Embed Size (px)
DESCRIPTION
Primer for APN Nephrology Practice or CNN-NP Certification Preparation. Renal Anatomy/Physiology Linda Shenton, MN, RN, ACNP, CNN-NP. References. ANNA Certification Review ANNA Certification Study Guide ANNA Core Curriculum KDOQI KDIGO National Kidney Foundation - PowerPoint PPT Presentation
Citation preview
Primer for APN Nephrology Practice or CNN-NP Certification Preparation
Renal Anatomy/PhysiologyLinda Shenton, MN, RN, ACNP, CNN-NP
References
•ANNA Certification Review •ANNA Certification Study Guide•ANNA Core Curriculum•KDOQI•KDIGO•National Kidney Foundation•Renal Physicians Association
Objectives
1.Interpret key lab and clinical data to develop the diagnosis of renal disease
2.Explain factors that contribute to chronic kidney disease and progression of renal disease and or AKI
3.Develop treatment strategies for management of a person with CKD
Kidney - Anatomy
1. 2 kidneys 150 grams each2. Size 5-7cm wide, 11-13cm long 3. Blood Supply: 1,200 ml/minute or
approximately 25% of CO4. Nephron 1 Million per kidney 5. Efferent arteriole/afferent arteriole6. Tubules
Basic Renal Anatomy
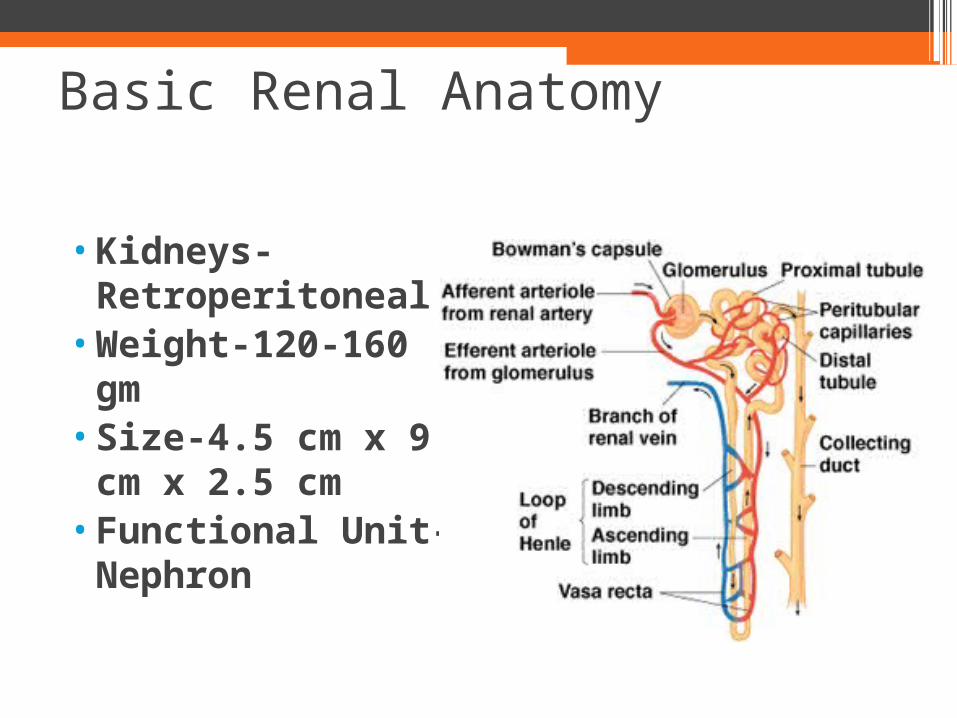
•Kidneys-Retroperitoneal
•Weight-120-160 gm
•Size-4.5 cm x 9 cm x 2.5 cm
•Functional Unit- Nephron
Nephron
•Filters the blood of it’s small molecules and ions
•Reclaims the amount of useful materials Did you Know?
In 24 hrs the kidneys reclaim•1,300g of NaCl•400 g NaHCO3•180 g Glucose
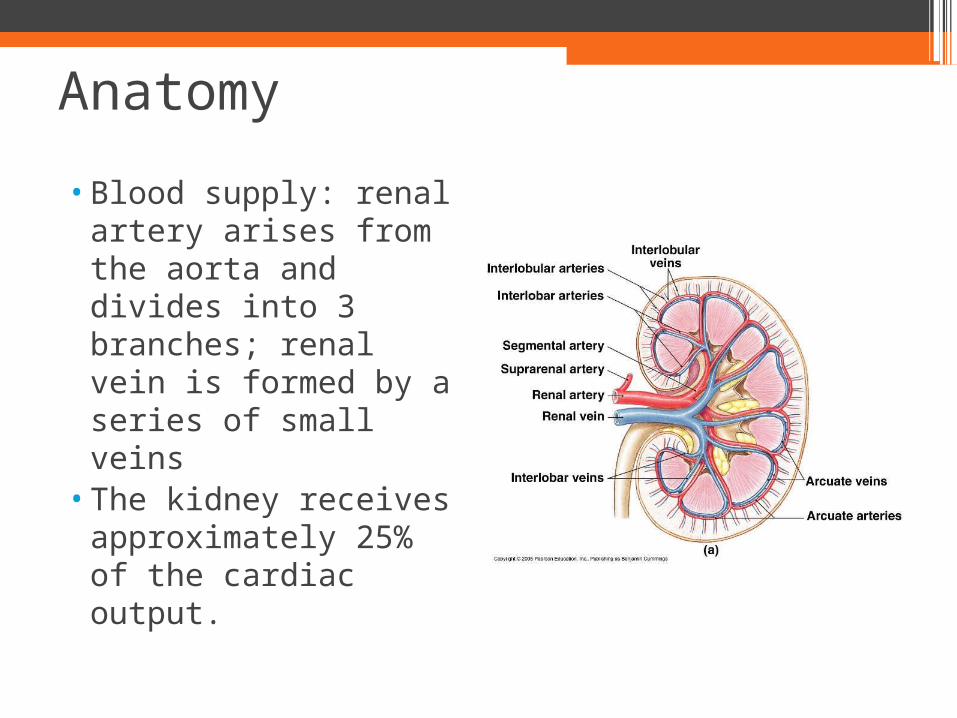
Anatomy
•Blood supply: renal artery arises from the aorta and divides into 3 branches; renal vein is formed by a series of small veins
•The kidney receives approximately 25% of the cardiac output.
Blood Supply
•Afferent artery supplies blood to the kidney
•Efferent artery returns blood to the systemic circulation
•Total blood volume circulates through the kidneys every 5 minutes
Functions of Healthy Kidney
1. Regulation of water and inorganic ion balance
2. Removal of metabolic waste products3. Removal of chemical toxins and drugs4. Regulates acid base balance of body fluids5. Production of hormones/enzymes
a) Erythropoietinb) Reninc) 1,25-dihydroxyvitamin D
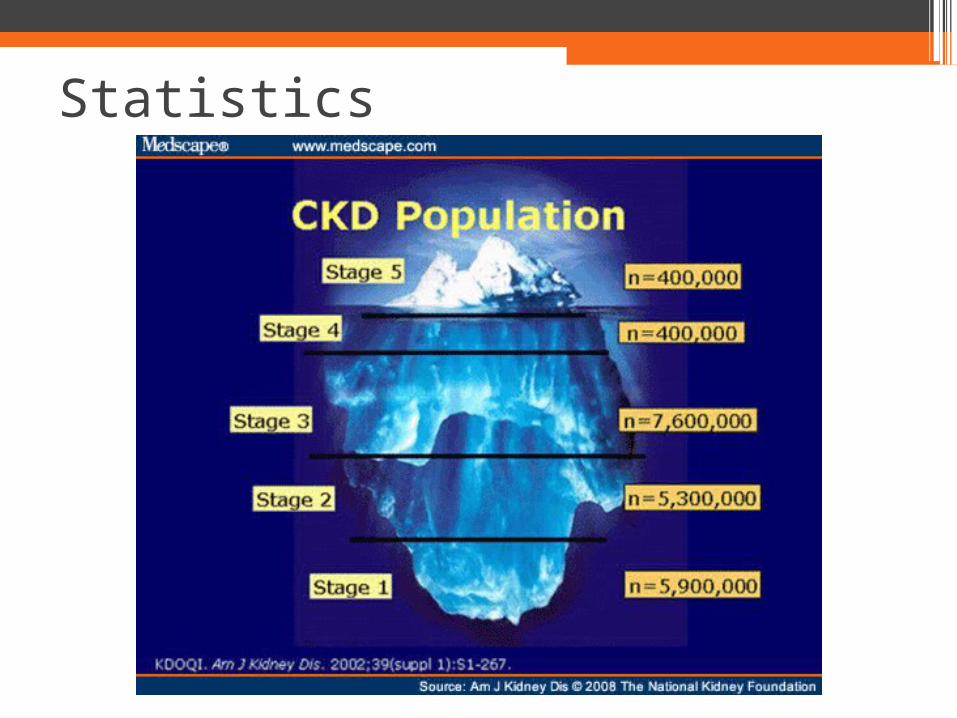
Statistics
Anemiain
CKD
Definition of Anemia
World Health Organization
•Males: hemoglobin less than 13g/dl•Females: hemoglobin less than 12g/dl
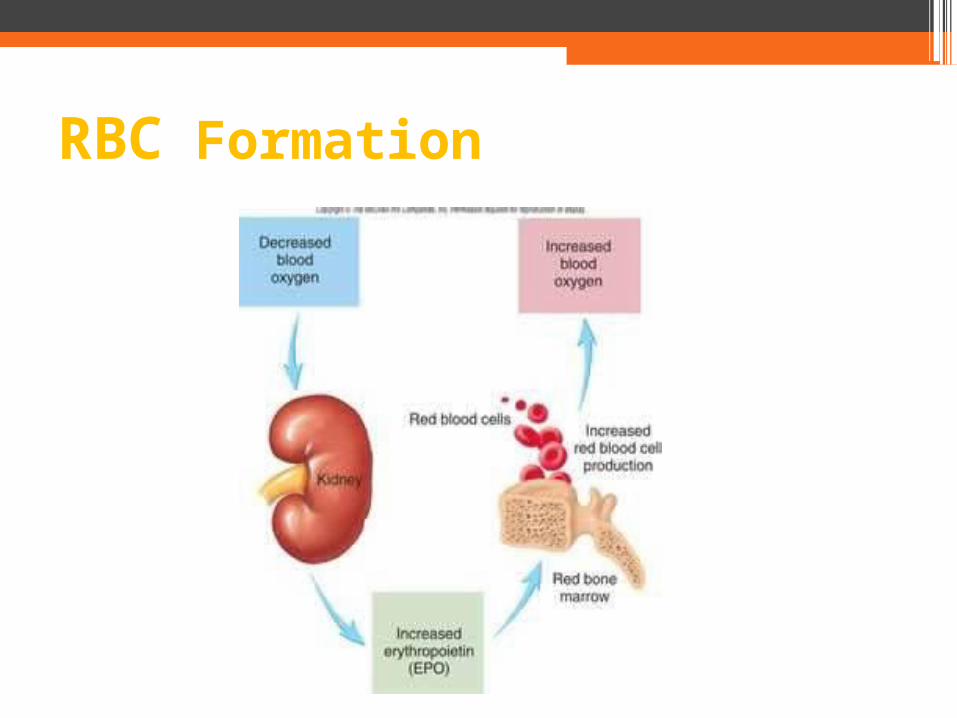
RBC Formation
•Undifferentiated cells gradually differentiate to become stem cells, that form blood cells
• Occurs in myeloid tissue (bone marrow of long bones) and lymphoid tissue
• 2 types of Hematopoiesis:Erythropoiesis: Formation of RBCsLeukopoiesis: Formation of WBCs
Hematopoiesis/Erythropoiesis
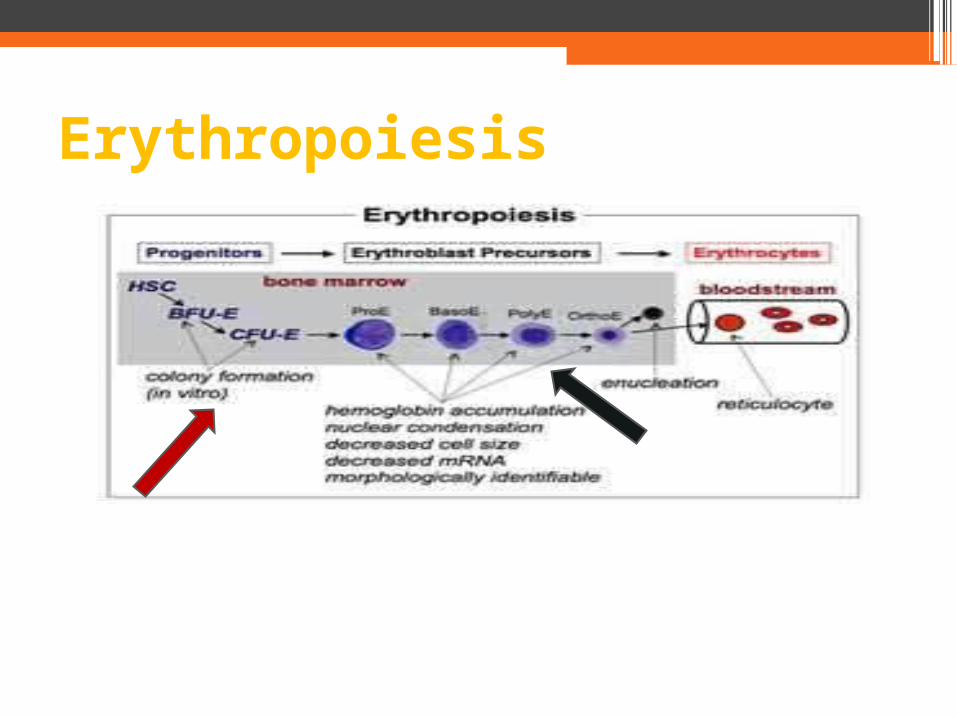
Erythropoiesis
•Relative or absolute iron deficiency•Decreased erythropoetin production• Increased risk for bleeding due to uremic effects
on platelets•Blood losses – GI, dialysis, lab draws•B12 and or folate deficiencies
•Hyperparathyroidism•Low grade hemolysis or hypersplenism•Other conditions: cancer, infections, medication
related
Causes of Anemia in CKD
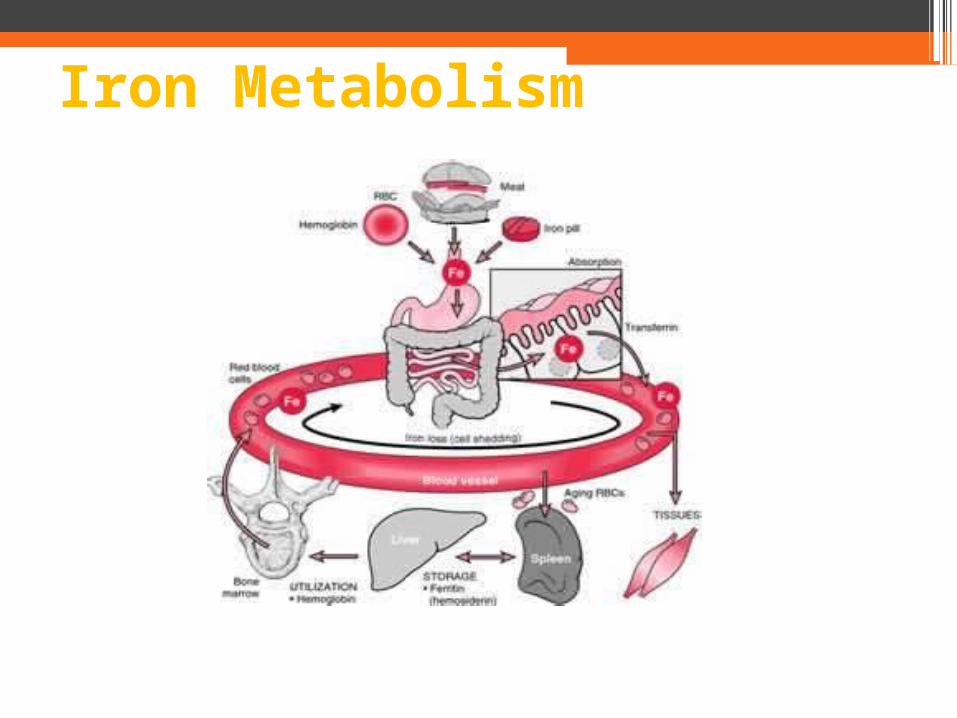
Iron Metabolism
•Relative or absolute iron deficiency•Decreased erythropoetin production• Increased risk for bleeding due to uremic effects
on platelets•Blood losses – GI, dialysis, lab draws•B12 and or folate deficiencies
•Hyperparathyroidism•Low grade hemolysis or hypersplenism•Other conditions: cancer, infections, medication
related
Causes of Anemia in CKD
Bone and Mineral Disorder
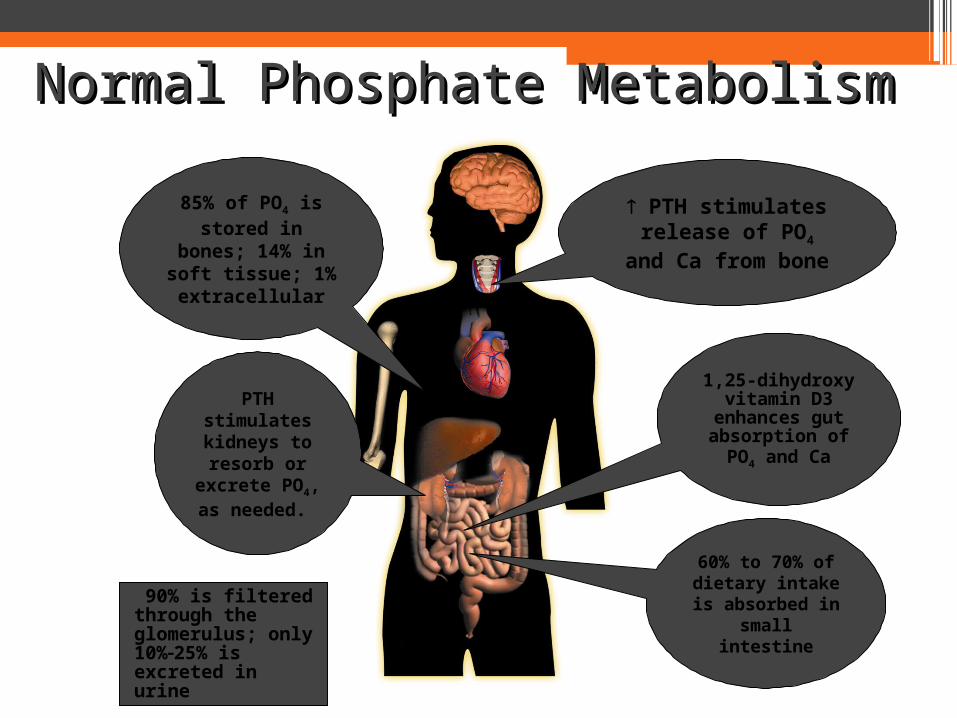
Normal Phosphate MetabolismNormal Phosphate Metabolism
60% to 70% of dietary intake is absorbed in
small intestine
PTH stimulates release of PO4 and
Ca from bone
PTH stimulates kidneys to resorb or
excrete PO4, as needed.
85% of PO4 is stored in
bones; 14% in soft tissue; 1% extracellular
90% is filtered through the glomerulus; only 10%25% is excreted in urine
1,25-dihydroxy vitamin D3
enhances gut absorption of PO4 and Ca
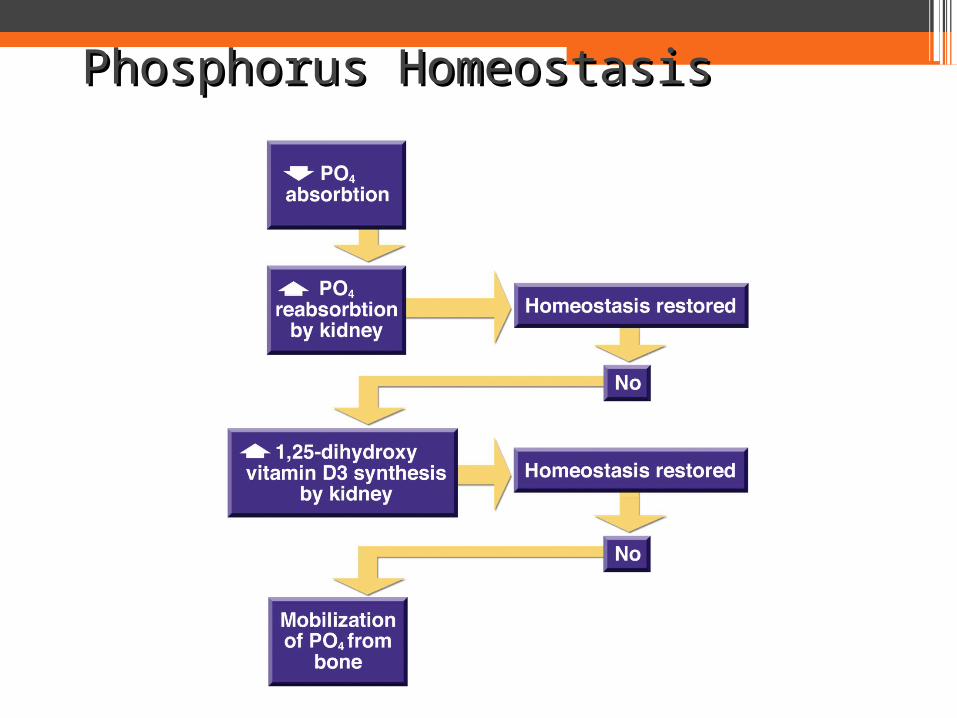
Phosphorus HomeostasisPhosphorus Homeostasis
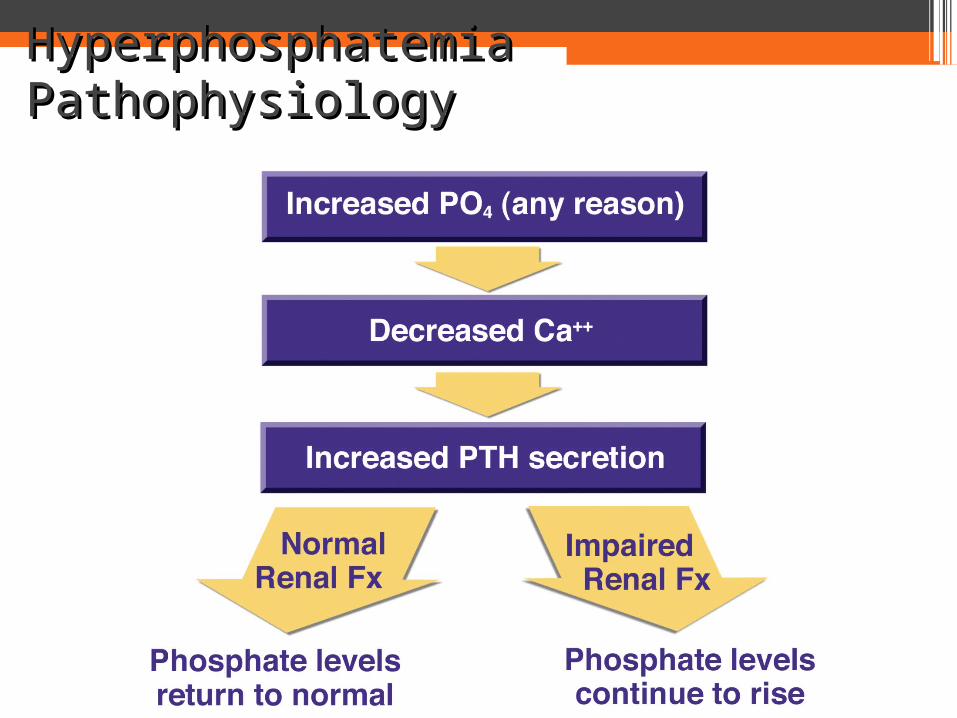
Hyperphosphatemia PathophysiologyHyperphosphatemia Pathophysiology
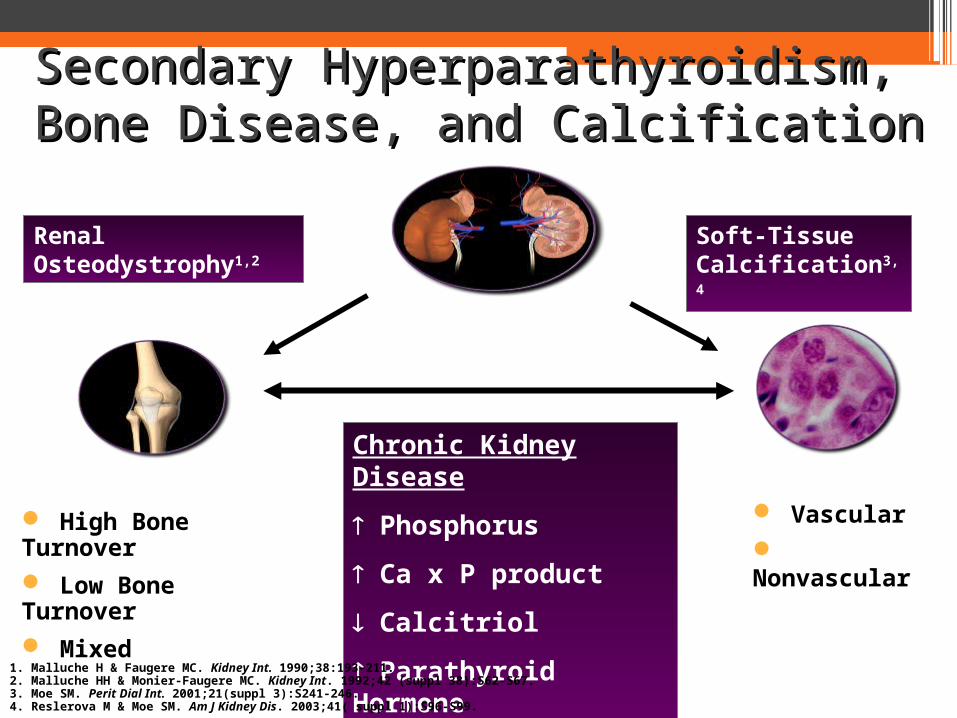
Secondary Hyperparathyroidism, Secondary Hyperparathyroidism, Bone Disease, and CalcificationBone Disease, and Calcification
High Bone Turnover Low Bone Turnover Mixed
Chronic Kidney Disease
Phosphorus
Ca x P product
Calcitriol
Parathyroid Hormone
Renal Osteodystrophy1,2
Soft-Tissue Calcification3,4
Vascular Nonvascular
1. Malluche H & Faugere MC. Kidney Int. 1990;38:193-211. 2. Malluche HH & Monier-Faugere MC. Kidney Int. 1992;42 (suppl 38):S62-S67. 3. Moe SM. Perit Dial Int. 2001;21(suppl 3):S241-246.4. Reslerova M & Moe SM. Am J Kidney Dis. 2003;41( suppl 1):S96-S99.
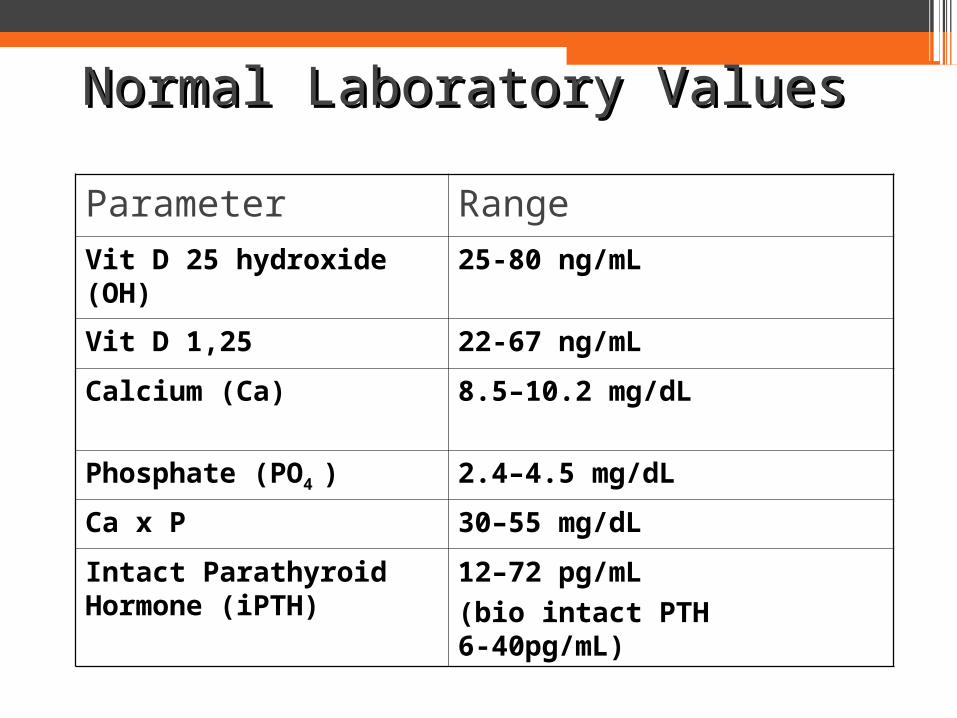
Normal Laboratory ValuesNormal Laboratory Values
Parameter Range
Vit D 25 hydroxide (OH) 25-80 ng/mL
Vit D 1,25 22-67 ng/mL
Calcium (Ca) 8.5–10.2 mg/dL
Phosphate (PO4 ) 2.4–4.5 mg/dL
Ca x P 30–55 mg/dL
Intact Parathyroid Hormone (iPTH)
12–72 pg/mL
(bio intact PTH 6-40pg/mL)