicum settings.
Of the twelve child clients, nine were black and six male. Nearly half their families received some form of public assistance. The med-
l ~ h e original sample was an accidental sample of clients who a p plied f o ~ service at the participating agencies during the beginning phase of the study. Cases selected for this study included all adults' and a random sample of children's cases which had received at least three intensive intervention interviews.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

361) JOURNAL O F SOCIAL SERVICE RESEARCH
ian age was 9 years, the range 6 t o 17 years. Most children were referred by school authorities, usually for chronic misbehavior. Children's chosen target problems generally related t o academic failure, t o classroom misbehavior such as fighting or extreme with- drawal, o r t o faulty peer interaction. The adults were all black, nine women and nine receiving public assistance. Median age was 27 with a range from 21 t o 52 years. Most adults were self-referred but frequently returning outpatients. Problems identified by adults in- cluded interpersonal, marital, and parent-child conflict; dissatisfac- tion with general social relations; depression; hallucinations; and difficulty handling stress o r making decisions.
CONTEXT OF THE INTERVIEWS
In the original study, treatment was divided into three phases: the problem specification phase, in which client and practitioner formulated target problems (median 3 interviews); the intensive intervention phase, during which tasks were formulated and carried out following the "prescribed" problem-solving steps (median 6 interviews); and an optional final phase of task-centered treatment which continued until the previously-agreed-upon termin- ation (median 3 interviews). This study analyzed only the intensive intervention phase, which focused on problem-solving and which usually included interviews 4 t o 9 in a case sequcnce. However, not all cases actually received six interviews, and the range of analyzable interviews per case was three t o seven. A total of 132 interviews, half from children's cases, was coded according to the communication typology described below.
MEASUREMENT PROCEDURES
The task-centered activities typology (Table 1) categorized verbal communication according to the problem-solving steps thought to be the crucial elements of task-planning and implementation (Reid, 1975, 1977). Entire interviews werc coded in their case sequence from audio tape-recordings.2 All time (practitioners' and clients' verbalizations and intervening pauses) was coded continuously as a given activity until focus shifted to another activity. For ex-
2 ~ 1 1 interviews were tape-recorded. Clicnts' (and children's parents') permission was secured for participation in the study and for audio recording of interviews.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

Anne E. Fortune
TABLE 1
Task-Centered Practitioner-Client Activities
Problem specification (identification. delineation and monitoring of problems)
Generating alternatives (strategies for problem-resolution) Task agreement (to proposed courses of action) Planning details of task implementation Obtaining contextual data (relevant to proposed tasks) Summarization (of tasks and task plans)
Establishing incentive and rationale (for proposed courses of action)
Analyzing obstaclcs ( t o task achievement--includes potential and actually- encountered obstacles)
Simulation-guided practice (rehearsal, role-playing, modeling, etc.)
Review of task progress (evaluation of tasks attempted by the client)
Practitioner task (all discussion of practitioner's tasks)
Structuring interview time (e.g. planning intervicw topics, scheduling, etc.)
Other (discussion unrelated to problem reduction)
a~dapted from W. J. Reid, A study of the characteristics and effectiveness of task-centered methods, report of the task-centered service project, volume 2 (Chicago: School of Social Service Administration, University of Chicago, 1977).
ample, chit-chat a t the beginning of an interview would be coded as "other." When either client or practitioner began discussing a problem, "problem specifi- cation" was coded and continued throughout an interchange until a new activity was initiated, for example, by a practitioner inquiry a6out previous tasks ("task review") or by a client comment about difficulties completing a task ("analyzing obstacles"). Time devoted t o each activity was expressed as a sum (hundredths of minutes) and converted to a percentage of total time. Interviews were coded by former task-centered students who received .approximately 20 hours of training. Intercoder reliability for each category, assessed on 13 interviews, ranged from a median agreement of 25% to 96%. Of the four categories with low reliability (obtaining contextual data, task agreement, summarization. and establishing in- centives), three occurred relatively rarely and the reliability calculations were susceptible to small time disagreements between coders about when an activity began or ended. Nevertheless, the low reliabilities for these categories indicate that the results must be interpreted with considerable caution. Overall agreement -percent of all tape recorder counting units in an interview coded the same by both coders-ranged from 55 to 95%, median 80% agreement.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

JOURNAL OF SOCIAL SERVICE RESEARCH
RESULTS
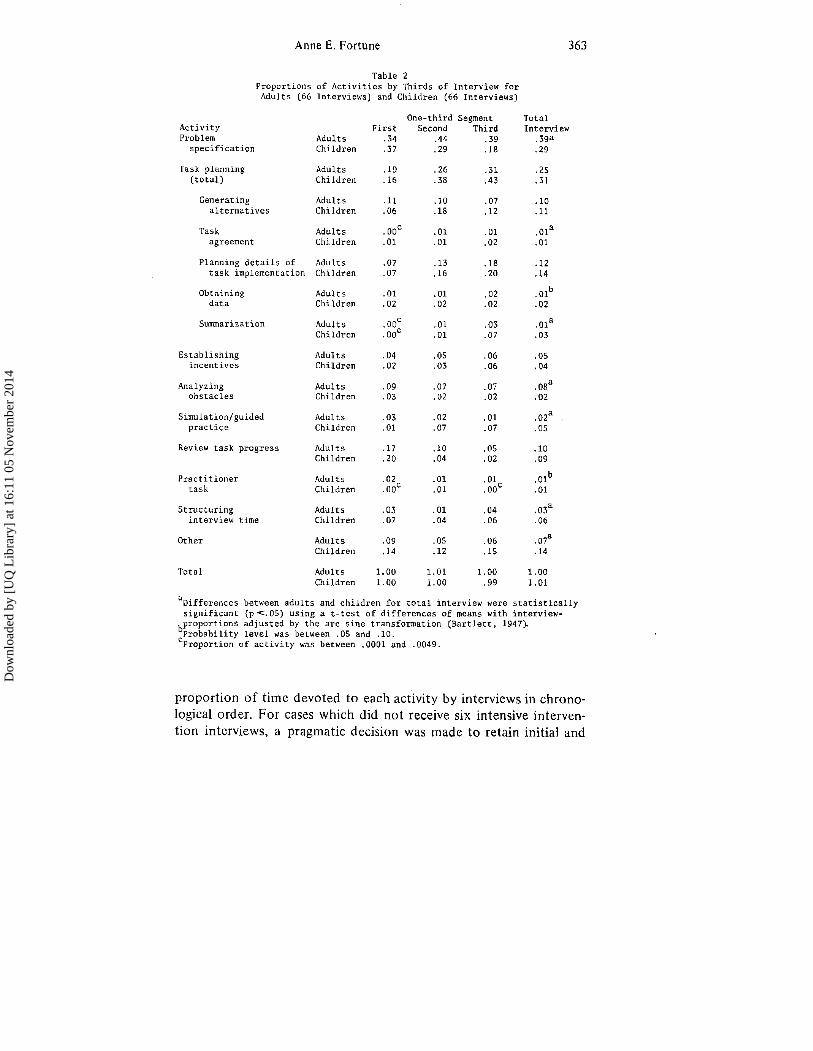
Interview patterns. The intensive intervention in- terviews were divided into one-third segments based on total inter- view length. Table 2 indicates the proportion of time devoted to each activity by thirds and for the entire interview.
For interview totals, there were a number of significant differences in activity proportions between adults and children. Children's inter- views devoted proportionately more time t o activities marginally re- lated t o problem-alleviation (other and structuring interview time), t o certain task-planning activities (task agreement and sunimariza- tion), and to practicing relevant behaviors (simulation/guided prac- tice) (p < .05).3 Adult cases devoted significantly more time t o pro- blem specification and t o analysis of actual or potential obstacles t o task accomplishment.
Activity use patterns across one-third seginents showed some sinii- larities between adults' and children's interviews. For both groups, review of task progress was a fairly large portion of the first third of interviews and then decreased significantly ( p < .05, paired t-tests), while two of the task-planning activities, summarization and planning details of task implementation, increased across segments ( p c .05, paired t-tests). Establishing incentives and rationale for proposed courses of action was also significantly higher in the final third among both groups. In other respects, however, patterns within children's interviews differed from patterns within adults' interviews. Children's interviews showed a decrease in problem specification and a middle-third increase in generating alternatives, but in adults' inter- views both activities were pervasive throughout the interview. Among adults, client agreement t o proposed tasks occurred in the later two- thirds of interviews, but in children's interviews task agreement came almost exclusively in the final third. Analysis of each interview indi- cated that the majority of individual interviews followed the average patterns presented in Table 2. For example, four-fifths of all inter- views used the activity "structuring interview time" mosl in either the first or final segment.
Patterns across interviews. Table 3 indicates the
3 ~ - t e s t of difference of means. Al l proportions used in subsequent calculations were t~ansformed by the inverse sine transformation (Bartlett, 1947).
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014
Anne E. Fortune
Table 2 Proportions of Activities by Thirds of Interview for Adults (66 Interviews) and Children (66 Interviews)
One-third Segment Total Activity First Second Third Interview Problem Adults .34 .44 .39 .39a specification Children .37 .29 .18 .29
Task planning Adults .19 .26 .31 .25 (total) Children .I6 .38 .43 .31
Generating Adults .11 .10 .07 .10 alternatives Children .06 .18 .12 .ll
Task Adults . 0oC .O1 .01 .Ola agreement Children .O1 .01 .02 .01
Planning details of Adults .07 .13 .18 .12 task implementation Children .07 .16 .20 .14
Obtaining Adults .01 .01 .02 . Olb data Children .02 .02 .02 .02
Summarization Adults . 0oC .01 .03 .Ola Children .OoC .01 .07 .03
Establishing incentives
Adults Children
Analyzing obstacles
Adults Children
Simulation/guided practice
Adults Children
Review task progress Adulrs Children
Practitioner task
Adults Children
Structuring interview time
Adults Children
Other Adults Children
Total Adults Children
"~ifferences between adults and children for total interview were statistically significant (p<.05) using a t-tcst of differences of means with interview- bproportions adjusted by the arc sine transformation (Bartlett, 1947). Probability level was between .05 and .lo. C~roportion of activity was between ,0001 and .0049.
proportion of time devoted t o each activity by interviews in chrono- logical order. For cases which did not receive six intensive interven- tion interviews, a pragmatic decision was made t o retain initial and
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

JOURNAL OF SOCIAL SERVICE RESEARCH
Tab le 3 P r o p o r t i o n s o f A c t i v i t i e s by I n t e r v i e w s
i n Sequence f o r Adu l t s and C h i l d r e n
A c t i v i t y I n t e r v i e w Number 2 3 4 5 6
. 45 . 49 . 43 . 3 9 . 25
. 31 .24 .32 . 2 6 .38 Problem
s p e c i f i c a t i o n Adu l t s Ch i l d r en
Task-planning ( t o t a l )
Adu l t s C h i l d r e n
Gene ra t i ng a l t e r n a t i v e s
A d u l t s C h i l d r e n
Task agreement
Adu l t s C h i l d r e n
P l ann ing d e t a i l s of t a s k imp lemen ta t i on
A d u l t s C h i l d r e n
Ob ta in ing d a t a
Adu l t s C h i l d r e n
Summarization Adu l t s .01 .02 . O 1 . O 1 .Ooa .O1 C h i l d r e n .05 .04 .02 .03 .02 .02
E s t a b l i s h i n g i n c e n t i v e s
Adu l t s C h i l d r e n
Analyzing o b s t a c l e s
A d u l t s C h i l d r e n
S imu la t i on /gu ided p r a c t i c e
Adu l t s C h i l d r e n
Rcview t a s k p r o g r e s s
Adu l t s C h i l d r e n
P r a c t i t i o n e r t a s k
Adu l t s C h i l d r e n
S t r u c t u r i n g i n t e r v i c w t i m e
Adu l t s C h i l d r e n
Other A d u l t s C h i l d r e n
T o t a l p r o p o r t i o n Adu l t s C h i l d r e n
Numbcr o f c a s e s Adu l t s 1 2 1 2 12 11 6 12 C h i l d r e n 12 12 1 1 10 8 1 2
a ~ r o p o r t i o n of a c t i v i t y was between .0001 and ,0049.
final interviews designated as first and sixth irrespective of the actual number of interviews. Thus, the next to last interview(s) were desig- nated as "missing" for data analysis. The middle of seven interviews in one child's case was omitted.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

Anne E. Fortune 365
Problem specification increased in middle interviews among adults but remained a t a relatively constant level among children. The task- planning activities as a group decreased considerably across inter- views; for each of the subcategories of task-planning, the later-in- treatment interviews contained significantly less of the activity than early-in-treatment interviews (p < .05, paired t-tests). Although other treatment-related activities increased slightly over time, increases were not significant and the overall picture was one of relative con- sistency in use of all activities except task-planning.
DISCUSSION
The task-centered activities typology applied t o the sample interviews was both a prescription for the practitioners and a description of practice as a problem-solving process. The dual pur- pose permits a comparison of prescribed to actual activity in task- centered interviews.
Problem specification, which included identifying and monitoring the client's problems, was not expected t o dominate interview time t o the extent it did (30 to 40% of time). Research on open-ended treatment modalities indicates that although communications related t o problem clarification may decrease over time, they remain a major proportion of treatment activity, e.g., Bales' orientation (Sucato, 1978), Hollis' exploration-ventilation-description (Boatman, 1975; Ehrenkranz, 1967; Hollis, 1968, 1972; Mullen, 1969; Orcutt, 1971). However, the task-centered model's short-term and action-oriented structure was expected'to limit the amount of problem specification. Furthermore, the selected interviews were from the middle phase of treatment, a phase intended t o formulate and implement tasks to change problems that supposedly had been clearly defined in earlier interviews. The level of problem specification was probably less than in the earlier interviews (as Tolson (1977) noted in a marital case), but it was clearly still a major focus of task planning interviews, and did not diminish across the sequence of interviews. Withm individual interviews, levels of problem specification decreased across thirds for children but not for adults. Some practitioners were probably not maintaining a problem-solving focus (Reid, 1978). However, both the high level and pervasiveness of problem specification when treatment is intentionally structured t o move into resolution-activity suggest that problem exploration should be considered an on-going aspect of
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

366 JOURNAL OF SOCIAL SERVICE RESEARCH
treatment rather than as a preliminary problem-solving step isolated from later steps.
The task planning activities-generating alternatives, task agree- ment, planning details of implementation, obtaining contextual data, and summarization-were not used as pervasively as anticipated in a model structured around the concept of tasks. Indeed, i t was expect- ed that as initial tasks were attempted and (whether the tasks suc- ceeded or failed) realistic approaches t o problems were delineated, task planning would increase. Howcvcr, the task planning activities decreased over six interviews. It is possible that the temporal de- crease was because clients became accustomed to the planning pro- cess, and that as they became more skilled in these aspects of pro- blem-solving less time was devoted t o task planning. On the other hand, i t is also possible that the six-interview prescription in the ori- gna l experiment was longer than optimal, that earlier tasks were so successful in alleviating the target problems that other treatment activities were used to "fill time" t o meet the study's requ i re~nents .~ Nevertheless, it is clear that task-centered treatment is less action- and task-oriented in actual practice than in the "on-paper" model.
Comparison of adults' t o children's cases indicated that while both were following the same general model, there were some dis- tinct differences in implementation. Within an interview, the child- ren's interviews followed task-centered and problem-solving expec- tations much more clearly than adults' inte~views. Review of task progress and problem specification, activities that provide informa- tion about the current situation, were greatest in the first third of an interview. Generating alternative strategies for problem alleviation peaked in the middle portion, and the activities related t o planning future tasks increased linearly t o a peak in the final one-third seg- ment. Simulation/gi~ided practice, which included modeling and re- hearsal of task-related behaviors, was greatest is the final two-thirds, although it is not clear i f simulation was related t o tasks that had been agreed upon or t o "trying out" different behaviors before sel- ecting an approach. Although among children's interviews analyzing obstacles occurred most in the first third, the differences among
4 ~ h e median of 1 2 interviews in this study is somewhat longer than the medians between 8 and 9 reported for similar cases receiving task-centered trcatment in general practice (Epslein, 1977;Brown, 1977).
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

Anne E. Fortune 367
segments were not statistically significant. The analyzing obstacles category unfortunately did not distinguish analysis of blocks t o tasks already attempted vs. tasks contemplated; consequently the inter- pretation of the pervasiveness of analyzing obstacles among children is unclear.
Adult interviews, by contrast, devoted greater time than children's interviews t o verbal analysis of problems (problem specification) and of blocks t o task achievement (analyzing obstacles) and less time t o rehearsing planned tasks (simulation/guided practice). Only the tem- poral decrease of task review and the increase in two of the subcate- gories of task planning (planning details of task implementation and summarization) gave indication of a shift from problem-focus to action-focus within adults' interviews.
Activities not related t o problem-solving showed silnilar patterns among adults and children. Both adults' and children's interviews decreased in use of structuring interview time across thirds and both used "other" (treatment unrelated discussion) least in the middle portion of interviews. This is similar to Pinkus' (1968) finding that practitioners' remarks directed toward structuring the therapeutic situation and routine mechanics of agency-client relations occurred primarily at the beginning and end of an interview. In the task- centered cluldren's interviews, however, the levels of both activities were considerably higher than in adults' interviews and remained quitc high even in the middle of an interview.
In short, children's cases spent more time structuring and main- taining the task formulation and planning focus, yet appeared t o ex- perience greater difficulty keeping the interview "on target" in rela- tion t o treatment activities generally. The adult-child differences may be due t o differing expectations and cognitive and emotional capa- bilities. The children appeared t o have shorter attention spans; work o n problems was frequently interupted by brief interludes of play ("other"). Children appeared more oriented toward action t o allevi- ate problems, often impulsively, and their target problems were more specific and circumscribed. The adults, by contrast, tended t o be chronic outpatients, often with previous experience and expectations of a "talking therapy," and were presumably socialized t o talk about problems, rather than t o take direct action t o alleviate them. Adults' problems also tended t o be more diffuse and to involve others in the environment not directly accessible to the practitioner (children's practitioners, however, intervened in the school environment relative-
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

368 JOURNAL OF SOCIAL SERVICE RESEARCH
ly rarely). These factors may contribute t o the greater emphasis on problem specification among adults and the task-orientation among children. However, because cach practitioner was involved in only one case in the sample, it is possible that some attribute of practi- tioners o r settings influenced the patterns. For example, practitioners in school settings may have become accustomed t o being viewed as adult authority figures, leading them to impose the problem- solving structure on their clients without thinking. Practitioners in the psychiatric clinic may have been more alert t o challenges t o their "expertise" and thus reluctant t o insist on systematic problem- solving.
Nevertheless, results from an analysis of the relation of activity- level t o case outcome, reported elscwhere (Fortune, 1978), suggest that some of the differences between child and adult activity use may be appropriate. For example, among children's cases, higher use of analyzing obstacles was negatively related to outcome, suggesting that although the activity was used less than in adults' cases, the lesser use may be appropriate. Conversely, adults' cases engaged in less structuring of interview time, but more of that activity was negatively related t o outcome; children's cases devoted twice as much time on the average t o structuring, but the level was unrelated t o outc.ome. However, the relationships are only suggestive and con- siderable further research on the issue of in-interview process in relation to outcome is necessary to establish if the elements of ef- fective problem-solving treatment are indeed different for adults and children.
The study poses several problems for generalizing results. The ser- vice offered clients was task-centered treatment, formulated specifi- cally around problem-solving steps. Whether similar problem-solving processes and profiles would emerge for other forms of treatment is questionable, although Sucato (1978) found evidence of Bales' problem-solving phases in psychosocial treatment.
A second major limitation on generalizability was the sample of participants. The practitioners were master's students and some of the results may be due t o their inexperience or t o the close super- vision they received. For example, practitioners may have floundered attempting t o specify problems with digressive adults, o r imposed their own or the school's definition of problems on children. How- ever, Moffatt (1977) regards the task-centered model as an introduc- tion t o casework that limits just such errors. Furthermore, the close
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

Anne E. Fortune 369
supervision ensured that a particular treatment model was imple- mented rather than nebulous therapeutic endeavors. Both factors minimize the possibility of what Jayaratne (1977) calls "multiple techniques," o r practitioners' inadvertant use of treatment techni- ques from other models, making more credible the suggestion that different patterns between adults and children were due t o age-group characteristics rather t h i n practitioner style.
The client participants were lower-class urban minorities, an im- portant segment of the population served by social workers but a client group often ignored in development and assessment of treat- ment models. Hallum (1978) argues that the task-centered approach may be one of sevcral treatment modalities particularly appropriate for lower-class groups because of the lower class' restricted language code. The problem-solving activity profiles described here may not be typical of task-centered practice with middle-class or white clients, although the model has demonstrated applicability for these groups (Reid & Epstein, 1977).
Despite its limitations, the study reported here indicates that task- centered practitioners and clients do generally engage in problem- solving activities as conceptualized in the task-centered activities. That is, there is a clear correspondence between the on-paper descrip- tion of the task-centered model and what its practitioners actually do when facing a client, although the actuality is not as structured or action-focused as the textbook model. However, levels and patterns of activity-use differ somewhat between adults and children. The children's cases appeared t o follow logical problem-solving steps more closely than adults' cases, but devote proportionately more time to activity unrelated t o target problems. Adults' cases devoted more time to treatment-relevant activity but there was less clear in- dication of problem-solving stages. Further research is necessary t o determine if the observed differences are therapeutically optimal, yet it is clear that the same general task-centered model can be used, with refinements, for both children and adults.
REFERENCES
Barrett, C. L., Hampe, I. E., & Miller, L. Resea~ch on psychotherapy with children. In S. L. Garfield & A. E. Bergin (Eds.), Handbook o f psychotherapy and behavior change: An empiriul analysis (2nd edition). New York: John Wiley & Sons, 1978.
Bartlett, M. S. The use of transformations. Biometries, 1947, 3, 39-52.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

JOURNAL OF SOCIAL SERVICE RESEARCH
Boatman, F. L. Caseworkers' judgments of clients' hopc: Some correlates among client- situation characteristics and among workers' communication patterns. Unpublishcd doc- tord dissertation, Columbia University, 1975.
Brown, L. B. Treating problems o f psychiatric outpatients. In W. J. Reid & L. Epstein (Eds.), Task-centered practice. New York: Columbia Univcrsity Press, 1977.
Cunningham, G. Caseworker support o f client problem solving. Unpublished doctoral disser- tation, University of Chicago, 1977.
D'ZuriUa, T. J., & Goldfricd, M. R. Problem-solving and behavior modification. Journal of Ahnormnl Psychology, 1971, 78, 107-126.
Ehrenkranz, S. M. A study of the techniques and procedures used in joint interviewing in the trcatmcnt o f marital problems. Unpublished doctoral dissertation, Columbia Univer- sity, 1967.
Epstein, L. A project in school social work. In W. J . Reid & L. Epstein (Eds.), Task-centered practice. New York: Columbia University Press, 1977.
Fortune, A. E. Verbal co~nmunication in task-centered treatment. Unpublished doctoral dissertation, University of Chicago, 1978.
Gurman, A. S. Instability of therapeutic conditions in psychotherapy. Journal of Counseling Psychology, 1973,20, 16-24.
Hallum, K. C. Social class and psychothcrapy: A sociolinguistic approach. C7inical Social Work Journal, 1978, 6, 188-201.
Heppncr, P. P. A review of the problem-solving literature and its relationship to the coun- seling process. Journal o f Co~mseling Psychology, 1978,25, 366-375.
Hollis, F. 02sework: A psychosocial therapy. New York: Random Housc, 1972. Hollis, F. A typology of casework treatment. New York: Family Service Association of
America, 1968. Jayaratne, S. Single-subject and group designs in treatment evaluation. Social Work Research
and Abstracts, 1977, 13, 35-42, Lennard, H. L., & Bernstein, A. Patterns in human interaction. San Francisco: Jossey-Bass,
Inc., 1969. Lennard, H. L., & Bernstein, A. The anatomy ofpsychotherapy: Systems of communication
and expectation. New York: Columbia University Press, 1960. Lish, R. Verbal techniques in casework with children. Unpublished doctoral dissertation,
University of Chicago, 1973. Moffatt, R. Using the task centered model as an introduction t o casework, in student super-
vision. Contemporary Social Work Education, 1977, 1, 24-37. Mullen, E. J. Differences in worker style in casework. Social Casework. 1969,50. 347-353. Orcutt, B. A. Process analysis of the fiist phase of treatment. In P. C. Cohen & M. S. Krause,
(Eds.), Casework with wives of alcoholics. New York: Family Service Association of America, 1971.
Pinkus, H. Casework techniques related to selected characteristics of clients and workers. Unpublished doctoral dissertation, Columbia University, 1968.
Proctor, E. K. Structuring of early treatmcnt interaction: An exploratory study of thera- pists' behaviors. Unpublished doctoral dissertation, Washington University, 1978.
Reid, W. J. The task-centered system New York: Columbia University Press, 1978. Reid, W. I. A study of thc characteristics and effectiveness of task-centered methods. Vol. 2,
Report of the task-centered service project (SRS grant no. 18-P-5777415-03). Chicago: School of Social Service Administration, University of Chicago, 1977.
Reid, W. J. A test of 3 task-centered approach. Social Work, 1975, 20, 3-9. Reid, W. J., 81 Epstein, L., eds. Task centered practice. New York: Columbia University
Press, 1977. Reid, W. J., & Epstein, L. Task-centered casework. New York: Columbia University Press,
1972.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014

Anne E . Fortune
Reid, W. J., & Shyne, A. W. BrieJandexrended casework. New York: Columbh University Prcss, 1969.
Roberts, R. W., & Northen, H. (Eds.), Theories of social work with groups. New York: Columbia University Press, 1976.
Sucato, V. The problem-solving process in short-term and long-term service. Social Service Review, 1978,52, 244-246.
Tolson, E. A singlc organism design for evaluating the effectiveness of the task implementa- tion scquence in modifying marital communication problems. Unpublished doctoral dissertation, University of Chicago, 1977.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
16:
11 0
5 N
ovem
ber
2014





























