Embed Size (px)
Citation preview
436
THE PROBLEM OF THE AGED AMPUTEEBy MARJORY WARREN, M.R.C.S., L.R.C.P.
Consultant Physician, Geriatric Unit, Deputy Medical Director, West Middlesex Hospital, Isleworth, Middlesex
It is well known that the population is ageingnot only in this country, but also in many othercountries. Morbidity is greater among the olderthan among the younger members of the popu-lation, and there is therefore a high and increasingincidence of those degenerative conditions whichresult in amputation of a limb or part of a limb.
Amputations which may be of the upper or oneor both of the lower limbs usually follow de-generative vascular changes, a malignant con-dition or trauma. In the elderly by far the com-monest condition necessitating amputation isgangrene, resulting from arteriosclerosis-in-cluding the so-called' diabetic gangrene,' which ismost probably also arteriosclerotic in origin. Thechanges occur much more frequently in the peri-pheral vessels of the lower limb than in those ofthe upper limb.
This article will not include a detailed discussionof the aetiology and underlying pathology of con-ditions leading to amputation nor will it describesurgical techniques. It sets out only to prescribein detail the correct management of the elderlyamputee and to emphasise points necessary to hisgood treatment.
It must be accepted therefore at the outset thatunless adequate overall and detailed care be under-taken much of the benfit of surgery will be lost,for the final success of the patient rests upon morethan surgical skill. Indeed, the actual surgicalremoval of a limb, essential as it is, may be thesimplest part of the treatment. In every case ofamputation, however old and/or frail the patientmay be, it is important for the surgeon to bear inmind that the stump must be adequate to carry apylon or prosthesis.A good psychological approach before operation
for amputation can do much to reassure. Everyamputee following operation needs very carefulmanagement, including full rehabilitation as wellas general treatment, physical and psychological.Throughout treatment, too, it is essential thatattention be given by the almoner (medical social
worker) to the patient's social conditions, for,without this, return to his home may become im-possible and much independence may thereforebe lost.Among elderly patients ,two important facts
must be remembered-firstly, that a variety ofarteriosclerotic manifestations are liable to occurin the same patient, namely coronary insufficiency,ischaemic heart disease, cerebro-vascular accidentswith resulting hemiplegia, Parkinson's disease,etc.; and, secondly, the frequency with which amultiple pathology is found. "
Both these factors add to the difficulties of fulland complete rehabilitation-but neither thepresence of other arteriosclerotic manifestationsnor yet the occurrence of multiple pathology mustbe used as an excuse for undertreatment. Suchpatients, after an amputation of one or even bothlower limbs, can be restored to considerablepersonal independence, when full and adequatetreatment is carried out.A study of such amputees' has shown that nearly
all suffer from other serious handicaps and thatmany develop additional handicaps while actuallyunder treatment. These episodes limit progressand cause delay in, but should not be used tocease, rehabilitation. In spite of these set-backsand from the total experience of centres treatingthese patients it is the opinion that most am-putees, single and double, should be educated towalk again using a single pylon or two rockerpylons. It has, moreover, been found that whentreatment is successful, then in the majority ofcases the patient can and does become almostcompletely independent for most of his personalneeds. He can leave the hospital and live at homewith his own people or can be accepted into aresidential home, where he can enjoy a reasonablynormal and interesting life. ^Without such facilities all elderly amputees, and
particularly double amputees, may become veryheavy nursing cases and as such a serious economicburden to the community.
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
September 1957 WARREN: The Problem of the Aged Amputee 437
Amputation of Lower LimbThe amputation of one lower limb may be
followed by an amputation of the other and,although in principle the general pattern oftreatment is the same for both, there are essentialpractical differences in the management of asingle and a double amputee.The different phases of treatment for both
include:(I) Pre-operative care.(2) Post-operative and pre-pylon care.(3) Post-pylon care.(4) Maintenance and follow-up care.
(i) Pre-operative careThis includes care of potential amputees and
those patients who, having already lost one lowerlimb, are about to lose the second and so to becomea double amputee.(A) GENERAL CAREWith elderly amputees it must be remembered
that in the majority of cases the gangrene isessentially a manifestation and part of a medicalcondition. There is, therefore, much to be gainedfor the patient, when he is seen by a physicianprior to amputation and then transferred back tohis care for full rehabilitation as soon as thesurgical technique is completed, that is when thesutures are out and the wound healed.
It is important, whenever possible, to see thepatient before operation in order to undertake athorough medical review and to reassure him,allay his fears and try to minimise the feeling offrustration concerning his disability and im-pending loss of independence. Such medicalreview must include correction of all conditionsfound which need treatment, including cardiacfailure, glycosuria, impaired sight and/or hearing,etc.Advice to the patient at this time concerning
his future should be guarded, but as optimistic asis reasonable and he should be told of the oppor-tunuties for re-education. Whenever it is possiblefor the patient to meet and talk to another amputeewho is doing well, this should be arranged, forsuch a contact is often most encouraging to the'new' patient, who at this time is generallymiserable, depressed and very apprehensive.When this opportunity is not possible, a talk
after his amputation is helpful. The knowledgethat he can become ambulant in a self-propelledwheel chair of his own and that he may be able toget about on pylon(s) gives ground for consider-able optimism to a patient, who feels doomed topermanent dependence upon others and can seeno future beyond his bed (and that perhaps in ahospital).
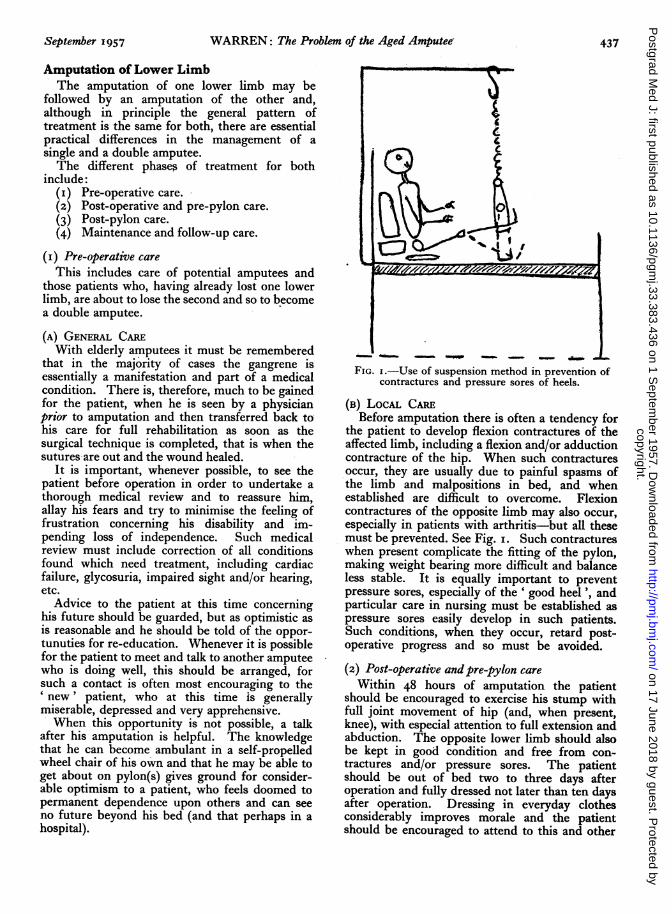
FIG. I.-Use of suspension method in prevention ofcontractures and pressure sores of heels.
(B) LocAL CAREBefore amputation there is often a tendency for
the patient to develop flexion contractures of theaffected limb, including a flexion and/or adductioncontracture of the hip. When such contracturesoccur, they are usually due to painful spasms ofthe limb and malpositions in bed, and whenestablished are difficult to overcome. Flexioncontractures of the opposite limb may also occur,especially in patients with arthritis-but all thesemust be prevented. See Fig. i. Such contractureswhen present complicate the fitting of the pylon,making weight bearing more difficult and balanceless stable. It is equally important to preventpressure sores, especially of the ' good heel', andparticular care in nursing must be established aspressure sores easily develop in such patients.Such conditions, when they occur, retard post-operative progress and so must be avoided.
(2) Post-operative andpre-pylon careWithin 48 hours of amputation the patient
should be encouraged to exercise his stump withfull joint movement of hip (and, when present,knee), with especial attention to full extension andabduction. The opposite lower limb should alsobe kept in good condition and free from con-tractures and/or pressure sores. The patientshould be out of bed two to three days afteroperation and fully dressed not later than ten daysafter operation. Dressing in everyday clothesconsiderably improves morale and the patientshould be encouraged to attend to this and other
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
438 POSTGRADUATE MEDICAL JOURNAL September 1957
personal needs himself, within a few days of hisamputation. As soon as the patient sits out ofbed in an armchair he should, if a single amputee,wear a leather lace-up walking shoe on his goodfoot to protect the foot from trauma, in order thathe can conveniently take weight on the foot whenstanding and for improvement of morale.As soon as possible after sutures are removed
and when the patient is fully dressed he shouldbe provided with a self-propelled wheel chairfitted with one, or preferably two, brakes in front,which he should occupy all day except when doingexercises. This use of a wheel chair not onlygives a measure of independence and freedom,but also allows a good deal of useful physiotherapyfor the trunk and upper limbs.
Occupational therapy and physiotherapy shouldbe utilised as much as possible at all stages.Occupational therapy will vary considerablyaccording to the tastes, mental capacity andphysical state of the patient, but should be full andcontinuous. The patient may take part in occu-pational therapy as individual exercise or as amember of a team, e.g. in games-such as pillowfighting, deck quoits, ball games, archery, etc.All these games encourage good balance, accuracyof movement, improved use of the upper limbs anda mental alertness and ambition.
Individual exercise, either as occupationaltherapy or as physiotherapy, emphasises the needfor full movement of the hip joints, includingflexion, extension, abduction and adduction ofstumps, fixation of the hips and lifting of thetrunk by the use of an overhead pulley. Acombination of these activities prepares theamputee physically and psychologically for maxi-mum independence and later for the use ofpylons.
So far such general principles apply equally toall amputees. The details of practical rehabilita-tion of the single and double amputee must, ofcourse, differ and will be described separately.In all instances, however, treatment must beadapted to the patient, considering his personaldisabilities.
(A) SINGLE AMPUTEEFully clad and in a leather lace-up shoe, with
sutures out and other medical conditions con-trolled, the new amputee should start on a plannedpattern of treatment in preparation for a pylonand later, perhaps, a prosthesis. The plan oftreatment includes:
i. Care of stump.ii. Exercise in a wheel chair.
iii. Bed-end exercises.iv. Exercises in hopping along on the flat and
on the stairs.
i. Care of stumpThe stump should be regularly bandaged
according to the Roehampton method and theaim is to produce a conical stump. Exercises, in-cluding full movement of the stump(s), if under-taken correctly, should prevent contracture of thejoint(s).ii. Exercise in a wheel chairAs early as possible the patient should get about
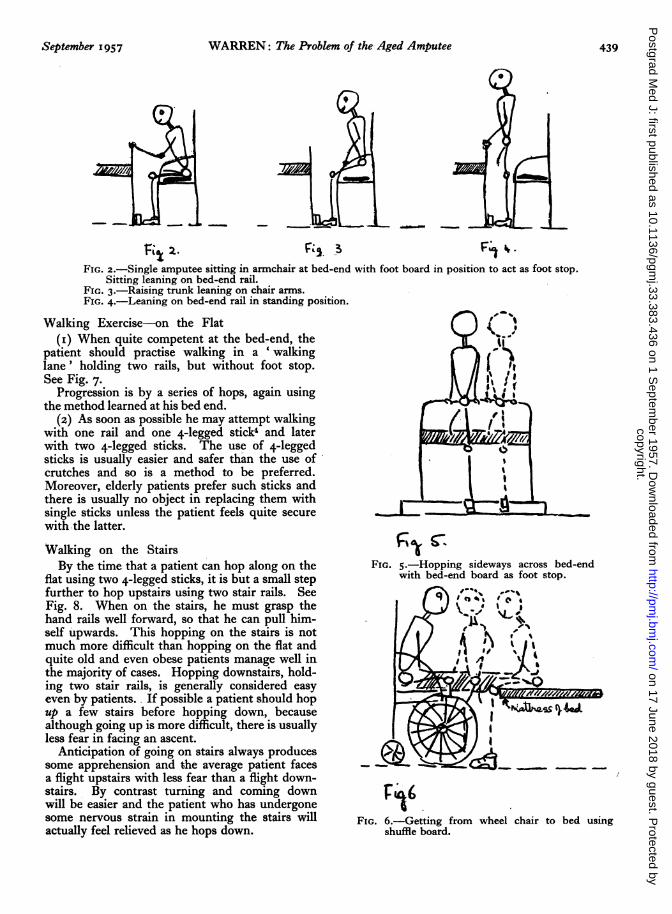
in a self-propelled wheel chair, both indoors andout of doors. He should learn to get from bed tochair and from chair to bed, using, when necessary,a' shuffle board.'2 See Fig. 6. During the wholeof this period the patient has the freedom of theward and can go to toilet unaided, although in theearly stages he may need help in getting from hischair to the toilet seat.
iii. Bed-end exercises3These exercises are done by the patient sitting
comfortably and well back in an armchair at theend of his bed. See Fig. 2. Such a chair shouldhave a firm seat, I7 in. to I8 in. from the floor andbe provided with a sorbo air ring, as this is lessliable to slip than a cushion on a polished seat.An upholstered chair, and especially one withinternal springs, is more difficult for the patientto rise from. If the patient is very short a lowerchair may be needed, in order that he can sit, asdescribed above, with his foot flat on the floor.The rail at the end of a hospital bed (33 in.
above the floor) gives support to the patient whenhe stands up.A wooden bed-end board, 4 ft. in length and
4 in. x 2 in. on section, placed on the floor acrossthe foot of the bed (on its 4 ft. x 2 in. surface) actsas a foot stop. Exercises in order of successionare as follows-using the bed-end board in allinstances as a foot stop:
(i) Patient is encouraged to lift himself in theseat of his chair by hand support on thearms of the chair. See Fig. 3. Thisexercise is a great help to all who nurse himas it allows clothes to be pulled up anddown easily, permits the patient to changehis position and relieves prolonged pres-sure on the sacral area.
(2) Patient should learn to stand up from asitting position leaning on the bed-endrail (see Fig. 4) and then to sit again inhis chair.
(3) While standing at the end of his bed thepatient must learn to stoop by flexing hissound leg and then to stand upright again.
(4) Later he should learn, using the aboveexercise, to hop across the end of his bed.See Fig. 5.
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
September 1957 WARREN: The Problem of the Aged Amputee 439
/1
K^ 2. F; 3 F4 .
FIG. 2.-Single amputee sitting in armchair at bed-end with foot board in position to act as foot stop.Sitting leaning on bed-end rail.
FIG. 3.-Raising trunk leaning on chair arms.FIG. 4.-Leaning on bed-end rail in standing position.
Walking Exercise-on the Flat(I) When quite competent at the bed-end, the
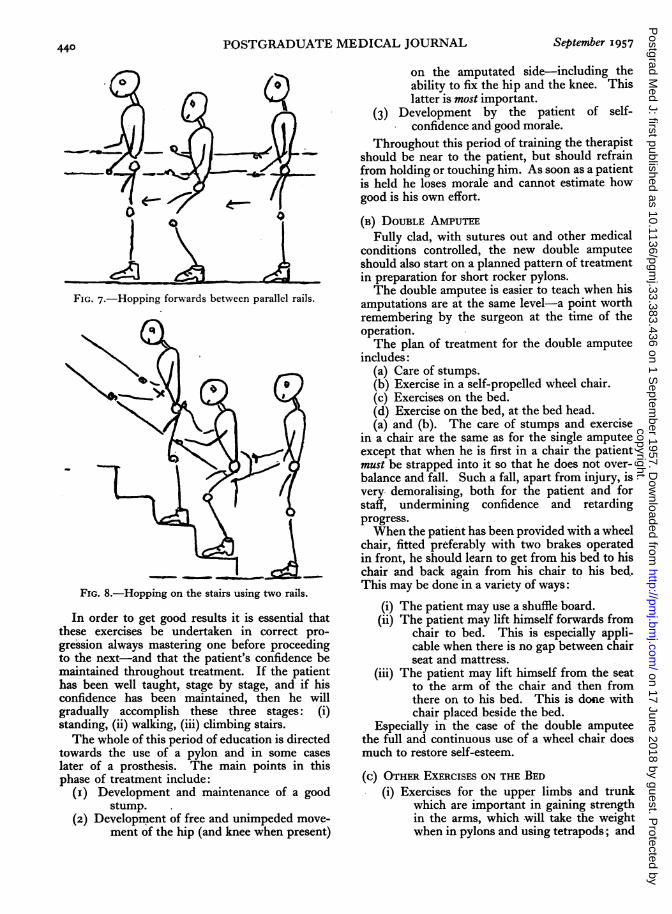
patient should practise walking in a 'walkinglane' holding two rails, but without foot stop.See Fig. 7.
Progression is by a series of hops, again usingthe method learned at his bed end.
(2) As soon as possible he may attempt walkingwith one rail and one 4-legged stick4 and laterwith two 4-legged sticks. The use of 4-leggedsticks is usually easier and safer than the use ofcrutches and so is a method to be preferred.Moreover, elderly patients prefer such sticks andthere is usually no object in replacing them withsingle sticks unless the patient feels quite securewith the latter.
Walking on the StairsBy the time that a patient can hop along on the
flat using two 4-legged sticks, it is but a small stepfurther to hop upstairs using two stair rails. SeeFig. 8. When on the stairs, he must grasp thehand rails well forward, so that he can pull him-self upwards. This hopping on the stairs is notmuch more difficult than hopping on the flat andquite old and even obese patients manage well inthe majority of cases. Hopping downstairs, hold-ing two stair rails, is generally considered easyeven by patients. If possible a patient should hopup a few stairs before hopping down, becausealthough going up is more difficult, there is usuallyless fear in facing an ascent.
Anticipation of going on stairs always producessome apprehension and the average patient facesa flight upstairs with less fear than a flight down-stairs. By contrast turning and coming downwill be easier and the patient who has undergonesome nervous strain in mounting the stairs willactually feel relieved as he hops down.
f.)
l' IY( !,
FIG. 5.-Hopping sideways across bed-endwith bed-end board as foot stop.
Fe"
FIG. 6.-Getting from wheel chair to bed usingshuffle board.
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
440 POSTGRADUATE MEDICAL JOURNAL September 1957
1L 1
FIG. 7.-Hopping forwards between parallel rails.
FIG. 8.-Hopping on the stairs using two rails.
In order to get good results it is essential thatthese exercises be undertaken in correct pro-gression always mastering one before proceedingto the next-and that the patient's confidence bemaintained throughout treatment. If the patienthas been well taught, stage by stage, and if hisconfidence has been maintained, then he willgradually accomplish these three stages: (i)standing, (ii) walking, (iii) climbing stairs.The whole of this period of education is directed
towards the use of a pylon and in some caseslater of a prosthesis. The main points in thisphase of treatment include:
(I) Development and maintenance of a goodstump.
(2) Development of free and unimpeded move-ment of the hip (and knee when present)
on the amputated side-including theability to fix the hip and the knee. Thislatter is most important.
(3) Development by the patient of self-confidence and good morale.
Throughout this period of training the therapistshould be near to the patient, but should refrainfrom holding or touching him. As soon as a patientis held he loses morale and cannot estimate howgood is his own effort.
(B) DOUBLE AMPUTEEFully clad, with sutures out and other medical
conditions controlled, the new double amputeeshould also start on a planned pattern of treatmentin preparation for short rocker pylons.The double amputee is easier to teach when his
amputations are at the same level-a point worthremembering by the surgeon at the time of theoperation.The plan of treatment for the double amputee
includes:(a) Care of stumps.(b) Exercise in a self-propelled wheel chair.(c) Exercises on the bed.(d) Exercise on the bed, at the bed head.(a) and (b). The care of stumps and exercise
in a chair are the same as for the single amputeeexcept that when he is first in a chair the patientmust be strapped into it so that he does not over-balance and fall. Such a fall, apart from injury, isvery demoralising, both for the patient and forstaff, undermining confidence and retardingprogress.When the patient has been provided with a wheel
chair, fitted preferably with two brakes operatedin front, he should learn to get from his bed to hischair and back again from his chair to his bed.This may be done in a variety of ways:
(i) The patient may use a shuffle board.(ii) The patient may lift himself forwards from
chair to bed. This is especially appli-cable when there is no gap between chairseat and mattress.
(iii) The patient may lift himself from the seatto the arm of the chair and then fromthere on to his bed. This is done withchair placed beside the bed.
Especially in the case of the double amputeethe full and continuous use of a wheel chair doesmuch to restore self-esteem.
(c) OTHER EXERCISES ON THE BED(i) Exercises for the upper limbs and trunk
which are important in gaining strengthin the arms, which will take the weightwhen in pylons and using tetrapods; and
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
September I957 WARREN: The Problem of the Aged Amputee 4
1-<;(?
FL/., ////,-/,,//,//,,////
f-Q3~ 'c V --
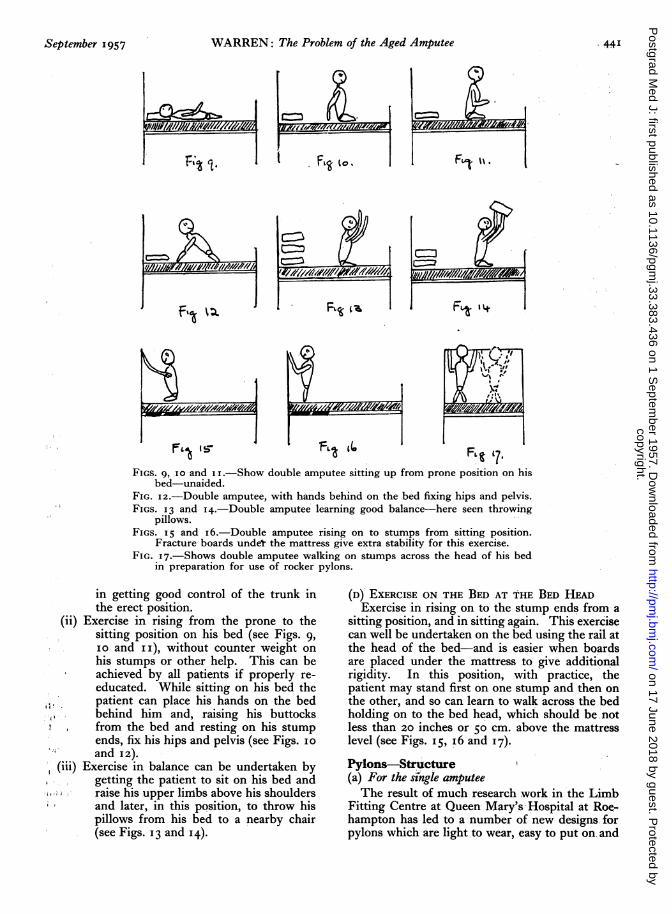
FIGS. 9, IO and I .-Show double amputee sitting up from prone position on hisbed-unaided.
FIG. 12.-Double amputee, with hands behind on the bed fixing hips and pelvis.FIGS. I3 and I4.-Double amputee learning good balance-here seen throwing
pillows.FIGS. 15 and i 6.-Double amputee rising on to stumps from sitting position.
Fracture boards undeT the mattress give extra stability for this exercise.FIG. 17.-Shows double amputee walking on stumps across the head of his bed
in preparation for use of rocker pylons.
in getting good control of the trunk inthe erect position.
(ii) Exercise in rising from the prone to thesitting position on his bed (see Figs. 9,io and 11), without counter weight onhis stumps or other help. This can beachieved by all patients if properly re-educated. While sitting on his bed thepatient can place his hands on the bed
:, behind him and, raising his buttocksfrom the bed and resting on his stumpends, fix his hips and pelvis (see Figs. ioand 12).
(iii) Exercise in balance can be undertaken bygetting the patient to sit on his bed and
, raise his upper limbs above his shouldersand later, in this position, to throw hispillows from his bed to a nearby chair(see Figs. 13 and 14).
(D) EXERCISE ON THE BED AT THE BED HEADExercise in rising on to the stump ends from a
sitting position, and in sitting again. This exercisecan well be undertaken on the bed using the rail atthe head of the bed-and is easier when boardsare placed under the mattress to give additionalrigidity. In this position, with practice, thepatient may stand first on one stump and then onthe other, and so can learn to walk across the bedholding on to the bed head, which should be notless than 20 inches or 50 cm. above the mattresslevel (see Figs. 15, i6 and i7).Pylons-Structure(a) For the sizngle amputeeThe result of much research work in the Limb
Fitting Centre at Queen Mary's Hospital at Roe-hampton has led to a number of new designs forpylons which are light to wear, easy to put on. and
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
442 POSTGRADUATE MEDICAL JOURNAL September 1957
simple to use. These offer great advantages overthe older types. It is important to be very surethat the length of the pylon is correct. An over-sight in this detail is not uncommon.
(b) For the double amputeeThe modern short rocker pylons have been
designed. These pylons are light in weight,average 8 lb. (3.6 kilograms), and measure approxi-mately 24 inches (60 cm.) from belt to floor. Thebuckets are made of plastic material held in posi-tion by a light metal frame and attached to thewaist belt by a strip of metal capable of movementabout a simple joint. The curved rocker footpieces are made of light plywood and pointbackwards, enabling the patient to throw hisweight forwards when walking.Post-pylon Care
In the case of both single and double amputeesvery little difficulty is experienced in the educationof walking in pylons provided that the patient hasbeen properly prepared for them by methods justdescribed.
Single AmputeeIn the case of the single amputee, provided the
pylon fits well and is comfortable, he continues toexercise as he did before he had his pylon and hefinds standing, walking and stair climbing easierwith the additional support. He should thengraduate to the use of two 4-legged sticks, but willmost probably soon take one 4-legged stick plusone single stick and later two single sticks. Forthose patients who continue to feel the need oftetrapods, no attempt to take them away shouldbe made.
In climbing stairs the patient raises the soundleg and draws the pylon up behind. In descend-ing he lowers his pylon first while flexing the hipand knee of the oncoming sound limb whichfollows. The patient must, before education iscomplete, be taught to put on his own pylon,which is not a difficult procedure, but which isimportant to his final independence.Double AmputeeUse ofpylons on the flatWhen the patient is as independent as possible
and competent in the exercises described, andNOT before, he should be provided with pylonsand these should be made with all speed. It isuseless to provide pylons until a patient is able tobalance himself well and to stand on his stumpends as previously described, and too early pro-vision will only frustrate a patient and retardprogress.As soon as he is ready, however, pylons should
be provided and it has been found from experiencethat the sooner he is fitted with pylons the shorteris the time needed to complete his re-education.In the earliest stages with pylons the best methodof education is to use two parallel rails-the'walking lane.' Following the use of the tworails the majority of elderly patients need two4-legged sticks in learning to walk and there isno good reason for withholding these and insistingon the use of ordinary sticks. In the past somepatients have been regarded as failures until thevalue of the four-legged sticks was appreciated.Use ofpylons on the stairsAs soon as a patient is competent to walk on the
flat with two 4-legged sticks and without helpthen, in the majority of cases, he should attemptstairs. The stairs must be provided with a railon each side of the staircase.
It has been established beyond any doubt thata patient should descend stairs backwards andascend forwards, when using the rocker pylons.To descend forwards throws the patient's weightto the edge of the stairs, and with narrow stairsactually beyond the edge, with the inevitable feel-ing of danger and tendency to fall forwards.Whereas descent backwards leaves the weightclose to the rise of the stairs in a safe position. Itwas lack of this knowledge which prevented there-education of earlier patients on the stairs andso deprived them of additional independence.
In spite of the simple structure of the modernshort pylon, elderly patients usually find itdifficult to get into them without help, but thisshould be learned whenever possible. Methodsinclude:
(I) Lying on the bed patient slips his stumpsinto the buckets of his pylons and thenlifts his pelvis, while still on the bed, inorder to draw the belt up over his pelvisbefore sitting up to fasten it.
(2) Sitting on the edge of the bed the patientplaces his pylons on the floor and slipsinto them in a vertical position, leaningagainst the side of the bed while hefastens the belt with a single buckle.
This method is made easier when a heavyboard, provided with rubber non-skid patches onthe under surface and wooden channels on theupper surface, is placed on the floor and the pylonfeet are placed in the channels. By this methodthe pylons are less likely to slip and/or rotate andgreater stability is provided.Post-pylon Care and MaintenanceAn essential service to the elderly amputee is
good continued supervision in order to note asearly as possible any fault or change in the pylon
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
September 1957 WARREN: The Problem of the Aged Amputee 443
or any deterioration of the patient and/or hisliving conditions.
Delay in repair of, or adjustment to, a pylon maywell cost a patient much loss of independence.While not wearing his pylon and with less exercisethan usual, he may put on so much weight that thebucket no longer fits. It is not surprising thatduring such a period he becomes frustrated andloses self-respect.When pylons need adjustment this should be
done at once and with no alteration that is notessential. Wearing a pylon is difficult for an oldperson and sudden changes of design put un-necessary strain upon him. Pylons need to bevery simple indeed. Limb fitting centres shouldwork in the closest liaison with the physician inwhose care the patient has had his rehabilitationand general medical treatment.
Pylon versus ProsthesisIn younger persons the pylon is usually regarded
as the first step towards the use of a prosthesis.In a large number of elderly persons it is medicallyunwise to abandon the pylon and provide aprosthesis and this applies particularly to thedouble amputee. The prosthesis is heavier, moredifficult to manage and apart from aesthetic pur-poses, has little to recommend it. The mech-anism of flexing the knee when sitting is certainlyhelpful when it is operated accurately, but this isnot always achieved by the old person. Sometypes of modern pylon are fitted with a simpleknee joint which allow flexion and give, in thisrespect, advantages similar to those of theprosthesis.
In the case of the double amputee the addedheight of a prosthesis seriously interferes withbalance, and often the change from pylons toprosthesis is one of great mental and physicalstrain. The physical strain is most often manifestby cardiac failure with oedema of stumps makingthe wearing of the prosthesis difficult.
It is sometimes the patient who makes therequest for a prosthesis, but a change from pylonto prosthesis should always be discussed at a con-sultation between the physician in charge of thepatient and the Limb Fitting Centre, before adecision is taken. Even a change in the detailof a pylon may be too much for a patient tomanage and such a suggested change should bediscussed with the physician in charge beforealterations are made. Those who work with thisproblem amongst the elderly have frequently seenthe amputee, perfect in pylons, converted intoan abysmal failure in prostheses.
Prostheses for the elderly should be the ex-ception rather than the routine, and should only
be provided after a careful and full medical review.
Upper LimbThe treatment of an elderly patient with an
amputation of an upper limb is essentially the re-education of the patient to undertake personalneeds with one instead of two hands and to transferto the left hand (in cases of an amputation of theright upper limb) those things which he hashitherto done with the right. The general manage-ment of the patient should be as already describedfor patients who sustain an amputation of thelower limb. In the early post-operative phase itmay be necessary to supervise balance in walkingand to treat conditions of psychological trauma.Although prostheses are available seldom would itbe considered necessary to burden the elderlypatient with one, except on occasion for aestheticpurposes.
Difficult ProblemsMany elderly amputees present with very
difficult additional disabilities which include:(I) One above knee and one below knee
amputation.(2) An above knee amputation combined with
a hemiparesis.(3) An above knee amputation with an un-
united fracture of the neck of one orother femur.
(4) A bilateral amputation with blindness.Such combined disabilities must always be
accepted as a challenge and treated on individuallines.
Summary of General Principles(i) Patients must be treated fully with meti-
culous care of detail and in continuity.(2) When possible patients should be seen and
assessed medically and psychologically beforeamputation by the physician in whose care theywill be after amputation.
(3) Education should be aimed at fullindependence.
(4) When necessary aids such as sticks (singleor tetrapod), chairs, gadgets, rails and rampsshould be provided.
(5) Post-pylon care and maintenance must beearly and efficient if success is to be maintained.
(6) With full team work and a planned patternof treatment most amputees should become in-dependent for personal needs, proficient in a wheelchair and able to walk on the flat and on the stairs.
I wish to acknowledge the help that I have hadfrom, a number of medical colleagues and especiallyto mention Dr. M. M. Pam and Dr. J. Kaminski.References continued on page 451
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from
September 1957 KNIGHT: Aetiological Factors in Trigeminal Neuralgia 451
trigger areas, the pain spots which are seen socharacteristically in this condition and no other ?That the virus of herpes simplex is present in
the majority of patients suffering from trigeminalneuralgia is evidenced by the fact that complementfixation tests are positive in ioo per cent. of casestested.We have performed complement fixation tests
upon a consecutive series of patients operated uponat the South-East Metropolitan Regional Neuro-surgical Centre, and in all of the subjects testedanti-bodies were present in high concentration ina serum dilution of I in 80 or i in 40.There is likewise the evidence provided by the
high incidence of post-operative outbreaks ofherpes simplex. Cushing12 described a form offacial herpes following section of the trigeminalsensory nerve and regarded it as a form of herpeszoster; Richter13 and more recently Carton andKilbourne have demonstrated by inoculationexperiments that this eruption was due to the virusof herpes simplex. The incidence of post-operative herpes has been assessed by Epstein14 atapproximately 25 per cent. Carton and Kilbournehave estimated that minute vesicles can be detectedwith the aid of a lens in over go per cent. of cases.In our experience outbreaks visible to the nakedeye occur in approximately 60 per cent. of the 175cases operated upon in recent years at the South-East Metropolitan Regional Neurosurgical Centreand bear no direct relationship to the occurrence ofpre-operative herpes simplex. Usually the erup-tion is seen about 24 hours after operation and nofurther attacks occur, but in rare cases post-operative herpes may be recurrent.There is sometimes a very close relationship
between the distribution of the post-operativeherpes and the distribution of the pre-operativepain, and I would like to quote one final case.A Mrs. E. S. had for three years suffered fromsevere recurrent neuralgia involving the seconddivision of the nerve. A complete Sensory RootSection was performed producing completeanaesthesia in all three divisions in April I947.Two days later she developed a massive outbreakinvolving the whole territory of the seconddivision associated later with crusting in the noseand ulceration of the ala, which was so severe thatin April 1948, I referred her for plastic repair toMr. F. T. Moore who produced a most satis-factory cosmetic result by grafting in a portion of
the cartilage of her ear. It appeared to me to besomething more than a coincidence that so severean outbreak should be confined exclusively to theterritory of the second division, which had beenthe principal site of her pain, in a patient in whomthe entire sensory root had been divided. Bearingthese facts in mind, together with the negativecharacter of any alternative evidence, I wouldsuggest that the possibility of virus infectionbeing the cause of trigeminal neuralgia is wellworthy of further consideration.
Primary infection with herpes simplex is com-mon and following this the virus persists in thebody as indicated by the persistently high titre ofantibiodies. The virus thus persisting seems tohave a special affinity for the trigeminal nerve, asindicated by the frequent recurrent outbreaks ofherpes simplex whether preceded by neuralgiaor not, in the maxillary and mandibular areas.It is further indicated by the fact that post-operative herpes is almost exclusively seenfollowing operations involving directly or in-directly the sensory root of the trigeminal nerveand its deeper connections.
All this evidence would suggest that there is areservoir of the virus of herpes simplex in relationto the trigeminal territory somewhat on the linesoriginally advanced by Goodpasture, that the virusof herpes simplex may reside indefinitely in alatent form in some central or peripheral portionof the trigeminal nerve. It is possible that in avery small proportion of infested individuals theconsequence of such nidification of the virus, maybe Tic Douloureaux.A paper developed in association with Dr.
Simon Behrman and read to the Society ofBritish Neurological Surgeons at Leeds 1952.
REFERENCESI. BEHRMAN, S., and KNIGHT, G. C. (1954), Neurology,
4, 525.2. BEHRMAN, S., and KNIGHT, G. C. (I956), Ibid., 6, 363.3. CARTON, C. A., and KILBOURNE, Ed. (1952), New Engl.
J. Med., 172, 246.4. CUSHING, H. (I920), Amer. J. med. Sci., 157, i6o.5. EPSTEIN, L. (1948), Acta. psychiat. (Kbh.), I3, 23.6. FRIEDENWALD, J. S. (I923), Arch. Opthalmol., 52, I05.7. GOODPASTURE, E. W. (I929), Medicine, 8, 223.8. HARRIS, W. (I937), ' Facial Neuralgias,' Oxf. Univ. Press.9. LOVE, J. G., and SVIEN, H. J. (1954), J. Neurosurg., 11, 499.Io. RICHTER, R. J. (1944), Nerv. Ment. Dis., 99, 356.I. SHEIDEN, C. H., PUDENZ, R. H., FRESHWATER, D.,
and GIVE, G. L. (1958), J. Neurosurg., 12, 123.I2. SMITH, M. C. (i954), Proc. roy. Soc. Med., 47, 788.I3. STENDER, A. (I954), J. Neurosurg., I1, 333.I4. TAARNHOJ, C. (1952), Ibid., 9, 288.
References from page 443, The Problem of the Aged AmputeeREFERENCES
I. 'Old Age in the Modem World,' published by E. & S. Living-stone, I955. 'The Management of the Elderly DoubleAmputee,' Warren, pp. 562-570.
2. Shuffle Board as described in the Brit, med. J., No. 4936, p. 432,August i3, I955,
3. Bed-end Exercises as described in 'Care of the Hemipleg:cPatient,' Med. Press, May 5, 1958, Vol. CCXIX, No. 5687.
4. Four-legged Sticks as described in 'Physical Agents ' in 'TheTreatment of Chronic Patients ' under paragraph 'MedicalAids,' Medical Annual, 1955, p. 30I,
copyright. on 17 June 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.383.436 on 1 Septem
ber 1957. Dow
nloaded from