Embed Size (px)
Citation preview

659
Malignant melanoma involving the ovary is uncommon. Most of the reported ovarian malignant melanomas are metastatic, and only 44 cases are primary.1-18 Teratoid elements must be identified in the ovary for the diagnosis of primary malignant melanoma because ovaries normally do not contain melanin-producing cells.4 However, it is challenging to assess the prima-ry site of ovarian malignant melanoma because it is almost al-ways found in an advanced state, replacing entire ovarian struc-tures, and this makes it difficult to determine whether the le-sion is a primary ovarian melanoma.
Mature cystic teratoma is the most common benign germ cell tumor of the ovary, and it constitutes 15-25% of ovarian tumors overall. A wide variety of malignant tumors may arise within a mature cystic teratoma, including squamous cell carci-noma (75%), adenocarcinoma (7%), undifferentiated carcino-ma, basal cell carcinoma, and various sarcomas (7%). Malignant melanoma arising from mature cystic teratoma has also been re-
ported, but it is very rare.Here, we report on an uncommon case of primary malignant
melanoma arising from a mature ovarian cystic teratoma with multiple metastatic lesions.
CASE REPORT
Clinical and radiological findings
A 71-year-old woman presented with general weakness, wei-ght loss of three kilograms over a three-month period, and a one-month history of lower back pain. Past medical and family histories were unremarkable. Physical examination revealed a palpable mass in the lower abdomen. Laboratory findings on admission showed anemia (hemoglobin 8.4 g/dL), markedly el-evated lactate dehydrogenase (LDH, 1,935 IU/L; normal range,
Primary Malignant Melanoma Arising in an Ovarian Mature Cystic Teratoma
- A Case Report and Literature Review -
Sangho Lee · Ji Hoon Kim1
Gyu Rak Chon2 · Aeree Kim3
Baek-Hui Kim3
Department of Pathology, Konkuk University Chungju Hospital, Konkuk University School of Medicine, Chungju; 1Department of Internal Medicine, Korea University Guro Hospital, Korea University College of Medicine, Seoul; 2Department of Internal Medicine, Konkuk University Chungju Hospital, Konkuk University School of Medicine, Chungju; 3Department of Pathology, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea
Ovarian primary malignant melanoma is very uncommon with only 44 reported cases in the litera-ture. A 71-year-old woman with an ovarian mass and multiple nodules in the liver presented to our hospital. She was treated with bilateral salpingo-oophorectomy, and malignant melanoma was found in the mature cystic teratoma of the ovary. Malignant melanoma cells were also found in the ascitic fluid. She died 5 months later. Here we report a very uncommon case of malignant melanoma arising in an ovarian mature cystic teratoma with a review of the literature.
Key Words: Melanoma; Teratoma; Ovary
Received: October 15, 2011Accepted: November 22, 2011
Corresponding AuthorBaek-Hui Kim, M.D.Department of Pathology, Korea University Guro Hospital, Guro 2-dong, Guro-gu, Seoul 152-703, KoreaTel: +82-2-2626-1485Fax: +82-2-2626-1486E-mail: [email protected]
The Korean Journal of Pathology 2011; 45: 659-664http://dx.doi.org/10.4132/KoreanJPathol.2011.45.6.659

� Sangho�Lee·Ji�Hoon�Kim·Gyu�Rak�Chon,�et�al.660
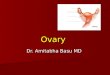
0 to 480 IU/L), and mildly increased cancer antigen 125 (47.3 U/mL) and carcinoembryonic antigen (8.3 ng/mL). Abdominal computed tomography revealed numerous hypodense nodules in the liver (Fig. 1A), a small nodule in the left adrenal gland,
and a 15 cm sized septate cystic mass with multiple internal fatty components in the pelvic cavity. Magnetic resonance im-aging findings of the pelvic mass were suggestive of ovarian mature cystic teratoma (Fig. 1B) but the nodules in the liver
A B
C
Fig. 1. (A) Abdominal computed tomography shows multiple metastatic nodules in the liver. (B) Pelvic magnitic resonance im-aging shows a 12 cm-sized multicystic mass with fat compo-nents. (C) Microscopic picture of liver needle biopsy. Melanoma cells with brown pigments are infiltrating the hepatic parenchyma.
A
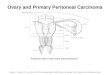
Fig. 2. (A) Internal surface of the ovarian cyst. A dark black elevated mass (arrow), measuring 6.5×6 cm, is seen. Adjacent cystic wall is of the mature cystic teratoma. (B) The cut surface of the mass. Dark pigmented area (yellow arrow) is seen with fatty area of the teratoma com-ponent (red arrow).
B

661Primary�Malignant�Melanoma�in�an�Ovarian�Mature�Cystic�Teratoma
and adrenal glands were more likely metastatic. The possibility of ovarian malignancy arising in a mature teratoma was consid-ered. A liver biopsy was performed, and in order to determine the primary tumor site and tumor stage, the patient underwent bilateral salpingo-oophorectomy, total hysterectomy, omentec-tomy, left adrenalectomy, and appendectomy.
Pathologic findings
Liver biopsy
The histologic features of the liver biopsy revealed a prolifera-tion of spindle-shaped cells showing pleomorphism, prominent nucleoli, and black-brown pigments (Fig. 1C). On immunohis-tochemical staining, the tumor cells expressed S-100, Melan A, human melanoma black-45 (HMB-45) and vimentin, but the cells were negative for leukocyte common antigen, cytokeratin, and hepatocyte antigen. The morphological and immunophe-notypic features were consistent with metastatic malignant mel-anoma, but no mass or pigmented lesion was found on her skin. Therefore, the differential diagnosis included clear cell sarcoma of the soft tissue and primary ovarian malignant melanoma aris-ing from a mature cystic teratoma.
Ovary
The right ovary showed an unruptured cystic mass, measur-ing 15×12×11 cm and weighing 920 g. The cyst contained dark brownish fluid with whitish-gray keratin and sebum-like materials. The internal surface of the cyst showed an elevated, black-colored solid mass, measuring 6.5×6 cm (Fig. 2A). On section, the black-colored mass was connected to the cystic le-sion (Fig. 2B). The ometum showed several conglomerated no-dules along with a dark black nodule in adrenal gland, measur-ing 2×1 cm. The uterus, left ovary, left salpinx, and appendix were unremarkable.
Microscopically the cystic portion of right ovarian mass re-vealed typical features of mature cystic teratoma, and the black solid portion was composed of large epithelioid cells with abun-dant eosinophilic cytoplasm, prominent nucleoli, frequent mi-toses, and dark brownish pigments. The tumor had abundant vascular structures with central coagulative necrosis. The ma-jority of the epidermal lining cells around the solid mass were denuded, so the relationship with epidermal lining or junction-al activity could not be evaluated (Fig. 3A, B). On immunohis-tochemical staining, the tumor cells were positive for S-100, Melan A, HMB-45, B cell lymphoma-2 (bcl-2), c-kit, and phos-phatase and tensin homolog (PTEN), but negative for cytokera-
tin, estrogen receptor, and progesterone receptor (Fig. 3C). The tumor cells were also positive for Fontana-Masson staining (Fig. 3D). These findings were consistent with malignant melanoma.
Metastatic lesions were found in the omentum, left adrenal gland, serosal surface of the appendix, peritoneum of the cul-de-sac, and uterosacral ligament. However, the uterus, left ovary, and salpinx were uninvolved.
Peritoneal washing fluid
The peritoneal washing fluid collected during the operation contained many atypical cells. These discohesive cells were round to oval in shape and had irregular nuclei, prominent nucleoli, vacuolated cytoplasm, and cytoplasmic melanin pigments in a background of reactive mesothelial cells (Fig. 3E, F).
Clinical course
After the operation, the patient was stable and was able to undergo two rounds of chemotherapy (cisplatin-dacarbazine-vincristine). However, the patient’s general condition deterio-rated, and there was no evidence of the therapeutic effect. She suffered from ascites and respiratory discomfort, and then died five months after initial presentation.
DISCUSSION
Malignant melanoma involving the ovary is uncommon. Most cases are metastatic lesions, and primary ovarian tumors are very rare. According to one study, only one case of primary ovarian melanoma was identified among 23 cases of malignant melano-ma involving the ovaries, and the melanoma originated from a mature cystic teratoma.19
Boughton et al.1 and Cronje and Woodruff3 proposed the fol-lowing criteria for the diagnosis of primary ovarian melanoma: 1) no other possible sites of a primary tumor; 2) unilateral tu-mor within the ovarian teratoma; 3) good correlation of the pa-tient’s age and symptoms with those of well-documented cases in the literature; and 4) demonstration of junctional activity (de-sirable but not necessary for diagnosis).
In our case, other possible primary sites of melanoma, such as the skin, intestine, and eyeball were examined but no pigment-ed lesions were found. The malignant melanoma arose in a uni-lateral ovarian teratoma. As in previously reported cases, the pa-tient was relatively old (71 years) and had general weakness, wei-ght loss, and a palpable abdominal mass.1,6,14,16,18 These findings

� Sangho�Lee·Ji�Hoon�Kim·Gyu�Rak�Chon,�et�al.662
C
A
D
B
E F
Fig. 3. (A) Malignant melanoma cells are located amongst the keratin material in the teratoma components. (B) Malignant melanoma cells have large nuclei, prominent nucleoli, and dark brown pigments. (C) Positive immunohistochemical staining of the tumor cells with human melanoma black-45. (D) Positive Fontana-Masson staining of the tumor cells. (E, F) Liquid-based cytology of the ascitic fluid. The tumor cells have enlarged eccentric nuclei, prominent nucleoli, and dark intracytoplasmic pigmentation (arrow) (Papanicolau stain).
all supported a diagnosis of primary ovarian malignant melano-ma. To date, only 44 cases of primary malignant melanoma aris-ing in a mature ovarian cystic teratoma have been reported. From these, we reviewed 17 cases, and the clinicopathologic features
are shown in Table 1.Junctional activity was not observed in our case, but the pres-
ence of junctional activity is not necessary for diagnosis and does not exist in every case (only in 5 of 11 cases with the available

663Primary�Malignant�Melanoma�in�an�Ovarian�Mature�Cystic�Teratoma
data). Junctional activity in primary ovarian malignant melano-mas may be destroyed by tumor invasion, or the malignant mel-anoma may originate from a component of the cystic teratoma rather than from a dermoepidermal junction.13
Melanotic metastases mainly involve the surrounding struc-tures or spread via the vascular or lymphatic systems. The most common sites of spread are the lymph nodes, liver, lung, and bones.17 In this case, there was no evidence of ovarian rupture; therefore, vascular or lymphatic metastases could be the cause of the liver, omental, adrenal, and peritoneal involvement.
In many studies, an increased serum LDH level is correlated with decreased survival in patients with advanced malignant melanoma.7,14,20 Our patient also had a high serum LDH level (1,935 IU/L), and she survived only 5 months after operation.
The immunohistochemical staining of tumor cells in previ-ously reported cases revealed positivity for S-100, Melan A, and HMB-45.2,4-7,9-11,13,14,16-18 There was also a case that was positive for c-kit and PTEN.11 Some cases were positive for Fontana-Ma-sson staining. Our case was positive for S-100, Melan A, HMB-45, bcl-2, c-kit, and PTEN, and Fontana-Masson, and negative for cytokeratin, estrogen receptor, and progesterone receptor, which were sufficient for a diagnosis of malignant melanoma. Common cytomorphologic features of malignant melanoma, such as discohesion, multinucleation, prominent nucleoli, and cytoplasmic vacuolization, were also observed in our case.
Surgical resection is the gold standard of treatment, but ma-
lignant melanoma arising in the ovary has a poor prognosis. In 17 reviewed cases, 10 cases had metastatic lesions2-4,6,7,12,14,15,17 and 9 cases had died within the 18 months.3-7,9,13,14,17 Chemo-therapy was performed in some studies.2,4,6,7,12,15,17 A study re-ported chemotherapy with intraperitoneal carboplatinum re-sulted in five-year disease-free survival;2 however, the evidence for a chemotherapeutic benefit remains inadequate. In our case, the patient underwent chemotherapy using cisplatin, dacarba-zine, and vinblastin, but the effect was not satisfactory, and the patient survived only five months.
In this case, the patient initially presented with multiple me-tastatic nodules in the liver and adrenal glands along with asci-tes. The metastatic nodules and the peritoneal washing cytology were morphologically consistent with malignant melanoma but no skin lesions were observed as a possible primary site. When metastatic malignant melanoma is found in biopsy specimens of internal organs or ascitic fluid cytology, the ovary should be considered a possible primary organ. In conclusion, we report a very uncommon case of primary ovarian malignant melanoma arising in a mature cystic teratoma.
REFERENCES
1.BoughtonRS,HughmanickS,Marin-PadillaM.Malignantmelano-maarisinginanovariancysticteratomainpregnancy.JAmAcad
Table 1. Clinicopathologic features of previously reported primary ovarian malignant melanomas arising in mature cystic teratomas
AuthorAge (yr)
Symptom OperationAddition-al therapy
DEJ activity
Serum LDH (IU/L)
Serum CA-125 (U/mL)
Distant metastasis
Follow-up time
Patient outcome
Cronje and Woodruff3 74 Abdominal distension Salpingo-oophorectomy No Yes ND ND Yes 18 mo DODBoughton et al.1 27 Pelvic mass Cystectomy No Yes ND ND No 2 yr NEDCarlson and Wheeler2 20 Abdominal pain TAH-BSO, rectosigmoid resection CTx ND ND ND Yes 5 yr NEDO’Leary and Tejura9 79 Abdominal pain TAH-LSO No No ND ND No 2 mo DODUeda et al.13 86 Autopsy Autopsy No No ND ND No No DODWatanabe et al.16 55 Ovarian mass TAH-BSO No No ND Normal No 6 mo NEDMcNeilage et al.7 19 Back pain TAH-BSO CTx, RTx No 2,346 93 Yes 37 days DODVigliani et al.14 67 Abdominal pain Myomectomy and BSO No Yes 1,290 ND Yes 3 mo DODVimla et al.15 42 Abdominal pain Ovarian cystectomy CTx ND ND ND Yes 18 mo NEDO’Gorman and Olaitan8 49 Abdominal distension BSO No Yes Normal Elevated No ND NEDZarbo et al.17 60 Abdominal distension TAH-BSO CTx No ND 203 Yes 4 mo DODTakubo et al.10 65 Abdominal distension TAH-BSO No Yes Normal Normal No 24 mo NEDGök et al.5 67 Abdominal distension TAH-BSO No ND ND ND No 7 mo DODTsukamoto et al.12 46 Abdominal distension TAH-BSO CTx No ND ND Yes 12 mo NEDGao et al.4 53 Abdominal distension BSO CTx ND ND 351.7 Yes 6 mo DODLee et al.6 46 Pelvic mass TAH-BSO CTx ND ND 260 Yes 2 mo DODChoi et al.18 45 Pelvic mass TAH-LSO CTx ND ND ND Yes 37 mo NEDPresent case 71 Abdominal mass TAH-BSO CTx No 1,935 47.3 Yes 5 mo DOD
DEJ, dermoepidermal junction; LDH, lactate dehydrogenase; CA-125, cancer antigen 125; ND, no data; DOD, dead of disease; NED, no evidence of disease; TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; CTx, chemotherapy; LSO, left salpingo-oophorectomy; RTx, radiotherapy.

� Sangho�Lee·Ji�Hoon�Kim·Gyu�Rak�Chon,�et�al.664
Dermatol1987;17(5Pt2):871-5.2.CarlsonJAJr,WheelerJE.PrimaryovarianmelanomaarisinginadermoidstageIIIc:long-termdisease-freesurvivalwithaggressivesurgeryandplatinumtherapy.GynecolOncol1993;48:397-401.
3.CronjeHS,WoodruffJD.Primaryovarianmalignantmelanomaarisingincysticteratoma.GynecolOncol1981;12:379-83.
4.GaoR,LiuNF,ShengXG.Malignantovarianmelanomawithex-tensivepelvicandperitonealmetastasis:acasereportandliteraturereview.ChinJCancer2010;29:460-2.
5.GökND,YildizK,CorakçiA.Primarymalignantmelanomaoftheovary:casereportandreviewoftheliterature.TurkPatolojiDerg2011;27:169-72.
6.LeeSH,LeeKB,ShinJW,ChungDH,ParkCY.Ovarianmalignantmelanomawithoutevidenceofteratoma.JObstetGynaecolRes2010;36:898-901.
7.McNeilageLJ,MorganJ,ConstableJ,JoblingTW.Metastaticmalig-nantmelanomaarisinginamatureovariancysticteratoma:acasereportandliteraturereview.IntJGynecolCancer2005;15:1148-52.
8.O’GormanT,OlaitanA.Primarymalignantmelanomaarisinginanovariancysticteratoma.EurJGynaecolOncol2009;30:88-9.
9.O’LearyAJ,TejuraH.Malignantmelanomaarisinginacystictera-tomaoftheovary.JObstetGynaecol2005;25:626-7.
10.TakuboK,KimuraT,SuzukiK,et al.Malignantmelanomaarisinginovariancysticteratoma.GynecolOncol1991;43:77-80.
11.TateG,TajiriT,SuzukiT,MitsuyaT.MutationsoftheKITgeneandlossofheterozygosityofthePTENregioninaprimarymalignantmelanomaarisingfromamaturecysticteratomaoftheovary.Can-
cerGenetCytogenet2009;190:15-20.12.TsukamotoN,MatsukumaK,MatsumuraM,KamuraT,Matsuya-maT,KinjoM.Primarymalignantmelanomaarisinginacysticter-atomaoftheovary.GynecolOncol1986;23:395-400.
13.UedaY,KimuraA,KawaharaE,KitagawaH,NakanishiI.Malig-nantmelanomaarisinginadermoidcystoftheovary.Cancer1991;67:3141-5.
14.ViglianiR,IandoloM,LacivitaA.Matureovariancysticteratomawithcombinedsquamouscellcarcinomaandmalignantmelano-ma.VirchowsArch1998;433:381-4.
15.VimlaN,KumarL,ThulkarS,BalS,DawarR.Primarymalignantmelanomainovariancysticteratoma.GynecolOncol2001;82:380-3.
16.WatanabeY,UedaH,NakajimaH,MinouraR,HoshiaiH,NodaK.Amelanoticmalignantmelanomaarisinginanovariancystictera-toma:acasereport.ActaCytol2001;45:756-60.
17.ZarboR,ScibiliaG,ConoscentiG,ScolloP.Ovariancysticteratomawithprimaryepithelialcellmelanoma.EurJGynaecolOncol2005;26:71-4.
18.ChoiYS,JungCW,KimJ,et al.Acaseoftheprimaryovarianmalig-nantmelanomaarisingfromacysticteratoma.KoreanJMed2004;66:644-8.
19.GuptaD,DeaversMT,SilvaEG,MalpicaA.Malignantmelanomainvolvingtheovary:aclinicopathologicandimmunohistochemicalstudyof23cases.AmJSurgPathol2004;28:771-80.
20.AgarwalaSS,KeilholzU,GillesE,et al.LDHcorrelationwithsurvi-valinadvancedmelanomafromtwolarge,randomisedtrials(Obli-mersenGM301andEORTC18951).EurJCancer2009;45:1807-14.