Embed Size (px)
Citation preview

CHAPTER 62
Maxillofacial injuries
62.1 The general method for maxillofacialinjuries
A patient with a severe facial injury is a very distressingsight—so distressing that you may feel that you can do noth-ing for him. In fact, you can do much, and maxillofacial in-juries are no more difficult (or easy) than any others. Theyare usually the result of road accidents, and seat belts pre-vent most of them.
Not suprisingly, the parts of the face which stick out arethose which are most often injured—a patient’s nose, his zy-goma, or his mandible. Fortunately, their injuries are usu-ally not too difficult to treat. Much greater force has to beapplied to fracture his maxilla, with the result that maxil-lary injuries are less common, but much more difficult. Al-though we describe each injury separately here, a patient islikely to have several of them, and other injuries also, espe-cially injuries to his head and eyes.
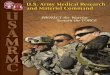
Fractures of the middle third of the face are so complexthat we shall not attempt to classify them except to say thatthe usual classification is that of Le Fort, who divided theminto Types One, Two, and Three, as shown in Fig. 62-1. Ina Type One fracture the alveolus, or tooth bearing part ofthe patient’s upper jaw, breaks off, and may drop onto hislower teeth. In Types Two and Three the fracture lines arehigher up in his maxilla. These fracture types may be com-bined, and may occur on one or both sides. The radiology,reduction, and fixation of the more difficult Le Fort fracturesis beyond a district hospital. But prompt treatment, partic-ularly in securing a patient’s airway, may save his life, afterwhich you have several days in which to refer him for ex-pert reduction and fixation. Failure to reduce one of thesefractures can cause severe deformities, which include a jawwhich does not close, ’dish face’, and diplopia. If you can-not refer a patient, we describe some of the easier methodsyou can use.
WHAT OTHER INJURIES DOES THE PATIENT HAVE?
The critical displacement in Le Fort fractures of TypesTwo and Three is the downward movement of the bones ofthe middle of the patient’s face, as shown in Fig. 62-2. Thestrong front of his cranium forms an inclined plane, downwhich his facial skeleton slides. (1) This lengthens his face.
FRACTURES OF THE MIDDLETHIRD OF THE FACE
3
2
1
fractures ofthe nasalcomplex
fractures of thezygomaticcomplex
alveolus
alveolus becomes loose and dropsIn a Le Fort type I fracture the
onto the lower teeth
Le Fort fractures
Fig. 62.1: FRACTURES OF THE MIDDLE THIRD OF THE FACE. In aType One fracture the alveolus, or tooth bearing part of the patient’s upperjaw, breaks off, and may drop onto his lower teeth. In Types Two and Threethe bones of the middle of the patient’s face slide downwards, as shown inthe next figure. These fracture types may be combined and may occur onone or both sides.
(2) It pushes his upper molars down onto his lower onesso that they gag (prevent his jaw closing properly). (3) Itpushes his soft palate down onto his tongue and preventshim breathing through this mouth. At the same time, hisfracture bleeds severely, and his nose is obstructed by bloodclot. The result is that he may suffocate, so the immediate lifesaving procedure is to hook two of your fingers round the back of ishard palate, and pull his maxilla back up the inclined plane of hisskull. This will allow him to breathe. His breathing can alsobe obstructed by bilateral fractures of his lower jaw whichallow his tongue to fall back against his pharynx.
Fractures of the middle third of a patient’s face have sev-eral other unfortunate features: (1) They are always multi-
1

62 Maxillofacial injuries
respiratory obstructiontreated with anasopharyngeal airway
the front of theskull forms oninclined plane
maxillapusheddownwards
respirationobstructed, softpalate pusheddown onto tongue
DOWNWARDDISPLACEMENTOF THE MAXILLA
A
B C D
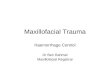
Fig. 62.2: DOWNWARD DISPLACEMENT OF THE MAXILLA. A,if the patient’s respiration is obstructed, push a nasopharyngeal airwaydown one or both sides of his nose. B, C, and D, show how the front of hisskull forms an inclined plane down which his maxilla can be pushed. AfterKilley, with kind permission.
ple, sometimes with 50 or more fragments. (2) Several ofhis cranial nerves may be injured, especially his infraorbitaland superior dental nerves. (3) His ethmoid may be frac-tured and his dura torn, so that CSF leaks from his nose.(4) His orbit may be fractured (Fig. 62-3), sometimes withthe displacement of its contents into his maxillary sinuses(the orbital blow-out syndrome). (5) The circulation to hiseye may be obstructed and make him blind if the obstruc-tion is not relieved within minutes of the accident (the oph-thalmic canal syndrome). (6) His maxillary sinuses may fillwith blood. (7) His nasolachrymal ducts may be injured andcause a flow of tears.
When you treat such a patient aim to: (1) Restore his air-way. (2) Control bleeding. (3) Make his teeth bite normally.You should be able to do this with most fractures of hismandible, and some fractures of his maxilla. If either hismaxilla or his mandible is intact, you can use one of them tosplint the other. If you can make his bite normal, reduction willbe perfect. (4) Prevent some deformities by reducing fracturesof his nose and zygoma.
If you can refer a patient, do so early because the longeryou wait, the more difficult reduction will become. If youcannot refer him, you can certainly save his life, but he mayhave to live with his deformities. Soon after the injury hisface will look distressingly swollen, so do your best to reas-sure him and his family. The face has a good blood supplyand will heal well, so that they can expect him to improveremarkably. But it can also swell quickly and hide under-lying deformities, so examine him with care when you firstsee him.
The methods we describe assume you don’t have a den-tal laboratory, and so cannot make cap splints, etc. Youwill however need a drill and some soft stainless steel wire
(70.9). Occasionally an arch bar is useful. If you can get thehelp of a dentist, always do so.
•ARCH BAR, stainless steel, five only. Sometimes, the most con-venient way to fix the fragments of a patient’s upper or lower jawis to bend a metal bar, to shape it, and to wire it to his teeth. Ifyou don’t have a proper arch bar, you can use any tough piece ofstainless steel wire, or even some paper clips twisted together.
A SWOLLEN FACE CAN CONCEAL A MAJOR INJURY
THE GENERAL METHOD FOR A MAXILLOFACIALINJURY
This extends Section 51.3 on the care of a severely injuredpatient. Injuries to his lower jaw are described i n Section62.7.
IMMEDIATE TREATMENT
CAN THE PATIENT BREATHE? If his breathing is difficult,look into his mouth to see if: (1) his airway has been ob-structed by blood and vomit, (2) his soft palate has beendriven down onto his tongue by displaced Le Fort fractures,or if, (3) his tongue has fallen backwards after a mandibularfracture?
If his soft palate has been driven onto his tongue,hook your fingers round the back of his hard palate, andpull the bones of the middle of his face gently upwards andforwards, so as to restore his airway and perhaps the circu-lation to his eyes. Reduction may not be easy, and you mayneed considerable force. If the fracture is impacted and youfail to reduce it, he may need a tracheostomy, as describedbelow.
If necessary, grip his maxillary alveolus with the specialforceps (Rowe’s) for this purpose, or with suitable strong
THE ORBITALBLOW−OUTSYNDROME
B
loss of upwardmovement
enophtalmus
depression
orbitalfloor antrum
A
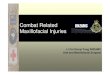
Fig. 62.3: THE ORBITAL BLOW-OUT SYNDROME. A, a blow to thepatient’s orbit has broken its floor, so that its contents have prolapsed intohis antrum. B, unless you refer him to have it repaired, he may have per-manent enophthalmos, diplopia and loss of upward eye movement. FromRutherford, Nelson, Weston and Wilson with kind permission.
2

62.1 The general method for maxillofacial injuries
A MAXILLOFACIALINJURY
A
C
B
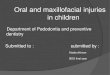
Fig. 62.4: A SEVERE MAXILLOFACIAL INJURY A, note that a con-scious patient is likely to be more comfortable sitting forward. B, and C, ifhe has much tissue loss, transport him face down like this. After Killey withkind permission.
sharp toothed forceps, and rock it to disimpact the frag-ments.
If his tongue or lower jaw has fallen backwards, putsome sutures or a towel clip through it, and gently pull itforwards. Lying him on his side will also help. When youtransport him, lie him on his side.
If he has a severe jaw injury with much tissue loss,transport him lying on his front with his head over the endof the stretcher and his forehead supported by bandagesbetween its handles, as in Fig. 62-4.
If he feels more comfortable sitting up, let him do so.His airway may improve remarkably when he does this.
Suck out his mouth, remove blood clots, debris, looseteeth, vomit, and foreign bodies.
A Guedel airway does not help, so don’t waste time tryingto insert one. Tracheal intubation is usually impractical.
If his nose is severely injured and bleeding, suck itclear and insert a nasopharyngeal tube, or any similar thickrubber tube, down one side. Put a safety pin through it tostop it slipping, as in A, Fig. 62-2.
CAUTION! A nasopharyngeal tube does not always en-sure a clear airway because it may kink or block againstthe posterior pharyngeal wall, so watch it carefully and twistand adjust it as necessary. Keep it sucked out by passinga smaller tube down it, attached to a sucker. Use the sameequipment to suck out the patient’s mouth, and keep it be-side his bed.
Tracheostomy. You may need to do a tracheostomy(52.2) if: (1) You cannot disimpact and reduce the fractureof the middle third of a patient’s face. (2) You cannot controlsevere posterior bleeding. (3) He has oedema of his glot-tis, particularly following a neck injury. (4) He has a severeinjury with much tissue loss. Tracheostomy will be difficult.Use ketamine, local anaesthesia and a cuffed tube.
CAUTION! If his breathing is in danger and you have torefer him, he will be safer with a tracheostomy than with asuture through his tongue to pull it forward, which is the otheralternative.
STOP BLEEDING Tie any large bleeding vessels. If there
Cerebrospinalrhinorrhoea
Retrobulbarhaemorrhage
TWO COMPLICATIONS
BA
Fig. 62.5: TWO COMPLICATIONS OF A HEAD OR MAXILLOFA-CIAL INJURY A, fractures of a patient’s ethmoid may make his CSF leak.B, a fracture of the base of his skull may cause severe proptosis and com-press his optic nerves. Drain the blood by making an incision near hisouter canthus. After Duke Elder.
is troublesome oozing, apply an adrenaline soaked packfirmly to the bleeding surface. A postnasal pack (Chapter24) will usually stop bleeding. If necessary, use large tempo-rary haemostatic sutures (3.1), but take care not to stranglethe tissues.
If a wound is deep, be prepared to pack it. Occasionally,you may have to tie a patient’s external carotid artery (3.5).
SHOCK is unusual. If a patient is shocked, suspect thathe also has an abdominal or a thoracic injury.
THE HISTORY AND EXAMINATION OF AMAXILLOFACIAL INJURY
The patient is probably unable to talk, so enquire from ob-servers if he lost consciousness and so might have a headinjury (63.1).
Gently wash his face with warm water to remove cakedblood. Look at it carefully for asymmetry. Compare one sidewith the other throughout the examination. Is his nose or hisface flattened? If you suspect a fracture of his zygoma, lookat it from above and below and use the two pencil test in Fig.62-12.
BRUISING This is a useful guide to underlying injuries.Zygomatic fractures There is always bruising round the
patient’s orbits, which develops rapidly as a uniform continu-ous sheet. It is limited peripherally by the attachments of hisorbicularis muscle, and extends subconjunctivally towardshis eye from the lateral side. Ask him to look inwards Youwill see bruising extending back into his orbit without a pos-terior limit.
Look inside his mouth and examine his upper buccal sul-cus for bruising, tenderness, and crepitation over his zygo-matic buttresses.
Nasal fractures There is bruising round his orbits whichis most severe medially.
Black eye This is the main differential diagnosis. Or-bita bruising is most severe medially. It is subconjunctival,patchy, and bright red.
EYES Has either of the patient’s eyes sunk inwards ordownwards? Are they level? Displacement may indicateherniation of the contents of his orbit through its floor into hismaxillary sinus, or a fracture at the fronto–zygomatic sutureline.
Separate his eyelids, and test the sight of each of his eyesseparately. If an eye is blind, its optic nerve may be injured.
3

62 Maxillofacial injuries
Ask him to follow your finger as you test for diplopia. Thismay be due to: (1) displacement of his orbit, (2) displace-ment of his globe, (3) a 6th nerve palsy, or (4) oedema. If hiseye is unable to look upwards, its inferior rectus is trapped,and his orbital floor is probably fractured. Note the size ofhis pupils and their reaction to light.
If he has massive proptosis, he has a retrobulbar haem-orrhage which may be compressing his optic nerve. Makea small incision at his outer canthus, take a haemostat andpush this into the incision (B, Fig. 62-5); blood will squirt out.If you don’t do this, his eye will become blind.
FRACTURES OF THE FACE AND SKULL Carefully feelall over the patient’s head and face for tenderness, step de-formities, irregularity, or crepitus. Feel his zygomatic bones,the edges of his orbits, his palate, and the bones of his nose.In a Le Fort Type Two or Three fracture you will feel manysmall bony fragments under the skin in his ethmoid region.
Hold the root of his nose between your finger and thumb.At the same time put two fingers from your other hand intohis mouth. If you can move his facial skeleton on his skull,he has a Le Fort fracture. You may feel it move more easilyif you hold his upper gum between your thumb and indexfinger.
Can he open and shut his mouth, bite normally, move hisjaw from side to side and protrude it? Do his teeth meetnormally? If his bite is abnormal, one or both of his jawshave been fractured. Failure to move his jaw normally mayindicate a displaced fracture of his zygoma or his mandible.
Examine the mucosa of both his jaws for bruising, tender-ness, irregularity, and crepitus.
NERVE INJURIES Test for anaesthesia of his cheeks (in-fraorbital nerves) and upper gums (superior dental nerves).
TOOTH INJURIES Feel his teeth and try to rock them.Individual teeth may move abnormally, so may several adja-cent teeth. Mobile teeth can be caused by: (1) A fracture.(2) Exposure of their roots. (3) Periodontal disease.
Inspect his teeth with a mirror and probe. Tap them; ifthey give a cracked cup’ sound, the bone above them maybe fractured. If a piece of tooth is missing, X-ray the patient’schest in case he has inhaled it.
NOSE INJURIES Epistaxis is usually unilateral or absentin zygomatic fractures, and bilateral in nasal ones. Examinethe patient’s nasal septum with a speculum. This may bedisplaced in a nasal fracture. However, it is often asymmet-rical in otherwise normal people. If he has a haematoma ofthe septum, it needs evacuating, goto 61.4.
LEAKING CSF may be anterior or posterior, and is usuallydiagnosed after a few days when bleeding and oedema havesubsided. The patient may complain of a salty taste in hismouth. If you are uncertain if a discharge is CSF or not,test it as in Section 63.12. CSF may leak in severe naso–ethmoidal ractures and in some Le Fort fractures.
OTHER INJURIES Look for these (51.3), and especiallyfor a head injury (63.1), or an injury to the patient’s cervicalspine (64.3). These may be more serious than those of hisface. A maxillofacial injury does not usually cause shock,so if he is shocked, suspect some other injury, especially anabdominal one, which may take priority.
X–RAYS are difficult to interpret, and involve turning thepatient into a position which may obstruct his airway. Askfor: (1) An AP view of his mandible. (2) A Waters view ofhis skull in which you maybe able to recognise: (a) filling ofhis maxillary antra, and (b) irregularities in the outlines of his
orbits showing they have been fractured.
WOUND TOILET AND CLOSURE AFTER AMAXILLOFACIAL INJURY
This must be thorough, especially if sand or tar are ingrainedIn the patient’s wounds. If you don’t remove them, severefibrosis and disfigurement will follow. You will find a steriletoothbrush useful.
Handle his tissues gently with skin hooks and fine for-ceps. Remove soiled tags of deeper tissues and mucosawith scissors. Trim only 1 or 2 mm of skin edge to providenon–bevelled uncontaminated skin edges which you can ap-proximate accurately. Use a sharp No. 15 blade and oph-thalmic scissors. Close his mucosa with 310 silk, or failingthis with fine chromic catgut. Close his skin by primary su-ture after you have fixed any fractures. If necessary, you canundermine the skin of his face for 2 to 3 cm to assist closure.
If part of the patient’s cheek Is missing, refer him im-mediately for primary reconstruction. If this is impractical,stitch his buccal mucosa to his skin (61-4). If necessary, dothe same with his nose.
If there are loose bone fragments, conserve them un-less they are grossly soiled. You can sterilize detached frag-ments in boiling water and replace them as chip grafts.
CAUTION! (1) Don’t close his skin under tension. (2)Don’t leave bone bare—try to cover all bony surfaces.
REDUCING FRACTURES AFTER A MAXILLOFACIALINJURY
Reduce and, where necessary, fix any fractures of the pa-tient’s nose (62.4), zygoma (62.5), and mandible (62.7).These are not urgent operations, so resuscitate him first.For anaesthesia, see A 6.4, and A 16.10. You can do mostoperations on an injured jaw using pterygopalatine blocks,bilaterally if necessary.
EXAMININGA ZYGOMATICINJURY
A B
C D E
antrum
if the body of hiszygoma is depressedone finger will be lowerthan the other feel for
tenderness
feel insidehis mouth
Fig. 62.6: EXAMINING A ZYGOMATIC INJURY A, the zygoma formsthe prominence of the check, and also the floor and lateral wall of the orbit.The maxillary antrum extends into it. B, if a fragment of the zygoma isdisplaced downwards, the patient’s lateral canthus will also be displaceddownwards, and his palpebral fissure will be oblique. C, press gently. Ifthe body of his zygoma is depressed, one finger will be lower than the other.D, press gently on the lower border of his orbit, you may elicit tendernessand feel a fracture between his zygoma and his maxilla. E, feel inside hismouth for a fracture in the lateral wall of his maxillary antrum. See alsoFig. 62-12. After Watson Jones with kind permission.
4

62.2 Injuries to the teeth an alveolus
CAUTION! Always protect a patient’s eyes when you op-erate on his face.
If he has a Lie Fort fracture, or an orbital floor fracture,refer him. If you cannot refer him, the next section (62.2)describes some methods you may be able to use.
NURSING A MAXILLOFACIAL INJURY
If the patient is conscious, sit him well forward, so that histongue falls forward, and blood and saliva can dribble out ofhis mouth. This will make him comfortable and also help himto breathe.
If he is unconscious, turn him onto his side into the re-covery position (51-2), so that blood and saliva can run outof his nose and mouth. If other injuries prevent this, put apillow under one shoulder, and turn his head to the otherside.
FOOD AND FLUIDS If the patient is to be operated on,withhold these. Otherwise feed him through a tube.
CLEANING AND DISINFECTION is critically important forthe healing of all wounds inside a patient’s mouth. Ask himto rinse out his mouth after eating, using :(1) a rinse contain-ing 10 ml of 0.5% chlorhexidine, or (2) 2% salt solution, orfailing either of these, (3) plain water. As soon as possible,encourage him to clean his teeth regularly with a toothbrushor a clean chewing stick.
Coat his lips liberally with vaseline to stop them stickingtogether and interfering with his respiration.
DRUGS FOR A MAXILLOFACIAL INJURY
Give the patient amoxycillin, ampicillin, or fortified procainepenicillin for one week. Start immediately (2.7). This usuallyprevents bone infection, and is important if a fracture opensinto his mouth.
If his CSF is leaking, give him 1 g of sulphadimidine 6hourly until 48 hours after it has stopped. Most leaks stopspontaneously, except in severely comminuted fractures.
CAUTION! Don’t give him powerful analgesics, such asmorphine, which will depress his cough reflex. If he is rest-less, give him paradelyde or diazepam.
Don’t forget tetanus prophylaxis (54.11).CHARTS Start a head injury chart (63-4) and a fluid bal-
ance chart (A 15-5).
FURTHER MANAGEMENT OF A MAXILLOFACIALINJURY
If possible, refer all more serious injuries. Read on for in-juries to a patient’s teeth and alveoli (62.2), simpler methodsfor maxillary fractures (62.3), fractures of the patient’s nose(62.4), fractures of his zygomatic complex (62.5), dislocationof his jaw (62.6), the general method for a dislocated lowerjaw (62.7), fractured condyles (62.8), fractures of the as-cending ramus of his mandible (62.9), fractures of the angleand body of his mandible (62.10), difficulties with mandibularfractures (62.11), and fixing mandibular fractures with acrylicresin (62.8).
TRANSPORT MAXILLOFACIAL INJURIES PRONE OR LYINGON THEIR SIDES
62.2 Injuries to the teeth an alveolus
The front of a patient’s upper jaw is most at risk. In less se-vere injuries only his teeth are damaged, in more severe oneshis alveolus may be fractured. Although injured teeth donot threaten life, they are acutely painful, especially whenthe pulp is hanging out. When a tooth is hit: (1) its crownmay fracture, (2) its root may fracture, (3) the whole toothmay subluxate, (4) it may be impacted into the surroundingtissue, or, (5) it may be inhaled, and be followed by a lungabscess.
INJURIES TO THE TEETH AND ALVEOLUS
If the patient’s oral mucosa is torn, suture it with fine 4/0waxed silk or chromic catgut.
If the crown of a patient’s tooth is missing, its exposedpulp will be visible as a pink spot on the root surface. It willbe acutely painful, so touch it with phenol on a small piece ofcotton wool. This will kill and anaesthetize the nerve. Takea chest X–ray in case he has inhaled the missing fragment.It will have to be removed by bronchoscopy.
If a tooth is only mildly subluxed, leave it in place; it willprobably tighten up and live. Meanwhile splint it with a pieceof lead foil or the top of a milk bottle moulded to the toothand gum.
If a tooth is so loose that you can lift it up and downin its socket, remove it. A dentist may be able to splint itand re–implant it, if he sees it soon enough, so don’t delay.
If there is an opening between a patient’s antrum andhis mouth, try to close it. If his antrum is already infected,leave it open and irrigate it daily. Don’t pack it.
COMMINUTED FRACTURES OF THE ALVEOLUS If thebony fragment with its teeth is still attached to periosteum,leave it, and splint the patient’s teeth as best as you canwith an arch bar. If the fragment of alveolus is completelydetached from the periosteum, dissect it out and remove it.
GAPS IN THE MAXILLARY SINUS Close these temporar-ily by packing them with gauze impregnated with bismuth,iodoform, and paraffin paste (BIPP), or with vaseline gauze.As soon as the patient’s general condition is stabilized, closethe gap with a flap of mucosa from his adjacent cheek. Su-ture it carefully, preferably with 3/0 black waxed silk sutures.Tell him not to blow his nose and to sneeze with his mouthopen.
MISSING DENTURES A piece of denture can also be in-haled. It is unlikely to be radio–opaque, so a normal chestX–ray does not exclude inhalation.
62.3 Simpler methods for maxillary fractures
There are few easy methods for Le Fort fractures. If the pa-tient is lucky enough to have an intact mandible, you canwire his broken maxilla to it. Packing his maxillary sinusesand repairing his orbital floor are beyond a district hospital.
Le Fort Type One fractures with an intact mandibleAlveolar fractures are quite common, so to be able to doanything for them is useful. Although they are much eas-ier to fix if the patient has an intact mandible, you may beable to fix a mandibular fracture with an arch bar, and thenproceed as if his mandible were intact.
5

62 Maxillofacial injuries
unilateralalveolarfractureLe Fort I
interdentalwiring on theother side
gross malocclusion
wire roundzygomaticarches Kirschner
wire
bilateral alveolarfractures, Le Fort I
eyeletwires
central part offace loose, Le Fort II
METHODS FORLE FORTFRACTURES
A
D
No!
B C
E F G
Fig. 62.7: SIMPLER METHODS FOR LE FORT FRACTURES. A, in-terdental wiring holding a unilateral fracture in place. B, wire roundthe patient’s zygomatic arches holding a bilateral fracture in place. C, aKirschner wire holding the central part of his face in place. D, this figurewas drawn from a cast, and shows what can happen if you fail to reduce asevere maxillary injury. Note the gross malocclusion. The patient’s jawswill have to be refractured and reset. Aligning them would have beenmuch easier at the time of the injury. E, a lumbar puncture needle hasbeen passed medial to his zygomatic arch into his upper buccal sulcus, andwas passed down it. F, the needle has been withdrawn. G, the needle is be-ing passed lateral to the zygomatic arch. Kindly contributed by Susan Likimaniand Andrew Curnock.
If he has a Le Fort Type One fracture on one side only, halfhis alveolus hangs loose on that side, as in A, Fig. 62-8. Ifhis mandible is intact you can wire it to the intact half of hisalveolus, so that it holds the fractured half reduced.
If his alveolus has fractured on both sides, and he has anintact mandible, you can wire his zygomatic arches on bothsides to his mandible, as in B, Fig. 62-8.
Type Two Fractures In some Type Two fractures the zy-gomatic arches are intact, but the bones of the centre ofthe patient’s face are displaced. You may be able to drilla Kirschner wire through one zygomatic arch, through thedisplaced central fragment of the face, and then out throughthe other arch.
WIRING THE ZYGOMATIC ARCH TO THE MANDIBLE
INDICATIONS Maxillary fractures with an intact mandible.ANAESTHESIA Premeditate the patient well and use in-
filtration anaesthesia of his gums (A 6.3).Fix wire eyelets to his teeth on both sides of his lowerjaw
as in Section 62.10.Protect his eyes as in Section 62.4. Push a blunt aspi-
ration needle or large lumbar puncture needle through hisskin just above his zygomatic arch and posterior to his outercanthus. Push the needle downwards behind his zygomaticarch into his superior buccal sulcus, as in E, Fig. 62-8.
Thread wire through the needle and then remove the nee-dle, leaving the wire in his tissues (F).
Now pass the needle up from his buccal sulcus, superficialto his zygomatic arch, under his skin, to come out of thesame hole in his skin as the wire (G).
Pass the other end of wire through the needle so that itemerges in his buccal sulcus. Remove the needle. You willnow have a loop of wire passing round his zygomatic archwith both ends emerging in his buccal sulcus.
Repeat the process on the other side, and then join thewire loops to the eyelets that you have previously fixed to hismandible.
62.4 Fractures of the nose
A patient’s injured nose is displaced, swollen and bleeding.Sometimes the swelling hides his displaced bones under-neath, so always suspect a fracture after any blow on thenose. He may have blood in his orbits and under the medialhalves of both his conjunctivae.
A force applied to the side of the nose pushes it sideways.A force applied from in front squashes it and splays it out-wards. If you don’t treat these injuries, they produce the de-formities shown in Fig. 62-9. If the force is severe enough,it can: (1) Fracture the frontal processes of a patient’s maxil-lae. (2) Displace his nasal cartilages. (3) Dislodge his septalcartilage from its groove in his vomer. (4) Comminute hisvomer. (5) Fracture his ethmoid bones so that CSF flowsfrom his nose.
TREATING A BROKEN NOSE
See also Section 61.4.CONTROLLING BLEEDING If this is severe, pack the pa-
tient’s nose with ribbon gauze soaked in saline. Treat him assoon as possible without waiting for the swelling to go down.
6

62.4 Fractures of the nose
UNREDUCEDNASAL FRACTURES
A blow from in front
A blow from the side
deviation of the nose
depressed bridgeof the nose
Fig. 62.8: UNREDUCED FRACTURES OF THE NOSE. If you don’treduce a patient’s broken nose, these are some of the possible results. AfterKilley, permission requested.
EQUIPMENT If possible, use Walsham’s forceps to re-duce his nasal bones, and Ash’s forceps to straighten hisnasal septum. If you don’t have them, you can use any stoutclamp, but don’t close it tight. Walsham’s forceps don’t quitemeet, and therefore don’t crush tissue.
ANAESTHESIA (1) Pterygopalatine block (A 6.4). (2)Give the patient a general anaesthetic, and pass a trachealtube (A 13.2). (3) Use local infiltration anaesthesia.
PROTECT THE PATIENT’S EYES Put squares of vaselinegauze over both his eyes to prevent plaster getting into them.
REDUCTION Clean the patient’s face with cetrimide to re-move grease. Examine his nose carefully with your fingers.
Cover one blade of Walsham’s forceps, or some other suit-able instrument, with rubber tube. Pass it into his nose andlever the fragments of his bridge into place. Then do thesame on the other side.
If necessary, mould his comminuted lachrymal bones, andthe medial walls of his orbits, so as to reconstitute the bridgeof his nose.
CAUTION! (1) Don’t forget to protect his eyes. (2) Try hardto restore the full height of the bridge of his nose.
When you have done this, pass one blade of Asch’s septalforceps, or any other suitable instrument, down each sideof the patient’s septum and straighten it, so that it lies inthe midline. If necessary, grasp his septal cartilage, bring itforward, and replace it in its groove in his vomer.
Pass an instrument down each side of the nose to makesure he has a clear nasal airway. Pack both his nostril’s with1 cm selvedgeless gauze soaked in liquid paraffin.
SPLINTING If the fracture is mild, no splint is needed. Ifthe fracture is severe, splint it, either with a plaster cast, orwith lead splints.
elevate thefracture andrestore theshape ofthe nose
anaesthetisethe fracture
curved arteryforceps
B
A
ELEVATING AFRACTURED NOSE
Fig. 62.9: ELEVATING A FRACTURE OF THE NOSE. A, inflitratingthe site of the fracture. B, raising the depressed bones with curved arteryforceps. Always suspect a fracture after any blow on the nose. Swelling ofthe soft tissues can easily hide it. Kindly contributed by Peter Bewes.
A plaster cast Make eight thicknesses of plaster bandageinto a T–shape. Wet this and put it on the patient’s nose andforehead. If any plaster overlaps the lower end of his nose,turn it up like a brim. As it sets, mould it to his forehead andthe sides of his nose. Strengthen the plaster over the bridgeof his nose with two more layers of plaster bandage.
Remove the vaseline gauze squares from his eyes, and
MAKING APLASTER NASAL SPLINT
A
B
C
T−shaped plaster splint
packs to preventplaster enteringthe nose
dryplasterbandage
Walsham’sforceps
straighteningthe nose
Fig. 62.10: A PLASTER NASAL SPLINT. A, reducing the fracture withWalsham’s forceps. B, the splint in place. C, dry plaster bandage ready forpreparing the splint. Kindly contributed by Peter Bewes.
7

62 Maxillofacial injuries
then wrap a crepe bandage round his head to hold the cast.Or, hold it in place with adhesive strapping. It will hold hisnose in place by suction.
CAUTION! Don’t fix the splint to a plaster headcap, be-cause if this displaces, it will displace his broken nose.
When oedema has subsided in a few days, fit a fresh cast.Leave this for 2 weeks.
A lead splint If the fracture is too severely comminuted tobe held in a plaster splint, hold it with two lead plates, oneon each side of the patient’s nose. You can use two or threelayers of the lead backing from some infra–oral X–ray films.Pass a mattress suture of 0.35 mm soft stainless steel wirethrough his nose with a straight needle.
62.5 Fractures of the zygomatic complex
A blow to the side of a patient’s face drives his zygoma in-wards, usually on one side only. The zygomatic bones are soclosely united to the frontal and temporal bones, that, whenthey fracture, the neighbouring parts of these other bonesusually do so too. The zygomatic complex therefore usuallyfractures as a whole. The displaced zygomatic fragment canrotate clockwise, or anticlockwise, and its orbital rim can beinverted or everted. The floor of the orbit is always partlycomminuted.
If you see a patient early enough, you may see that theside of his face is flattened. Oedema fills out this flatteningwithin three hours, and it does not return for a week, afterthe oedema has subsided. If you are in doubt, there is a use-ful test for flattening of the zygoma. Put two pencils on ei-ther side of his face. They should lie parallel to one another.If the lower end of a pencil is tilted inwards, the patient’szygoma is flattened on that side, as in Fig. 62-12. The ob-viousness of this flattening depends greatly on whether hehas a thin bony, face which accentuates the displacement, ora fat one, which hides it.
When a patient’s zygoma is injured, his maxillary sinusfills with blood, so that his nose bleeds from that side. In-
use tworulers
deviationof theruleron thefracturedside
TESTING FOR A FRACTUREOF THE ZYGOMA
Fig. 62.11: EXAMINING FOR A FRACTURE OF THE ZYGOMA. Seealso Figure 62-6. Kindly contributed by Peter Bewes—it is a good likeness of him!.
jury to his infra–orbital nerve makes his cheek numb, anddisplacement of the lower part of his orbit pushes his eyedownwards, and restricts its movements. Herniation of thefat in his orbit into his maxillary sinus may also make hiseye sink inwards and downwards, and cause diplopia. Thiscan also be caused by injuries of his 6th nerve, or his ocularmuscles or their attachments. It can be temporary or per-manent. If it is due to a fracture of his zygomatic complex,reducing this may correct it.
Fractures of the zygomatic arch Sometimes, only thearch of a patient’s zygoma is fractured. There is a depres-sion over it, and the movement of the coronoid process ofhis mandible is restricted. Although the depression maybeobvious at the time of the injury, it may rapidly fill withoedema and become invisible. If his mouth was open whenhe was injured, he may be unable to close his jaw. Don’t tryto elevate the fragment, unless he has difficulty moving hisjaw.
Reducing fractures of the zygomatic complex Frag-ments of the zygomatic arch are held by the zygomatic fas-cia, and although they may displace inwards, they don’tmove in other directions. The patient’s temporalis fasciais attached to the superior border of his zygomatic arch,whereas his temporalis muscle is attached to his coronoidprocess. This enables you to pass an elevator between thefascia and the muscle, and lever his zygomatic arch out-wards into place. Try to operate within the first 48 hours,when the replaced fragment is more likely to be stable andless likely to need wiring. After two weeks, the ends of thefragments will have softened and rounded, and you willprobably need to wire them, after 4 weeks they will haveunited so that you cannot move them. After this length oftime they will probably need open refracture, open reduc-tion, and wiring.
The methods below do not include packing the maxillarysinus, and repairing the orbital floor. If the contents of apatient’s orbit have prolapsed into his maxillary sinus, andyou cannot refer him, he will have to live with his enoph-thalmos and wear an eye patch.
ELEVATING A FRACTURED ZYGOMA
INDICATIONS (1) Inability of the patient to open and closehis jaw. (2) Diplopia. If you are inexperienced, and he canmove his jaw normally and can see straight, disregard anydeformity and don’t operate.
The method described here is for the zygomatic arch. Bya slight change in the position of the lever, you can also useit for fractures of the body of his zygoma and the adjacentpart of his maxilla.
EQUIPMENT A general set with a Bristowe’s elevator, ora McDonald’s elevator, or a long secrewdriver.
ANAESTHESIA Give the patient a general anaestheticand intubate him (13.2).
REDUCTION Be sure to protect the patient’s eyes. Makea 2 cm antero–posterior incision in his temporalfossa, justabove his hairline, as in A, Fig. 62-13.
Reflect his skin. Underneath the skin and the superficialfascia you will see his auricularis superior muscle. Cut inthe line of Its fibres (B). If his hairline is low, and the inci-sion is lower, you may meet the fibres of auricularis anterior.
8

62.6 Dislocation of the jaw
ELEVATING ADEPRESSED ZYGOMA
A B
D
C
E
F
smallincision
superficialhisavoid
temporalartery
cut auricularis superiorin the line of its fibres
gauzeroll asfulcrum
cut the temporalfascia
elevator passingbetween thetemporalis muscleand the temporalisfascia
most surgeons make theincision more anteriorly
if the body of the zygoma isfractured, pass the elevatorforwards
X
Fig. 62.12: ELEVATING A DEPRESSED FRACTURE OF THEZYGOMATIC-MAXILLARY COMPLEX. A, the initial incision avoid-ing the superficial temporal vessels. B, dividing the auricularis superior.C, incising the temporalis fascia. D, passing an elevator. E, elevating thearch. F, elevating the body of the zygoma. Kindly contributed by John M LoreJr.
These run more horizontally, so separate them in a horizon-tal plane. Underneath them lies his tough deep temporalfascia. Cut this to expose his temporalis muscle (C). Thefascia may have two layers. If so, incise them both.
Pass a Bristow’s elevator between his temporalis fascia,and the surface of his temporalis muscle. Push it down untilits end lies between his zygomatic bone and his temporalismuscle (D). It should slip easily between the bone and themuscle.
Using a gauze roll as a fulcrum to protect the upper skinedge, gently lever his zygoma into a slightly overcorrectedposition (E).
If the body of a patient’s zygoma is fractured, pass theelevator forwards, and lever it into position (F).
If the fragment is stable, no wiring is necessary.If the fragment is unstable, wire its junctions with his
frontal or maxillary bones, or with both of them, through sep-arate small incisions.
WIRING A ZYGOMATIC–FRONTAL FRACTURE Expose
the fracture line by blunt dissection through an incision inone of the wrinkles at the corner of the patient’s eye. Takecare to avoid the branches of his facial nerve supplying hisorbicularis muscle. Drill small holes in the bone and fix thefragments in place with soft stainless steel wire.
WIRING A ZYGOMATIC–MAXILLARY FRACTURE Makea 1 cm incision just below the lower rim of the patient’s orbit.Drill small holes and wire the fragments together.
ALTERNATIVELY, in some fractures you may be able tograsp the fragments through his skin with tenaculum for-ceps.
CLOSING THE WOUND Close his deep temporal fasciawith a few monofilament sutures. Put a firm pressure padover the skin incision.
62.6 Dislocation of the jaw
When a patient dislocates his jaw, his mandibular condylesslip forward in their sockets over the articular eminences ofhis temporomandibular joints. This can happen when helaughs or yawns, or is hit in the face with his mouth open.The mouth of a patient with a dislocated jaw remains per-manently half open in an anterior open bite. Swallowingis difficult, so that saliva dribbles from the corners of hislips. When you examine him, you find a small depressionover his temporomandibular joints. If his mandible dislo-cates one side only, it deviates away from the midline.
THERESA was cultivating her fields in Zaire when she yawnedand dislocated her jaw. She had been told that patients had to payat the Catholic hospital, and as she had no money, she had to waitsome weeks to sell some produce before she could go there. Thedoctors there failed, because her dislocation was no longer recent,so she waited a few more weeks, sold some more produce, and triedthe Protestants. Her dislocation was now even older, and they toofailed, so she now walks about with her mouth permanently open.LESSONS Dislocations of the jaw are much easier to reduce if theyare done early. The tragedy of this patient is that both hospitalswould have treated her for free, if she had come early and told themshe could not pay.
REPLACING A DISLOCATED JAW
RECENT DISLOCATIONS Most patients need no anaes-thetic.
Sit the patient forward in a chair. Ask an assistant to standbehind him and hold his head. Put some gauze over hislower posterior teeth on each side. Press his premolar teethdownwards. At the same time press the underneath of hischin upwards and backwards.
If he opens his mouth too wide again, the dislocation mayrecur. So bandage his jaw to keep his mouth shut for 3 days.Allow him to open it just a little for eating.
OLD DISLOCATIONS Fix arch bars to each jaw (62.10).Cut an ordinary rubber eraser into two pieces, and put apiece between the patient’s posterior molars on each side toact as a fulcrum. Fix strong rubber bands between the archbars in front. During the following few days they will exertsteady traction and close his anterior open bite. If this fails,refer him.
9

62 Maxillofacial injuries
press his premolarteeth downwards,at the same timepress the underneathof his chinupwards and backwards
REDUCING ADISLOCATED JAW
Fig. 62.13: REPLACING A DISLOCATED JAW Most patients don’tneed an anaesthetic. If necessary, give a patient pethidine or diazepam.
62.7 The general method for an injured lowerjaw
A patient is hit on his jaw. One or more fractures tear themucoperiosteum covering the body of his mandible. Hedribbles bloody saliva, and can neither speak, swallow, norclose his teeth normally. Moving his injured jaw may be sopainful that he holds it in his hands. If you move it gentlyfor him, you may be able to feel crepitus.
Mandibular fractures can be unilateral or bilateral. Theweak parts of the bone and the common sites for fracturesare: (1) the neck of the condyles (B in Fig. 62-15), (2) theangles of the mandible (E, and F), and (3) the premolar re-gion (G). Fractures of the angle and body of the mandibleare open, but not those of the rami, condyles, or coronoidprocesses. Often, the patient has other injuries too, and thecombination of a jaw injury and a head injury is common.But, provided there is no gross comminution or tissue loss,you should be able to treat most of these fractures success-fully. The mandible remodels readily, even after a commin-uted fracture, and left untreated, many fractures will healthemselves, but only with considerable disability.
The purpose of the mandible is to bite, so decide whether ornot the patient has a normal bite. If he has not, think how best youcan restore it. The methods described below are for singlefractures. You will have to adapt them for multiple ones.
THE GENERAL METHOD FOR AN INJUREDLOWER JAW
This extends what has already been said in Section 62.1, onthe care of a severe maxillofacial injury. If possible, consulta dentist early.
EXAMINATION Feel both the patient’s condyles with thetips of your fingers, and then continue feeling downwardsalong the borders of his mandible. Feel for tenderness, stepdefects, alterations in contour, and crepitus.
Look inside his mouth with a good light. Gently swab awayany clotted blood. Lift any loose pieces of tooth and alveolus
out of his mouth.Examine his buccal and lingual sulci. Bruising in his buc-
cal sulcus does not necessarily indicate a fracture, but bruis-ing in his lingual sulcus almost certainly does. Palpate hismandible down the whole length of each sulcus carefully. Ifyou suspect a fracture, can you make the fragments moverelative to one another?
Examine the patient’s ears for bleeding. Put both yourlittle fingers into them and compare the movement of hiscondyles. If you cannot feel a condyle moving, suspect afracture.
BITE AND MOVEMENTS Examine the patient’s bite. If hecan cooperate, ask him to carry out a full range of mandibu-lar movements, and note any pain and limitation of move-ment.
Test for anaesthesia of his mental nerve. Is he anaestheticbelow his lower lip to one side of the midline?
X–RAYS Take antero–posterior, and right and left lateraloblique views to show his rami, condyles, and coronoid pro-cesses.
SOFT TISSUE INJURIES Do a careful wound toilet in-side and outside his mouth. Remove any foreign bodies andall loose teeth in the line of the fracture, together with theirroots. If there is loss of soft tissue, stitch his mucous mem-brane to the skin around the defect as best you can.
ANTIBIOTICS If a patient has an open fracture, give himan antibitoic, such as amoxycillin, ampicillin, or fortified pro-caine penicillin, daily for 5 days in the hope of preventingbone infection.
BANDAGES are usually unnecessary. If a patient needsone, apply a simple suspensory barrel bandage, not a four–tail bandage.
METHODS FOR PARTICULAR FRACTURES Apply theappropriate methods for fractured condyles (62.8), for frac-tures of the ramus (62.9), and for fractures of the body ofthe mandible (62.10). The coronoid processes (C, Fig. 62-15) can also be fractured, but the diagnosis is difficult. The
PATTERNS OF MANDIBULAR FRACTURE
A B
C
D
HE
FG
fracture ofthe ramus
condyle
coronoidfractured
process
displacementfracture withbilateral
fractured
allowing displacementunilateral fracture
with minimalmidline fracture
displacement
muscle pull
fracture of theangle in a directionthat does not causedisplacement
fracture of theangle allowingdisplacement
NORMAL
Fig. 62.14: PATTERNS OF MANDIBULAR FRACTURES. The princi-ple of reducing these fractures is to make the patient’s bite normal.
10

62.9 Fractures of the ascending ramus of the mandible
treatment is active movements, so disregard this fracture.
62.8 Fractured mandibular condyles
These are the most common mandibular fractures (B, Fig.62-15). They are often undiagnosed, and are often bilateral.
Unilateral condylar fractures The patient has pain,swelling, and tenderness over his temporomandibular jointon the injured side. He cannot move his jaw normally.Movement away from the injured side is particularly dif-ficult. When he tries to move his jaw, it deviates towards theside of the fracture. His bite may or may not be normal andhe occasionally bleeds from his ear.
Bilateral fractures All movements are painful and lim-ited. Sometimes the patient’s bite is normal, or he may havean anterior open bite. Often he has a midline fracture also.
The mandibular condyles are difficult to X–ray, and needspecial views, so it is fortunate that X–rays are not essential.Management depends on whether or not the patient has ananterior open bite. If you fail to correct this, his molar teethmay later have to be ground away, so that his incisors canmeet. If he has no teeth, an anterior open bite is less impor-tant, because it can be corrected with dentures.
FRACTURES OF THE MANDIBULAR CONDYLES
If possible, refer the patient, because ankylosis and devi-ation of his jaw may follow unsuccessful treatment. If youcannot refer him, proceed as follows.
FRACTURES WITH A NORMAL BITE
All unilateral fractures have a normal bite (if there is no otherassociated fracture) and so do some bilateral ones.
Encourage the patient to move his jaw. Deviation of hismandible towards the injured side is usually due to musclespasm, and soon improves, so that his bite becomes normal.Observe him to make sure that it does so.
CAUTION! If you decide to immobilize his jaw because ofpain, don’t do so for more than 10 days, or he may later haveso little movement that he will be unable to open his mouthnormally.
FRACTURES WITH AN ANTERIOR OPEN BITE
All these patients have bilateral fractures, or fracture dislo-cations.
If the fragments are not impacted, you may be able tosplint them using interdental wiring. If the patient has fewteeth, you may need to use an arch bar.
If the fragments are impacted, splint his jaws so as todistract the ramus in the condylar region. Take an ordinaryrubber. Cut two pieces from it 6 mm thick, and put thembetween his molar teeth on both sides. Then use adhesivetape traction or interdental wiring to make his incisors meet,as in treating an old dislocation (62.6). Maintain this splintingfor 5 weeks.
DIFFICULTIES WITH FRACTURES OF THEMANDIBULAR CONDYLES
If the patient Is a CHILD, no treatment is needed ini-tially. But follow him up carefully, because the growth of hismandible may be arrested.
If a patient’s BITE DOES NOT IMPROVE, refer him toa dentist. If serious malunion occurs condylectomy may benecessary.
FRACTURES OF THE CONDYLES ARE OFTEN MISSED
62.9 Fractures of the ascending ramus of themandible
The ramus of the patient’s injured mandible is tender,swollen, and bruised, both outside and inside his mouth (A,Fig. 62-15). The fracture does not open into his mouth andthere is little displacement unless violence has been extreme,because the muscles attached to the ramus splint it so well.If there is no displacement, encourage him to move his jaw.If there is significant displacement, fix his mandible by in-terdental wiring as described below.
62.10 Fractures of the angle or body of themandible
The angle of the mandible is one of its weak points, and isthe next most common site for fractures after the condyles.The fragments may or may not be displaced, depending onthe severity of the injury and the direction of the fractureline (E, or F, in Fig. 62-15). If the fragments are displaced,the anterior one is pulled downwards by the muscles at-tached to it, while the posterior one is pulled upwards bythe patient’s masseter (F). Sometimes there is a tooth on theposterior fragment.
If the fragments are not displaced, as in A, Fig. 62-15, youcan bandage the patient’s jaws together, and need not wirethem, although it is good practice to do so.
If the fragments are displaced, you will have to reduce andfix them. If they have enough teeth in them, you can usethe patient’s upper jaw as a splint and wire the teeth of bothhis jaws together (interdental eyelet wiring or intermaxillaryfixation, IMF), or you can use an arch bar. Fortunately, mostpatients are young and have enough teeth to let you do this.Interdental eyelet wiring (occasionally with an arch bar) isthus all that is necessary in most cases. If you don’t have anarch bar, you can use Risdon wiring, as in Fig. 62-19, whichis as good if not better. Or you can make an improvised archbar with paper clips or fencing wire. If you don’t have theright kind of stainless steel wire, you can use ordinary brasswire, but it is not so strong.
If a patient does not have suitable teeth for interdental wiring,you can drill holes in the fragments and wire them together(interosseous wiring). Or, you can combine interdental andinterosseous wiring. For example, if the anterior fragmenthas enough teeth to wire it to the maxilla, but the posteriorfragment has not, you may be able to wire it to the anteriorone. Interosseous wiring is never enough by itsef and is only anadjunct to interdental wiring.
11

62 Maxillofacial injuries
interdental wiringhas been completed.interosseous wiringis now necessary
FRACTURE OFTHE ANGLE OFTHE MANDIBLE
A
B
Fig. 62.15: A FRACTURE OF THE ANGLE OF THE MANDIBLE. A,shows the fracture after interdental wiring and before interosseous wiring.B, shows it before wiring. This is the patient whose mandible is beingwired in Fig. 62-19. John Maina’s patient.
Interosseous wiring is the most practical way of fixingthose fractures in which there is no other way of control-ling the posterior fragment. The inferior alveolar nerveruns through the centre of the mandible, so always wire themandible through its edges. You may need to wire it any-where along its length. Wiring is easiest on the front of apatient’s chin. There are two approaches: (1) You can wirethe lower border of his mandible from outside his mouth.(2) It is possible to wire the upper border from inside it, butthis is more difficult, so avoid it if you can. The patient islikely to be elderly and will probably tolerate his malocclu-sion.
If a patient wears a denture, you may be able to use thisas a splint, You can wire a lower denture to his mandible bycircumferential wiring, or you can suspend an upper den-ture from his zygomatic arches by an adaptation of methodB, in Fig. 62-8.
Fractures of the ramus are open, and are easily infectedby bacteria from the mouth. Osteomyelitis, sometimes withextensive fistulae, is thus an important complication, andmay follow interosseous wiring. Fortunately, prophylacticantibiotics will usually prevent it.
If for any reason you cannot fix these fractures, remod-elling will occur in those which involve the angle with up-ward and forward displacement of the posterior fragment,and in most comminuted fractures. It will not occur in frac-tures near the genial tubercles.
CAREFUL REGULAR ORAL HYGIENE IS ESSENTIAL TOPREVENT OSTEOMYELITIS
Anaesthesia is critical. If neither you nor your assistantis an anaesthetic expert, the patient is probably safest underlocal anaesthesia. The alternative is to give him a generalanaesthetic, pass a nasotracheal tube, and pack his throat.The dangerous moment comes when you remove the packbefore you finally close his jaws. While you are doing this,blood and saliva can collect in his pharynx. You cannot suckthis out through wired jaws. So, when you do finally pullthe tube out, he may inhale the collected blod and saliva,perhaps fatally, or he may have a severe inhalation pneumo-nia. Another moment of danger occurs as he recovers fromthe anaesthetic, when he may try to cough or vomit throughclosed jaws, so that you have to open them urgently. Localanaesthesia also reduces this risk. You can use ketamine, butit is not ideal.
MOST FRACTURES OF THE BODY OF THE MANDIBLENEED FIXING
FRACTURES OF THE BODY OF THE MANDIBLE
FRACTURES WITHOUT DISPLACEMENT
If the patient’s upper and lower teeth oppose one another, sothat he bites normally, there is no displacement. Provided heis cooperative, there is no need to wire his fracture, althoughit is better practice to do so.
If the patient is cooperative, bandage his mandible tohis maxilla, so that his teeth are firmly together. Use a crepebandage, adhesive strapping, or a plaster bandage roundhis chin, his face, and his forehead. If you use a crepe ban-dage, rewrap it every day to maintain tension.
CAUTION! A bandage can be detrimental if you apply it ina displaced fracture.
If a patient is uncooperative, he may remove his ban-dage, so you had better wire his fracture.
FRACTURES WITH DISPLACEMENT BUT NO TISSUELOSS
If the fracture lies within the tooth bearing area, you havetwo choices.
(1) If the patient is cooperative, unlikely to take the wiresoff, and has plenty of teeth, use interdental eyelet wiring.
(2) If he is uncooperative, if he has few teeth, or if there isgross displacement, use arch bars or Risdon wiring.
If the fracture lies outside the tooth bearing area, useinterosseous wiring combined with interdental wiring, or archbars or Risdon wiring on the same criteria as (1) and (2)above.
If he has no teeth, refer him. If you cannot refer him, doyour best with interosseous wiring.
If you have no suitable wire, do your best with a headbandage, as in Fig. 62-17.
If possible, operate during the first 24 hours, but if oedemais severe, you can wait up to a week to let it subside. If youare in any doubt about the patient’s general condition, wait.
12

62.10 Fractures of the angle or body of the mandible
FIXING THEMANDIBLE A
B
C
D
E
1
2
3
4
MAKINGRUBBER BANDS
A WIRE EYELET A BANDAGE FOR ANUNDISPLACED FRACTURE
FIXING AN EYELET
INTERDENTAL EYELET WIRING
rubberband
Fig. 62.16: FIXING THE MANDIBLE. A, this patient has an undisplacedfracture, so he only needs a bandage. B, keep rubber bands and eyeletsready in the theatre. C, the steps in making an eyelet. D, the eyelets madeinto hooks and held with a rubber band. E, passing wires between theeyelets. With the kind permission of Michael Wood and Hugh Dudley.
FRACTURES WITH SEVERE TISSUE LOSS
Usually, there is severe displacement also. Toilet the pa-tient’s wound, replace the bone and soft tissues as best youcan, and fix the remains of his mandible to his maxilla byany suitable method. Close his wound, suture his skin to hismucous membrane, and refer him.
INTERDENTAL EYELET WIRING FOR MANDIBULARFRACTURES
INDICATIONS Displaced fractures of the mandible with: (1)a sound maxillary arch, and (2) enough teeth opposite oneanother to take the wire.
CONTRAINDICATIONS If a patient is drunk and there isany danger of vomiting, don’t wire his teeth until his stomachis empty.
ANAESTHESIA FOR EYELET WIRING OR ARCH BARSSee above. There are several possibilities. (1) If displace-ment is mild and he is cooperative, use local anaesthesiaonly. Premedicate him with pethidine and diazepam (A 5.2).Use pterygopalatine (A 6.4) and mandibular (A 6.3) blocks,if necessary on both sides. Supplement these where re-quired, by infiltrating the mucosa round his teeth (A 6.3). Al-ternatively, use infiltration anaesthesia only. If you are usinglocal anaesthesia, sit him in a dental chair. (2) If his injuriesare severe and you are an anaesthetist expert, induce himwith ether or halothane (A 11.3), and intubate him throughhis nose (A 13.4). (3) Ketamine can be used.
CAUTION! Pass a nasogastric tube and aspirate his stom-ach before inducing him.
WORKING WITH WIRE Use soft 0.35 mm stainless steelwire, or any convenient soft wire. Stretch it before you useit, or it will become slack, but don’t over-stretch it, or it willbecome hard and brittle.
Making eyelets Cut the wire into 150 mm lengths, takehold of each end in a pair of artery forceps, and twist it rounda 3 mm bar to make the eyelets shown in B, Fig. 62-17.Keep 20 of them ready in a box in the theatre.
Twisting wire inside the mouth Twist it by holding itsends in a stout pair of artery forceps. Pull the ends taughtfrom time to time, and rotate them in your fingers, as in Fig.62-18. You will need to make many twists and this is muchthe quickest way of making them.
Precautions with wire Whenever you work with wire, pro-tect the patient’s eyes, because a loose end can spring backand injure them. (1) Close them, and cover them with vase-line gauze and a dressing. (2) When you are not workingwith the free end of a piece of wire, anchor it with a pair offorceps.
arch bar beingwired in place
hold the wire instrong artery forcepsand twist themround on yourmiddle finger
TWISTINGDENTAL WIRE
Fig. 62.17: TWISTING DENTAL WIRE. Use soft 0.35 mm stainless steelwire, or any convenient soft wire, and take care to protect a patient’s eyes.Kindly contributed by Frederick Onyango.
13

62 Maxillofacial injuries
INSERTING THE EYELETS Look carefully at the facetson the patient’s teeth and study the way his jaws fit together.If there is any abnormality in the way they occlude, allow forit when you immobilize the fragments.
Push an eyelet well down between two teeth (1) as shownin C, Fig. 62-17, bring the ends of the wire back betweentwo adjacent teeth (2), pass one end of the wire through theeye (3), twist both ends together, pulling tightly as you do so,and cut them off (4). Tuck the sharp ends between his teeth.Pull on the eye to bring it nearer to the occlusal surface andmake sure it is secure.
Fix about five eyelets in either jaw in suitable places, sothat when they are joined by tie wires, these will run diag-onally in both directions and brace his jaws together. Don’tplace the eyelets immediately above one another, or you willnot be able to anchor the fragments.
Alternatively, wire the teeth directly as in D, and E, Fig.62-19. This is a quick temporary measure if you have manycasualties, but the wires loosen more easily.
REDUCING A FRACTURED MANDIBLE If there are anyloose teeth in the fracture line, this is the time to removethem. Bleeding sockets will not now obscure the wiring.
CAUTION! (1) Control bleeding. (2) If you have intubatedthe patient and his throat is packed, remove the pack beforeyou wire his teeth. Leave his nasotracheal tube down. (3)Suck out his throat before you close his jaw.
Reduce the fracture by closing his jaws. When thepatient’s teeth fit together properly, the fragments will bealigned. Place the tie wires loosely at first, and only tightenthem after you have checked the occlusion. Tighten themlittle by little, first in the molar area on one side, then in themolar area on the other side, working round towards the in-cisors as you do so.
CAUTION! (1) If you tighten the wires firmly on one sideonly first, you will cause a crossover bite. (2) If you tightenthe incisor wires first, you will cause a posterior open bite.(3) Don’t twist the wire too tightly on a single rooted tooth, oryou may pull it out. You can exert more tension on a multi–rooted one. (4) Make sure that you have not trapped histongue.
Finally, run your finger round his mouth to make sure thatthere are no loose wires which might injure his lips. Coat hislips and the inner surfaces of his cheeks with vaseline.
ALTERNATIVE METHOD OF EYELET WIRING USINGHOOKS AND RUBBER BANDS
This is shown in D, Fig. 62-17. Use it when there is anydanger of vomiting, or if a patient has to travel. You will needthicker wire than with eyelet wiring.
Surround the neck of every second or third tooth with aloop of wire. Leave the two ends free towards the lips. Twistthem a few times and then make a small hook with the freeends. Make sure they really are smooth.
Pass short rubber bands diagonally over these wirehooks. If necessary, cut them from a suitable size of rub-ber tube as in B, in this figure.
RISDON WIRING FOR A FRACTURED MANDIBLE
INDICATIONS As an alternative to an arch bar for a fractureof the mandible that needs fixation. Some surgeons prefera Risdon wire to an arch bar.
MORE WIRINGMETHODS FORTHE TEETH
A
B C
D
E Interdental wiring
Risdon wiring
Fig. 62.18: MORE METHODS OF WIRING THE TEETH. A, B, andC, Risdon wiring—a useful alternative to an arch bar. D, and E, directinterdental wiring—an alterntive to eyelet wiring if you have many casu-alties; it is quicker, but not so secure as using eyelets. After Killey with kindpermission.
METHOD Take two pieces of soft 1 mm stainless steelwire about 25 cm long. In the middle of each piece twist aloop that will fit over one of the posterior teeth of the patient’sbroken lower jaw. Fit the loops over these teeth, and twistthem secure. Then twist the ends of each wire double. Bringthe twisted strands from each side together, reducing thefracture as you do so. Twist them together in the midline,so that they lie along the necks of the teeth. Cut the joinedpieces of wire short. Fix the twisted wires to some individualteeth with 0.35 mm wire loops. Finally, wire the mandible toeyelets placed on the maxillae.
FITTING ARCH BARS FOR MANDIBULAR FRACTURES
This is not as easy as it looks! Use a pair of heavy cuttingpliers to cut the bars to the right length for each jaw; try tomake them span as many teeth as possible; and leave themlong enough for the end to be bent towards the posteriorsurface of the last available tooth. Bend them to shape alongthe necks of the teeth with the hooks facing towards oneanother. The patient’s lower jaw will be displaced, so shapethe arch bar for it to fit round his upper jaw, or fit it round thelower jaw of another person with the same size of arch.
Use 15 cm lengths of 0.35 mm wire to wire the arch barto the teeth. It is usually best to start in the premolar regionby wiring one tooth on each side. Pass the wires round thenecks of the teeth and wire as many as you can. Becauseof their shape, incisor teeth are usually difficult to wire, soyou may have to leave them. If the wire tends to slip off, be
14

62.10 Fractures of the angle or body of the mandible
FITTING ANARCH BAR
A
B
C
D
E
Fig. 62.19: FITTING AN ARCH BAR. A, bending it to shape. B, fittingit round the maxilla. C, wiring it to the maxilla. D, passing a win round atooth. E, fixing the rubber bands. After R.O. Dingman and P. Navig ’Surgeryof Facial Fractures’ W.B. Saunders Co. Publishers, permission requested.
prepared to raise the gum with a periosteal elevator. Tuckthe ends of the wires aside where they will not injure thelips. Fix the arch bars with rubber bands.
AN IMPROVISED ARCH BAR Take some paper clips,open them, twist them together, make side hooks on them,point these upwards on the top teeth, and downwards onthe bottom ones. Fix this improvised arch bar to the teethwith ordinary stainless steel wire, and pass rubber bandsbetween the hooks.
LOWER BORDER INTEROSSEOUS WIRING FORMANDIBULAR FRACTURES
INDICATIONS (1) Control of the posterior fragment whenthis has no teeth. (2) Control of both fragments when the pa-tient has no teeth or insufficient teeth for interdental wiring.You will usually need interdental wiring or an arch bar also.
CONTRAINDICATIONS (1) Established infection of thefracture site. (2) Children in whom unerupted teeth may beinjured.
ANAESTHESIA Endotracheal anaesthesia is essential (A13.2).
METHOD Make a 3 cm incision over the fracture site inline with the patient’s facial nerve, as in A, Fig. 62-20. The
exact site of the incision will depend on where his fractureis. Reflect the skin. Under the incision you will find the su-perficial fascia and the platysma muscle.
Cut across the fibres of his platysma, and use blunt dis-section to find his facial artery and his anterior facial vein.These pass diagonally upwards and forwards across thelower border of his mandible at the anterior edge of his mas-seter. Retract these vessels gently backwards or forwardsaway from the line of the fracture. If necessary, cut and tiethem. Often, the fracture line will lie just posterior to theanterior edge of his masseter. If so, retract the vessels an-teriorly.
Use a rongueur to strip his masseter and the periosteumaway from the lower border of his mandible (B).
Define the fracture line. You will probably find that theposterior fragment lies deep to the anterior one and overlapsit. Disimpact the two fragments and remove any oId bloodclots and loose fragments of bone, which may prevent youaligning the two parts of his mandible.
Now pass your finger under the lower border of the pa-tient’s mandible (C), and separate It from the deep tissuesof the floor of his mouth. Replace your finger with a flatbroad retractor in this position (D).
Drill a hole in each fragment about 3 mm from the fractureedge—be certain the holes pass through both cortical platesof the bone. You will feel the drill touch your retractor whenthis has happened.
CAUTION! Don’t make the holes in the middle of the pa-tient’s mandible, or you may injure his inferior alveolar nerve.
Keep the retractor blade in place deep to his mandible.Take two 15 cm lengths of wire. Pass the first wire throughone of the holes in his mandible from the buccal to the lingualside. Secure it with artery forceps at both ends. Now take asecond wire and twist a small eye onto one end. Pass thiseye through the hole in the other fragment of his mandiblefrom the buccal to the lingual side. Thread the deep end ofthe first wire through the loop and twist it round itself (E).Use it to pull the second wire through the first hole. Removethe ’eye’ wire and twist the two ends of the first wire gentlytogether to reduce the fracture until there is only a hair–linecrack (F).
When you have secured the fracture (G), cut the twistedends of the wire off short and tuck the cut end into one of theholes, so that it doesn’t stick out into the soft tissues (H). Cuta very fine strip of rubber glove and insert this as a drain.
Close the wound in layers and bandage it with a light pres-sure bandage. Remove the drain after 24 hours.
UPPER BORDER INTEROSSEOUS WIRING FORMANDIBULAR FRACTURES
INDICATIONS This is seldom necessary. In bilateral frac-tures insert an upper border wire to prevent the musclespulling the anterior fragment downwards, and making thefracture line gape.
METHOD Wire the upper border before the lower one.Make an incision along the crest of the alveolus inside thepatient’s mouth. Drill small holes on either side of the frac-ture line, pass a piece of soft stainless steel wire through it,reduce the fragments, and twist the ends of the wire tight.Cut the ends short and tuck them into the nearest drill hole.Close the incision very carefully, because infection is com-mon.
15

62 Maxillofacial injuries
LOWERBORDERWIRING
A
B
C
D
E
F
G
Hwire endstucked in
hair line crack
2nd wire
1st wire
fracturebeingreduced
retractor underthe mandible
this patient’sfacial arterywas divided
mandible beingseparatedsubperiostallyfrom the tissueunderneath
rongeur
facialartery
nasotrachealtube
Fig. 62.20: LOWER BORDER WIRING. A, a nasotracheal tube has beenpassed and the patient’s head turned to one side. B, the periosteum is beingremoved from around the fracture line with a rongeur. C, the undersurfaceof his mandible is being freed from the tissues under it. D, the first drillhole. E, the two pieces of wire joined to one another under the mandible.F, and G, the fracture being reduced. H, the wound ready for closure. JohnMaina’s patient.
POSTOPERATIVE CARE FOR MANDIBULARFRACTURES
Don’t remove the patient’s tracheal tube until anaesthesia isreally light. If you have wired his teeth under general anaes-thesia, send him back to the ward with a nasopharyngealairway in place and his tongue held with a strong suture.Use a large cutting needle to insert it transversely throughthe dorsum of the back of his tongue. Lead Its end betweenhis teeth and hold them with haemostats. Some surgeonsconsider this is unnecessary. Lie the patient on his side andhave a sucker ready, with a tube attached which you canpass down his nasopharyngeal tube.
If he has been starved preoperatively, any vomit will bewatery and will pass between his wired teeth.
CAUTION! Have wire cutters beside his bed or with thenurse, in charge. Be sure that the nurses know how to re-move the wire, if he wants to vomit. Tell, them to cut theclosing wires, not the eyelets. Later, he will be more com-fortable if you nurse him sitting up.
POST REDUCTION X–RAYS If these are not satisfactory,correct the malposition as soon as possible.
ANTIBIOTICS Give these as described earlier (A 62.7).FEEDING A PATIENT WITH A CLOSED JAW Feed him
frequently with liquid food through a rubber tube betweenhis teeth. Let him suck between his teeth or round the backof his molars. Feeding will be easier if he has a few teethmissing. He will probably lose much weight. If he cannotswallow, feed him through a nasogastric tube.
Careful oral hygiene Is essential to prevent osteomyeli-tis. Ask him to clean his teeth with a tooth-brush after everymeal. Or, irrigate his mouth with saline or 0.5% chlorhexi-dine from a Higginson’s syringe.
FOLLOW–UP FOR A MANDIBULAR FRACTURE If yousend a patient home wired, tell him to keep a pair of pliersavailable, so that he can remove the wire if necessary. Askhim to reattend regularly, so that his wire can be tightenedor renewed. Keep children wired for 4 weeks before youtest for union, young adults for 5 weeks, and elderly onesfor 7 weeks. If you immobilize a patient’s jaw too long, it willankylose.
TESTING FOR UNION Remove the tie wires and gentlytest for union across the fracture line. If the fragments seemfirm, clean the patient’s mouth and remove the eyelet wires.Leave interosseous wire in place unless it becomes infected.
DIFFICULTIES WITH MANDIBULAR FRACTURES
If a patient CANNOT OPEN HIS JAW, don’t worry for thefirst week or two. It will open more easily after a few weeksof active use. If, however, he fails to reattend to have thewires removed, so that his jaw remains closed for too long,his jaw movements may be limited permanently. Encouragehim to exercise his jaw regularly and to progressively inserta wooden cone between his teeth, so as to separate them alittle more each day.
If his JAW HAS FAILED TO UNITE, encourage him to ac-cept his disability. Non–union is rare. It may follow infection,or be the result of leaving a tooth in the fracture line.
If his MANDIBLE HAS BECOME INFECTED, give himantibiotics (2.7), clean up his jaw as much as possible, re-move loose teeth in the fracture site and rewire his teeth.Osteomyelitis is an important complication and is more likelyto occur if you fall to fix a fracture, so that the fragments are
16

62.11 Fixing mandibular fractures with resins
kept moving, of if you try to wire one which is already in-fected. Prevent it by always giving prophylactic antibioticswhenever the mucoperiosteum is torn.
If his LOWER LIP IS NUMB, it will probably recover.Warn him of the danger of burning his lower lip with hotdrinks or cigarettes.
If his TEETH DO NOT MEET when the fixation is re-moved, his malocclusion will probably correct itself if it ismild. If it is more severe, his cusps can be ground away. Ifit is gross, refer him for refracture of his mandible, or the re-moval of selected teeth. If he adopts a bite of convenienceacross a partly healed fracture, it may cause a fibrous union,so refer him for a suitable denture.
If the patient is a CHILD manage his fracture as if hewere an adult, but remember the following differences: (1)Growth disturbances of his condyles may follow, particularlyin condylar fractures. (2) Don’t use interdental eyelet wiringunless he has a sufficient number of firm teeth, either decid-uous or permanent. (3) Don’t use interosseous wires, be-cause you may damage his unerupted teeth. (4) Mild mal-occlusion will correct itself as his mandible grows and hisdeciduous teeth erupt. A bandage, as in A, Fig. 62-17, maybe all he needs.
62.11 Fixing mandibular fractures with resins
You can use two types of synthetic resin to fix a patient’sbroken mandible, as an alternative to wiring it. The methodis quick, easy, and non–traumatic. Fixing hooks with com-posite is easier than wiring them directly to his teeth, lesstraumatic, and more comfortable for him because there areno wire ends to scratch his mouth.
Cold curing quick setting acrylic resin is weaker than thecomposite material described below, but is cheap andwidely available from dental supply houses or dental tech-nicians. It will allow you to fix an arch bar to a mandible,but it is not strong enough to let you stick hooks to it.
Composite filling materials of the ’Adaptic’ or ’Isopaste’ type,together with a bonding agent are more expensive and lessreadily available than quick curing acrylic resin. A compos-ite is supplied as two pastes which you mix together andwhich then set solid. It is usually used for filling cavities,but you can use it to make bridges between the teeth of a pa-tient’s upper and lower jaw, or you can use it to stick hooksto his teeth, and then pass rubber bands or wire over themas with interdental wiring (D, Fig. 62-17). To allow the com-posite to stick you will have to clean the surfaces of his teethat each fixation point, wash them, etch them with phospho-ric acid, wash them again, dry them, coat them with a spe-cial bonding agent, and then press the composite onto them.This is not difficult, but it needs care. Be sure you followthe instructions exactly. If you use bridges of composite be-tween a patient’s jaws, one difficulty will be getting theminto the right position and getting the composite into placesimultaneously. Using hooks avoids this difficulty.
At present, proprietary dental resins are unnecessarily ex-pensive, for example, proprietary compound filling materialcosts $75 for 100 g, whereas it only costs $6 to manufacture.Fortunately, cheaper ’generic’ dental materials are now be-ing made, and when they became available this method offixing mandibular fractures will become more economicallyfeasible.
ANOTHER METHOD OF FIXING THE MANDIBLE
Bridges of compound materialbetween the jaws
Hooks stuck on withcompound material
Fig. 62.21: ANOTHER WAY OF FIXING THE MANDIBLE. A, usingbridges of filling material. B, using hooks. Kindly contributed by W.J. Bailey.
FIXING THE MANDIBLE IN OTHER WAYS
ANAESTHESIA (1) Mandibular block (A 6-3). (2) Ketamine(A 8.1). (3) Diazepam (A 8.6). Atropinize the patient to dryhis saliva.
USING ACRYLIC TO FIX AN ARCH BAR
MATERIALS Ordinary cold cure acrylic (’Simplex’), as usedby dental technicians to repair broken dentures. This is sup-plied as a liquid monomer and a powdered polymer.
Put some of the powdered polymer into a small pot. Dropthe liquid monomer onto it and stir it with a spatula until it isthe consistency of putty.
METHOD Sit the patient up in a chair. Make an arch barfrom several strands of thick (2 mm) stainless steel wire, andfashion it to fit the arch of his mandible, lingually, or buccally,or both.
To stop the resin sticking, lightly spread vaseline on thepatient’s lips, mucous membrane and tongue-but not histeeth.
Hold the arch bar in place with blobs or a continuous wadof cold cure acrylic. Lightly spread vaseline on your fingers(to stop the acrylic sticking) and press the acrylic into placeover the arch bar. Press it firmly between the bases of thepatient’s teeth. If the arch bar is going to stay in place, theresin must go between the overhanging parts of his adjacentteeth. If he is older, and his gingival papillae have resorbed,or he has missing teeth, the resin will be able to pass be-tween them and stick more firmly.
Hold the arch bar in place until the resin has set (in about10 minutes).
USING COMPOUND FILLING MATERIAL TO STICKHOOKS ON
INDICATIONS (1) Conscious and cooperative patients. (2)This method is particularly suited to unilateral fractures. (3)Recent fractures that will be fairly easy to reduce.
CONTRAINDICATIONS Much bleeding which makescleaning and drying the surfaces of a patient’s teeth imprac-tical.
MATERIALS Compound filling material, such as ’Adaptic’or ’Isopaste’ and their special bonding compounds, or theirgeneric equivalents. 50% phosphoric acid, 2 mm stainlesssteel wire. Rubber bands.
METHOD The patient will probably need about six hooksdepending on the site of his fracture.
17

62 Maxillofacial injuries
Sit him up in a chair. Clean the surfaces of his teeth ateach fixation point carefully, and dry them free of saliva. Usespirit on a pledget of cotton wool, or a dental engine brush.
While his teeth are still dry, apply phosphoric acid on apaint brush for 60 seconds.
Wash his tooth for 30 seconds, and then dry it again.Keep his teeth dry with suction, rolls of paper tissue, or
cotton wool in his buccal sulcus.Apply the bonding material to the dry, etched surface with
a small brush or a wisp of cotton wool.Mix a little of the the compound material and the catalyst
with a spatula on a small paper pad, and immediately pressit into place with lightly vaselined fingers over the preparedsurfaces of his upper and lower teeth. While it is still soft,press a hook into it.
Join up the hooks with rubber bands or wire. Rubber willplace less strain on the hooks. If you join them with wire,take care not to exert too much force, or you may displacethem. After 6 weeks you can chip composite away quiteeasily. The last remaining pieces may have to be removedwith a dental drill.
ALTERNATIVE NOT USING HOOKS Hold the patient’sjaws together with bridges of filling material passing fromone jaw to another. You will probably only need about 4bridges. As they set, keep his jaws aligned and his teeth inocclusion.
18