Embed Size (px)
Citation preview
Principals, Approaches and Tools
for Stigma-Reduction in
Health Facilities
Laura Nyblade, PhDSenior Technical Advisor, Stigma &
DiscriminationHealth Policy Project and RTI
BackgroundWhyDefinitions & ConceptualizationForms & consequences
Overview of general stigma-reduction program strategies
Examples of how they have been applied in health care settings
Tools & Resources
Presentation “Guide”
“…. If we do not appreciate the natureand impact of stigma,
none of our interventions can begin
to be successful.”– Edward Cameron,
Constitutional Court Justice in South Africa
Powerful social process that:Turns “difference” into inequity & disadvantage
Maintains/upholds inequitable structuresLeads to social & economic exclusion Fuels and can be used to justify violations of human rights, discriminatory policies & laws
Intensifies & sustains vulnerabilityImpedes access to health & other services
Why?
Stigma impedes programmatic efforts
Prevention Testing Disclosure Risk Recognition Treatment
Treatment Access Timely uptake Adherence Delivery/Quality of Care Human Capital
Health care providers receiving care
Secondary S&D
Forms-Impact on People’s Lives
Physical and social isolationLoss of relationshipsGossip & Verbal AbuseLoss of livelihoodLoss of housingRejection by peersLoss of reputationViolenceDenial or sub-standard health careInternalized stigma
Forms-Health ProvidersStigma Indicators Working Group, Tanzania, 2005
Neglect Had to wait longer Not having bed pans
changed Receiving less care/attention
Denied care Denied treatment Referral to another
provider/faci l i ty Senior provider pushed cl ient to a
junior provider Junior provider pushed cl ient to a
senior providerDifferential treatment HIV test required before
care was given HIV test required before
scheduling surgery Using gloves for non-
invasive exams Extra precautions in
steri l izing instruments
Lack of consent HIV testing without consent Disclosing HIV status to
family without cl ient’s consent
Verbal stigma • Gossip about a client’s HIV
status• Scolding or blaming a client
“…I overheard two nurses talking about me…. that I am HIV positive. After having the baby, they put me in a separate room, no one came to look after me. …When I went home, family members refused to let me stay there. I had to rent my own room and stay alone with my baby and no one from the family came to see me. ….As soon as our customers learned that we are HIV positive, they stopped coming and our business collapsed.”
Shared in an ISDS/ICRW stigma-reduction workshop, 2002
Definitions and Conceptualization
“An attribute that is deeply discrediting [and that reduces the bearer] …from a whole and usual person to a tainted, discounted one.”
By regarding “others” negatively, an individual or group confirms their own “normalcy” and legitimizes their devaluation of the “other.”
“Disqualification from full social acceptance”
Stigma-Goffman, 1963
Social Process (Link & Phelan, 2001)
Distinguish & label differencesAssociate negative attributes to perceived differences
Separation of ‘us’ from ‘them’Status loss & discrimination
Unfair and unjust treatment of an individual based on the basis of the:real or perceived status or attribute (e.g. medical condition)
belonging, or being perceived to belong, to a particular group (UNAIDS)
Discrimination
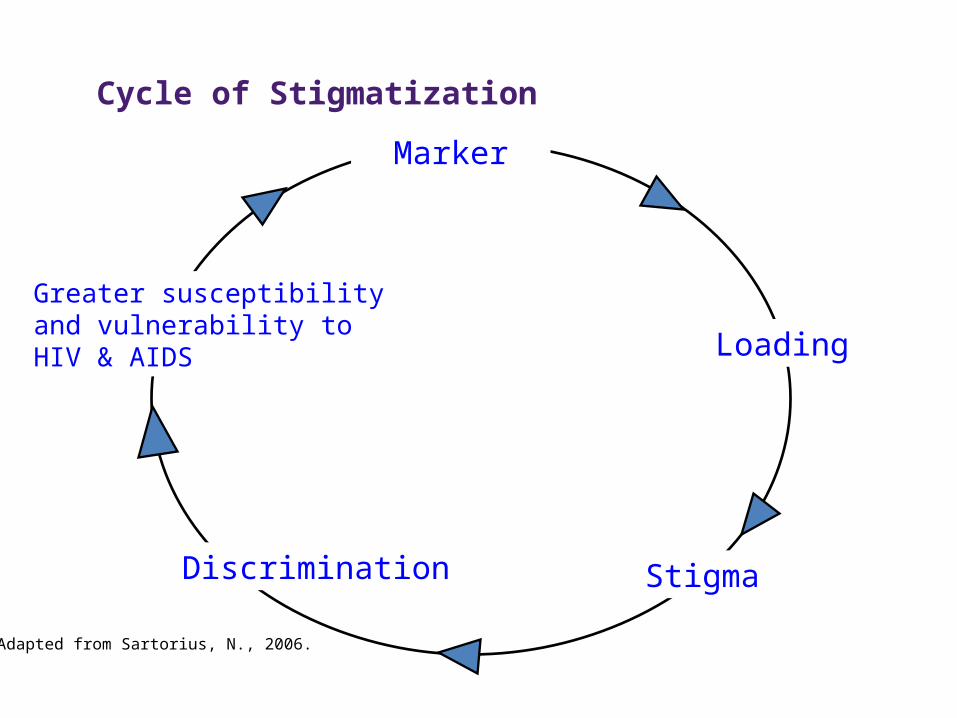
Adapted from Sartorius, N., 2006.
Cycle of Stigmatization
Discrimination
Marker
Greater susceptibility and vulnerability to HIV & AIDS
Stigma
Loading
What works to reduce HIV Stigma and Discrimination
Put stigmatized groups at the core
Target a range of groups; Create alliances & form new partnerships for influence and expanded reach Foster interaction between groups experiencing stigma
& those perpetrating it. “Contact strategies”
Model desirable behavior, hold up & reward role models
Employ a combination of approaches, while targeting a range of groups
Address immediately actionable drivers
Successful programs
Foster understanding and motivation for stigma reduction by creating:–Recognition of stigma –The benefits of reducing it–Safe space to reflect and gain skills for change
Create Understanding: Close the Intention-Action Gap

Address HIV Transmission Fears & MisconceptionsHow it is and is not transmittedIn-depth informationInteractively: Allow for • “Yes I know that, but why…?”
Listen, learn & respond to specific fears related to daily living & work context
Discuss and Challenge the ‘Taboo’ Provide safe spaces to discuss,
reflect, understand and question:– The values and beliefs that underlie
stigma and discrimination Where they come from What they do
– Address the multiple intersecting & associated stigmas of HIV
– Sex workers, men who have sex with men, drug users
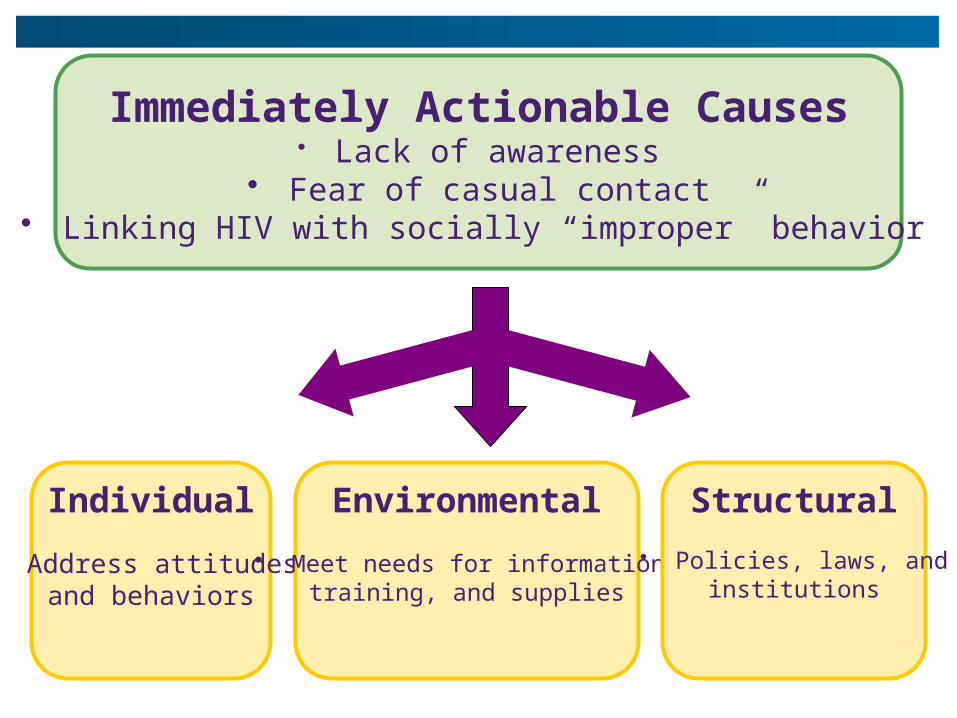
Individual
• Address attitudes and behaviors
Immediately Actionable Causes• Lack of awareness
• Fear of casual contact• Linking HIV with socially “improper” behavior
Environmental
• Meet needs for information,training, and supplies
Structural
• Policies, laws, andinstitutions
Stigma & Discrimination-
Reduction program in Health Services
Some examples
Building institutional Support for change in Vietnam (Horizons/ISDS/ICRW)
Relationship building with hospital authoritiesConducted & shared Baseline Research ResultsTrained all cadres on:
Fear Driven Stigma: HIV transmission and universal precautions
Socially Driven Stigma (“blame & “shame”)Tools Development: Checklist, toolkitParticipatory development of hospital policiesImprovements in structural environment
E.g. hand-washing facilities, sharps containers
Training
4 half-days½ day basic HIV knowledge1 day on Universal Precautions½ day on social stigma co-facilitated by PLHIVNaming stigma through picturesWhat is the meaning of stigmaNaming stigma in hospitals
Forms, Causes, ConsequencesHow it feels to be stigmatized
Each trained group developed their own policy & presented it in plenary to hospital
Steering committee took all comments & combined for final hospital policyAccess to services by PLHIVHIV counseling and testingConfidentialityUniversal PrecautionsTraining on HIV and AIDSDissemination of policy
Posters of policy posted throughout hospitals
Joint development of “Safe and Friendly” hospital policies
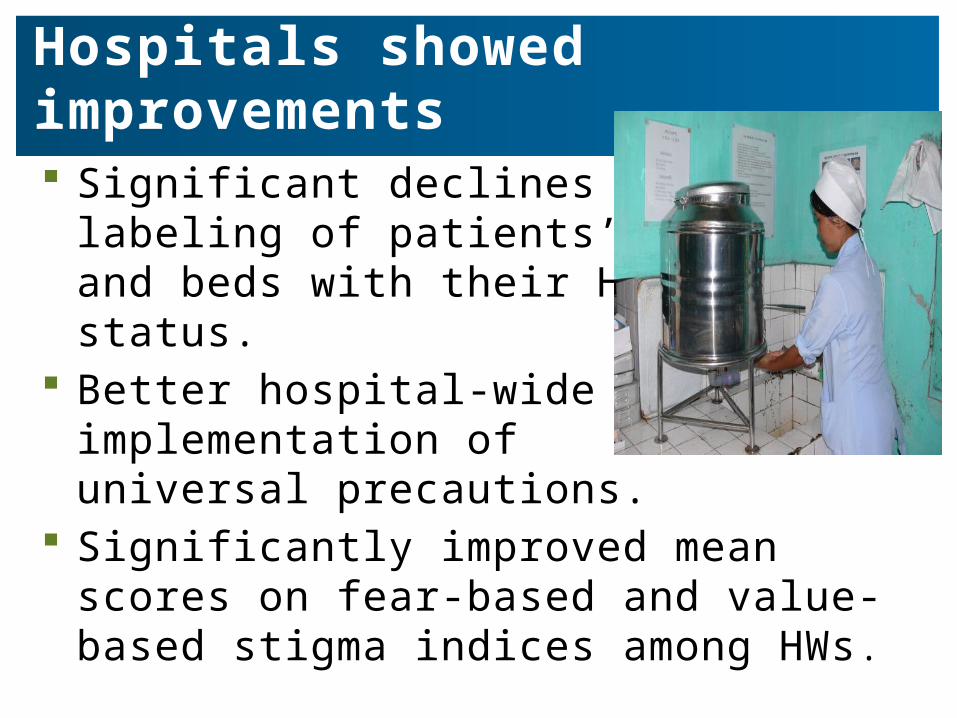
Hospitals showed improvements
Significant declines in the labeling of patients’ files and beds with their HIV status.
Better hospital-wide implementation of universal precautions.
Significantly improved mean scores on fear-based and value-based stigma indices among HWs.
Building institutional Support for change
Partnering with hospitals as partners not critics
Participatory approaches; evidence of need/problem
Involving all categories of hospital staff
Inclusion of people living with HIV as co-facilitators
Development of practical tools

Creating partnerships &
reducing distance between health
care providers and stigmatized clients
Reducing Stigma & Discrimination Towards Sex Workers
Ashodaya-Samithi, Mysore, India
• Trained Peer Patient advocates placed in Public Hospitals
• Sex workers found easier to access services
• Opportunity for increased contact and understanding
Swathi Mahila Sangha & partners, Bangalore, India
• Ensuring Dignity and Rights among Sex Workers in Bangalore
• Rose Campaign– Hold up & ‘reward’
positive behavior– Opened space for
dialogue

Resources
General Tools• Challenging & Addressing
Stigma towards– People living with HIV– Men who have sex with men– Sex workers– Drug users
• Guidance Documents
Health Care Specific
• Safe & Friendly Health Facility Trainers Guide (ISDS/ICRW/Horizons tools, Vietnam)
• Reducing Stigma and Discrimination Related to HIV and AIDS: Training for Health Care Workers (Engender Health)
• Reducing HIV Stigma & Gender Based Violence: Toolkit for Health Care Providers in India (ICRW/BPWT/Levi Strauss Foundation)
• Global Stigma-Reduction toolkit for health care settings (Draft)

Stigma Action Network‘Working for a World Free of
HIV-related Stigma’
www.stigmaactionnetwork.org
SAN Mission & Goals
‘To reduce HIV-related stigma and discrimination through a dynamic network that will catalyze action and commitment locally, regionally and globally through knowledge sharing, dialogue and partnerships’
1. Bring together diverse stakeholders to share experiences, best practices, knowledge, tools, and research around HIV-related stigma and discrimination.
2. Facilitate innovative solutions and expand the reach of best and promising practices to reduce HIV-related stigma and discrimination.
3. Promote research across disciplines to expand the evidence base for HIV-related stigma and discrimination reduction efforts

How can you participate?
• Join the network:– Go to www.stigmaactionnetwork.org– Click on the ‘Join Us’ link in the top right-hand corner
and register– Log-in to the site and create your member profile and
organization profile• Share materials & resources for posting on web site
– Upload documents, weblinks and events via the CONTRIBUTE box
– Post to the SAN blog – Participate in the discussion forum
• Participate in our upcoming e-survey– Share your ideas about how best to expand the website– Forthcoming in August, 2011
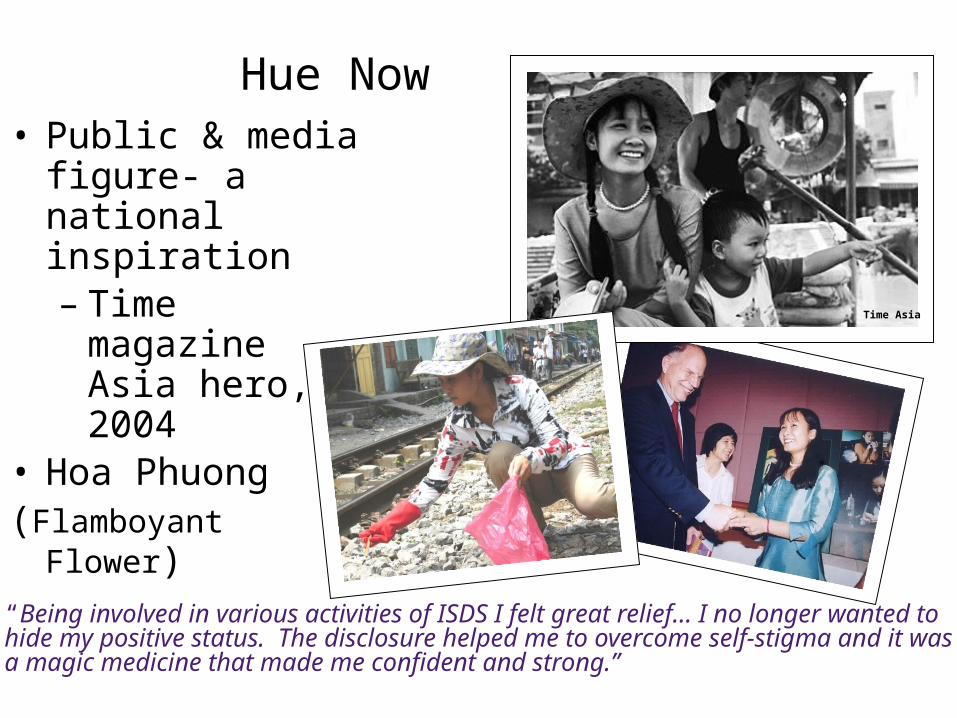
Hue Now• Public & media
figure- a national inspiration– Time magazine
Asia hero, 2004• Hoa Phuong(Flamboyant Flower)
“Being involved in various activities of ISDS I felt great relief… I no longer wanted to hide my positive status. The disclosure helped me to overcome self-stigma and it was a magic medicine that made me confident and strong.”
Time Asia
www.healthpolicyproject.com
Thank You!
The Health Policy Project is a five-year cooperative agreement funded by the U.S. Agency for International Development (USAID) under Cooperative Agreement No. AID-OAA-A-10-00067, beginning September 30, 2010. It is implemented by Futures Group, the Centre for Development and Population Activities (CEDPA), Futures Institute, Partners in Population and Development Africa Regional Office (PPD ARO), Population Reference Bureau (PRB), Research Triangle Institute (RTI) International, and the White Ribbon Alliance for Safe Motherhood (WRA)





























