-
Principles of diagnosis, work-up and therapy
The Gastroenterologist’s role
Dr. Christos G. Toumpanakis MD PhD FRCPConsultant in
Gastroenterology/Neuroendocrine Tumours
Hon. Senior Lecturer University College of London
Neuroendocrine Tumour Unit - ENETS Centre of Excellence
ROYAL FREE HOSPITAL, London,UK
-
IPSEN
Honoraria for lectures
Educational Grants for RFH NET Unit
Advisory Board
AAA
Honoraria for lectures
Educational Grants for RFH NET Unit
NOVARTIS
Honoraria for lectures
Educational Grants for RFH NET Unit
Advisory Board
LEXICON
Advisory Board
-
Diagnosis of NEΝs
History and clinical examination
Biochemical tests (Biomarkers)
Imaging studies
( for localization of primary and metastatic lesions)
Histology - “ gold standard”
-
Differential Diagnosis –
Diarrhoea + Abdominal pain
“Small bowel NENs” associated
diarrhoea + abdominal pain
• Diarrhoea always secretory
(persists with fasting)
• Abdominal pain
- Even during the night- Usually periumbilical
- Occurring > 2 h after meals
- Not settling after defecation
- Features of sub-acute bowel obstruction
Diarrhoea and abdominal
pain due to IBS
• Usually young females
• Non-secretory diarrhoea
• Alternating with constipation
•Abdominal pain settling with defecation,
not occurring during the night
-
Diagnosis of NEΝs
History and clinical examination
Biochemical tests (Biomarkers)
Imaging studies
( for localization of primary and metastatic lesions)
Histology - “ gold standard”
-
Diagnosis of NEΝs
History and clinical examination
Biochemical tests (Biomarkers)
Imaging studies
( for localization of primary and metastatic lesions)
Histology - “ gold standard”
-
The role of upper GI endoscopy for
diagnosis of gastric NEΝs
Type 1 gNEN
Type 2 gNEN
Type 3 gNEN
Type 4 gNEC
The surrounding mucosa
should be ALWAYS biopsied
especially in gastric NENs
-
Types of G-NENs
Type I Type ΙΙ Type ΙΙΙ
Relative frequency 70 – 80% 5 – 6% 14 – 25%
Features Usually multiple
( 80%
-
The role of lower GI endoscopy for diagnosis of rectal NEΝs
-
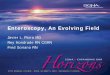
Role of wireless small bowel capsule endoscopy
Indications :
- To detect the primary (-ies) in
suspected small intestinal
NENs
- To identify source of small
bowel bleeding in NENs
Sensitivity : 75 – 83%
(CT : 62.5 %, Push enteroscopy :
44%, colonoscopy : 22%)
Specificity : 37.5%
Positive Predictive Value : 55%
Negative Predictive Value : 60%
Nujaim et al, Gastroenterology Res 2017
Furnari et al, J Gastrointersin Liver Dis 2017
-
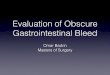
Role of double balloon enteroscopy
Rarely, small bowel
NENs can be diagnosed
only with DBE
* * *#++*
Indications :
- To precisely localize the
primary (-ies) in suspected
small intestinal NENs
- To identify +/- treat the cause of
small bowel bleeding in NENs
DBE vs Capsule endoscopy
DBE identified additional lesions in 62%
of patients in a recent surgical series(82% of them confirmed in
histology)
Gangi et al, J Gastointerstinal Surg 2018
Rossi et al, United European Gastroenterology J 2017
Telese et al, UKI NETS 2017
-
The role of Endoscopic Ultrasound in G-I NENs
Type 1 and 2 gastric NENs: to evaluate the depth of invasion and
indication to endoscopic treatment that is reserved to lesions not
infiltrating beyond the muscularis propria.
Type 3 gastric NENs: to stage the disease by assessing the
presence of regional lymph-node involvement.
To stage duodenal NENs with diameter >2 cm. To exclude
loco-regional lymph node metastases and thus indication for
endoscopic mucosal resection.
To determine the indication of endoscopic removal in Rectal NENS
versus transanal excision or radical surgery, in particular for
those with diameter >2 cm, by assessing depth of invasion and
the presence of lymph node metastases. To follow up patients after
resection.
Zilli at al, Dig Liver Dis 2018
-
The role of Endoscopic Ultrasound
in pancreatic NENsTo differentiate pancreatic NENs
from adenocarcinoma
To localize small pancreatic
NENs, mainly insulinomas or
gastrinoma, before surgery,
especially if other non-invasive
imaging studies are negative
To stage the NEN by evaluating
the presence of vascular invasion
or loco-regional lymph node
To evaluate the distance
between pancreatic lesion and the
main pancreatic duct in a pre-
operative setting, thus predicting
the risk of developing pancreatic
fistulaZilli at al, Dig Liver Dis 2018
Diagnostic accuracy of EUS
• Pooled sensitivity: 87%
• Pooled specificity: 98%
• Mean detection rate: 90% in suspected p NENs
(mean detection rate of CT/MRI : 73%)
• Increased pre-op p NEN detection by 25%
Puli et al, World J Gastroenterol 2013
James et al, Gastrointest Endosc 2015
Manta et al, J Gastrointest Liv Dis 2016
-
Endoscopic management of GEP NENs
-
Type I G-NENs
55-years female with hypothyroidism on
levothyroxin, insulin-dependent diabetes,
pernicious anemia on B12, underwent an
upper GI endoscopy because of
persistent dyspepsia
- “Atrophic mucosa, multiple polyps of
body and fundus < 1 cm, CLO and
biopsies were taken”
- Atrophic gastritis with ECL hyperplasia,
and well differentiated, G1 NET with Ki67 <
2%.
- CLO : + (H. pylori positive)
- Serum Gastrin > 400
- Serum Chromogranin : 82
- Anti-parietal cell Ab : +
- Anti-intrinsic factor Ab: +
-
Management suggestions
Endoscopic polypectomy ?
Annual endoscopic surveillance ?
Commencement of somatostatin
analogues or new agents ?
Gastrectomy ?
-
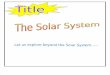
45 years old male
Hypothyroidism
Asthma
Atrophic gastritis
G1 NET
Raised gastrin,
Chromogranin-A
Positive auto-antibodies
One of the polyps is
measuring 1.5 cm
Type I G-NEN
-
Management suggestions
Endoscopic polypectomy ?
Annual endoscopic surveillance ?
Commencement of somatostatin
analogues or new agents ?
The overall metastatic risk is low in type 1 g-NENs and has been
directly
correlated with tumor size (10 mm appearing to be the
cut-off)
Therefore, the minimal approach should be to resect tumors ≥ 10
mm.
Resection should be performed by experienced endoscopists
in gastric tumors using either Endoscopic Mucosal Resection
or
Endoscopic Submucosal Dissection (ESD);
the latter has the benefit of an en bloc resection for complete
histological appraisal.
Delle Fave et al, ENETS Consensus Guidelines, Neuroendocrinology
2016
-
Endoscopic resection in G-NENs
Snare polypectomy, Endoscopic Mucosal Resection (EMR)
or Endoscopic Submucosal Dissection (ESD) ?
33 pts, (polyps 2 – 20 mm), 45% polypectomy with snare.
63.6% had recurrence (within 8 months).
Merola et al, Neuroendocrinology 2011
• 62 pts had either EMR or ESD.
• The overall ESD complete resection rate was
higher than that of the EMR rate (94.9%
versus 83.3%, P value = 0.174).
• A statistically lower vertical margin
involvement rate was achieved when ESD
was performed compared to when EMR was
performed (2.6% versus 16.7%, P value =
0.038).
• The complication rate was not significantly
different between the two groups.
Kim et al, Gastroenterol Res Pract 2014
-
Role of EUS for treatment of p NENs
24 patients with EUS-guided
Ethanol ablation (67%
insulinomas)
7 patients with EUS-guided
RFA (42% insulinomas)
Encouraging results in the
majority of patients
Mild pancreatitis in 20% in
ethanol ablation, no
complications in RFA
Lakhtakia, Clin Endoscopy 2017
-
Take Home messages
Upper and lower GI endoscopy provide the diagnosis of
gastric,
duodenal and rectal NENs
Wireless capsule endoscopy can identify the primary (-ies)
and
cause of obscure GI bleeding in small bowel NENs
Double balloon enteroscopy can localize precisely the primary
(-ies)
in small bowel NENs
EUS can assess the depth of invasion of G-I wall, from a G-I
NEN
prior to endoscopic treatment
EUS can be very important in diagnosis, localization, staging
and
pre-op assessment of p NENs
EMR & ESD are the methods of choice in endoscopic treatment
of
gastric and rectal NENs, when indicated, with ESD being
associated
with higher R0 resection rates
EUS RFA seems promising for endoscopic treatment of
localized
/functional p NENs
-
Thank you