Embed Size (px)
Citation preview
Principal results of the Prospective comparison of Angiotensin Receptor
neprilysin inhibitor with Angiotensin Receptor blocker MEasuring arterial sTiffness in the eldERly
(PARAMETER) Study
B. Williams,1 JR. Cockcroft,2 K. Kario,3 DH. Zappe,4 Q. Wang,5 W. Guo4 1University College London, London, UK, 2Cardiff University, Wales, UK, 3Jichi Medical School, Tochigi, Japan, 4Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA, 5Beijing Novartis Pharma Co. Ltd, Shanghai, China.
Clinical Trials Identifier: EUDract number 2012-002899-14; ClinicalTrials.gov NCT01692301
Study code: CLCZ696A2216
Protocol: Williams B. et al, BMJ Open, 2014
• Systolic hypertension and an increased pulse pressure (PP) are indicative of arterial ageing and large artery stiffening
• Systolic hypertension and an increased PP are also predictive of incident cardiovascular disease and heart failure - especially nocturnal hypertension
• Large artery stiffness also increases central aortic systolic pressure (CASP) and central aortic pulse pressure (CPP) relative to brachial blood pressure, which increases left ventricular loading conditions and this abnormal ventricular:vascular coupling contributes to the development of heart failure
• The purpose of the PARAMETER study was to assess both the short and long-term effects (12 and 52 weeks) of LCZ696, an angiotensin receptor neprilysin inhibitor, compared with olmesartan an angiotensin receptor blocker, on measures of central aortic hemodynamics and arterial stiffness in older patients with systolic hypertension and an increased PP
3
Background
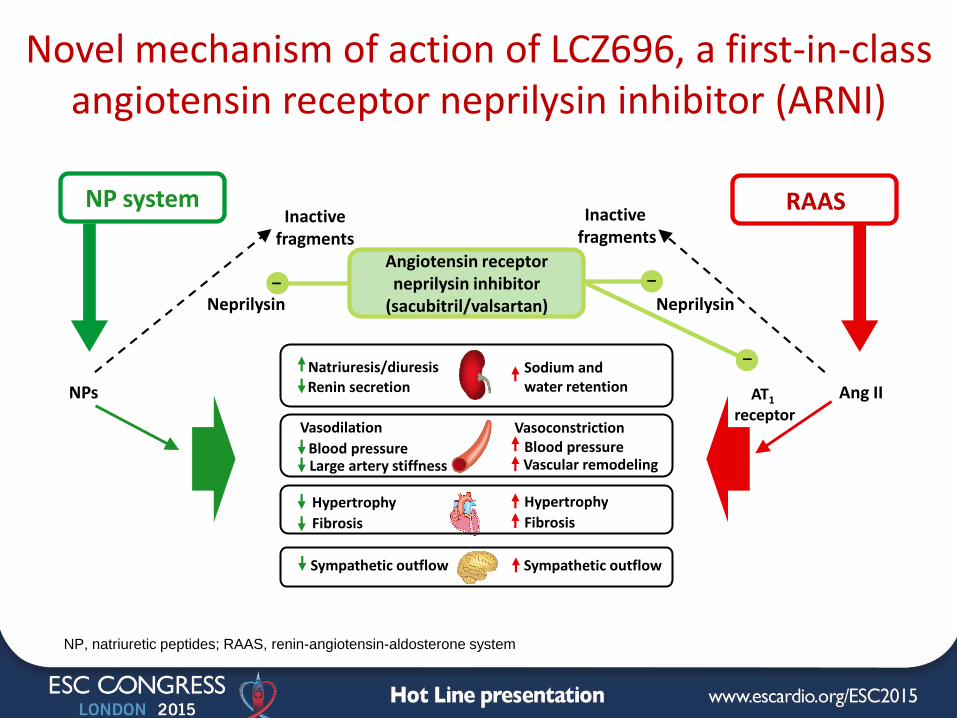
Novel mechanism of action of LCZ696, a first-in-class angiotensin receptor neprilysin inhibitor (ARNI)
NP system
Angiotensin receptor neprilysin inhibitor
(sacubitril/valsartan)
RAAS Inactive
fragments
Inactive fragments
Neprilysin
NPs Ang II AT1 receptor
Neprilysin – –
– Natriuresis/diuresis Sodium and
water retention Renin secretion
Vasodilation
Blood pressure
Hypertrophy
Fibrosis
Large artery stiffness
Sympathetic outflow
Vasoconstriction Blood pressure
Hypertrophy
Fibrosis
Sympathetic outflow
Vascular remodeling
NP, natriuretic peptides; RAAS, renin-angiotensin-aldosterone system
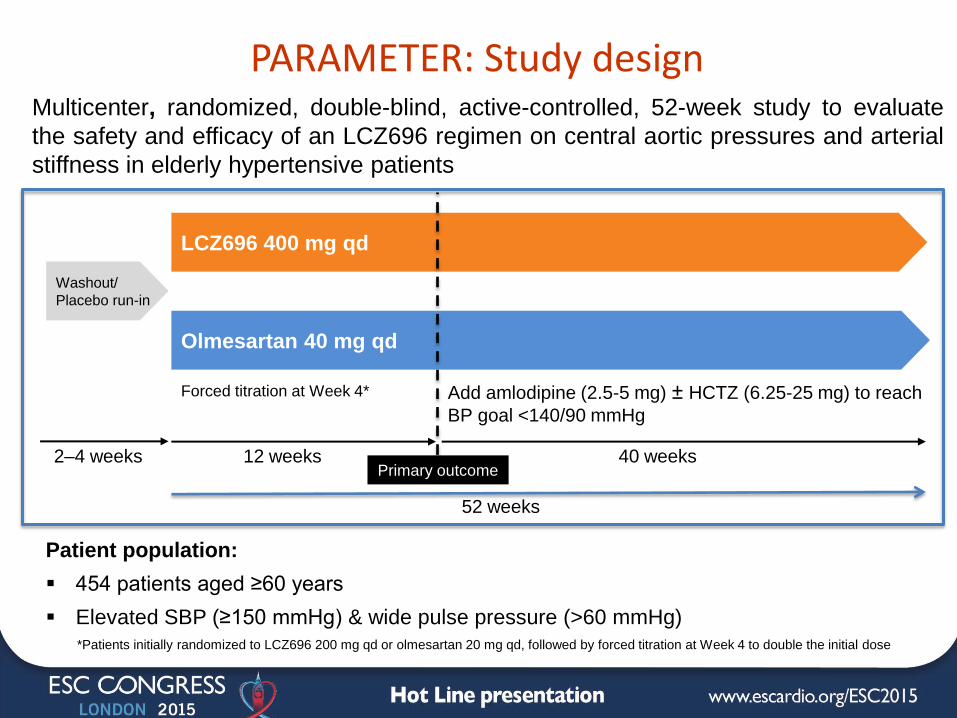
PARAMETER: Study design
Patient population:
454 patients aged ≥60 years
Elevated SBP (≥150 mmHg) & wide pulse pressure (>60 mmHg)
2–4 weeks
Olmesartan 40 mg qd
LCZ696 400 mg qd
12 weeks
Washout/
Placebo run-in
40 weeks
Add amlodipine (2.5-5 mg) ± HCTZ (6.25-25 mg) to reach
BP goal <140/90 mmHg
Multicenter, randomized, double-blind, active-controlled, 52-week study to evaluate
the safety and efficacy of an LCZ696 regimen on central aortic pressures and arterial
stiffness in elderly hypertensive patients
52 weeks
Primary outcome
*Patients initially randomized to LCZ696 200 mg qd or olmesartan 20 mg qd, followed by forced titration at Week 4 to double the initial dose
Forced titration at Week 4*
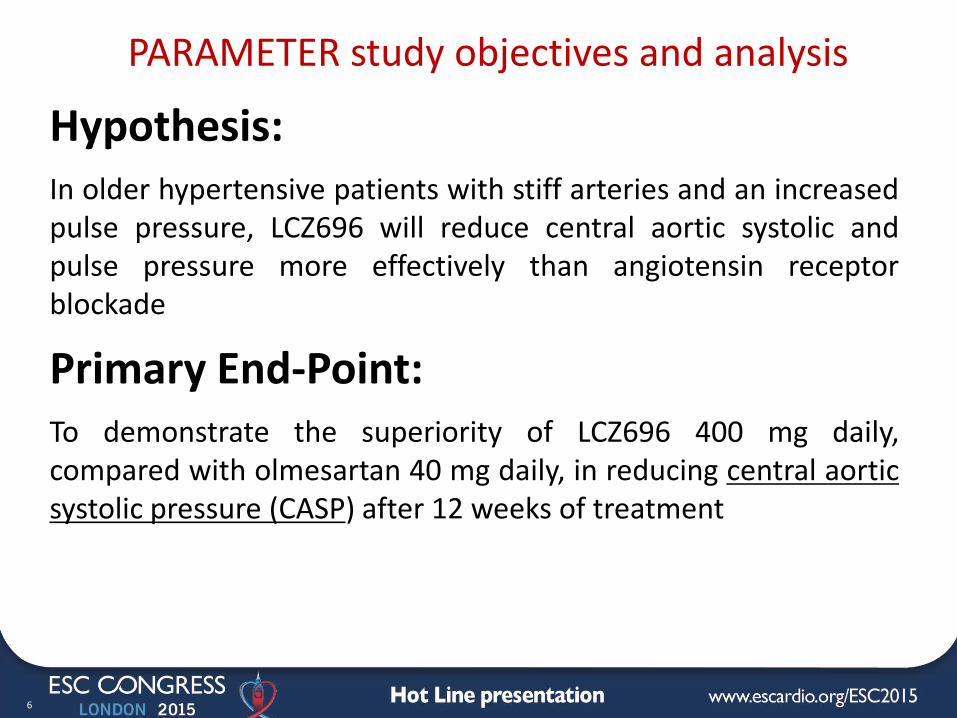
PARAMETER study objectives and analysis
6
Hypothesis: In older hypertensive patients with stiff arteries and an increased pulse pressure, LCZ696 will reduce central aortic systolic and pulse pressure more effectively than angiotensin receptor blockade
Primary End-Point: To demonstrate the superiority of LCZ696 400 mg daily, compared with olmesartan 40 mg daily, in reducing central aortic systolic pressure (CASP) after 12 weeks of treatment
7
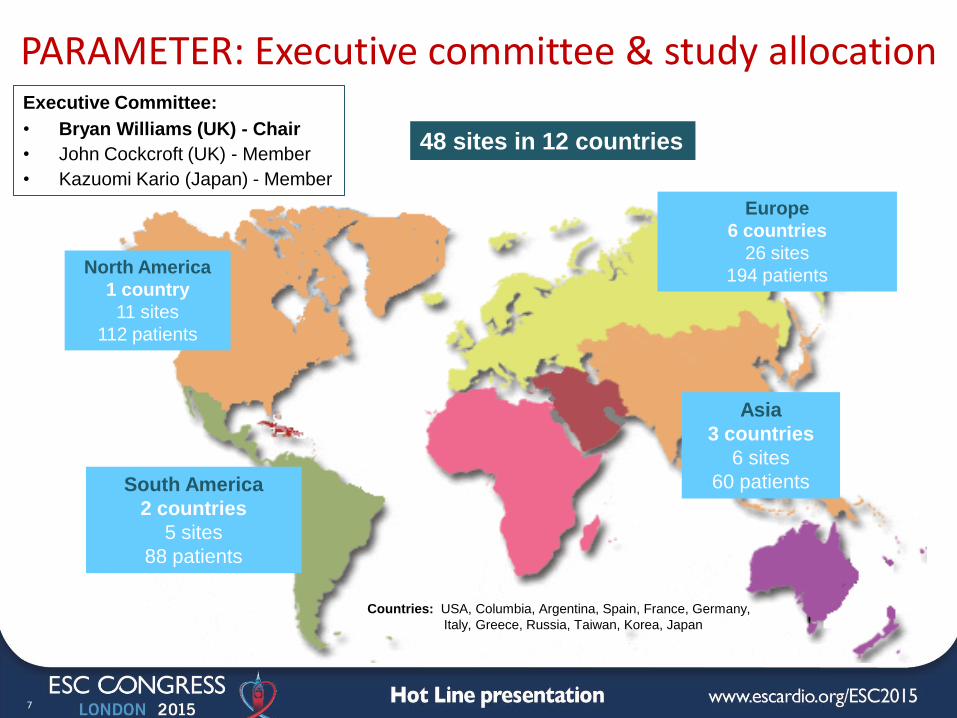
North America
1 country
11 sites
112 patients
South America
2 countries
5 sites
88 patients
Europe
6 countries
26 sites
194 patients
Asia
3 countries
6 sites
60 patients
PARAMETER: Executive committee & study allocation Executive Committee:
• Bryan Williams (UK) - Chair
• John Cockcroft (UK) - Member
• Kazuomi Kario (Japan) - Member
48 sites in 12 countries
Countries: USA, Columbia, Argentina, Spain, France, Germany,
Italy, Greece, Russia, Taiwan, Korea, Japan
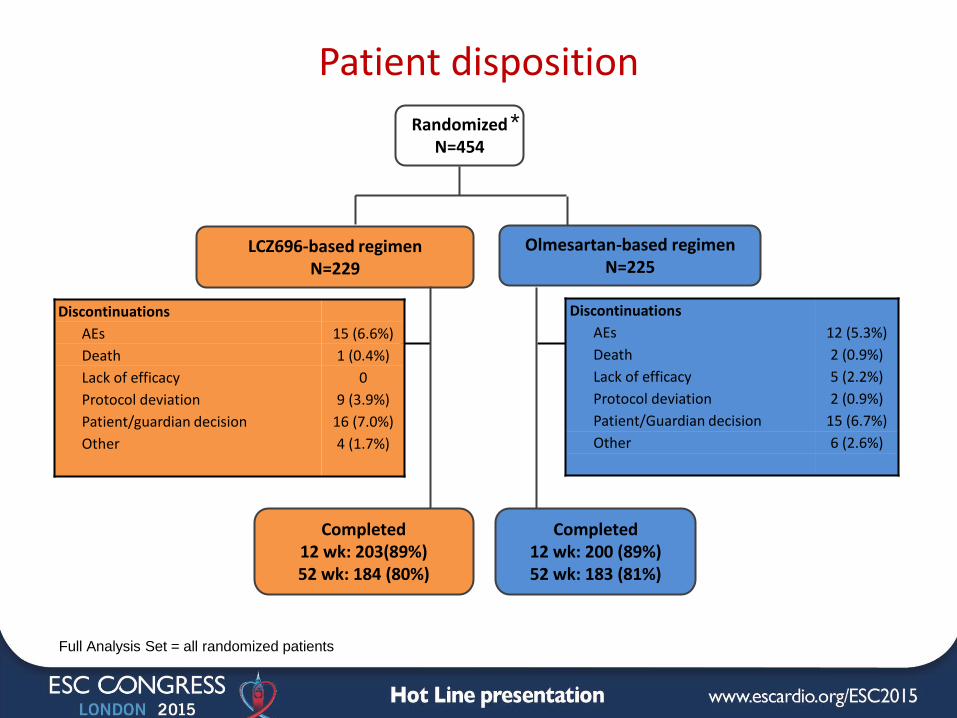
Patient disposition
* Randomized N=454
LCZ696-based regimen N=229
Olmesartan-based regimen N=225
Completed 12 wk: 203(89%) 52 wk: 184 (80%)
Discontinuations
AEs 15 (6.6%)
Death 1 (0.4%)
Lack of efficacy 0
Protocol deviation 9 (3.9%)
Patient/guardian decision 16 (7.0%)
Other 4 (1.7%)
Completed 12 wk: 200 (89%) 52 wk: 183 (81%)
Discontinuations
AEs 12 (5.3%)
Death 2 (0.9%)
Lack of efficacy 5 (2.2%)
Protocol deviation 2 (0.9%)
Patient/Guardian decision 15 (6.7%)
Other 6 (2.6%)
Full Analysis Set = all randomized patients
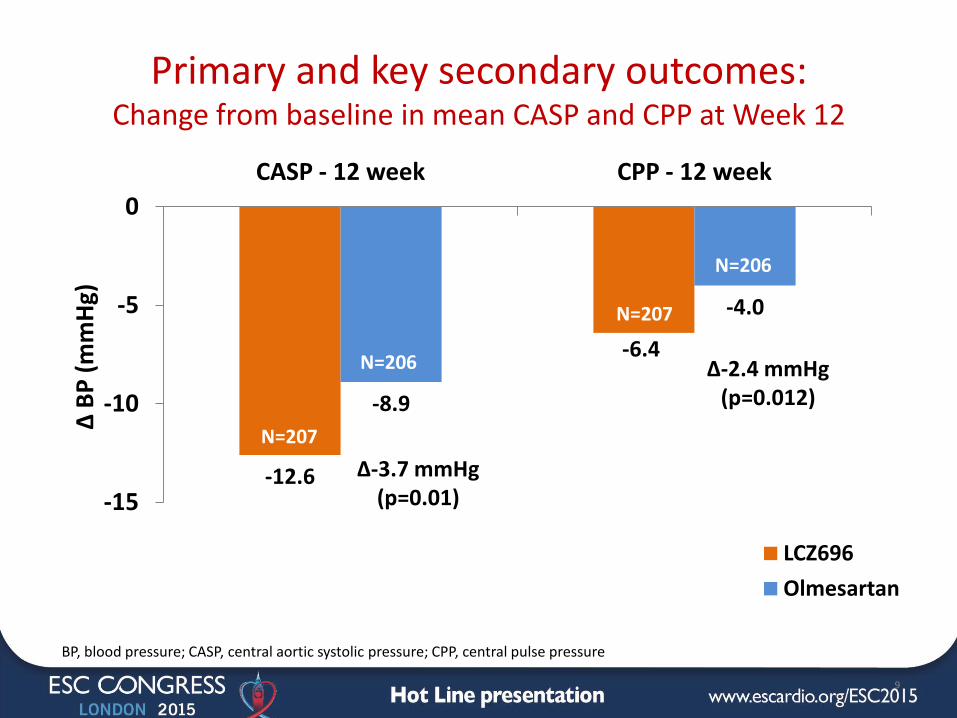
-12.6
-6.4
-8.9
-4.0
-15
-10
-5
0
CASP - 12 week CPP - 12 week
∆ B
P (
mm
Hg)
LCZ696
Olmesartan
Primary and key secondary outcomes: Change from baseline in mean CASP and CPP at Week 12
9
∆-2.4 mmHg (p=0.012)
∆-3.7 mmHg (p=0.01)
BP, blood pressure; CASP, central aortic systolic pressure; CPP, central pulse pressure
N=207
N=207
N=206
N=206
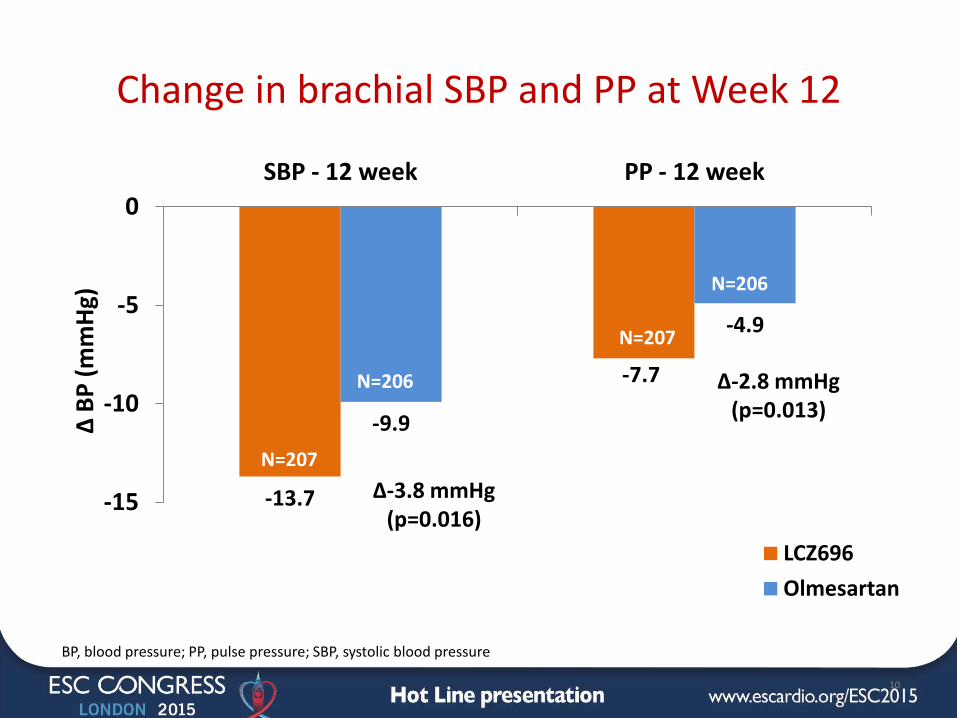
-13.7
-7.7
-9.9
-4.9
-15
-10
-5
0
SBP - 12 week PP - 12 week
∆ B
P (
mm
Hg)
LCZ696
Olmesartan
∆-3.8 mmHg (p=0.016)
Change in brachial SBP and PP at Week 12
10
∆-2.8 mmHg (p=0.013)
BP, blood pressure; PP, pulse pressure; SBP, systolic blood pressure
N=207
N=207
N=206
N=206
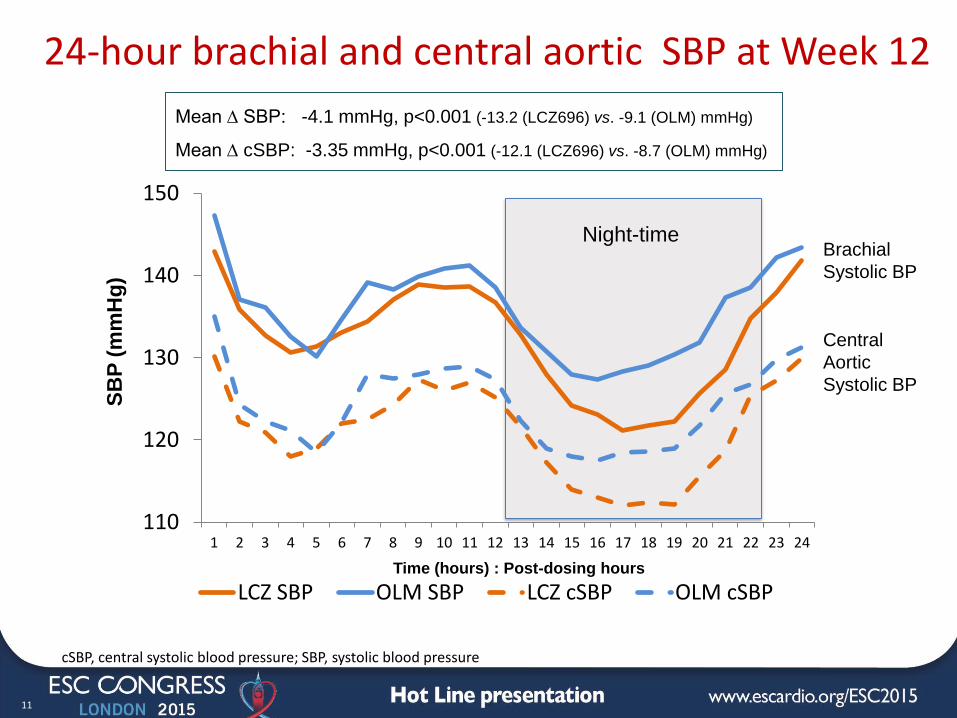
110
120
130
140
150
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
LCZ SBP OLM SBP LCZ cSBP OLM cSBP
11
24-hour brachial and central aortic SBP at Week 12
SB
P (
mm
Hg
)
Night-time
Time (hours) : Post-dosing hours
cSBP, central systolic blood pressure; SBP, systolic blood pressure
Mean ∆ SBP: -4.1 mmHg, p<0.001 (-13.2 (LCZ696) vs. -9.1 (OLM) mmHg)
Mean ∆ cSBP: -3.35 mmHg, p<0.001 (-12.1 (LCZ696) vs. -8.7 (OLM) mmHg)
Brachial
Systolic BP
Central
Aortic
Systolic BP
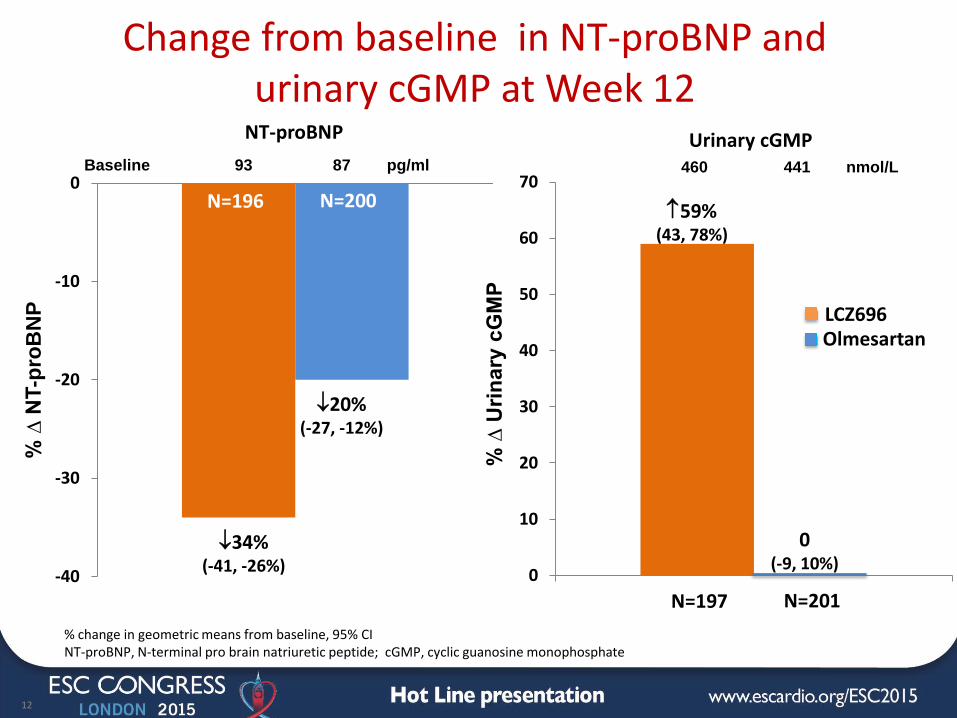
Change from baseline in NT-proBNP and urinary cGMP at Week 12
-40
-30
-20
-10
0
12
% ∆
NT-p
roB
NP
%
∆ U
rin
ary
cG
MP
0
10
20
30
40
50
60
70 Baseline 93 87 pg/ml 460 441 nmol/L
NT-proBNP Urinary cGMP
34% (-41, -26%)
20% (-27, -12%)
59% (43, 78%)
0 (-9, 10%)
% change in geometric means from baseline, 95% CI NT-proBNP, N-terminal pro brain natriuretic peptide; cGMP, cyclic guanosine monophosphate
LCZ696 Olmesartan
N=196 N=200
N=197 N=201
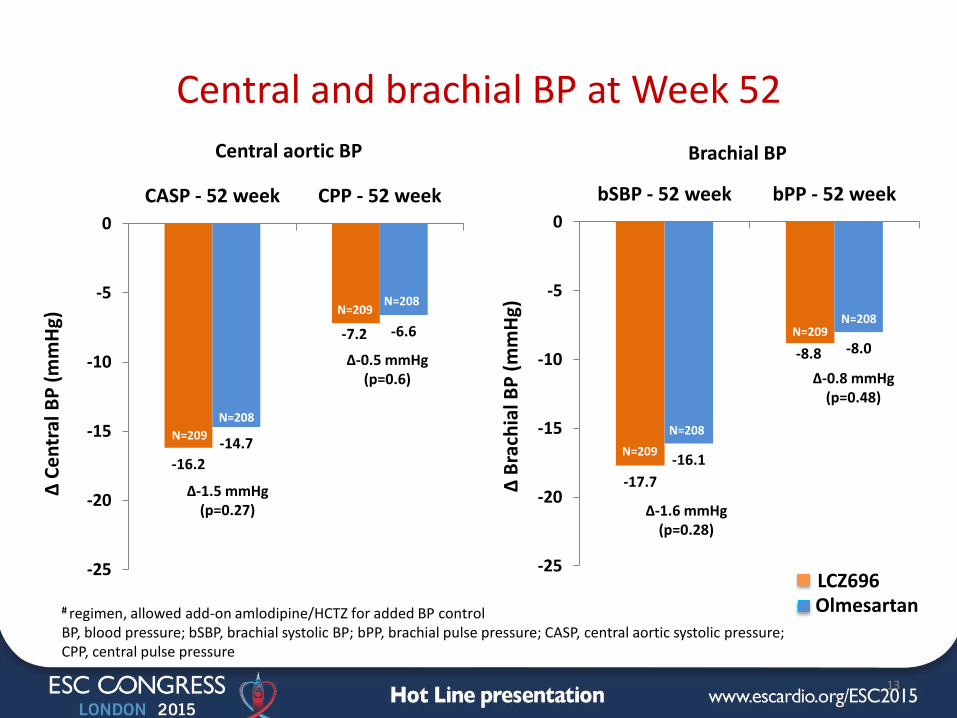
# regimen, allowed add-on amlodipine/HCTZ for added BP control BP, blood pressure; bSBP, brachial systolic BP; bPP, brachial pulse pressure; CASP, central aortic systolic pressure; CPP, central pulse pressure
-16.2
-7.2
-14.7
-6.6
-25
-20
-15
-10
-5
0
CASP - 52 week CPP - 52 week
∆ C
en
tral
BP
(m
mH
g)
Central and brachial BP at Week 52
13
-17.7
-8.8
-16.1
-8.0
-25
-20
-15
-10
-5
0
bSBP - 52 week bPP - 52 week
∆ B
rach
ial B
P (
mm
Hg)
Brachial BP Central aortic BP
∆-1.5 mmHg (p=0.27)
∆-0.5 mmHg (p=0.6) ∆-0.8 mmHg
(p=0.48)
∆-1.6 mmHg (p=0.28)
LCZ696 Olmesartan
N=209
N=209
N=209
N=209
N=208
N=208
N=208
N=208
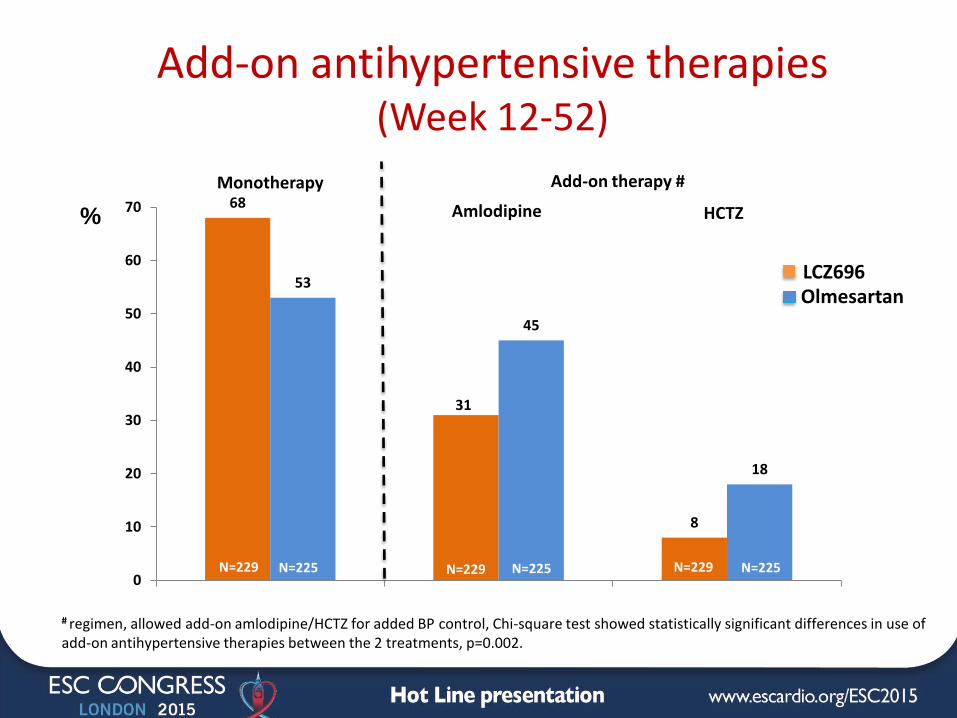
68
31
8
53
45
18
0
10
20
30
40
50
60
70
Monotherapy
%
Add-on antihypertensive therapies (Week 12-52)
Add-on therapy #
Amlodipine HCTZ
LCZ696 Olmesartan
N=229 N=229 N=229 N=225 N=225 N=225
# regimen, allowed add-on amlodipine/HCTZ for added BP control, Chi-square test showed statistically significant differences in use of add-on antihypertensive therapies between the 2 treatments, p=0.002.
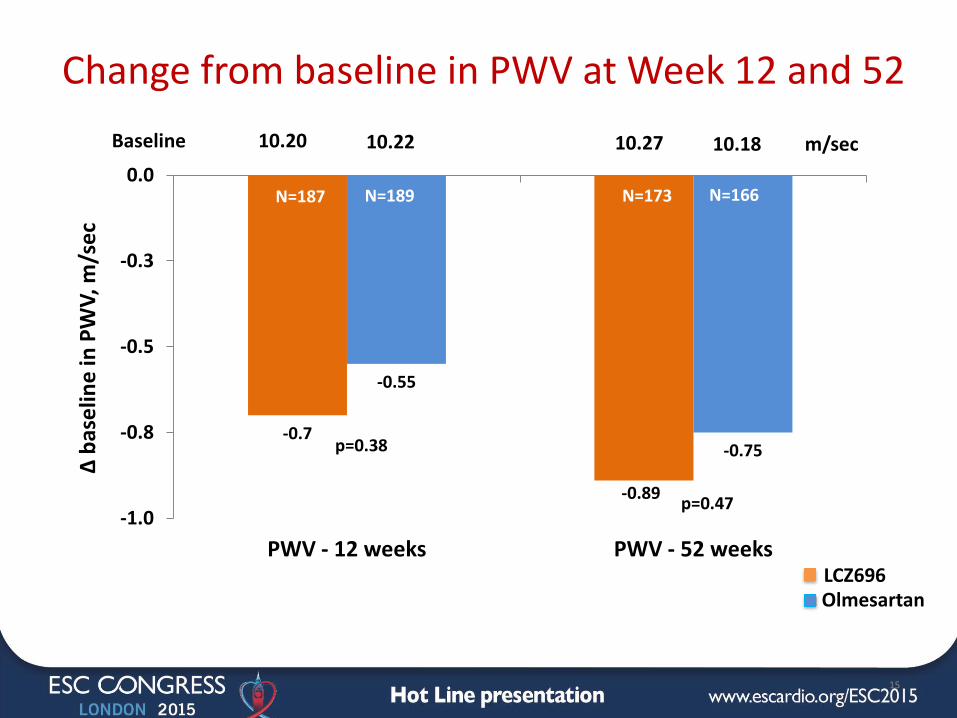
Change from baseline in PWV at Week 12 and 52
-0.7
-0.89
-0.55
-0.75
-1.0
-0.8
-0.5
-0.3
0.0
PWV - 12 weeks PWV - 52 weeks
∆ b
ase
line
in P
WV
, m/s
ec
15
p=0.38
p=0.47
10.20 10.27 10.22 10.18 m/sec Baseline
LCZ696 Olmesartan
N=187 N=189 N=173 N=166
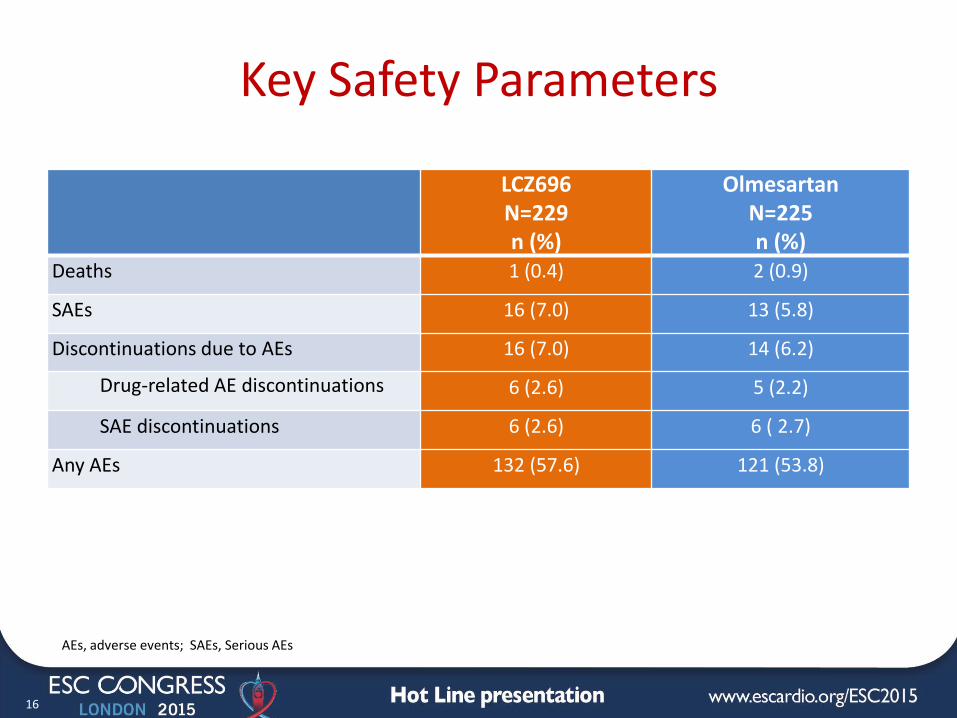
Key Safety Parameters
LCZ696 N=229 n (%)
Olmesartan N=225 n (%)
Deaths 1 (0.4) 2 (0.9)
SAEs 16 (7.0) 13 (5.8)
Discontinuations due to AEs 16 (7.0) 14 (6.2)
Drug-related AE discontinuations 6 (2.6) 5 (2.2)
SAE discontinuations 6 (2.6) 6 ( 2.7)
Any AEs 132 (57.6) 121 (53.8)
16
AEs, adverse events; SAEs, Serious AEs
Summary
17
In older patients with systolic hypertension and an increased pulse pressure, indicative of arterial stiffening:
• The PARAMETER study met its primary and key secondary objectives by demonstrating superior efficacy of LCZ696 400 mg/day, compared to olmesartan 40 mg/day, in lowering both CASP and CPP after 12-weeks monotherapy
• LCZ696 also lowered 24-hour ambulatory SBP compared to olmesartan after 12-week monotherapy, with more significant BP reduction observed during the night-time period
• There was no difference between the two regimens in central and brachial BP profiles at Week 52 due to the allowance of add-on antihypertensive therapy; however, a higher percentage of patients in the olmesartan group requiring add-on amlodipine and/or HCTZ
Conclusions
18
• PARAMETER is the first randomized study demonstrating the ability of LCZ696 to reduce central BP and PP, more effectively than an ARB, in high-risk older patients with systolic hypertension and an increased pulse pressure
• These results suggest that LCZ696 provides beneficial effects on central aortic hemodynamics and function, that could provide a therapeutic advantage beyond those observed with RAS blockade alone
Acknowledgements
N. America (US) • H. Resnick
• G. Sack
• T.R. Smith
• M.E. Trevino
• A.L. Phillips
• D.H. Sugimoto
• J.I. Fidelholtz
• S.C. Gorton
• V.E. Miller, A. Salahudeen, V. Garcia-Fragoso
• J. Mersey • J.L. Izzo
S. America • C.R. Majul (AG) • O.R. Montana (AG) • D. Piskorz (AG) • M. Urina (CO)
• A. Cadena (CO)
Europe
• R.E. Schmieder (DE)
• J. Scholze (DE)
• L. Sans (ES)
• J. Olivan (ES)
• C. Calvo (ES)
• J.M. Pascual (ES)
• P. Gomez (ES)
• L. Ruilope, J. Segura (ES)
• J.L. Zamorano (ES)
• A. de la Sierra (ES)
• S. Narejos (ES)
• L.P. Fernandez (ES)
• G. Chironi (FR)
• K. Tsioufis (GR)
• A. Spanos (GR)
• M. Doumas (GR)
• S. Taddei (IT)
• M. Destro (IT)
• L. Mos (IT)
• Z.D. Kobalava (RU)
• S.Y. Martsevich (RU)
• L.I. Pavlova (RU)
• E.I. Barnova (RU)
• A.O. Konrady (RU)
• T.V. Treshkur (RU)
• M.E. Mozheiko (RU)
Asia
• S. Hoshide (JP)
• H. Lee (KR)
• S. Ihm (KR)
• K-C. Chang (TW)
• C-H. Chen (TW)
• B-H. Tzeng (TW)
We would like to thank the patients, the clinic staff and all of the
investigators listed below, who contributed to this study