Embed Size (px)
Citation preview

1
Primary Care Physical Therapist?
The Role of PT’s in Population Health
Owen Lennon PT, DPT, OCSRegional Clinical Excellence Director - NJ
Financial Disclosure
• No conflicts to report.
Courtesy R. Panariello

2
About Me
• B.S. Medical Biology – University of New England
• Doctor of Physical Therapy– University of New England
• Orthopedic Clinical Specialist (OCS)
• 11 years of practice in orthopedics
• Regional Clinical Excellence Director – New Jersey (Professional PT)

3
• Respond at Pollev.com/owenlennon308
• Text: OWENLENNON308 to 22333 once to join. Then answer questions as they appear.
Program Description
• As national obesity rates rise, associated disease processes are becoming more pervasive and financially burdensome to the country and healthcare system. This course will discuss relevant research regarding PT’s role in reducing healthcare costs via a primary care/annual musculoskeletal exam model. The program will highlight global population health trends and more specifically the epidemiological data in the metro NJ/NYC region. The potential challenges and barriers to implementation will also be addressed.

4
• Course Outline: • 8:30 - 8:50: Introduction • 8:50- 9:40: Current state of chronic
disease (epidemiology and healthcare spending)
• 9:40 - 10:30: Regional considerations in the NJ/NYC market
• < 40 minute break > 1030 - 1110• 11:10 – 11:45: The annual exam: The role
of PT in the changing tides of public health
• 11:45-12:15: Can we make a difference? • 1215 – 1:00: Challenges/Barriers to
implementation of the PT annual exam.• 1:00 – 1:10 Q&A Session: Concluding
remarks.
Objectives
• Briefly describe the history/safety of direct access.• Identify US specific population health concerns.• Identify population health concerns relevant to the
NY/NJ metro area. • Describe the role of Physical Therapist’s in a
primary care model. • Design the basic components of an annual exam• Develop recommendations based on common exam
findings as relevant to public health.

5
Introduction
• July 21, 2017 (Gov. Christie)
By expanding the scope of practice of physical therapists to include: identification of balance
disorders; wound debridement and care; utilization review; screening, examination, evaluation, and application of interventions for the promotion,
improvement, and maintenance of fitness, health, wellness, and prevention services in populations of all ages exclusively related to
physical therapy practice.
Direct Access

6
Multiple studies suggest that the availability of the choice to pursue direct access to physical therapy for back and neck pain is safe and provides similar outcomes with cost savings comparing to traditional medical referral.
Is Direct Access Safe?
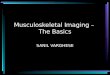
Chronic Diseases: The Leading Causes of Death and Disability in the United States
CDC. Quick Stats: Number of Deaths from 10 Leading Causes. March 2013

7
Staggering Statistics
• As of 2012, about half of all adults—117 million people—had one or more chronic health conditions. One in four adults had two or more chronic health conditions. Ward et al. Prev. Chronic Dis.
• Seven of the top 10 causes of death in 2014 were chronic diseases. Two of these chronic diseases—heart disease and cancer—together accounted for nearly 46% of all deaths. CDC. Health, US, 2015.
• Obesity is a serious health concern. During 2011–2014, more than one-third of adults (36%), or about 84 million people, were obese (defined as body mass index [BMI] ≥30 kg/m2). About one in six youths (17%) aged 2 to 19 years was obese (BMI ≥95th percentile)
NCHS Data Brief 2015
• Arthritis is the most common cause of disability. Brault et al, MMWR 2009.
• Of the 54 million adults with doctor-diagnosed arthritis, more than 23 million say they have trouble with their usual activities because of arthritis. Barbour et al MMWR 2017.

8
Health Risk Behaviors
• Four modifiable health risk behaviors cause much of the illness, suffering, and early death related to chronic diseases and conditions:
1) lack of exercise/activity 2) poor nutrition 3) tobacco use4) excess alcohol consumption
• In 2015, 50% of adults aged 18 years or older did not meet recommendations for aerobic physical activity. In addition, 79% did not meet recommendations for both aerobic and muscle-strengthening physical activity US DHHS 2017.
• More than 1 in 3 adults (about 92.1 million) have at least one type of cardiovascular disease. Benjamin et al. Circulation 2017.

9
• In 2015, more than 37% of adolescents and 40% of adults said they ate fruit less than once a day, while 39% of adolescents and 22% of adults said they ate vegetables less than once a day. CDC. 2017
Costs
• 86% of the nation’s $2.7 trillion annual health care expenditures are for people with chronic and mental health conditions. These costs can be reduced! Gerteis et al Mult. Chronic Conditions. 2014.

10
• Annual direct medical expenses for cardiovascular disease totaled approx. $190 billion in 2012–2013.
Benjamin et al Circulation 2017.
• Cancer care cost $157 billion in 2010 dollars. National Cancer Institute 2010.
• In 2012, $176 billion in direct medical costs associated with diagnosed diabetes.
ADA 2012.
• The direct medical cost of arthritis and related conditions was about $81 billion in 2003. CDC 2013.
• Medical costs linked to obesity were estimated to be $147 billion in 2008. Annual medical costs for people who were obese were $1,429 higher than those for people of normal weight in 2006.
Finkelstein et al. Health Aff. 2009

11
Role of Environment in Supporting Health & Wellness
• Ecological Model: ‘describes the interaction between individuals and their physical and sociocultural environments.’
– Sallis et al. Health Behavior & Health Education. 2008 (text).
Ecological Model of Public Health

12
Regional Considerations in the NJ/NYC market
NJ Personal Per Capita Income: $50,781 (2010)
NJ Median Household Income: $71,637 (2012)
NJ Median family income: $87,389 (2012)
Census.gov
The “Average” NJ Home
• It's about 70 years old, detached, with three bedrooms. It'll run you between $300,000 and $500,000. And the driveway must have space for at least two cars.
• Sound familiar? These are the characteristics of the quintessential New Jersey home.

13

14

15
• NJ average tax bill: $8,690 (2017)
• NJ average commute time 30.4 minutes
NY/NJ Bureau of Labor Statistics 11/15/17

16
Cost of Housing & Public Health
Superior Court: Mercer County Ruling March 2018
Mandating low/middle income affordable housing
– 753 new affordable units Princeton– 1500 new affordable units West
Windsor.
• Recommendation of need for >154,000 affordable housing units in NJ
You Cannot Outrun a Bad Diet

17
What about Childhood Obesity
• 1 in 5 school age children and young people (6 to 19 years) in the United States has obesity.
Hales et al. NCHS Data Brief 2015-2016
• Percentage of children and adolescents affected by obesity has more than tripled since the 1970s!
Fryar et al. Health E-Stats 2014

18

19
NFL Play 60
Insurmountable Odds? or a Great Opportunity!

20
PT’s are in a perfect position to effect change!
• Why not an annual musculoskeletal exam?
Opportunities to act Locally and Globally!
• PT’s are in an ideal position to promote health and wellness to their existing patients/clients!

21
Screen your Patients
• Take Vitals and Screen your Patients
Treat the Whole Patient!

22
Don’t “Discharge” Your Patient
• Instead ‘end the episode of care’
Become Their ‘Lifetime PT’
• During Episode of Care:– Vary frequency more than standard
(2-3x/week x 6 weeks). – Call after exam/eval to ‘check in’
• After Episode of Care:– Check In (email, card, call)– Offer cash based services– Offer yearly ‘wellness check up’– Send Holiday/Birthday Cards

23
Questions/Comments
Grab some coffee &check out the exhibitors (10:30-11:10)
The Annual Musculoskeletal Exam

24
Defining the terms Health and Wellness
• Health: “a state of complete physical, mental, and social well-being and not merely the absence of disease.” WHO 1946.
• Wellness: “the sense that one is living in a manner that permits the experience of consistent, balanced growth in the physical, spiritual, emotional, intellectual, social, and psychological dimensions of human existence.” Adams et al Am J Health Promotion 1997

25
Health-disease/wellness-illness continuum
It doesn’t have to be complicated/difficult!
• Information on wellness can be gathered through history and casual conversation.
• Or can be collected by using specific wellness questionnaires.

26
Perceived Wellness Survey
• Adams et al. Am. J Health Studies. 1998
• See Paper Handout (provided during lecture)
Who Better than PT’s?
• A greater % of physical therapists maintain a healthy weight and consume more than 5 servings of fruits and vegetables per day compared with the general population.
Black et al. Phys Ther. 2012.
• Engagement in health behaviors can improve health/wellness & enables the PT to more effectively promote the adoption of these behaviors in their patients and clients.

27
Health & Wellness Knowledge and Skills
5 important physical behaviors:
1) physical activity
2) nutrition/weight management
3) smoking cessation
4) sleep
5) stress management
Physical Activity Promoting Approaches
1) Educate patients/clients about the health benefits of
physical activity
2) Make patients and clients aware of the current
recommended minimum guidelines for physical activity
3) Explore perceived barriers to physical activity.
4) Promote self-efficacy for exercise.
5) Encourage goal setting and monitoring of outcomes.

28
Physical Activity Promoting Approaches
6) Include strategies for helping patients and clients to prevent relapse
7) Build social support.
“Stand Up, Sit Less, Move More, Move Often” Dunston et al. Diabetes Res Clin Pract. 2012.

29
Not so fast
Lancet: Lower Back Pain (3 Part Series)

30

31
Nutrition & Weight Management
• Specific nutrition counseling for medical conditions such as diabetes and obesity is outside of the scope of PT; however, PT’s can screen for and identify health problems that may be related to nutritional deficits.

32
Smoking Cessation
• Single greatest cause of morbidity and mortality in the US is tobacco use or smoking.
DHHS 2008.
• Guidelines suggest that clinicians consistently and intentionally identify tobacco use and encourage quitting.

33
• Prevalence of smoking in patients and clients with disabilities has been shown to be twice as high as in those without a disability.
Dean et al Physiother Theory Pract. 2009
What if you feel undertrained?
Ask (about tobacco use)
Advise (to quit)
Assess (willingness to quit)
Assist (through referral)
Arrange (follow-up)
“5 A’s”
US Dept. of Health and Human Services

34
For Those Unready / Unwilling to Quit
Relevance
Risks (patient identifies risk)
Rewards (patient identifies rewards)
Roadblocks
Repetition
“5 R’s”

35
Sleep Hygiene
• An estimated 50-70 million Americans experience a chronic sleep disorder.
Dean et al. Physiother Theory Pract. 2011.
• Developing evidence also supports the importance of adequate sleep in improving functional motor learning and chronic pain.
Al Sharman et al. Phys Ther 2013.
Cognitive-Behavioral Interventions Have Proven Effective
• Follow instructions such as:– Do not go to bed until you are sleepy.
– Use the bedroom or room where you sleep only for
sleeping (do not read, watch TV, eat, etc)
– Get our of bed if you are unable to sleep after 15
minutes and do something relaxing while avoiding
stimulating activities
– Get out of bed at the same time every day.
– Do not take naps late in the day (after 3pm) Institute of Medicine of the National Academies. April 2006.

36
Other things to consider/educate regarding…
• Participate in regular daytime physical activity
• Ensure bed/bedroom are comfortable, dark, and quiet
• Reduce evening caffeine, nicotine, and alcohol intake
• Reduce fluid intake in the evening
• Eat regular meals

37
Stress Management
• Stress: ‘nonspecific response of the body to any demand and can occur in response to positive or negative circumstances.’
• Stress management: Refers to techniques aimed at address distress (situations viewed negatively)
Positive vs. Negative Stress
• Positive stress (eustress): stress that is typically motivating, short-term, and within our coping abilities.
• Negative stress (distress): aka chronic stress is stress that has a negative impact of health and wellness.

38
Framework to Address Stress
• Identify the stressor
• Relieve stress by incorporating a relaxation or
coping strategy
• Seek solutions to avoid, control, or manage the
stress
• Improve overall fitness and health
• Think differently to respond differently to the
stressor. Thompson et al. Prevention Practice. 2007 (text)

39
Seem a little daunting???
• Counseling: “patient consultation aimed at health behavior change.”
Friedrich et al. Physiother Theory Pract 2012.
• Effective counseling requires:
– Knowledge of strategies to encourage behavior change, including theories of behavior change and motivational interviewing.
Motivational Interviewing
• Expand here

40
• Simple question: ‘Are you engaging in health promoting activities?’
Challenges/Barriers to Implementation

41
Barriers/Challenges
• Time• Lack of Interest/Awareness• Lack of reimbursement• Lack of Resources
• Limited Counseling Skills• Lack of Self-Efficacy• Focus on secondary or tertiary
prevention by PT’s• Perception that PT work
environment is not suitable for health promotion.
Barriers
• Lack of involvement of PT’s in research, policy, and action related to health promotion and wellness.
• Payments systems based on illness rather than wellness
• Lack of recognition of PT’s as primary care practitioners
• Lack of emphasis of health promotion in entry level education programs.

42
Barriers
• Resistance to advocacy efforts that support the payment for primary care services by physical therapists.
If you can’t adapt, changes become threats instead of opportunities.
Opportunities
• Shift how you view yourself relative to health promotion and wellness.
• Think biopsychosocial / ecological approach.
• Be aware of current public health trends and priorities
• Accept, embrace, and act on your role in primary prevention of to first assess then discuss healthy behaviors.

43
Opportunities
• Engage in continuing education to build competency in health behavior change.
• Partner with other health care practitioners to ensure that health promoting interventions are coordinated and reinforced across clinical encounters.

44
Questions/Comments
Thank You for Your Attention
Owen Lennon PT, DPT, OCS
[email protected](207) 749 - 6842
www.professionalpt.com

45
References

46

47