Embed Size (px)
Citation preview

World Development Vol. 39, No. 6, pp. 1002–1025, 2011� 2011 Elsevier Ltd. All rights reserved
0305-750X/$ - see front matter
www.elsevier.com/locate/worlddevdoi:10.1016/j.worlddev.2010.01.003
Pro-equity Effects of Ancillary Benefits of Climate Change Policies:
A Case Study of Human Health Impacts of Outdoor
Air Pollution in New Delhi
AMIT GARG *
Indian Institute of Management Ahmedabad, India
Summary. — This paper looks at the human health impacts from urban air pollution in India. Such pollution is especially harmful topoor people, so the co-benefits from global climate change policies in terms of reduced local air pollution can have positive equity im-pacts. Health impacts (mortality and morbidity) of PM10 pollution are quantified for different socio-economic groups in Delhi. The spa-tial PM10 concentration levels are overlaid with spatial socio-economic data. Improvement in air quality would result in bigger healthbenefits for the poor. Most measures that reduce PM10 pollutants also reduce CO2 emissions while simultaneously imposing more costson the better-off.� 2011 Elsevier Ltd. All rights reserved.
Key words — human health impacts, particulate emissions, CO2 mitigation, ancillary benefits, income, equity
*Final revision accepted: January 19, 2010.
1. INTRODUCTION
Global climate change policies on reducing GHG emissionin urban transportation can result in reduced health impacts.A number of international and country studies have estimatedthese benefits and have concluded that in many developingcountries local air pollution reduction benefits are large com-pared to mitigation costs. The benefits might even be greaterthan previously assessed if the health status of the peoplewho are exposed to local air pollution is taken into consider-ation. If people who are living in urban area with high pollu-tion loads are relatively poor, they are also expected to sufferrelatively more from bad health, and improvements in airquality could be particularly beneficial for this group. The pa-per analyzes whether climate change policies impose biggercosts on the rich for GHG emission mitigation while providingmore benefits to the poor through reduced local pollutantemissions.
Local air quality has been an issue of social concern be-cause of rising industrial and vehicular pollution in most In-dian cities and urban areas. The national capital Delhi is noexception. Fossil fuel combustion, especially in the roadtransport sector, is the main contributor of these emissions.Exposure to these pollutants causes health impacts, alsocalled the Burden of Disease (BOD), which can be estimatedin terms of mortality (premature deaths) and morbidity (sick-ness and lower activity levels). Do different income groupshave similar health risks owing to local air pollution or dothe poor bear a disproportionately higher burden of diseases?Does income inequality play a role in people’s vulnerabilityto air pollution related health impacts? Do polluters pay?Do the policies that reduce greenhouse gas emissions, espe-cially in the transport sector, also reduce local air pollutants,especially particulate emissions? What is the cost of such pol-icies implemented in Delhi and who bears the major costs?Have policies and measures to reduce pollution levels beeneffective in Delhi? What is the likely benefit distributionacross income groups if pollution levels are brought downwithin permitted limits in Delhi? We try to address someof these issues in this paper.
1002
We chose PM10 as the most damaging air pollutant for hu-man health impact assessment. 1 The official daily concentra-tion data from seven monitoring locations in Delhi havebeen used to map PM10 concentration levels during 2000–07.The census data for 27 tehsils in Delhi (sub-districts) providedthe geographical spread by income groups. The two GISdistributions were superimposed to study the inter-linkagesbetween PM10 concentrations and income-wise populationdistribution.
The National Family Health survey data for Delhi wereused to estimate mortality and morbidity incidences on vari-ous income groups. These, in conjunction with concentra-tion–response functions, were then for burden of diseaseestimates due to ambient PM10 concentration on differentincome groups. The avoided annual health costs (or likelybenefits) were estimated for each income group. The costs ofvarious measures to reduce the emissions in Delhi over the last10-years were also estimated. These results are then analyzedto answer the questions posed earlier.
2. HEALTH RISKS AND INCOME INEQUALITY
Exposure of different income groups to outdoor air pollu-tion in Indian cities 2 is not well studied mainly because oflarge gaps in data (World Bank, 2002a). These include insuffi-cient locations for monitoring ambient PM10 concentrationlevels, no PM2.5 monitoring, no concentration–response func-tions for Indian populations, lack of studies to identify pollu-tion sources and assess effects on public health, and lack ofstudies on morbidity treatment and costs for different incomegroups. However, data improvement is not the focus of thepresent study. We use available data to estimate the impactof outdoor PM10 pollution on populations. However, theimportance of strengthening data collection, management,and dissemination cannot be overemphasized.

HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1003
In attempting to reduce risks to health and, in particular, toredress the imbalance that leaves the poor and the disadvan-taged with the greatest burden of disease, the first steps areto quantify health risks and to assess the distribution of riskfactors by poverty levels. In this study, we only consider theseailments that can be directly or indirectly attributed to out-door PM10 pollution.
The inequality in risk and prevalence of outdoor air pollu-tion related health impacts on urban and rural populationsare estimated from the second National Family Health Survey(NFHS-2) data for Delhi. 3 This survey, conducted during1998–99, provides information on fertility, mortality, familyplanning, and important aspects of health, nutrition, healthcare, and prevalence of some diseases. NFHS-2 provides prev-alence (and not incidence) 4 of asthma, tuberculosis, jaundice,and malaria in household population by income group, age,sex, and residence (Table 1). In Delhi, NFHS-2 field staff col-lected information from 2763 households between 10 March1999 and 18 April 1999. NFHS-2 data report self- or respon-dent-perceived ailments. Disease prevalence should, therefore,be interpreted with caution since it does not indicate medicallycertified ailment conditions. Data reliability is also influencedby the answers provided by poor people who have lower edu-cation and knowledge. For them it may have been difficult toanswer the questionnaire NFHS-2 although facilitators aresupposed to explain the questions to each respondent. More-over the sample size was small for some income-age groupsin rural Delhi. Delhi has below 7% rural population and therisk values estimated from these should also be interpretedwith caution (Tables 4 and 5).
According to the Census of India (CoI) (2001), Delhi had apopulation of 13.78 million, with 55% males. Over 93% ofDelhi’s population is urban. The Indian official annual surveyfor consumption behavior of the population conducted by theNational Sample Survey Organization (NSSO) classifies theIndian population in 12 income categories based on monthlyper capita expenditure (MPCE) giving estimated cumulativepercentage frequency distribution of persons by MPCE forrural and urban separately (National Sample Survey Organi-zation (NSSO), 2001). For India, MPCE could be considereda proxy for standard of living in a household since it captures
Table 1. Sample size for the NFHS-2 Delhi survey, 1998–99
Standard ofliving
Total samplesize
Male age (years) Female age (years)
<15 15–59 60+ <15 15–59 60+
Urban
Low 855 170 264 24 149 222 26Medium 3,751 770 1,142 67 720 973 79High 9,331 1,422 3,026 413 1,249 2,890 331
Rural
Low 56 7 18 5 9 14 3Medium 477 105 130 12 97 122 11High 621 116 199 21 88 177 20
Source: NFHS-2 data.
Table 2. Details of standard of
Standard ofliving index
Score range All India% of householdsin urban area
Low 0–14 14.3Medium 15–24 45.2High 25–67 39.0Missing 1.5
Source: International Institute for Population Sciences (IIPS) (2000).
detailed household living expenses for almost all items of con-sumption. Moreover, reliable data on household income arenot readily available, while MPCE data are collected on an an-nual basis.
For the present study, we have used standard of living datafrom two NSSO studies/datasets (National Sample SurveyOrganization (NSSO), 2002; NSSO, 2001) and NFHS-2 data-base for disease prevalence in Delhi (NFHS-2 data). TheNSSO MPCE classifications are the same over its various re-ports (12 MPCE categories for urban and rural areas each),while NFHS-2 employs three standard of living categories;low, medium, and high (International Institute for PopulationSciences (IIPS), 2000). The standard of living index (SLI) iscalculated by adding scores for over a dozen indicators forhousing, water, electricity, water, and possession of land,household assets, goods, and appliances. 5
Table 2 provides details of the SLI ranges and percentage ofhouseholds falling under each SLI category in urban and ruralIndia separately. No monetary values or specific income levelsare provided for the NFHS-2 household categories. Therefore,no direct income based matching is possible between NFHS-2,which are index based, and MPCE classification, which has adirect monetary basis. However, percentage of households ineach category could provide a common ground for matching.We have, therefore, clubbed 12 MPCE classifications intothree income categories so that the percentage of householdsin the three clubbed categories is almost similar to the threeNFHS-2 categories (Table 3). This implies that for urbanhouseholds at all India level, the MPCE range for low stan-dard of living households becomes Indian rupees (INR) 0–425, medium INR 425–775, and high above INR 775. 6 Forrural areas these translate into low INR 0–420, mediumINR 420–775, and high above INR 775.
We also compared the low, medium, and high categorieswith the World bank classification of people living on less than1 US$ PPP/capita/day income, between 1 and 2 US$ PPP/ca-pita/day income, and above 2 US$ PPP/capita/day income inIndia for 1999–2000 for a consistency check. The World Bankpopulation cut-offs were 34.7% (up to US$ 1) and 79.9% (up toUS$ 2) of the total national population (WDR, 2005). 7 Inter-estingly these are very close to NFHS-2 national cut-offs of36.3% and 80.6%.
The all India low, medium, and high cut-offs are used formerging Delhi’s 12 MPCE classifications into three categories(low, medium, and high). Delhi household average income dis-tribution is on a higher side than the national average (Ta-ble 3). As such, only 5% urban households (1.3% rural) fallin low, 23.6% urban households (34.8% rural) fall in medium,and remaining 71.4% urban households (63.9% rural) fall inhigh category for the clubbed MPCE classification. Consider-ing 93% of Delhi households being urban (Census of India,2001), the weighted averages are 4.7% (low), 24.4% (medium),and 70.9% (high). These are using MPCE classification forDelhi. Using direct NFHS-2 survey samples (Table 1, column2) for Delhi, these percentages are 6%, 28%, and 66% respec-tively. These are very close and validate our methodology for
living categories in NFHS-2
All India% of householdsin rural area
All India overall%of households
44.7 36.344.0 44.310.3 18.21.0 1.2

Table 3. Details of household income classifications
MPCE categoriesas per NSSO data(Indian rupees)
All India number of householdsper 1000 households for
each MPCE category
All India cumulativenumber of householdsper 1000 households
Clubbed MPCE classificationequivalent NFHS-2SLI categories
Delhi number of householdsper 1000 households for
each MPCE category
Urban
0–300 52 52 Low 1300–350 50 102 Low 8350–425 96 198 Low 41425–500 101 299 Medium 40500–575 99 398 Medium 58575–665 100 498 Medium 66665–775 101 599 Medium 72775–915 100 699 High 134915–1120 100 799 High 1171120–1500 101 900 High 1521500–1925 50 950 High 1191925–more 50 1000 High 193
Rural
0–225 52 52 Low 0225–255 50 102 Low 0255–300 100 202 Low 0300–340 100 302 Low 0340–380 103 405 Low 7380–420 97 502 Low 6420–470 102 604 Medium 6470–525 93 697 Medium 41525–615 103 800 Medium 93615–775 99 899 Medium 208775–950 50 949 High 225950-more 50 999 High 415
Source: National Sample Survey Organization (NSSO) (2001, 2002), and NFHS-2 data.
Table 4. Deaths and attributed causes per 1000 population for urban areasin Delhi in 1999
Cause of death Standard of living
Low Medium High All Delhi
Not classifiable respiratorydisorders
0 0.09 0 0.02
Tuberculosis of lungs 0.84 0.62 0 0.19Asthma or allergic disorders ofrespiratory system
0.84 0.27 0.21 0.24
Heart attack (all types) 0.84 0.71 1.39 1.15Malignant neoplasm (cancer—alltypes)
0 0.44 0.43 0.41
Senility 0 0.44 0.82 0.67Not known 0.84 0.44 0.21 0.29All deaths (minus accidents andhomicides)
7.56 4.80 4.61 4.59
Source: NFHS-2 data.
1004 WORLD DEVELOPMENT
matching the MPCE and NFHS-2 income classifications usingall India number of households. We have used the latter per-centages to allocate district level population to income catego-ries.
Delhi has 9 districts and 27 sub-districts (tehsils). 8 Totalpopulation data are available for each of the 27 sub-districts(Census of India, 2001). Slum population data are also avail-able for the 9 districts and slum dwellers are considered to bein low SLI category for each district. 9 Each district populationis thus divided into low, medium, and high income categoriesbased on percentage shares as explained earlier. However, thelow income category is taken as either 6% of the district pop-ulation (equivalent to low cut-off) or the total slum populationin that district, whichever is higher. In the case of latter, theremaining district population is distributed into medium(32.6%) and high (67.4%) categories. 10 For each district there-after, the low, medium, and high population is distributed toits sub-districts in proportion to the total population of eachsub-district, assuming that there is no difference in incomeclassification of all the sub-districts of a particular district.Population has been thus allocated to low, medium, and highcategories in all the 27 sub-districts. There may be some over/under estimates in population distribution in the three incomecategories, especially between low and medium categoriessince some of the “up-market” slum population may be arguedto be falling under the medium income category in Delhi.However, since both are below US$ 2 PPP/capita/day, whichare distinctly different from the high income category, thesemarginal differences would not alter the findings. We haveused 2001 census data for the year 2000 analysis presentedin this paper assuming that the population distribution wouldnot have changed much in one year.
We estimate income related BOD estimates for acute respi-ratory infections (ARI), asthma, chronic obstructive pulmon-ary disease (COPD), ischemic heart disease, lung cancer, andtuberculosis from the NFHS-2 data. This survey is based oncohorts of people exposed to various air pollutants (includingPM10) for different periods of time, followed up for varyingperiods of time, with varying periods of time between exposurecessation and follow-up. The duration of exposure for thesampled population is not certain. These, however, cover agood sample size (Table 1) and provide linkages between theliving standard of a household and estimation of outdoor airpollution related mortality and morbidity for Delhi.

HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1005
Table 4 lists air pollution related-cause wise average annualdeaths per 1000 population and provides data on prevalenceof asthma, tuberculosis, jaundice, and malaria in householdpopulation by standard of living, age, and sex. Although itis inconclusive to attribute a proportion of these deaths di-rectly or indirectly to outdoor air pollution, recent studiesincluding combined efforts of scientists from several disci-plines, have raised serious concerns about the impact of airpollutants on human health (Bai, Khazaei, Stephan, & Laher,2007; Lewtas, 2007; Liaw, Ting, Kuo-Kang, & Yang 2008;Møller et al., 2008; Smith & Mehta, 2003). Environmental pol-lutants are rapidly being recognized as important and indepen-dent risk factors for several diseases, such as asthma, chronicobstructive pulmonary disease, lung cancer, atherosclerosis,ischemic heart disease, and stroke. 11
NFHS-2 has reported death data for the period January1996 to March/April 1999 which was averaged for annual esti-mation (Table 4). As discussed above, these causes could havehad direct or indirect attribution to air pollution (outdoorand/or indoor and/or active/passive smoking) or could alsohave had air pollution as one of the contributing factors toultimate death. In some cases air pollution could aggravatethe condition of the patient but may not be the primary cause.Data on smoking habits of the deceased were not, however,collected during the survey and, therefore, the risk estimatesreported should be interpreted with caution. 12 Moreover thesecauses are as indicated by the respondents and are not medi-cally certified.
Rural households have not reported deaths from the topthree causes. The mortality rates (minus accidents and homi-cides) per 1000 population for rural areas and all Delhi were3.47 and 4.59, respectively.
Table 6. Number of persons suffering from tuberculosis per 1000 population(separately for individual age groups and sex) in Delhi in 1999
Standard of living Male age (years) Female age (years)
<15 15–59 60+ <15 15–59 60+
Urban
Low 6 8 0 7 5 0Medium 1 16 60 3 13 13High 1 4 10 2 4 3
Rural
Low 0 0 0 0 0 0Medium 0 8 0 0 0 0High 0 0 0 0 0 0
Source: NFHS-2 data.
Table 5. Number of persons suffering from asthma per 1000 population(separately for individual age groups and sex) in Delhi in 1999
Standard of living Male age (years) Female age (years)
<15 15–59 60+ <15 15–59 60+
Urban
Low 6 27 83 7 9 77Medium 3 19 134 4 10 51High 1 10 56 2 12 39
Rural
Low 0 0 200 0 0 333Medium 0 8 83 0 8 91High 0 10 0 0 17 50
Source: NFHS-2 data.
The low and medium income urban households have consid-erably higher risks of suffering from asthma than those in thehigh income category (Table 5). This is true for rural areas aswell, except for the age group 15–59 years. But since only 7%of Delhi population is rural, the overall conclusions on asthmaprevalence in Delhi are dominated by the urban populationprofile. For the overall Delhi population, 18.82 people per1000 population in low income categories suffer from asthma.This number is 12.98 and 11.14 for medium and high incomecategories, respectively. We should also bear in mind thathealth consciousness and morbidity reporting increase with in-come (refer Section 5) and, therefore, the actual asthma riskscould be even much higher for the poor. Persons above60 years of age have 3–6 times higher risks than those in the15–59 age group. The elderly face higher risks since they aremore vulnerable to the health impacts of air pollution, andthey are often in poor health. These people would, therefore,be more fragile and susceptible to PM10 levels exceeding thethreshold levels during a day (refer Table 5). 13 They would,therefore, be beneficiaries of air pollution mitigation policies.
Tuberculosis repeats a similar story with the poor and med-ium income categories suffering much more than the rich inage groups below 60 years (Table 6). The medium income cat-egory has the highest prevalence in all age groups. The abnor-mally lower incidence in rural areas may cause from actual lowincidence rate, misreporting, or low sample size. The all Indiarural TB prevalence rate was 0.83 per 1000 population in1995–96 (National Sample Survey Organization (NSSO),1998).
3. EXTENT OF OUTDOOR AIR POLLUTION IN DELHI
Delhi is one of the mega cities of the world that experiencesserious photochemical pollution. The Delhi state (includingurban agglomerate and nearby rural areas) is highly populated(almost 14 million inhabitants) with a density of about10,000 persons/km2. Delhi has vehicular fleet of approxi-mately five million vehicles, three coal-based power plants,and many brick kilns on the city outskirts that are responsiblefor a major portion of the emissions, characterized by high ur-ban PM10, nitrogen oxides, hydrocarbons, and carbon monox-ide. Of course fossil fuel combustion also contributesconsiderable carbon emissions.
The Central Pollution Control Board of India (CPCB) reg-ularly monitors air quality of 92 cities/towns in India with re-spect to three criteria pollutants (sulfur dioxide, oxides ofnitrogen, respirable suspended particulate matter includingPM10). Besides this, additional parameters such as respirablelead and other toxic traces matters and polycyclic aromatichydrocarbons are also monitored in selected cities. Suspendedparticulates below ten-micron diameter (10�5 m), called PM10,are the most critical local pollutants since they travel deeperinto the respiratory tract and cause infections (Cohen et al.,2003; Holgate, Samet, Koren, & Maynard, 1999; World Bank,2002b). PM10 concentration is taken as the prevalence crite-rion for morbidity and mortality assessment owing to outdoorair pollution (World Health Organization (WHO), 2002).Automobile exhaust, combustion (fossil fuel and biomass),re-suspension of ambient dust, metallurgical processes, andsecondary sulfate and nitrate particles are the sources of thesesmaller particles. Particles below 2.5 micron are even moredamaging, but their ambient concentrations are not measuredin Indian cities as yet.
The National Ambient Air Quality Standards (NAAQS)for India are presented in Table 7. There are seven CPCB

Table 7. National ambient air quality standards (NAAQS) for India
Pollutants Time-weighted average Concentration in ambient air (lg/m3)
Industrial areas Residential, rural and other areas Sensitive areas
Sulfur dioxide (SO2) Annual averagea 80 60 1524 hb 120 80 30
Oxides of nitrogen as (NOx) Annual averagea 80 60 1524 hb 120 80 30
Suspended Particulate Matter (SPM) Annual averagea 360 140 7024 hb 500 200 100
Respirable Suspended Particulate Matter (RSPM) c Annual averagea 120 60 5024 hb 150 100 75
Source: Central Pollution Control Board (CPCB) (2008).a Annual arithmetic mean of minimum 104 measurements in a year taken twice a week 24 hourly at uniform interval.b 24 hourly/8 hourly values should be met 98% of the time in a year. However, 2% of the time it may exceed but not on two consecutive days.c Same as PM10.
1006 WORLD DEVELOPMENT
monitoring locations in Delhi; five of these are in residentialareas and two in industrial areas. Concentration levels ofPM10 have been 2–3 times higher than that considered danger-ous for public health since several years (Table 13 later inSection 7), whereas those of SO2 and NOx have remained wellwithin the standards. Low sulfur diesel, conversion of all pub-lic transport to CNG, and the gradual phasing out of oldervehicles have contributed to this. Exposure to elevated levelsof SO2 and NOx also results in higher hospital admissionsand emergency room visits, but these effects are small as com-pared to those of PM10 (Brandon & Hommann, 1995; Pandeyet al., 2005; World bank, 2003). We, therefore, discuss the hu-man health impact of PM10 alone.
Sameer (2004) has indicated that there is no single dominantsource of particulate emissions in Delhi; rather biomass com-bustion, road dust re-suspension, diesel combustion, andunidentified sources each contribute around 20% on averageannually. Various secondary particles (such as nitrates andsulfates) contribute 14%, coal 3%, and gasoline 4%. In addi-tion to sources of air pollution, meteorological parametersand seasons play an important role in influencing ambientair quality. Winter has the highest PM concentrations becauseof inversion layer effect, while monsoon season has the lowestas suspended particles settle down because of rain. High rain-fall and wind speeds reduce PM levels. Effect of land-use on airquality in Delhi is difficult to discern since land developmenthas a mixed pattern (World Bank, 2002c).
For sub-district level PM10 concentrations in Delhi, we haveused CPCB monthly air quality data on PM10 concentrationsat 7 monitoring stations for 2000–06. Annual PM10 emissionsand carbon dioxide (CO2) emissions, which are our own esti-mates (Garg & Shukla, 2002; Garg, Shukla, & Kapshe,2006; Garg, Shukla, & Menon-Chaudhury, 2007), the estima-tion methodology is given in Section 7.
4. POPULATION, INCOME, AND POLLUTION PRO-FILES
Slums are a major constituent of data on urban poverty.However, the slum population for Delhi could be under-reported. One factor responsible for under-estimation ofpoverty is that the category “slum” often excludes some ofthe poorest settlements, that is, squatters. The term “slum”has a wide range of meanings—squatter settlements, privatesub-divisions, traditional inner city quarters, urban villages,or any settlement which does not conform to state definednorms. In Delhi many poor groups are located in squatter
colonies, and the poorest of them have the most insecure ten-ure. Smaller and less established squatter settlements are oftennot covered. For instance, the more “temporary” settlementshousing workers in the construction industry (a very large em-ployer, with almost 100% being deprived poor families withhigh exposure to PM10 levels at worksites), may be missedout to some extent, if not completely. 14 Street and pavementdwellers who are without an ‘address’ (and being daily work-ers, are among the poorest) are also omitted in estimates ofurban poverty. These are also one of the highly exposedpopulation groups to outdoor air pollution. There are alsoneighborhoods on the urban periphery that have not beenlegalized, especially in mega cities like Delhi that are witness-ing rapid urbanization and outward expansion. Therefore,accounting for un-declared slums and further disaggregationof data is likely to result in higher estimates of urban poverty.The percentage of poor could, therefore, be higher than theofficially reported estimates—and that too in the categoriesmost exposed to outdoor air pollution.
Urban poverty conditions are more extensive and possiblyworse than is indicated by MPCE estimates since these donot capture municipal dimensions, such as actual access towater, sanitation, and hygienic surroundings by poor groups.Even in cities like Delhi with 100% coverage, per capita wateravailability could vary 10 times between low and high incomelocalities. Urban poverty and urban disparities in access to ba-sic services are issues that have a bearing on general health ofthe poor, even though the urban population as a whole is bet-ter off in many respects compared to rural areas. Poorer gen-eral health could make poor people more vulnerable toadverse impacts of outdoor air pollution.
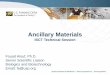
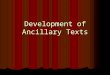
The annual 24-hourly average PM10 concentration levelsfrom seven CPCB monitoring stations have been used to con-struct a sub-district level PM10 concentration grid for Delhiusing GIS-based interpolation technique and knowledge aboutlocal topology. 15 The 7 monitoring stations are located in 6sub-districts (Figure 1b). This leaves some areas of Delhi, suchas west and north-west districts, unmonitored. Seven monitor-ing stations are possibly inadequate to represent actual ambi-ent PM10 concentration levels in all the 27 sub-districts ofDelhi spread over 1,483 km2. This is corroborated by theGIS-based interpolation techniques using the 7 locations alonewhich projected much lower PM10 levels in west and north-west Delhi districts compared to other parts (Figure 1). Thisis unrealistic considering absence of monitoring stations inthese districts, Delhi’s geography and topology, trafficpatterns and general understanding of pollution levels allover Delhi. Therefore, 6 dummy monitoring locations were

SN Sub-district name District name SN Sub-district name District name1 Chanakyapuri New Delhi 16 Hauz Khas South Delhi 2 Parliament Street New Delhi 17 Kalkaji South Delhi 3 Connaught Place New Delhi 18 Defence Colony South Delhi 4 Karolbagh Central Delhi 19 Vasant Vihar South-West Delhi 5 PaharGanj Central Delhi 20 Najafgarh South-West Delhi 6 Daryaganj Central Delhi 21 Delhi Cantonment South-West Delhi 7 Kotwali North Delhi 22 Punjabibagh West Delhi 8 Sadarbazar North Delhi 23 Patelnagar (East)* West Delhi 9 Civil Lines North Delhi 24 Patelnagar (West)* West Delhi 10 Seelampur North-East Delhi 25 Rajouri Garden West Delhi 11 Shahdara North-East Delhi 26 Saraswati Vihar North-West Delhi 12 Seemapur North-East Delhi 27 Narela North-West Delhi 13 Preet Vihar East Delhi 28 Model Town North-West Delhi 14 Gandhinagar East Delhi 15 Vivek Vihar East Delhi
* Patel Nagar (East) and Patel Nagar (West), which are item number 23 and 24 respectively as above, have been combined and taken as one sub-district for the purpose of this study.
Sub-District Boundary
District Boundary
LegendTotal Population (Thousand Persons)
Up to 50
50 - 100
100 - 150
150 - 250
250 - 400
400 - 650
More than 650
27
20
26
16
19
9
22
17
18
21
10
13
1
24
28
6
23
25
12
151423
4
11
58 7
Figure 1a. Delhi map showing districts, sub-districts, and year 2000-level population profiles. Data source: Central Pollution Control Board (CPCB) (2008).
HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1007
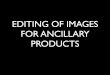
included in the GIS to create average annual PM10 concentra-tion profile for all the 27 sub-districts (Figure 2). Concentra-tion levels in these dummy monitoring stations were takento be equal to the average of annual PM10 concentration levelsat existing monitoring stations (Figure 2). 16 This GIS-interpo-lation may not be a perfect representation of the reality, but inour opinion, may not be too far off.
Table 8 provides details of population and PM10 concen-tration levels in various sub-districts in 2000. No sub-district had annual average PM10 concentrations within
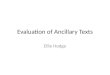
NAAQS. The cleanest levels were just below 120 lg/m3.The income level population profile of Delhi is mappedin Figures 3–5 for low, medium, and high income catego-ries. Overlaying these income level population profiles withpollution profile provides some interesting observations. Allpeople residing at a location are assumed to be exposed toambient PM10 concentrations. The exposure is based onpeople residing at a location and does not consider eithertheir commuting to other areas or floating population in/out of Delhi.

!
!
!
!
!
!!
27
20
26
16
19
9
22
17
18
21
10
13
1
24
28
6
2 3
25
12
1514234
11
58 7
ITO
Siri Fort
Janakpuri
Nizamuddin
Ashok Vihar
Shahadara (I)Shehzada Bagh (I)
CPCB Monitoring Station
Sub-District Boundary
District Boundary
Legend: Annual average PM10 concentration level (µg/m3)
> 60 61 - 120 121 - 145 146 - 165 166 - 185 186 - 205 > 205
Figure 1b. Sub-regional PM10 concentration profile of Delhi in 2000 using GIS-based interpolation technique using 7 CPCB monitoring stations alone. Data
source: Central Pollution Control Board (CPCB) (2008). Note: CPCB monitoring stations are located at Janak Puri (R), Siri Fort (R), Nizamuddin (R),
ITO (R), Ashok Vihar (R), Shahdra (I), and Shahzada Bagh (I), where R indicates residential area and I indicates industrial area.
1008 WORLD DEVELOPMENT
1. About 74% of population in the low income group isexposed to annual 24-hourly average PM10 concentrationlevels above 150 lg/m3, compared to only about 58% eachin the medium and high income categories. The safe levelstandards for residential areas are up to 60 lg/m3 (India).2. More population in the low income group is exposed tovery high PM10 concentration levels (above 180 lg/m3) incertain sub-districts (e.g., Daryaganj and Paharganj).About two-thirds of the time in a year, these levels exceedthe safe NAAQS limits.3. North Delhi and Central Delhi districts have very highpopulation in the low income category (over 400,000 each),and, respectively, 52% and 71% of the population of thesetwo districts reside in slums. These districts had PM10
concentration levels around 170–180 lg/m3 in 2000. Theconcentrations exceeded the safe NAAQS limits around60% of the time for North Delhi and 80% of the time forCentral Delhi. This indicates that the poor are exposedmore to higher air pollution levels.4. New Delhi district, which is the seat of the government ofIndia, has the distinction of having the highest PM10 levels(around 180–190 lg/m3). This district, however, does nothave much residential population because of higher shareof offices and business complexes. Moreover only 20%people residing in this district are in the low income category,26% are in the medium income, and 54% are in the highincome category. Two of its three sub-districts—ConnaughtPlace and Parliament Street—have considerable business
establishments. However, the population commuting toand through this district for work/business daily could bemuch higher than the residential population of thedistrict, and is more likely to be in the medium and highincome categories, although a fair estimate of the incomedistribution of this commuting population is not available.Therefore, the daily population exposed to the highPM10 levels for different intervals of time could be muchhigher. 17
5. There are 165 children (in the age group of 0–6 years)per 1000 population in the slum areas, while in other areasthere are 134 children. The Delhi average for all incomecategories is 140. Among the highly polluted areas (PM10
levels around 170–190 lg/m3), the Central, North, andNew Delhi districts have, respectively, 80%, 58%, and35% of children in the age group of 0–6 years living inslums. This indicates that more children in the low incomegroup are exposed to higher pollution than the medium andhigh income counterparts.6. The relatively affluent residential localities in the Southand Southwest Delhi districts have a relatively lowerannual average PM10 concentration levels of around 120–140 lg/m3. These districts together had only 9% people liv-ing in slums and only about 15% people living below 1 US$PPP/capita/day income, much below those of the less efflu-ent North and Central Delhi districts.7. The medium and high income population groups tend toreside away from the more polluted central areas of Delhi.

!
!
!
!
!
!!
!
!
!
!
!
!
27
20
26
16
19
9
22
17
18
21
10
13
1
24
28
6
2 3
25
12
1514234
11
58 7
ITO
Siri Fort
Janakpuri
Nizamuddin
Ashok Vihar
Shahadara (I)Shehzada Bagh (I)
CPCB / Dummy Monitoring Station
Sub-District Boundary
District Boundary
Legend: Annual average PM10 concentration level (µg/m3)
> 60 61 - 120 121 - 145 146 - 165 166 - 185 186 - 205 > 205
Figure 2. Sub-regional PM10 concentration profile of Delhi in 2000 using 7 existing and 6 dummy monitoring locations through GIS-based interpolation
technique. Data source: Central Pollution Control Board (CPCB) (2008).
HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1009
8. If literacy level is taken as one of the indicators ofawareness about pollution related health impacts, it isway below in slum and low income categories than in othercategories. The literacy level in Delhi slum areas was 56%while in other areas it was 73% in 2001. For females in slumareas, it was much lower at 48%.
Figure 6 plots the weighted average income for each of the27 sub-districts against their respective annual average PM10
concentration levels for years 2000 and 2005. Areas with loweraverage income have higher PM10 concentration levels. Theconcentration levels have decreased in 2005, with ConnaughtPlace and Daryaganj being the two exceptions where the levelshave gone up, mainly because of increased traffic and con-struction activities.
5. INCOME INEQUALITY AND GENERAL HEALTH
The general health status of the low income groups is poorcompared to that of the medium and high income groups. Thiscould mean that even a lower exposure to outdoor air pollu-tion could increase their chances of having an adverse healthimpact. And if the poor are exposed to higher levels ofPM10 concentrations, as appears to be the case in Delhi, theycould bear disproportionately higher risks of adverse healthimpacts because of outdoor air pollution than their rich coun-terparts.
The general health status of a population is exploredthrough the following three evidences for various income cat-egories:
(1) linking infant mortality rate (IMR) with monthly percapita expenditure (MPCE);(2) incidence of fevers of short duration for population liv-ing in different environments;(3) morbidity reporting and level of living.
Infant mortality rate is a well-accepted indicator for the gen-eral health of population and health care services available tothem. Linking infant mortality rate with monthly per capitaexpenditure (MPCE) indicates that households with lowMPCE have a higher infant mortality rate in India (Figure 7).IMR reduces with increased MPCE and the average IMR forlow, medium, and high MPCE classes is around 80, 60, and 40per 1000 at all India level. Urban areas have a lower IMRsince they have a higher MPCE than rural areas.
Another interesting evidence that low income groups havepoorer general health is the incidence of fevers of short dura-tion for population living in different environments. People liv-ing in dirtier surroundings, such as in the vicinity of animalsheds and having no or open drainage arrangements, reportmore fevers of short duration compared to people living incleaner surroundings in urban India (Table 9). Low incomehouseholds and slum areas have dirtier surroundings thanmedium and higher income localities. Rural areas do notshow any difference in incidence of fever because of living

Table 8. Population and concentration profile in various sub-districts
Districts Sub-districts Population in various income categories(thousands)
Annual average PM10
concentration (lg/m3)
Low Medium High Year 2000
NW Delhi Saraswati Vihar 199 523 1081 151Narela 55 145 301 151Model Town 62 162 334 173
North Delhi Civil Lines 275 82 169 173Sadarbazar 70 21 43 173Kotwali 64 19 39 173
NE Delhi Seelam Pur 55 257 607 170Shahdara 19 89 210 170Seema Pur 32 148 349 170
East Delhi Gandhinagar 29 111 229 171Vivek Vihar 16 63 131 170Preet Vihar 69 266 550 170
Central Delhi Daryaganj 218 29 61 186Paharganj 140 19 39 182Karolbagh 99 13 28 176
New Delhi Connaught Place 9 12 24 191Parliament Street 12 15 32 180Chanakyapuri 15 20 41 180
South Delhi Defence Colony 68 177 365 166Kalkaji 70 181 374 144Hauz Khas 115 299 618 122
SW Delhi Delhi Cantonment 18 86 203 122Vasant Vihar 32 150 354 122Najafgarh 55 255 601 141
West Delhi Rajouri Garden 55 135 280 143Punjabibagh 69 171 354 143Patel Nagar 124 307 634 143
1010 WORLD DEVELOPMENT
environments. This may be due to lower variations in sur-roundings among households with wider prevalence of animalsheds and lower share of cemented or underground drainagefacilities.
The last evidence explored is through linking morbidityreporting with MPCE, which reveals a positive association be-tween the two (Figure 8). Morbidity rates are estimated basedon a country-wide survey on prevalence of morbidity, measuredas the number of persons reporting ailment during 15 days per1000 persons (National Sample Survey Organization (NSSO),1998). 18 If MPCE is considered a proxy for level of livingin households, the data appear to show that the level of morbid-ity tends to rise with the level of living. This may either meanthat the poor are less prone to sickness than the rich, or thatreporting of morbidity improves with improvement in thestandard of living. The first hypothesis may be contrary to thepoorer health care indicators for low income groups, such asinfant mortality rates, expectation of life at birth, and mortalityrates at other ages. In general, health care facilities are alsopoorer and less available to the poor. However, a likely explana-tion could be the higher health consciousness in higher incomecategories, leading to higher illness reporting. Also in light ofthe evidence of a negative correlation between IMR and MPCEand higher incidence of fever of short duration in households indirtier surroundings, the second hypothesis seems to be moreplausible. This indicates rising health consciousness as incomesrise. 19
6. POOR GAIN MORE DUE TO IMPROVEMENT INAMBIENT AIR QUALITY
We analyze the health costs avoided 20 to the three incomegroups if the year 2000 PM10 concentration levels are broughtdown to 60 lg/m3 throughout Delhi, which is the NAAQS forresidential areas. The health impacts covered include changesin premature mortality, chronic bronchitis in adults, respira-tory hospital admissions, cardiac hospital admissions, emer-gency room visits, asthma symptom days, restricted activitydays, days with acute respiratory symptoms, and acute bron-chitis in children below 15 years of age (Table 10). We haveused concentration–response (C–R) functions estimated fordeveloped countries since no better estimates are yet availablefor India (Table 11). These could result in an underestimationof the actual impact of local air pollution in Delhi since PM10
concentration levels have remained appreciably and consis-tently high in Delhi compared to the places where these C–Rfunctions have been derived, and also since the average healthstatus of an average person in Delhi could be below that indeveloped country cities. 21 The C–R functions have been ap-plied to the three income categories in each sub-district sepa-rately and then summed up to arrive at Delhi estimates. Thedisease incidence rates estimated for various income groupsin Delhi (Tables 4–6) and the population profiles have beenused to make the estimates Delhi-centric to the extent possible.There are specifically listed in column 3 of Table 11.

Sub-District Boundary
District Boundary
Legend
Total Population (Thousand Persons)
Up to 50
50 - 100
100 - 150
150 - 250
250 - 400
400 - 650
More than 650
Up to 50
50 - 100
100 - 150
150 - 250
27
20
26
16
19
9
22
17
18
21
10
13
1
24
28
6
23
25
12
151423
4
11
58 7
Figure 3. Sub-regional low income population distribution pattern in Delhi, 2000.
HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1011
The results in Table 10 indicate that low income populationgains maximum in terms of percentages of cases avoided foreach income category. For instance, low income populationis estimated to gain more by way of higher percentages ofavoided mortality cases between 0.077 and 0.271% of totalpopulation in the low income category compared to 0.044–0.156% in the medium income, and 0.043–0.149% in the highincome category. Similarly avoided new cases of chronic bron-chitis in adults are 1.146% (low income), 0.744% (medium),and 0.638% (high income) of the respective low, medium,and high income total population. This income level differen-tiation in avoided morbidity is most pronounced for avoidedacute bronchitis in children below 15 years of age. It is1.655% for the low income category, while for the medium in-come category it is 0.362% and for the high income category itis 0.239%. It is evident that higher percentage of poor wouldbenefit from air quality improvement in Delhi, the reasonsbeing their higher susceptibility to respiratory diseases andhigher exposure levels.
The monetary implications of these health benefits are esti-mated based on per case health cost valuation for India by aWorld Bank study (Brandon & Hommann, 1995). This studyassumes for valuation of mortality that these individualswould have lived an additional 10 years. The lower estimateof VSL uses a human capital approach, and values one statis-tical life as equal to the discounted value of a 10-year wagestream. Brandon and Hommann have taken the average In-dian daily wage as US$ 1.93 with average 250 days/year.The Indian VSL estimate thus works out to US$ 4208 per life.If we apply average MPCE for low, medium, and high incomecategories for Delhi based on Table 3 data and work out the
10-year discounted value of annual MPCE for each incomecategory, the respective VSL estimates are US$ 1167 (low),US$ 1890 (medium), and US$ 5107 (high). 22 Their weightedaverage works out to US$ 4380 per life, which is quite closeto the Brandon and Hommann value for average Indian life.
Brandon and Hommann have based their higher cost esti-mates per premature mortality based on hedonic wage andcontingent valuation statistics conducted in the United States.They have used US$ 300,000 per life for USA. This figure isdiscounted for India in the ratio of Indian and US per capitaGNPs, which works out to US$ 40,017 per case for India. Forour study, however, we have used US$ 9000 per life as thehigher cost estimate. 23 The higher per case estimates are ap-plied uniformly to the three income categories (Table 12),which may not represent a realistic assumption especially forthe mortality costs per case. A more realistic valuation of mor-tality would also require consideration of willingness to pay(WTP) for each income category separately. However, becauseof absence of better information, these estimates have beenused.
Per case morbidity cost valuation is based on the WorldBank study (Brandon & Hommann, 1995) and are based onmedical treatment costs per case. These are taken as samefor all income categories. 24 However, to capture the socialcosts of morbidity from air pollution, the cost estimate shouldinclude medical treatment costs and loss of income arisingfrom morbidity impacts. To reflect the full welfare cost, thehuman costs from suffering should also be included. However,we have considered only direct medical treatment costs.
Annual health costs avoided due to reduced mortality(Table 12) are higher for high income groups than for low

Sub-District Boundary
District Boundary
Legend
Total Population (Thousand Persons)
Up to 50
50 - 100
100 - 150
150 - 250
250 - 400
400 - 650
More than 650
Up to 50
50 - 100
100 - 150
150 - 250
250 - 400
400 - 650
More than 650
27
20
26
16
19
9
22
17
18
21
10
13
1
24
28
6
23
25
12
151423
4
11
58 7
Figure 4. Sub-regional Medium income population distribution pattern in Delhi, 2000.
1012 WORLD DEVELOPMENT
income groups. But comparing Table 10 with Table 12, we seethat a higher percentage of poor would benefit from a decreasein PM10 concentration. Total avoided costs are lower for thepoor since their per case health costs are much lower thanfor the rich (column 2 in Table 12).
It is seen that the maximum health benefits from reducedPM10 concentrations are derived for restricted activity days(adults), followed by the number of days with acute respira-tory symptoms. Losses from these two account for almost90% of all avoided morbidity costs. The monetary valuationof these two health effects is comparable to mortality costs(lower per case cost estimates) for all income categories. Thisis an interesting result indicating that inhaling polluted aircould even cost almost equally in morbidity and mortalitylosses.
Since most of the poor and some of the medium income cat-egories are daily wage earners, they cannot afford to skip workwithout loss of earnings. Many of them may, therefore, beforced to work even with acute respiratory infections. Thiscould even put their co-workers at a higher risk of infection.A reduction in acute respiratory symptoms days would, there-fore, not only reduce monetary losses drastically but wouldalso result in a healthier work environment and increased effi-ciency of the labor force.
In case the current PM10 concentration levels in Delhi arebrought down to those in the cleanest large cities in theworld, 25 the health benefits would accrue more to the poorthan the rich (Table 14). Comparing Tables 10 and 14 wesee that avoided premature mortality (lower estimates) for
the poor is further reduced by 34% {(2.1 � 1.6)/1.6} whenPM10 concentration levels are brought down from 60 to25 lg/m3. The low income population is estimated to gainmore by way of higher increase in avoided mortality casesfrom 0.077% to 0.104% of the population in low income cate-gory where PM10 concentration levels are brought down,compared to gains of 0.044–0.061% (medium income), andof 0.043–0.059% (high income).
Annual health costs avoided by achieving PM10 concentra-tion levels of 25 lg/m3 are presented in Tables 15 and 16.For the low income category, the incremental savings betweenachieving PM10 concentration levels of 60 lg/m3 and 25 lg/m3 are US$ 0.7–17 million per year for mortality ranges(Tables 12 and 15) and US$ 2.2–3.4 million per year formorbidity (Tables 13 and 16). The values for the medium in-come category are US$ 1.2–20 million for mortality andUS$ 4.1–6.2 million per year for morbidity. The values forthe high income category are US$ 6.6–41 million for mortalityand US$ 8.7–13.4 million per year for morbidity. The cumula-tive savings arising from improved health for all categories areUS$ 23.5–101 million when PM10 concentration levels arebrought down to 25 lg/m3 throughout Delhi.
7. ANCILLARY BENEFITS OF GHG EMISSION MITI-GATION IN DELHI
When comparing the annual average PM10 concentrationsthroughout Delhi with the corresponding levels in 2006 over

Sub-District Boundary
District Boundary
Legend
Total Population (Thousand Persons)
Up to 50
50 - 100
100 - 150
150 - 250
250 - 400
400 - 650
More than 650
100 - 150
150 - 250
250 - 400
400 - 650
150 - 250
250 - 400
400 - 650
27
20
26
16
19
9
22
17
18
21
10
13
1
24
28
6
23
25
12
151423
4
11
58 7
Figure 5. Sub-regional High income population distribution pattern in Delhi, 2000.
-
50
100
150
200
250
300
– 0.50 1.00 1.50 2.00 2.50 3.00 3.50
Weighted average income for sub-districts (US$ PPP/capita/day)
Ann
ual a
vera
ge P
M10
con
c in
sub
-dis
tric
ts (
µg/m
3) 2000 2005
Figure 6. Weighted average income against annual average PM10 concentration in the 27 sub-districts of Delhi in 2000 and 2005.
HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1013
2000–05, the trend for reduction is stronger than that for in-crease until 2005 (Table 17). During 2005–06, there is an in-crease in PM10 levels in all the monitoring locations, exceptthe most polluted ITO crossing. The Delhi annual averagePM10 concentration has also increased from 140 lg/m3 in2005 to 158 lg/m3 in 2006.
If we analyze the public policies to mitigate various types ofemissions in Delhi over the last decade, the following wouldhave affected the PM10 concentration levels directly or indi-rectly:
1. Introduction of low sulfur diesel (from 1% max to 0.25%max sulfur by volume) during 1996–98.2. 1,160 industries closed or relocated during 1997–99including hot mix plants, arc induction furnaces, and brickkilns.3. Supply of only premix gasoline in all gasoline filling sta-tions to two-stroke engine vehicles; ban on supply of loose2T oils since 1998.4. Phasing out/ban on old commercial/transport vehicles(>15 year old) since 1998.

0
200
400
600
800
1000
1200
0 20 40 60 80 100 120
Infant Mortality Rate
Mon
thly
per
cap
ita
expe
ndit
ure
(Rs)
Rural Urban
Figure 7. Rural and urban infant mortality rates and MPCE in 15 major Indian states. Source: NSSO Report No. 441 (52/25.0/1) (1998).
Table 10. Estimated annual cases of mortality and morbidity prevented in different income groups (low, medium, high) if PM10 concentration levels in 2000were reduced to 60 lg/m3 through out Delhi
Health effect Annual cases prevented (thousands) % of respective income category population
Low incomegroup
Medium incomegroup
High incomegroup
Low incomegroup (%)
Medium incomegroup (%)
High incomegroup (%)
Premature mortality (lower mortality estimates) 1.6 1.7 3.4 0.077 0.044 0.043Premature mortality (Higher mortality estimates) 5.5 5.8 12.0 0.271 0.156 0.149Chronic bronchitis in adults (new cases) 23.4 27.9 51.3 1.146 0.744 0.638Respiratory hospital admissions 2.7 4.5 9.6 0.131 0.120 0.120Cardiac hospital admissions (daily) 0.0 0.1 0.1 0.408 0.264 0.226Emergency room visits (daily) 1.5 2.5 5.4Asthma symptoms days(moderate or worse asthma status)
8.3 9.9 18.2
Restricted activity days (adults) 1797 3029 6490Days with acute respiratory symptoms 19,016 31,629 67,760Acute bronchitis in children (0–15 years)a 12.6 5.1 7.2 1.655 0.362 0.239
a Percentage is of all children in age 0–15 years.
0
20
40
60
80
100
0-10 10 to 20 20-40 40-60 60-80 80-90 90-100
MPCE (%) fractile-groups
Mor
bidi
ty r
epor
ting
(pe
r 10
00 p
erso
ns
Rural Urban
Figure 8. Rural and urban morbidity reporting and level of living in India.
Source: NSSO Report No. 441 (52/25.0/1) (1998).
Table 9. Incidence of fevers of short duration for population living indifferent environments in urban India
Environment Number of ailments per 1000persons
Male Female Person
Animal sheds in the neighborhood
Attached to the residence 16 16 16Detached from the residence 19 19 19No animal shed 15 15 15
Household drainage system
No drainage 19 21 20Open clay-based drainage 16 14 15Open cemented drainage 14 15 15Covered cemented drainage 12 13 12Underground drainage 15 14 14
Source: NSSO Report No. 441 (52/25.0/1) (1998).
1014 WORLD DEVELOPMENT
5. Introduction of Euro I equivalent fuel emission normsfor all private non-commercial road vehicles from 2000,and Euro II from 2005.
6. Introduction of low sulfur gasoline (from 0.2% max to0.05% max sulfur by volume) during 2000.

Table 11. Concentration–response functions and Delhi specific values used
ealth endpoint C–R function Delhi specific values, where ever used Source of C-R function
hange in premature mortality D Premature mortality = P � Ba � DPMa � POP whereP = percentage effect (�1/100) of mortality rate per lg/m3
of PM10 Ba = baseline annual mortality rate (minusaccidents and homicides) for different income groups inDelhi DPMa = change in annual average PM10
concentration POP = population exposed to DPMa
1. Lower estimates of P are derived from a 1% in-crease in mortality per 10 lg/m3 of PM10 increasebased on acute exposure studies, and higher esti-mates of a 3.5% increase in mortality per 10 lg/m3 of PM10 increase based on chronic exposurestudies. The latter likely includes the effects ofboth chronic and acute exposures2. Ba is analyzed from NFHS-2 data for Delhi as7.56, 4.8, and 4.6 per 1000 population for low,medium, and high income categories, respectively
Ostro and Chestnut (1998)
hronic bronchitis in adults DChronic bronchitis = �[y0 � (e �b � DPM10 � 1)] �POP where y0 = annual bronchitis incidence rate perperson (for different income categories) b = estimatedPM10 logistic regression coefficient = 0.00932DPM10 = change in annual average PM10 concentrationPOP = population ages 27 and older “without chronicbronchitis”
y0 is analyzed from NFHS-2 data for Delhi as0.01882, 0.01298, and 0.01114 per 1000population for low, medium, and high incomecategories, respectively
Abbey, Petersen, Mills, and Beeson (1993)Location: California, United StatesOther pollutants in model: NoneComments: Used TSP to measure PM. The TSPcoefficient is applied to changes in PM10
espiratory hospital admissions DAll respiratory daily hospital admissions ¼�½y0 � ðe�b�DPM2:5–10 � 1Þ� � POP where y0 = daily hospitaladmission rate for all respiratory per person = 2.58E�5b = PM2.5–10 coefficient = 0.00147 DPM2.5–10 = changein daily average PM2.5–10 concentrationPOP = population of all ages
The daily estimation is multiplied by 365 days forannual estimation
Burnett et al. (1995) Location: Toronto, CanadaOther pollutants in model: O3, NO2, SO2
ardiac hospital admissionsdaily)
DCardiac hospital admissions ¼ �½y0 � ðe�b�DPM2:5–10 � 1Þ��POP where y0 = daily hospital admission rate for cardiacper person = 3.81E�5, b = PM2.5–10
coefficient = 0.00704, DPM2.5–10 = change in dailyaverage, PM2.5–10 concentration, POP = population of allages
Since daily data were not available for all theseven CPCB locations, annual average levels havebeen used for daily PM2.5–10 concentrations. Acheck on daily and annual PM10 concentrationCPCB data for ITO indicates that this is areasonable assumption for Delhi
Burnett et al. (1995)Location: Toronto, CanadaOther pollutants in model: CO, O3
mergency room visits DChronic bronchitis ¼ �½y0 � ðe�b�DPM10 � 1Þ� � POP wherey0 = daily ER visits for asthma per person under 65 yearsold = 7.69, E�6, b = PM10 coefficient = 0.00367,DPM10 = change in daily average PM10 concentration,POP = population ages 0–64 years
1. Since daily data were not available for all theseven CPCB locations, annual average levels havebeen used for DPM10 concentrations. A check ondaily and annual PM10 concentration data forITO indicates that this is a reasonable assumption2. Population up to 64 years for Delhi is taken asthe national average of 95% of total population(Census of India, 2001)
Schwartz, Slater, Larson, Pierson, and Koenig(1993)Location: Seattle, United States
Other pollutants in model: None
sthma symptoms daysmoderate or worse asthmatatus)
DDays moderate=Worse asthma ¼�b � ln½PM2:5; after=PM2:5;before� � POP whereb = estimated PM2.5 concentration for year, i = 0.0006,PM2.5 = change in daily average, PM2.5 concentrationPOP = asthmatic population of all ages
Asthmatic population of all ages is analyzed fromNFHS-2 data for Delhi as 1.882%, 1.298%, and1.114% of the population of all ages for low,medium, and high income categories, respectively
Ostro, Lipsett, Wiener, and Selner (1991)Location: Denver, United StatesOther pollutants in model: NoneComments: The study estimated 5.61% asasthmatic population of all ages
(continued on next page)
HU
MA
NH
EA
LT
HIM
PA
CT
SO
FO
UT
DO
OR
AIR
PO
LL
UT
ION
INN
EW
DE
LH
I1015
H
C
C
R
C(
E
A(s

Table 11—Continued
Health endpoint C–R function Delhi specific values, where ever used Source of C-R function
Restricted activity days (RAD) DRAD ¼ �½y0 � ðe�b�DPM2 :5 � 1Þ� � POP where y0 = dailyRAD incidence rate per person = 0.0177, b = inverse-variance weighted, PM2.5 coefficient = 0.00475,DPM2.5 = change in daily average PM2.5 concentrationPOP = adult population ages 18–65 years
1. The daily estimation is multiplied by 365 daysfor annual estimation2. Since daily data were not available for all theseven CPCB locations, annual average levels havebeen used for DPM2.5–10 concentrations. A checkon daily and annual PM10 concentration datafor ITO indicates that this is a reasonable assump-tion3. PM2.5 is taken as 60% of PM10 concentration4. Adult population between 18 and 65 years forDelhi is taken as the national average of 54% oftotal population (Census of India, 2001)
Ostro (1987)Location: US metropolitan areasOther pollutants in model: None
Acute respiratory symptoms(presence of any of 19 acuterespiratory symptoms)
DARS ¼ bPM10 � DPM10 � POP where b = first derivative ofthe stationary probability = 0.000461, DPM10 = changein daily average, PM10 concentration, POP = populationages 18–65 years
1. Adult population between 18 and 65 years forDelhi is taken as the national average of 54% oftotal population (Census of India, 2001)2. The daily estimation is multiplied by 365 daysfor annual estimation
Krupnick, Harrington, and Ostro (1990)Location: Glendora-Covina-Azusa, CA, UnitedStatesOther pollutants in model: O3, SO2
Acute bronchitis in children DAcute bronchitis ¼ �½fy0=ðð1� y0ÞðeDPM2:5 �bþy0ÞÞg � y0��POP where y0 = annual bronchitis incidence rate perperson (for different income categories), b = estimatedPM2.5 logistic regression coefficient = 0.0272DPM2.5 = change in annual average PM2.5 concentration,POP = population ages 8–12 years
1. y0 is analyzed from NFHS-2 data for Delhi as0.0207, 0.0047, and 0.0031 for low, medium, andhigh income categories, respectively2. PM2.5 is taken as 60% of PM10 concentration3. Acute bronchitis is estimated for populationaged up to 15 years. 37.3% of total population isin this age group in India (Census of India,2001) and the same average is assumed to applyfor Delhi as well
Dockery et al. (1996)Location: 24 US and Canadian cities
Other pollutants in model: None
1016W
OR
LD
DE
VE
LO
PM
EN
T

Tab
I
LLMMHHT
# B
Tab
H
PPCRCEA(RDA
a Pe
Ta
H
CRCEARDAT
a B
HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1017
7. Buses more than 8 years phased out or to ply on com-pressed natural gas (CNG) since 2000.8. Three coal-based power plants to switch over to benefi-ciated coal.9. Supply of piped natural gas started since 2000 to a fewspecific domestic, small, and large commercialestablishments.10. Introduction of very low sulfur diesel (from 0.25% maxto 0.05% max sulfur by volume) during 2001.
le 12. Estimated annual costs avoided due to prevented deaths for different incomreduced to 60 lg/m3 thro
ncome categories Per case health2
Lower costestimates
ow income (lower mortality estimates) 1,167ow income (higher mortality estimates) 1,167edium income (lower mortality estimates) 1,890edium income (higher mortality estimates) 1,890igh income (lower mortality estimates) 5,107igh income (higher mortality estimates) 5,107otal mortality costs avoided (US$ million)
ased on Brandon and Hommann (1995).
le 14. Estimated annual cases of mortality and morbidity avoided in different incoreduced to 25 lg/m3 (equivalent to 15 lg/m
ealth effect Annual cases prevented (th
Low incomegroup
Medium incomegroup
remature mortality (lower estimates) 2.1 2.3remature mortality (higher estimates) 7.4 8.1hronic bronchitis in adults (new cases) 27.6 33.7espiratory hospital admissions 3.5 6.0ardiac hospital admissions (daily) 0.0 0.1mergency room visits (daily) 2.0 3.5sthma symptoms days
moderate or worse asthma status)15.7 19.2
estricted activity days (adults) 2303.2 3985.2ays with acute respiratory symptoms 25514.0 43570.1cute bronchitis in children (0–15 years)a 14.0 5.7
rcentage is of all children in age 0–15 years.
ble 13. Estimated annual morbidity costs avoided for different income groups (lo60 lg/m3 through o
ealth effect Per case health costestimates (US$, 2001)a
Ann
cat
Lower costestimates
Higher costestimates
Low
hronic bronchitis in adults (new cases) 2.52 6.31espiratory hospital admissions 121 301ardiac hospital admissions (daily) 542 1354mergency room visits (daily) 3.40 8.50sthma symptom days 0.57 1.42estricted activity days (adults) 2.77 2.77ays with acute respiratory symptoms 0.10 0.26cute bronchitis in children (0–15 years) 0.10 0.26otal morbidity costs avoided (US$ million)
ased on Brandon and Hommann (1995).
11. Phasing out of old (and thus inefficient) three-wheelerssince 2001.12. Gradual reduction in aggregate technical and commer-cial (AT&C) losses for electricity distribution in Delhi since2002.13. Conversion of all diesel-driven public road transport toCNG completed during 2000–03.14. Gradual introduction of metro rail transport in somecongested areas since 2002.
e groups (low, medium, high) if PM10 concentration levels in 2000 wereugh out Delhi
cost estimates (US$,001)#
Annual health costs avoided(US$ million, 2001)(higher per case cost
estimates)Higher cost
estimates
9,000 1.8 149,000 6.5 509,000 3.2 159,000 11.1 539,000 17.5 319,000 61.3 108
23–79 60–211
me groups (low, medium, high) if PM10 concentration levels in 2000 were3 for PM2.5) throughout Delhi
ousands) % of respective income category population
High incomegroup
Low incomegroup (%)
Medium incomegroup (%)
High incomegroup (%)
4.7 0.104 0.061 0.05916.5 0.364 0.215 0.20662.0 1.351 0.898 0.77012.9 0.172 0.161 0.1610.2 0.768 0.513 0.4407.435.4
8539.393356.4
8.1 1.835 0.409 0.270
w, medium, high) if PM10 concentration levels in 2000 were reduced tout Delhi
ual health costs (US$ million,2001) for various income
egories (lower cost estimates)
Annual health costs (US$ million,2001) for various income
categories (higher cost estimates)
er incomegroup
Mediumincomegroup
Highincomegroup
Lower incomegroup
Mediumincomegroup
Highincomegroup
0.06 0.07 0.13 0.15 0.18 0.320.32 0.54 1.16 0.81 1.35 2.900.02 0.04 0.08 0.05 0.09 0.20
-0.005 -0.009 -0.018 -0.013 -0.021 -0.0460.005 0.006 0.010 0.012 0.014 0.0265.0 8.4 18.0 5.0 8.4 18.01.9 3.2 6.8 4.9 8.2 17.5
0.001 0.001 0.001 0.003 0.001 0.0027.3 12.2 26.1 10.9 18.2 38.8

1018 WORLD DEVELOPMENT
15. Gradual replacement of traffic lights at major intersec-tions with flyovers, including the entire 55-km long RingRoad since 2001.16. Providing timer indicators at major traffic intersectionsto encourage engine turn-offs for longer waiting periods.
Table 16. Estimated annual morbidity costs avoided for different income groups25 lg/m3 throug
Health effect Per case health costestimates (US$, 2001)#
Lower costestimates
Higher costestimates
Chronic bronchitis in adults (new cases) 2.52 6.31Respiratory hospital admissions 121 301Cardiac hospital admissions (daily) 542 1354Emergency room visits (daily) 3.40 8.50Asthma symptom days 0.57 1.42Restricted activity days (adults) 2.77 2.77Days with acute respiratory symptoms 0.10 0.26Acute bronchitis in children (0–15 years) 0.10 0.26
Total morbidity costs avoided (US$ million)# Based on Brandon and Hommann (1995).
Table 17. PM10 concentration trend over 2000–06 in
PM10 parameters (24 hourly averages) 2000 2001
Minimum daily concentration levels
Mean (lg/m3) 107 98Standard deviation (lg/m3) 54 66% change in mean over previous year – �9%
Maximum daily concentration levels
Mean (lg/m3) 253 195Standard deviation (lg/m3) 158 139% change in mean over previous year – �23%
Mean daily concentration levels
Mean (lg/m3) 162 134Standard deviation (lg/m3) 66 70% change in mean over previous year – �17%
Percentage of time concentration levels exceed NAAQS in a day
Mean (%) 43 53Standard deviation (%) 44 37% change in mean over previous year – 23%
Source: Analyzed using CPCB database (Central Pollution Control Board (CP
Table 15. Estimated annual costs avoided because of prevented deaths for differreduced to 25 lg/m3
Income categories Per case health costestimates (US$, 2001)#
Lower costestimates
Higher cosestimates
Low income (lower mortality estimates) 1,167 9,000Low income (higher mortality estimates) 1,167 9,000Medium income (lower mortality estimates) 1,890 9,000Medium income (higher mortality estimates) 1,890 9,000High income (lower mortality estimates) 5,107 9,000High income (higher mortality estimates) 5,107 9,000
Total mortality costs avoided (US$ million)# Based on Brandon and Hommann (1995).
There has been a gradual reduction in PM10 levels in Delhiduring 2000–05, except in 2002 when the situation had deteri-orated. May be it precipitated the action on phasing out ofdiesel-driven public transport during 2003, which was entan-gled in legal controversies over some time. CNG is a cleaner
(low, medium, high) when PM10 concentration levels in 2000 are reduced tohout Delhi
Annual health costs(US$ million, 2001) for
various income categories(lower cost estimates)
Annual health costs (US$ million,2001) for various income categories
(higher cost estimates)
Lowerincomegroup
Mediumincomegroup
Highincomegroup
Lowerincomegroup
Mediumincomegroup
High incomegroup
0.070 0.085 0.156 0.174 0.213 0.3910.424 0.729 1.561 1.059 1.821 3.9010.026 0.046 0.098 0.065 0.114 0.2450.007 0.012 0.025 0.017 0.029 0.0630.009 0.011 0.020 0.022 0.027 0.0506.371 11.024 23.623 6.371 11.024 23.6232.560 4.372 9.367 6.583 11.241 24.0860.001 0.001 0.001 0.004 0.001 0.002
9.5 16.3 34.8 14.3 24.4 52.2
Delhi as per the records of 7 monitoring stations
2002 2003 2004 2005 2006
114 96 96 94 94.158 58 52 52 43.6
17% �16% 0% �2% 1%
247 222 224 210 256159 123 142 141 12826% �10% 1% �6% 22%
170 147 146 140 15871 63 59 73 60
26% �13% �1% �4% 13%
72 59 59 51 65.530 35 37 38 34.9
36% �18% �1% �13% 29%
CB) (2008).
ent income groups (low, medium, high) when PM10 concentration levels arethroughout Delhi
Annual health costs avoided(US$ million, 2001)
(lower per case cost estimates)
Annual health costs avoided(US$ million, 2001)
(higher per case cost estimates)t
2.5 198.7 674.4 2115.2 7324.1 4384.5 149
31–108 82–288

HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1019
fuel from climate change perspective as well since CO2 emis-sions from vehicles running on CNG are lower than those run-ning on diesel and/or gasoline.
Most of these policies, while contributing to PM10 and otherlocal pollutant emission reductions, have also contributed toCO2 emission mitigation 26 directly or indirectly because ofefficiency improvement of fossil fuel combustion. CO2 is themost prominent greenhouse gas (GHG) and contributed67% to India’s total GHG emissions in 2000 (Garg et al.,2006). PM10 is a local pollutant and, as discussed in an earliersection, has the most adverse human health impacts vis-a-visother local pollutants. CO2 and PM10 emissions, therefore,represent global and local implications of any policy to miti-gate air pollution.
We now try to estimate reduction in PM10 and CO2 annualemission loads owing to a reduction in ambient PM10 concen-tration levels. However, estimating a decrease in annual PM10
emission loads from the data on ambient PM10 concentrationlevels would involve intricate modeling and is outside thescope of. 27 We, therefore, follow a more direct methodologyof estimating annual CO2 and PM10 (only combustion based)emission loads by multiplying the total activity levels (fuelcombusted here) during a year with respective technology le-vel emission factors. This methodology is based on Intergov-ernmental Panel on Climate Change (IPCC) (2006) and Garget al. (2001, 2006). Emissions are attributed to specific sourcecategories. For example, source categories for CO2 emissionsare combustion of various fossil fuels (such as coal, petroleumoil products, and natural gas), industrial processes (such ascement, iron and steel, lime and ammonia production), andcoal mining. According to the IPCC methodology (Intergov-ernmental Panel on Climate Change (IPCC), 2006), activitydata for each source category are multiplied by respectiveemission factor to obtain emissions from that source cate-gory. To calculate the total emissions from all its sourcecategories, the emissions are summed over all source catego-ries as shown below
Emissions ¼X
source cat
Activity Datasource cat
� Emission Factorsource cat
0
4
8
12
16
20
1990 1995
CO
2 em
issi
ons
(Mill
ion
tons
)
Other coal use Co
High Speed Diesel Ga
Figure 9. Trend in energy sector CO2 emissions (million tons per
where Emissions is emissions of a given pollutant from all itssource categories; Activity Datasource_cat is the amount of indi-vidual source category utilized that generates emissions of thepollutant under consideration; and Emission Factorsource_cat isthe emission factor by type of source category (emissions perunit of activity data utilized).
We have used actual activity data for various source catego-ries for CO2 and PM10 emissions. These are primarily derivedfrom published documents of the Government of India andstate governments, reputed data organizations in India, suchas Centre for Monitoring Indian Economy (CMIE), industrialassociations such as Cement Manufacturers’ Association(CMA), and some of our own surveys (Garg & Shukla,2002; Garg et al., 2006).
The CO2 and PM10 emission trends for Delhi are shown inFigures 9 and 10, respectively. 28 These indicate that total CO2
emissions continue to rise continuously over 1990–2005, whiletotal PM10 emissions (and not ambient concentration levels)have declined after 2000. The driving forces of CO2 andPM10 emission growths are also inherently different. Whileformal public initiatives are being increasingly instituted tomitigate PM10 pollution, the CO2 emission intensity has im-proved mainly because of increased competition in the wakeof economic reforms such as energy efficiency measures bycompanies, and more fuel efficient vehicles. The expectationsof higher activity levels in the coming years, namely morepower generation, increased industrial outputs, and more pri-vate transport, imply that CO2 emissions would continue torise in absolute terms, though the emissions intensity wouldcontinue to improve (Garg et al., 2007).
Table 18 captures the mitigative impact of policies high-lighted earlier. During 2000–05, average annual PM10 concen-tration levels in Delhi decreased by 22 lg/m3 (Table 17).
Energy-based PM10 emissions reduced by 8.4% in the interimperiod according to Figure 10 (only combustion based 29)while there was a 10.2% increase in CO2 emissions based onactual fuel consumption data (Figure 9). 30
We also analyze two scenarios: (1) reduction in CO2
emissions if annual average PM10 concentration is broughtdown to 60 lg/m3 throughout Delhi and (2) reduction inPM10 emissions if CO2 emissions are brought down by 5%over 2000 CO2 emission levels. The first scenario analyzes
2000 2005
al (Power) Coal (Brick)
soline Other liquid fuels
year) in Delhi over 1990–2005. Source: Garg et al. (2007).

0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1990 1995 2000 2005
PM
10 e
mis
sion
s (t
hous
and
tons
)
High Speed Diesel Gasoline Coal (Brick)
Coal (Power) Other liquid fuels Other coal use
Biomass
Figure 10. Trend in energy sector PM10 emissions (thousand tons per year) in Delhi over 1990–2005. Source: Garg et al. (2007).
Table 18. Ancillary emission benefits of CO2 and PM10 emission mitigation in Delhi
Description Change in PM10 emissions (%) Change in CO2 emissions (%)
Overall change in emissions from year 2000 to year 2005 (%) �8.4 10.2Estimated overall change in emissions if annual average PM10 concentration isbrought down to 60 lg/m3 through out Delhi (%)
�59 �9.6
Estimated overall change in emissions if annual CO2 emissions are broughtdown by 5% below 2000 emissions in Delhi (%)
�11.3 �5
1020 WORLD DEVELOPMENT
the global implications of a local clean air policy, while thesecond scenario does the reverse.
For the first scenario, changes in PM10 emission loadsneeded to bring the PM10 concentration levels of 162 lg/m3
in the year 2000 (Table 17) to 60 lg/m3 have been estimatedseparately for each of the 27 sub-districts. For this we have as-sumed that the relationship between changes in PM10 mea-sured concentration levels during 2000–05 and respectivechanges in estimated emission load continues for each of the27 sub-districts. 31 The resulting fuel consumption levels arethen used to estimate CO2 emission reduction. The PM10 emis-sion load reduces by 59% while the CO2 emissions reduce by9.6%. It is, however, noted that reduction in PM10 emissionsbecause of fossil fuel combustion activities is only 31%, whichalso results in CO2 mitigation. For the remaining 28%, bio-mass combustion contributes 11% to PM10 emissions reduc-tion, mainly owing to higher penetration of cleanercombustion technologies. The remaining 17% reduction comesfrom other measures that reduce ambient dust such as plantingmore grass and trees and cleaner construction activities. Bio-mass combustion and other measures do not result in anyCO2 mitigation.
For the second scenario, the effect of a climate policy to re-duce CO2 emissions by 5% below the 2000 emissions is esti-mated to result in 11.3% reduction in PM10 emissions. 32 Thecontribution by different sources varies with coal use takingthe maximum hit as coal-based power generation becomesmore efficient.
Direct CO2 mitigation policies (e.g., energy efficiencyimprovements and fuel switch from coal to natural gas) re-sult in PM10 emission mitigation as an ancillary benefit and
vice versa. However, the ancillary benefits for PM10 mitiga-tion policy and CO2 mitigation policy are asymmetric. Theemission elasticity of PM10 emissions because of direct CO2
mitigation policy is around 2.2, while the CO2 elasticity be-cause of direct PM10 mitigation policy is around 0.16(Table 18). 33 This implies that direct CO2 mitigation as a cli-mate change policy would also result in substantial PM10
mitigation. While comparing these results with some otherestimates for developing countries (Connor, 2000), there isa consistency in trend that the level of ancillary benefits ex-ceeds the direct CO2 mitigation benefits in developing coun-tries. However, the benefits of PM10 mitigation are higherfrom a direct policy to reduce them, compared to thosethrough a CO2 mitigation policy (Garg, Shukla, Rana,Kapshe, & Nair, 2003).
8. WHO PAYS FOR MITIGATING AIR POLLUTION?
The rich could bear a much higher share of costs of mitigat-ing air pollution - both for PM10 and CO2, mainly since theyconsume more of energy intensive and emission producinggoods such as electricity and private transport. Only 38.2%households owned personal motorized transport vehicles (carsand/or motorcycles) in Delhi (NFHS-2 database), mostly inhigh and medium income categories. The polluters’ profile isskewed toward the rich for private transport. Any policy tomitigate emissions from the transport sector, such as higherfuel taxes, and higher capital costs of vehicles with inefficienttechnology would, therefore, target the higher income catego-ries.

HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1021
After the transport sector, coal combustion in brick kilnsand power plants are other large contributors of PM10 in Del-hi. All the brick kilns around Delhi are owned by people inhigh income categories. Most of these kilns employ inefficientfixed chimney technology without any end-of-the-pipe tech-nologies for PM10 mitigation (Clancy & Garg, 2002). Effi-ciency improvement in existing kilns and cleaner technologyadoption would reduce PM10 emissions while simultaneouslyreducing CO2 emissions per unit of bricks manufactured. Evenif owners of kilns pass on the costs to consumers or to factorsof production, the brick consuming class also has a higher pro-portion of high and medium income households. 34
Two coal-based power plants are close to one of the mostpolluted areas in Delhi (ITO crossing). Their average plantload factors (PLF), heat rates, and auxiliary power consump-tion are worse than the central sector’s average in India, indi-cating that the Delhi plants burn more coal and, therefore,emit more CO2 per unit of power produced. The perfor-mance of particulate emission control devices (electro staticprecipitators) also has considerable room for improvement. 35
Moreover, the aggregate technical and commercial (AT&C)losses in Delhi for 2001 were 50.7%, indicating that morethan half of the electricity generated is either lost in transitor not paid for. AT&C losses approved by the Delhi Electric-ity Regulatory Commission in 2001 were 57.2% for Centraland East Delhi districts where high income population is86% of total population. For North, North West, South,and South West Delhi districts, the approved losses were48.1% where the high income population was 58% cumula-tive (Government of National Capital Territory of Delhi(GoNCTD), 2007). Some of the high power theft-prone areasas shown on the Delhi utility company BSES’s website areJanakpuri (West Delhi) with over 50–70% theft (Janakpurihas 12% low income households), Sarita Vihar (South Delhi)with over 60% theft (12% low income households), Nazaf-garh with over 30% theft (6% low income households), andPaschim Vihar in Punjabi Bagh with 60% theft (10% low in-come households) (BSES(a), 2008). This is indicative but notconclusive evidence that power theft is more where more richpeople stay.
On the other hand, the advantage of negligible agriculturalpower consumption is partially offset by the presence of unau-thorized residential areas. It is accepted that electricity is sto-len in unauthorized areas and slums, which are not formallyelectrified and metered. But the area’s share of total theft isnot reported. However, it is also a known fact that many me-ters are tempered with to record lower or negligible consump-tion. The Distribution Company BSES has initiated anamnesty scheme where consumers with defective, tempered,and non-working meters have been asked to get them replacedfree of charge as a one-time measure (BSES(b), 2008). Meterreplacement is a high priority measure under power sector re-forms in Delhi. It may be noted here that electricity meters aremostly found in medium and high income group categories’residences. However, with almost three fourth of “paid” elec-tricity consumed directly or indirectly by higher incomegroups, the rich are likely to benefit more from this ‘unac-counted’ and unpaid for electricity in Delhi. Improvement inelectricity generation, distribution, and rent collection effi-ciency are, therefore, likely to result in more revenue collectionfrom higher income households.
PM10 mitigation measures where the government will haveto bear major expenses, such as planting more grass, wouldalso utilize taxes paid for by the higher income categoriessince the poor and slum-dwellers do not fall in tax payingcategories. Expenditure to maintain cleaner construction sites
to reduce suspended dust will also affect builders who fall inthe rich income category.
9. CONCLUSIONS
This paper has first estimated the health benefits associatedwith a reduction in PM10 concentration for different socio-eco-nomic groups in the population of Delhi, based on income le-vel. Sub-district level population in Delhi has been classifiedinto three different income groups; low, medium and high.The health impacts for each group are estimated for mortalityand morbidity. The low and medium income urban house-holds have higher mortality rates (7.56 per 1000 persons inthe low income category, 4.8 in medium, and 4.61 in high)and risks of suffering from asthma, than those in the high in-come category (18.82 low, 12.98 medium, and 11.14 high).
Health benefits were estimated using following data:Second National Family Health Survey (NFHS-2) 1998–99, for data about mortality and morbidity rates (basedon self-reported answers about health status.Standard of living data from two different NSSO studies/datasets (NSSO, 2001, 2002) based on monthly per capitaexpenditure (MPCE)CPCB air quality data for the period 2000–06 (CentralPollution Control Board (CPCB), 2008) for concentrationlevels of PM10.Annual CO2 and PM10 emission estimates by the author(Garg & Shukla, 2002; Garg et al., 2006).
Health benefits are estimated in terms of avoidance of mor-tality and morbidity, and associated health costs by reducingthe existing PM10 concentration levels to 60 lg/m3, which isthe upper boundary of ambient air quality norm for residentialareas in India. Health impacts are estimated using concentra-tion–response functions from developed countries moderatedby using Delhi-specific income related baseline health indices.Results show that the percentage reduction of avoided cases ismore for the poor than for the rich. Lower income groups areexposed to higher concentrations of pollutants, and have high-er baseline mortality and morbidity rates. Moreover there isunequal access to healthcare, because of the expenditure re-quired. All these factors contribute in reducing the capacityof lower income groups to deal with air pollution impactson health.
The second objective of the paper is to estimate a reductionin PM10 and CO2 annual emissions because of the applicationof specific policies aimed at reducing PM10 concentration lev-els in Delhi. Results show that ancillary benefits in the form ofPM10 mitigation exceed direct CO2 mitigation benefits in Del-hi, and may be in developing countries in general, and that thecosts of such policies would be borne by high-income catego-ries, as they are the major consumers of energy and CO2 inten-sive goods and services.
The paper shows that major PM10 emission sources areowned by the higher income groups and their economic bene-fits also accrue to them, while the poor bear a disproportion-ately higher share of the resultant air pollution health burden.Most measures that reduce PM10 are measures that (a) havecarbon emission reductions, (b) impose more costs on the bet-ter-off and (c) provide higher health benefits to the poor. Cli-mate and local pollution mitigation policies could, therefore,be interlinked to provide health benefits to the poor.
If PM10 concentration levels are to be reduced to 60 lg/m3
throughout Delhi, which is a very steep decline from the exist-ing average of over 150, a combination of policies have to beadopted such as some direct PM10 mitigation policies for

1022 WORLD DEVELOPMENT
cleaner local air (e.g., controlling re-suspension of road dustand enforcing soot emission standards in industry), some di-rect climate change policies (e.g., switching from coal to natu-ral gas), and some common policies (e.g., natural gas for roadtransport and energy efficiency improvements in various sec-tors). Their investment requirements and costs would be differ-ent. While cleaning the local air is the government’s liability toits citizens, the incremental costs for cleaning it through a cli-mate change policy are not. 36 Switching away from coal raises
energy security concerns for India. The conventional view,therefore, has been that climate change policies would haveto be pursued for their own sake in India (Garg et al., 2003;MoEF, 2004). This paper has offered another viewpoint thatclimate change mitigation policies would also have substantialpro-equity effects through larger health benefits for the poorwhile the rich will bear higher costs, and these should be con-sidered while formulating an appropriate policy response for alarge developing country like India.
NOTES
1. Although PM2.5 is more damaging, its concentration level is notmonitored in Delhi. PM10 is commonly used as a surrogate for PM2.5 forsuch studies (Ostro & Chestnut, 1998; World Bank, 2002a; Kumar &Foster, 2001). Health damages caused by other common local pollutantsfrom energy combustion activities (such as SO2, NOx, and CO) are not sopronounced (Brandon & Hommann, 1995; World Bank, 2003; Pandey,Kumar, & Devotta, 2005), more so since Delhi is supplied entirely withultra low sulfur and lead-free diesel and gasoline.
2. Indoor air pollution could be a larger cause of burden of air pollutionrelated diseases in India (WHO, 2006). The main source is solid fuel burntfor cooking in households. However in Delhi, liquefied petroleum gas(LPG) is the dominant fuel used in 68% households, kerosene in 24%, andsolid fuels (mainly biomass) only in 7% (http://des.delhigovt.nic.in/Publications/HB2004/hb2004I.pdf on 13 June 2006). Therefore, indoorair pollution may not be that large a pollution source in Delhi.
3. While this paper relies on data from NFHS-2 that was conducted in1999, it is noted that the NFHS-3 survey was carried out during 2005–06and the final report was published in November 2007 much later than thepresent analysis was conducted and manuscript submitted. Moreover sincethe Delhi population data are available for 2001 (Census of India (CoI),2001), we have kept the focus of present study on NFHS-2, which wasconducted around the same time as the Indian census of 2001.
4. Prevalence measures how much of some disease or condition in apopulation at a particular point in time. Incidence measures the rate ofoccurrence of new cases of a disease or condition.
5. The following scores are applied for each household separately: House
type: 4 for pucca (brick and concrete), 2 for semi-pucca, 0 for kachha (mudor thatched); Toilet facility: 4 for own flush toilet, 2 for public or sharedflush toilet or own pit toilet, 1 for shared or public pit toilet, 0 for nofacility; Source of lighting: 2 for electricity, 1 for kerosene, gas, or oil, 0 forother source of lighting; Main fuel for cooking: 2 for electricity, liquidpetroleum gas, or biogas, 1 for coal, charcoal, or kerosene, 0 for other fuel;Source of drinking water: 2 for pipe, hand pump, or well in residence/yard/plot, 1 for public tap, hand pump, or well, 0 for other water source;Separate room for cooking: 1 for yes, 0 for no; Ownership of house: 2 foryes, 0 for no; Ownership of agricultural land: 4 for 5 acres or more, 3 for2.0–4.9 acres, 2 for less than 2 acres or acreage not known, 0 for noagricultural land; Ownership of irrigated land: 2 if household owns at leastsome irrigated land, 0 for no irrigated land; Ownership of livestock: 2 ifowns livestock, 0 if does not own livestock; Ownership of durable goods: 4each for a car or tractor, 3 each for a moped/scooter/ motorcycle,telephone, refrigerator, or color television, 2 each for a bicycle, electricfan, radio/transistor, sewing machine, black and white television, waterpump, bullock cart, or thresher, 1 each for a mattress, pressure cooker,chair, cot/bed, table, or clock/watch.
6. Next higher MPCE level has been taken in case the NFHS-2equivalent population percentage lies in between an MPCE category.For instance, the MPCE category up to INR 425 is used as cut-off for low
urban even though it cumulatively covers higher percentage of households(19.8%) than those stipulated for urban low by NFHS-2 (14.3%) inTable 2.
7. The World Bank poverty estimates for India year 2000 are 34.7%(below US$ 1 PPP/capita/day) and 79.9% (below US$ 2 PPP/capita/day)(WDR, 2005). India’s national estimates of poverty levels for urban andrural areas for 1999–2000 were 24.7% and 30.2% of total population,respectively. The Indian poverty line for urban areas in 2001 was per
capita monthly income of nominal INR 111.23 (or around US$ 0.5 PPP/capita/day).
8. Patel Nagar (East) and Patel Nagar (West) in West Delhi district,although physically separated and sometimes shown as two separate sub-districts, are counted as one sub-district in this study.
9. The Census of India, 2001, has defined slum areas broadly as follows:(1) All specified areas notified as “Slum” by State/Local Government andUT Administration under any Act. (2) All areas recognized as ’Slum’ byState/Local Government and UT Administration which may have notbeen formally notified as slum under any Act. (3) A compact area of atleast 300 populations or about 60–70 households of poorly built congestedtenements, in unhygienic environment usually with inadequate infrastruc-ture and lacking in sanitary and drinking water facilities.
10. 32.6% = 0.93 � (28/(28 + 66)) + 0.07 � (66/(28 + 66)), and67.4% = 100% � 32.6%.
11. Møller et al. (2008) show that air pollution exposure increases therisk of lung cancer. The paper concludes that collectively there is evidenceindicating that exposure to traffic-related air pollution particles isassociated with oxidative damage to DNA and this might be associatedwith increased risk of cancer. Liaw et al. (2008) have also indicated that acorrelation exists between air pollution and lung cancer (cell typeadenocarcinoma). Human exposure to combustion emissions includingthe associated airborne fine particles and mutagenic and carcinogenicconstituents (e.g., polycyclic aromatic compounds (PAC) and nitro-PAC)have been studied in populations in Europe, America, Asia, andincreasingly in third-world counties (Lewtas, 2007). A number of thesecomponents are significant sources of human exposure to mutagenic andcarcinogenic chemicals that may also cause oxidative and DNA damage,leading to reproductive and cardiovascular effects. Although there issubstantial evidence that PAH or substituted PAH may be causativeagents in cancer and reproductive effects, an increasing number of studiesare investigating these and other potential causative agents from airpollution combustion sources.
12. Tobacco consumption is reported to increase the risk of cancer threeto fourfolds, heart diseases two to threefolds, acute respiratory infectionstwo to three and a half-folds than a non-tobacco consuming person(National Sample Survey Organization (NSSO), 1998). The risks aregenerally lower in urban areas compared to rural areas. WHO BOD

HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1023
estimates for India indicate that trachea/bronchus/lung cancer account for15% of all types of cancer deaths; and ischemic heart diseases account for55% of total deaths from heart attack.
13. Only 3.6% urban households use solid fuels for cooking in Delhi(2.5% for urban). Liquefied petroleum gas is used in almost 80% ofhouseholds and kerosene stoves in another 16% (DHS data archive).
14. Although government documents do not indicate whether construc-tion workers have been missed out in the slum population survey, thechances are that, many smaller construction sites could be missed out. Aconstruction site with 60–70 households at one place and at least 300population implies a reasonably big construction activity, which may notbe the case for many other smaller sites in a rapidly expanding city likeDelhi where construction workers stay in much smaller groups than 300 atconstruction site locations utilizing under construction buildings asshelters.
15. The GIS-based interpolation technique creates PM10 level contoursfor entire Delhi based on a number of independent parameters, such asPM10 concentration levels in existing monitoring stations, relativedistances, and topology.
16. Average of six CPCB locations was taken since ITO levels were toohigh due to its specific location and traffic patterns and was, therefore,considered as a special case in Delhi. We also analyzed alternate GIS-interpolation scenarios using 60 lg/m3 for the 6 dummy locations as theseare the permitted NAAQM standard PM10 concentration levels forresidential areas (Table 2). This, however, again projected very low PM10
concentration levels in west and north-west districts, making them much“cleaner” than the rest of Delhi, which were considered as unrealistic.
17. Average one-way daily commuting time for work in Delhi is 60–75min, limiting the total exposure to around 2.5 h (http://www.igovernment.in/site/traffic-snarl-snaps-42-cr-man-hour-from-delhi-ncr-workers/ ac-cessed on 25th May 2008). Since passage through New Delhi districtcould cover below one-fourth of a representative commuting cycle, totalexposure through New Delhi district will be below one hour per day.
18. This morbidity rate is different from the prevalence rate, asrecommended by the WHO Expert Committee on Health Statistics.Generally, prevalence rate is defined as the ratio between the number ofspells of ailment suffered at any time during the reference period and thepopulation exposed to the risk. It measures the frequency of illnessesprevailing during the reference period, whereas the figure here gives theestimated proportion of persons reporting ailment suffered at any timeduring the reference period. Strictly speaking, these estimates are,therefore, not prevalence rates. Moreover as the estimates are based onself reported morbidity data, rather than on medical examination, theinformation on number of spells of different ailments suffered during thereference period is not likely to reflect the objective illness-status of thepatients, particularly the number of diseases a patient is afflicted with.However, this could be used as good indicator for morbidity prevalencecomparison across different income groups over the years and to capturethe general morbidity status in the target groups.
19. NSSO (1998) is used for the purpose of figures and table in thissection alone to highlight that poor have poorer health compared to theirricher counterparts and may also have lower reporting of diseases becauseof lower health consciousness. It implies that the disease prevalence ratesin the health status data discussed earlier in Section 2, which alreadyindicates higher disease prevalence rates for low and medium incomecategories than the high income categories, could be even higher for thepoor. This would mean that the poor suffer even more than what we haveanalyzed in Section 2 and would, therefore, gain even more from airpollution control policies.
20. These health costs avoided may also be seen as health benefitsaccruing to the respective population.
21. Empirical estimates of C–R functions (or dose–response functions)from developed countries continue to be used to estimate the healthimpacts of air pollution in developing countries with a caveat that theestimates are obviously conservative. Muenning, Franks, Haomiao,Lubetkind, and Goldd (2005) have analyzed the income-associated burdenof disease in the United States using different regression analyses on USnational health survey data. They have inferred that bottom 80% of adultincome earners’ life expectancy is 4.3 years and 5.8 health adjusted lifeyears (HALYs) shorter relative to those in the top 20% of earnings. Thesevalues were 5.6 years and 8.5 HALYs lower for those below the povertythreshold than those above. No literature could be found for incomerelated C-R functions. We have used income related total mortality dataand specific morbidity rates in an effort to bring the C–R functions closerto represent the contextual environment.
22. The discount rate is taken as 5%, same as in the Brandon andHommann study.
23. This is taken from Indian government instituted compensation for lossof life in accidents on the Indian Railways (IR), which is a fully governmentowned organization. In the case of accidents, passengers or their families canclaim compensation through the “passenger liability insurance,” enacted bythe Indian Parliament since 1994. The amount is up to US$ 9000 in the caseof death and permanent disability, and up to US$ 2000 in the event ofinjuries. This is irrespective of income level of the deceased. The insurancepolicy is currently reinsurance driven and IR pays an annual premium ofaround US$ 9 million for the policy. (http://www.thehindubusiness-line.com/2006/07/13/stories/2006071304010900.htm).
24. In Delhi, a poor household could be spending up to 40% of its MPCEon treatment per ailment, while for the richer households it is up to 20%(NSSO, 1998). Poor households could also lose part of their total incomeif a member of the household is hospitalized since earning members maynot be able to work while tending the sick in the hospital. The estimatesfor Delhi are up to 20% for poor households per hospitalized case and upto 4% for richer households (NSSO, 1998).
25. In 1997, USEPA added two new PM2.5 standards, set at 15 lg/m3
and 65 lg/m3, respectively, for the annual and 24-h standards. ForEurope, 20 lg/m3 is indicated as the 2010 limit for annual average PM10
concentration levels, while the current average PM10 is 15–30 lg/m3
(Medina, Plasencia, Ballester, Mucke, & Schwartz, 2004).
26. The Government of India does not have any GHG mitigation targetsunder the Kyoto Protocol. However the emission impacts would remainunchanged for individual emissions if these policies were adopted forreasons of cleaning the local air or to mitigate GHG emissions. The samemay not be concluded for cost-effectiveness of separate policies withalternative objectives of local air cleaning or of mitigating climate change(Garg et al., 2003).
27. Linking emission loads (usually in tons) to emission concentrations(usually in lg/m3) remains a modelling challenge (Connor, 2000; Ho &Jorgensen, 2003). These may be either modelled using an intricate bottom-up dispersion model, or assuming a simple linear relationship betweenregional emissions and ambient concentration measures in major cities.
28. Biomass combustion is considered carbon neutral and therefore noCO2 emissions are estimated from Energy sector emissions contribute over95% of total CO2 emissions in Delhi (Garg & Shukla, 2002).
29. The white paper on pollution in Delhi attributed 72% of ambient airpollution to vehicular transport for 2000–01 (Ministry of Environment,2000). Sameer (2004), quoting ESMAP studies for India, attributes almost20% each to diesel combustion, road dust, biomass combustion, and

1024 WORLD DEVELOPMENT
unidentified sources, as their annual average contribution towardsambient PM10 concentration levels. The remaining 20% is contributedby secondary sulphates/ nitrates/ ammonium, and coal and gasolinecombustion. There is a seasonal variability to these shares, with diesel anddust increasing during summers, while biomass increasing during winters.The URBAIR report (1997) for Mumbai suggested 30% of PM10 fromvehicle exhausts and another 20% from road dust re-suspension. ForKanpur, the eighth largest Indian city, auto exhausts contributed 16%PM10, re-suspension of dust and the (33%), remaining came fromindustrial and other sources (Mashelkar et al., 2002).
30. Despite these policies resulting in a reduction in average emissionfactors for CO2 and PM10 emissions from almost all technology types,CO2 emissions have continued to rise because of a substantial increase intotal activity levels during 2000–05. The CO2 and PM10 emission trendsalso indicate that these policies were more focused towards cleaning thelocal air as against CO2 emission mitigation.
31. For instance, the total PM10 emissions declined by 8.4% during 2000–05 (Figure ure10) while the average PM10 concentration levels declined by22 lg/m3 (Table 17). This relationship is assumed to continue for furthermitigation policies.
32. A simple spreadsheet based model has been used that estimates fueluse (for a 5% annual reduction in CO2 emissions over 2000 level) based onfuel carbon contents, existing activity and efficiency levels of majoremission sources in Delhi. We have not considered any additionalmeasures in this scenario that specifically reduce only PM10 emissions.
33. In economics, elasticity is the ratio of the change in one variable withrespect to change in another variable. The elasticity of PM10 emissionswith respect to CO2 emissions is therefore the percentage change in PM10
emissions because of 1% change in CO2 emissions.
34. Almost all the houses are owned by high and medium incomehouseholds. Low income categories own a very small percentage. Furthernot much of energy intensive construction materials and bricks are used inslum housing.
35. ESPs result in lower PM10 emissions and lower auxiliary powerconsumption (thus lower coal consumption per unit of power delivered)besides meeting environmental norms.
36. See end of Footnote 30.
REFERENCES
Abbey, D. E., Petersen, M. P. H., Mills, P. K., & Beeson, W. L. (1993).Long-term concentrations of total suspended particulates, ozone, andsulfur dioxide and respiratory symptoms in a nonsmoking populations.Archives of Environmental Health, 48, 33–46.
Bai, N., Khazaei, M., Stephan, F. V. E., & Laher, I. (2007). Thepharmacology of particulate matter air pollution-induced cardiovas-cular dysfunction. Pharmacology and Therapeutics, 113(1), 16.
Brandon, C., & Hommann, K. (1995). The cost of inaction: Valuing theeconomy-wide cost of environmental degradation in India. Washington,DC: Asia Environment Division World Bank.
BSES(a). (2008). [WWW page]. URL. <http://bsesdelhi.com/high_loss_dt.asp> Accessed on 5th June 2008.
BSES(b). (2008). [WWW page]. URL <http://bsesdelhi.com/BSES_AD.pdf> Accessed on 5th June 2008.
Burnett, R. T., Dales, R., Krewski, D., Vincent, R., Dann, T., & Brook, J.F. (1995). Associations between ambient particulate sulfate andadmissions to Ontario hospitals for cardiac and respiratory diseases.American Journal of Epidemiology, 142(1), 15–22.
Census of India (CoI). (2001). Government of India. [WWW page]. URL<http://www.censusindia.net/> Accessed on 10th May 2007.
Central Pollution Control Board (CPCB). (2008). Government of India.[WWW page]. URL <http://www.cpcb.nic.in/>.
Clancy, J., & Garg, A. (2002). Energy management and environmentalprotection in India. The Netherlands: University of Twente.
Cohen, A., Anderson, R., Ostro, B., Pandey, K. D., Krzyzanowski, M., &Kunzli, N. (2003). Mortality impacts of particulate air pollution in theurban environment. In M. Ezzati, A. D. Lopez, A. D. Rodgers, & C. J.L. Murray (Eds.), Comparative quantification of health risk: Global andregional burden of disease due to selective major risk factors. Geneva:World Health Organization.
Connor, D. O. (2000). Ancillary benefits estimation in developingcountries: A comparative assessment. [WWW page]. URL <http://www.airimpacts.org/documents/local/M00007487.pdf> Accessed on19 June 2006.
Dockery, D. W., Cunningham, J., Damokosh, A. I., Neas, L. M.,Spengler, J. D., & Koutrakis, P. (1996). Health effects of acid aerosolson North American children: Respiratory symptoms. EnvironmentHealth Perspective, 104(5), 500–505.
Garg, A., Bhattacharya, S., Shukla, P. R., & Dadhwal, V. K. (2001).Regional and sectoral assessment of greenhouse gas emissions in India.Atmospheric Environment, 35(15), 2679–2695.
Garg, A., & Shukla, P. R. (2002). Emissions inventory of India. New Delhi:Tata McGraw-Hill.
Garg, A., Shukla, P. R., & Kapshe, M. (2006). The sectoral trends ofmultigas emissions inventory of India. Atmospheric Environment, 40,4608–4620.
Garg, A., Shukla, P. R., & Menon-Chaudhury, D. (2007). Aligning energyuse, air quality and climate change through sustainable development:A case study of Delhi. Engineering Journal. Columbia. #25 revista deingenierıa. Universidad de los Andes. rev.ing. ISSN 0121-4993. May2007.
Garg, A., Shukla, P. R., Rana, A., Kapshe, M. M., & Nair, R. (2003).Future greenhouse gas and local pollutant emissions for India: Policylinks and disjoints. Mitigation and Adaptation Strategies for GlobalChange, 8(1), 71.
Government of National Capital Territory of Delhi (GoNCTD). (2007).Power sectors reforms. Government of National Capital Territory ofDelhi. [WWW page]. URL <http://delhigovt.nic.in/power.asp#6>Accessed on 4th May 2007.
Ho, M.S., & Jorgensen, D.W. (2003). Air pollution in China: Sectorallocation of emissions and health damage. A report of InternationalCooperation on Environment and Development. [WWW page].URL <http://www.ksg.harvard.edu/cbg/ptep/CCICED.report1.pdf>Accessed on 10 May 2006.
Intergovernmental Panel on Climate Change (IPCC). (2006). Guidelinesfor National Greenhouse Gas Inventories. Japan: IntergovernmentalPanel on Climate Change.
International Institute for Population Sciences (IIPS). (2000). NationalFamily Health Survey (NFHS-2): 1998–99. Mumbai: InternationalInstitute for Population Sciences (IIPS) and ORC Macro.
Krupnick, A. J., Harrington, W., & Ostro, B. (1990). Ambient ozone andacute health effects: Evidence from daily data. Journal of EnvironmentalEconomics and Management, 18(1), 1–18.
Kumar, N., & Foster, A. (2001). Respirable particulate matter and itshealth effects. New Delhi: Central Pollution Control Board.
Lewtas, J. (2007). Air pollution combustion emissions: Characterization ofcausative agents and mechanisms associated with cancer, reproductive,and cardiovascular effects. The Sources and Potential Hazards ofMutagens in Complex Environmental Matrices – Part II, 636(1–3),95–133.
Liaw, Yung-Po, Ting, Tih-Fen, Kuo-Kang, Ho, & Yang, Chin-Fen(2008). Cell type specificity of lung cancer associated with air pollution.Science of the Total Environment, 395(1), 23–27.
Mashelkar, R. A., Biswas, D. K., Krishnan, N.R., Mathur, O. P.,Natarajan, Niyati, K. P., Shukla, P. R., Singh, D.V., & Singhal, S.(2002). Report of the Expert Committee on Auto Fuel Policy. NewDelhi: Ministry of Petroleum and Natural Gas.
Medina, S., Plasencia, A., Ballester, F., Mucke, H. G., & Schwartz, J.(2004). Public health impact of PM10 in 19 European cities. Journal ofEpidemiology and Community Health, 58, 831–836. [WWW page].URL <http://jech.bmjjournals.com/cgi/reprint/58/10/831> Accessedon 17 February 2006.

HUMAN HEALTH IMPACTS OF OUTDOOR AIR POLLUTION IN NEW DELHI 1025
Ministry of Environment and Forests (MoEF). (2000). White paper on airpollution in Delhi. New Delhi: Ministry of Environment and Forests.
Ministry of Environment and Forests (MoEF) (2004). India’s InitialNational Communication to UNFCCC. New Delhi: Ministry ofEnvironment and Forests. [WWW page]. URL <www.natcomindia.org> Accessed on 5th July 2007.
Møller, P., Folkmann, J. K., Forchhammer, L., Brauner, E. V., Danielsen,P. H., Risom, L., et al. (2008). Air pollution, oxidative damage toDNA, and carcinogenesis. Cancer Letters, 266(1), 84–97.
Muenning, P., Franks, P., Haomiao, J., Lubetkind, E., & Goldd, Marthe.R. (2005). The income-associated burden of disease in the UnitedStates. Social Science & Medicine, 61(9), 2018–2026.
National Family Health Survey (NFHS-2). Demographic and healthsurveys. NFHS-2 dataset for Delhi. [WWW page]. URL <http://www.measuredhs.com/>.
National Sample Survey Organization (NSSO). (1998). Morbidity andtreatment of ailments. New Delhi: National Sample Survey Organiza-tion, Ministry of Statistics and Programme Implementation. ReportNo. 441 (52/25.0/1).
National Sample Survey Organization (NSSO). (2001). Differences in levelof consumption among socio-economic groups 1999–2000. New Delhi:National Sample Survey Organization, Ministry of Statistics andProgramme Implementation. Report No. 472 (55/1.0/10).
National Sample Survey Organization (NSSO) (2002). Household con-sumer expenditure and employment – Unemployment situation inIndia, 2000–2001. New Delhi: National Sample Survey Organization,Ministry of Statistics and Programme Implementation.
Ostro, B. D. (1987). Air pollution and morbidity revisited: A specificationtest. Journal of Environmental Economics and Management, 14(1), 87–98.
Ostro, B., & Chestnut, L. (1998). Assessing the health benefits of reducingparticulate matter air pollution in the United States. EnvironmentalResearch, Section A, 76(2), 94–106.
Ostro, B. D., Lipsett, M. J., Wiener, M. B., & Selner, J. C. (1991).Asthmatic responses to airborne acid aerosols. American Journal ofPublic Health, 81(6), 694–702.
Pandey, J. S., Kumar, R., & Devotta, S. (2005). Health risks of NO2, SPMand SO2 in Delhi (India). Atmospheric Environment, 39(36), 6868–6874.
Holgate, S., Samet, J., Koren, H., & Maynard, R. (Eds.) (1999). Airpollution and health. San Diego, CA: Academic Press.
Sameer, A. (2004). Ten years of urban air quality management in India:Findings of a recent study across five cities. In Presented at theworkshop on urban air quality management in India: Progress andfuture challenges. New Delhi.
Schwartz, J., Slater, D., Larson, T. V., Pierson, W. E., & Koenig, J. Q.(1993). Particulate air pollution and hospital emergency room visits forasthma in Seattle. The American Review of Respiratory Disease, 147(4),826–831.
Smith, K. R., & Mehta, S. (2003). The burden of disease from indoorair pollution in developing countries: Comparison of estimates.International Journal of Hygiene and Environmental Health, 206(4–5),279–289.
URBAIR, Shah, J. J., & Nagpal, T. (Eds.), (1997). Urban Air QualityManagement Strategy in Asia: Greater Mumbai Report. Washington,DC: World Bank.
World Bank. (2002a). What do we know about air pollution? – India casestudy. South Asia Urban Air Quality Management Briefing Note No.4. [WWW page]. URL <http://www.worldbank.org/sarurbanair>Accessed on 9th July 2006.
World Bank. (2002b). Improving air quality in metropolitan Mexico City:An economic valuation. World Bank Research Working Paper 2785.Washington, DC [WWW page]. URL <http://econ.worldbank.org/files/12030_wps2785.pdf> Accessed on 9th July 2006.
World Bank. (2002c). For a breath of fresh air: Ten years of progress andchallenges in urban air quality management in India 1993–2002.Washington, DC: World Bank. [WWW page]. URL <http://www.worldbank.org/sarurbanair> Accessed on 9th July 2006.
World Bank. (2003). Health impacts of outdoor air pollution. South AsiaUrban Air Quality Management Briefing Note No. 11, February 2003.Washington, DC: World Bank. [WWW page]. URL <http://www.worldbank.org/sarurbanair> Accessed on 26th April 2004.
World Bank. (2005). World Development Report 2005. Washington, DC:The World Bank.
World Health Organization (WHO). (2002). The World Health Report.World Health Organization. [WWW page]. URL <www.who.int/whr/2002/en/whr2002_annex6.pdf> Accessed on 10th May 2007.
World Health Organization (WHO). (2006). Fuel for life: Householdenergy and health. URL <http://www.who.int/indoorair/publications/fuelforlife/en/index.html> Accessed on 4th May 2008.
.sciencedirect.com
Available online at www