Embed Size (px)
Citation preview

1
© 2019 PRIME® Education, LLC. All Rights Reserved..
This activity is provided by PRIME Education. There is no fee to participate. This activity is supported by education grants from AbbVie, Inc., Sanofi Genzyme and Regeneron Pharmaceuticals.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 2
Overview
This fact‐sheet provides a comprehensive look at the evolving landscape of psoriatic arthritis (PsA) and rheumatoid arthritis (RA).
The assessment, treatment, and management strategies included can be implemented in daily practice to support teams in providing
patients with the best treatment aligned with evolving evidence and expert recommendations.

2
© 2019 PRIME® Education, LLC. All Rights Reserved.. 3
Disclosure Policy
PRIME Education, LLC (PRIME®) endorses the standards of the ACCME, as well as those of the AANP, ANCC, and ACPE, which require everyone in a position of controlling the content of a CME/CE activity to disclose all financial relationships with commercial interests related to the activity content. CME/CE activities must be balanced, independent of commercial bias, and designed to improve quality in health care. All recommendations involving clinical medicine must be based on evidence accepted within themedical profession. A conflict of interest is created when individuals in a position of controlling the content of CME/CE activities have a relevantfinancial relationship with a commercial interest which therefore may bias his/her opinion and teaching. This may include receiving a salary, royalty, intellectual property rights, consulting fee, honoraria, stocks, or other financial benefits. PRIME® will identify, review, and resolve all conflicts of interest that speakers, authors, course directors, planners, peer reviewers, or relevant staff disclose prior to an educational activity being delivered to learners. Disclosure of a relationship is not intended to suggest or condone bias in any presentation but is made to provide participants with information that might be of potential importance to their evaluation of a presentation. Disclosure information for speakers, authors, course directors, planners, peerreviewers, and/or relevant staff is provided with this activity.Presentations that provide information in whole or in part related to non‐FDA‐approved uses of drugs and/or devices will disclose the unlabeled indications or the investigational nature of their proposed uses to the audience. Participants should refer to theofficial prescribing information for each product for discussion of approved indications, contraindications, and warnings. Participants should verify all information and data before treating patients or employing any therapies described in this educational activity. The opinions expressed in the educational activity are those of the presenting faculty and do not necessarily represent the views of PRIME®, ACCME, AANP, ACPE, ANCC, or other relevant accreditation bodies.
© 2019 PRIME® Education, LLC. All Rights Reserved..
AccreditationIn support of improving patient care, PRIME® is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the healthcare team.
This activity was planned by and for the healthcare team, and learners will receive 2.5 Interprofessional Continuing Education (IPCE) credits for learning and change.
Physician Credit Designation Statement
PRIME Education, LLC (PRIME®) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.PRIME® designates this Enduring material for a maximum of 2.5 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity.
Physician Assistant Credit Designation Statement
PRIME® has been authorized by the American Academy of PAs (AAPA) to award AAPA Category 1 CME credits for activities planned in accordance with AAPA CME Criteria. This activity is designated for 2.5 AAPA Category 1 CME credits. PAs should only claim credit commensurate with the extent of their participation..
Nurse Practitioner Credit Designation Statement
PRIME® is accredited by the American Association of Nurse Practitioners as an approved provider of nurse practitioner continuing education. Provider number: 060815. This activity is approved for 2.5 contact hours of continuing education (which includes 1 hours of pharmacology).
Pharmacist Credit Designation Statement
This Application‐based activity has been approved for 2.5 contact hours (0.25 CEUs) by PRIME® for pharmacists. The Universal Activity Number for this activity is JA0007144‐0000‐19‐086‐H01‐P. Pharmacy CE credits can be electronically submitted to the NABP upon successful completion of the activity. Pharmacists with questions can contact NABP customer service ([email protected]).
Nurse Credit Designation Statement
PRIME Education, LLC (PRIME®) is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation.PRIME® designates this activity for 2.5 contact hours.

3
© 2019 PRIME® Education, LLC. All Rights Reserved.. 5
Faculty Disclosures
The following individuals have identified relevant financial relationships with commercial interests to disclose:
• Laura K Ferris, MD, PhD (Lead Faculty)
Advisory Board/Panel – Dermavant, JanssenPrincipal Investigator of Research Grant – AbbVie, Amgen, Celgene, Dermavant, Eli Lilly and Company, Janssen, Leo Pharma, Novartis
• Grant W Cannon, MD (Lead Faculty)
Principal Investigator of Research Grant – Amgen
The following individuals have no relevant financial relationships with commercial interests to disclose:
• Heidi Wynn Maloni, PhD, ANP‐BC, CNRN, MSCN (Planner)
• Ryan Burke, PharmD (Planner/Reviewer)
All PRIME staff participating in planning and content development have no relevant financial relationships with commercial interests to disclose.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 6
Learning Objectives
• Identify major barriers to evidence‐based treatment and management in federal and public sectors
• Implement appropriate methods for diagnosis and assessment of disease activity
• Assess current evidence on targeted biologic and small‐molecule therapies to guide treatment decisions for patients with moderate to severe disease
• Monitor treatment responses according to treat‐to‐target principles and methods
• Apply current evidence and guidelines to inform treatment decisions for patients with inadequate responses to initial therapies
• Incorporate patient‐reported outcomes and shared decision‐making into clinical practice
• Apply effective strategies for multidisciplinary care coordination and shared patient management

4
© 2019 PRIME® Education, LLC. All Rights Reserved..
PSORIATIC ARTHRITIS
© 2019 PRIME® Education, LLC. All Rights Reserved..
Clinical Features, Classification, & Assessment

5
© 2019 PRIME® Education, LLC. All Rights Reserved.. 9
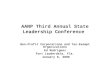
Psoriatic Arthritis (PsA) is a Heterogeneous Disease with a Wide Spectrum of Clinical Manifestations
• Affects <30% of patients with psoriasis 75% of patients develop skin symptoms first
Joint symptoms typically begin at ages 30–55
• PsA more likely to develop in patients with moderate to severe psoriasis (PsO)
• Significant impact on: Disability
Quality of life
Comorbidities
Economic burden
• To achieve best outcomes, guidelines call for collaboration between: Dermatology and rheumatology specialties
Specialists and interprofessional team
PIP = Proximal Interphalangeal; DIP = Distal Interphalangeal.
Image adapted from: Giannelli A. Rheumatol Ther. 2019;6(1):5–21.
Coates LC, et al. Arthritis Rheumatol. 2016;68(5):1060–1071.
Scalp Psoriasis
Psoriatic Lesions
Tender/SwollenSacroiliac Pain
Nail Psoriasis
Plantar FasciitisAchilles Tendon Pain
Dactylitis
PIP/DIP Joint Inflammation
Enthesitis of superior/inferior patella or lateral epicondylar
Grappa Domains of PsA
Peripheral Arthritis Dactylitis
Axial Disease Nails
Enthesitis Skin
© 2019 PRIME® Education, LLC. All Rights Reserved.. 10
What Does PsA Look Like?
DIP joint involvement Symmetric arthritis Asymmetric oligoarthritis
Spondylitis Dactylitis Enthesitis
DIP = Distal Interphalangeal.
Images courtesy of Paul S Yamauchi, MD, PhD.

6
© 2019 PRIME® Education, LLC. All Rights Reserved.. 11
Distinguishing Clinical Features of PsA, Rheumatoid Arthritis, and Osteoarthritis (OA)
Features PsA RA OA
Peripheral disease Asymmetric Symmetric Asymmetric
DIP joint involvement Yes No Yes
Sacroiliitis Asymmetric No No
Morning stiffness Peripheral joints,
some spinePeripheral joints
Peripheral or spine joints, especiallyfollowing physical activity
Gender ratio (M:F) 1:1 1:3 1:1
Rheumatoid factor, anti‐CCP
No Yes No
Enthesitis Yes No Yes
Nail lesions Yes No No
Skin involvement Yes No NoMcArdle A, et al. Clin Rev Allergy Immunol. 2017. Epub ahead of print; Mease P, et al. J Am Acad Dermatol. 2005;52(1):1–19.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 12
Classification Criteria for Psoriatic Arthrits (CASPAR)
Symptom Domain Criterion
Clinical
Psoriasis (current*, history, or family history)
Nail changes
Dactylitis (current or history)
Serology Rheumatoid factor negative
Radiology Juxta‐articular new bone formation
*Active psoriasis accounts for two points.
Taylor W, et al. Arthritis Rheum. 2006;54(8):2665‐2673.
Established inflammatory articular disease (joint, spine, entheseal) plus ≥ 3 points from the following criteria:

7
© 2019 PRIME® Education, LLC. All Rights Reserved.. 13
Early Diagnosis of PsA is Critical for Long‐Term Outcomes
• PsA is a progressive disease
40–70 % of patients have joint damage within 2 years of disease onset
50% of patients have chronic‐progressive disease
• PsA is underdiagnosed
<40% of PsO patients have undiagnosed PsA
70% of patients have their 1st rheumatologist visit after 2 years of joint symptom onset
Untreated PsA leads to:
Persistent inflammation
Progressive and irreversible joint damage
Severe physical limitations and disability
Onset of related comorbidities
Increased mortality
*Confidence rated on a 5‐point Likert scale (1 = very low; 5 = very high). Percentages shown represent pooled represent pooled ratings of 4 and 5 on this scale.
McArdle A, et al. Clin Rev Allergy Immunol. 2018;55(3):271–294; Mease PJ, et al. J Am Acad Dermatol. 2013;69(5):729–735; Ritchlin CT, et al. N Engl J Med. 2017;376(10):957–970; Menter A, et al. J Am AcadDermatol. 2008;58(5):826–850; Haroon M, et al. Ann Rheum Dis. 2013;72(5):736–740; Haroon M, et al. Ann Rheum Dis. 2015;74(6):1045–1050; Boehncke WH, et al. J Eur Acad Dermatol Venearol. 2014;28(3):264–270.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 14
What Measurements Do We Use for Axial Involvement?
Gladman DD. Rheum Dis Clin N Am. 2015;41(4):569–579.
May be detected with:
Finger to floor Tragus to wallSchober’s testLateral flexion of the spineChest expansion

8
© 2019 PRIME® Education, LLC. All Rights Reserved.. 15
Tools for Assessing PsA Disease Severity
See appendix for list of abbreviations.
Raychaudhuri SP, et al. J Autoimmun. 2017;76:21–37.
Disease Assessment Tools for Measurement
Peripheral Joint 68/66 tender/swollen joint count, DAS28, CDAI*, DAPSA, cDAPSA, and ACR20/50/70
Composite MDA, VLDA, PASDAS, CPDAI
Axial Joint ASDAS, BASDAI, BASFI, BASMI
Skin PASI, BSA, Target lesion, Physician static global
Enthesitis Leeds, SPARCC, MASES, 4‐point
Dactylitis Leeds, present/absent, DSS (dactyliits severity score)
Patient Global VAS (global, skin + joints)
Physician Global VAS (global, skin + joints)
Pain VAS, NRS
Function / QOL HAQ, SF‐36, PsAQOL, DLQI
© 2019 PRIME® Education, LLC. All Rights Reserved..
Therapeutic Management

9
© 2019 PRIME® Education, LLC. All Rights Reserved.. 17
PsA in the US: Quick Statistics
Mease PJ, et al. J Am Acad Dermatol. 2013;69(5):729–735; Armstrong AW, et al. JAMA Dermatology. 2013;149(10):1180–1185; Lebwohl MG, et al. Am J Clin Dermatol. 2016; 17(1):87–97.
• Patients with moderate to severe PsA who report not receiving any form of treatment or topical therapy alone53%
• Patients with PsA who are dissatisfied with their current treatment55%
• Patients with PsA who do not think their current treatment meets their primary goals of therapy40%
• Incremental adjusted direct and indirect costs of PsA as a comorbidity with PsO>$10,000
© 2019 PRIME® Education, LLC. All Rights Reserved..
Targeting Minimal Disease Activity To Achieve Goals of PsA Therapy
Minimal Disease Activity (MDA)
Tender joint count ≤1
Swollen joint count ≤1
PASI ≤1 or BSA ≤3
Patient pain VAS ≤15
Patient global activity VAS ≤20
HAQ ≤0.5
Tender entheseal points ≤1
Coates LC, et al. Arthritis Rheumatol. 2016;68(5):1060–1071; Coates LC, et al. Ann Rheum Dis. 2010;69(1):48–53; Coates LC, et al. Lancet. 2015;386(10012):2489–2498.
Goals of PsA Therapy:
Achieve lowest possible level of disease activity
Improve quality of life and functional status
Minimize or prevent complications
Using a Treat‐to‐Target Approach to Achieve MDA:Results from the TICOPA Study
• 206 patients with early PsA randomized to receive treatment through:
Tight control: review every 4 weeks, escalate treatment if MDA not met
Standard control: review every 12 weeks, treatment according to clinician
Early intervention + tight control of inflammation led to higher ACR20, ACR70, and PASI75 scores after 48 weeks vs standard care

10
© 2019 PRIME® Education, LLC. All Rights Reserved.. 19
GRAPPA PsA Treatment Recommendations 2015
*Open‐label data available.
Coates LC, et al. Arthritis Rheumatol. 2016;68(5):1060–1071.
Standard therapeutic route
Expedited therapeutic route
Assess activity, im
pact
and progn
ostic factors
DMARDs (MTX, SSZ, LFN), TNFi
or PDE4i
Biologics (TNFi, IL12/23i IL17i)
or PDE4i
Peripheral arthritis
Switch biologic (TNFi, IL12/23i
or IL17i)
NSA
IDs an
d IA
I corticosteroids as in
dicated
NSAIDs only
TNFi, IL17i or *IL12/23i
Axial disease
Switch biologic (TNFi, IL17i or *IL12/23i)
Physiotherap
y an
d NSA
IDs
No direct evidence for therapies in axial PsArecommendations based on axial SpA literature
NSAIDs
Biologics (TNFiIL12/23i, IL17i)
or PDE4i
Enthesitis
Switch biologic (TNFi, IL12/23i, IL17i) or PDE4i
Physiotherap
y
CS injections: consider on an individual basis due to potential for serious side effects; no clear evidence for efficacy
NSAIDs
DMARDs (MTX, LEF, SSZ) or
PDE4i
Dactylitis
Biologics (TNFi, IL12/23i)
Corticosteroid in
jections as in
dicated
Switch biologic (TNFi, IL12/23i, IL17i) or PDE4i
Topicals(keratolytics, steroids, vit. D analogues, emollients, calcineurin i)
Phototherapy or DMARDs (MTX, CSA, acitretin, fumaric acid
esters) or PDE4i
Skin
Biologics (TNFi, IL12/23i, IL17i) or
PDE4i
Topicalsas in
dicated
Switch biologics (TNFi, IL12/23i, IL17i)
or PDE4i
Biologics (TNFi, IL12/23i, IL17i)
or PDE4i
Topical or procedural or DMARDs (CSA,
LEF, MTX, acitretin)
Nails
Switch biologic (TNFi, IL12/23i, IL17i) or PDE4i
Which domains are involved?
Consider previous therapy, patient choice, other disease involvement, and comorbidities. Choice of therapy should address as many domains as possible.
Treat, periodically re‐evaluate, and modify therapy as required.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 20
ACR/NPF Guidelines for the Management of Active PsA (2018)
ACR = American College of Rheumatology; OSM = Oral Small Molecules, defined as methotrexate, sulfasalazine, leflunomide, cyclosporine, and apremilast. Does not include tofacitinib or abatacept.
Sing JA, et al. Arthritis Rheumatol. 2019;71(1):5–32.
• Use a treat‐to‐target strategy to make decisions based on individual patient factors: severity or activity of PsA, severity or activity of PsO, comorbidities, contraindications to medications, preferences to route or frequency of administration, concerns over therapies, and others.
• At each point, discuss with the patient, since all recommendations are conditionally based on low/very low quality of evidence: conditional recommendations are preference‐sensitive and always warrant a shared decision‐making approach.
Treatment‐Naïve Active PsA
Start TNFiover OSM, IL 17i, or IL 12/23i
Start OSMover IL 17i or IL 12/23i
Start MTX over NSAIDs
Start IL17iover IL 12/23i
If active despite TNFi monotherapy:• Switch to different TNFi over IL 17i, IL 12/23i, abatacept,
tofacitinib, or adding MTX• Switch to IL 17i over IL 12/23i, abatacept, or tofacitinib• Switch to IL 12/23i over abatacept or tofacitinib
If active despite TNFi + MTX therapy:• Switch to different TNFi + MTX over TNFi monotherapy• Switch to IL 17i monotherapy over IL 17i + MTX• Switch to IL 12/23i monotherapy over IL 12/23i + MTX
If active despite OSM:• Switch to TNFi over another OSM, IL 17i, IL 12/23i,
abatacept, or tofacitinib• Switch to IL 17i over another OSM, IL 12/23i, abatacept,
or tofacitinib• Switch to IL 12/23i over another OSM, abatacept or
tofacitinib
If active despite IL 17i monotherapy:• Switch to TNFi over IL 12/23i, a different IL 17i, or
adding MTX• Switch to IL 12/23i over a different IL 17i, or adding MTX
If active despite IL 12/23i monotherapy:• Switch to TNFi over IL 17i or adding MTX• Switch to IL 17i, adding MTX
ACR/NPF Disclosure: The order of listing of various conditional recommendations or of different treatment choices within a conditional statement does not indicate any sequence in which treatment options would be chosen.

11
© 2019 PRIME® Education, LLC. All Rights Reserved.. 21
Conventional DMARDs in PsA
• DMARDs: Decrease pain and inflammation
• Many are used off‐label in PsA Approved for other inflammatory conditions
• Modest effects/efficacy on arthritis and skin disease Minimal effect on preventing radiological progression
No effect on axial disease
• Risk for adverse events
DMARD = Disease‐Modifying Antirheumatic Drug.
Raychaudhuri SP, et al. J Autoimmun. 2017;76:21‐37; Mease PJ, et al. Drugs. 2014;74(4):423‐441; Kingsley GH, et al. Rheumatology. 2012;51(8):1368‐1377.
Methotrexate Leflunomide
Sulfasalazine Cyclosporine
© 2019 PRIME® Education, LLC. All Rights Reserved..
22
Biologic and Small Molecule Therapies for PsA
Therapy Target Key Trial Dosing* Considerations*
Abatacept CD 80/86 PsA‐I/PsA‐II IV: weeks 0, 2, 4, then Q4W SC: QW (no loading dose)
• Available as powder for reconstitution, PFS, or autoinjector• Dosing based on patient weight
Apremilast PDE4 PALACE/ACTIVE Oral: titrate‐up over 1 week until 30 mg BID • Adjust dose if renal impairment
Tofacitinib JAK 1/3 OPAL Oral: 5mg BID or 11mg QD• Adjust dose if renal or hepatic impairment; concomitant CYP‐2C19
and/or ‐3A4 inhibitors; or lymphopenia, neutropenia, anemia
Etanercept TNF‐α Ph3 Etanercept in PsA SC: 50mg QW • Available as powder for reconstitution, PFS, or autoinjector
Infliximab TNF‐α IMPACT 2 IV: weeks 0, 2, 6, then Q8W. • Dosing based on patient weight (5 mg/kg)
Adalimumab TNF‐α ADEPT SC: 40mg Q2W or QW • Available as single‐dose vial, PFS, or autoinjector
Golimumab TNF‐α GO‐REVEAL/GO‐VIBRANT SC: 50 mg Q4W • Available as PFS or autoinjector
Certolizumab TNF‐α RAPID‐PsA SC: 400mg at week 0, 2, 4, then 200mg Q2W • Available as powder for reconstitution or PFS
Ustekinumab IL 12/23 PSUMMIT 1 SC: 45mg at week 0, 4, then Q12W• Available as singe‐dose vial or PFS• Double the dose for patients weighing ≥100kg
Secukinumab IL 17A FUTURE 2 SC: 150mg week 0, 1, 2, 3, 4, then Q4W• Available as singe‐dose vial or PFS• Double the dose for patients with active PsO
Ixekizumab IL 17 SPIRIT‐P1 SC: 160mg at week 0, then 80mg Q4W • Different loading dose for patients with active PsO
Phase 3
Upadacitinib JAK 1 SELECT‐PsA Oral
Guselkumab IL 23 DISCOVER SC
*Per prescribing label. Please refer to label for full information on dosing and administration.PFS = Prefilled Syringe.

12
© 2019 PRIME® Education, LLC. All Rights Reserved.. 23
Anti‐TNF Therapies in PsA: ACR and PASI Responses
Mease PJ, et al. Arthritis Rheum. 2005;52(10):3279–3289; Mease PJ, et al. Ann Rheum Dis. 2014;73(1):48–55; Mease PJ, et al. Lancet. 2000;356(9227):385–390; Mease PJ, et al. Arthritis Rheum. 2004;50(7):2264–2272; Kavanaugh A, et al. Arthritis Rheum. 2009;60(4):976–986; Antoni C, et al. Ann Rheum Dis. 2005;64(8):1150–1157; Antoni CE, et al. Arthritis Rheum. 2005;52(4):1227–1236.
57
39
23
5958
36
25
47
73
50
13
26
59
38
11
23
48
32
18
5858
36
15
6465
46
29
68
0
10
20
30
40
50
60
70
80
ACR20 ACR50 ACR70 PASI75
Adalimumab (n = 405) ‐14 wks
Certolizumab (n = 409) ‐12 wks
Etanercept (n = 60) ‐12 wks
Etanercept (n = 205) ‐24 wks
Golimumab (n = 405) ‐14 wks
Infliximab (n = 200) ‐14 wks
Infliximab (n = 104) ‐16 wks
1
2
3
4
5
6
7
Patient Response (%)
Please note: data presented in this graph come from different trials and are not directly comparable.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 24
Impact of Switching on PsA Outcomes
• 30–40% of patients switch to a second or third therapy mainly due to lack of effect or adverse events
• Data from observational studies show a trend toward poorer responses to and lower drug survival for 2nd TNFi compared with 1st TNFi No difference found between TNFi
• GRAPPA recommendations: Switch to either an alternative biologic within a
drug class or to a drug with a different mechanism of action
Add conventional DMARDs (e.g., methotrexate) to biologic therapy, but there is little evidence of added benefit
DANBIO Registry 10‐year Observational Cohort
D’Angelo S, et al. Open Access Rheumatol. 2017;9:21–28; Glintborg B, et al. Arthritis Rheum. 2013;65(5):1213–1223; Coates LC, et al. Arthritis Rheumatol. 2016;68(5):1060–1071; Fagerli KM, et al. Ann Rheum Dis. 2013;72(11):1840–1844; Lubrano E, et al. J Rheumatol. 2016;43(5):918–923.
TNF therapy # of Switches
Patients (%)
47%
22%18%
0%
10%
20%
30%
40%
50%
1st 2nd 3rd
57%
47%
None Any
ACR20 Response by Anti‐TNF Switch
3–6 Months 2 Years

13
© 2019 PRIME® Education, LLC. All Rights Reserved.. 25
Efficacy of Apremilast (PDE4) in PsA Patients with Prior Biologic‐Therapy Exposure or Failure
24
5 6
31 31
21
43
2823
0
10
20
30
40
50
60
Biologic‐Naïve Patients Biologic‐Experienced Patients Biologic Failures
Placebo Apremilast 20 mg twice a day Apremilast 30 mg twice a day
†P <0.007.
Kavanaugh A, et al. Ann Rheum Dis. 2014;73(6):1020–1026.
Results from PALACE‐1 TrialACR20 Response by Biologic Experience
Responders (%)
n = 118 125 120 40 36 39 18 14 13
†
††
© 2019 PRIME® Education, LLC. All Rights Reserved.. 26
0
20
40
60
80
0 1 2 3 4 5 6
Efficacy of Tofacitinib (JAK 1/3 inhibitor) in PSA Patients with Prior Anti‐TNF Treatment Failure: OPAL‐Beyond Phase 3 Results
ACR20 Response PASI‐75 Response
At 3 Months
Placebo(n = 131)
Tofacitinib5 mg
(n = 131)
Tofacitinib10 mg
(n = 132)
12/86 (14%) 17/80 (21%) 35/81 (43)
At 6 MonthsPbo → Tofa
5 mg(n = 66)
Pbo → Tofa10 mg(n = 65)
Tofacitinib5 mg
(n = 131)
Tofacitinib10 mg
(n = 132)
11/42 (26%) 14/44 (32%) 27/80 (34%) 37/81 (46%)
Tofa = Tofacitinib
Gladman D, et al. N Engl J Med. 2017;377(16):1525–1536.
Month
Responders (%)
PlaceboTofacitinib 10mg
Tofacitinib 5mg
Placebo Tofacitinib 10mg
Placebo Tofacitinib 5mg

14
© 2019 PRIME® Education, LLC. All Rights Reserved.. 27
0
20
40
60
80
0 4 8 12 16 20 24 28 32 36 40 44 48 52
n = 62n = 60n = 58
Efficacy of Ustekinumab (Anti‐IL12/23) in PsA Patients with Prior Anti‐TNF Exposure: PSUMMIT 2 Trial
*Ustekinumab was administered at week 0, week 4 and every Q12W thereafter.
†Among randomized patients with ≥3% body surface area with PsO skin involvement at baseline.
‡For pa ents who qualified for early escape, data at or prior to Week 16 were carried forward through Week 24. A er Week 24, observed data were used.
Ritchlin C, et al. Ann Rheum Dis. 2014;73(6):990–999.
10
7058
79
63
82
0
25
50
75
100
2
434636
49 50
0
25
50
75
100
Responders (%)
Responders (%)
n = 30 36 40 27 33 33
n = 50 44 41 30 36 40
Week 24 Week 52
0
20
40
60
80
0 4 8 12 16 20 24 28 32 36 40 44 48 52
n = 42
n = 43
n=47
Prior Anti‐TNF
Exposure
† ‡
Week 24 Week 52Weeks
Weeks
No Prior Anti‐TNF
Exposure
† ‡
Responders (%)
Responders (%)
ACR20
ACR20
PASI75
PASI75
Placebo Ustekinumab 45mg Ustekinumab 90mg
© 2019 PRIME® Education, LLC. All Rights Reserved.. 28
Efficacy of Secukinumab (Anti‐IL17A) in PsA Patients With or Without Prior Anti‐TNF Exposure
*Secukinumab was given QW from week 0–4, then Q4W thereafter.
IR = Inadequate Response.
McInes IB, et al. Lancet. 2015;386(9999):1137–1146.
58%
45%
63%
30%
16% 14%
0%
20%
40%
60%
80%
Anti‐TNF Naïve Anti‐TNF IR
Secukinumab 300mg Secukinumab 150mg Placebo
63% 64%
56%
36%
19%
8%
Anti‐TNF Naïve Anti‐TNF IR
ACR20 Response PASI75 Response
FUTURE 2: Phase 3 Trial
Patients (%)
n = 67 63 63 33 37 35 30 36 31 11 22 12

15
© 2019 PRIME® Education, LLC. All Rights Reserved.. 29
Efficacy of Ixekizumab (Anti‐IL17A) in PsA Patients with Prior Anti‐TNF Treatment Failure: SPIRIT‐P2 Phase 3 Results
*P <0∙0001
Patients in both ixekizumab treatment groups received a loading dose of 160 mg at week 0, then 80 mg per dose thereafter.
Nash P, et al. Lancet. 2017;389(10086):2317–2327.
ACR20 Scores ACR70 Scores
0 4 8 12 16 20 24
19%
53%*
48%*
Patients with ACR‐20 (%)
Week
Placebo (n = 118)Ixekizumab Q4W (n = 122)Ixekizumab Q2W (n = 123)
0 4 8 12 16 20 240%
22%*
12%*
Patients with ACR‐70 (%)
Week
© 2019 PRIME® Education, LLC. All Rights Reserved..
Interdisciplinary Collaboration and Management

16
© 2019 PRIME® Education, LLC. All Rights Reserved.. 31
PPACMAN: National Initiative to Improve Collaboration Between Dermatologists and Rheumatologists
Combined Clinic Model
Cross training between specialties
One‐stop‐shop for patient education and support
Cohesive management ofpatients with psoriatic disease
Development of validated tools and measures between specialties
Perform observational and interventional trials activities
GoalsResearch
• Barriers and facilitators• Patient perspectives and attitudes• Improved diagnosis
Education
• Build networks and relationshipso Referral practiceso Tele‐management o EMR links, forms, templateso Community outreach o Provider database (NPF)o Education partnership (GRAPPA/PRIME)
• Best practices toolkit for building clinics and assessing patients
© 2019 PRIME® Education, LLC. All Rights Reserved.. 32
Initial Findings from PPACMAN’s Research Projects
Demographics:
• 25 clinics across the US
• 32 physician responses 16 dermatologists
14 rheumatologists
2 dual‐trained physicians
• 1 in private practice
• 5 collaborated virtually
• 25 reported having trainees
Okhovat JP, et al. J Rheumatol. 2017;44(5):693–694.
Cross‐sectional survey of 25 participating centers with dual rheumatology‐dermatology clinics
Benefits:• Improved communication among healthcare teams• Excellent training opportunities• Prompt and accurate diagnosis of PsA• Frequent monitoring of symptoms and medication• Increased professional development/satisfaction
Challenges:• Scheduling the right mix of patients• Filling both specialists’ schedules appropriately• Demonstrating value to the institution

17
© 2019 PRIME® Education, LLC. All Rights Reserved.. 33
Real‐World Evaluation of Multidisciplinary Care in PsA: The NEXUS Project in Spain
Queiro R, et al. Reumatol Clin. 2017;13(2):85–90.
Interviews with 24 clinicians (12 rheumatologists and 12 dermatologists) to characterize the different multidisciplinary care units currently functioning in Spain
Key Steps for Success:
Enlist involved specialist and staff with experience and interest in PsA who get along well
Define collectively the type of model that best fits the center/professionals, referral criteria and access, visit intervals,method of communication, office location, and other logistics
Develop templates and formulas to facilitate visits, discharge, and follow up
Share visit reports with patient and with other attending physicians
Evaluate model and make adjustments every 3–6 months for the first 2 years
Face‐to‐Face Approach (n = 9)
• Same office
• Attend patients simultaneously
• Make decisions together
• “One stop shop” for patients
Parallel Approach (n = 1)
• Different but contiguous offices
• Attend patients in separate but successive appointments
• Discuss cases by phone or attend patients jointly when needed
Preferential Circuits (n = 2)
• Different offices in corresponding department
• Attend patients separately
• Highly trained in PsA with specific referral criteria
• Discuss cases by phone or attend patients jointly when needed
© 2019 PRIME® Education, LLC. All Rights Reserved.. 34
Comorbidities and Extra‐Articular Manifestations of PsA
Incidence of Comorbidities of Interest among PsO Patients ± PsA (PSOLAR Registry)
Most Common Comorbidities
*Self‐reported PsA, established by a HCP; **Self‐reported PsA.
Kavanaugh A, et al. BMC Rheumatol. 2018;29(2):29; Kaine J, et al. J Manag Care Spec Pharm. 2019;25(1):122–132; Merola JF, et al. Clin Rheumatol. 2018;37(10):2751–2761.
• Cardiovascular/Metabolic Hypertension
Hyperlipidemia
Coronary artery disease
Fatty liver disease
Diabetes
Obesity
• Immune/Inflammatory Psoriasis
Inflammatory bowel disease
Uveitis
• Psychiatric Anxiety
Fatigue
Depression
47%
27%
3%
44%
26%
3%
35%
18%
1%0%
10%
20%
30%
40%
50%
Cardiovascular Psychatric IBD
PsO + PsA* (n = 1,719)
PsO + PsA** (n = 4,315)
PsO only (n = 7,775)P < 0.001 vs patients with psoriasis only

18
© 2019 PRIME® Education, LLC. All Rights Reserved.. 35
Management Considerations for Patients with Comorbidities
Husni ME. Rheum Dis Clin North Am. 2015;41(4):677–698; Husni ME, et al. Curr Rheumatol Rep. 2010;12(4):281–287; Ogdie A, et al. Curr Opin Rheumatol. 2015;27(2):118–126.
Comorbidity Practice Tips
CVD
• Check blood pressure, lipid panel• Encourage smoking cessation• Assess risk‐benefit of NSAIDs use • Identify high‐risk patients
Depression/Anxiety
• Ask about symptoms of depression and anxiety • May impact adherence to treatment • Refer to psychosocial support • Certain medications may worsen depression
Diabetes • Check fasting glucose or hemoglobin A1c
IBD• Ask about gastrointestinal symptoms• Certain medications may exacerbate disease• Not all targeted therapies approved or effective in IBD
Liver/Kidney Disease• Check serologies before starting therapy• Certain medications may exacerbate function
Malignancy • Consider periodic skin check for patients
Obesity• Council patients on the benefits of weight loss • Certain medications can help with weight loss• Certain medications are not as effective in heavier patients
Ophthalmic Disease• Ask about ophthalmic symptoms• Certain medications may aggravate symptoms
© 2019 PRIME® Education, LLC. All Rights Reserved.. 36
Interprofessional Collaboration and Co‐Management of PsA
QoL = Quality of Life
• Engage entire interprofessional team and establish roles for:
Monitoring, treatment decisions, adherence, patient education, etc.
• Improve communication between specialists, primary care, and others
Share patient notes
Call provider to discuss
• Create workflow process for:
Timely and appropriate referrals
Ensuring patient follow‐up and monitoring
Dermatology
RheumatologySupport
QoLPain
DisabilityFunctioningComorbidities
Joint symptoms
Skin symptomsScreening
Co‐managementMonitoring
Primary CarePsychology
Physical therapyCounseling Pharmacy

19
© 2019 PRIME® Education, LLC. All Rights Reserved.. 37
Patient Perspectives on PsA Treatment and Disease Burden
Kavanaugh A, et al. Rheumatol Ther. 2016. 3(1):91–102; Mease PJ, et al. J Am Acad Dermatol. 2013;69(5):729–735; Armstrong AW, et al. JAMA Dermatology. 2013;149(10):1180–1185; Lebwohl MG, et al. Am J Clin Dermatol. 2016; 17(1):87–97.
• Patients who report that PsA has either prevented them from going to work in the past year or impacted ability to work full time32%
• Patients with moderate to severe PsA who do not think their current treatment meets their primary goals of therapy40%
• Patients with moderate to severe PsA who report not receiving any form of treatment or topical therapy alone53%
• Patients with PsA who are dissatisfied with their current treatment 55% • Patients with PsA who are concerned about health risks with long‐term therapy64%
© 2019 PRIME® Education, LLC. All Rights Reserved.. 38
Eliciting Patient‐Reported Outcomes
Validated Tools•Patient Global Assessment (PGA)
•Routine Assessment of Patient Index Data (RAPID‐3)
•Work Productivity/Activity Impairment Questionnaire (WPAI)
•Functional Assessment of Chronic Illness Therapy (FACIT)
Pain and Function
•Health Assessment Questionnaire (HAQ)
•Study Short Form 36 (SF‐36)
•Psoriatic Arthritis Quality of Life (PsAQoL)
•Dermatology Life Quality Index (DLQI)
•Psoriatic Arthritis Impact of Disease (PsAID)
Quality of Life
•Patient Health Questionnaire (PHQ)‐2 or ‐9
•Generalized Anxiety Disorder‐7 Tool (GAD‐7)
•Center for Epidemiological Studies Depression Scale(CES‐D)
•Beck Depression Inventory‐II (BDI‐II)
Mental Health
Interview Questions • Assessing Disease Activity
Do you have trouble in performing daily tasks?
Do you wake up at night because of low back pain?
Have you ever experienced pain in your heel, knee, or elbow?
Have you ever noticed pain and complete swelling of a single finger/toe?
Have you ever had red, itchy, and scaly patches on your skin?
Do your fingernails or toenails have holes or pits?
• Monitoring Treatment Response
Have you noticed reduced pain or swelling in your wrists or finger joints?
Are you now able to sleep through the night?
Has your ability to climb stairs improved?
Have you noticed a reduction in swelling of the enlarged finger/toe?
Has there been improvement to areas of your skin affected by psoriasis?
Has the appearance of your fingernails/toenails improved?
Giannelli A. Rheumatol Ther. 2019 Mar;6(1):5–21; Wong PC, et al. Int J Rheumatol. 2012;2012:839425.

20
© 2019 PRIME® Education, LLC. All Rights Reserved.. 39
Strategies for Engaging Patients in Shared Decision‐Making
Needs
• Ask about disease impact, personal circumstances, and therapy preferences
• Assess health literacy and knowledge gap
Support
• Share and encourage use of NPF resources
• Provide patient education literature and tools
• Define treatment needs and goals
Quality
• Use patient decision aids
• Empower patients for active participation in care
• Guide decision‐making with clinical expertise
Outcomes
• Improve communication
• Increase likelihood of patient adherence to and satisfaction with therapy
NPF. For Your Patients. https://www.psoriasis.org/health‐care‐providers/for‐your‐patients. Accessed 9/21/17. Tan J, et al. Br J Dermatol. 2016;175(5):1045–1048; Strohal R, et al. J Eur Acad Dermatol Venereol. 2015; 29(12):2390–2398.
© 2019 PRIME® Education, LLC. All Rights Reserved..
RHEUMATOID ARTHRITIS

21
© 2019 PRIME® Education, LLC. All Rights Reserved..
Overview of Paradigms and Challenges
© 2019 PRIME® Education, LLC. All Rights Reserved.. 42
Disease and Economic Burden of Rheumatoid Arthritis (RA) in US
CDC. Arthritis. Available at https://www.cdc.gov/arthritis/index.htm. Accessed 6/8/18; Arthritis Foundation. Arthritis By The Numbers: 2018. Available at: https://www.arthritis.org/Documents/Sections/About‐Arthritis/arthritis‐facts‐stats‐figures.pdf Accessed 6/11/2018; Birnbaum H, et al. Curr Med Res Opin. 2010;26(1):77–90; Hresko A, et al. Arthritis Care Res (Hoboken). 2018. Epub ahead of print; Cooper NJ. Rheumatology (Oxford). 2000;39(1):28–33; Sokka T. Clin Exp Rheumatol. 2003;21(5 Suppl 31):S71–S74; Strand V, et al. Ann Rheum Dis. 2012;71(7):1143–1150.
$39 billion in medical costs, including direct and indirect costs (2010)
About 1.3 million Americanssuffer from RA
Women are 2–3 times more likely to get RA than men
High incidence of co‐morbidities andextra‐articular manifestations:
Underlying inflammation leads to cardiovascular disease, interstitial lung disease, and depression
Significant burden in QoL, which can be improved by effective treatment
If left untreated, 20–30% of RA patients become work‐disabled within 3 years
Total direct medical costs range from $12,000–$52,000 per patient (2015)

22
© 2019 PRIME® Education, LLC. All Rights Reserved.. 43
Therapeutic Window of Opportunity in Early RA
Image on the right courtesy of Peng T Fan, MD.
Singh JA, et al. Arthritis Care Res. 2012;64(5):625–639.
Early Established End StageDiseaseOnset
Critical Window of Opportunity
Functional impairment
Work disability
Radiographic damage
50–70% of patients have radiographic damage within the first 2 years of onset of symptoms
Intervention
RA Untreated
Disease Duration (time)
Prevents Progression
Natural Course
Population X‐Ray Score
© 2019 PRIME® Education, LLC. All Rights Reserved.. 44
Core Principles in RA Management
DMARDs = Disease‐Modifying Antirheumatic Drugs.
Singh JA, et al. Arthritis Rheumatol. 2016;68(1):1–26; Singh JA, et al. Arthritis Care Res. 2016;68(1):1–25; Smolen JS, et al. Ann Rheum Dis. 2014;73(3):492–509; Smolen JS, et al. Ann Rheum Dis. 2010;69(4):631–637; Smolen JS, et al. Ann Rheum Dis. 2016;75(1):3–15.
Early recognition and
diagnosis
Early use of DMARDs
Treat‐to‐target (T2T)
Target of remission or low disease activity
Frequent monitoring of disease activity
Individualized treatment
Shared decision‐making

23
© 2019 PRIME® Education, LLC. All Rights Reserved.. 45
Evolving RA Treatment Landscape: Pre‐Biologic Era
ASA = acetylsalicylic acid; AZA, azathiopine; Ig, immunoglobulin; HCQ, hydroxychloroquine; LEF, leflunomide; SSZ, sulfasalazine.
Treat signs and symptoms• Aggressive MTX dosing• Combination therapy• Disease modification
1930s
Injectablegold
1950s
HCQ,Steroids
1970s
D‐Pen,AZA
1980s
MTX,Oral gold
1990s
Leflunomide
1960s
SSZ
ASA
1900
Biologic DMARDs(see next slide)
2000s
© 2019 PRIME® Education, LLC. All Rights Reserved.. 46
The Evolving RA Treatment Landscape:The Rise of Biologic and Small Molecule Agents
MTX = Methotrexate; LEF = Leflunomide; JAK = Janus Kinase
1988 2001 2005 2012
MTXLEF
(ARAVA)
Etanercept(ENBREL) TNF‐α
Infliximab(REMICADE)
TNF‐α
Anakinra(KINERET)
IL‐1R
1998
Adalimumab(HUMIRA)
TNF‐α
Abatacept(ORENCIA)CD80/86
2008
Certolizumab(CIMZIA)TNF‐α
2010
Golimumab(SIMPONI)
TNF‐α
Rituximab(RITUXAN)
CD‐20
Tocilizumab(ACTEMRA)
IL‐6R
Tofacitinib(XELJANZ)JAK 1/3
FDA APPROVED
Phase 3
MTX
2013
Tocilizumab(ACTEMRA)
IL‐6R
Oral
Infusion
Injection
Golimumab(SIMPONI)
TNF‐α
Infliximab‐dyyb*(INFLECTRA)
TNF‐ α
2016
Adalimumab‐atto*(AMJEVITA)
TNF‐α
Etanercept‐szzs*(ERELZI) TNF‐α
2017
Sarilumab(KEVZARA)
IL‐6R
Adalimumab‐adbm*(CYLTEZO) TNF‐α
Infliximab‐qbtx*(IXIFI)TNF‐ α
Infliximab‐abda*(RENFLEXIS)
TNF‐ α
Baricitinib
(OLUMIANT)JAK 1/2
Filgotinib
JAK 1
OlokizumabIL‐6
Peficitinib
JAK 1/3
2019
Upadacitinib
(RINVOQ)JAK 1/2
* Biosimilar

24
© 2019 PRIME® Education, LLC. All Rights Reserved.. 47
The “Problem of Choice” in RA Treatment Decision‐Making
Karaca‐Mandic P, et al. Health Serv Res. 2010;45(5 Pt 1):1227–1250; Gleason P, et al. J Manag Care Pharm. 2013;19(7):542–548; Schneider CK. Ann Rheum Dis. 2013;72(3):315–318; CVS Caremark. Insights 2013 Specialty Trend Management. Retrieved from www.info.cvscaremark.com/sites/default/files/Insights%202013.pdf. Accessed 3/9/16.
Need for personalized treatment approach
RA disease
Patient factors
Drugs
• Complex and evolving treatment armamentarium:
New and emerging therapies with novel mechanisms
Increasing number and cost of specialty drugs
Utilization of biologics & biosimilars
• Marked heterogeneity of RA disease
• Numerous patient‐specific factors
© 2019 PRIME® Education, LLC. All Rights Reserved..
Disease Assessment andInitial Treatment

25
© 2019 PRIME® Education, LLC. All Rights Reserved.. 49
Patient Global Assessment
Components of Different RA Disease Activity Measures
DAS28=disease activity score using 28 joint counts. SDAI=simplified disease activity index. CDAI=clinical disease activity index. RAPID3=. Routine Assessment of Patient Index Data CRP= C‐reactive protienESR=erythrocyte sedimentation rate (in mm). HAQ = Health Assessment Questionnaire
Patient Reported Outcomes
Laboratory Measures
Provider Reported Outcomes
HAQ
CRP
ESRTender Joint Count
Swollen Joint Count
Patient Pain Score
Provider Global Assessment
RAPID3
DAS28
CDAI
SDAI
© 2019 PRIME® Education, LLC. All Rights Reserved.. 50
ACR‐Recommended Instruments and Measures for Assessing Disease Activity
DAS28 = Disease Activity Score Using 28 Joint Counts; SDAI = Simplified Disease Activity Index; CDAI = Clinical Disease Activity Index; TJC28 = Tender Joint Count (Of 28); SJC28 = Swollen Joint Count (Of 28); ESR = Erythrocyte Sedimentation Rate (In Mm); GH = Global Health.
Anderson JK, et al. Arthritis Care Res (Hoboken). 2012;64(5):640–647; Singh JA, et al. Arthritis Care Res. 2012;64(5):625–639.
Instrument/
Measure
Administration
Method
Measurement
Scale
Disease Activity Levels
Remission Low ActivityModerate Activity
High Activity
Patient‐Driven Composite Tools
PAS or PASII Patient questionnaire Scale: 0–10 0–0.25 0.26–3.7 3.71– <8 >8
RAPID3 Patient questionnaire Scale: 0–30 0–1.0 >1.0–2.0 2.0–4.0 4.0–10
Patient and Provider Composite Tool
CDAIProvider item; patient
itemScale: 0–76 <2.8 > 2.8–10.0 >10.0–22.0 >22
Patient, Provider, and Laboratory Composite Tools
DAS28
(ESR or CRP)
Provider assessment;
patient item; labScale: 0–9.4 <2.6 > 2.6 – <3.2 >3.2 – <5.1 >5.1
SDAIProvider item; patient
item; labScale: 0–86 <3.3 >3.3 – <11.0 >11.0 – <26 >26

26
© 2019 PRIME® Education, LLC. All Rights Reserved.. 51
EULAR 2017 RA Recommendations: Prognostic Factors for Poor Disease
EULAR = European League Against Rheumatism; csDMARD = Conventional, Synthetic DMARD; RF = Rheumatoid Factor; ACPA = Anticitrullinated Protein Antibody.
Smolen JS, et al. Ann Rheum Dis. 2017;0:1–18.
Unfavorable Prognostic Factors
• Moderate to high disease activity after csDMARD therapy
• High acute phase reactant levels
• High swollen joint counts
• Presence of RF and/or ACPA, especially at high levels
• Presence of erosions
• Failure of ≥2 csDMARDS
© 2019 PRIME® Education, LLC. All Rights Reserved..
52
TICORA Study: Treatment Strategy of Tight Control for RA
Grigor C et al. Lancet. 2004;1(9430):263‐269.
Single‐blind, randomized controlled trial in 111 patients allocated toeither intensive management or routine care
A strategy of intensive outpatient management of rheumatoid arthritis substantially improves disease activity, radiographic disease progression,physical function, and quality of life at no additional cost
Sulfasalazine, increasing every week to target
dose of 40 mg/kg per day
• Sulfasalazine• Methotrexate• Folic acid• Hydroxychloroquine
Triple therapy with monthly increments of methotrexate followed by weekly increments of
sulfasalazine
Addition of prednisolone
Change triple therapy to:• Ciclosporin• Methotrexate• Folic acid
Change to alternative DMARD (leflunomide or sodium aurothionalate)
0
1
2
3
4
5
6
0 3 4 5 12 15 18Month
Disease activity score
Intensive Routine

27
© 2019 PRIME® Education, LLC. All Rights Reserved..
53
64
18 16
91
7165
0
20
40
60
80
100
ACR20 ACR70 Remission
Patients (%)
Routine Care (n = 55) Intensive Management‡ (n = 55)
TICORA Study: Combination of Non‐Biologic DMARDs
*With protocol-based escalation of DMARDs: SSZ, MTX, hydroxychloroquine; †P <0.0001; ‡P = 0.02.SSZ = sulfasalazine; TSS = Total Sharp Score.
Grigor C et al. Lancet. 2004;1(9430):263–269.
Single‐blind, randomized controlled trial in 111 patients allocated toeither intensive management or routine care
Disease Activity Score Radiographic Progression
†
†
†
8.5
4.5
0
1
2
3
4
5
6
7
8
9
Increase in
Median TSS From
Baselin
e
Routine Care (n = 55) Intensive Management‡ (n = 55)
© 2019 PRIME® Education, LLC. All Rights Reserved..
54
Treat‐to‐Target (T2T) in RA
• Treat to desired goal: REMISSION For long‐standing disease, goal may be
low disease activity
• Measure disease activity High/moderate disease activity: monthly
Remission/low disease activity: x6 months
• Adjust therapy At least x3 months until target is reached
• Personalize treatment strategy Consider all factors (comorbidities and
other patient factors)
*2010 T2T recommenda ons updated in 2014 to reflect be er suppor ve evidence; †Shared decision‐making criteria not applied to visits that did not address changing targets or treatment; ‡Treatment decision based on target and disease ac vity measure.
Smolen JS, et al. Ann Rheum Dis. 2010;69(4):631–637; Singh JA, et al. Arthritis Rheumatol. 2016;68(1):1–26; Singh JA, et al. Arthritis Care Res. 2016;68(1):1–25; Smolen JS, et al. Ann Rheum Dis. 2017;0:1–18; Solomon DH, et al. Arthritis Care Res. 2018 [ePub ahead of print].
ACR 2015 Guidelines: Use a T2T strategy in all patients regardless of disease activity level
TRACTION Trial11 rheumatology sites participated in a Learning Collaborative to implement
best practices that support the T2T approach in RA.
T2T Implementation Score Phase I Intervention Phase II Intervention
Months 0 9 18Change(09) 0 9 18
Change(918)
Primary Outcome
Implementation score 11% 57% 52% 46% 11.0% 13% 58% 45%
Visits with components present
Treatment Target <1% 46% 51% 45% 0% 1% 52% 51%
Disease Activity 20% 89% 71% 69% 30% 34% 85% 51%
Shared Decision‐Making 51% 86% 43% 35% 25% 30% 67% 37%
Treatment Decision‐Making <1% 28% 37% 27% 0% 1% 37% 36%

28
© 2019 PRIME® Education, LLC. All Rights Reserved.. 55
Established RA†
Early RA‡
Biologic and Small Molecule Agents Are a Mainstayin RA Patients with Moderate to High Disease Activity
* According to the 2015 ACR RA treatment recommendations, combination therapy with MTX is recommended, when possible, due to superior efficacy of this combination over biologic monotherapy (no particular order or preference of treatment options).
† Dura on of disease/symptoms ≥6 months of mee ng 1987 ACR RA criteria.
‡ Dura on of disease/symptoms <6 months.
Singh JA, et al. Arthritis Rheumatol. 2016;68(1):1–26; Singh JA, et al. Arthritis Care Res. 2016;68(1):1–25; Smolen JS, et al. Ann Rheum Dis. 2017;0:1–18.
Combination DMARD Therapy
Anti‐TNF Biologic+/‐ MTX
Non‐TNF Biologic+/‐ MTX
JAK Inhibitor+/‐ MTX
After Failure with DMARD Monotherapy in RA Patients with Moderate or High Disease Activity*
EULAR 2017 RA Recommandations:In patients with poor prognostic factors, add a biologic or small‐molecule therapy
© 2019 PRIME® Education, LLC. All Rights Reserved.. 56
Real‐World Response to csDMARDs and bDMARDsAfter 1 year of Treatment
*Includes patients on tocilizumab, certolizumab pegol, golimumab, etanercept, adalimumab, and rituximab.
Boyadzhieva V, et al. EULAR 2019. Madrid, Spain. Abstract AB0233.
Prospective assessment of 344 patients with RA starting treatment with csDMARDS and/or corticosteroids vs bDMARDs* for 1 year
The bDMARD group had higher disease activity at BL vs the csDMARD group
11%
1%
13.50%
71%
16%
27%
0%
10%
20%
30%
40%
50%
60%
70%
80%
ACR50 ACR70 MDA
6‐Month Follow Up
csDMARDs (n = 220) bDMARDs (n = 124)
P = 0.002
P <0.001
20%
10%13%
36%
52%
30%
0%
10%
20%
30%
40%
50%
60%
ACR50 ACR70 MDA
12‐Month Follow Up
csDMARDs (n = 220) bDMARDs (n = 124)
P <0.001
P = 0.0102
P = 0.0186
P = 0.0025

29
© 2019 PRIME® Education, LLC. All Rights Reserved.. 57
Approved & Emerging Targeted Therapies for RA
Status Therapy Target Key Trials RouteDose
Frequency*
Approved
Rituximab CD‐20 IMAGE, DANCER, REFLEX IV Q6M (2 doses)
Abatacept CD80/CD86 AGREE, AIM, ATTAIN SC/IV QW/Q4W
Adalimumab TNF‐α ARMADA, DE019, DE011, ReAct SC Q2W
Certolizumab TNF‐α RAPID (1, 2), FAST4WARD SC Q2W/Q4W
Etanercept TNF‐α TEMPO, COMET, ERA SC QW
Golimumab TNF‐α GO (BEFORE, FORWARD, AFTER) SC/IV Q4W/Q8W
Infliximab TNF‐α ATTRACT IV Q8W
Anakinra IL ‐1R TRACK SC QD
Sarilumab IL‐6R SARIL‐RA (ONE, TARGET, ASCERTAIN, EXTEND, MONARCH, MOBILITY, EASY) SC Q2W
Tocilizumab IL‐6R FUNCTION, OPTION, RADIATE SC/IV QW/Q4W
Upadacitinib* JAK 1 SELECT (NEXT, BEYOND, EARLY, MONOTHERAPY, CHOICE, COMPARE) Oral QD
Baricitinib JAK 1/2 RA (BEGIN, BEYOND, BEACON, BUILD, BEAM) Oral QD
Tofacitinib JAK 1/3 ORAL (START, STANDARD, STEP) Oral BID/QD
Phase 3(Completed or ongoing)
Filgotinib JAK 1 FINCH 1‐3 Oral QD
Peficitinib JAK 1/3 NCT02305849, NCT01638013, NCT02308163 Oral QD
Olokizumab IL‐6 CREDO1‐4 SC Q2W/Q4W
*Not accounting for a loading dose; **Submitted for FDA approval. Estimated approval: Q3 2019.R = Receptor; SC = Subcutaneous; IV = intravenous; BID = Twice a Day.US Food and Drug Administration (FDA). www.accessdata.fda.gov. Accessed 6/7/18.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 58
Head‐to‐Head Comparison of TNF Inhibitorsin MTX‐IR and TNF‐IR Patients
Schiff M, et al. Ann Rheum Dis. 2014;73(1):86–94; Smolen JS, et al. Lancet. 2016;388(10061):2763–2774.
EXXELERATE: Certolizumab (TNF) vs Adalimumab (TNF)
Week
• Certolizumab vs adalimumab show comparable long term (2 years) efficacy and safety• In some patients, after primary failure of each of the two TNF therapies, the switch to the other therapy was associated with a potential
response
MTX Failure First TNF Failure
Patients (%)
100
80
60
40
20
0
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Non‐responders switch treatment at week 12
ACR20
ACR50
ACR70
Primary responders to certolizumab pegol plus methotrexate (n = 353)
Primary responders to adalimumab plus methotrexate (n = 361)
Week
Patients (%)
100
80
60
40
20
0
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Non‐responders switch treatment at week 12
Double non‐responders withdrawn at week 24

30
© 2019 PRIME® Education, LLC. All Rights Reserved.. 59
Blocking Signaling by Cytokine Receptors: Anti‐IL and ‐JAK Therapies
Figure adapted from Schwartz DM, et al. Nat Rev Drug Discov. 2017;16(12):843–862; Nakayamada S, et al. BioDrugs. 2016;30(5):407–419.
• T‐cell differentiation• Lymphocyte effector function• Macrophage activation
• T‐cell proliferation •T cell memory •T regulatory cell function • B cell function
JAK1JAK3
IFN‐γ
IL‐2, ‐4, ‐7‐9, ‐15, ‐21
IL‐6, ‐11
IL‐12, ‐23
• Acute phase response• Lymphocyte growth/differentiation• Catabolic metabolism • Lipid metabolism• Bone resorption• T‐cell differentiation • Lymphocyte effector function
• T‐cell differentiation • Lymphocyte effector function
IL‐3, ‐5,GM‐CSF
• Myeloid/lymphoid differentiation• T‐cell prolideration/survival •Lymphocyte effector function
JAK2JAK2JAK2JAK2
JAK2
JAK1
TYK2
TYK2 TYK2JAK1 JAK1JAK2 JAK2
EPO, TPO, C‐CSF, GH, Leptin
• Growth • Anabolic metabolism
IFN‐α / β
• Anti‐viral responses
© 2019 PRIME® Education, LLC. All Rights Reserved.. 60
Efficacy and Safety of Tocilizumab (IL‐6R) in MTX‐IR RA Patients
ACT‐RAY Phase 3b Trial ADACTA Phase 4 Trial
*An open‐label csDMARD other than MTX was added after Wk 24 for patients who did not achieve DAS28 <3.2 by 24 wks.
Dougados M, et al. Ann Rheum Dis. 2014;73(5):803–809; Gabay C, et al. Lancet. 2013;381(9877):1541–1550; Mohan S, et al. ACR 2017. San Diego, CA. Abstract 550.
3537
40
46
0
10
20
30
40
50
Week 24 Week 52*
Patients (%)
Tocilizumab (n = 229) Tocilizumab + MTX (n = 243)
P = 0.21 P = 0.03
DAS28‐ESR <2.6
8
7
6
5
4
3
2
1
0
Mean change = ‐1.8
Mean change = ‐3.3
0 4 8 12 16 20 24
DAS2
8
Time (Weeks)
Adalimumab (n = 162)Tocilizumab (n = 163)
Long‐term safety results across 12 RA clinical trials + global post‐marketing safety database (~600,000 patients) indicate that there is no increased safety risk with increasing exposure to tocilizumab.

31
© 2019 PRIME® Education, LLC. All Rights Reserved.. 61
Efficacy and Safety of Sarilumab (IL‐6R) in MTX‐IR RA Patients
MOBILITY Phase 3 Trial
33 32
17 18
7 9
58 54
37 40
20 25
66 59
46 43
25 27
‐
20
40
60
80
Week 24 Week 52 Week 24 Week 52 Week 24 Week 52
Patients
Placebo + MTX (n = 398) Sarilumab 150 mg + MTX (n = 400) Sarilumab 200 mg + MTX (n = 399)
MONARCH Phase 3 Trial
*P <0.0001
LS = Least Square.
Genovese MC, et al. Arthritis Rheumatol. 2015;67(6):1424–1437; Burmester GR, et al. Ann Rheum Dis 2017;76:840–847; Genovese MC, et al. Rheumatology (Oxford). 2018;57(8):1423–1431;
Genovese MC, et al. ACR 2018. Chicago, IL. Abstract 2509; Curtis JR, et al. EULAR 2019. Madrid, Spain. Abstract FRI0081.
‐1.88‐2.2
‐2.77*
‐3.28*‐4
‐3
‐2
‐1
0
0 12 24
LS M
ean
Chan
geFrom Baselin
e
Adalimumab (n = 185)
Sarilumab (n = 184)
DAS28‐ESR
ACR20 ACR50 ACR70
*
*
**
*
**
*
** * *
• Safety: neutropenia, injection site erythema, increased alanine aminotransferase, and URTI. Efficacy and safety profile of sarilumab remained consistent over 4 years.
• Post‐hoc analysis of EXTEND open‐label extension study: sarilumab monotherapy shows similar efficacy as sarilumab + csDMARDs
© 2019 PRIME® Education, LLC. All Rights Reserved..
62
ORAL Strategy Phase 3b/4 Trial
Clinical Outcomes at Month 6
Efficacy and Safety of Tofacitinib (JAK 1/3) in MTX‐IR Patients
38
18
10
46
25
12
44
21
12
0
10
20
30
40
50
ACR 50* ACR 70 DAS28‐4(ESR) < 2.6
Patients (%)
Tofacitinib (n = 384) Tofacitinib + MTX (n = 376) Adalimumab + MTX (n = 386)
*Primary endpoint.
Fleischmann R, et al. Lancet. 2017;390(10093):457–468; Cohen S, et al. ACR 2018. Chicago, IL. Abstract 963; Dikranian A, et al. EULAR 2019. Madrid, Spain. Abstract AB0454.
• Long‐term safety analysis with up to 9.5 years of follow‐up and 22,875 patient years of tofacitinib exposure indicate that incidence rates for AEs did not increase with prolonged tofacitinib exposure
• Non‐infectious non‐serious AEs were mild/moderate and the majority were self‐limiting (pooled analysis of 6 ORAL trials in 2,657 pts)

32
© 2019 PRIME® Education, LLC. All Rights Reserved.. 63
Efficacy and Safety of Peficitinib (JAK 1/3) in MTX‐IR Patients
Phase 3 Trial: Clinical Outcomes at Weeks 28 and 52/ET
ET = Early Termination.
*P <0.001 vs PBO; **For the calculation of mTSS, patients who discontinued at or before week 28/52 or were switched from PBO to peficitinib at week 12/28 due to lack of efficacy, week 28/ET was extrapolated using a linear extrapolation method based on the mTSS at BL and ET or week 12/28 (before switching).
Genovese MC, et al. Arthritis Rheumatol. 2017;69(5):932–942; Kivitz AJ, et al. Arthritis Rheumatol. 2017;69(4):709–719; Takeuchi T, et al. ACR 2018. Chicago, IL. Abstract 888; Takeuchi TT, et al. EULAR 2019. Madrid, Spain. Abstract OP0026; Tanaka YT, et al. EULAR 2019. Madrid, Spain. Abstract FRI0134.
• For weeks 0–12 there was similar overall incidence of AEs between PBO and peficitinib groups. For the overall study period (52 weeks), the incidence rate of serious infections per 100 patient years was higher with peficitinib than PBO.
• Peficitinib is also effective at reducing RA symptoms in DMARD‐IR patients
29
116
74
51
27
79
59
40
0
20
40
60
80
ACR20 ACR50 ACR70
Placebo (n = 170)Peficitinib 100mg QD (n = 174)Peficitinib 150mg QD (n = 174)
Patients (%)
* *
**
*
*
ACR20/50/70 at Wk 28 Modified Total Sharp Score (mTSS) at Wks 28 & 52
Mean (SD) mTSSchange from baseline
Placebo Peficitinib100 mg QD
Peficitinib150 mg QD
Week 28/ET(primary outcome)**
3.37 (5.46) 1.62 (4.23)* 1.03 (2.86)*
Week 52/ET 6.27 (10.18) 2.12 (5.83)* 1.54 (4.11)*
© 2019 PRIME® Education, LLC. All Rights Reserved.. 64
Efficacy and Safety of Baricitinib (JAK 1/2) in MTX‐IR Patients
*P ≤0.001 vs PBO; †P ≤0.05 vs adalimumab; ‡P ≤0.01 vs adalimumab
HAQ‐DI = Health Assessment Questionnaire Disability Index; PtGA = Patient Global Assessment of Disease Activity; FACIT = Functional Assessment of Chronic Illness Therapy; SF‐36 = Short Form Health Survey;
WPAI = Work Productivity and Activity Impairment; RTC = Renal Tubular Acidosis
Taylor PC, et al. N Engl J Med. 2017;376(7):652–662; Keystone EC, et al. Ann Rheum Dis. 2017;76(11):1853–1861; Dougados M, et al. Ann Rheum Dis. 2017;76(1):88–95; Kunwar S, et al. ACR/ARHP 2017. San Diego, CA. Abstract 530; Genovese MC, et al. EULAR 2019. Madrid, Spain. Abstract THU0078.
40
17 5
37
19 8
70
45
19
74
50
30
61
35
13
66
46
22
0
20
40
60
80
ACR20 ACR50 ACR70 ACR20 ACR50 ACR70
PBO + MTX (n = 488) Baricitinib + MTX (n = 487) Adalimumab + MTX (n = 330)
RA‐BEAM Phase 3 Results
Week 12 Week 24* †
*
* ‡
*
* †
*
* †
*
**
* †
*
• At week 52, baricitinib groups demonstrated significant improvements (P ≤0.05) in HAQ‐DI, PtGA, pain, FACIT, SF‐36, EQ‐5D and WPAI‐RA scores vs PBO and adalimumab groups.
• In the RA‐BUILD Phase 3 Trial, baricitinib monotherapy also showed significant improvements in clinical and patient‐reported outcomes.• In a meta‐analysis of 5 RTC, baricitinib:
– Demonstrated greater efficacy in improving clinical outcomes vs PBO– Increased AEs, but not severe or serious infections, vs PBO
• Integrated safety analysis demonstrated that baricitinib maintained safety profile for up to 7 years

33
© 2019 PRIME® Education, LLC. All Rights Reserved.. 65
Efficacy and Safety of Upadacitinib (JAK 1) in MTX‐IR Patients
¶ Indicates multiplicity‐controlled comparisons of upadacitinib vs placebo
UPA = Upadacitinib; ADA = Adalimumab; IR = Inadequate Response; PBO = Placebo; AE = Adverse Event; MTX = Methotrexate.
Burmester GR, et al. Lancet (London, England). 2018;391(10139):2503–2512; Fleischmann R, et al. Arthritis Rheumatol. 2019:art.41032. Epub ahead of print; Buch M, et al. EULAR 2019. Madrid, Spain. Abstract THU0165; Kremer L, et al. EULAR 2019. Madrid, Spain. Abstract FRI0155.
• Overall safety profile of upadacitinib was similar to that of adalimumab. The proportions of patients with serious AEs and AEs leading to discontinuation were highest for adalimumab; the proportion with herpes zoster and creatine phosphokinase elevations was highest for upadacitinib.
• Efficacy of UPA was comparable when administered as monotherapy or when given in combination with MTX or non‐MTX csDMARDS.
SELECT‐COMPARE Phase 3 (vs Adalimumab)
**P ≤0.01 vs PBO***P ≤0.001 vs PBO#P ≤0.05 vs ADA##P ≤0.05 vs ADA###P ≤0.001 vs ADAWeek
% Responders: ACR20
% Responders: DAS2
8CRP<2
.6
2 4 8 12 14 18 22 262 4 8 12 14 18 22 26
100
80
60
40
20
0
100
80
60
40
20
0
Week
© 2019 PRIME® Education, LLC. All Rights Reserved.. 66
Efficacy and Safety of Filgotinib (JAK 1) in MTX‐IR Patients
FINCH1 Phase 3 Trial
Combe B, et al. EULAR 2019. Madrid, Spain. Abstract LB001; Genovese MG, et al. EULAR 2019. Madrid, Spain. Abstract FRI0092; Kalunian K, et al. EULAR 2019. Madrid, Spain. Abstract FRI0154;
Westhovens R, et al. EULAR 2019. Madrid, Spain. Abstract LB0003.
Efficacy at Week 24
Patient with event, %FIL 200 mg(n = 475)
FIL 100 mg(n = 480)
ADA 40 mg(n = 325)
PBO(n = 475)
Serious AEs 4.4 5 4.3 4.2
Serious infections 1.7 1.7 2.5 0.8
Herpes zoster 0.4 0.4 0.6 0.4
Adjudicated MACEs 0 0.2 0.3 0.4
Venous thrombotic events
0.2 0 0 0.4
Malignancies 0 0.2 0.3 0.6
Deaths 0.4 0.2 0 0.4
Safety through Week 24
• Filgotinib was similarly safe and effective in younger and older (>65 yrs) patients (subanalysis of FINCH2)• Filgotinib + MTX therapy was effective and well tolerated in early RA patients naïve to MTX (FINCH 3)• Additional studies are being conducted to assess testicular safety of filgotinib
78
36
48
78
29
35
75
30
36
59
15 16
0
20
40
60
80
100
ACR20 ACR70 DAS28‐CRP≤2.6
FIL 200 mg (n = 475) FIL 100 mg (n = 480)ADA 40 mg (n = 325) PBO (n = 475)

34
© 2019 PRIME® Education, LLC. All Rights Reserved.. 67
ACR 2015 Recommendations for RA Patients with High‐Risk Comorbidities
*Consider using csDMARDs other than MTX or leflunomide.
TNF = Tumor Necrosis Factor; CHF = Congestive Heart Failure; HBV = Hepatitis B Virus; HCV = Hepatitis C Virus.
Singh JA, et al. Arthritis Rheumatol. 2016;68(suppl 1):1–26; Singh JA, et al. Arthritis Care Res. 2016;68(suppl 1):1–25.
High‐Risk Condition Recommendation(s) Evidence Type
CHF, including worsening on current TNF inhibitorUse combination DMARDs, non‐TNF biologic, or tofacitinib over anti‐TNF
Very low/moderate
Conditional
Active HBV infection, and receiving/received effective antiviral RxSame recommendations as in patients without HBV
Very low Strong
HCV infection, and receiving/received effective antiviral Rx Same recommendations as in pts without HCV Very low Conditional
HCV infection, and NOT receiving or requiring effective antiviral Rx Use csDMARDs* over anti‐TNF Very low Conditional
Previously treated or untreated skin cancer Use csDMARDs over biologics and tofacitinib Very low Conditional
Previously treated lymphoproliferative disorder Use rituximab over anti‐TNF Very low Strong
Previously treated lymphoproliferative disorderUse combination csDMARDs or abatacept or tocilizumab over anti‐TNF
Very low Conditional
Previously treated solid organ malignancySame recommendation as in patients without this malignancy
Very low Conditional
Previous serious infection(s)Use combination csDMARDs over anti‐TNFUse abatacept over anti‐TNF
Very low Conditional
© 2019 PRIME® Education, LLC. All Rights Reserved..
Management Following TNF Failure

35
© 2019 PRIME® Education, LLC. All Rights Reserved.. 69
After TNFi Failure – Cycle or Swap?
• Optimal treatment after TNFi failure remains unclear
Mostly registry studies and observational research
• Switching to another TNFi
May offer clinical benefit in some RA patients
Antidrug antibodies and seropositivity/negativity may guide choice of second biologic
• Switching to non‐TNFi biologic with different mode of action
Sarilumab, tocilizumab, tofacitinib, rituximab, abatacept effective after TNFi‐IR
• Choice may be driven by contraindications and safety factors
Nam JL, et al. Ann Rheum Dis. 2014;74(3):516–528; Schoels M, et al. Ann Rheum Dis. 2012;71(8):1303–1308; Favalli EG, et al. Rheumatology. 2014;53(9):1664–1668; Sullivan SD, et al. J Med Econ. 2013;16(3):391–396; Chatzidionysiou K, et al. Ann Rheum Dis. 2015;74(5):890–889; Emery P, et al. Ann Rheum Dis. 2015;74(6):979–984; Smolen JS, et al. Ann Rheum Dis. 2017;0:1–18; Smolen JS, et al. Lancet. 2016;388(10061):2763–2774.
© 2019 PRIME® Education, LLC. All Rights Reserved.. 70
2015 ACR RA Treatment Recommendations for After Biologic Therapy Failure
*e.g., If patient declines non‐TNF biologic therapy due to inefficacy or side effects.
Singh JA, et al. Arthritis Rheumatol. 2016;68(1):1–26; Singh JA, et al. Arthritis Care Res. 2016;68(1):1–25.
Failure Type Conditional Recommendation ± MTX
• Single TNFi or non‐TNF biologic failure • Non‐TNF biologic
• ≥1 TNFi and ≥1 non‐TNF biologic failure • ≥2 TNFi failures
• Non‐TNF biologic • Tofacitinib if non‐TNF biologic is not an option*
• ≥2 non‐TNF biologic failures and patient is TNFi‐naive • TNFi
Failure defined as patients with moderate or high disease activity despite biologic DMARD therapy

36
© 2019 PRIME® Education, LLC. All Rights Reserved.. 71
Head‐to‐Head Comparison of TNF Inhibitorsin MTX‐IR and TNF‐IR Patients
Schiff M, et al. Ann Rheum Dis. 2014;73(1):86–94; Smolen JS, et al. Lancet. 2016;388(10061):2763–2774.
EXXELERATE:Certolizumab (TNF) vs Adalimumab (TNF)
Week
• Certolizumab vs adalimumab show comparable long term (2 years) efficacy and safety• In some patients, after primary failure of each of the two TNF therapies, the switch to the other therapy was associated with a potential
response
MTX Failure First TNF Failure
Patients (%)
100
80
60
40
20
0
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Non‐responders switch treatment at week 12
ACR20
ACR50
ACR70
Primary responders to certolizumab pegol plus methotrexate (n = 353)
Primary responders to adalimumab plus methotrexate (n = 361)
Week
Patients (%)
100
80
60
40
20
0
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Non‐responders switch treatment at week 12
Double non‐responders withdrawn at week 24
© 2019 PRIME® Education, LLC. All Rights Reserved.. 72
70%
60%52%
43%
0%
20%
40%
60%
80%
24 Weeks 52 Weeks
Non‐TNF Biologic Group (N=146) Second Anti‐TNF Group (N=146)
Non‐TNF vs TNF Treatment Efficacy After 1st TNF Failure*
HAQ = Health Assessment Questionnaire .
Gottenberg JE, et al. JAMA. 2016;316(11):1172–1180.
• HAQ Scores did not differ between the two groups at week 12, 24, and 52• ~50% of patients with insufficient response to a TNF‐α inhibitor might respond to a second anti‐TNF agent• However, a therapeutic response was more frequent with non–TNF‐targeted biologics
Response Criteria in the Non‐TNF Biologic and Second Anti‐TNF Groups
45%41%
28%23%
24 Weeks 52 Weeks
EULARGood or Moderate Response
Low Disease ActivityDAS28‐ESR <3.2
27% 27%19%
14%
24 Weeks 52 Weeks
DAS28 RemissionDAS28‐ESR <2.6
Patients (%)

37
© 2019 PRIME® Education, LLC. All Rights Reserved..
Considerations for Payer & Provider Collaboration
© 2019 PRIME® Education, LLC. All Rights Reserved.. 74
Payers’ and Providers’ Perceptions in RA Management
Greenaple R. Am Health Drug Benefits. 2012;5(2):83–92.
2011 parallel‐structure online surveys of 100 rheumatologists and 50 health plan payers representing >80 million covered lives
Ranked Order of Importance for Choosing Preferred Biologics
Question: Please rank in order of importance (from highest to lowest) the reasons for your choice of preferred biologic(s).
Rheumatologists (n = 53) Rank Payers (n = 28)
Efficacy profile 1 Efficacy profile
Safety profile 2 Contracting/rebating
My personal experience 3 Safety profile
Mode of administration 4 Mode of administration
Frequency of dosing 5 Market share
Reimbursement easier to obtain on most health plans
6Utilization rate among plan’s
in‐network physicians

38
© 2019 PRIME® Education, LLC. All Rights Reserved.. 75
Actions to Improve Payer‐Provider Collaboration
With payers…
• Develop positive working relationships with key decision‐makers
• Ensure both parties are working under the same expectations and timelines
• Become familiar with the terminology and buzzwords used by payers
• Ask to speak with peers within the organization
Within your practice…
• Document patient and clinical information thoroughly
• Verify patient coverage before prescribing therapy or service
• Enlist team members to take the lead on the PA process and other payer‐related processes
• Use electronic methods for completing and submitting PAs
© 2019 PRIME® Education, LLC. All Rights Reserved.. 76
Supporting Patient Navigation of and Access to Care
PSP = Patient Support Program; PA = Prior Authorization.
Rubin DT, et al. J Manag Care Spec Pharm. 2017;23(8):859–867.
Patient Support Programs
• Available through patient advocacy organizations and pharmaceutical companies
• Offer nurse navigators, financial assistance, educational resources, adherence support, and others
• Participation in PSPs increases adherence and persistence to TNF therapy by while reducing medical costs
Case Management
• Offered through insurance companies, health‐care systems, or patient support programs
• Instrumental in assisting both providers and patients navigate clinical care and managed care processes
• They build relationship with patients, and can identify adherence or socio‐economic issues that impact clinical outcomes
Specialty Pharmacy
• Key player in the management of patients with chronic illnesses (e.g., medication reconciliation and patient education)
• Support practices on PA‐related processes like submission and appeals,
• Triage between practices and insurance companies to improve communication and comply with required processes

39
© 2019 PRIME® Education, LLC. All Rights Reserved.. 77
Benefits of Involving an NP/PA Within Rheumatology Care
Observational Cohort Study in 7 Rheumatology Practices in the US
APP = Advanced Practice Provider.
van Eijk‐Hustings Y, et al. Ann Rheum Dis. 2012;71(1):13–19; Solomon DH, et al. Arthritis Care Res (Hoboken). 2015;67(12):1664–1670.
RA patients seen in practices with NP/PAs had lower disease activity over 2 years vs those in rheumatologist‐only practices
For APPs, the scope of practice (practice autonomy and prescriptive authority) varies
state to state and is often defined by a practice agreement with the leading specialist.
• Rheumatology nurse care for people with these conditions has been shown to: Better education and improve psychosocial support for
patients
Reduce delays in access to specialist care
Improve care coordination and continuity of care
Reduce health system costs in primary and secondary care
Improve patient outcomes and satisfaction with care
With NP/PAs MD Only P
Patient Load 158 143 ‐
Total Visits 1,168 814 ‐
Visits per Patient 7.4 ± 2.6 5.7 ± 1.9 <0.0001
Laboratory Test 950 (81%) 501 (62%) <0.001
Radiology Tests 232 (20%) 110 (14%) <0.001
High Disease Activity 15 (15%) 27 (44%) <0.0001
DMARD Starts 103 (9%) 62 (8%) 0.01
Patients on Synthetic DMARDs 135 (85%) 105 (73%) 0.01
Patients on Biologic DMARDs 126 (80%) 67 (47%) <0.0001
© 2019 PRIME® Education, LLC. All Rights Reserved.. 78
Credit Center
To receive credit please visit
www.primeinc.org/credit
and enter program code
11PR193