Embed Size (px)
Citation preview

A malignant lymphoma of the breast may present as aprimary or secondary tumor. Both tumor types are rareand there are no morphological criteria to differentiatebetween them. The majority of primary breast lym-phomas are diffuse large B-cell lymphomas and a minorproportion reflect a Burkitt lymphoma, an extranodularmarginal zone B-cell lymphoma of mucosa-associatedlymphoid tissue (MALT) type, a follicular lymphoma, alymphoblastic lymphoma of either B or T type, and inextremely rare cases, T-cell lymphomas of variable sub-types as described by the current WHO classification. A
primary breast MALT lymphoma is very rare (1, 2). Wereport the mammographic, sonographic images andpathological findings of a low-grade lymphoma of mu-cosa-associated lymphoid tissue with multifocal trans-formation into a large cell lymphoma.
Case Report
A 37-year-old woman presented with a painless palpa-ble mass in the inner portion of the left breast. The pa-tient incidentally detected the mass three weeks prior tothe clinical visit. The patient was taking no medicationand had no history of trauma or a previous biopsy. Aphysical examination revealed a large firm, and fixedmass in the left breast. There was no skin change. Alllaboratory findings were normal. Mammogramsshowed a 4.5 cm sized isodense mass without internalcalcifications in the inner portion of the left breast and
J Korean Radiol Soc 2007;57:489-492
─ 489 ─
Primary Mucosa-Associated Lymphoid Tissue Lymphoma of the Breast: A Case Report1
Jong Heon Park, M.D., Dae Bong Kim, M.D., Mi Kyung Shin, M.D.2, Suk Ki Jang, M.D., Su Min Kang, M.D., In Oak Ahn, M.D.
1Department of Radiology, Bundang Jesaeng General Hospital 2Department of Pathology, Bundang Jesaeng General HospitalReceived May 10, 2007 ; Accepted September 10, 2007Address reprint requests to : Dae Bong Kim, M.D., Department ofRadiology, Bundang Jesaeng General Hospital, 255-2, Seohyun-dong,Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea.Tel. 82-31-779-0051 Fax. 82-31-779-0062E-mail: [email protected]
A primary mucosa-associated lymphoid tissue lymphoma (MALT lymphoma) of thebreast is extremely rare. We report a case of a MALT lymphoma of the breast that pre-sented as a palpable left breast mass in a 37-year-old woman. A physical examinationrevealed a large firm, and fixed mass in the left inner breast. Mammograms showed alarge, isodense mass in the lower inner quadrant of the left breast and an enlargedlymph node in the axilla. A sonogram demonstrated a 5 cm sized, oval, circumscribed,and heterogeneously hypoechoic mass with posterior acoustic enhancement. A surgi-cal biopsy was performed, and the pathology revealed a MALT lymphoma.
Index words : BreastUltrasonographyMammographyLymphoma, mucosa-associated lymphoid tissue Breast neoplasmsUltrasongraphy, mammography

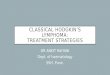
an enlarged lymph node in the left axilla (Fig. 1A, B). Asonogram showed a 5 cm sized, oval, circumscribed,and heterogeneously hypoechoic mass with posterioracoustic enhancement at the 9 o’clock direction of theleft breast and an enlarged lymph node in the left axilla(Fig. 1C, D). We classified the lesion as BI-RADS catego-ry 4b and recommended performing a core-neddle biop-sy (3). However, surgical excision was performed with-out a preoperative pathological diagnosis. Based on afrozen specimen, the diagnosis was an invasive lobularcarcinoma, and a left radical mastectomy was per-formed. An histopathological examination revealed dif-
fuse infiltration of the small and large lymphoid tumorcells in and around the breast ducts (Fig. 1E), and the re-sults of immunohistochemical staining were LCA (+),CD79a (+), CD20 (+) and CD3 (-), indicating a B-cellorigin of the tumor cells (Fig. 1F). The final diagnosiswas a low-grade lymphoma of mucosa-associated lym-phoid tissue, with multifocal transformation into a largeB-cell lymphoma. A bone marrow biopsy, abdomen CT,chest CT and bone scan showed no evidence of a distantmetastasis. Chemotherapy, including CHOP, was ad-ministered successfully for six cycles.
Jong Heon Park, et al : Primary Mucosa-Associated Lymphoid Tissue Lymphoma of the Breast
─ 490 ─
A B
Fig. 1. A 37-year-old woman with apalpable mass in the left breast.A, B. A Craniocaudal (A) and mediolat-eral oblique view (B) of a mammo-gram shows a large, isodense mass (ar-rows) in the lower inner quadrant ofthe left breast and an enlarged denselymph node (arrowhead) in the left ax-illa.C, D. An ultrasonogram shows an ovalshaped circumscribed margin, andheterogeneous hypoechoic mass in theleft breast (C) and an enlarged lymphnode in the left axilla (D).
C D

Discussion
A primary malignant lymphoma of the breast is a raredisease, representing 0.04% to 0.53% of all primary ma-lignancies of the breast and 2.2% of extranodal malig-nant lymphomas (4). Among the types of breast lym-phomas, MALT lymphomas constitute a variable sub-group with frequencies ranging from 0% to 44%, as re-ported in the clinical literature (5).
A MALT lymphoma or extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissuetype is an extranodal lymphoma comprised of morpho-logically heterogeneous small B-cells including marginalzone cells, monocytoid B cells, small lymphocytes andscattered immunoblasts. The lymphoepithelial lesionsare pathognomic for a MALT lymphoma (1, 2).
As seen on a mammogram, a MALT lymphoma re-veals diffuse involvement or masses with irregular, par-tially defined, or well-defined margins. As seen on asonogram, a wide spectrum of appearances rangingfrom well-defined to poorly defined, focal to diffuse,and hypoechoic to hyperechoic lesions have been de-scribed (6).
In this case, a mammogram revealed a lesion with anirregular margined isodense mass without internal calci-fication. A sonogram showed an oval, circumscribed,and heterogeneously hypoechoic mass with posterioracoustic enhancement.
A Palpable mass with an indistinct margin as seen on
a mammogram and hypoechogenicity as seen on a sono-gram is suggestive of a malignant lesion. An oval andcircumscribed margin of a mass seen on a sonogram issuggestive of a benign lesion. Thus, we classified thismass as BI-RADS category 4b and considered a ductalcarcinoma in situ, a lymphoma, an invasive ductal carci-noma, and a metastasis as possible malignant lesionsand a fibroadenoma as a possible benign lesion.
A malignant non-Hodgkin’s lymphoma of the breastincluding a MALT lymphoma may clinically mimic acarcinoma, and it is difficult to differentiate one lesionfrom the other by a physical examination and imagefindings (2). A core needle biopsy is a useful diagnostictool to distinguish between these types of masses.However, the pathological diagnosis of a MALT lym-phoma would not have been possible if the whole tumorwas not examined. Therefore, surgical resection of thetumor is also an optional local therapy (2, 7). The sys-temic treatment of malignant non-Hodgkin’s lymphomaof the breast including the MALT lymphoma ischemotherapy including the CHOP regimen (8). The 5-year survival rate of a non-Hodgkin’s lymphoma includ-ing a MALT lymphoma in the breast has been reportedas 37.6%. Younger patients tend to have a poorer prog-nosis, and the survival rate improves with increasingage.
Regarding the tumor size, it has been reported that thesurvival rate is poor when the maximum tumor diame-ter was larger than 5 cm (9).
In conclusion, since a MALT lymphoma in the breast
J Korean Radiol Soc 2007;57:489-492
─ 491 ─
E FFig. 1. E. A photomicrograph shows diffuse infiltration of small and large lymphoid tumor cells in and around the breast duct (H &E staining; ×200).F. Lymphoid tumor cells are positive in and around the duct for CD79a immunohistochemical staining (×200).

is extremely rare and is diverse in images, it is difficultto differentiate this type of lesion from other malignantmasses.
References
1. Tavassoli FA, Devilee P. World Health Organization: Tumours of thebreast and female genital organs. 2003;107-109
2. Taeda Y, Ariga N, Okamura K, Takei N, Komeno T, Ueki H, et al.Primary breast mucosa-associated lymphoid tissue (MALT) lym-phoma with high-grade transformation evidenced by prominentlymphoepithelial lesions. Breast cancer 2006;13:322-327
3. American College of Radiology. Breast imaging reporting and datasystem: BI-RADS Atlas, 4th ed. Reston, Va: American College ofRadiology, 2003
4. Cohen PL, Brooks JJ. Lymphomas of the breast. a clinicopatholog-
ic and immunohistochemical study of primary and secondary cas-es. Cancer 1991;67:1359-1369
5. Brogi E, Harris NL. Lymphomas of the breast: pathology and clini-cal behavior. Semin Oncol 1999;26:357-364
6. Sabate JM, Gomez A, Torrubia S, Camins A, Roson N, De LasHeras P, et al. Lymphoma of the breast: clinical and radiologic fea-tures with pathologic correlation in 28 patients. Breast J 2002;8:294-304
7. Levine PH, Zamuco R, Yee HT. Role of fine-needle aspiration cy-tology in breast lymphoma. Diagn Cytopathol 2004;30:332-340
8. Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, BouabdallahR, et al. CHOP chemotherapy plus rituximab compared withCHOP alone in elderly patients with diffuse large-B-cell lym-phoma. N Engl J Med 2002;346:235-242
9. Uesato M, Miyazawa Y, Gunji Y, Ochiai T. Primary non-Hodgkin’s lymphoma of the breast: report of a case with specialreference to 380cases in the Japanese literature. Breast Cancer2005;12:154-158
Jong Heon Park, et al : Primary Mucosa-Associated Lymphoid Tissue Lymphoma of the Breast
─ 492 ─
대한영상의학회지 2007;57:489-492
유방의 일차성 점막관련림프조직 림프종: 증례 보고1
1분당제생병원 영상의학과2분당제생병원 진단병리과
박종헌·김대봉·신미경2·장석기·강수민·안인옥
유방의 일차성 점막관련림프조직 림프종은 아주 드문 질환이며 국내에는 영상소견이 보고된 적이 없어 저자들은
좌측 유방의 만져지는 종괴를 주소로 내원한 37세 여자 환자에서 1예를 경험하였기에 유방촬영술 및 초음파 소견
을 보고하고자 한다. 이학적 검사에서 단단한 종괴가 좌측 유방의 내측에서 만져졌으며 고정되어 있었다. 유방촬영
술에서는 좌측 유방 내측에 실질조직과 비슷한 음영의 종괴로 보였으며 내부에 석회화는 보이지 않았다. 초음파 검
사에서 모양은 난원형이고 경계가 좋으나 내부는 불균일한 저에코의 병변을 보이면서 후방 음영 증강을 동반하는
5 cm 크기의 종괴였다.