Embed Size (px)
Citation preview

PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON PUBLIC/ MEETING
Tuesday 25th August 2020 10:00-12:00 NOON
MEETING HELD VIRTUALLY
This meeting will be held in public and will be recorded purely as an aide memoir for the minute taker to ensure an accurate transcript of the meeting, decisions and actions. The recording will destroyed once the minutes have been formally approved. All care is taken to maintain your privacy; however, as a visitor in the public gallery, your presence may be recorded. Should you contribute to the meeting during questions from the public, this will be interpreted as your agreement to you being recorded for the purposes as set out above.
A G E N D A
Time No Agenda Item CCG decision Attachment Presented By Decision/
Assurance/ Information
1.0 Apologies Chair
10:00 2.0
Declarations of Interest To request members to disclose any interest they have, direct or indirect, in any items to be considered during the course of the meeting and to note that those members declaring an interest would not be allowed to take part in the consideration for discussion or vote on any questions relating to that item.
10:00 3.0 Minutes of meetings held on Tuesday 23 June 2020 Enclosed Chair Decision
10:05 4.0 Matters Arising/Action Log - Terms of Reference Enclosed
Enclosed Chair Decision
10:10 5.0 Primary Care Commissioning Committee Effectiveness Survey
Enclosed Chair Decision
Contractual
10:20 6.0 Chairs Action – Red Site Review Report Enclosed Chair
10:30 7.0 Risk register Verbal Mrs S Saville
10:35 8.0 Practice merger Hill Street Surgery
Wolverhampton CCG Enclosed Mrs G Shelley Decision
10:40 9.0 Extended Access Wolverhampton CCG Enclosed Mrs G Shelley Decision
10:45 10.0 BCWB Primary Care Frameworks All CCGs Enclosed Mrs S Southall Decision
Assurance
10:50 11.0 Digital Deferred Mr M Hastings Assurance
10:55 12.0 Finance Enclosed Finance Leads Assurance

11:00 13.0 Restoration and Recovery Update CCGs Verbal Mrs S Southall Assurance
11:05 14.0 Quality & Safety Report CCGs Enclosed Mrs S Quinton Assurance
11:10 15.0 Training Hub Report Enclosed Mrs S Southall Assurance
11:15 16.0 Primary Care Operational Group Report CCGs Enclosed Mrs J
Robinson Assurance
11:20 17.0 BCWB Flu Plan & Primary Care Assurance CCGs Enclosed Mrs S Quinton Assurance
11:25 18.0 Estates Report CCGs Enclosed Mr A Lawley Assurance
Discussion
11:30 19.0 Falsified Medicines Directive Enclosed Mr G Westgate Decision
Exclusion of the Press and Public That under the Public Bodies (Admission to Meetings) Act 1960, the public and representatives of the press and broadcast media be excluded from the meeting during the consideration of the following items of business as publicity would be prejudicial to the public interest because of the confidential nature of the business to be transacted.
Date and Time of Next Meeting • Tuesday 27 October 2020 – 10:00-12:00 noon • Tuesday 15 December 2020 – 10:00-12:00 noon • Tuesday 23 February 2021 – 10:00-12:00 noon
Please note venue details are to be confirmed

04.08.20
Black Country and West Birmingham Primary Care Commissioning Committee’s Held in common
Members register of interests Agenda Item: 2.0
Name Position CCG Interest Declared & Nature Alan Johnson Secondary Care
Consultant Dudley CCG Daughter works at Royal Wolverhampton Trust
Andrew Lawley Head of Premises and Capital Development
SWB CCG None
Andy Cave Healthwatch Birmingham
SWB CCG None
Anna Nicholls Interim Deputy Head of Commissioning (Primary Care) NHS England (West Midlands)
External Employed by NHS England
Bal Dhami NHS England SWB CCG None Carla Evans Head of Primary Care SWB CCG Regis Medical Centre Patient of Regis Medical Centre
Linkway Medical Practice Aunt is Deputy Practice Manager Carlos Marques Pestana
CCG Employee SWB CCG Halcyon Medical Centre Patient
Carly Sheldon Primary Care Finance Lead
SWB CCG South Warwickshire CCG Husband is CFO at south Warwickshire CCG
Carters Green Medical Centre Patient Carol Marston Primary Care
Commissioning Manager
Walsall CCG None
Christopher Handy Lay member, Vice Chair
Dudley CCG Chief Executive, Accord Group
Visiting Professor at Birmingham City University

04.08.20
Board Member of: - Black Country LEP Board - Redditch Co-operative Homes - Black Country Consortium - Walsall Housing Regeneration Agency - Direct Health - Eurohnet - Trident Housing andCare
Daniel King Head of Primary Care Dudley CCG None David Hughes Deputy Chief Officer -
Finance SWB CCG Partner is Employee at SWB CCG - Head of Contracts
David Pitches Public Health Representative - Primary Care Commissioning Committee
Dudley CCG Church organist fees received for giving recitals or playing for services
Primary Care Commissioning Committee Member at Dudley CCG Consultant in Public Health Medicine, Dudley MBC Wife is a Consultant Obstetrician at Heart of England Foundation Trust Wife is a Consultant Obstetrician at Birmingham Women's Hospital Occasional
David Stenson Patient Opportunity Panel Representative
Dudley CCG Non-Executive Director - Black Country Partnership NHS Foundation Trust Volunteer, Healthwatch Dudley Volunteer, Healthwatch Dudley
Dr Ayaz Ahmed Governing Body GP SWB CCG Village Medical Centre Sole GP Partner Malling Health Urgent Care Centre (Russells Hall Hospital) Two GP Session Per Week Faculty of Forensic and Legal Medicine Member Sandwell Health Partnership Federation GP Shareholder Jubilee Health Centre GP Partner with Dr Bhadauria Jubilee Health Centre GP Partner with Dr Bhamik

04.08.20
Dr David MacKenzie Bush
Governing Body – Locality Lead
Wolverhampton CCG GP Owner/Contractor, Penn Surgery
Medical Referee, City of Wolverhampton Council (employee) Owner and Managing Director, DMB Consultancy LTD, provider of occupational medicine services to various commercial clients, including City of Wolverhampton Council
Dr Harinder Baggri CCG Clinical Executive Member, Modality GP Partner Berkley Practice
Walsall CCG GP Partner, Kingfisher Berkley
GP Partner, Walsall Modality has entered into long term partnership with Push Doctor Spouse is a salaried GP at Kingfisher Berkley Walsall Modality GP Partner
Dr Karlis Armands Grindulis
Secondary Care Consultant
SWB CCG BMI Priory Hospital Birmingham Private Practice in Rheumatology at BMI Priory Hospital Birmingham Orchard School Oldbury Spouse is Chair of Governors Babylon GP at Hand Son-in-law is a GP who undertakes sessional work for babylong gp at hand The Feeding Clinic CIC Wife is director
Dr Mohammad Asghar
Governing Body GP Wolverhampton CCG GP and Director Health and Beyond Ltd.
Dr Priyanand Hallan Governing Body GP Member
SWB CCG Parkhouse Surgery Partner at Parkhouse Surgery, proving GMS services
Scott Arms Medical Centre involved in a new primary care development Scott Arms Medical Centre that is under development. Practice Development LTD director of Practice Development LTD which provides non-GMS medical services and Aesthetic medicine Providers 4 Health PCN Member Great Barr PCN Member

04.08.20
Dr Salma Reehana Chair of the Governing Body
Wolverhampton CCG Member of BMA Fellow of RCGP Member of MDU Member of FSRH
Mr Manjt Jhooty, Director of Health & Beyond is Governing Body Lay Member for Audit and Governance at Walsall CCG Practice is part of Primary Care Home 2 and partners have lead roles in the organisation Some of my partners within Health & Beyond are also part of WDL which manages Showell Park and AMPS Practice. I have no links directly with Showell Park. Board Member - Accord Housing Group Director - Matrix Global Holdings LLtd.
Dr Tim Horsburgh Clinical Executive for Primary Care & LMC Representative
Dudley CCG Clinical Executive for Primary Care
Clinical Lead for SWITCH Clinical Lead GP MCP Designated Medical Officer Dudley CCG Secretary for Dudley LMC Salaried GP - Waterfront surgery
Dr Uzma Ahmad Walsall LMC Representative
External Member of BMA
Member of RCGP Named GP is the principle GP who provides GMS and Enhanced Services Named GP is a shareholder of Walsall Alliance Federation LMC Member Medical Advisor for NHSE, PLDP

04.08.20
Helen Mosley Lay Member Dudley CCG Voluntary Director, Wyre Community Land Trust James Green Chief Financial Officer Black Country and
West Birmingham CCG's
Oxford Biomedica PLC Small shareholding in Oxford Biomedica PLC
Registered patient at The Northway Medical Centre (Dudley CCG) James Smith Head of Financial
Management - Corporate and financial planning
Dudley CCG Wife is employed by DMBC in the Place Accountancy Department
James Young Head of Quality Assurance
Dudley CCG None
Jane McGrandles Head of Primary Care Contracts
SWB CCG None
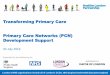
Janette Rawlinson Lay Member SWB CCG Just Real Solutions Principal Consultant SCVO (sandwell council for Voluntary Organisations) and BVSC (Birmingham Voluntary Service Council) Clients of Just Real Solutions - Consultancy Work CRUK (Cancer Research UK) Stratified Medicine Programme Board Lay Governance Member NCRAS Clinical Reference Group (National Cancer Registration and Anaylsis Service) Member of RICCR working group- (Review of Informed consent cancer registry) Macmillan User Reference Group Member – Horizons Survivorship Study British Thoracic Oncology Group Advocate at conferences, clinical trials, annual meetings and Steering Group Member(Apr 2017) Society of Cardiothoracic Surgery Patient Advocate NHS England Member of Clinical Expert Group (lung cancer) and LC Screening Advisory Group European Respiratory Society Speaker at annual congress on lung screening, member of screening group University of Birmingham PPI Member for medical school, speaker at UG Genomics session
04.08.20
EORTC - European Organisation for Research and Treatment of Cancer Speaker at 3rd international survivorship summit and Patient Days Workshop Takeda Speaker at industry workshop ECCO - European Cancer Organisation Speaker at resolution passing summit, Vienna European Lung Foundation Member of Patient Advisory Group (lung cancer) and cross patient advisory group Roy Castle Lung Cancer Foundation Advocate / Fundraiser, member of patient literature review panel Grant Thornton Atend Non-Exec directors trainer sessions WM Cancer Alliance Lung Cancer and Mesothelioma Expert Advisory Group and PPI group NCRI Lung Group - Advanced disease Subgroup Member of Lung Group University of Birmingham - Member of ICRB group
EORTC - European Organisation for Research and Treatment of Cancer - member of Patient panel UCL CTC - member of EARL clinical trial TMG (March 2019) and PPI group (Nov 2019)
Jaspreet Mander CCG Employee SWB CCG Modality's Handsworth Wood Medical Practice Patient Jayne Emery Chief Officer of Dudley
Healthwatch External Employee of Dudley CVS which holds contracts funded by Dudley CCG
Jayne Salter-Scott Head of Communications and Engagement
SWB CCG Agewell CiC (Non paid capacity) Director
NHS Bank Staff as a Covid Support Worker Daughter Joanne Taylor Primary Care
Commissioning Manager
Dudley CCG None
John Taylor Chair - Healthwatch Walsall, Observer, Governing Body
External Director John Taylor Consultancy
04.08.20
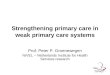
Trustee, Heart of England Community Funds Presiding Justice Magistrates Courts Member of the Lord Chancellors Advisory Committee Volunteer, Oxfam Chair, Healthwatch Walsall Chair, Healthwatch Sandwell Consultant, CQC and Healthwatch England
Julie Jasper Lay member - Audit SWB CCG Member of CIPFA Westlands Associates Ltd. Managing Director Rowley View Nursery School I am Chair of Governers (this is an unpaid position)
Julie Robinson Primary Care Contracts Manager
Dudley CCG None
Leon Mallett CCG Employee SWB CCG None Lisa Maxfield PCCC- Member,
Deputy at GB for Sharon Liggins
SWB CCG None
Lorraine Gilbert Head of Finance Walsall CCG Membership of CIPFA Close relative is an employee of a service contracted by Walsall MBC, included in Better Care Fund
Manoj Behal CCG Employee SWB CCG Takeda Pharmaceutical Company Sister is regional account director Martin Stevens Head of Contracts and
Performance SWB CCG Sandwell Parents for Disabled Children Trustee of Charity (SPDC)
Matthew Hartland Deputy Accountable Officer
Black Country and West Birmingham CCG's
Director of Dudley Infracare Lift LTD
Director of Infracare (Walsall and Wolverhampton) Limited Director of Whitbrook Management Company Member of Chartered Institute of Public Finance and Accountancy
Michelle Carolan Sandwell Managing Director
Wound Care Alliance UK Vice Chair and Trustee (ended July 2020)

04.08.20
Black Country and West Birmingham CCG's
Daughter employed at SWB CCG in Quality team
Mike Abel Lay Member Commissioning
Walsall CCG Chair, Director Chuckery Festival
Chair. Chuckery NHW Partner works for Black Country Healthcare NHS Foundation Trust
Morley Robert Executive Secretary of Birmingham LMC
SWB CCG General practitioner Defence Fund LTD Director
Philip Cowley Senior Finance Manager
Dudley CCG Wife works for Midlands and Lancs CSU
Philip Lydon CCG Employee SWB CCG VCS ORG - SMETHICK CAH Wife works for charity Rachel Barber Public & Patient
Participation Involvement
Walsall CCG A2Dominion Industry Advisor
Brighter Futures NED Justice of the Peace NED Housing Plus Group Onward Housing NED Sister in law is a Health Care Assistant at Wolverhampton Eye Infirmary North Wales Police Joint Audit Committee Chair
Ranjit Sondhi Lay member, Vice Chair
SWB CCG Hope Projects Birmingham Trustee National Citizens UK Trustee Nishkam Health Project Board Member Sampad Chairman Birmingham and Solihull CCG Wife is Non-Executive Director Guide dogs for the Blind Board Member
Raymond Sullivan Sandwell LMC Chair SWB CCG Gelebefields Surgery Principal GP Lex Medicus Ltd. Director/Owner Sandwell Local Medical Committee Chair
04.08.20
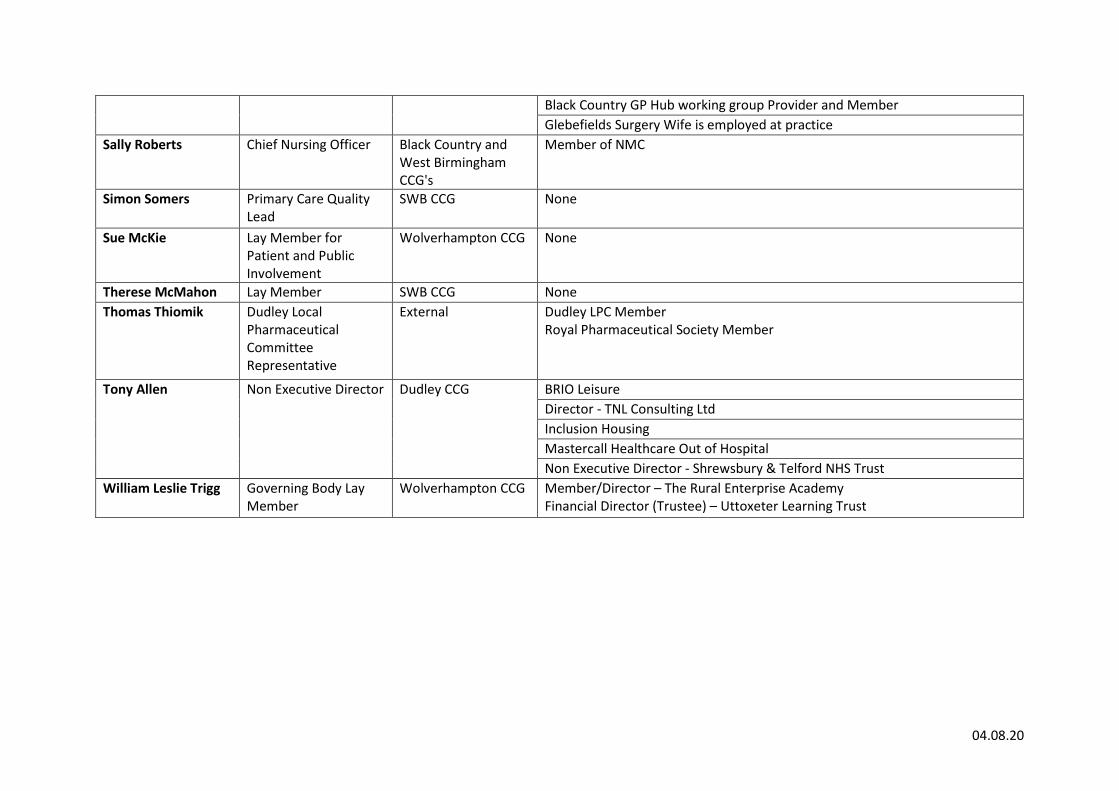
Black Country GP Hub working group Provider and Member Glebefields Surgery Wife is employed at practice
Sally Roberts Chief Nursing Officer Black Country and West Birmingham CCG's
Member of NMC
Simon Somers Primary Care Quality Lead
SWB CCG None
Sue McKie Lay Member for Patient and Public Involvement
Wolverhampton CCG None
Therese McMahon Lay Member SWB CCG None Thomas Thiomik Dudley Local
Pharmaceutical Committee Representative
External Dudley LPC Member Royal Pharmaceutical Society Member
Tony Allen Non Executive Director Dudley CCG BRIO Leisure Director - TNL Consulting Ltd Inclusion Housing Mastercall Healthcare Out of Hospital Non Executive Director - Shrewsbury & Telford NHS Trust
William Leslie Trigg Governing Body Lay Member
Wolverhampton CCG Member/Director – The Rural Enterprise Academy Financial Director (Trustee) – Uttoxeter Learning Trust

1 | P a g e
PRIMARY CARE COMMISSIONING COMMITTEE MEETING IN COMMON
MINUTES OF THE MEETING HELD IN PUBLIC ON
TUESDAY 23RD JUNE 2020 ATTENDEES: Mr M Abel Lay Member for Commissioning, Walsall CCG (Chair) Mrs H Mosley Lay Member for Patient and Public Engagement, Dudley CCG Dr A Johnson Secondary Care Clinician, Dudley CCG Prof C Handy Lay Member for Quality & Safety, Dudley CCG Dr T Horsburgh Clinical Executive, Dudley CCG Mrs A Nicholls Head of Service - General Medical Advice and Support Team (GMAST) NHS
England and NHS Improvement – Midlands – Dudley CCG Mrs J Taylor Primary Care Commissioning Manager – Dudley CCG Mrs J Robinson Primary Care Contracts Manager - Dudley CCG Mr P Cowley Senior Finance Manager – Primary Care – Dudley CCG Dr D Pitches Consultant in Public Health – Dudley CCG Mrs A Farrer Healthwatch Walsall, Walsall CCG Miss R Barber Lay Member for Patient and Public Involvement, Walsall CCG Mrs S Saville Head of Corporate Governance, Walsall CCG Mrs L Gilbert Deputy Chief Finance Officer, Walsall CCG Mrs C Marston Primary Care Contracting Manager, Walsall CCG Mrs J Bryan Senior Commissioning Manager – Walsall CCG Dr P Myers Consultant in Public Health Medicine - Walsall Council Mrs G Shelley Primary Care Contracting Manager, Wolverhampton CCG Mr P McKenzie Corporate Operations Manager, Wolverhampton CCG Mr J Blankley Chief Officer of Wolverhampton LPC - Wolverhampton CCG Ms S Mckie Vice Chair/Lay Member, Wolverhampton CCG Mrs L Sawrey Deputy Chief Finance Officer, Wolverhampton CCG Mrs S Southall Head of Primary Care - Wolverhampton CCG & GPFV Programme Director, Black
Country STP Mrs J Worton Primary Care Liaison Manager, Wolverhampton CCG Mr P Lydon Senior Engagement Manager – Sandwell & West Birmingham CCG Mrs J McGrandles Head of Primary Care Contracts - Sandwell & West Birmingham CCG Mrs J Jasper Lay Member, Sandwell and West Birmingham CCG Dr K Grindulis Secondary Care Consultant, Sandwell and West Birmingham CCG Mr M West Financial Controller - Sandwell & West Birmingham CCG Mr S Somers Primary Care Quality Lead - Sandwell & West Birmingham CCG Mr R Sondhi Vice Chair & Lay Member, Sandwell and West Birmingham CCG Mrs A Clarke Primary Care Contracts Manger – Sandwell & West Birmingham CCG Mr A Cave Chief Executive Officer, Healthwatch Birmingham – Sandwell & West Birmingham
CCG Mrs H Peach High Cost Drugs Pharmacist (Medicines Quality) – Sandwell & West Birmingham CCG Mrs J Rawlinson Lay Member - Sandwell and West Birmingham CCG Mrs C Evans Head of Primary Care - Sandwell & West Birmingham CCG Mr M Behal CCG IT Lead – Sandwell & West Birmingham CCG Miss J Woodhouse Acting Head of Corporate Governance, Sandwell and West Birmingham CCG Mrs L Maxfield Deputy Chief Officer (Primary and Community Transformation) – Sandwell & West
Birmingham CCG
2 | P a g e
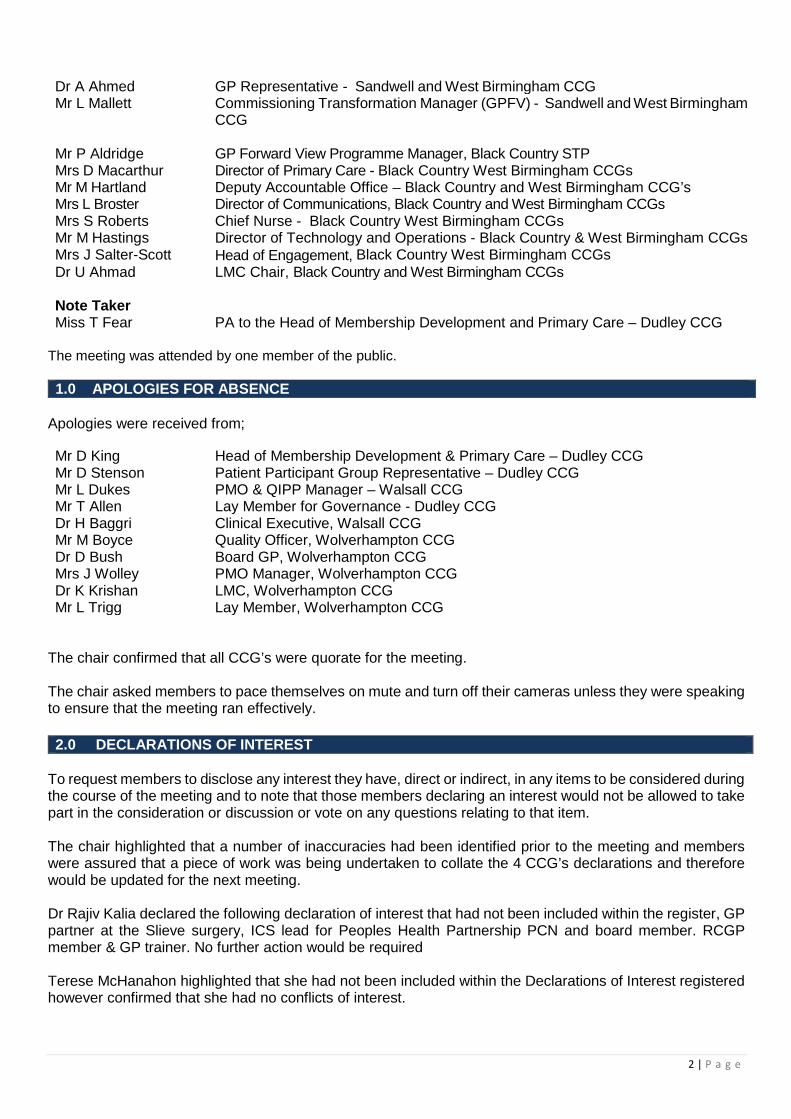
Dr A Ahmed GP Representative - Sandwell and West Birmingham CCG Mr L Mallett Commissioning Transformation Manager (GPFV) - Sandwell and West Birmingham
CCG Mr P Aldridge GP Forward View Programme Manager, Black Country STP Mrs D Macarthur Director of Primary Care - Black Country West Birmingham CCGs Mr M Hartland Deputy Accountable Office – Black Country and West Birmingham CCG’s Mrs L Broster Director of Communications, Black Country and West Birmingham CCGs Mrs S Roberts Chief Nurse - Black Country West Birmingham CCGs Mr M Hastings Director of Technology and Operations - Black Country & West Birmingham CCGs Mrs J Salter-Scott Head of Engagement, Black Country West Birmingham CCGs Dr U Ahmad LMC Chair, Black Country and West Birmingham CCGs Note Taker Miss T Fear PA to the Head of Membership Development and Primary Care – Dudley CCG
The meeting was attended by one member of the public. 1.0 APOLOGIES FOR ABSENCE
Apologies were received from;
Mr D King Head of Membership Development & Primary Care – Dudley CCG Mr D Stenson Patient Participant Group Representative – Dudley CCG Mr L Dukes PMO & QIPP Manager – Walsall CCG Mr T Allen Lay Member for Governance - Dudley CCG Dr H Baggri Clinical Executive, Walsall CCG Mr M Boyce Quality Officer, Wolverhampton CCG Dr D Bush Board GP, Wolverhampton CCG Mrs J Wolley PMO Manager, Wolverhampton CCG Dr K Krishan LMC, Wolverhampton CCG Mr L Trigg Lay Member, Wolverhampton CCG
The chair confirmed that all CCG’s were quorate for the meeting. The chair asked members to pace themselves on mute and turn off their cameras unless they were speaking to ensure that the meeting ran effectively.
To request members to disclose any interest they have, direct or indirect, in any items to be considered during the course of the meeting and to note that those members declaring an interest would not be allowed to take part in the consideration or discussion or vote on any questions relating to that item. The chair highlighted that a number of inaccuracies had been identified prior to the meeting and members were assured that a piece of work was being undertaken to collate the 4 CCG’s declarations and therefore would be updated for the next meeting. Dr Rajiv Kalia declared the following declaration of interest that had not been included within the register, GP partner at the Slieve surgery, ICS lead for Peoples Health Partnership PCN and board member. RCGP member & GP trainer. No further action would be required Terese McHanahon highlighted that she had not been included within the Declarations of Interest registered however confirmed that she had no conflicts of interest.
2.0 DECLARATIONS OF INTEREST

3 | P a g e
Resolved:
1) Committees noted the inaccuracies within the declarations of interest 2) Committees noted that the declarations of interest would be rectified in time for the next
meeting in common. 3) Committees noted the additional declarations of interest to be added to the declarations of
interest register.
3.0 MINUTES OF THE LAST MEETING OF INTERST The minutes of each CCG’s Primary Care Commissioning Committee were submitted to Committee. Dudley CCG Committee noted that the minutes relating to the meeting held on Friday 27 March 2020 were agreed as an accurate record of the meeting with the exception of a typing error under agenda item 7.0. Walsall CCG Committee noted that the minutes relating to the meetings held on Thursday 20 February & Tuesday 24 March 2020 were agreed as an accurate record of the meeting. Wolverhampton CCG Committee noted that the minutes relating to the meeting held on Tuesday 3 March 2020.were agreed as an accurate record of the meeting. Sandwell & West Birmingham CCG. Committee noted that the minutes relating to the meeting held on Thursday 5 March 2020 were agreed as an accurate record of the meeting. Sandwell & West Birmingham members were advised that an extra ordinary Primary Care Commissioning Committee meeting held in private took place on .21 May 2020 to finalise the Primary Care Commissioning Framework payments. The minutes for the meeting were electronically ratified by Committee members. An update was also provided in relation to 7.8 a facilitator from Cancer Research UK was working with the practice to improve cancer screening uptake however the staff member had recently returned to work after being placed on the Government Furlough scheme. Resolved:
1) The Primary Care Commissioning Committee for Dudley approved, the minutes of the meeting held on the Friday 27 March 2020 were agreed as an accurate record of the meeting with the exception of a typing error under agenda item 7.0
2) The Primary Care Commissioning Committee for Walsall approved the minutes relating to the meetings held on Thursday 20 February & Tuesday 24 March 2020 were agreed as an accurate record of the meeting.
3) The Primary Care Commissioning Committee for Wolverhampton Committee approved the minutes relating to the meeting held on Tuesday 3 March 2020.were agreed as an accurate record of the meeting.
4) The Primary Care Commissioning Committee for Sandwell & West Birmingham Committee the minutes relating to the meeting held on Thursday 5 March 2020 were agreed as an accurate record of the meeting.
4 | P a g e
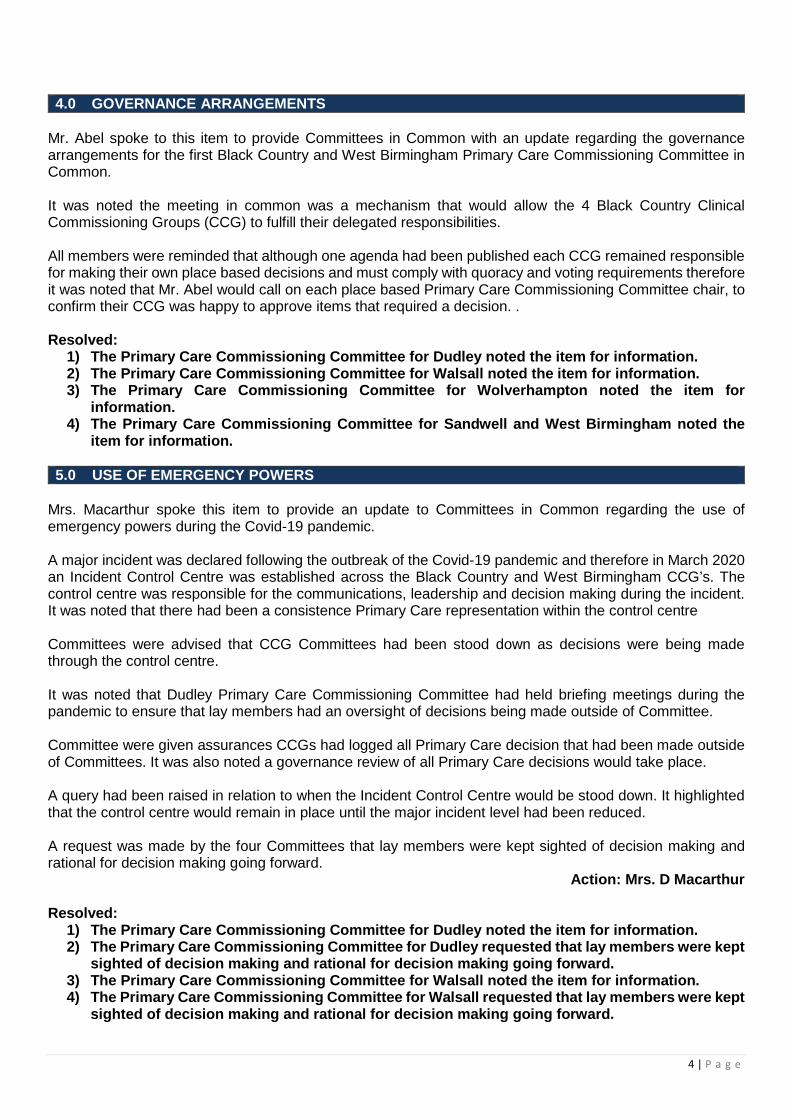
4.0 GOVERNANCE ARRANGEMENTS
Mr. Abel spoke to this item to provide Committees in Common with an update regarding the governance arrangements for the first Black Country and West Birmingham Primary Care Commissioning Committee in Common. It was noted the meeting in common was a mechanism that would allow the 4 Black Country Clinical Commissioning Groups (CCG) to fulfill their delegated responsibilities. All members were reminded that although one agenda had been published each CCG remained responsible for making their own place based decisions and must comply with quoracy and voting requirements therefore it was noted that Mr. Abel would call on each place based Primary Care Commissioning Committee chair, to confirm their CCG was happy to approve items that required a decision. . Resolved:
1) The Primary Care Commissioning Committee for Dudley noted the item for information. 2) The Primary Care Commissioning Committee for Walsall noted the item for information. 3) The Primary Care Commissioning Committee for Wolverhampton noted the item for
information. 4) The Primary Care Commissioning Committee for Sandwell and West Birmingham noted the
item for information. 5.0 USE OF EMERGENCY POWERS
Mrs. Macarthur spoke this item to provide an update to Committees in Common regarding the use of emergency powers during the Covid-19 pandemic. A major incident was declared following the outbreak of the Covid-19 pandemic and therefore in March 2020 an Incident Control Centre was established across the Black Country and West Birmingham CCG’s. The control centre was responsible for the communications, leadership and decision making during the incident. It was noted that there had been a consistence Primary Care representation within the control centre Committees were advised that CCG Committees had been stood down as decisions were being made through the control centre. It was noted that Dudley Primary Care Commissioning Committee had held briefing meetings during the pandemic to ensure that lay members had an oversight of decisions being made outside of Committee. Committee were given assurances CCGs had logged all Primary Care decision that had been made outside of Committees. It was also noted a governance review of all Primary Care decisions would take place. A query had been raised in relation to when the Incident Control Centre would be stood down. It highlighted that the control centre would remain in place until the major incident level had been reduced. A request was made by the four Committees that lay members were kept sighted of decision making and rational for decision making going forward.
Action: Mrs. D Macarthur Resolved:
1) The Primary Care Commissioning Committee for Dudley noted the item for information. 2) The Primary Care Commissioning Committee for Dudley requested that lay members were kept
sighted of decision making and rational for decision making going forward. 3) The Primary Care Commissioning Committee for Walsall noted the item for information. 4) The Primary Care Commissioning Committee for Walsall requested that lay members were kept
sighted of decision making and rational for decision making going forward.
5 | P a g e
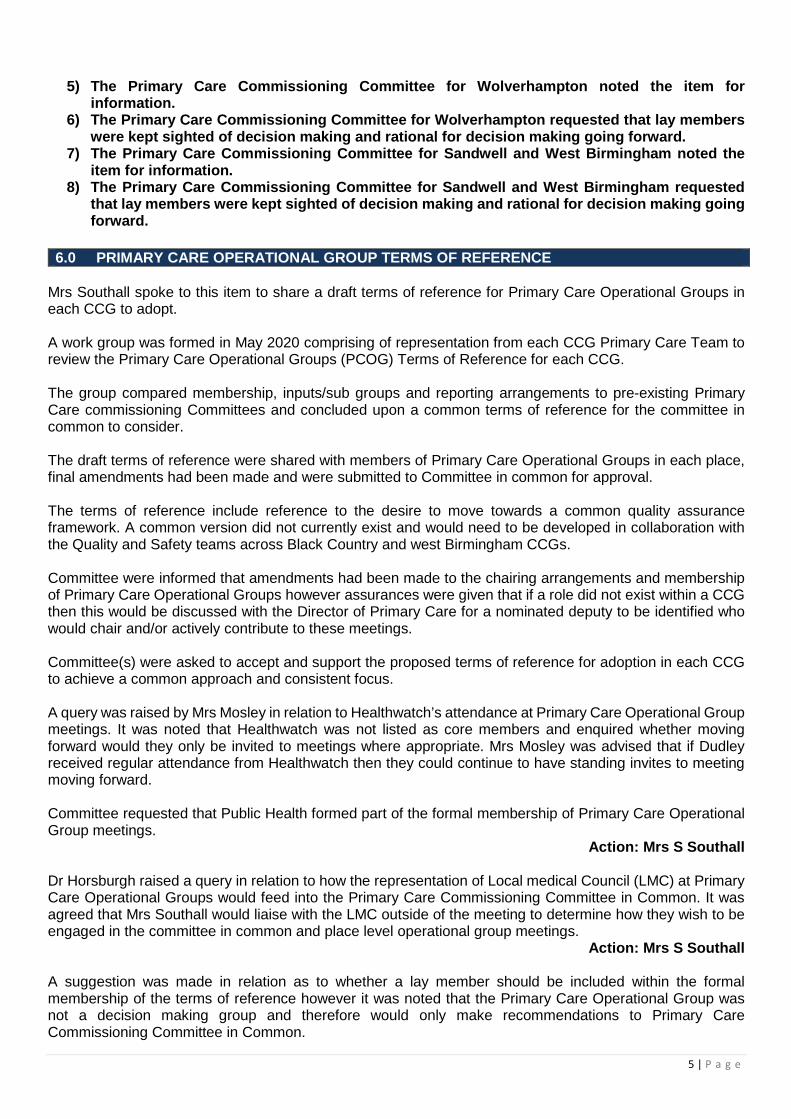
5) The Primary Care Commissioning Committee for Wolverhampton noted the item for information.
6) The Primary Care Commissioning Committee for Wolverhampton requested that lay members were kept sighted of decision making and rational for decision making going forward.
7) The Primary Care Commissioning Committee for Sandwell and West Birmingham noted the item for information.
8) The Primary Care Commissioning Committee for Sandwell and West Birmingham requested that lay members were kept sighted of decision making and rational for decision making going forward.
Mrs Southall spoke to this item to share a draft terms of reference for Primary Care Operational Groups in each CCG to adopt. A work group was formed in May 2020 comprising of representation from each CCG Primary Care Team to review the Primary Care Operational Groups (PCOG) Terms of Reference for each CCG. The group compared membership, inputs/sub groups and reporting arrangements to pre-existing Primary Care commissioning Committees and concluded upon a common terms of reference for the committee in common to consider. The draft terms of reference were shared with members of Primary Care Operational Groups in each place, final amendments had been made and were submitted to Committee in common for approval. The terms of reference include reference to the desire to move towards a common quality assurance framework. A common version did not currently exist and would need to be developed in collaboration with the Quality and Safety teams across Black Country and west Birmingham CCGs. Committee were informed that amendments had been made to the chairing arrangements and membership of Primary Care Operational Groups however assurances were given that if a role did not exist within a CCG then this would be discussed with the Director of Primary Care for a nominated deputy to be identified who would chair and/or actively contribute to these meetings. Committee(s) were asked to accept and support the proposed terms of reference for adoption in each CCG to achieve a common approach and consistent focus. A query was raised by Mrs Mosley in relation to Healthwatch’s attendance at Primary Care Operational Group meetings. It was noted that Healthwatch was not listed as core members and enquired whether moving forward would they only be invited to meetings where appropriate. Mrs Mosley was advised that if Dudley received regular attendance from Healthwatch then they could continue to have standing invites to meeting moving forward. Committee requested that Public Health formed part of the formal membership of Primary Care Operational Group meetings.
Action: Mrs S Southall
Dr Horsburgh raised a query in relation to how the representation of Local medical Council (LMC) at Primary Care Operational Groups would feed into the Primary Care Commissioning Committee in Common. It was agreed that Mrs Southall would liaise with the LMC outside of the meeting to determine how they wish to be engaged in the committee in common and place level operational group meetings.
Action: Mrs S Southall A suggestion was made in relation as to whether a lay member should be included within the formal membership of the terms of reference however it was noted that the Primary Care Operational Group was not a decision making group and therefore would only make recommendations to Primary Care Commissioning Committee in Common.
6.0 PRIMARY CARE OPERATIONAL GROUP TERMS OF REFERENCE

6 | P a g e
An amendment was suggested to the quoracy to include representation from finance in order for the meeting to be quorate. However members were reminded that financial implications should be included within the papers to ensure the group were appropriately informed.
Action: Mrs S Southall Discussions took place in relation to whether the Committee Terms of References needed to be reviewed as a result of Primary Care Operational Groups adopting a common terms of reference and the implementation of the Joint Commissioning Board. It was recognised that a review should be undertaken however assurances were given that the terms of reference of each CCG’s Primary Care Commissioning Committees were already similar due to the delegated powers given to CCG’s via NHS England.
Action: Committee Chairs/Governance leads Resolved:
1) The Primary Care Commissioning Committee for Dudley accepted and supported the proposed terms of reference for adoption in each CCG to achieve a common approach and consistent focus, subject to the amendments listed above.
2) The Primary Care Commissioning Committee for Walsall accepted and supported the proposed terms of reference for adoption in each CCG to achieve a common approach and consistent focus, subject to the amendments listed above.
3) The Primary Care Commissioning Committee for Wolverhampton accepted and supported the proposed terms of reference for adoption in each CCG to achieve a common approach and consistent focus, subject to the amendments listed above.
4) The Primary Care Commissioning Committee for Sandwell and West Birmingham accepted and supported the proposed terms of reference for adoption in each CCG to achieve a common approach and consistent focus, subject to the amendments listed above.
Mr Abel spoke to this item to compare the current risks held by each Primary Care Commissioning Committee and determine the issues that are common to all or that would be better addressed at a regional level rather than locally. A paper was submitted to the Committees in Common detailing each CCG’s rational and systems for Primary Care risks. The chair made a proposal that Committee chairs, Primary Care and Governance leads review the risk registers outside meeting and update Committees in Common at a future meeting.
Action: Committee Chairs, Primary Care and Governance Leads Resolved:
1) The Primary Care Commissioning Committee for Dudley accepted the proposal that Committee chairs, Primary Care and Governance leads review the risk registers outside meeting and update Committees in Common at a future meeting.
2) The Primary Care Commissioning Committee for Walsall accepted the proposal that Committee chairs, Primary Care and Governance leads review the risk registers outside meeting and update Committees in Common at a future meeting.
3) The Primary Care Commissioning Committee for Wolverhampton accepted the proposal that Committee chairs, Primary Care and Governance leads review the risk registers outside meeting and update Committees in Common at a future meeting.
4) The Primary Care Commissioning Committee for Sandwell and West Birmingham accepted the proposal that Committee chairs, Primary Care and Governance leads review the risk registers outside meeting and update Committees in Common at a future meeting.
7.0 RISK REGISTER

7 | P a g e
8.0 SANDWELL AND WEST BIRMINGHAM CCG - APPLICATION FOR THE CLOSURE OF CENTRAL CLINIC BRANCH SITE
Mrs McGrandles spoke to this item to request Committee consider the application from Linkway Medical Practice to close their branch site Central Clinic, Horseley Road, Tipton, DY4 7NB. The Chair reminded members that the item required a decision from Sandwell and West Birmingham Primary Care Commissioning Committee only. Committee was advised that an application had been received by Linkway Medical Practice in regards to closing their branch site – Central Clinic Tipton. The practice has a registered list size of 14,000, it has a main site at the Lyng Medical Centre and two branch sites one at Dartmouth Medical Centre and the second at Central Clinic. It was not that of the 14,000 registered list size approximately 800 patients had accessed health services from the Central Clinic branch sites, the patients were happy to receive their health care at either Lyng Medical Centre or Dartmouth Medical Centre. However there were a small number of patients who chose to register with another GP practice and Linkway Medical Practice supported those patients accordingly. Following a meeting with the CCG, the Practice agreed to undertake a more detailed consultation, in particular with their vulnerable patients and/or carers who were contacted via telephone. It was noted that over half of the Central Clinic site was empty costing the CCG £61,000 per annum for the void space, in addition to this, the GP section of the building costs the CCG £25,500 per annum, should the application for closure be approved, the CCG would be able to declare the whole building as surplus, resulting in its sale and removal from the CCG system costs. Committee were advised that the Premises Review Panel had also reviewed the application submitted by Linkway medical Centre and made a recommendation to approve the closure. Resolved:
1) The Primary Care Commissioning Committee for Sandwell and West Birmingham approved the application made by Linkway Medical Centre to close the Central Clinic branch site with immediate effect.
Mrs Evans spoke to this item to inform Committee of the work that has been undertaken to review the Primary Care Commissioning Framework (PCCF) for 20/21 in light of COVID 19 and the options that have been considered in finalising an amended framework and to gain approval for the amended framework and the principles around delivery and payment. The Chair reminded members that the item required a decision from Sandwell and West Birmingham Primary Care Commissioning Committee only. Dr Ahmed & Dr Suleman declared their interest in this item as they held direct financial interests relating to the Primary Care Commissioning Framework as GMS contract holders within Sandwell and West Birmingham CCG. No further action was required. The Primary Care Commissioning Framework was previously agreed at Committee in March 2020 however due to the pandemic and the decision to suspend formal Committees the framework had not been formally commissioned by Sandwell and West Birmingham members. Following the confirmation of General Practice entering the second phase of the pandemic a review of the previously agreed framework for 20/21 had been undertaken and the following options were considered;
9.0 SANDWELL AND WEST BIRMINGHAM CCG AMENDED PRIMARY CARE COMMISSIONING FRAMEWORK FOR 2020/21
8 | P a g e
• Option 1 – To launch the PCCF as agreed in March 2020 with no amendments. • Option 2 – To undertake a review of each standard to assess deliverability during COVID 19, making
any necessary amendments. • Option 3 – To undertake a more radical review of the PCCF to refocus efforts on targeting work
towards population groups most adversely affected by COVID 19. In considering the options the feedback from Clinical and Commissioning Leads and Primary Care Network Clinical Directors on behalf of their member practices was also taken into consideration. It was noted that option two was the preferred option. It was expected that the CCG would launch the new framework in July 2020. NHS England mandated CCGs support care homes during the Covid-19 pandemic and therefore Sandwell and West Birmingham CCG were required to commission a separate Care Home Local Improvement Scheme. The monies associated with the Primary Care Commissioning framework was repurposed to fund the Local Improvement Scheme. Committee were informed in light of the uncertainty for the remainder of the financial year, and that income from the framework represented a significant percentage of the total practice income, Committee were asked to consider approving an income guarantee for practices. The framework was paid on the principle of 70% payment for delivery which had been made in advance through quarterly payments and a balancing payment of up to 30% based on achievement of the various outcome requirements in each standard. It is therefore recommended a guarantee is provided to practices that the funding for the framework would continue to be ring-fenced with practices guaranteed to retain their 70% delivery payments. It was noted if further spikes in COVID 19 and practices had achieved at least the minimum outcome targets, practice would receive the full payment for those particular requirements. Resolved:
1) The Primary Care Commissioning Committee for Sandwell and West Birmingham approved the outcome of the review of the Primary Care Commissioning Framework 20/21 in light of COVID 19 and the amended framework requirements would be commissioned from 1st July 2020.
2) The Primary Care Commissioning Committee for Sandwell and West Birmingham approved the continued ringfencing of Primary Care Commissioning Framework funding and provided a guarantee to member practices that they would retain their 70% delivery payments and if further spikes in COVID 19 occurred during 20/21 and at least the minimum outcome targets were met, practices would receive the full payment for those particular requirements.
Mrs Southall spoke to this item to provide an overview position for each CCGs Primary Care Frameworks and enhanced service payments/activity. Declarations of interests were made by all GP members of the Committee meetings in common as they held direct financial interests relating to the Primary Care Commissioning Framework as GMS contract holders within their respective CCGs. No further action was required. Committee members were advised that a work stream had been formed to review the position within each place/CCG for their respective Primary Care Frameworks and Local Improvement/Enhanced Services. It was noted that Dudley CCG had opted out of the National Quality Outcomes Framework (QOF) and therefore held their own locally agreed framework which was approved at the Primary Care Commissioning Committee for Dudley in March 2020 for implantation in April 2020. The remains CCGs held quality improvement frameworks in place with variation in the level of investment and state of readiness to launch with practices within their respective membership(s).
10.0 CCG FRAMEWORKS
9 | P a g e
The Committee’s in Common were asked Members of the Primary Care Commissioning Committees were asked to approve the following recommendations;
• Support the recommendations made pertaining to local frameworks and the timescales for implementation.
• Consider and confirm their support for further work to be undertaken to reduce the variation in content of quality frameworks and locally commissioned service, including consistent service specifications and payment.
• Confirm their support for a consistent approach to preserving practice income across all CCGs, and the importance of managing demand from October to March 2021 to achieve a comparable level of performance with 2019/20 activity.
Resolved:
1) The Primary Care Commissioning Committee for Dudley approved recommendations made pertaining to local frameworks and the timescales for implementation.
2) The Primary Care Commissioning Committee for Dudley gave their support for further work to be undertaken to reduce the variation in content of quality frameworks and locally commissioned service, including consistent service specifications and payment.
3) The Primary Care Commissioning Committee for Dudley gave their support for a consistent approach to preserving practice income across all CCGs, and the importance of managing demand from October to March 2021 to achieve a comparable level of performance with 2019/20 activity.
4) The Primary Care Commissioning Committee for Walsall approved recommendations made pertaining to local frameworks and the timescales for implementation.
5) The Primary Care Commissioning Committee for Walsall gave their support for further work to be undertaken to reduce the variation in content of quality frameworks and locally commissioned service, including consistent service specifications and payment.
6) The Primary Care Commissioning Committee for Walsall gave their support for a consistent approach to preserving practice income across all CCGs, and the importance of managing demand from October to March 2021 to achieve a comparable level of performance with 2019/20 activity.
7) The Primary Care Commissioning Committee for Wolverhampton approved recommendations made pertaining to local frameworks and the timescales for implementation.
8) The Primary Care Commissioning Committee for Wolverhampton gave their support for further work to be undertaken to reduce the variation in content of quality frameworks and locally commissioned service, including consistent service specifications and payment.
9) The Primary Care Commissioning Committee for Wolverhampton gave their support for a consistent approach to preserving practice income across all CCGs, and the importance of managing demand from October to March 2021 to achieve a comparable level of performance with 2019/20 activity.
10) The Primary Care Commissioning Committee for Sandwell and West Birmingham approved recommendations made pertaining to local frameworks and the timescales for implementation.
11) The Primary Care Commissioning Committee for Sandwell and West Birmingham gave their support for further work to be undertaken to reduce the variation in content of quality frameworks and locally commissioned service, including consistent service specifications and payment.
12) The Primary Care Commissioning Committee for Sandwell and West Birmingham gave their support for a consistent approach to preserving practice income across all CCGs, and the importance of managing demand from October to March 2021 to achieve a comparable level of performance with 2019/20 activity.
10 | P a g e
Mr Hastings spoke to this item to provide Committees in Common with an update regarding a review of digital changes implemented as a result of covid 19 across Primary Care, Acute and Mental Health Services. The paper submitted to Committee in Common provided a high level overview of Digital services across the Black Country and West Birmingham. It was noted that a detailed review had been commissioned by Midlands & Lancashire CSU to undertake a detailed review of the Digital offerings that had been implemented across all settings. It was expected that the review would be completed early July 2020. Mr Hastings advised that a further piece of work was required to consolidate digital applications to ensure interoperability is maintained across the different systems. A brief discussion took place in relation to ensuring that digital offers did not disadvantage cohorts of patients assurances where given this was being considered at the Digital Board. It was suggested that a patient representative/ lay member be included during these discussions. Members of the Primary Care Commissioning Committees were asked to note that the piece of work would be managed by the Sustainability and Transformation Plan (STP) Digital Board. Resolved:
1. The Primary Care Commissioning Committee for Dudley noted that the piece of work would be managed by the Sustainability and Transformation Plan (STP) Digital Board.
2. The Primary Care Commissioning Committee for Walsall noted that the piece of work would be managed by the Sustainability and Transformation Plan (STP) Digital Board.
3. The Primary Care Commissioning Committee for Wolverhampton noted that the piece of work would be managed by the Sustainability and Transformation Plan (STP) Digital Board.
4. The Primary Care Commissioning Committee for Sandwell and West Birmingham noted that the piece of work would be managed by the Sustainability and Transformation Plan (STP) Digital Board.
Mr Cowley spoke to this item to provide information to the Committees on the financial expenditure of the Black Country and West Birmingham CCGs’ delegated Primary Care resource for the 2019/20 financial year. All were informed that each CCG remained as separate statuary NHS bodies and therefore finances were also managed separately. An overview for the financial position 2019/20 was provided to the Committee’s in common. It was noted that the financial position for delegated Primary Care was expected to operate within its allocated resource and the over performance at Sandwell and West Birmingham CCG was funded using the CCG core allocation. The contingencies, recurrent and non-recurrent reserves were held in accordance with the NHSE business rules and in 2019/20 all contingencies have been utilised. Committees were advised that no surpluses were required against the delegated resource in 2019/20. In relation to the 2020/21 financial plan it was noted that during the current COVID-19 initial response phase an alternative financial regime was in place which ensured a short-term break-even position across these budgets, however the regime is currently only in place until the end of July. It was recognised that financial planning gaps had been identified for Dudley CCG & Sandwell & West Birmingham CCG which would need to be addressed to ensure that the CCG’s remained in financial balance across the remaining financial year. Committee was given assurances that the issues had already been discussed at individual Committees. It was expected that individual management plans would be produced to ensure a break-even position is achieved across the financial year and discussed with local Primary Care Operational Group meetings in August, with further discussions to place at Committee’s in Common in Augusts 2020.
11.0 DIGITAL REPORT
12.0 FINANCE REPORT
11 | P a g e
Committee then held discussions in relation to the financial implications following the Covid-19 pandemic. It was noted that financial arrangements for practices have been subject to a number of changes in response to the outbreak, which were in line with guidance from NHSE to protect practice income and reimburse genuine additional costs incurred by practices. Discussions took place in relation to the difference in the number of claims made by each CCG during March & April. It was noted that a reason for this may be due to how each CCG commissioned their bank holiday provision and the numbers of practices open. It was also recognised that not claims had been submitted prior to the publication of the paper however it was expected that a there would be reduction in variation for the following months. Members of the Primary Care Commissioning Committees were asked to:
• Discuss the contents of the report; • Approve the contents of the report and the financial position for the year 2019/20 and 2020/21. • Note the residual risks identified in this report.
Resolved:
1. The Primary Care Commissioning Committee for Dudley discussed the contents of the report.
2. The Primary Care Commissioning Committee for Dudley approved the contents of the report and the financial position for the year 2019/20 and 2020/21.
3. The Primary Care Commissioning Committee for Dudley noted the residual risks identified in the report.
4. The Primary Care Commissioning Committee for Walsall discussed the contents of the report.
5. The Primary Care Commissioning Committee for Walsall approved the contents of the report and the financial position for the year 2019/20 and 2020/21.
6. The Primary Care Commissioning Committee for Walsall noted the residual risks identified in the report.
7. The Primary Care Commissioning Committee for Wolverhampton discussed the contents of the report.
8. The Primary Care Commissioning Committee for Wolverhampton approved the contents of the report and the financial position for the year 2019/20 and 2020/21.
9. The Primary Care Commissioning Committee for Wolverhampton noted the residual risks identified in the report.
10. The Primary Care Commissioning Committee for Sandwell and West Birmingham discussed the contents of the report.
11. The Primary Care Commissioning Committee for Sandwell and West Birmingham approved the contents of the report and the financial position for the year 2019/20 and 2020/21.
12. The Primary Care Commissioning Committee for Sandwell and West Birmingham noted the residual risks identified in the report.
Mrs Roberts spoke to this item to provide assurance to the committees on the core quality and safety activities relating to primary care during the reporting period April 2020- June 2020. In order to fully discharge the statutory duties, each CCG submitted a detailed report in accordance with its usual reporting mechanisms and were attached as appendices to the report.
13.0 QUALITY AND SAFETY REPORT
12 | P a g e
Care Quality Commission (CQC) Committees were advised that due to the Covid-19 pandemic CQC routine inspections were paused effective 16 March 2020 however assurances were given that CQC had developed an Emergency Support Framework to follow during the pandemic. A list of the practices rated as inadequate by the CQC and the date of publication were provided to Committees. It was noted that two list dispersals were carried out for two inadequate rated practices within Sandwell and West Birmingham CCG, Fiveways Health Centre & Bloomsbury Medical Centre on 31 March 2020 following CQC enforcement action. In relation a practice within Walsall CCG, Forrester Street Surgery the practice were subject to a re-inspection 4 February 2020 as a ‘Special Measures’ practice where improvements were noted. A further follow up visited was carried out in April 2020 where the CQC action was reviewed and further improvements were identified. Walsall CCG were also due to visit the practice to discuss the full action plan and update to Committee would be provided within a future report. Health Protection In relation to Personal Protection Equipment (PPE) all primary care teams had worked in partnership with the distribution centre provision at Jubilee House to ensure sufficient supplies and replenishment of stock was prioritised. The service had been in place since early April 2020 and continued to provide stability to the provision of PPE in line with national guidance for general practice. It was noted that the distribution centre would remain in place over the coming months and would be reviewed in line with the national arrangements. Infection Prevention and Control The planned 2020/21 work programme for infection prevention and control had been placed on hold due to the Covid-19 pandemic. However advice and support has been ongoing in respect of IPC during Covid-19 and provided together with advice for managing differing cohorts of patients, including those requiring face to face consultations, this includes PPE advice, decontamination and waste management advices. Immunisation Routine immunisation and vaccination activity was in place however CCGs had been had been asked to ensure that plans were in for the forthcoming flu season. However it was noted that work continued at a local place to promote and increase uptake of immunisations and flu vaccination. CCG also took into consideration in regards to the social distancing measures that had been implemented to enable clinics to continue within Primary Care. Patient Experience In relation to the Friends and Family test national guidance had been published advising that the contractual quality metric be placed on hold during the pandemic. Committees were advised that 1 serious incident was currently being reviewed by Dudley CCG. Committee members passed comment in relation to a set of embedded documents contained within one of the appendices and requested for future reports not contain such formatting. All Primary Care Commissioning Committees formally thanked those involved within the PPE distribution centre for ensuring Primary Care colleagues remained resilient during the pandemic. Committee requested that a future report highlighted the work that had been carried out in relation to the flu campaign.
Action: Mrs S Roberts
13 | P a g e
Members of the Primary Care Commissioning Committees were asked to receive the report for assurance and support the monitoring arrangements and actions taken Resolved:
1. The Primary Care Commissioning Committee for Dudley received the report for assurance and supported the monitoring arrangements and actions taken.
2. The Primary Care Commissioning Committee for Walsall received the report for assurance and supported the monitoring arrangements and actions taken.
3. The Primary Care Commissioning Committee for Wolverhampton received the report for assurance and supported the monitoring arrangements and actions taken.
4. The Primary Care Commissioning Committee for Sandwell and West Birmingham received the report for assurance and supported the monitoring arrangements and actions taken.
Mrs Southall spoke to this item to update Committees on the work of the new single STP Training Hub since April 1st 2020 and also to seek approval to mobilise a number of new schemes Context. The Chair reminded members that the item contained one recommendation that required a decision from Wolverhampton Primary Care Commissioning Committee only. Committees were advised that the STP had undergone a significant piece of organisational development and transition to ensure that its Training Hubs delivered the expectations within the Long Term Plan and those from Health Education England. As a result there was now a single Training Hub in place serving the 4 CCGs and 5 places across the STP. It was noted that a detailed programme of work had been provided within an appendix to the report. The Training Hub had supported the Primary Care response to the Covid- 19 pandemic, whilst also continuing to support the development of the workforce where possible utilising digital technology and remote working. A full update on the work of the Training Hub and key next steps were included within Appendix B. It was noted that funding allocations were yet to be confirmed in writing with supporting Memorandums of Understanding. However it was expected this would be received imminently. Wolverhampton Primary Care Commissioning Committees members were asked to
• Approve the implementation of the Learner Management System at a cost of £22k in the first instance, with the acknowledgment that should the number of licenses required increase, there will be a pro- rata increase in cost for the remainder the year up to a maximum level of 28k.
It was noted that Information Governance had been fully involved in the process and had approved the Data Privacy Impact Awareness document to enable the work to proceed should the recommendation be approved at this Committee. All members of the Primary Care Commissioning Committees were asked to
• Note and approve the proposed governance arrangements for the Training Hub as outlined in Appendix A
• To note and recognise the work of the Training Hub in supporting the Covid-19 response and to approve the mobilisation of the new schemes that were approved in principle by the Primary and Community Care Workforce Implementation Group on 2nd June 2020 and included in the Appendices to this report.
.
14.0 TRAINING HUB REPORT
14 | P a g e
Resolved: 1) The Primary Care Commissioning Committee for Wolverhampton approved the
implementation of the Learner Management System at a cost of £22k in the first instance, with the acknowledgment that should the number of licenses required increase, there will be a pro- rata increase in cost for the remainder the year up to a maximum level of 28k.
2) The Primary Care Commissioning Committee for Wolverhampton noted and approved the proposed governance arrangements for the Training Hub as outlined in Appendix A
3) The Primary Care Commissioning Committee for Wolverhampton noted and recognised the work of the Training Hub in supporting the Covid-19 response and approved the mobilisation of the new schemes that were approved in principle by the Primary and Community Care Workforce Implementation Group on 2nd June 2020 and included in the Appendices to this report.
4) The Primary Care Commissioning Committee for Dudley noted and recognise the work of the Training Hub in supporting the Covid-19 response and to approve the mobilisation of the new schemes that were approved in principle by the Primary and Community Care Workforce Implementation Group on 2nd June 2020 and included in the Appendices to this report.
5) The Primary Care Commissioning Committee for Walsall noted and recognise the work of the Training Hub in supporting the Covid-19 response and to approve the mobilisation of the new schemes that were approved in principle by the Primary and Community Care Workforce Implementation Group on 2nd June 2020 and included in the Appendices to this report.
6) The Primary Care Commissioning Committee for Sandwell and West Birmingham noted and recognise the work of the Training Hub in supporting the Covid-19 response and to approve the mobilisation of the new schemes that were approved in principle by the Primary and Community Care Workforce Implementation Group on 2nd June 2020 and included in the Appendices to this report.
Mrs McGrandles spoke to this item to provide assurance to Primary Care Commissioning Committee in Common on Primary Issues. Committees were advised that the report had been produced in collaboration with the other CCG’s Primary Care Leads. As discussed under item 6.0 a single Primary Care Operational Group Terms of Reference had been produced. Committees requested that discussions were held with the lay members for each CCG in relation to whether additional items needed to be included with the Primary Care Operational Group report following the publication of a single terms of reference.
Action: Sarah Southall It was noted that each of the Black Country and West Birmingham CCGs completed a rolling programme of GP contract visits on 31 March 2020 and work was underway in each area to develop a new 3-year rolling programme from 1 April 2020 which was stood down in response to Covid-19. Resolved:
1. The Primary Care Commissioning Committee for Dudley noted the report for assurance. 2. The Primary Care Commissioning Committee for Walsall noted the report for assurance 3. The Primary Care Commissioning Committee for Wolverhampton noted the report for
assurance 4. The Primary Care Commissioning Committee for Sandwell and West Birmingham noted the
report for assurance
15.0 PRIMARY CARE OPERATIONAL GROUP REPORT

15 | P a g e
Patient involvement Mrs Jasper enquired as to the numbers of public attendee’s to the meeting and whether discussions had been held outside Committee as to gaging their views about holding Primary Care Commissioning Committees in common. Mrs Jasper was advised that all members would be asked for feedback after the meeting. Members formally thanked those involved with the organisation of the first Primary Care Commissioning Committee in Common for ensuring that the meeting run smoothly.
Tuesday 25th August 2020 10:00-12:00 noon Meeting to be held virtually MINUTES ACCEPTED AS A TRUE AND CORRECT RECORD Name Title
Signed Date
16.0 AOB
16.0 DATE AND TIME OF THE NEXT MEETING
1 | P a g e
PRIMARY CARE COMMISSIONING COMMITTEE IN COMMON
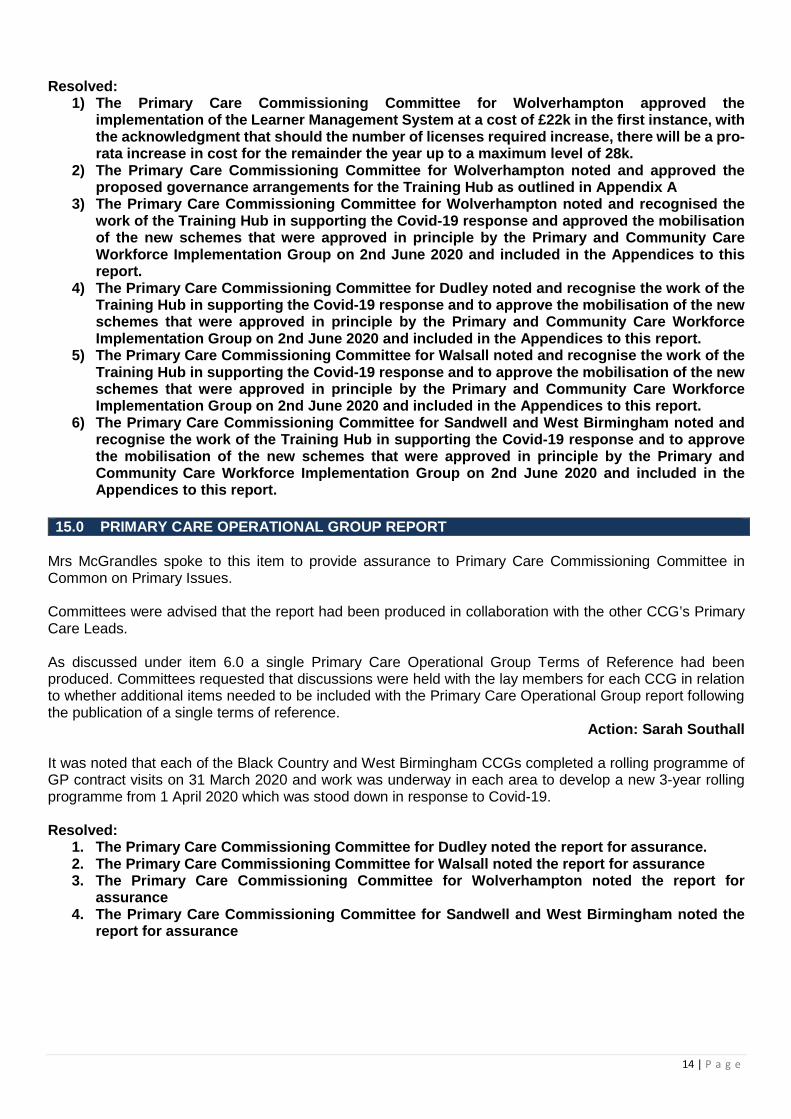
OUTSTANDING ACTION LIST – 25 AUGUST 2020
MEETING REFERENCE ACTION ACTION OWNER STATUS
DEADLINE DATE
PCCCIC/JUNE/20/5.0
Use of Emergency Powers All CCG’s to ensure lay members were kept sighted of decision making and rational for decision making going forward.
Mrs D Macarthur On-going August 2020
PCCCIC/JUNE/20/6.0
Primary Care Operational Group Terms of Reference Mrs Southall to make the following amends to the terms of reference
• Public Health to be included in formal membership • Finance to be included with the quoracy
Mrs S Southall On-going August 2020
PCCCIC/JUNE/20/6.1
LMC Representation Mrs Southall to liaise with LMC representatives determine how they wish to be engaged in the committee in common and place level operational group meetings.
Mrs S Southall On-going August 2020
PCCCIC/JUNE/20/6.2
Primary Care Commissioning Committee’s - Terms of Reference A review to be undertaken of each Primary Care Commissioning Committee’s Terms of Reference following the implementation of the Joint Commissioning Board and the adoption of common Primary Care Operational Group terms of reference.
Committee Chairs & CCG Governance
Leads On-going August 2020
PCCCIC/JUNE/20/7.0
Risk Register Risk registers to be reviewed by Committee chairs, Primary Care and Governance leads and update Committees in Common at a future meeting.
Committee Chairs, Primary Care Leads Governance Leads
On-going August 2020
2 | P a g e
MEETING REFERENCE ACTION ACTION OWNER STATUS
DEADLINE DATE
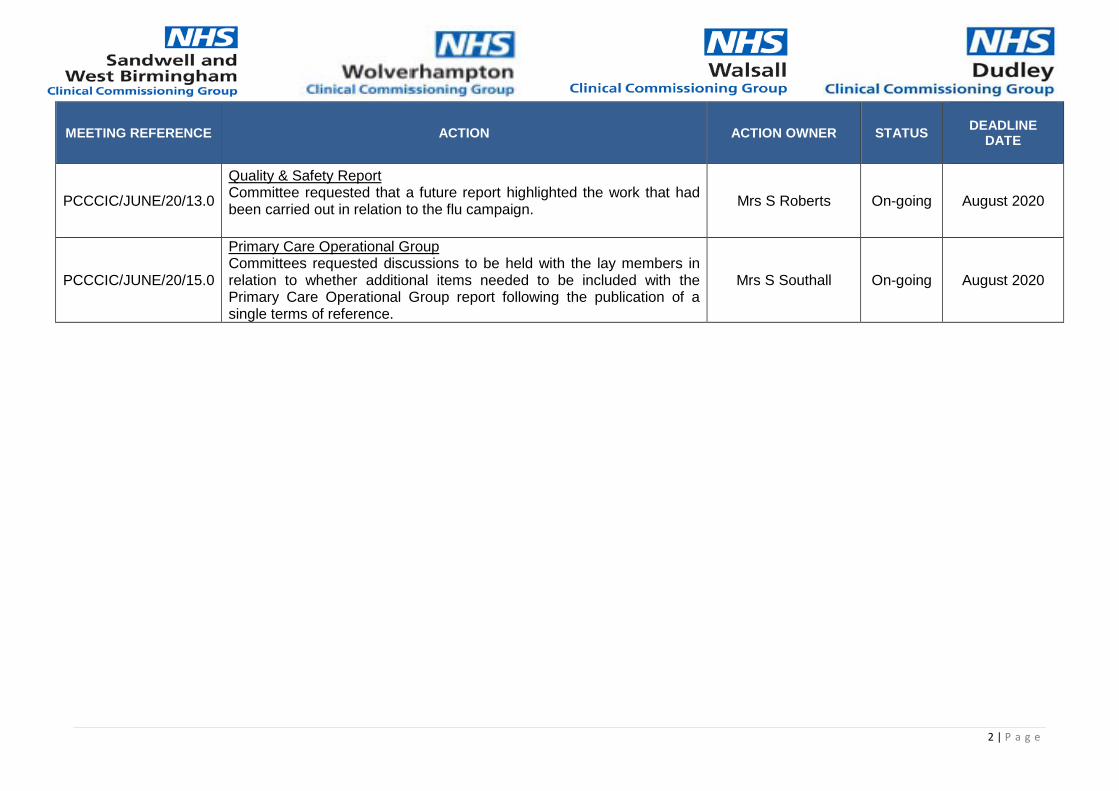
PCCCIC/JUNE/20/13.0
Quality & Safety Report Committee requested that a future report highlighted the work that had been carried out in relation to the flu campaign.
Mrs S Roberts On-going August 2020
PCCCIC/JUNE/20/15.0
Primary Care Operational Group Committees requested discussions to be held with the lay members in relation to whether additional items needed to be included with the Primary Care Operational Group report following the publication of a single terms of reference.
Mrs S Southall On-going August 2020
Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group
NHS Walsall Clinical Commissioning Group
NHS Wolverhampton Clinical Commissioning Group
PRIMARY CARE OPERATIONAL GROUP
Terms of Reference
Purpose The role of the Primary Care Operational Group (PCOG) is to operationally support delivery of the delegated responsibilities relating to the commissioning of primary medical services. The PCOG will have delegated responsibility from the Primary Care Commissioning Committee (held in common for all CCGs) and the respective terms of reference. The purpose of this group is to maintain an overview of the CCG(s) operational support to primary care providing assurance to the Primary Care Commissioning Committee that will be held in common. Duties & Responsibilities The overall objective for this group will be to ensure that the work required by the Primary Care Commissioning Committee delegated and held at CCG level to maintain an overview of activity and will require routine reporting to the committee include:-
Strategy - implementation of the CCG and STP strategies for primary care based on national and local priorities that ensure stakeholders remain engaged at place level and priorities both national and local are recognised including GPFV strategic changes.
Workforce – in addition to the workforce component of the STP Primary Care Strategy general practice training and development will be fundamental to the Black Country Training Hub operating standards. Needs analysis spanning all staff groups, recruitment attraction and retention initiatives plus quality assurance of training practices and student placements.
Quality – Triangulate all relevant data and information to identify issues and concerns through routine review of the primary care assurance framework. This will be a standard information set designed to identify patient safety, experience and clinical effective trends and queries for discussion and where necessary improvement and assurance measures will be identified.
Contract management – discussing and agreeing actions or recommendations to support local practices and practitioners whose performance is giving cause for concern and requires action as per their respective contractual terms. Maintain timely delivery of a prioritised contract review for all contracts (GMS/APMS practices) extending to QOF and Locally Commissioned Services in partnership with other commissioners including Public Health using the approved review tool.
Proposed Mergers/Practice Developments – discussing initial proposals and supporting programmes of development within local practice and consideration of all amendments to the contract register in the wider context of safe services and sustainable general medical service provision. Make recommendations to the Primary Care Commissioning Committee in relation to contract changes, the establishment of new GP practices, re-procurement of existing practices and closure of GP practices.
Enhanced Services – discussing issues such as uptake and performance of existing services and the development of new proposed services including time limited incentives to improve performance and/or address population health need. The clinical governance model should seek to ensure both national and local population health needs are recognised and prioritised for inclusion in the respective framework/offer to general practice to secure on-going quality improvements.
Digital – work programmes to enable the ongoing development of new and existing technology and informatics within primary care will be considered as part of the GPIT update. The respective programme of work will be recognised and considered to ensure timely and effective delivery and also extends to data quality considerations pertaining to GP clinical systems and clinical coding ie QOF, enhanced services etc.

Document name goes here, document name goes here | 2 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group
NHS Walsall Clinical Commissioning Group
NHS Wolverhampton Clinical Commissioning Group
Estates – primary care estate development updates will be discussed spanning the range of programme opportunities prioritised in line with the Estates Strategy. Regular reports from the strategic estates and Capital Review Group and details of Primary Care Infrastructure fund bids will be shared.
The group will use this overview to direct action within both the CCG and make recommendations to the committee for decision, assurance and/or approval. Given the extensity of this group reports from sub groups including QOF/Frameworks, Training Hub, Quality including flu planning etc will be accepted and form the basis for discussions at the Primary Care Operational Group Meetings. Membership
Representatives for this group comprise of regular formal members and other representatives who may
attend periodically:- Formal Membership
Head of Primary Care (Chair)
Primary Care Contracting
Quality Team
Medicines Optimisation
IM&T Programme Manager
Estates
Place Based Commissioning Team
NHS England Primary Care Contracting
Finance
Practice Manager
Training Hub
Public Health
GP member (may be governing body)
Local Medical Committee (LMC)
Other representatives that may attend intermittently including:-
Local Pharmaceutical Committee (LPC)
Care Quality Commission
Health Watch
Integrated Care Partnership
Communications Team
Engagement Team
In order to assist with agenda setting other representatives will be encouraged to attend at least one in three meetings, one per quarter. Meetings will be supported by dedicated administrative support to ensure agenda setting takes place with the chair ahead of each meeting and also to enable timely distribution of meeting papers, no less than 3 working days prior to the meeting date. Meeting Frequency Meetings should be held at monthly intervals with the expectation that there will be no less than ten meetings held per financial year.

Document name goes here, document name goes here | 3 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group
NHS Walsall Clinical Commissioning Group
NHS Wolverhampton Clinical Commissioning Group
Quorum Requirements Meetings will be deemed quorate provided there are 4 formal representatives present and must include representation from the CCG Primary Care and Finance Team representative(s). Recognition is given to the need for formal representatives to identify a nominated deputy to attend these meetings on their behalf should they be unable to attend in person. Governance & Assurance Reporting As a sub group of the Primary Care Commissioning Committee in Common regular assurance reports will be prepared and shared collectively among all CCGs to enable one combined report to be considered at each committee meeting. Report to the Committee will confirm progress on all areas responsibility delegated and for decision making and will escalate other issues on an exception basis as required. This will include supporting the Committee in reporting its decisions and actions to other groups and committees at place and strategic level, where appropriate as structures become established. Decision making regarding finance will be as per the respective CCGs scheme of delegation allowing the respective budget holder/manager to approve expenditure within his/her delegated limits and in accordance with the requirements of the respective standing financial instructions / procurement rules. The committee will be furnished with a breadth of information as per the group’s responsibilities detailed above. There may be items requiring furtherance and in exceptional circumstances matters of concern will be raised with the CCG Executive Team in the period between committee meetings, should the need for urgent decision arise. Representatives from CCG Teams including quality, finance, commissioning etc will be expected to ensure they also provide assurance within their respective departmental reporting to other relevant committees including Audit, Quality and Safety etc. Any conflict(s) of interest in membership/involvement in this group will be declared by those involved & managed via the Chair of the group. The agenda will include Declarations of Interest at the top of the agenda to ensure conflicts are managed accordingly by the chair before any detailed discussions take place. There will be practice level information discussed within these meetings that will require colleagues attending these meetings to observe confidentiality of information shared and its sensitivity. Therefore, members and those in attendance will be asked to sign and abide by a confidentiality statement. Audit & Review Periodic review of the role of this group & its performance may be undertaken in conjunction with the CCGs Audit Program and/or instruction from the Audit & Governance Committee. The group will review its terms of reference annually. Any changes identified will be made to the terms of reference and version control adjusted accordingly prior to submission to the Primary Care Commissioning Committee for approval. SLS/PCOG-TOF/V1.3FINAL-Aug20

Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Primary Care Commissioning Committee Effectiveness Survey
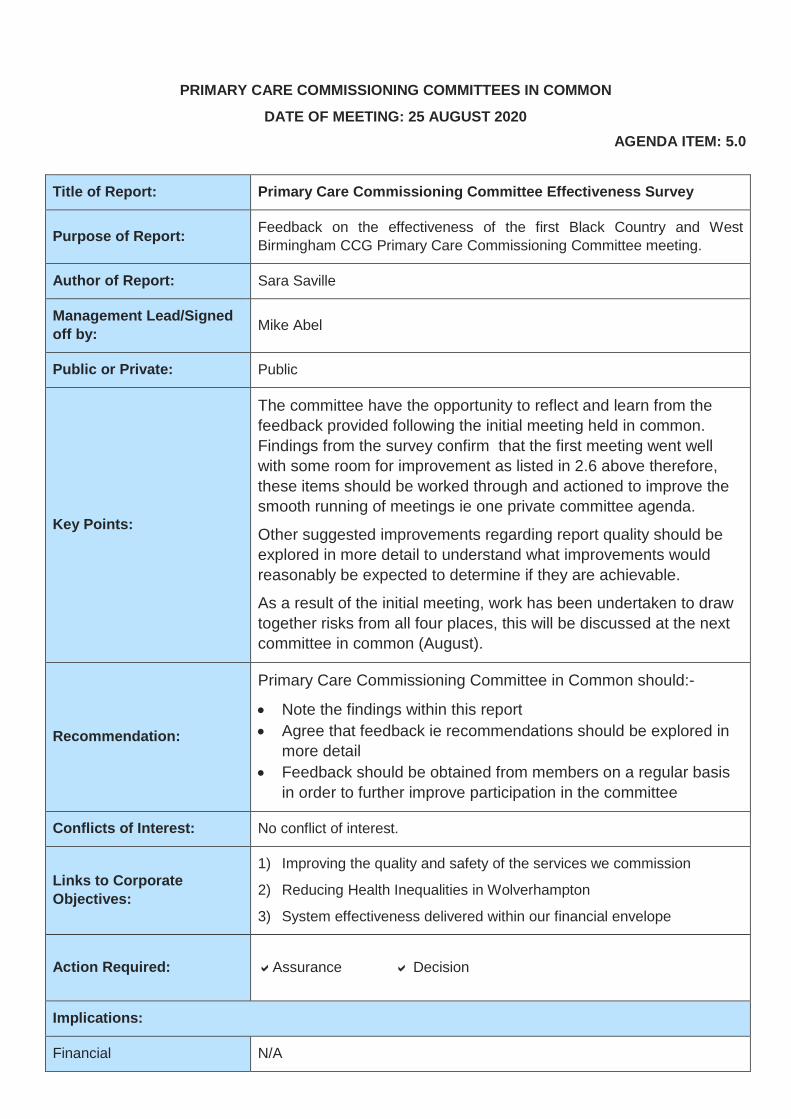
PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: 25 AUGUST 2020 AGENDA ITEM: 5.0
Title of Report: Primary Care Commissioning Committee Effectiveness Survey
Purpose of Report: Feedback on the effectiveness of the first Black Country and West Birmingham CCG Primary Care Commissioning Committee meeting.
Author of Report: Sara Saville
Management Lead/Signed off by: Mike Abel
Public or Private: Public
Key Points:
The committee have the opportunity to reflect and learn from the feedback provided following the initial meeting held in common. Findings from the survey confirm that the first meeting went well with some room for improvement as listed in 2.6 above therefore, these items should be worked through and actioned to improve the smooth running of meetings ie one private committee agenda.
Other suggested improvements regarding report quality should be explored in more detail to understand what improvements would reasonably be expected to determine if they are achievable.
As a result of the initial meeting, work has been undertaken to draw together risks from all four places, this will be discussed at the next committee in common (August).
Recommendation:
Primary Care Commissioning Committee in Common should:-
• Note the findings within this report • Agree that feedback ie recommendations should be explored in
more detail • Feedback should be obtained from members on a regular basis
in order to further improve participation in the committee
Conflicts of Interest: No conflict of interest.
Links to Corporate Objectives:
1) Improving the quality and safety of the services we commission
2) Reducing Health Inequalities in Wolverhampton
3) System effectiveness delivered within our financial envelope
Action Required: Assurance Decision
Implications:
Financial N/A
Assurance Framework N/A
Risks and Legal Obligations N/A
Equality & Diversity N/A
Other N/A
Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Primary Care Commissioning Committee Effectiveness Survey
Primary Care Commissioning Committee in Common Effectiveness Survey
1 Introduction 1. On the 17 July 2020 a survey was created and sent to members to obtain feedback on the
effectiveness of the first Black Country and West Birmingham CCG Primary Care Commissioning Committee meeting.
2 Findings 2.1 Committee members were asked 5 questions assessing both the positive and negatives
from the meeting.
2.2 A total of 27 responses were received from the survey all of which participated in the meeting held 23 June 2020.
2.3 The survey did not highlight attendee’s experiencing difficulties accessing the Primary Care Commissioning Committee meeting via Microsoft Teams.
2.4 When respondents were asked if they thought the Primary Care Commissioning Committee in Common was successful 22 out of 27 responded to say they thought it was successful.
2.5 The following themes were highlighted;
• Committee meeting ran well by the Chair • Discussions were kept in line with the agenda and timings. It was also useful to see each
member who presented a paper. • Well attended and all CCG’s remain quorate • Well-structured and organised meeting • Ability to learn from other CCG’s • Clear succinct presentation of some reports with clear decisions to be made
2.6 When respondents were asked if improvements were required following the Primary Care Commissioning Committee in Common the following themes were heighted;
• Meeting needs to feel less like 4 separate meetings • Conflicts of interest needed to be updated, too much discussion on this item • More succinct reports • Limit to one private agenda • No discussion due to size of the agenda • Managing of comments to allow time for equal input from each CCG • Better reports specifically from Operational groups on Quality & Safety and Contracting. • There was lack of local patient intelligence. • Risk Register not discussed, unbailable for the meeting • Papers and agenda were not easy to follow • Local Committee’s still required • Due to the size of the meeting Committee didn’t demonstrate the application of security • Committee too big unsure the purpose of meeting as no powers. • Some members sat through a presentation/report which was of no relevance to them,
could this not be approved at place level • It was hard for people to contribute especially those from outside organisations
3 Next steps The committee have the opportunity to reflect and learn from the feedback provided following the initial meeting held in common. Findings from the survey confirm that the first meeting went well with some room for improvement as listed in 2.6 above therefore, these items should be worked through and actioned to improve the smooth running of meetings ie one private committee agenda.
Other suggested improvements regarding report quality should be explored in more detail to understand what improvements would reasonably be expected to determine if they are achievable.
As a result of the initial meeting, work has been undertaken to draw together risks from all four places, this will be discussed at the next committee in common (August).
4 Recommendation Primary Care Commissioning Committee in Common should:-
• Note the findings within this report • Agree that feedback ie recommendations should be explored in more detail • Feedback should be obtained from members on a regular basis in order to further improve
participation in the committee
Agenda Item 6.0
Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Virtual Meeting of PCCC Chairs – COVID-19 Red Sites
Date: 13th July 2020
Time: 11:00 – 12:00
Note Taker: Craig O’Keeffe (Business Support, Sandwell and West Birmingham CCG)
Attendees:
Name Role
Dan King (DK) Head of Membership Development and Primary Care, Dudley CCG
Helen Moseley (HM) Lay Member for Patient and Public Engagement, PCCC chair of Dudley CCG
Jackie Bryan (JB) Senior Commissioning Manager, Walsall CCG
Lisa Maxfield (LM, Chair) Deputy Chief Officer (Primary and Community Transformation), Sandwell and West Birmingham CCG
Lorraine Gilbert (LG) Head Of Finance, Wallsall CCG
Mike Abel (MA) Lay Member for Commissioning, PCCC Chair for Walsall CCG
Phil Cowley (PC) Senior Finance Manager, Dudley CCG
Ranjit Sondhi (RS) Vice Chair & Lay Member, PCCC Chair for Sandwell and West Birmingham CCG
Sarah Southall (SS) Head of Primary Care (Wolverhampton CCG) and GPFV Programme Director (BCWB STP)
Sue McKie (SM) Vice Chair/Lay Member, PCCC Chair of Wolverhampton CCG
Notes
Introduction
LM welcomed everybody to the meeting and thanked them for joining the meeting at short notice and introductions were shared.
Red Sites Report
1. LM confirmed a drafted report including recommendations in relation to the future arrangements for Red Sites had been shared with those members present to aid with discussion, it was noted that some members had not received the report until that morning, apologies were shared for the unavoidable late circulation of the paper given the late receipt of some key national guidance necessary to finalising its detail.

PCCC Chairs Virtual Meeting – Red Sites Discussion | 2 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
2. MA queried if it was intended for this report to be shared at the Black Country and West Birmingham Governing Body in Common meeting the following day. It was not thought necessary to submit the report as a separate paper to Governing Body given the recommendations and associated funding fell within the remit of the Primary Care Commissioning Committee.
3. A summary of the background information contained within the report regarding the mandate for and purpose of Red Sites as a part of the COVID-19 outbreak response was shared. NHSE/I had now confirmed that Red Site provision would need to continue.
4. A summary of the current provision formed part of the circulated report, as a part of a review of these current arrangements a number of variations had been highlighted as well as some suggested opportunities through an aligned approach across all 5 places.
5. RS noted the suggested aligned operating times included only weekday access to the services (Monday – Friday) and queried if this was sufficient or should be a 7 day service. It was confirmed that NHSE/I’s expectation was for a Monday – Friday core service provision whilst Primary Care Leads from each CCG confirmed they had been working closely in development of the report and proposed model which had been based upon analysis of available capacity and actual demand in each place. It was noted that although it currently differed between each place (with the example of Walsall CCG’s current provision forming an extension of its extended access / out of hours provision) out of hours provision remained available for those patients who may need it. The role of 111 as first point of contact was highlighted as particularly key, with patients being referred to the appropriate out of hours services where required and appropriate.
6. HM queried if 111 had shared any details around the weekend activity and if this could be a potential pressure for the service. It was noted that no concerns or pressures had been shared from 111 up to that point as a part of regular reporting, Primary Care Leads present also agreed that the capacity of their services had far exceeded the levels of demand experienced which included very minimal appropriate weekend activity, it was noted that further details regarding the rationale and justification for the proposed capacity was included within the report.
7. It was confirmed that it was initially thought that Red Site provision would be separate from GMS core services, although it was noted that recent BMA guidance had confirmed that the provision fell within core GMS services. As such it was expected that all CCGs would be in a position where COVID funding would cease for Red Site provision.
8. PC confirmed that leads had explored different options together but had reached an agreement that it would be potentially destabilising and inappropriate for the funding to be assumed directly by practices and as such were recommending funding from each of the CCG’s delegated primary care budgets be identified with the possibility of top slicing some income guarantees under current COVID arrangements if necessary.
PCCC Chairs Virtual Meeting – Red Sites Discussion | 3 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
9. It was confirmed that the finance teams from each CCG were still exploring this but that they were positive of identifying the £200k per Red Site per place outlined within the report although it was noted that each CCGs had some of their own unique challenges. It was also confirmed that CCGs would continue to reclaim costs from COVID funds for as long as it was possible.
10. MA queried if the BMA advice which had been highlighted as a part of the report had been published in the public domain / was accessible by practices. It was noted that the advice had been shared from Dudley LMC and confirmed that a link was present on the BMA website containing this information, it was agreed that this link would be shared with the group (please find link here).
11. LG outlined a potential challenge faced by Walsall CCG in relation to their current Red Site provider (an external provider operating out of hours) in switching to a normal in-hours provision, it was agreed that there had been variances in models initially given the pace at which the Red Sites were required but the importance of maintaining a consistent approach across all places moving forward was agreed.
12. It was confirmed that as part of the report a breakdown of staffing against available capacity and cost had been provided for three different scenarios (developed through use of appropriate national but also local information and analysis) depending on demand with £200k being the minimum and £380k being maximum required. SM queried how increased funding from the currently proposed £200k would be sourced in the event of a further spike in demand, It was noted that it would be challenging to source the additional funds necessary in the event of an escalation but confirmed that if required an alternative collaborative approach could also be explored. SM also noted that the Wolverhampton PCN Model appeared on the face of it to be a very cost-effective option for a Red Site.
13. LG noted the costing model included within the report included only direct costs for staff for the service provision, it was suggested there could be potential additional costs if services were to be provided by an independent commercial provider such as to support central and organisational overheads.
14. HM further queried the capacity specified as part of the model. It was confirmed that this had been exaggerated and was based on local utilisation information, feedback from clinicians at the red sites and appropriate external information sources.
15. It was noted within the paper that provided hours were recommended to be aligned to 10-6, Monday to Friday and would also require inclusion of a home visiting service. It was acknowledged that home visiting varied across each of the places at present but further work would be conducted to align this in the event of recommendations being agreed.
16. It was noted that current sites had been found to be in a central location within each place representing no longer than a 15-minute drive for patients. It was noted that the current Red Site location within Sandwell was under review given the intention to repatriate the walk in centre currently operating as a Red Site but that location would be a factor in exploration of a new site, work which was underway.

PCCC Chairs Virtual Meeting – Red Sites Discussion | 4 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
17. The recommended timescale for start of the new alignment had been set from 1st August 2020 based upon use of COVID funding for sites ceasing from 31st July 2020.
18. MA shared a concern around the timescale given the highlighted potential challenges faced in Walsall and other areas. It was agreed that implementation within the tight timeframe had been highlighted as a risk during discussions whilst it was noted that given the mandate it would be important to maintain a collective approach and aim for implementation by this date.
19. Following further discussion, it was agreed to retain the 1st August date and revisit this in the event of any significant issues within any place meaning it will be unable to meet the timeframe.
20. MA queried if the clinical chairs of each CCG had been sighted on the proposal. It was acknowledged that discussions had been held with Matt Hartland and Paul Maubach but clarity would be sought if all clinical chairs had been briefed.
21. Recommendations outlined in the report were summarised for confirmation of final decisions:
• Start Date: Launch date of 1st August agreed in principle with any significant issues in any place to warrant further review.
• Provision: 1 Red Site within each 5 places agreed providing it represents a convenient location for all patients in that place (including public transport).
• Staffing Costs: Recommendation for use of normal staffing rates (as supposed to higher time and half rates previously utilised) are adopted for Red Sites in all places.
• Home Visiting: Agreed that home visiting be included within Red Sites service from 1st August.
22. Following query from RS it was noted that each CCG Primary Care Commissioning Committee Chair were in effect agreeing a chairs action and as such decisions would be circulated to respective PCCC members.
23. It was agreed that further updates would be provided via email with the possibility of another meeting being convened if felt necessary.
24. Chairs were thanked for their time and the meeting was bought to a close.

Comparison of PCCC risk register May 2020 Agenda Item: 7.0
CCG Risk description Actions Residual risk rating System/Place Walsall Workforce 4x4=16 S Walsall Estates NHS PS GP leases 4x5=20 S Walsall GP premises 4x5=20 P Walsall GP engagement with PBC 2x4=8 S Walsall GP SI process 3x4=12 P Walsall GP IT 4x3=12 P Walsall Extended hours contract 3x3=9 P Walsall Slippage of town centre dev 3x4=12 P Walsall PCN dev 3x4=12 P Walsall Improve support to PC 2x3=6 P Walsall PC informatics resource 3x4=12 P Dudley Regulatory issues 2x4=8 S Dudley Workforce 4x3=12 S Dudley Estates NHSPS 2x3=6 S Dudley Finance - sustainability 2x4=8 P SWB Regulatory issues 2x4=8 S SWB Measles immunisation 2x3=6 P SWB Financial – Babylon 3x4=12 S SWB PCN dev 3x3=9 S SWB Workforce 3x4=12 S SWB Latent TB 3x3=9 S SWB Social prescribing 2x2=4 P SWB Financial - overspend 3x2=6 S SWB Capacity pressure on individual practice 3x4=12 P SWB Health app uptake 3x3=9 P W’ton PC Counselling service 12 P W’ton Workforce 9 S W’ton Digital first 8 S W’ton Patient Choice 6 P W’ton New ways of working 8 S W’ton Access to estates funding 8 S
PCCCiC Tuesday 25th August 2020
PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: Tuesday 25th August 2020
AGENDA ITEM: 8.0
Title of Report: Application for the merger of Hill Street Surgery, with Grove Medical Practice
Purpose of Report: To inform the committee of the request to merge the 2 practices and to gain committee approval for this to go ahead
Author of Report: Gill Shelley, Primary Care Contracts Manager Management Lead/Signed off by: Sarah Southall
Public or Private: Public
Key Points: • Application received to merge Hill St Surgery with Grove Medical
Practice, both practices hold GMS contracts • Hill Street Surgery is currently working under the umbrella of Grove
Medical practice.
Recommendation: • For the committee to review the information submitted to make a decision with regard to the application.
• For the committee to approve the application Conflicts of Interest: N/A
Links to Corporate Objectives:
Action Required: Approval
Implications:
Financial N/A
Assurance Framework N/A
Risks and Legal Obligations N/A
Equality & Diversity N/A
Other N/A

PCCCiC Tuesday 25th August 2020
1. BACKGROUND AND CURRENT SITUATION
1.1 The following practices have submitted a business case (appendix 1) to the CCG for the merger of Hill Street Bilston (M92003) with Grove Medical Centre (M92612)
1.2 Hill Street Surgery.
Dr’s Mehta and New are partners on the contract
The number of patients registered at this practice is c.1700.
1.3 Grove Medical Practice
Grove Medical Practice has a main surgery at 175, Steelhouse Lane with the following branch surgeries at:
• All Saints Medical Centre, All Saints Road, Wolverhampton • RoseVillas Surgery, Shale Street, Bilston • Caerleon Surgery, Dover Street Bilston • Church Street Surgery, Bilston • Bradley Medical Centre, Hall Green Street, Bradley Bilston • Parfields Medical Centre • Woodcross Surgery
1.4 Grove Medical Practice currently provides medical services to a population of c23,700 patient population
2. Key issues
The proposal as detailed in the business case is to merge the 2 GMS practices
The merged practices will use the current practice code for Grove Medical Practice Centre: M92612
3 Premises and Location of practices.
All current practices are located in the South East Locality of Wolverhampton. Grove Medical Practice is the main surgery in this hub. The distance between Grove Medical Centre and Hill St Surgery is 3.7 miles and 0.2 miles from Bradley Medical Centre.
Appendix 2 shows where the all practice sites are located in relation to the proposed merger
4. Timescales
The merger is dependent on the merging of clinical systems but will be completed by December 2020
PCCCiC Tuesday 25th August 2020
5. Benefits to Patients
5.1 The business case provides full details of benefits to patients but included are:
• Patient choice of clinician will be improved along with continuing access to a female GP and a range of other clinicians and specialist skills.
• All patients will have access to a full range of enhanced services. • Patients can be seen at any practice site.
6 Patient Engagement
6.1 The business case provides full details of the patient engagement process to date.
6.2 Patients have been engaged via the PPG – see appendices 3 – 5
6.3 So far feedback from patients appears to be positive with patients keen to make use the increased patient access and the wider range of health care professionals.
7. CLINICAL VIEW
The view of the clinical partners involved in this scheme is that a larger practice along with a more corporate business structure will allow for the multiple benefits a larger organisation can offer and is detailed in the business case.
8. PATIENT AND PUBLIC VIEW
8.1 To date the views of the patients have been positive
9.0 KEY RISKS AND MITIGATIONS
9.1 There are risks relating to IT/System mergers and data collection issues (QOF) should this merger not be planned within appropriate timescales. To mitigate this risk the merger will be planned to go ahead before December 2020.
9.2 The timescales allow for adequate and appropriate planning for the systems merger
10. IMPACT ASSESSMENT
10.1 Financial and Resource Implications
There are no adverse financial implications to this process
There are resource and finance implications attached to the merger of the clinical systems. The IT team are aware of the proposals and have plans in place and to meet the requirements.
10.2 Quality and Safety Implications
There are no implications for Quality and Safety as long as the planning stages are completed and the merger takes place within the planned timescales
10.3 Equality Implications

PCCCiC Tuesday 25th August 2020
There are no equality implications as there is no change to access for patients to primary medical services
10.4 Legal and Policy Implications
There are no legal and policy implications
10.5 Other Implications
The partners are consulting/engaging with all staff and there are no plans for any reduction in staff numbers and no redundancies are anticipated.
11.0 Recommendation 11.1 The recommendation is that approval is given for this merger, dependent on assurance that the
merger is well planned; timescales are in line with IT workload and can be managed safely with no detriment to patient care during this process.
Name Gill Shelley Job Title Primary Care Contracts Manager Date: August 25th 2020
ATTACHED: Appendix 1. Business Case: Grove Medical Practice Appendix 2. Map of practice sites Appendices 3, 4 &5 notes of PPG/practice meetings

Appendix 1
Health and Beyond
Business Case: Merger of Grove Medical Practice Centre with Hill Street Surgery, Bilston, Wolverhampton, WV14 8SB VERSION 2.1 AUTHOR: DR. RAJ MOHINDROO, JOHN SEYMOUR
2020

Page 2 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
Health and Beyond Partnership
Introduction
Grove Medical Practice is a corporate body which has GMS contracts within the Locality of South East of Wolverhampton. The GMS contracts are held by Grove Medical Practice then the APMS contracts by Health and Beyond Limited.
The GMS sites all are under 1 M Code which are, Grove Medical Practice (main site) and branch sites to include: All Saints Surgery , Caerleon Surgery, Church Street Surgery, Bradley Medical Centre , Parkfields Medical Centre and Woodcross Health Centre, the three AMP practices are Ettingshall Medical Practice, Bilston Urban Village, Pennfields Medical Centre.
Historically, existing GMS practices merged to create this corporate body. Together they have agreed to work together to improve patient experience and to deliver more efficient, effective high-quality services by using the available resources to its optimum.
The aim of these GMS merger was to help patients but also to introduce modern digital practices, patient services, and procedures as this will be beneficial to all the stakeholders of this corporate body. It will benefit the stakeholders in a several ways i.e. enhance the efficiency, enable them to compete and continue in the challenging environment this health-care industry.
The Grove Medical Practice has created a total list size of 36,500 across the 7 GMC sites.
This initial document helps to summaries the recommendations and key proposals that can be used for due diligence of the proposed merger of Hill Street Surgery this is currently held under one contract in the name of Dr B Mehta and Dr N New and the merger into Health and Beyond Partnership.
1. Goal, Vision, Principles
Our Vision is to develop is to merge Hill Street into our GMS Contract allowing us and the patients to benefit from the resources, economies and efficiency of a larger organisation to survive, compete and prosper in the new and evolving competitive landscape, including the Primary Care Network - Wolverhampton South East Collaboration (WSEC), which has the majority of the patient list for that group.
Our aim is to develop cost-effective community solutions by working closely with social care and other community and voluntary sector assets to manage and deliver holistic health and social care. Creating an integrated health and social care ecosystem within Health and beyond and sharing it within the WSEC.
The company already own the Hill Street premises.

Page 3 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
1.1 Core principle
Our core principle is to continue to nurture and preserve all the excellence of traditional GP services. We want local GPs leading and working in local surgeries to provide long-term doctor/patient relationships based on the established values of trust and personalised care, enabling us to improve the range and quality of patient services including, current services provided in secondary care locations at reduced costs, greater access, patient responsiveness and robust organizational learning.
2. Background
Grove Medical Practice, has built up services across a number of locations in Wolverhampton, our current locations are, Grove Medical Practice, All Saints Medical Centre, Caerleon Surgery, Church Street Surgery, Bradley Medical Centre, Parkfield Medical Centre and Woodcross Medical Centre, the two later sites merged in November 2019. Hill Street Surgery will form part of Health and Beyond.
3. Proposed Merger of Hill Street Surgery
Hill Street Surgery sits within WSEC locality PCN. There is a workforce, 3 GP’s including 1 locum and 2 partners, 1 Nurses, 1 Healthcare Assistants, 2 Practice Managers, 5 Admin Staff. The staff have been involved in a number of engagement meetings, over the last 18 months, which has always return positive feedback. Currently the back-office functions are delivered by Health and Beyond Partnership under a Service Level Agreement.
Meetings with the staff have included information around processes should the merger be agreed and their positions moving forward in relation to TUPE and their ongoing employment terms and conditions remaining unchanged. Two of the current GP’s are already partners in Health and Beyond Partnership and Grove Medical Practice.
There have also been a number of engagement meetings with the PPG over the last 18 months all have been extremely positive towards the proposed merger. The PPG openly supporting the merger from day one and see the solution as the only way to move the practice forward in a positive and sustainable way see appendices 3,4,5.
3.1 The new merger plans
Hill Street will slot into a Bilston Hub in relation to administration options but will retain its own clinical identity. However, in line with the Equality Impact Assessment we undertook, that the merger will increase patients’ access across the partnership to a wider range of doctor’s, along with allied healthcare professionals to include ANP’s, MSK and Clinical Pharmacist which has been restricted in the past.
There will be a partnering practice known as Bradley Medical Centre, which is within 600 meters, of Hill Street Surgery, along with extended hour’s availability at Bilston Urban Village some 1.1 kilometers away.
Within the Hill Street merger, we have already performed a due diligence equality impact exercise, which highlights that an improved mix of clinicians will deliver greater equality to the population, in line with the PPG wishes.

Page 4 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
The current Service Level Agreement will no longer apply, with Health and Beyond taking over full control of managerial and administration support.
Hill Street will be included in the current single M code.
Clinical service delivery will remain unchanged and reflect the current services in each of the sites; patients will experience no changes to the traditional practice mechanism and the future proofing of their practice, or a change of name.
In an ever-evolving NHS that is focused on delivering primary care at scale, the partners within the sites feel it was still a good idea to work together and develop clinical services which will benefit the patients. This remains the same concept that led to the idea of mergers between the original three practices, and in the long- term, delivering scaled up primary care services for our patients, which will make Grove Medical Practice more resilient in the longer term.
There will be NO IMMEDIATE CHANGE to service delivery.
4. Health and Beyond Partnership Model
Model 1: Acquisition Model
Health and Beyond board
14 GP partners100% stake (10%
each)
Council/Local Authority Non Voting
Exec
Ambulance/111 /Fire service corporate
partner
Primary Care Network Practice

Page 5 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
4.1 Health and Beyond Strategic SWOT
Health and Beyond
Practices willing to
allow merger /Partnership
H&Bwith new partner will
be an associate partner with shares in the
business. Will continue to be a fixed share partner in the GMS
contract.
Strengths - Ablity to offer high quality services - Enables rationalisation of quality frameworks and policies- Partners are well motivated and are always striving achieve the success of the company. NHS is less expensive that the medical systems which may come into our favour when organizing structures. -According to WHO, we have the best systems with outcomes
Weaknesses - May require extensive ‘soft change management’ to facilitate a new, standardised set of operational and managerial processes and protocols within a newly merged group of personnel- Individual GPs may have less influence in the decison-making process within a large partnership.
Opportunities
- Merging parties do not need to have equal viabilty
- Can offer significant benefits through economic of scale- Can establish joint ventures with other GP, NHS, Social and Heathcare organisations in the future. - There is fragmented healthcare across the globe whereas there is more standardization within the NHS. The NHS PC comes across as an organized system with available systems in place to look at payment models and hence forth could be adapted to the current insurance models too.
Threats- Poor planning and preparation can lead to future spilts following disintergration of relationship- Collaborating with a largers GP organisation can temporarily incur an initial decline in income due to profit sharing arrangements - Substantial risk of losing local connections and continuity with patients if staff become remote or too centralized. There is financial risk to practices if not also incorporating a limited company (in a standard partnership model the individual partners are, unless contrary written agreement dictates otherwise, all equally and personally liable for the liabilities and losses of the partnership they are involved in);
Page 6 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
4.1.1 Legal Process
The legal process has been robust throughout our organization. Our partnership operates in accordance with our written Partnership Agreement which forms part of the governance of the partnership.
Furthermore, we have an extensive Shareholder’s Agreement between our shareholders listing their roles, rights, power’s, and obligations in relation to Health and Beyond Ltd. We have Articles of Associations in place which forms the constitution of the Limited Company which all Shareholders’ must adhere to.
Health and Beyond Limited have a Service Level Agreement (SLA) which sets out that Health and Beyond Limited is the Service Provider for Grove Medical Practice. The SLA also defines the services that the Customer will receive from the Limited Company. The SLA helps to draw a clear distinction and clarity between the two entities.
Quality and Patient Safety
QOF RESULTS
To ensure a high standard is maintained when practice’s merge, they will agree to have a dedicated administrator who will organize by monthly QOF meetings with nurses and GPs to focus on areas where performance is low, develop a practice action plan where the admin will monitor and ensure delivery. The newly formed practice intends to improve nursing capacity by employing an additional nurse.
Practice Name QOF Overall Performance (2017-2018) Grove Medical Practice 98.5%
The data used is from 2018-19 & 2019-20 collected from (http://qof.digital.nhs.uk/search/index.asp)
Quality and Patient Safety
Health and Beyond Ltd Company
Site 1 Church Street
Surgery
Dr. Saini
Dr. Mehta
Site 2AlL Saints
Dr.Praveen Mundlur
Dr.Salma Reehana
Site 3Grove Medical Practice Centre
Centre
Dr.Rajnish Mohindroo
Site 4Caerleon Surgery
Dr.Arshad Asghar
Site 5 Ettinghall Medical
Centre
Site 6Bradley Medical
Centre
Site 7 Bilston Urban Village Hill Street
Dr.Natasha New Dr.Natasha New
Page 7 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
Health and Beyond are adopting new quality improvement methods and factors that promote high and robust quality across both service delivery and safe patients care, our actions are at multiple levels within the health system to nurture and support improvements of quality in general practice.
We have increased the number of members our governance team, not only to include GP’s but also a range of other skills, to match modern day workings across both our on-going growth and promote new reassurance to patients and commissioners.
We are making commitments to building a culture and capability to support continual quality improvement, which includes validate our vision and values by ensure practice teams to actively embrace an ethos of putting patients first and seeking to provide excellent care, involving every member of staff in the mission of continually improving care, and valuing and incorporating patients in measuring and improving their care.
Quality improvement flourishes best in a culture that promotes: engaging and empowering all staff in measuring, understanding and improving quality accountability for improving, employing openness about performance and variability and incorporating rewards and penalties continual, rather than periodic, improvement, where improvement contributes to the fabric of the practice and is a part of every person’s working day.
Effective leadership in a practice does not necessarily have to be given by a doctor, but it must be acceptable and effective for all staff. Adopting structures that value the contribution of all disciplines may sometimes involve non-medical partners – a move that a growing number of practices are finding helpful to fulfil ongoing improvement.
We are adding several clinical posts to our team; these include additional Clinical Pharmacists, Advanced Clinical Practitioners, and First Contact Practitioners, over the next three months. Working towards on development of First Contact Physiotherapy (FCP) service within Health and Beyond which view of extending it to larger MSK service consisting of multidisciplinary team of professionals involved in providing Physiotherapy/MSK/T&O/Rheumatology/Pain Management services.
With the NHS Long Term to development of new ways of working in primary and community will increase the focus on safety. We believe the inclusion and development of integrated care pathways with new types of clinicians in primary care and with patients moving seamlessly between primary, community care services is an opportunity for local systems as described above will develop robust clinical governance with clear lines of accountability for safer and bespoke care.
Our new primary care network gives us the opportunity to promote a robust safety culture couple with continuous quality improvement around patient safety in primary care. We see the role of the PCN clinical director will be developed to ensure the right expertise is in place to facilitate this within the group to support the new safety ascendancies.
These changes to improving the quality and safety of care across Health and Beyond, while meeting the demands of a more outcomes-based performance framework, together with the regulatory requirements of Commissioning Boards and Care Quality Commission. Making greater time commitments to patients in such a way we can use and adapt quality concepts of continual improvement, imparting practical skills, and the coaching of staff
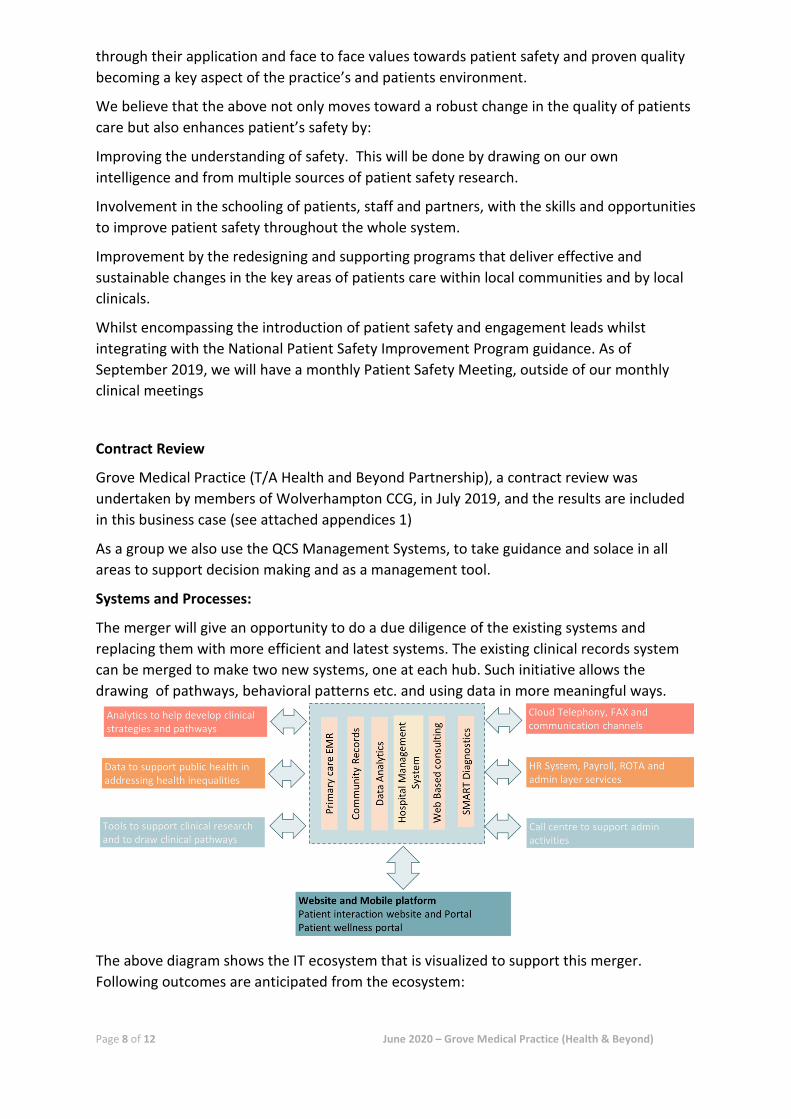
Page 8 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
through their application and face to face values towards patient safety and proven quality becoming a key aspect of the practice’s and patients environment.
We believe that the above not only moves toward a robust change in the quality of patients care but also enhances patient’s safety by:
Improving the understanding of safety. This will be done by drawing on our own intelligence and from multiple sources of patient safety research.
Involvement in the schooling of patients, staff and partners, with the skills and opportunities to improve patient safety throughout the whole system.
Improvement by the redesigning and supporting programs that deliver effective and sustainable changes in the key areas of patients care within local communities and by local clinicals.
Whilst encompassing the introduction of patient safety and engagement leads whilst integrating with the National Patient Safety Improvement Program guidance. As of September 2019, we will have a monthly Patient Safety Meeting, outside of our monthly clinical meetings
Contract Review
Grove Medical Practice (T/A Health and Beyond Partnership), a contract review was undertaken by members of Wolverhampton CCG, in July 2019, and the results are included in this business case (see attached appendices 1)
As a group we also use the QCS Management Systems, to take guidance and solace in all areas to support decision making and as a management tool.
Systems and Processes:
The merger will give an opportunity to do a due diligence of the existing systems and replacing them with more efficient and latest systems. The existing clinical records system can be merged to make two new systems, one at each hub. Such initiative allows the drawing of pathways, behavioral patterns etc. and using data in more meaningful ways.
The above diagram shows the IT ecosystem that is visualized to support this merger. Following outcomes are anticipated from the ecosystem:

Page 9 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
• Two clinical systems one at each hub. • Setting up a call Centre where in the patient can call to book appointments, order
repeat prescriptions and to sign post the patients etc., it is hoped that this will be in place January 2021.
• A single system known as Rota Master is already being used to manage the HR, Payroll including staff ROTA.
• New telephony systems are already in place which can cater for all our current sites which Hill Street is included in with multiple lines with automated call handling facility
• Introduction of analytics tools which will enable to enhance the patient care, social care, and community care.
• One website which will have information for patients and enable them to access relevant healthcare apps.
• Provision of web consultation to be integrated to the website • Tools for Inventory management, budget management etc. • Insurance sector support integration
Finance analysis:
The merger will garner a combined income of GBP 7.7 million per annum. Looking at law of averages and economies of scale the combined expenditure can vary.
Advantages and outcomes of Merger
i) For Patients: • Centralised patient appointment booking facility through call Centre. • Implementation of longer opening hours to accommodate more patients in a day. • Value-added Patient care from a modern, fit for purpose building with modern
facilities. • Access to experienced primary care health team with an excellent skill mix. • Patients will have increase in access and more flexibility in terms of appointment
times and choice of clinician. • Provision of enhanced services and community-based services as well as continuing
to maintain high QOF achievement to maximize quality of service provision for patients.
• Focus upon long term conditions, developing and maintaining care plans for patients and ensuring access to the appropriate services for these patients.
• Provision to deliver enhanced services such as minor surgery and family planning for the patients.
• Continued enhanced services from the WSEC
ii) For Stakeholders: • Enhanced buyer power. This merger will give the partnership the power to bargain
and get the best prices from suppliers. • Centralised admin team reducing admin burden.

Page 10 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
• Integrated services to be delivered through common premises to ensure the sharing of good practice and a consistent approach to the delivery of high-quality care.
• Guaranteed cost saving using unified and better systems, moving completely to digital and reducing paper administration.
• Proper exit strategy for partners who want to retire. • Development of new innovative care pathways which will work at the interface of
social and healthcare system. • Proposal of incorporation of two existing pharmacy units at each proposed new hub
which will be a value-add service and will provide rental for such initiative which is and added advantage.
• Discussion with private insurance providers/insurers to facilitate private clinical work and insurance work.
• Enhanced services from the WSEC
Equality Analysis – Proposed Merger between Grove Medical Practice with Hill Street Surgery
EQUALITY IMPACT ASSESSMENTS (EIA)
We have a legal responsibility to assess how they will monitor any possible negative impact on (age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex and sexual orientation) equality, whilst promoting good relationships among communities.
The key purpose of our Equality Impact Assessment is to:
• Promote all aspects of equality.
• Identify whether certain groups are excluded from any of our services.
• Identify any direct or indirect discrimination.
• Assess if there is any adverse (negative) impact on groups.
• Promote good relations between people of different equality groups.
• Act as a method to improve services.
Other reasons for our Equality Impact Assessments are:
• It increases user/public/staff trust.
• It enhances value for money.
• It informs business plans.
• It increases social inclusion.
• It promotes understanding and sensitivity.

Page 11 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
Equality Impact Assessment should not be a separate exercise for Managers to undertake. It should be built in as an integral part of continuous service and performance review. Assessing for equality impact is an aspect of delivering service improvements. For some of the services, equality considerations may already be well integrated into service planning and review. The Equality Impact Assessment Process will simply enable services to document equality deliberations and conclusions and show transparency and accountability to the wider community.
As both parties are existing providers of services for patients for some years in close proximity to areas that form part of the South East locality of Wolverhampton CCG, we have identified several groups who have cosseted characteristics by analysis of our combined patient data. We as an organisation will ensure that due regard is given to the needs of our patient population during the said service mergers, including that of vulnerable groups, through effective engagement aligned with the profile of those possible affected by such changes.
1) Age: Older people preferred to see their named GP coupled with a regular Nurse and Health Care Assistant, which is dealt with within our workforce planning and recruitment, in the case of locums, we will be using affiliated GP’s to the practice, and of course the current partners to ensure continuity of care, which is key to this proportion of the population. In the case of the merger then all clinicians will be available across the locality thus meeting the patient’s wishes and supporting an allaying their anxiety.
2) Disability: Carers and people with disabilities were concerned primarily about journey times, the difficulties of getting on and off buses, ample disabled parking facility and access within practices including vulnerable groups. Carers of people with Learning Disabilities were concerned about a lack of understanding of the impact of intellectual disabilities that relate to their charges and their on-going illness e.g. pain control. They preferred to request a visit from their own GP due to issues with access. People with mental health problems were described as finding busy practice environment as an issue. We have protected supervised area for patients to discuss or sit and wait if they had severe and enduring mental illness which needed urgent medical appointment and plan to develop inclusive, supportive values and competencies across this sector. This has been considered when looking at the merger and having 7 sites within the South East of Wolverhampton CCG and each site have proximity to at least one other. There is a mixture of sites facility both which matches the needs identified in this analysis and in fact the merger gives improved access by public transport and has improved general parking and disabled parking across the 7 sites.
3) Gender reassignment: We have limited numbers to undertake an analysis current across the group, all requests are dealt with in line with the equality act 2010 in relation to gender dysphoria a plan to develop inclusive, supportive values and competencies across and currently sit with one GP at a single site, who has two patients looking to pursue GR.
4) Pregnancy and maternity: pregnant and expectant mothers prefer to see midwife’s in practices, therefore avoiding unnecessary drawn out hospital journeys. There is also preference to see a female GP who has special interest in women’s health. The merger will enhance this with great access across the locality and the the opportunity of seeing a female
Page 12 of 12 June 2020 – Grove Medical Practice (Health & Beyond)
doctor. With a viable appoint scheduled to match patient’s needs, which will include a request for a great depth of information and consistency which many younger mothers feel is missing and increasing concerns around Pre-eclampsia. The merger of Hill Street Surgery will increase the female population by around 798
5) Race: We found little to differentiate minority ethnic experiences within our local practices have an absolute majority of white British. There was a sense from some professionals that people from ethnic minorities had language and cultural barriers to access and needed longer appointment times creating a wait in the waiting room, there is very little if any evidence to support this statement. When auditing the clinical system there was no differential between timings, the main difference was around presenting conditions. Our population demographics by race show that 96% of the population is white, with White British at 94% and the remaining being Eastern European. Over 1.66% patients are South Asian and are mainly Indian Punjabi, with 2% split mixture of races.
6) Religion or belief: The South Asian population is mainly split between Sikhism, Muslim or Hindu, Christian was the highest and the remainder very low numbers but 43% registered as having no religious beliefs.
7) Sexual Health: We found no differentiation between the reported experience of men and women, except for females in many cases preferring female GP’s, following the merger there will be more availability for patients to see female doctors.
8) Sexual orientation: No specific issues for this group.
9) Civil Partnerships and Marriage: all our current staff are trained and have mandatory equality training which if not in will be extended to new staff allowing for everyone to be treat without any prejudice, we offer impartial accessible and equitable services to all patients.
10) Access to Services (opening times), is a topic that always divides young, old and carers and those that work and those that do not, to bridge this gap against normal opening times within our practices that are in close proximity to areas that form part of this merger, we have extended hours that cover five nights to 8pm, Saturday and Sunday 8am to 12.30pm from Bilston Urban Village and that gives additional appointments beyond the national average set against patient lists.
We have ensured that we have the right clinical skills in our practice’s to meet the diverse needs of our patients, including those with protected characteristics, such as dermatology, diabetes, respiratory disease-asthma and COPD, child health surveillance, minor surgery , orthopedics, rheumatology, mental health, dementia, obstetrics, gynecology and cardiology. We also have strong values around safeguarding both in adult and children areas. Our entire clinical workforce will interchange within our sites to maximise and provide such skills locally, whilst promoting community healthcare, and providing familiar faces with admin staff, doctors across South East locality of Wolverhampton CCG and the WSEC. The rationalization will also offer a larger range of services to patients that was previous the case with prior to the newly proposed merger.

Appendix 2 Grove Medical Practice: Practice sites
All Saints Surgery
Grove Medical Practice
Parkfields Medical Practice
Church Street Surgery
Bradley Medical Centre
Hill Street Surgery
Woodcross Surgery
Appendix 3
Hill Street PPG
Friday 24th July 2020
Agenda
1). Discuss with patients their wellbeing during the pandemic.
2). Merger between Hill Street and Health and Beyond will still go ahead but has been delayed by the Covid 19 situation.
3). Recap from last meeting about new services such as in-house pharmacists, female GP and counselling services
4). Recap on PCN and what it involves.
5). Staff will all be remaining the same with introduction of HR team to utilise space in the surgery.
6). General chat and feedback.
7). AOB
8). Date of next meeting
Appendix 4
Hill Street PPG
Friday 24th July 2020
Minutes
Due to the current covid 19 situation this agenda is based upon telephone calls to the patients rather than video link or face to face meetings. The patients were given the option of Microsoft Team but were not willing to use this or do not have smart phones or email address.
Patients chatted/discussed with:
Paul Edwards, Jennifer Hayfield, Deidre Stevens, Patricia Weeks, Gaynor WQeeks, Doreen Burbridge, Peter Phillips. Oliver Beery, Linda Preece, Brian Preece, Stephen Artess, Margaret Artess, Mavis Durnell. Patricia Blakemore.
I called each patient to catch up following the previous meeting in February.
I discussed with everyone how they had been during the lockdown or shielding period.
I informed them the merger between Hill Street and Health and Beyond had been delayed due to the Covid 19 situation but would still be going ahead as planned. I reminded them of the services that will be available such as later appointment times. A female GP. In house pharmacists for medication reviews.
We also discussed PCN and the extra services such as physio and counselling held at a local site. Also the evening and weekend appointments.
I did reassure the patients that there will be no staff changes at Hill Street and our HR team have been deployed there to utilise the space they have free.
I chatted with each patient who gave me their feedback which is very positive about the services available.
They asked questions about where they can have their bloods taken and will we remind them when it is flu season and any reviews they may be due.
I did reassure them that this would happen and we would be in touch and advice of any changes.
All patients were happy and appreciative of the call and no complaints or concerns to the services.

Appendix 5
Patient Participation Meeting
11th February 2020
Patient’s Attending Meeting: P. Edwards, J. Hayfield, D. Stevens, P. Weeks, G. Weeks, D. Burbridge,
P. Phillips, O. Berry, L. Preece, B. Preece.
Staff: Dr. Mehta, Anita Small, Nita McElroy, Jackie Griffiths (minutes).
Apologies: S. Artess, M. Artess, M.Durnall, P. Blakemore.
1. Anita opened the meeting by introducing herself to everyone; she works across eleven Health & Beyond surgeries in the Wolverhampton area which are all part of the NHS.
2. Doctor Suryani left the Hill Street practise in December 2019, so a merger had taken place over the previous few months, which meant that Dr Mehta and Dr New were the new partners until Dr Suryani left, Dr Cheema who also works at Hill Street as a locum Doctor, will still continue to work two days a week.
3. Health & Beyond which have 10 surgeries across Wolverhampton (South East) and 54,000 patients will be the new team that will also include Hill Street surgery. This will offer patients much more flexibility in future. Hill Street patients already, can book via reception for weekend and evening appointments up to 8pm at night at the Urban Village surgery opposite Morrison’s Bilston. Hill Street opening hours will remain the same which are 8.30 am to 6.30pm every day Monday to Friday.
4. Anita and Dr Mehta explained to the meeting about the PCN, of which Health and Beyond is part of, this is a government funded project that offers better services for practises that have 30,000 or more patients.
The other surgeries which all form part of Health and Beyond Wolverhampton East are, Bilston Urban Village, Bradley Medical Centre, Parkfields Medical Centre, Woodcross Medical Centre, Bilston Urban, Ettingshall Surgery, All Saints Surgery, Grove Medical Practise, Caerlon Surgery, Church Street, Surgery and Pennfields.
5. Some services such as Physiotherapy, Musk skeletal. H.C.A. Vaccinations, could be offered in different surgeries which Health and Beyond, Wolverhampton East already run, so Hill Street Doctors for you patients can choose rather than patients going to hospital and facing lengthy clinic waits, parking problems etc., if the services are available or nearer, more convenient for each patient and H & B already has these links it can only be better for everyone concerned.

Appendix 5
6. Receptionists are requested to ask patients for further details if no appointments are available any time, or on that particular day, so as the details can be passed onto Doctor and the decision can then be made to signpost each individual person to the correct clinician. However if the patient cannot speak to reception about their problem a message can be given to Doctor and the next available appointments will also be offered also.As from April the 1st the phone and computer network will change, staff will be given training on this before it happens. Repeat Prescriptions will no longer be accepted over the telephone, you may still come into Hill Street and order in person at reception or put your slip in the box, or you may organise this with the pharmacy you choose. The main reason for this is safety verbally over the phone mistakes can happen this cannot be allowed to happen, as it is dangerous for both staff and patients alike.
Repeat Prescriptions will no longer be accepted over the telephone, you may still come into Hill Street and order in person at reception or put your slip in the box, or you may organise this with the pharmacy you choose. The main reason for this is safety, verbally over the phone mistakes can happen this cannot be allowed to happen, as it is extremely dangerous for all concerned.
Also the phone system gets very clogged up for prescriptions so the new system will be on a menu where you will automatically asked to press which service you need, this can be frustrating but necessary as the calls then can be given priority of need.
7. If patients would like to get on-line access please ask at reception and this can be arranged for each patient as requested.
Dr Mehta said once Hill Street has been integrated in April, although the system will be frozen over the weekend and records may be a bit delayed coming through and we will need a little time to get, organised as long as we all communicate properly the advantages for better services will hopefully out way the changes. No one likes change and we all appreciate how difficult it must be when you patients have used this surgery for decades in some cases.

PCCCiC Tuesday 25th August 2020
PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: Tuesday 25th August
AGENDA ITEM: 9.0
Title of Report: Primary Care Contracting Report
Purpose of Report: To inform PCCCic of change to the Extended Access Specification and to request approval for the changes
Author of Report: Jo Reynolds Management Lead/Signed off by: Sarah Southall
Public or Private: Public
Key Points:
There have been amendments to last year’s specification, to reflect the additional restraints and demands of COVID response. Networks have been given a number of options in order to flex the additional capacity that is built into this specification locally. There is an additional 15 minutes over the national requirement that is commissioned, therefore PCNs can remodel their delivery to support the restoration and recovery that is required. This is demonstrated in section 3.4 of appendix 1
Recommendation: Approval
Conflicts of Interest: N/A
Links to Corporate Objectives:
Action Required: Approval
Implications:
Financial N/A
Assurance Framework N/A
Risks and Legal Obligations N/A
Equality & Diversity N/A
Other N/A

Appendix 1
1
SCHEDULE 2 – THE SERVICES
A. Service Specifications This is a non-mandatory model template for local population. Commissioners may retain the structure below, or may determine their own in accordance with the NHS Standard Contract Technical Guidance.
Service Specification No.
Service Extended Access 2020/21
Commissioner Lead Jo Reynolds
Provider Lead
Period March 2020/21
Date of Review December 2020
1. Population Needs
1.1 National/local context and evidence base The General Practice 5 Year Forward View, published in April 2016, committed to improve patient care and access, and invest in new ways of providing care. The General Practice Forward View provides the support for practices to build the capacity and capabilities required to meet these needs, including support to adopt new ways of working (at individual, practice and network or federation level) and to develop different ways of managing clinical demand. In addition to increasing self-care, this includes the use of different triage methods and development of the broader workforce, or alternative services. since 2018/19 there has been a requirement for practices to provide appointments 8-8 weekdays and availability weekends and bank holidays through the General Practice Five Year Forward View. This has been superseded by the NHS Long Term Plan, which continues to build on the work to improve access for patients through working as part of Primary Care Networks, through digital transformation and the delivery of Extended Access. Extended access arrangements continue to be facilitated through Hub working and delivery agreements between PCNs, with practices sharing booking processes and patient records under data sharing agreements using EMIS systems to enable functionality and cross site working.
Extended access 2020/21 recognises the need to continue to meet the national requirements, to support capacity within the system, to be flexible and meet the needs of our population.
2. Outcomes

Appendix 1
2
2.1 NHS Outcomes Framework Domains & Indicators
Domain 1 Preventing people from dying prematurely Domain 2 Enhancing quality of life for people with long-term
conditions √
Domain 3 Helping people to recover from episodes of ill-health or following injury
Domain 4 Ensuring people have a positive experience of care √ Domain 5 Treating and caring for people in safe environment and
protecting them from avoidable harm √
2.2 Local defined outcomes
The following outcomes are taken from the CCG Primary Care Strategy • promote the health and wellbeing of our local community • ensure that our population receive the right treatment at the right time and in the
right place • reduce early death and improve the quality of life of those living with long term
conditions; and • reduce health inequalities • Access to a range of standard primary medical services 8am to 8 pm 7 days a week
through a combination of GP practice, extended Hours and Out of Hours Services provision with full access to a patient’s notes irrespective of how or where access occurs.
3. Scope 3.1 Aims and objectives of service The purpose of extended access is to ensure patients have easier and more convenient access to GP services, including appointments at evening and weekends. These need to be routine, pre-bookable and urgent on the day to enable patients to access in a timely and appropriate manner.
Extended access is part of the wider transformation of Primary Care, which aims to provide sustainability in general practice, while improving patient care and access and investing in new ways of providing care.
The General Practice Forward View set out plans to enable clinical commissioning groups (CCGs) to commission and fund additional capacity across England to ensure that, by 2020 everyone has improved access to GP services including sufficient routine appointments at evenings and weekends to meet locally determined demand, alongside effective access to out of hours and urgent care services. 3.2 Service Description and Care Pathway

Appendix 1
3
In Wolverhampton there is already a successfully supported extended access scheme in place across the Primary Care Networks, providing 45 minutes consultation capacity per 1000 patients. This will need to continue to be provided in line with the core requirements as outlined below.
The additional clinical appointments provided by a PCN are to be held at times that take account of patient’s expressed preferences and are outside the hours that the PCN Core Network Practices’ are required to provide as part of their primary medical services contracts.
Access will be provided at scale, within locality based networks. Networks may offer a wider array of services through extended access appointments and these may be particularly beneficial for patients with complex issues. Networks help to create opportunities for greater skill mix and evidence suggests that primary care at scale is better for staff development through working across areas with a greater number of patients.
Geographical locations of extended access hubs will need to be in line with Primary Care Networks and locality based modelling, to ensure equality of access for patients across the city. Planning for the hubs will need to be within the most deprived areas and based on population need, to improve access for those that need it the most. 3.3 Core Requirements The following requirements are essential to the effective delivery of access and the overall patient experience and will be monitored and enforced both locally and nationally. In order to be eligible for funding, practices need to be able to demonstrate they are meeting the seven core requirements.
Timing of appointments: Patients will need to have access to pre-bookable and same day appointments for 8am- 8pm weekdays, weekends and on bank holidays that meet local population needs. Times outside of core practice hours will need to be covered by extended access appointments within the network, as well as any need identified for in hours provision. Appointments can be both in hours and out of hours, as long as the service is accessible for the durations stated above. Some appointments can be provided in core hours if supported by evidence of need, taking into consideration population and demand for types of appointments. Appointments can be utilised to aide PCN development, either to support the delivery of PCN specifications or in the delivery of specialist clinics, that have been identified through patient demand. This is an opportunity for community based clinics to be held, in collaboration with secondary care.
Advertising and ease of access All practices are responsible and will be required to advertise the availability of extended access appointments. It needs to be clear to patients how they can access these appointments and associated services. This includes but is not restricted to-
• All practice receptionists able to direct patients to the service and offer appointments to extended hours service on the same basis as appointments to non-extended hours services. Patients should be offered a choice of evening or weekend appointments on an equal footing to core hours appointments.
• Patients have the ability to cancel appointments, up to the day of the appointment.
• Practice websites display current, up to date information regarding appointments and how to access them on the home page. This needs to be clearly visible, easily accessed and accurate. Practices are recommended to place a promotional banner on the practice website advertising

Appendix 1
4
any new or extended services and the times they are available. A template web banner is available at www.england.nhs.uk/gpaccess.
• NHS choices will also need to reflect access to additional appointments, in the overview / out of hours section.
• Notices need to be in place in local urgent care services, community venues and publically within other community locations e.g. pharmacies, supermarkets, places of worship etc.
• Patient participation groups should be encouraged to support promotion of the service.
Digital
Under the NHS Long Term Plan, digital-first primary care will become a new option for every patient improving fast access to convenient primary care. Use of digital approaches, such as online consultation, apps for smart devices and two way texting, will need to be utilised within extended access provision. This will support patient access and will be pivotal to the success of working at scale. Suitable and sufficient interoperability within clinical systems to enable information sharing must be in place for practices and patients to benefit from these technologies. Patients must be able to see a GP face to face, but other appointment types can be offered to complement this. Through planning the makeup of different appointment types will form part of the arrangements.
Inequalities
Practices will be required to demonstrate that they have not only involved patients in the delivery plan but also on an ongoing basis demonstrate how they have collected and reviewed patient feedback. This will of course assist them in identifying early indications of patient satisfaction levels and areas that may require change/ intervention. Any inequalities in patients experience can then be identified as an early warning and addressed.
Practices will need to demonstrate that an assessment of population requirements has taken place, and that work has been done to identify and plan pathways for vulnerable patients. Equality of access needs to be in place for all patients, and adjustments need to be demonstrated. Practices should, as a minimum, ensure that Networks are placed in areas with the greatest needs (i.e. poorer health outcomes) and monitor utilisation to ensure that key groups are not excluded.
Effective access to wider whole system services
The planning of appointment type will enable patients to access the most appropriate professional/service within the practice team and/ or via social prescribers that will be readily available in the city. Pathways for referrals to other professionals will be part of access working, with patients receiving the same level of service as with a routine appointment. This will support effective connection to other services enabling patients to receive the right care at the right time in the right place. Integration with 111, including direct booking, will also need to be in place to support urgent care.
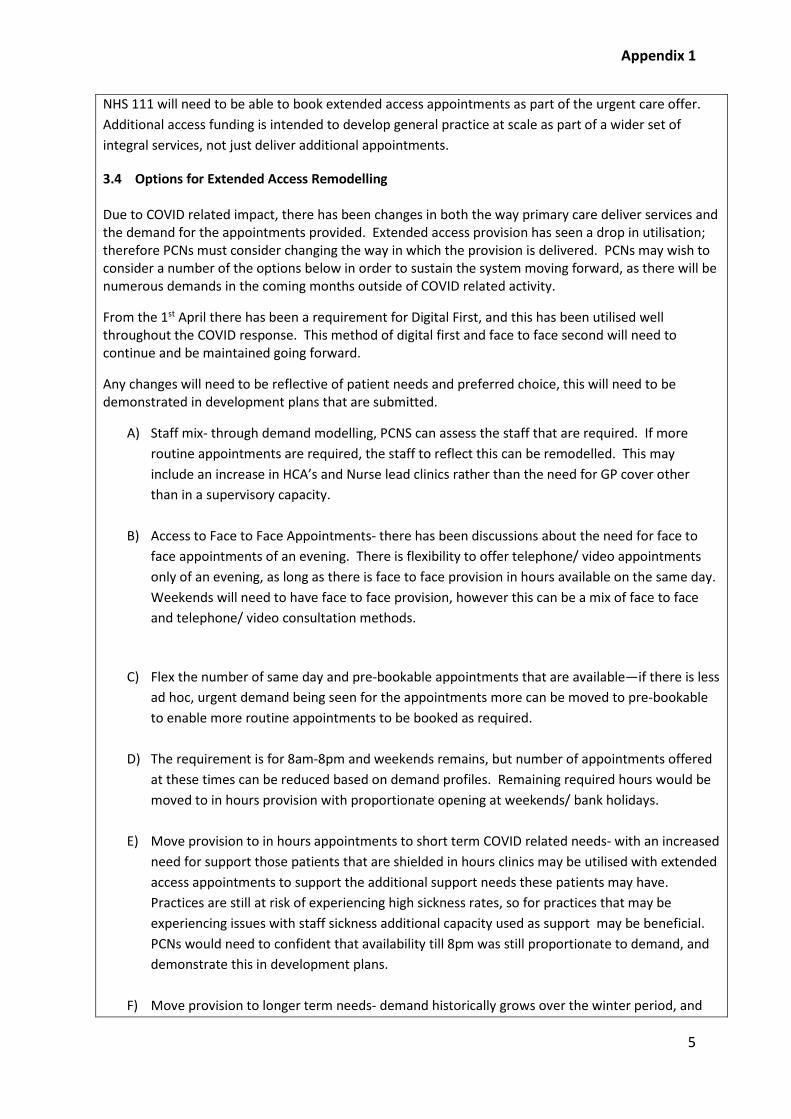
Appendix 1
5
NHS 111 will need to be able to book extended access appointments as part of the urgent care offer. Additional access funding is intended to develop general practice at scale as part of a wider set of integral services, not just deliver additional appointments.
3.4 Options for Extended Access Remodelling Due to COVID related impact, there has been changes in both the way primary care deliver services and the demand for the appointments provided. Extended access provision has seen a drop in utilisation; therefore PCNs must consider changing the way in which the provision is delivered. PCNs may wish to consider a number of the options below in order to sustain the system moving forward, as there will be numerous demands in the coming months outside of COVID related activity.
From the 1st April there has been a requirement for Digital First, and this has been utilised well throughout the COVID response. This method of digital first and face to face second will need to continue and be maintained going forward.
Any changes will need to be reflective of patient needs and preferred choice, this will need to be demonstrated in development plans that are submitted.
A) Staff mix- through demand modelling, PCNS can assess the staff that are required. If more routine appointments are required, the staff to reflect this can be remodelled. This may include an increase in HCA’s and Nurse lead clinics rather than the need for GP cover other than in a supervisory capacity.
B) Access to Face to Face Appointments- there has been discussions about the need for face to face appointments of an evening. There is flexibility to offer telephone/ video appointments only of an evening, as long as there is face to face provision in hours available on the same day. Weekends will need to have face to face provision, however this can be a mix of face to face and telephone/ video consultation methods.
C) Flex the number of same day and pre-bookable appointments that are available—if there is less ad hoc, urgent demand being seen for the appointments more can be moved to pre-bookable to enable more routine appointments to be booked as required.
D) The requirement is for 8am-8pm and weekends remains, but number of appointments offered at these times can be reduced based on demand profiles. Remaining required hours would be moved to in hours provision with proportionate opening at weekends/ bank holidays.
E) Move provision to in hours appointments to short term COVID related needs- with an increased need for support those patients that are shielded in hours clinics may be utilised with extended access appointments to support the additional support needs these patients may have. Practices are still at risk of experiencing high sickness rates, so for practices that may be experiencing issues with staff sickness additional capacity used as support may be beneficial. PCNs would need to confident that availability till 8pm was still proportionate to demand, and demonstrate this in development plans.
F) Move provision to longer term needs- demand historically grows over the winter period, and
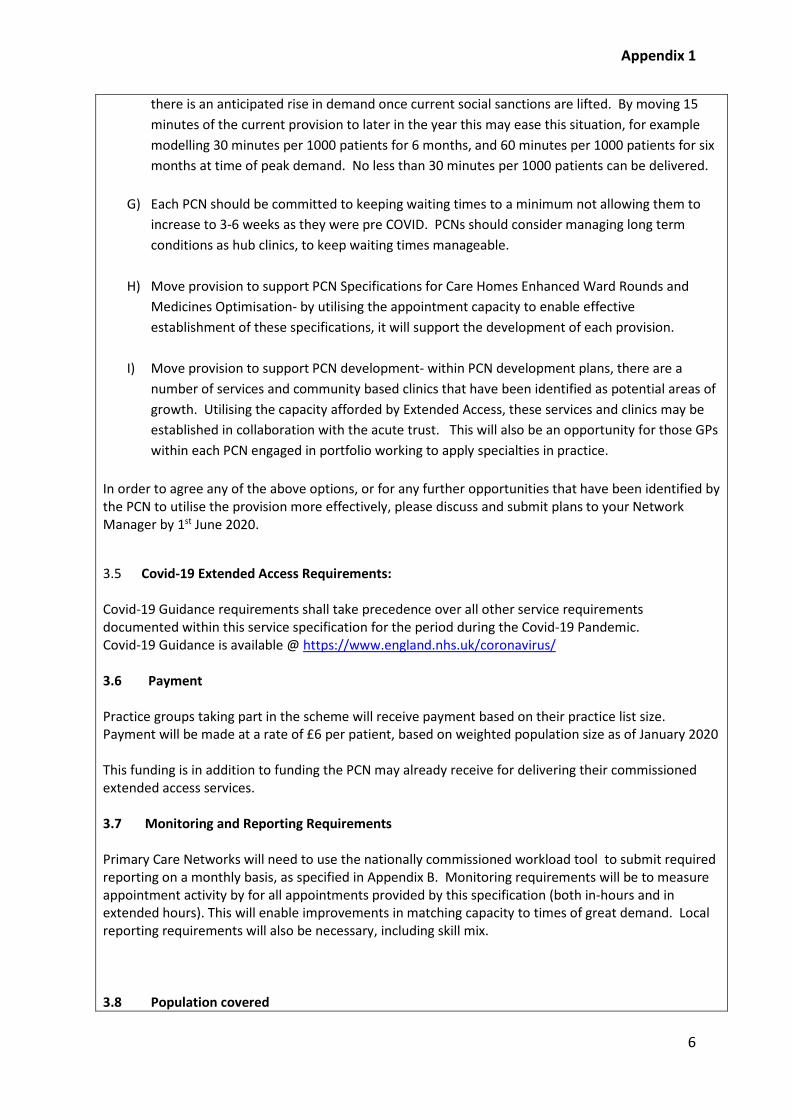
Appendix 1
6
there is an anticipated rise in demand once current social sanctions are lifted. By moving 15 minutes of the current provision to later in the year this may ease this situation, for example modelling 30 minutes per 1000 patients for 6 months, and 60 minutes per 1000 patients for six months at time of peak demand. No less than 30 minutes per 1000 patients can be delivered.
G) Each PCN should be committed to keeping waiting times to a minimum not allowing them to increase to 3-6 weeks as they were pre COVID. PCNs should consider managing long term conditions as hub clinics, to keep waiting times manageable.
H) Move provision to support PCN Specifications for Care Homes Enhanced Ward Rounds and Medicines Optimisation- by utilising the appointment capacity to enable effective establishment of these specifications, it will support the development of each provision.
I) Move provision to support PCN development- within PCN development plans, there are a number of services and community based clinics that have been identified as potential areas of growth. Utilising the capacity afforded by Extended Access, these services and clinics may be established in collaboration with the acute trust. This will also be an opportunity for those GPs within each PCN engaged in portfolio working to apply specialties in practice.
In order to agree any of the above options, or for any further opportunities that have been identified by the PCN to utilise the provision more effectively, please discuss and submit plans to your Network Manager by 1st June 2020.
3.5 Covid-19 Extended Access Requirements: Covid-19 Guidance requirements shall take precedence over all other service requirements documented within this service specification for the period during the Covid-19 Pandemic. Covid-19 Guidance is available @ https://www.england.nhs.uk/coronavirus/ 3.6 Payment Practice groups taking part in the scheme will receive payment based on their practice list size. Payment will be made at a rate of £6 per patient, based on weighted population size as of January 2020 This funding is in addition to funding the PCN may already receive for delivering their commissioned extended access services. 3.7 Monitoring and Reporting Requirements Primary Care Networks will need to use the nationally commissioned workload tool to submit required reporting on a monthly basis, as specified in Appendix B. Monitoring requirements will be to measure appointment activity by for all appointments provided by this specification (both in-hours and in extended hours). This will enable improvements in matching capacity to times of great demand. Local reporting requirements will also be necessary, including skill mix. 3.8 Population covered

Appendix 1
7
All patients registered with a practice in Wolverhampton will need to be able to benefit from the interventions proposed for the funding to be accessed. Combined with the core standards, every effort must be made at network level to prevent inequalities for patients registered with Wolverhampton practices. 3.9 Any acceptance and exclusion criteria and thresholds Practices must be open during core hours (between the hours of 8:00 am and 6:30 pm) as part of their standard contract. Practices that regularly close for half a day on a weekly basis will not ordinarily qualify for the DES. Practices must ensure they are open with a level of reception and medical cover also available. Practices should be offering a minimum of 70 appointments per 1000 patients per week, where this is not being achieved an improvement trajectory will be required to achieve the standard within the financial year. 3.10 Interdependencies with other services/ providers Close liaison between the commissioned out of hours provider, 111 provider and GP access Networks should be maintained. There will be a nominated point of contact for both clinical and non clinical issues, to represent each network. They will liaise on all matters pertaining access ie Clinical Director & a nominated Practice Manager leading on the group’s behalf. 4. Applicable Service Standards 4.1 Applicable national standards (e.g. NICE)
All practices taking part in the scheme are expected to work within usual contractual terms and conditions.
4.2 Applicable standards set out in Guidance and/or issued by a competent body (e.g. Royal
Colleges) 4.3 Applicable local standards National standards will be monitored and reported locally, within set timelines. 5. Applicable quality requirements and CQUIN goals 5.1 Applicable Quality Requirements (See Schedule 4A-C)
5.2 Applicable CQUIN goals (See Schedule 4D)
N/A 6. Location of Provider Premises The Provider’s Premises are located at: This will be confirmed within the individual delivery plans.
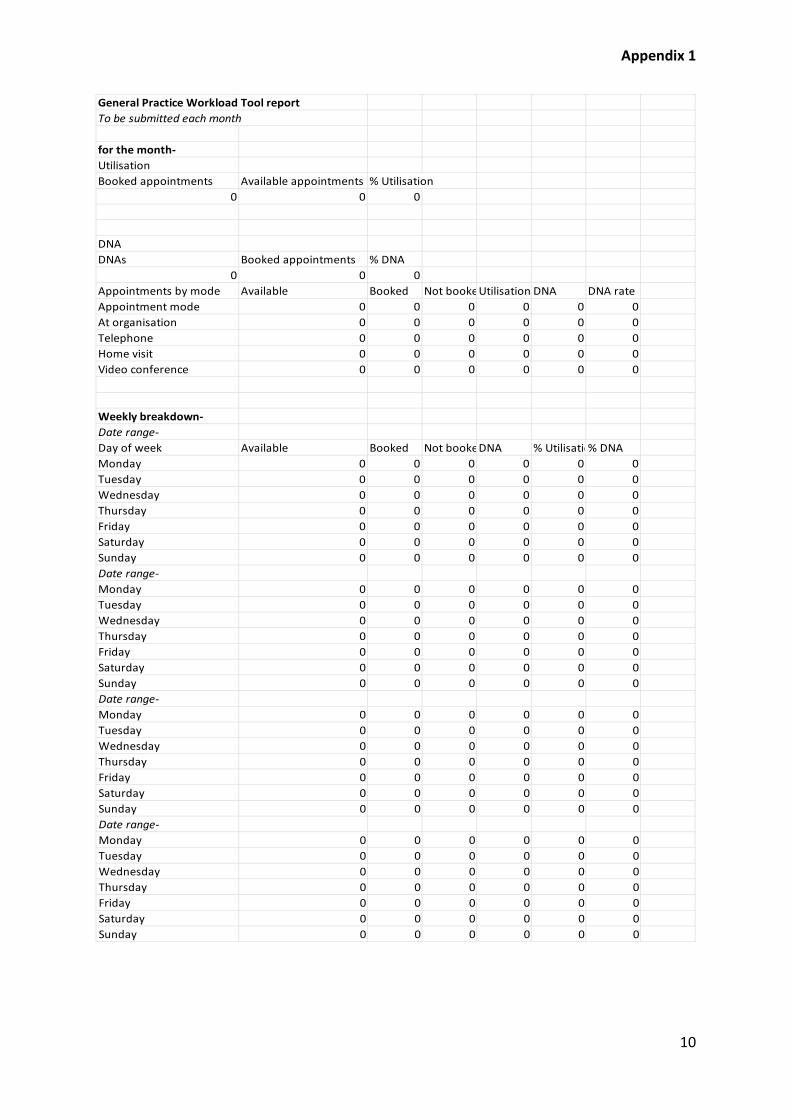
Appendix 1
10
General Practice Workload Tool report To be submitted each month
for the month- UtilisationBooked appointments Available appointments % Utilisation
0 0 0
DNADNAs Booked appointments % DNA
0 0 0Appointments by mode Available Booked Not bookeUtilisation DNA DNA rateAppointment mode 0 0 0 0 0 0At organisation 0 0 0 0 0 0Telephone 0 0 0 0 0 0Home visit 0 0 0 0 0 0Video conference 0 0 0 0 0 0
Weekly breakdown- Date range- Day of week Available Booked Not bookeDNA % Utilisatio% DNAMonday 0 0 0 0 0 0Tuesday 0 0 0 0 0 0Wednesday 0 0 0 0 0 0Thursday 0 0 0 0 0 0Friday 0 0 0 0 0 0Saturday 0 0 0 0 0 0Sunday 0 0 0 0 0 0Date range- Monday 0 0 0 0 0 0Tuesday 0 0 0 0 0 0Wednesday 0 0 0 0 0 0Thursday 0 0 0 0 0 0Friday 0 0 0 0 0 0Saturday 0 0 0 0 0 0Sunday 0 0 0 0 0 0Date range- Monday 0 0 0 0 0 0Tuesday 0 0 0 0 0 0Wednesday 0 0 0 0 0 0Thursday 0 0 0 0 0 0Friday 0 0 0 0 0 0Saturday 0 0 0 0 0 0Sunday 0 0 0 0 0 0Date range- Monday 0 0 0 0 0 0Tuesday 0 0 0 0 0 0Wednesday 0 0 0 0 0 0Thursday 0 0 0 0 0 0Friday 0 0 0 0 0 0Saturday 0 0 0 0 0 0Sunday 0 0 0 0 0 0
Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Primary Care Frameworks and Locally Enhanced Service Payments Quarter 2 2020/21
PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: Tuesday 25th August 2020 AGENDA ITEM: 10.0
Title of Report: Primary Care Frameworks and Enhanced Services Update (Quarter 2)
Purpose of Report: To update the committee on the position for each CCGs primary care framework, enhanced service payments and scoping of enhanced services commissioned by CCGs.
Author of Report: Sarah Southall, Head of Primary Care Wolverhampton/GPFV Programme Director
Management Lead/Signed off by: Matthew Hartland, Deputy Accountable Officer
Public or Private: Public
Key Points:
Work Stream Meetings continue to be held with representation from each primary care team. The priorities for focus in July and August have been; 1. Primary Care Frameworks – progress to full implementation 2. Enhanced Service Payments – quarter 1 payments have been
made in line with income protection expectations 3. Commissioned Enhanced Services – opportunities have been
identified to achieve a common approach to how activities are commissioned
This report provides assurance regarding the work undertaken in these areas since the last committee meeting in June.
Recommendation:
The committee accept all 3 recommendations listed below within the report.
1) Frameworks : Approval for frameworks based on recommendations from Primary Care Operational Groups (Wolverhampton and Walsall)
2) Enhanced Service Payments : Note that all payments have been made to practices for enhanced services (quarter 1)
3) Enhanced Services Review: further work should be undertaken to reduce variation across CCG commissioning ie frameworks and enhanced services.
Conflicts of Interest:
No conflicts of interest identified whilst preparing this report. However, CCG committee members who are GPs will be conflicted regarding the findings in this report as they are commissioned providers of service(s).

Links to Corporate Objectives:
1) Improving the quality and safety of the services we commission 2) Reducing Health Inequalities in Wolverhampton 3) System effectiveness delivered within our financial envelope
Action Required: Assurance Decision
Implications:
Financial NA
Assurance Framework N/A
Risks and Legal Obligations
N/A
Equality & Diversity None of the protected characteristics are affected by the content of this report.
Other N/A

1 Purpose To provide a further update to the committee in common on the work of the task and finish group that had been formed to focus on primary care frameworks, enhanced service commissioning and payments. The group has met regularly with representation from each CCGs primary care team. The committee in common agreed in June that income protection should be consistently applied for all Black Country and West Birmingham practices and that further work should be undertaken to determine the extent of commissioning for other enhanced services in primary care. Updates for each of the above are contained within this report.
2 Key Points 2.1 CCG Quality Improvement Frameworks
The committee in common were assured of the progress that had been made in each CCG in regard to the mobilisation of their locally commissioned framework. The table below confirms the status of each framework:-
CCG 2019/20 Reconciliation
2020/21 Scheme Value
2020/21 Scheme Anticipated Launch
Status
Dudley Complete (Quarter 1) £7.2 million Scheme live
April 2020 Live
Sandwell and West Birmingham
Complete (Quarter 1) £8.3 million
Scheme went live 1 July 2020 (repurposed funding to address Covid-19 Care Home Response)
Live
Walsall Complete (Quarter 1) £1 million September 2020
Scheme finalised due to go live 1 September 2020
Wolverhampton Complete (July 2020) £2.1 million September 2020
Scheme finalised due to go live 1 September 2020
2.1.1 Dudley Quality Outcome for Health (DQOFH)
DQOFH was reviewed in light of COVID-19 to determine the focus areas for 2020/21 in line with the National QoF contract, which has eluded that QoF points will be re-allocated to further strengthen the emphasis and support delivery of the Flu campaign during 2020/21. As currently there is no specific indicator for flu within the DQOFH framework, the DQOFH review group will re-convene to look at where indicator values could be reduced or suspended to accommodate this in line with the National QoF. This cannot be finalised until further guidance has been released nationally. We will ensure that practice income remains stable in line with guidance from NHSE.
2.1.2 Sandwell & West Birmingham CCG Primary Care Framework Following approval at the June Primary Care Commissioning Committee in Common the revised PCCF for 2020/21 went live on 1st July 2020. All of the corresponding changes to the searches, prompts and templates are in place and the Primary Care Development Managers have begun a series of virtual PCN support visits.

2.1.3 Walsall Primary Care Offer The offer has been agreed locally, except two specifications linked to QOF (COPD and diabetes) as awaiting guidance on QOF repurposing. Work commenced on amending templates and searches within GP clinical systems however due to accessibility issues this may cause a slight delay hence go live is expected early September rather than 1 September. Final versions of specifications still need to be sent out to practices to sign up to, although all have seen the drafts that went out to consultation.
2.1.4 Wolverhampton QOF+ Framework
Since the last committee in common held in June the framework has been finalised via the QOF+ Development Group, with representation from each primary care network and also LMC. All indicator sets (existing and new) have been aligned to SNOMED coding and revised/new searches built to enable practices to identify patients they should be prioritising for the range of activities detailed within the framework. Changes have been made to reflect the shorter duration of the scheme ie 7 months, thresholds have been adjusted encouraging a minimum level of achievement and where practices have been able to excel to achieve an incentive for higher levels of achievement. Each practice will receive an aspiration payment based on 2019/20 payment with the opportunity to achieve a top up should they exceed the minimum level of achievement by March 31st 2021. The scheme was agreed in principle at Primary Care Operational Management Group in August 2020 following agreement from the QOF+ Development Group.
2.1.5 Framework Content A review of content within each framework has taken place to confirm the indicator set(s) and detail within each and to determine the extent of similarity. During this piece of work it has become increasingly evident that there are opportunities, identified in the table below, where there could be more consistency among indicator sets, this would reduce gaps and/or variation in commissioned activities CCGs and provide a more targeted approach to population health needs. In some CCGs to qualify for sign up to their framework there are access requirements that should be fulfilled in Dudley, Sandwell and West Birmingham, these aren’t currently required in the other CCGs but should be explored in future years to ensure patients have access to equivocal service wherever they are registered in the Black Country and West Birmingham footprint. During the review of frameworks it became evident that there a number of variances in indicator wording and thresholds/targets that had been set, there are therefore opportunities to explore the feasibility of adopting a consistent indicator set with corresponding thresholds. However, recognition should be given to the extent of additionality this would constitute particularly in Walsall, both from a workload and investment perspective. In Sandwell and West Birmingham some locally enhanced services such as ECGs are already included with their framework, other CCGs could adopt this approach or explore a standard tariff should the activity continue to be offered as an enhanced service. There are however some indicator set(s) that aren’t evident in some places at all and consideration could be given to whether they are consistently included for all places or removed.
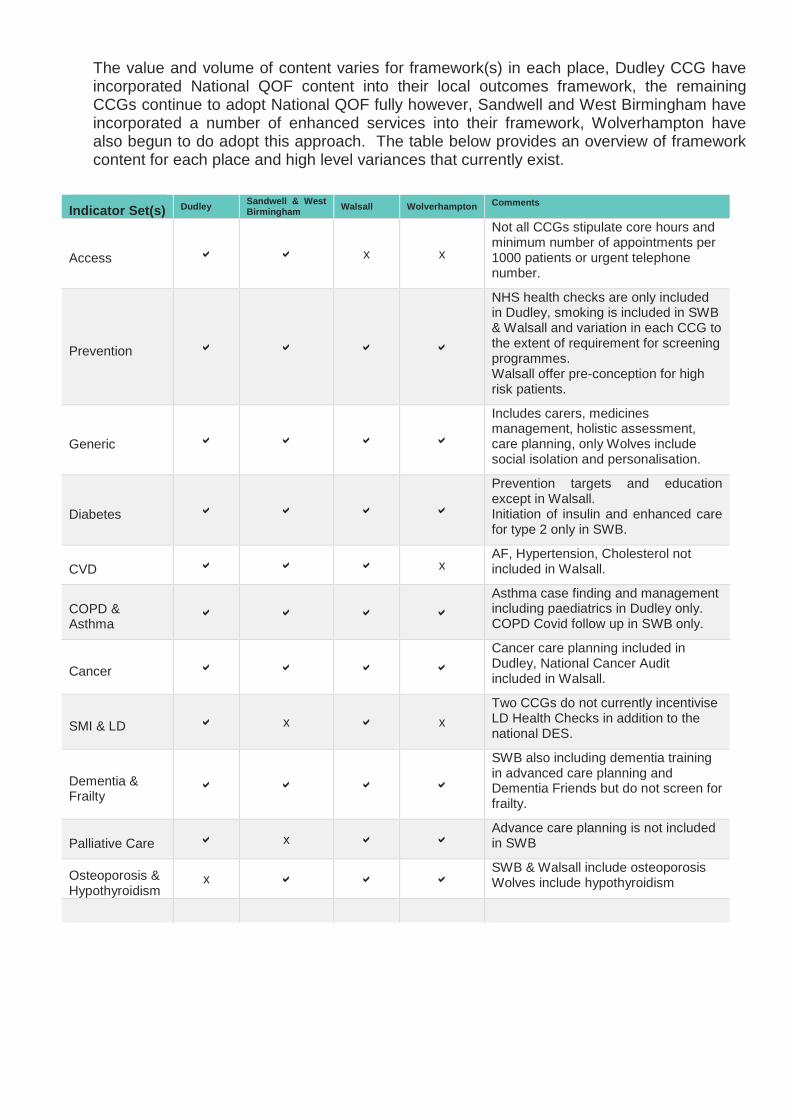
The value and volume of content varies for framework(s) in each place, Dudley CCG have incorporated National QOF content into their local outcomes framework, the remaining CCGs continue to adopt National QOF fully however, Sandwell and West Birmingham have incorporated a number of enhanced services into their framework, Wolverhampton have also begun to do adopt this approach. The table below provides an overview of framework content for each place and high level variances that currently exist.
Indicator Set(s) Dudley Sandwell & West
Birmingham Walsall Wolverhampton Comments
Access x x
Not all CCGs stipulate core hours and minimum number of appointments per 1000 patients or urgent telephone number.
Prevention
NHS health checks are only included in Dudley, smoking is included in SWB & Walsall and variation in each CCG to the extent of requirement for screening programmes. Walsall offer pre-conception for high risk patients.
Generic
Includes carers, medicines management, holistic assessment, care planning, only Wolves include social isolation and personalisation.
Diabetes
Prevention targets and education except in Walsall. Initiation of insulin and enhanced care for type 2 only in SWB.
CVD x AF, Hypertension, Cholesterol not included in Walsall.
COPD & Asthma
Asthma case finding and management including paediatrics in Dudley only. COPD Covid follow up in SWB only.
Cancer Cancer care planning included in Dudley, National Cancer Audit included in Walsall.
SMI & LD x x Two CCGs do not currently incentivise LD Health Checks in addition to the national DES.
Dementia & Frailty
SWB also including dementia training in advanced care planning and Dementia Friends but do not screen for frailty.
Palliative Care x Advance care planning is not included in SWB
Osteoporosis & Hypothyroidism
x SWB & Walsall include osteoporosis Wolves include hypothyroidism
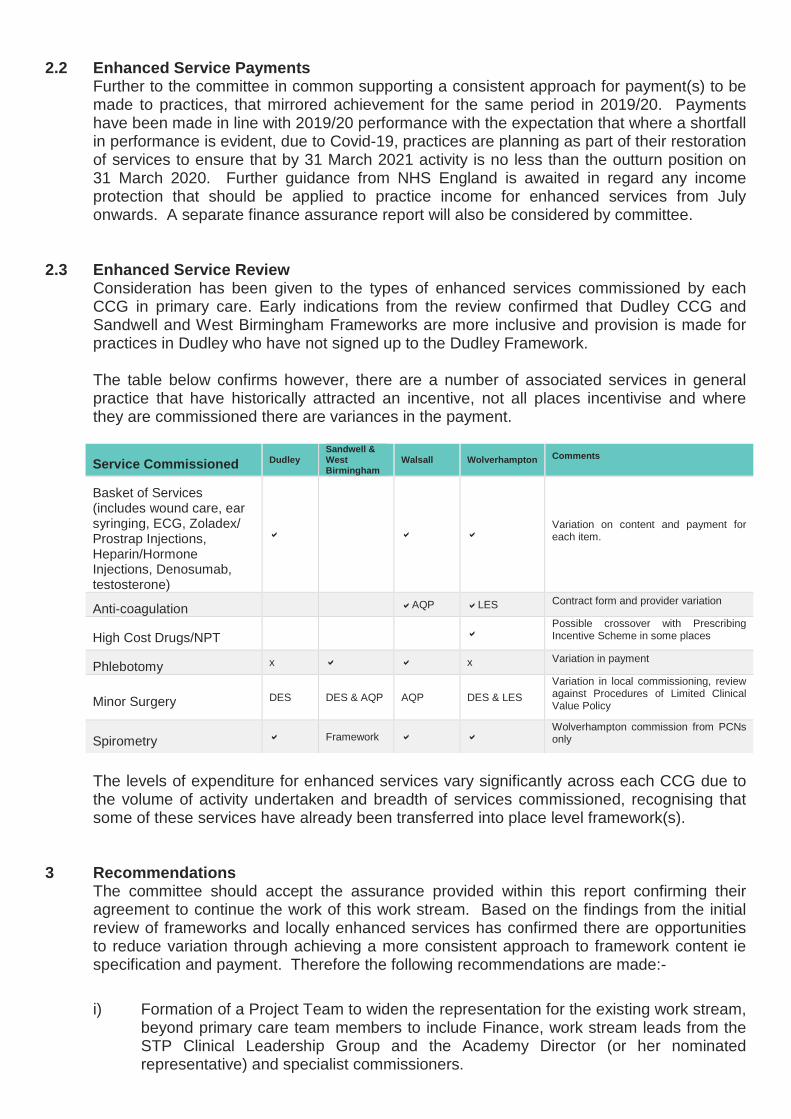
2.2 Enhanced Service Payments Further to the committee in common supporting a consistent approach for payment(s) to be made to practices, that mirrored achievement for the same period in 2019/20. Payments have been made in line with 2019/20 performance with the expectation that where a shortfall in performance is evident, due to Covid-19, practices are planning as part of their restoration of services to ensure that by 31 March 2021 activity is no less than the outturn position on 31 March 2020. Further guidance from NHS England is awaited in regard any income protection that should be applied to practice income for enhanced services from July onwards. A separate finance assurance report will also be considered by committee.
2.3 Enhanced Service Review Consideration has been given to the types of enhanced services commissioned by each CCG in primary care. Early indications from the review confirmed that Dudley CCG and Sandwell and West Birmingham Frameworks are more inclusive and provision is made for practices in Dudley who have not signed up to the Dudley Framework. The table below confirms however, there are a number of associated services in general practice that have historically attracted an incentive, not all places incentivise and where they are commissioned there are variances in the payment.
Service Commissioned Dudley Sandwell & West Birmingham
Walsall Wolverhampton Comments
Basket of Services (includes wound care, ear syringing, ECG, Zoladex/ Prostrap Injections, Heparin/Hormone Injections, Denosumab, testosterone)
Variation on content and payment for each item.
Anti-coagulation AQP LES Contract form and provider variation
High Cost Drugs/NPT Possible crossover with Prescribing Incentive Scheme in some places
Phlebotomy x x Variation in payment
Minor Surgery DES DES & AQP AQP DES & LES Variation in local commissioning, review against Procedures of Limited Clinical Value Policy
Spirometry Framework Wolverhampton commission from PCNs only
The levels of expenditure for enhanced services vary significantly across each CCG due to the volume of activity undertaken and breadth of services commissioned, recognising that some of these services have already been transferred into place level framework(s).
3 Recommendations The committee should accept the assurance provided within this report confirming their agreement to continue the work of this work stream. Based on the findings from the initial review of frameworks and locally enhanced services has confirmed there are opportunities to reduce variation through achieving a more consistent approach to framework content ie specification and payment. Therefore the following recommendations are made:- i) Formation of a Project Team to widen the representation for the existing work stream,
beyond primary care team members to include Finance, work stream leads from the STP Clinical Leadership Group and the Academy Director (or her nominated representative) and specialist commissioners.

ii) Consider how Indicator Set(s) in frameworks can be consistent ie wording and range of requirements, points/payment allocation(s).
iii) Identify opportunities for enhanced services to be incorporated into frameworks in subsequent years ie commencing 2021/22 and transference of funding to increase framework value.
iv) For services that remain outside of frameworks, locally commissioned services should also be reviewed to determine scope and cost of activity in order for consistent rates of pay for commissioned activities to be achieved ie commencing 2021/22.
v) Review of investment arrangements for each place in regard to frameworks to address the variation among CCGs.
The objective of this work will be to reduce variation and improve population health management through commissioning consistently where reasonably practical to do so. There is an opportunity for the work stream to explore in more detail the feasibility of whether some of the enhanced services could/should be included in each CCGs framework and where this wouldn’t be viable but the service is still required to achieve a consistency in specification and payment for that service. This approach would seek to achieve a reduction in the current gap in variation and could be the next area of focus for the work stream.
SLS/FW-PCCIC/AUG20/V1.0
Finance Briefing Report | 1 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: 25 August 2020 AGENDA ITEM: 12.0
Title of Report: Finance briefing report for the period ending 31 July 2020 (Month 04)
Purpose of Report: To provide information to the Committee on the financial expenditure of the Black Country and West Birmingham CCGs delegated primary care resource for the 2020/21 financial year.
Author of Report:
Lorraine Gilbert Head of Finance Walsall CCG
Phil Cowley – Senior Finance Manager – Primary Care, Dudley CCG
Carly Sheldon – Senior Primary Care Accountant, Sandwell & West Birmingham CCG
Jonathan Mason – Senior Finance Manager – Wolverhampton CCG
Management Lead/Signed off by:
James Green Chief Finance Officer Black Country & West Birmingham CCGs
Public or Private: Public
Key Points:
• This report is formed from the four individual CCGs reported position • The Black Country and West Birmingham CCG’s overall primary care
co-commissioning delegated expenditure for the 4 month period was £71.763m
• The total spend for GP Forward View was £3.607m
• Spend on Other Primary Care Funding totalled £22.889m (Please note
the budget lines reported are not consistent between CCG’s
Recommendation:
Members of the Primary Care Co-Commissioning Committee are asked to:
1. Discuss the contents of the report;
2. Approve the contents of the report and the financial position for the 4 month period in 2020/21.
3. Note the residual risks identified in this report
Conflicts of Interest:
Links to Corporate Objectives:
Action Required: Assurance

Document name goes here, document name goes here | 2 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Implications:
Financial N/A
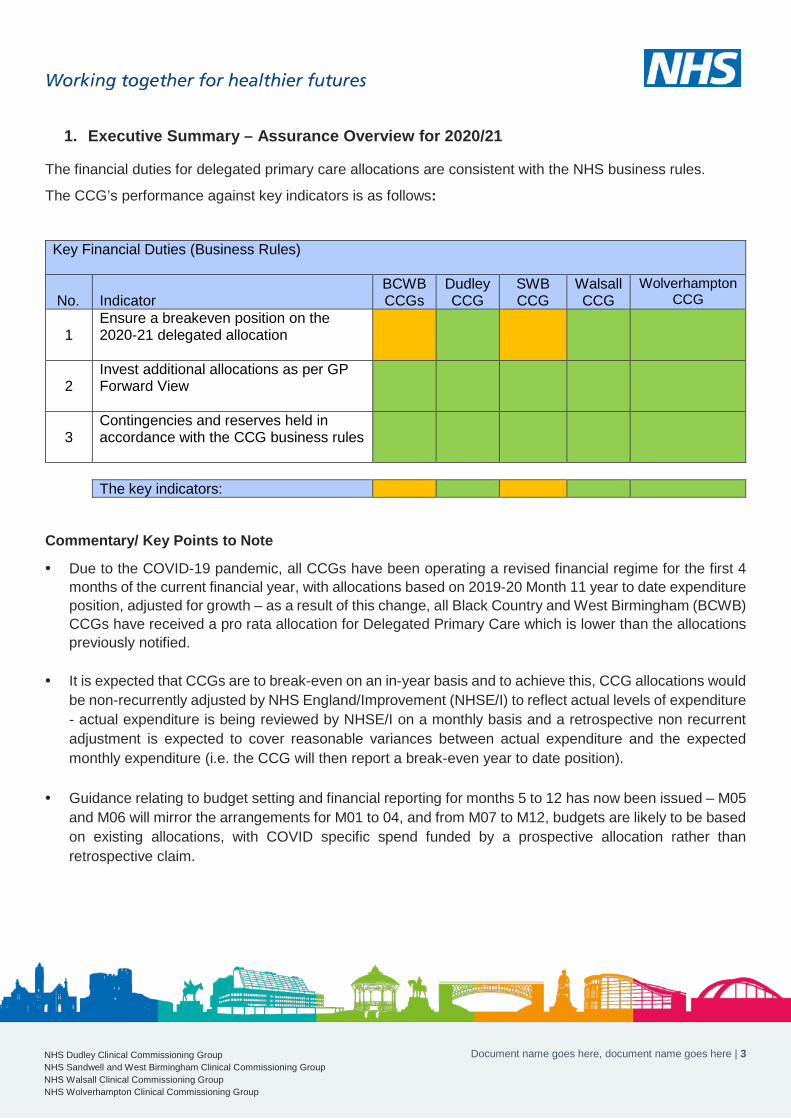
Document name goes here, document name goes here | 3 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
1. Executive Summary – Assurance Overview for 2020/21
The financial duties for delegated primary care allocations are consistent with the NHS business rules.
The CCG’s performance against key indicators is as follows:
Key Financial Duties (Business Rules)
No. Indicator
BCWB CCGs
Dudley CCG
SWB CCG
Walsall CCG
Wolverhampton CCG
1
Ensure a breakeven position on the 2020-21 delegated allocation
2
Invest additional allocations as per GP Forward View
3
Contingencies and reserves held in accordance with the CCG business rules
The key indicators:
Commentary/ Key Points to Note
• Due to the COVID-19 pandemic, all CCGs have been operating a revised financial regime for the first 4 months of the current financial year, with allocations based on 2019-20 Month 11 year to date expenditure position, adjusted for growth – as a result of this change, all Black Country and West Birmingham (BCWB) CCGs have received a pro rata allocation for Delegated Primary Care which is lower than the allocations previously notified.
• It is expected that CCGs are to break-even on an in-year basis and to achieve this, CCG allocations would be non-recurrently adjusted by NHS England/Improvement (NHSE/I) to reflect actual levels of expenditure - actual expenditure is being reviewed by NHSE/I on a monthly basis and a retrospective non recurrent adjustment is expected to cover reasonable variances between actual expenditure and the expected monthly expenditure (i.e. the CCG will then report a break-even year to date position).
• Guidance relating to budget setting and financial reporting for months 5 to 12 has now been issued – M05 and M06 will mirror the arrangements for M01 to 04, and from M07 to M12, budgets are likely to be based on existing allocations, with COVID specific spend funded by a prospective allocation rather than retrospective claim.

Document name goes here, document name goes here | 4 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
2. Financial Position as at March 2020 (Month 12)
Dudley CCG SWB CCG Walsall CCG Wolverhampton
CCG Total M4 2020/21
Plan Actual Plan Actual Plan Actual Plan Actual Plan Actual
Fav / (Adv)
Variance £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
Primary Care Co-commissioning General Practice – GMS 9,704 9,753 19,415 19,294 7,507 7,508 7,750 7,750 44,377 44,305 72 General Practice – PMS 286 274 - 485 485 771 758 13 Other List-Based Services (APMS incl.) 185 185 811 885 1,518 1,516 723 723 3,238 3,309 (72) Premises cost reimbursements 1,051 1,069 1,947 1,864 823 834 595 595 4,416 4,362 54 Primary Care NHS Property Services Costs 537 537 1,215 1,183 1,389 1,389 227 227 3,368 3,336 32 Other premises costs 4 28 20 24 4 4 28 56 (28) Enhanced services 3,210 3,261 3,572 3,539 1,325 1,379 1,034 1,034 9,141 9,213 (72) QOF 64 65 2,333 2,198 1,401 1,401 1,211 1,211 5,009 4,876 134 Other - GP Services 494 502 (1,757) (672) (274) 434 1,179 1,149 (358) 1,413 (1,771) Delegated Contingency (10) - 144 - 74 - 135 135 342 135 207 Total Primary Care Co-commissioning 15,240 15,400 27,986 28,588 13,763 14,461 13,342 13,313 70,331 71,763 (1,432)
Delegated Primary Care
As at 31 July 2020, the overall position for BCWB CCGs is a net overspend of £1.432m, and the key issues relating to each individual CCG are as follows:
Dudley CCG
There is a net overspend of £160K for the period of which
• £100K relates to the additional costs incurred following the transfer of a branch surgery from South Staffs CCG to Dudley – in normal circumstances, an allocation adjustment would have been actioned between the 2 CCGs, but this has not occurred due to the COVID finance regime, but this variance will be mitigated on receipt of in year allocation adjustment as referenced earlier in the report.
• A further £60K adverse variance is due to the reduced allocation received to date, which will again be adjusted in future months.
Sandwell & West Birmingham CCG (SWBCCG)
There is a net overspend of £602K, with the main areas analysed as follows:
• Other GP services overspent by £1,085K in total, of which £639K relates to the year to date underlying deficit in the original notified allocation, further compounded by a shortfall of £437K on the allocation received under the current COVID finance regime
• Overspend of £74K on other list size services due to late submission of claims for locum reimbursement costs
• Underspend of £121K on GMS due to lower growth in patient list sizes, together with slippage on revised contract for Walk in centre services
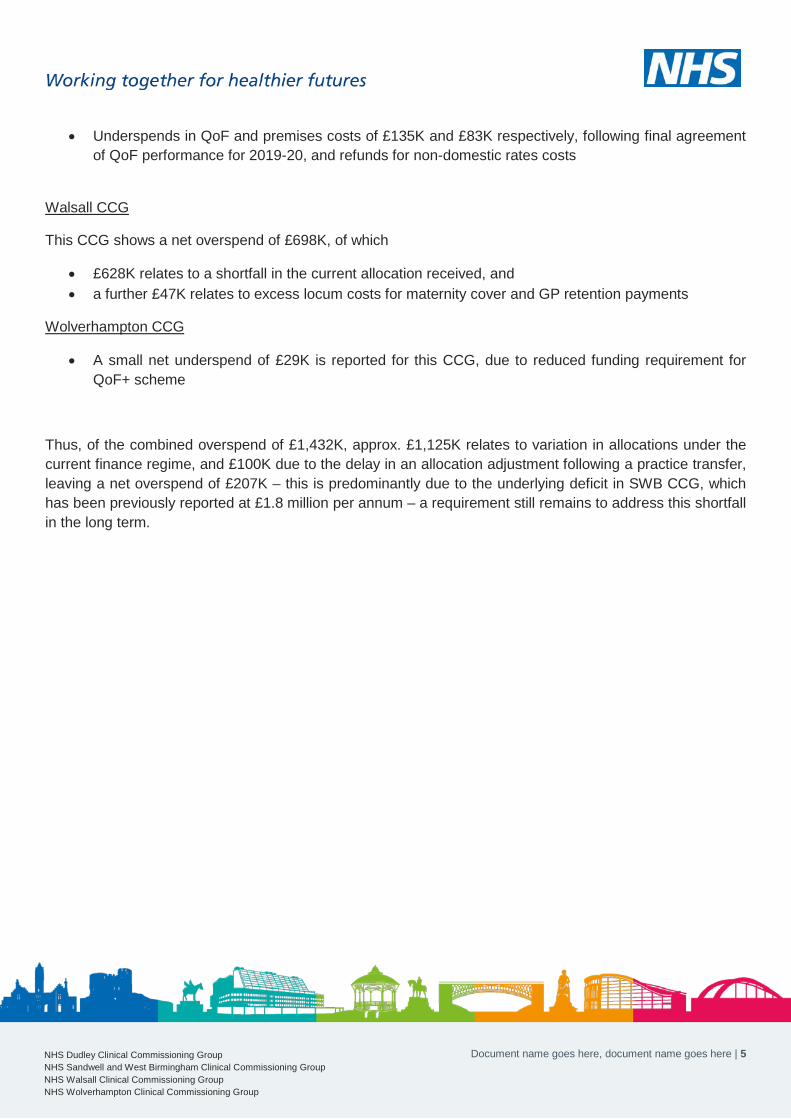
Document name goes here, document name goes here | 5 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
• Underspends in QoF and premises costs of £135K and £83K respectively, following final agreement of QoF performance for 2019-20, and refunds for non-domestic rates costs
Walsall CCG
This CCG shows a net overspend of £698K, of which
• £628K relates to a shortfall in the current allocation received, and • a further £47K relates to excess locum costs for maternity cover and GP retention payments
Wolverhampton CCG
• A small net underspend of £29K is reported for this CCG, due to reduced funding requirement for QoF+ scheme
Thus, of the combined overspend of £1,432K, approx. £1,125K relates to variation in allocations under the current finance regime, and £100K due to the delay in an allocation adjustment following a practice transfer, leaving a net overspend of £207K – this is predominantly due to the underlying deficit in SWB CCG, which has been previously reported at £1.8 million per annum – a requirement still remains to address this shortfall in the long term.
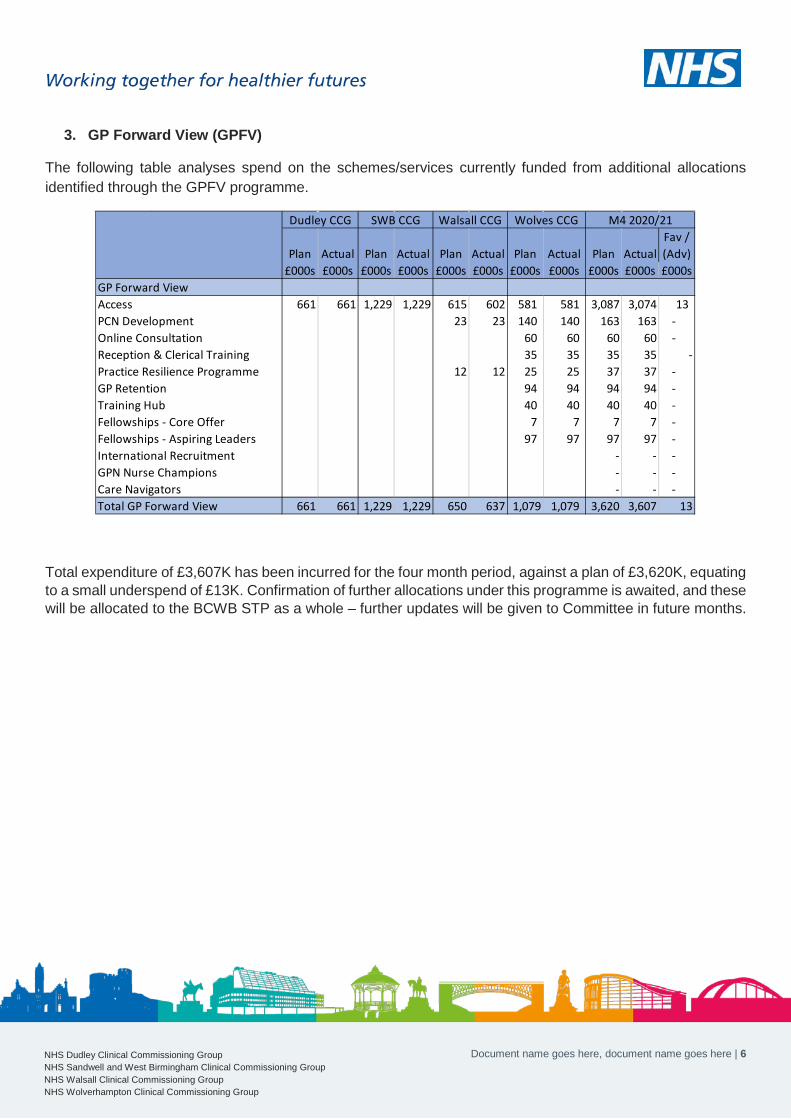
Document name goes here, document name goes here | 6 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
3. GP Forward View (GPFV)
The following table analyses spend on the schemes/services currently funded from additional allocations identified through the GPFV programme.
Total expenditure of £3,607K has been incurred for the four month period, against a plan of £3,620K, equating to a small underspend of £13K. Confirmation of further allocations under this programme is awaited, and these will be allocated to the BCWB STP as a whole – further updates will be given to Committee in future months.
Plan Actual Plan Actual Plan Actual Plan Actual Plan ActualFav / (Adv)
£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000sGP Forward ViewAccess 661 661 1,229 1,229 615 602 581 581 3,087 3,074 13 PCN Development 23 23 140 140 163 163 - Online Consultation 60 60 60 60 - Reception & Clerical Training 35 35 35 35 -Practice Resilience Programme 12 12 25 25 37 37 - GP Retention 94 94 94 94 - Training Hub 40 40 40 40 - Fellowships - Core Offer 7 7 7 7 - Fellowships - Aspiring Leaders 97 97 97 97 - International Recruitment - - - GPN Nurse Champions - - - Care Navigators - - - Total GP Forward View 661 661 1,229 1,229 650 637 1,079 1,079 3,620 3,607 13
M4 2020/21Dudley CCG SWB CCG Walsall CCG Wolves CCG
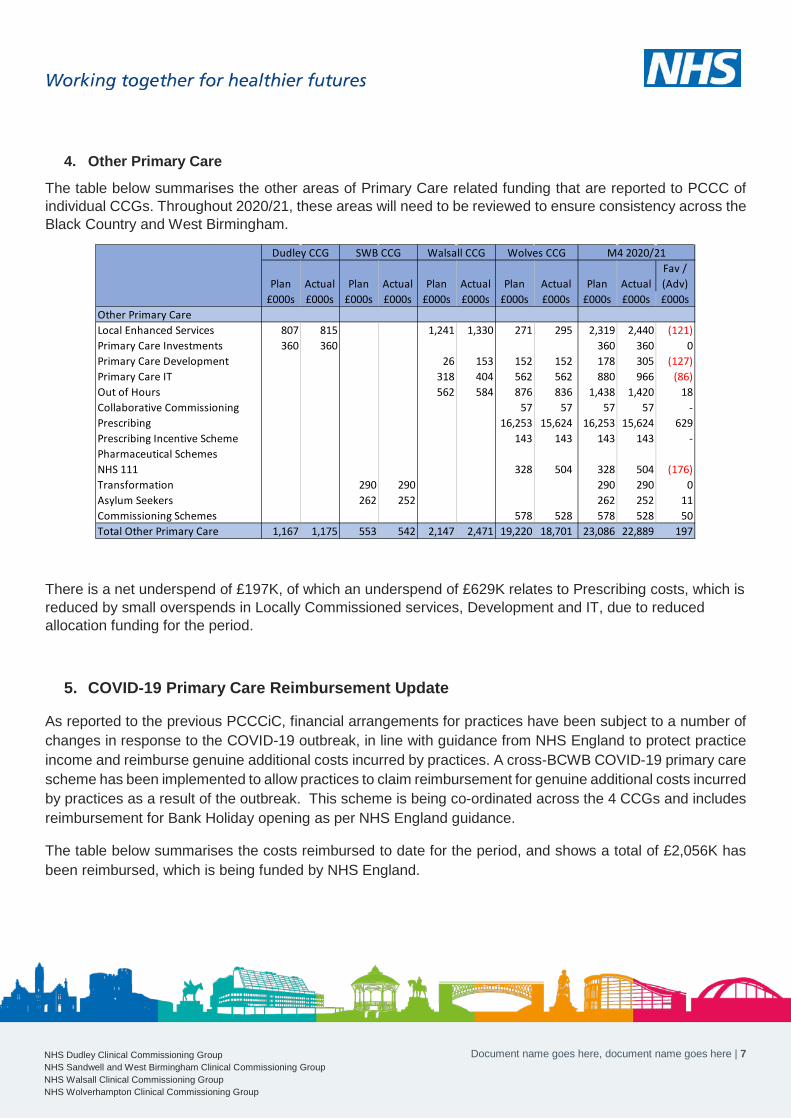
Document name goes here, document name goes here | 7 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
4. Other Primary Care
The table below summarises the other areas of Primary Care related funding that are reported to PCCC of individual CCGs. Throughout 2020/21, these areas will need to be reviewed to ensure consistency across the Black Country and West Birmingham.
There is a net underspend of £197K, of which an underspend of £629K relates to Prescribing costs, which is reduced by small overspends in Locally Commissioned services, Development and IT, due to reduced allocation funding for the period.
5. COVID-19 Primary Care Reimbursement Update
As reported to the previous PCCCiC, financial arrangements for practices have been subject to a number of changes in response to the COVID-19 outbreak, in line with guidance from NHS England to protect practice income and reimburse genuine additional costs incurred by practices. A cross-BCWB COVID-19 primary care scheme has been implemented to allow practices to claim reimbursement for genuine additional costs incurred by practices as a result of the outbreak. This scheme is being co-ordinated across the 4 CCGs and includes reimbursement for Bank Holiday opening as per NHS England guidance.
The table below summarises the costs reimbursed to date for the period, and shows a total of £2,056K has been reimbursed, which is being funded by NHS England.
Plan Actual Plan Actual Plan Actual Plan Actual Plan ActualFav / (Adv)
£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000sOther Primary CareLocal Enhanced Services 807 815 1,241 1,330 271 295 2,319 2,440 (121)Primary Care Investments 360 360 360 360 0Primary Care Development 26 153 152 152 178 305 (127)Primary Care IT 318 404 562 562 880 966 (86)Out of Hours 562 584 876 836 1,438 1,420 18Collaborative Commissioning 57 57 57 57 -Prescribing 16,253 15,624 16,253 15,624 629Prescribing Incentive Scheme 143 143 143 143 -Pharmaceutical SchemesNHS 111 328 504 328 504 (176)Transformation 290 290 290 290 0Asylum Seekers 262 252 262 252 11Commissioning Schemes 578 528 578 528 50Total Other Primary Care 1,167 1,175 553 542 2,147 2,471 19,220 18,701 23,086 22,889 197
M4 2020/21Dudley CCG SWB CCG Walsall CCG Wolves CCG
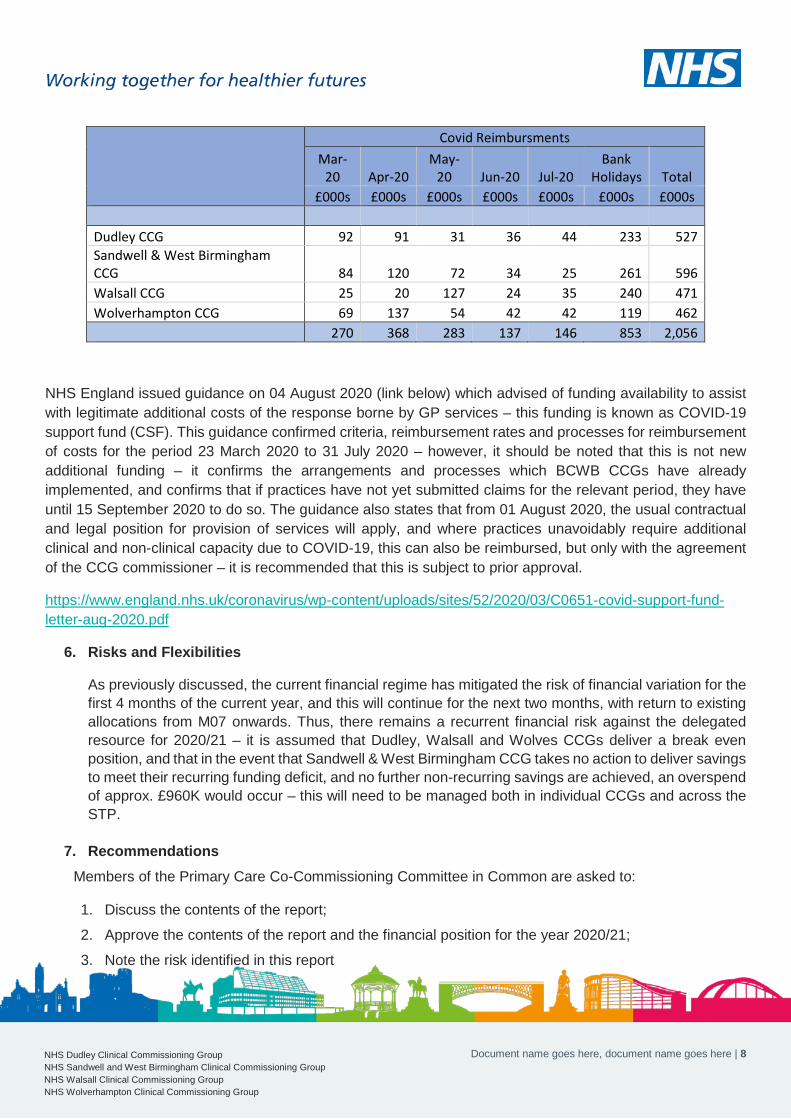
Document name goes here, document name goes here | 8 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Covid Reimbursments Mar-
20 Apr-20 May-
20 Jun-20 Jul-20 Bank
Holidays Total £000s £000s £000s £000s £000s £000s £000s
Dudley CCG 92 91 31 36 44 233 527 Sandwell & West Birmingham CCG 84 120 72 34 25 261 596 Walsall CCG 25 20 127 24 35 240 471 Wolverhampton CCG 69 137 54 42 42 119 462
270 368 283 137 146 853 2,056
NHS England issued guidance on 04 August 2020 (link below) which advised of funding availability to assist with legitimate additional costs of the response borne by GP services – this funding is known as COVID-19 support fund (CSF). This guidance confirmed criteria, reimbursement rates and processes for reimbursement of costs for the period 23 March 2020 to 31 July 2020 – however, it should be noted that this is not new additional funding – it confirms the arrangements and processes which BCWB CCGs have already implemented, and confirms that if practices have not yet submitted claims for the relevant period, they have until 15 September 2020 to do so. The guidance also states that from 01 August 2020, the usual contractual and legal position for provision of services will apply, and where practices unavoidably require additional clinical and non-clinical capacity due to COVID-19, this can also be reimbursed, but only with the agreement of the CCG commissioner – it is recommended that this is subject to prior approval.
https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0651-covid-support-fund-letter-aug-2020.pdf
6. Risks and Flexibilities
As previously discussed, the current financial regime has mitigated the risk of financial variation for thefirst 4 months of the current year, and this will continue for the next two months, with return to existingallocations from M07 onwards. Thus, there remains a recurrent financial risk against the delegatedresource for 2020/21 – it is assumed that Dudley, Walsall and Wolves CCGs deliver a break evenposition, and that in the event that Sandwell & West Birmingham CCG takes no action to deliver savingsto meet their recurring funding deficit, and no further non-recurring savings are achieved, an overspendof approx. £960K would occur – this will need to be managed both in individual CCGs and across theSTP.
7. RecommendationsMembers of the Primary Care Co-Commissioning Committee in Common are asked to:
1. Discuss the contents of the report;
2. Approve the contents of the report and the financial position for the year 2020/21;
3. Note the risk identified in this report

PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: 25 August 2020 AGENDA ITEM: 14.0
Title of Report: Primary Care Quality Report
Purpose of Report: To provide assurance to the committee on the core quality and safety activities relating to primary care during the reporting period June – August 2020
Author of Report: Primary Care Quality Leads Management Lead/Signed off by:
Sally Roberts, Chief Nursing Officer, Black Country and West Birmingham CCGs
Public or Private: Public
Key Points:
In order to fully discharge the statutory duties, each CCG has submitted a detailed report in accordance with its usual reporting mechanisms.
An over-arching report has also been submitted which provides detail across the on the key areas of
• Care Quality Commission inspections• Serious incidents and reported patient safety concerns• Infection prevention and control• Flu and vaccination update• Patient Experience and Complaints
Recommendation: To receive the report for assurance and support the monitoring arrangements and actions taken
Conflicts of Interest: N/A
Links to Corporate Objectives:
Action Required: X Assurance Approval For Information
Implications:
Financial
Assurance Framework X
Risks and Legal Obligations
Equality & Diversity
Other
1. IntroductionIt is the responsibility of each CCG to have an established Primary Care Commissioning Committee accountable to the Governing Body. This report provides an overarching update to the committee of the key areas of escalation and assurance relating to the quality and safety of services in Primary Care across the Black Country and West Birmingham CCGs. This over-arching report focusses on the key areas of
• Care Quality Commission inspections• Serious incidents and reported patient safety concerns• Infection prevention and control• Flu and vaccination update• Patient Experience and Complaints
2. Care Quality Commission (CQC) InspectionsDue to the covid-19 pandemic the CQC paused routine inspections (effective 16th March 2020 to date) and developed an Emergency Support Framework to follow during the pandemic.
The interim approach has a number of elements:
• using and sharing information to target support where it’s needed most• having open and honest conversations• taking action to keep people safe and to protect people’s human rights• capturing and sharing actions taken.
Provider Collaboration Reviews (PCRs)
During July & August CQC have undertaken a series of PCRs with the specific aim of:
• Support providers across systems by sharing learning around the positive impact of partnership efforts,resulting in improved experiences and outcomes for those who have used services during thepandemic.
• Share the learning of approaches underway to support preparation for re-establishing services.• To share learning with DHSC, providers and stakeholders at local and national levels in advance of any
subsequent peaks and pre winter 20/21, driving improvement.
Walsall CCG was one of the areas in the 11STP’s chosen across the country to participate in this process
It is hoped that these reviews will help identify where provider collaboration has worked well to the benefit of people who use services. Sharing that learning will help drive further improvements across systems.
2.1 CQC Inadequate Rated Practices The table below highlights the practices rated as inadequate by the CQC and the date of publication.
CCG Practice Date of publication

Dudley CCG Dudley Wood Practice 13th March 2020
Sandwell and West Birmingham CCG
Primary Care Centre, West Bromwich 2nd March 2020
Clifton Lane Medical Practice 12th March 2020
Stonecross Medical Centre 2nd March 2020
Swanpool Medical Centre 12th March 2020
Walsall CCG Moxley Medical Centre 8th January 2020 (see narrative below)
Wolverhampton CCG No inadequate rated practices
Walsall CCG Moxley Medical Centre - a notice of decision to cancel registration was issued and appealed by the GP, the practice was subsequently de-registered. The practice has now been re-registered with a partnership arrangement in place. The CQC rating of Inadequate has been transferred to the new provider, an assurance plan has been sent to CQC as part of the registration process, the Quality Team are continuing to monitor and support Forrester St - was subject to a re-inspection on 4th February as a ‘Special Measures’ practice and notable improvements seen against their action plan and a further update is expected in August 2020. The CQC published the report on 13th April 2020, with the practice rated as requires improvement. SWB CCG Primary Care Centre - the GP’s have agreed to come off the GMS contract and the contract has now been taken on by St Pauls, the practice is now named St Pauls Primary Care Centre. The practice has worked with RCoGP and met the conditions placed by CQC, the practice will be applying for new registration Swan Pool / Stone Cross / Clifton Lane – CCG has commissioned further support work from RCoGP in readiness for re-inspections, which are expected in Sept 2020
3. Health Protection3.1 Personal Protective Equipment (PPE) The supply cell at Jubilee House has been in place since early April and continues to provide stability to the provision of PPE in line with national guidance for general practice.
3.2 Infection Prevention and Control The 2020/21 work programme for infection prevention and control remains on hold due to the Covid -19 pandemic. Support from CCG continues
3.2 Immunisation Each CCG has a local workstream in place to plan for the forthcoming flu season and these will feed into the BCWB STP Strategic Flu Planning Group which is now meeting monthly. The first draft of the STP Flu Plan has been submitted to NHSE/I and the group is awaiting feedback.
National Flu Immunisation Programme Update has been received which indicates an expansion to the programme and subject to contractual negotiations, this season flu vaccination will be additionally offered to:
• household contacts of those on the NHS Shielded Patient List. Specifically, individuals who expect to shareliving accommodation with a shielded person on most days over the winter and therefore for whomcontinuing close contact is unavoidable.
• children of school Year 7 age in secondary schools (those aged 11 on 31 August 2020).
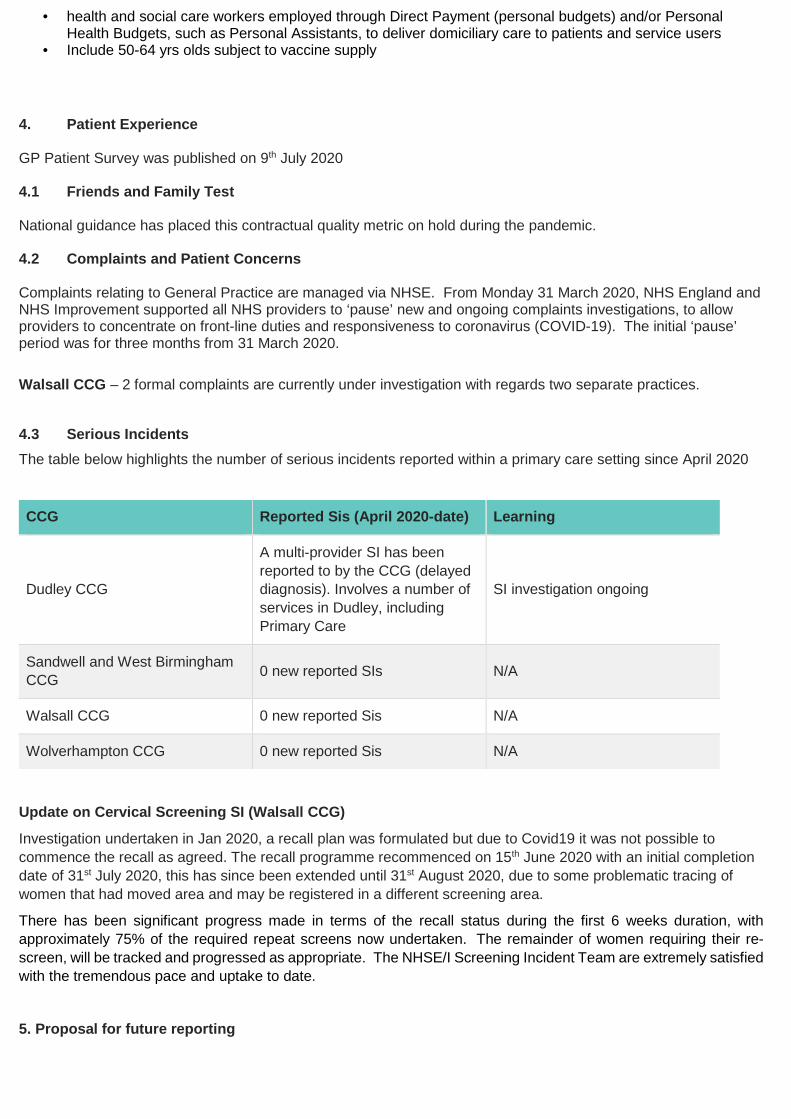
• health and social care workers employed through Direct Payment (personal budgets) and/or PersonalHealth Budgets, such as Personal Assistants, to deliver domiciliary care to patients and service users
• Include 50-64 yrs olds subject to vaccine supply
4. Patient Experience
GP Patient Survey was published on 9th July 2020
4.1 Friends and Family Test
National guidance has placed this contractual quality metric on hold during the pandemic.
4.2 Complaints and Patient Concerns
Complaints relating to General Practice are managed via NHSE. From Monday 31 March 2020, NHS England and NHS Improvement supported all NHS providers to ‘pause’ new and ongoing complaints investigations, to allow providers to concentrate on front-line duties and responsiveness to coronavirus (COVID-19). The initial ‘pause’ period was for three months from 31 March 2020.
Walsall CCG – 2 formal complaints are currently under investigation with regards two separate practices.
4.3 Serious Incidents The table below highlights the number of serious incidents reported within a primary care setting since April 2020
CCG Reported Sis (April 2020-date) Learning
Dudley CCG
A multi-provider SI has been reported to by the CCG (delayed diagnosis). Involves a number of services in Dudley, including Primary Care
SI investigation ongoing
Sandwell and West Birmingham CCG 0 new reported SIs N/A
Walsall CCG 0 new reported Sis N/A
Wolverhampton CCG 0 new reported Sis N/A
Update on Cervical Screening SI (Walsall CCG)
Investigation undertaken in Jan 2020, a recall plan was formulated but due to Covid19 it was not possible to commence the recall as agreed. The recall programme recommenced on 15th June 2020 with an initial completion date of 31st July 2020, this has since been extended until 31st August 2020, due to some problematic tracing of women that had moved area and may be registered in a different screening area.
There has been significant progress made in terms of the recall status during the first 6 weeks duration, with approximately 75% of the required repeat screens now undertaken. The remainder of women requiring their re-screen, will be tracked and progressed as appropriate. The NHSE/I Screening Incident Team are extremely satisfied with the tremendous pace and uptake to date.
5. Proposal for future reporting
In order to ensure consistency in reporting a Task & Finish Group has been established to agree core metrics and a standardised reporting template that can be used by each Place for the Primary Care Operational Group, this will then provide a summary report for the Primary Care Commissioning Committee in Common.
There has been work to develop a Primary Care Assurance Tool (PCAT) in Dudley CCG which can provide a ranking system based on a variety of quality indicators which will aid identification of GP practice performance, it is proposed that this tool is utilised across all CCG’s moving forward. This information can also be triangulated with soft intelligence to enable ongoing monitoring and quality assurance
The work is ongoing and it is expected to be able to report in the new template for the October 2020 meeting
END

Agenda Item 15.0
NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Black Country and West Birmingham Sustainability and Transformation Partnership (STP) Training Hub Assurance and Update Report to Primary Care Commissioning Committee in Common 25th August 2020
Author: Paul Aldridge, General Practice Forward View (GPFV Programme Manager for the Black Country and West Birmingham STP
Authorised by: Sarah Southall, Head of Primary Care (Wolverhampton CCG) and GPFV Programme Director for the Black Country and West Birmingham STP

15.0 - BCWB STP Training Hub Report PCCCiC 25082020 | 2 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Table of Contents 1 Purpose ..................................................................................................................................... 3
2 Key Points ................................................................................................................................ 3
3 Recommendations ................................................................................................................... 6
4 Financial Implications .............................................................................................................. 6
5 Risks and Legal Obligations ................................................................................................... 6
6 Equality and Diversity .............................................................................................................. 6
7 Table of Appendices ................................................................................................................ 6

15.0 - BCWB STP Training Hub Report PCCCiC 25082020 | 3 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
1 Purpose 1.1 To update the Committee on the work of the Black Country and West Birmingham STP
Training Hub over the period July to August 2020.
2 Key Points 2.1 Since the last update to Committee a significant amount of work has taken place to produce
and submit an infrastructure plan for the Hub to Health Education England (HEE). The purpose of this plan is to draw down the funding available to support the workforce and other infrastructure costs associated with delivering the core functions required of the Hub as defined by HEE. This plan has subsequently been approved, including being held up by HEE as the best plan in the Region. With this approval now in place, the Hub can start drawing down the STP full £404k funding allocation and continue the work to reach full maturity by March 2021. It is important that Committee note that any formal staffing structure for the Hub will be incorporated into the CCG Management of Change process and therefore subject to those policies and timescales.
2.2 NHSE/I have confirmed that the annual funding allocation for 2020/21, based on a weighted capitation for the STP, is imminent. This will support the following elements of the work of the Training Hub:-
• General Practice Fellowships for GPs and Nurses New to Practice Programme for newly qualified GPs and Nurses. This will enable the Hub to mobilise and extend the reach of its current plans to offer GP and Nurse Fellowships.
• Local GP Retention: To support areas in delivering local activities which retain their GP workforce. National Priority is for retaining as many GPs as possible and contributing to the manifesto commitments of growing the GP workforce nationally by 6,000. The current target that has been submitted to NHSE/I for the STP is to increase the GP FTE numbers by 13 FTE to 690 FTE before the end of March 2021. Committee are asked to note that the STP may be challenged to increase this number as feedback from NHSE/I Regional colleagues is that the Government is concerned about the number of GPs nationally and may look to increase the target of 6,000 made in the manifesto – therefore the schemes that are designed for the recruitment and retention of GPs across the STP will be a priority for the Hub namely GP Fellowships (including the HEE Trailblazer Fellowships scheme), Mentoring, Portfolio Careers, First 5 Support Offer, Phoenix GP Programme and our Welcome Back/Legacy Scheme.
• Training Hubs Funding will be available to systems to commission primary care workforce transformation activities from their local training hub. The utilisation of this will be driven by priorities identified by the Training Needs Analysis and PCN Workforce Implementation Plans currently being drawn up.

15.0 - BCWB STP Training Hub Report PCCCiC 25082020 | 4 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
• Reception and Clerical Training – this is specific ring fenced funding to support training and development of Reception and Clerical staff. The training hub has already canvassed staff across the STP to identify key priorities.
• Primary Care Network Development Funding – to support PCNs to develop the maturity of their networks.
This means that the Hub can begin to mobilise those plans already approved by the Primary Care and Community Care Workforce Implementation Group (and brought to PCCCiC in June 2020) and work to develop further schemes to support the workforce going forward.
2.3 The Hub is also progressing work to support the recruitment and transition into Primary Care of the new roles supported by the Additional Role Reimbursement Scheme aspect of the Primary Care Network (PCN) Directed Enhanced Service (DES). Progress made over the past 2 months includes:-
• Plans in place to enable the Hub to be the single point of contact for PCNs, practices and staff for information, guidance and support for the new roles. This will include a web based product as well as direct access to the team, networks and ambassadorial/clinical support for those roles most in demand. See figure 1 below:-
Figure 1 – Proposed New Role Offer
• Mobilisation of a virtual network/forum for Physician Associates that is designed to offer peer support and also to identify further training and support needs which can be developed into an offer from the Hub.
• Webinar organised and delivered showcasing a number of the new roles including presentations by front line colleagues who are trailblazing in these currently roles
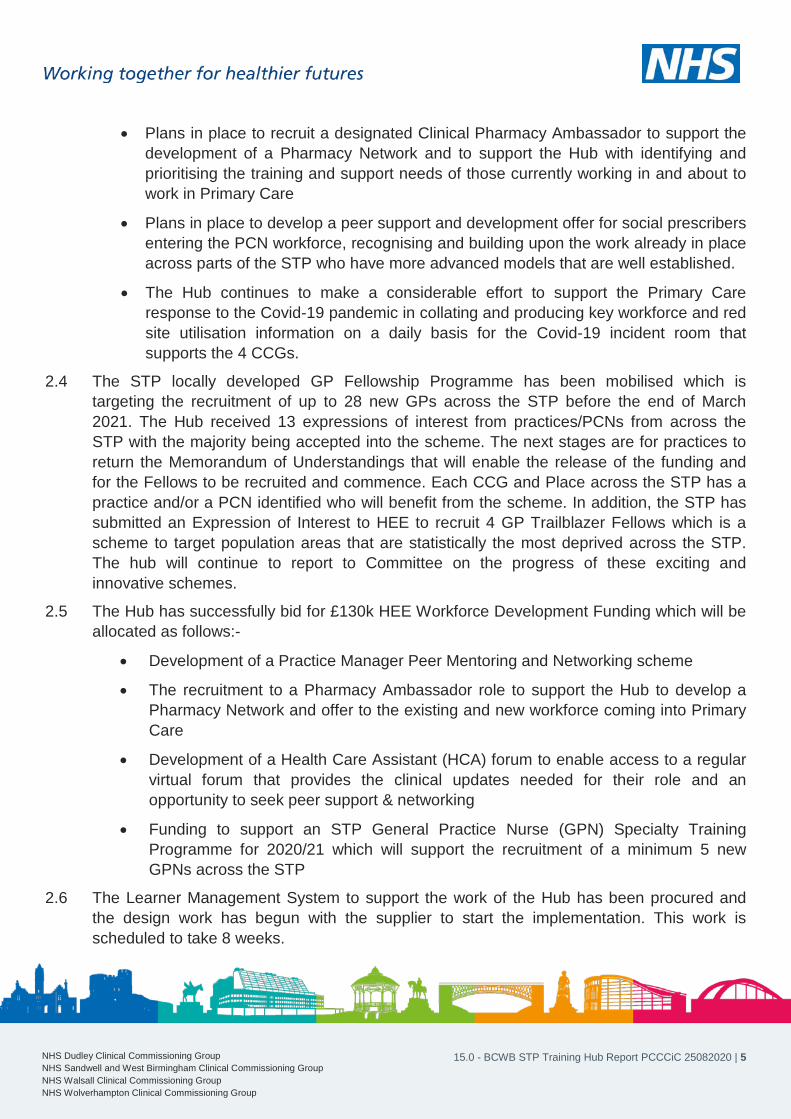
15.0 - BCWB STP Training Hub Report PCCCiC 25082020 | 5 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
• Plans in place to recruit a designated Clinical Pharmacy Ambassador to support the development of a Pharmacy Network and to support the Hub with identifying and prioritising the training and support needs of those currently working in and about to work in Primary Care
• Plans in place to develop a peer support and development offer for social prescribers entering the PCN workforce, recognising and building upon the work already in place across parts of the STP who have more advanced models that are well established.
• The Hub continues to make a considerable effort to support the Primary Care response to the Covid-19 pandemic in collating and producing key workforce and red site utilisation information on a daily basis for the Covid-19 incident room that supports the 4 CCGs.
2.4 The STP locally developed GP Fellowship Programme has been mobilised which is targeting the recruitment of up to 28 new GPs across the STP before the end of March 2021. The Hub received 13 expressions of interest from practices/PCNs from across the STP with the majority being accepted into the scheme. The next stages are for practices to return the Memorandum of Understandings that will enable the release of the funding and for the Fellows to be recruited and commence. Each CCG and Place across the STP has a practice and/or a PCN identified who will benefit from the scheme. In addition, the STP has submitted an Expression of Interest to HEE to recruit 4 GP Trailblazer Fellows which is a scheme to target population areas that are statistically the most deprived across the STP. The hub will continue to report to Committee on the progress of these exciting and innovative schemes.
2.5 The Hub has successfully bid for £130k HEE Workforce Development Funding which will be allocated as follows:-
• Development of a Practice Manager Peer Mentoring and Networking scheme
• The recruitment to a Pharmacy Ambassador role to support the Hub to develop a Pharmacy Network and offer to the existing and new workforce coming into Primary Care
• Development of a Health Care Assistant (HCA) forum to enable access to a regular virtual forum that provides the clinical updates needed for their role and an opportunity to seek peer support & networking
• Funding to support an STP General Practice Nurse (GPN) Specialty Training Programme for 2020/21 which will support the recruitment of a minimum 5 new GPNs across the STP
2.6 The Learner Management System to support the work of the Hub has been procured and the design work has begun with the supplier to start the implementation. This work is scheduled to take 8 weeks.

15.0 - BCWB STP Training Hub Report PCCCiC 25082020 | 6 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
2.7 Committee are also asked to note and recognise that the Hub continues to support the primary care covid-19 response. Daily reports are still collated and produced for the incident room on vital workforce and red site activity across the STP. The Professional Nurse Lead aligned to the Hub is also still working part time on the front line supporting the swabbing effort.
2.8 The latest metrics information and participation across PCNs for the Hub can be found at Appendix B
3 Recommendations 3.1 There are no specific recommendations in this report.
4 Financial Implications 4.1 There are no financial implications arising from this report but a Financial Monitoring
Statement is included at Appendix A for information
5 Risks and Legal Obligations 5.1 The key risk that Committee are asked to note that are associated with this report are
concerned with the impact of the Covid-19 pandemic on staff resources to manage the full programme and clinician time to allocate to their own development
5.2 There are no legal obligations or implications to consider from this report.
6 Equality and Diversity 6.1 There are no implications associated with this report.
7 Table of Appendices
Appendix Reference Name
Appendix A Financial Monitoring Statement
Appendix B Training Hub Metrics and PCN Participation

Scheme/Activity Status GPFV
Funding
Carried
Forward from
2019/2020
SWB
Funding
C/Fwd from
2019/2020
NHSE/I GPFV
Estimated GP
Retention
Funding
2020/2021
NHSE/I GPFV
Estimated GPN
Retention
Funding
2020/2021
NHSE/I
GPFV Estimated
Reception and
Clerical 2020/21
HEE Training
Hub 2020/21
418751-
G8030
HEE
CPD for Nurses,
Midwives and
Allied Health
Professionals
2020/21
HEE Workforce
Development
Funding 2020/21
(assuming
approved)
Total
Funding
Available
Total
Committed
Expenditure to
Date
Estimated
Funding
Remaining
Total Forecast
Expenditure
Purpose
GP Primary Care Network Portfolio Careers Mobilised 184,807 0 0 0 0 0 184,807 184,807 0 184,807 To fund Cohort 2 and the remaining balance from cohort 1 GP Portfolio Careers
Primary Care Network Portfolio Careers Approved -
awaiting
Funding
0 156,280 0 0 0 0 0 156,280 0 156,280 156,280 To fund a new PCN based portfolio careers scheme for all clinical staff centred around the population health
needs of each PCN.
GP Fellowships and First 5 Programme Mobilised 181,000 0 0 0 0 0 0 181,000 19,690 161,310 181,000 To fund a redesign of the GP First 5 offer to extend to supporting practices who wish to take on a newly
qualified GP (Fellowships Offer)
Mentoring (GPs, Pas and Clinical Pharmacists) Mobilised 6,540 65,000 0 0 0 0 0 71,540 10,049 61,491 71,540 Structured mentoring support offer delivered by the GP Mentors to GPs, PAs and Clinical Phamacists across
the STP
GP Clinical Lead for Retention/Single Point of Access Mobilised 3,575 30,000 0 0 0 0 0 33,575 15,079 18,496 33,575 Clinical leadership and support for the Training Hub
GP Welcome Back and Legacy Scheme Carried
Forward from
19/20
26,918 0 0 0 0 0 0 26,918 0 26,918 26,918 Scheme carried forward from 19/20 to incentivise practices to support GPs who would otherwise choose to
retire/leve the profession to remain in practice longer whilst legacy planning can be undertaken. In addition
funding available to incentivise practices to ease GPs back into work who wish to return following extended
leave of absence e.g. maternity, sickness, career break etc
GP Mid-Career Scheme (Phoenix GP Programme) Carried
Forward from
19/20
22,625 0 0 0 0 0 0 22,625 2,933 19,693 22,625 To fund Phoenix GP Programme - carried forward from previous year due to covid-19
GP Locum Champion Carried
Forward from
19/20
18,360 0 0 0 0 0 0 18,360 0 18,360 18,360 To fund Locum Champion roles to help develop a locum offer for the STP
General Practice Nurse - PCN Nurse Champions Carried
Forward from
19/20
9,002 0 46,463 0 0 0 0 55,465 450 55,015 55,465 Scheme to facilitate getting the GPN voice heard and involved in the leadership of PCNs and to develop a
structured two way communication process between PCN leads and GPNs on the ground. Needs review and
consideration around funding into current years and beyond
General Practice Nurse - Network and Recognition
Event/Awards
Carried
Forward from
19/20
0 0 10,000 0 0 0 0 10,000 4,000 6,000 10,000 Structured Peer network support and develpoment opportunties for GPNs. Virtual network proposal completed
for first few months of 20/21.
General Practice Nurse - Peer Mentoring and
Preceptorship Support
Carried
Forward from
19/20
46,000 0 0 0 0 0 46,000 5,279 40,721 46,000 GPNs and HCAs have aceess to a structrued peer mentoring scheme, with nurses new in practice having
preceptorship support to help transition them into practice following academic studies
General Practice Nurse - Pipeline Development (includes
GPN Specialty Project)
Carried
Forward from
19/20
148,959 0 0 0 0 0 79,635 228,594 125,214 103,380 228,594 Includes Fundamantals + commissioned from the HEI at £45,314. Awaiting confirmation of Fellowships
Funding for 20/21. Consideration to developing and funding our local Speciality Nurse Programme to further
develop the pipeline. Follow up and outcomes of the speciality training programme currently live to be
reported
General Practice Nurse - GPN Professional Lead/Single
Point of Contact
Carried
Forward from
19/20
22,863 0 50,137 0 0 0 0 73,000 24,129 48,871 73,000 Clinical leadership and support for the Training Hub and delivery of the STP GPN Strategy
CPD for Nurses, Midwives and Allied Health
Professionals 2020/21 to
Mobilised 0 0 0 0 0 189,000 189,000 0 189,000 189,000 Funding from HEE to support skills and capability buidling across the wider primary care workforce
HCA Forum Mobilised 0 9,500 9,500 0 9,500 9,500 Virtual HCA Network across the STP
Pharmacy Network and Pharmacy Ambassador Carried
Forward from
19/20
5,000 5,000 0 0 0 0 8,300 18,300 3,200 15,100 18,300 Peer network support and development opportunities for Pharmacists across system and sectors
Physican Associates Network Mobilised 0 0 0 0 0 0 0 0 0 0 0 To develop a network of support for PA s across the STP in conjunction with Ambassador
Reception and Clerical Skills and Capability Development
(including Practice Manager Network, Mentoring and
Care Navigation - Silver Level)
Design 58,309 28,500 0 0 245,346 0 0 34,500 366,655 8,470 358,185 366,655 Ensure reception and clerical staff have access to schemes to enable continual professinal development, key
updates and pathways to develop into other workforce roles if they wish e.g. HCA, Care Navigators etc
Four Pillars - Medical Education Academy Carried
Forward from
19/20
61,497 63,520 0 0 0 0 0 125,017 60,196 64,821 125,017 Funding has been utilised to develop a medical education programme that Clinical leads have identified as
priorities for general practice staff. The areas which are being progressed in 2019/20 are:
• End of Life: Sage & Thyme foundation level communication training for all staff groups and Advance Care
Planning training for GPs and ANPs
• Paediatrics: Newborn and infant physical examination (NIPE) training for GPs
• Respiratory: asthma treatment resources and launch events for GPs, nurses and clinical pharmacists
• Frailty: workshops for all clinical staff
Other areas to be developed in 2020/21 include diabetes, CVD, mental health, pharmacy and personalisation
for all staff groups.
Training Hub Operational Costs Mobilised 130,736 0 0 130,736 32,684 98,052 130,736 Core funding from HEE to cover infrastructure costs for Training Hubs e.g. staffing and overheads
Training Hub Development and Transtion Plan Delivery Carried
Forward from
19/20
129,610 9,500 0 0 0 0 0 0 139,110 94,187 44,923 139,110 Includes Project Management, Learner Management System, Organisational Development and Training
Needs Analysis
Communications and Publicity Carried
Forward from
19/20
57,375 0 0 0 0 0 0 57,375 57,375 0 57,375 To provide specialist support to produce marketing and branding information to ensure all the workforce have
access to the Hub and its offer. Commissioned support from the CSU.
`
Total 982,440 38,000 319,800 106,600 245,346 130,736 189,000 131,935 2,143,857 647,741 1,496,116 2,143,857
Black Country and West Birmingham STP Training Hub
Financial Monitoring 2020-2021

BCWB STP Training Hub Metrics
GP Scheme Dashboard 2020/2021 as at 14/8/2020
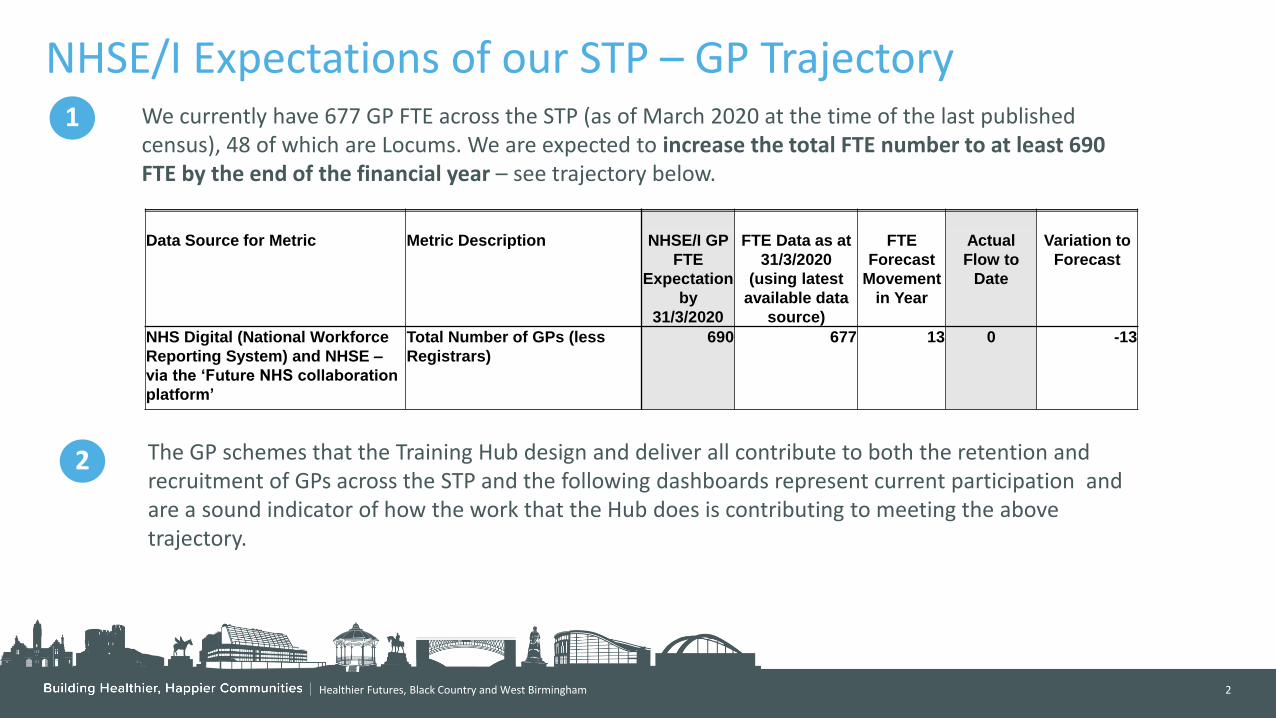
Healthier Futures, Black Country and West Birmingham 2
NHSE/I Expectations of our STP – GP Trajectory
Data Source for Metric Metric Description NHSE/I GP
FTE
Expectation
by
31/3/2020
FTE Data as at
31/3/2020
(using latest
available data
source)
FTE
Forecast
Movement
in Year
Actual
Flow to
Date
Variation to
Forecast
NHS Digital (National Workforce
Reporting System) and NHSE –
via the ‘Future NHS collaboration
platform’
Total Number of GPs (less
Registrars)
690 677 13 0 -13
1 We currently have 677 GP FTE across the STP (as of March 2020 at the time of the last published census), 48 of which are Locums. We are expected to increase the total FTE number to at least 690 FTE by the end of the financial year – see trajectory below.
2 The GP schemes that the Training Hub design and deliver all contribute to both the retention and recruitment of GPs across the STP and the following dashboards represent current participation and are a sound indicator of how the work that the Hub does is contributing to meeting the above trajectory.
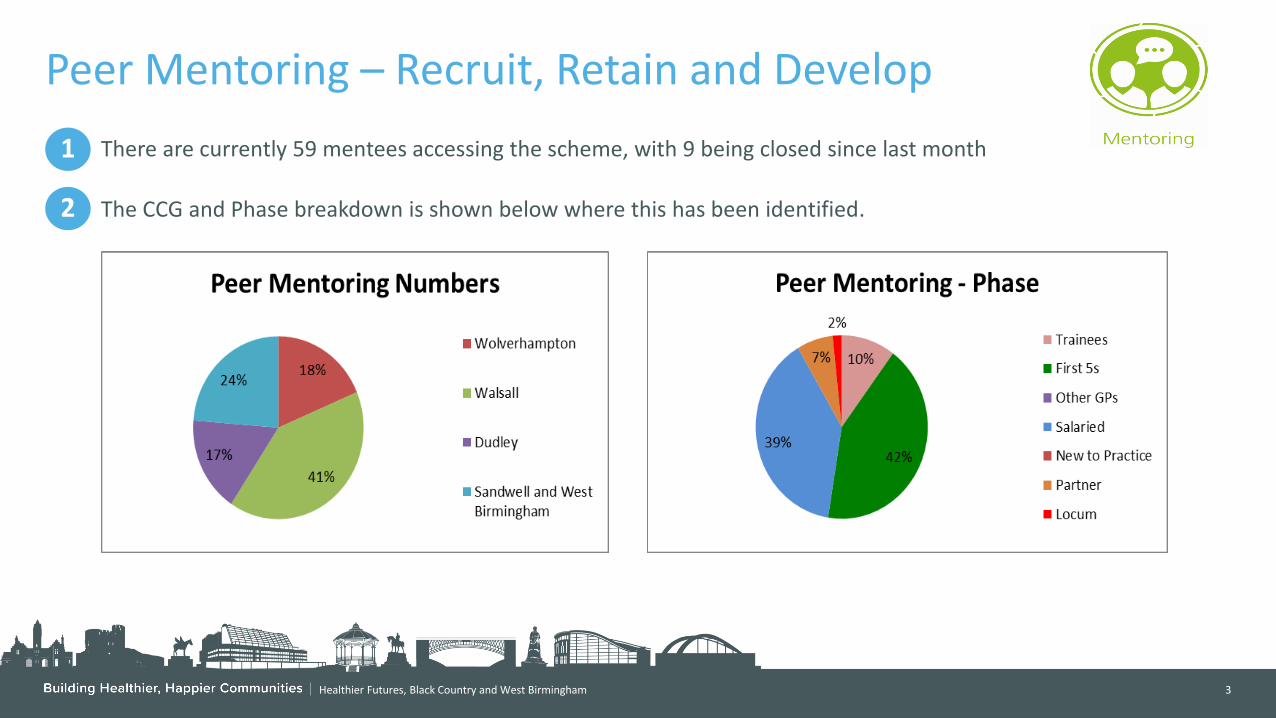
Healthier Futures, Black Country and West Birmingham 3
Peer Mentoring – Recruit, Retain and Develop
1
There are currently 59 mentees accessing the scheme, with 9 being closed since last month
The CCG and Phase breakdown is shown below where this has been identified.
2

Healthier Futures, Black Country and West Birmingham 4
Fellowships and First Five Development – Recruit, Retain and Develop
1
2
Fellowships - A new scheme is being mobilised over the next to recruit up to 28 GP Fellows across the STP during 2020/21. 13 EOI have been received from practices/PCNs across the STP that incorporates each CCG and place. Metric data will be collated and presented in future packs as the scheme moves on. Main outcome is to recruit and retain GPs who have trained and recently qualified across the STP
First 5 Development - A new scheme is currently being mobilised to develop facilitated learning sets for First 5 GPs to support their continual transition into General Practice and to enhance their career development. This scheme will also develop peer support networks which from insight gained from our First 5 Network in that past has proved vital in retaining GPs who are new into roles across general practice. Once this scheme is live the metrics will be reported. Main outcome of this programme is to retain and develop
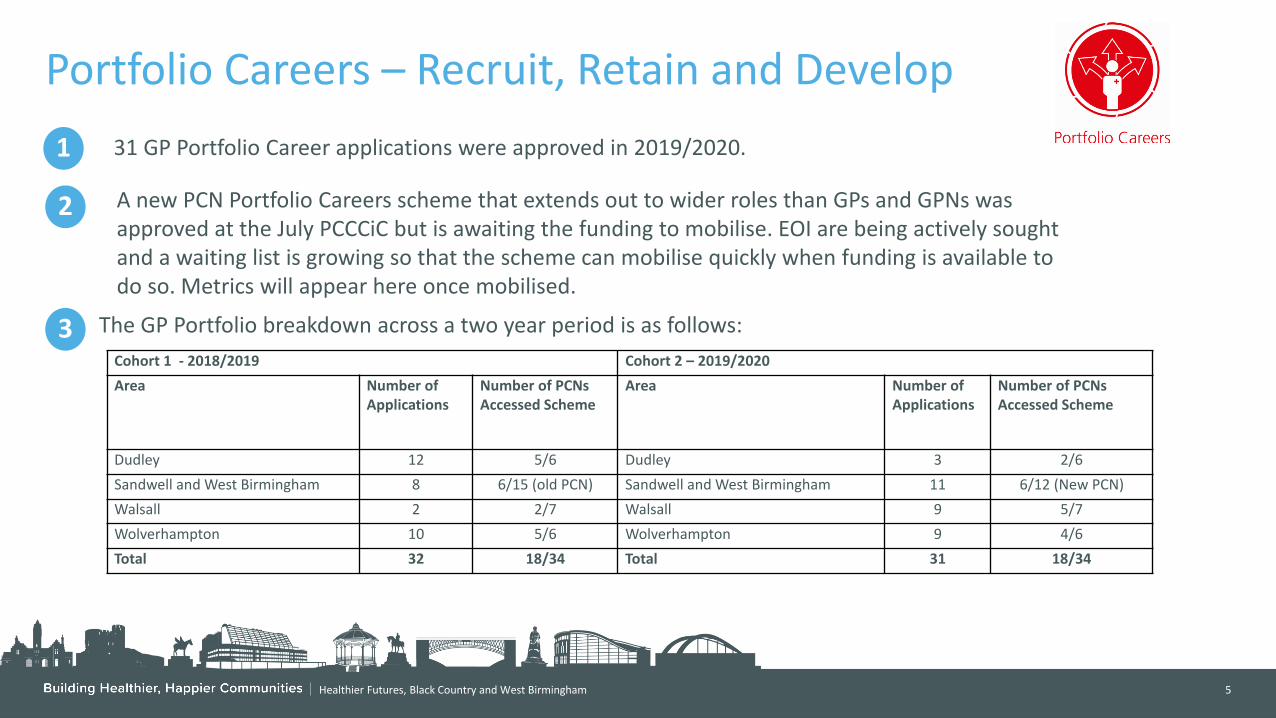
Healthier Futures, Black Country and West Birmingham 5
Portfolio Careers – Recruit, Retain and Develop
1
2
31 GP Portfolio Career applications were approved in 2019/2020.
3
The GP Portfolio breakdown across a two year period is as follows:
Cohort 1 - 2018/2019 Cohort 2 – 2019/2020
Area Number of Applications
Number of PCNs Accessed Scheme
Area Number of Applications
Number of PCNs Accessed Scheme
Dudley 12 5/6 Dudley 3 2/6
Sandwell and West Birmingham 8 6/15 (old PCN) Sandwell and West Birmingham 11 6/12 (New PCN)
Walsall 2 2/7 Walsall 9 5/7
Wolverhampton 10 5/6 Wolverhampton 9 4/6
Total 32 18/34 Total 31 18/34
A new PCN Portfolio Careers scheme that extends out to wider roles than GPs and GPNs was approved at the July PCCCiC but is awaiting the funding to mobilise. EOI are being actively sought and a waiting list is growing so that the scheme can mobilise quickly when funding is available to do so. Metrics will appear here once mobilised.
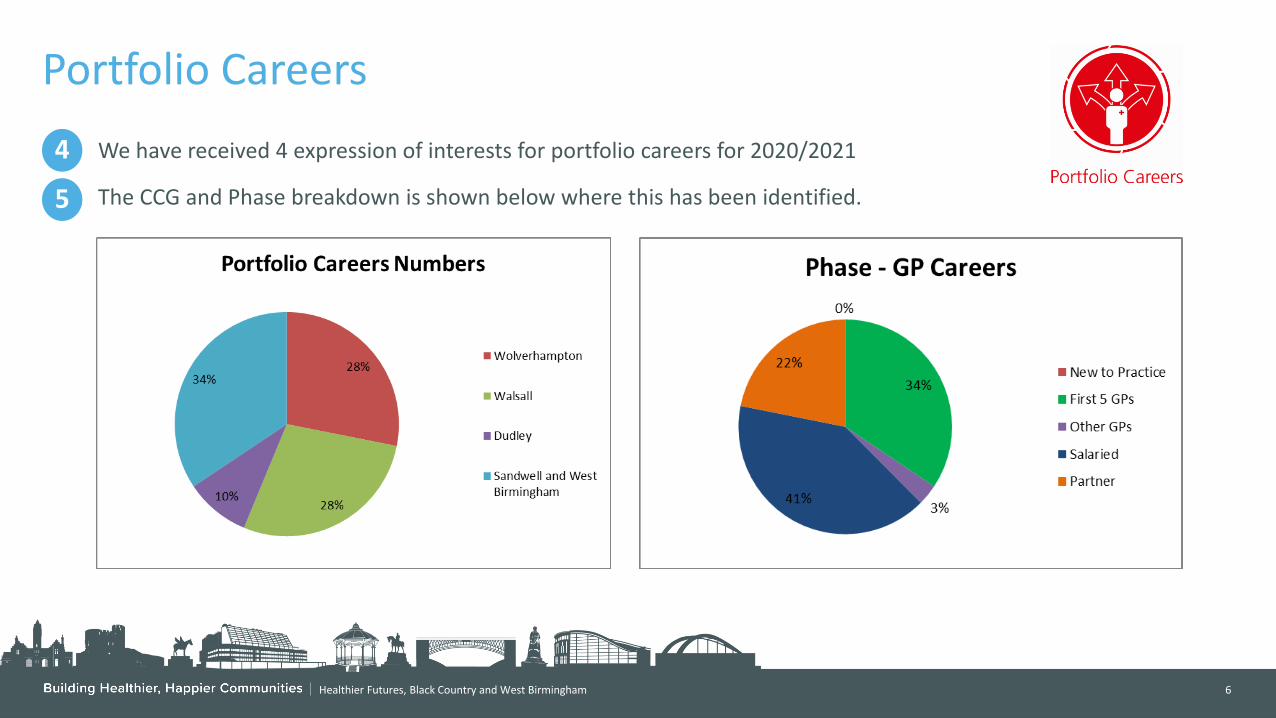
Healthier Futures, Black Country and West Birmingham 6
Portfolio Careers
5
The CCG and Phase breakdown is shown below where this has been identified.
4
We have received 4 expression of interests for portfolio careers for 2020/2021

Healthier Futures, Black Country and West Birmingham 7
Portfolio Careers Summary of Portfolio Specialties 2019/2020 Cohort 2
CCG PCN Portfolio Speciality
Dudley Dudley and Netherton Diabetes
Dudley Dudley and Netherton Pain Management
Dudley Stourbridge, Wollescote & Lye Neurolinguistic Programming and Coaching
Walsall West One Paediatrics and Child Health
Walsall West One Woman's Health
Walsall West One Palliative Care
Walsall East Two Sexual and Reproductive Health
Walsall East Two Mental Health
Walsall East Two Mental Health
Walsall West Two Minor Surgery
Walsall South 1 Pain Management
Walsall North Women's Health

Healthier Futures, Black Country and West Birmingham 8
Portfolio Careers Summary of Portfolio Specialties 2019/2020 Cohort 2
CCG PCN Portfolio Speciality
Sandwell and West Birmingham I3 Women’s health
Sandwell and West Birmingham Central Healthcare Partnership Medical Education
Sandwell and West Birmingham Newcomen Minor Surgery
Sandwell and West Birmingham Urban Health Gynaecology
Sandwell and West Birmingham Urban Health Medical Education
Sandwell and West Birmingham Your Health Partnership Life Style Medicine
Sandwell and West Birmingham Your Health Partnership Palliative Care
Sandwell and West Birmingham Citrus Health Urology
Sandwell and West Birmingham Citrus Health Medical Education
Sandwell and West Birmingham I3 Diabetes
Sandwell and West Birmingham I3 Cardiology
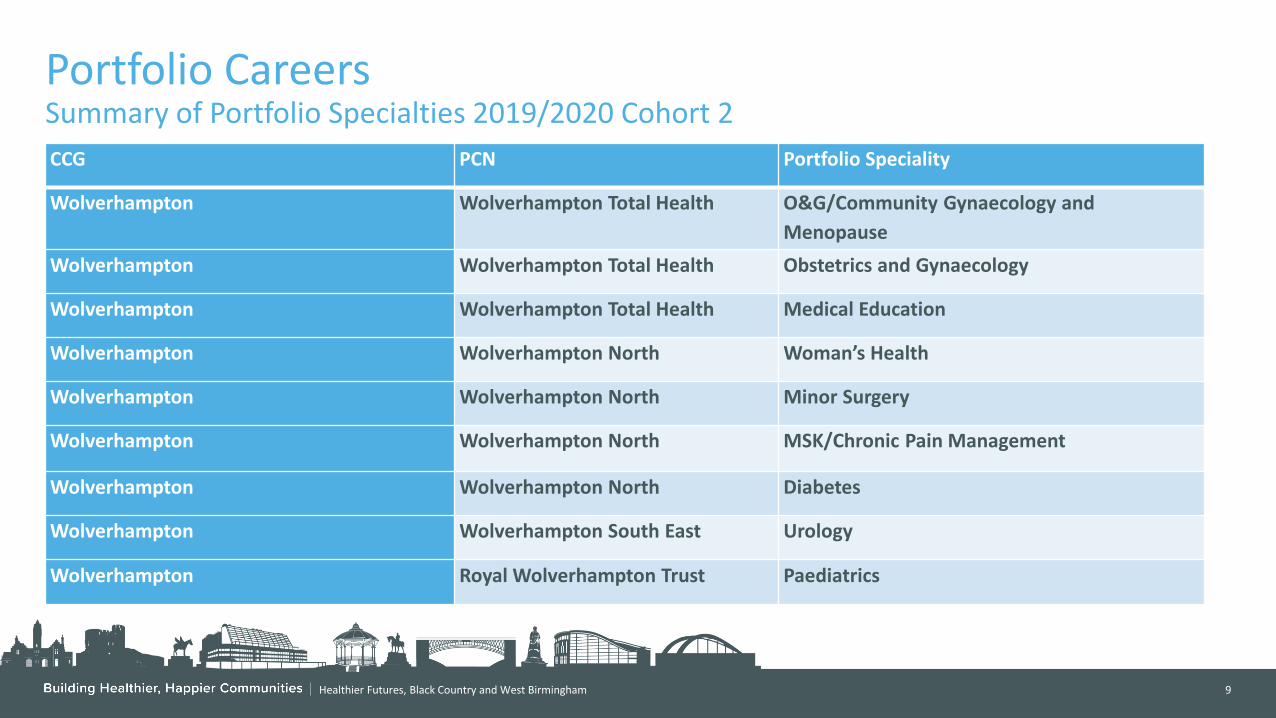
Healthier Futures, Black Country and West Birmingham 9
Portfolio Careers Summary of Portfolio Specialties 2019/2020 Cohort 2
CCG PCN Portfolio Speciality
Wolverhampton Wolverhampton Total Health O&G/Community Gynaecology and
Menopause
Wolverhampton Wolverhampton Total Health Obstetrics and Gynaecology
Wolverhampton Wolverhampton Total Health Medical Education
Wolverhampton Wolverhampton North Woman’s Health
Wolverhampton Wolverhampton North Minor Surgery
Wolverhampton Wolverhampton North MSK/Chronic Pain Management
Wolverhampton Wolverhampton North Diabetes
Wolverhampton Wolverhampton South East Urology
Wolverhampton Royal Wolverhampton Trust Paediatrics
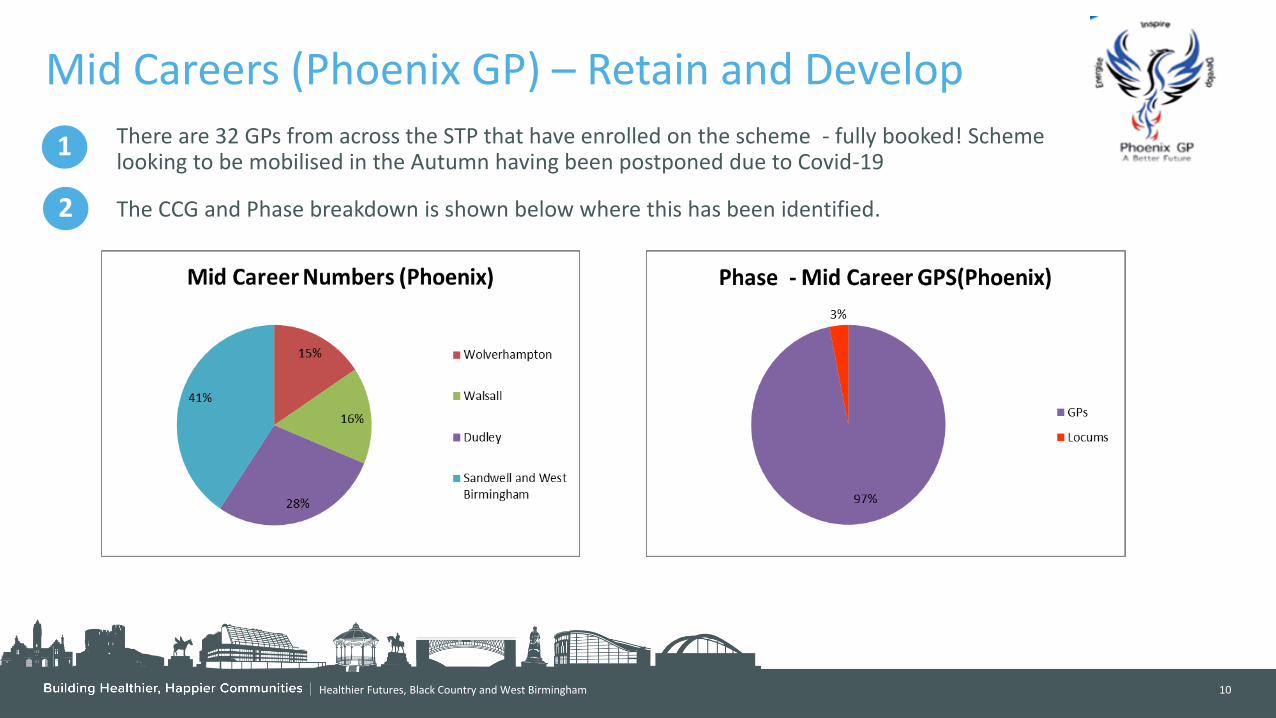
Healthier Futures, Black Country and West Birmingham 10
Mid Careers (Phoenix GP) – Retain and Develop
1
There are 32 GPs from across the STP that have enrolled on the scheme - fully booked! Scheme looking to be mobilised in the Autumn having been postponed due to Covid-19
The CCG and Phase breakdown is shown below where this has been identified.
2
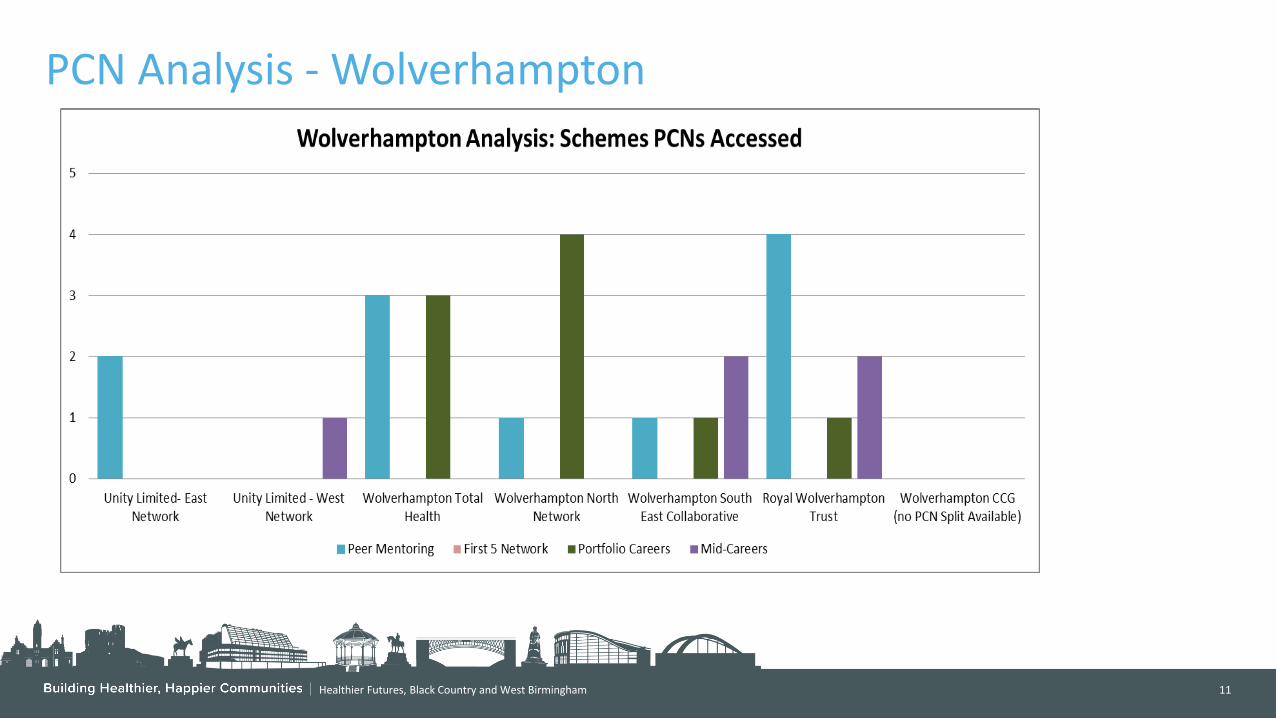
Healthier Futures, Black Country and West Birmingham 11
PCN Analysis - Wolverhampton
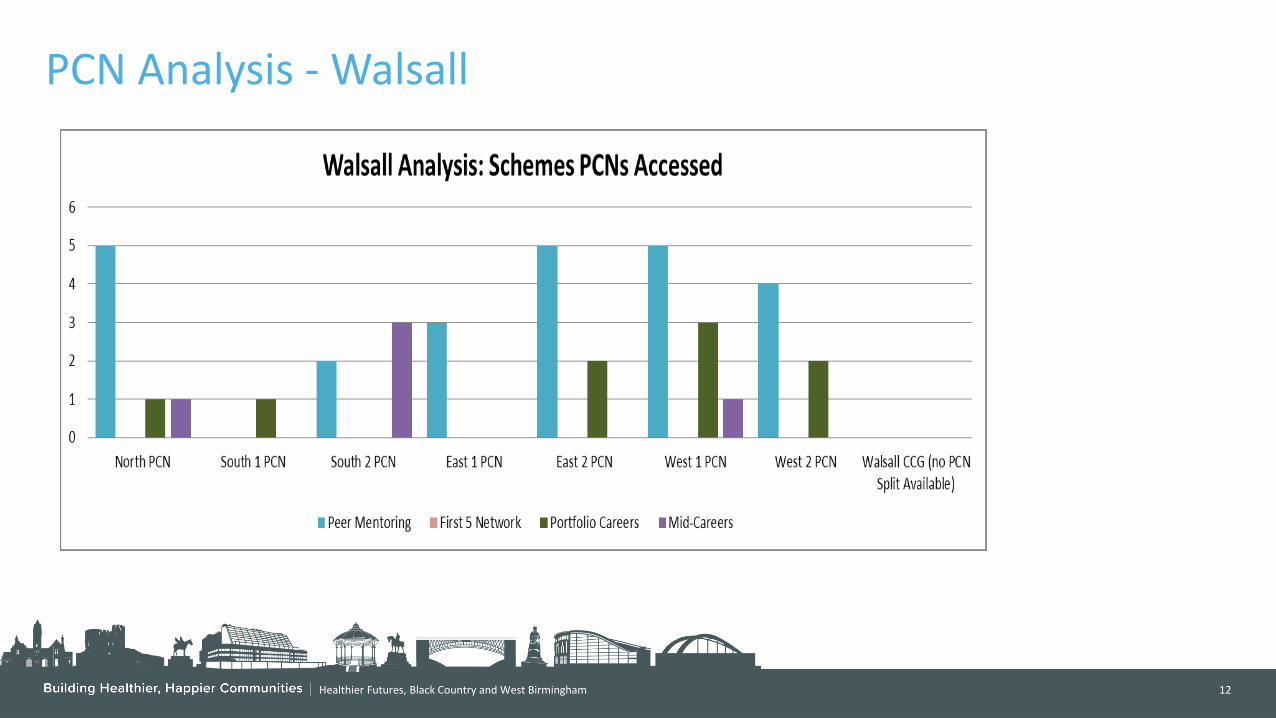
Healthier Futures, Black Country and West Birmingham 12
PCN Analysis - Walsall
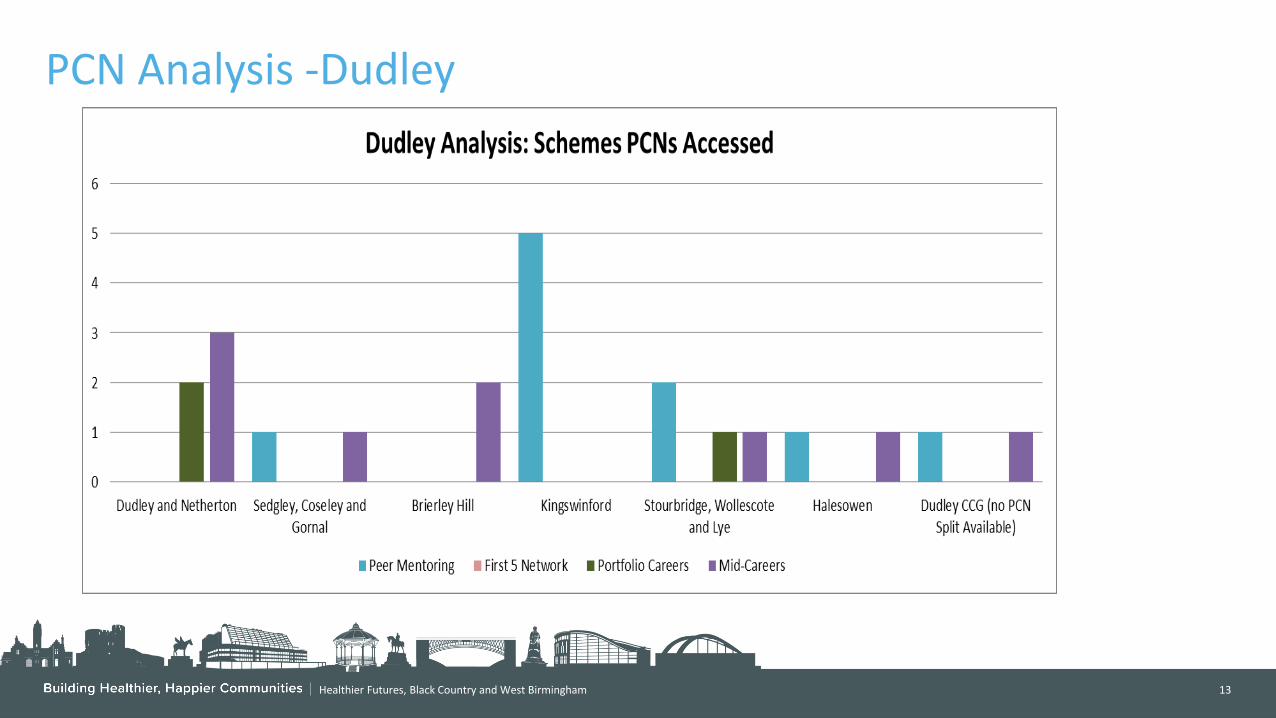
Healthier Futures, Black Country and West Birmingham 13
PCN Analysis -Dudley

Healthier Futures, Black Country and West Birmingham 14
PCN Analysis – Sandwell and West Birmingham

BCWB STP Training Hub
GPN Scheme Dashboard 2020/2021 as at 14/08/2020
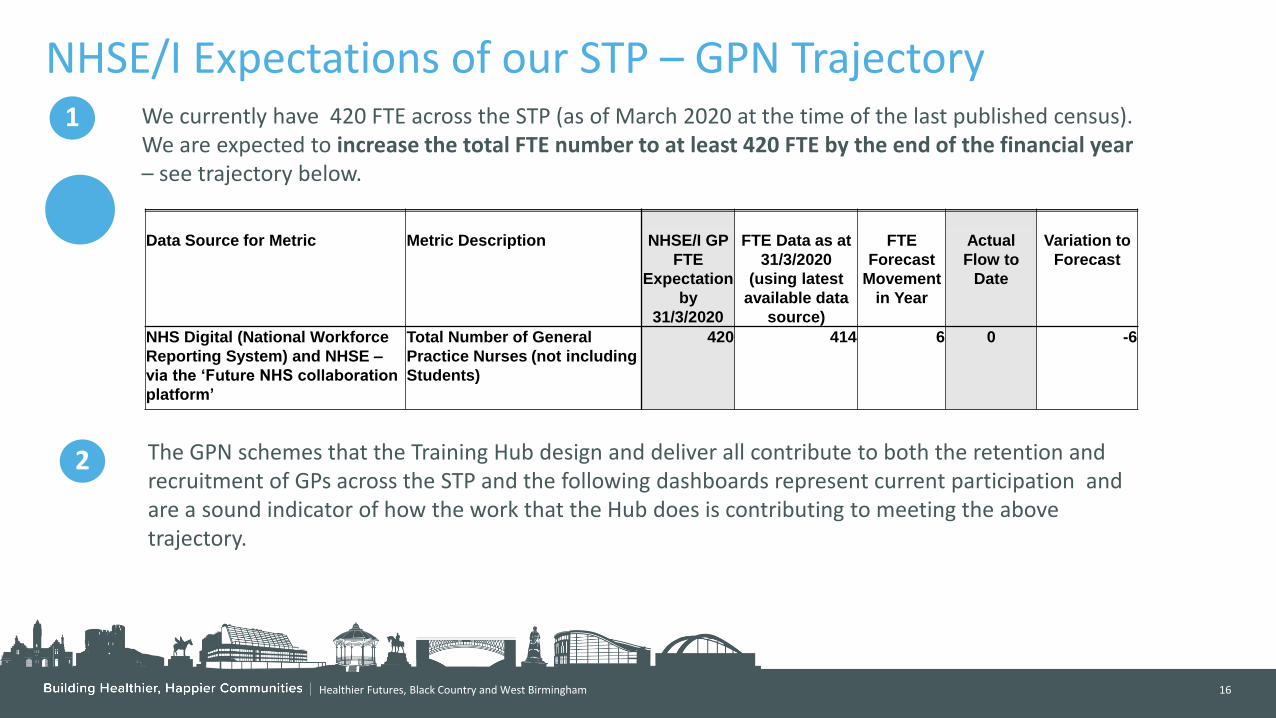
Healthier Futures, Black Country and West Birmingham 16
NHSE/I Expectations of our STP – GPN Trajectory
Data Source for Metric Metric Description NHSE/I GP
FTE
Expectation
by
31/3/2020
FTE Data as at
31/3/2020
(using latest
available data
source)
FTE
Forecast
Movement
in Year
Actual
Flow to
Date
Variation to
Forecast
NHS Digital (National Workforce
Reporting System) and NHSE –
via the ‘Future NHS collaboration
platform’
Total Number of General
Practice Nurses (not including
Students)
420 414 6 0 -6
1 We currently have 420 FTE across the STP (as of March 2020 at the time of the last published census). We are expected to increase the total FTE number to at least 420 FTE by the end of the financial year – see trajectory below.
2 The GPN schemes that the Training Hub design and deliver all contribute to both the retention and recruitment of GPs across the STP and the following dashboards represent current participation and are a sound indicator of how the work that the Hub does is contributing to meeting the above trajectory.

Healthier Futures, Black Country and West Birmingham 17
GPN Nurse Forums – Retain and Develop
1 All April 2020 Nurse Forums were cancelled due to COVID- 19. Since May 2020 the Nurse Forums will be delivered virtually and topics and speakers have been confirmed for the next three months.
2 Topics over the last month have included Womans Menopause, Asthma & Allergy in Children, Allergic Rhinitis
and Introduction to Venepuncture – over 270 of our nurses have attended one or more of these over the month which represents almost half the headcount of nurses across the STP
3
The split in attendance by CCG can be found below.

Healthier Futures, Black Country and West Birmingham 18
GPN Champions – Retain and Develop
1 10 General Practice Nurse Champions have been appointed.
2 The Champions are being overseen by Liz Corrigan, GPN Professional Lead, who has met with each of them individually and will arrange regular group meetings throughout the year. A two day leadership development programme has been commissioned from the RCN to support the Champions in their role.
20%
10%
20%
50%
GPN Champions
Wolverhampton
Walsall
Dudley
Sandwell and WestBirmingham
3
The split by CCG can be found below.
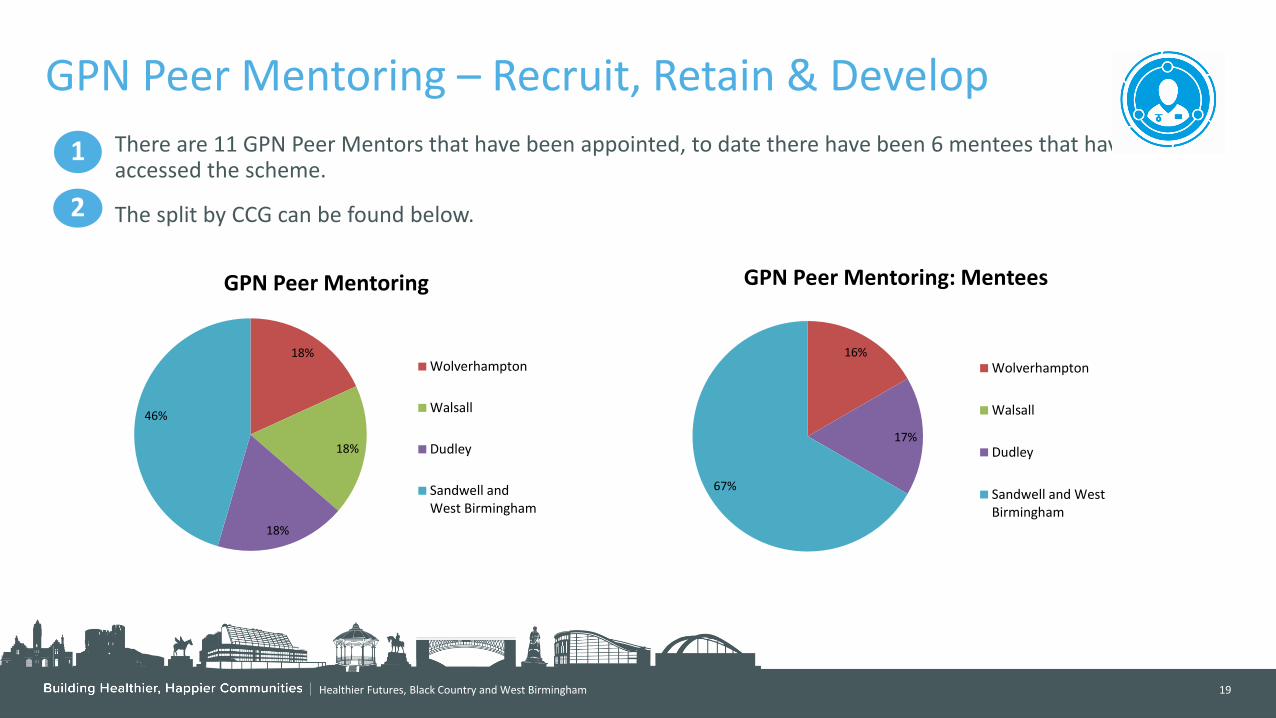
Healthier Futures, Black Country and West Birmingham 19
GPN Peer Mentoring – Recruit, Retain & Develop
1 There are 11 GPN Peer Mentors that have been appointed, to date there have been 6 mentees that have accessed the scheme.
2 The split by CCG can be found below.
18%
18%
18%
46%
GPN Peer Mentoring
Wolverhampton
Walsall
Dudley
Sandwell andWest Birmingham
16%
17%
67%
GPN Peer Mentoring: Mentees
Wolverhampton
Walsall
Dudley
Sandwell and WestBirmingham

Healthier Futures, Black Country and West Birmingham 20
GPN Specialty Training – Recruit
1 There are 9 GPNs who have accessed the GPN Specialty Training Programme
The split by CCG can be found below. 2
12%
50%
13%
25%
GPN Specialty Training
Wolverhampton
Walsall
Dudley
Sandwell and West Birmingham

Healthier Futures, Black Country and West Birmingham 21
PCN Analysis - Wolverhampton
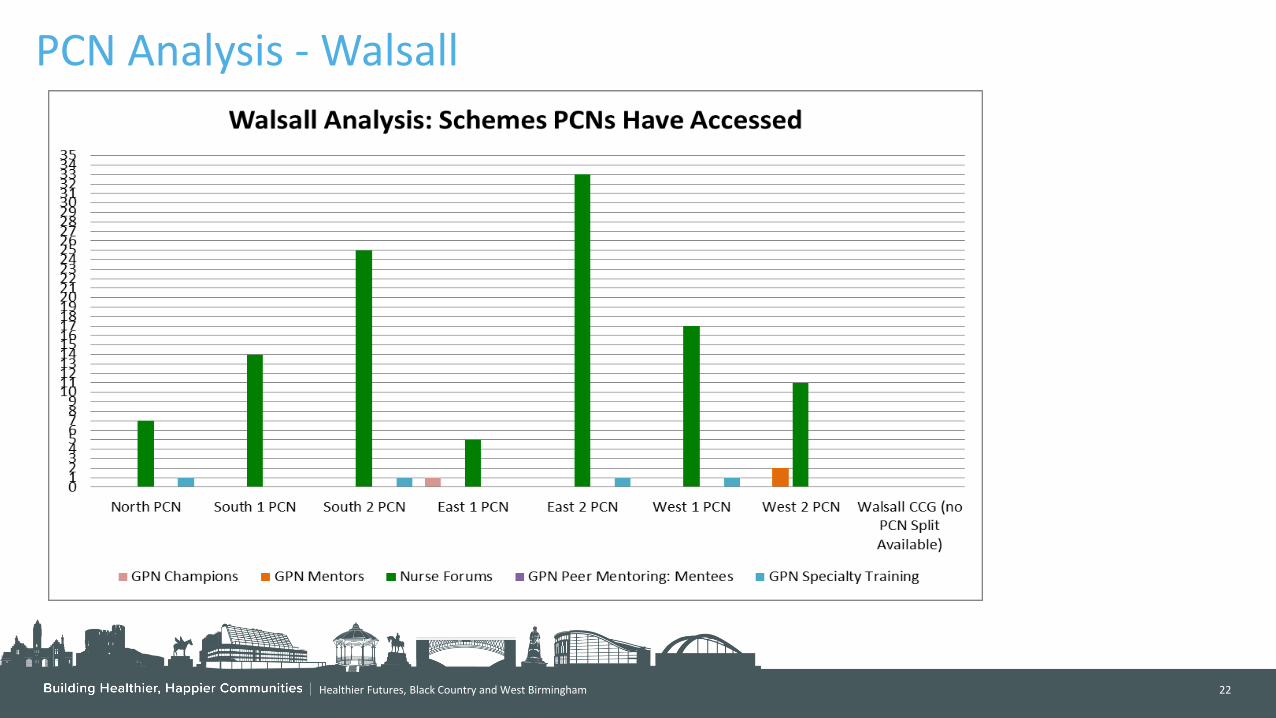
Healthier Futures, Black Country and West Birmingham 22
PCN Analysis - Walsall

Healthier Futures, Black Country and West Birmingham 23
PCN Analysis -Dudley

Healthier Futures, Black Country and West Birmingham 24
PCN Analysis – Sandwell and West Birmingham

BCWB STP Training Hub
Other Schemes Dashboard 2020/2021 as at 14/8/2020

Healthier Futures, Black Country and West Birmingham 26
Physical Health Assessment Level 6
1 2
The split by CCG can be found below;
The staff numbers allocated are:
• Wolverhampton – 1
• Walsall – 3
• Dudley - 4
• Sandwell and West Birmingham - 3
9%
27%
37%
27%
Physical Health Assessment Level 6
Wolverhampton
Walsall
Dudley
Sandwell andWest Birmingham
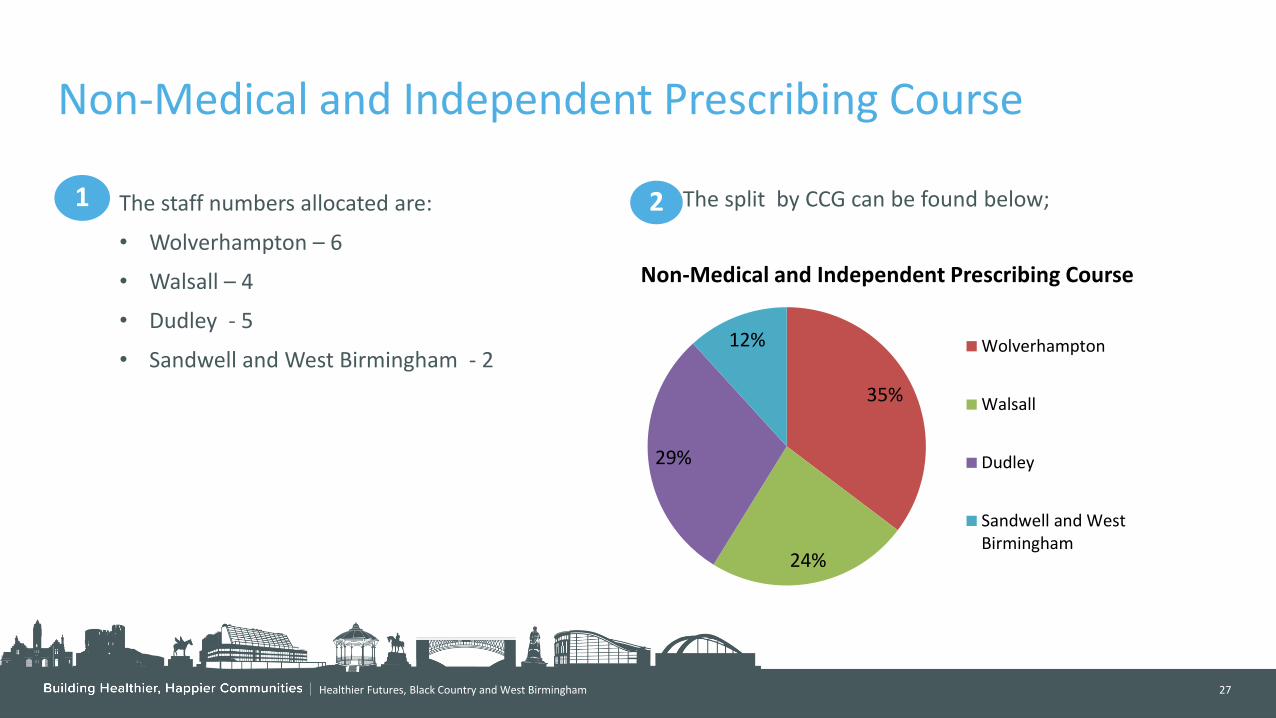
Healthier Futures, Black Country and West Birmingham 27
Non-Medical and Independent Prescribing Course
35%
24%
29%
12%
Non-Medical and Independent Prescribing Course
Wolverhampton
Walsall
Dudley
Sandwell and WestBirmingham
2
The split by CCG can be found below;
1 The staff numbers allocated are:
• Wolverhampton – 6
• Walsall – 4
• Dudley - 5
• Sandwell and West Birmingham - 2
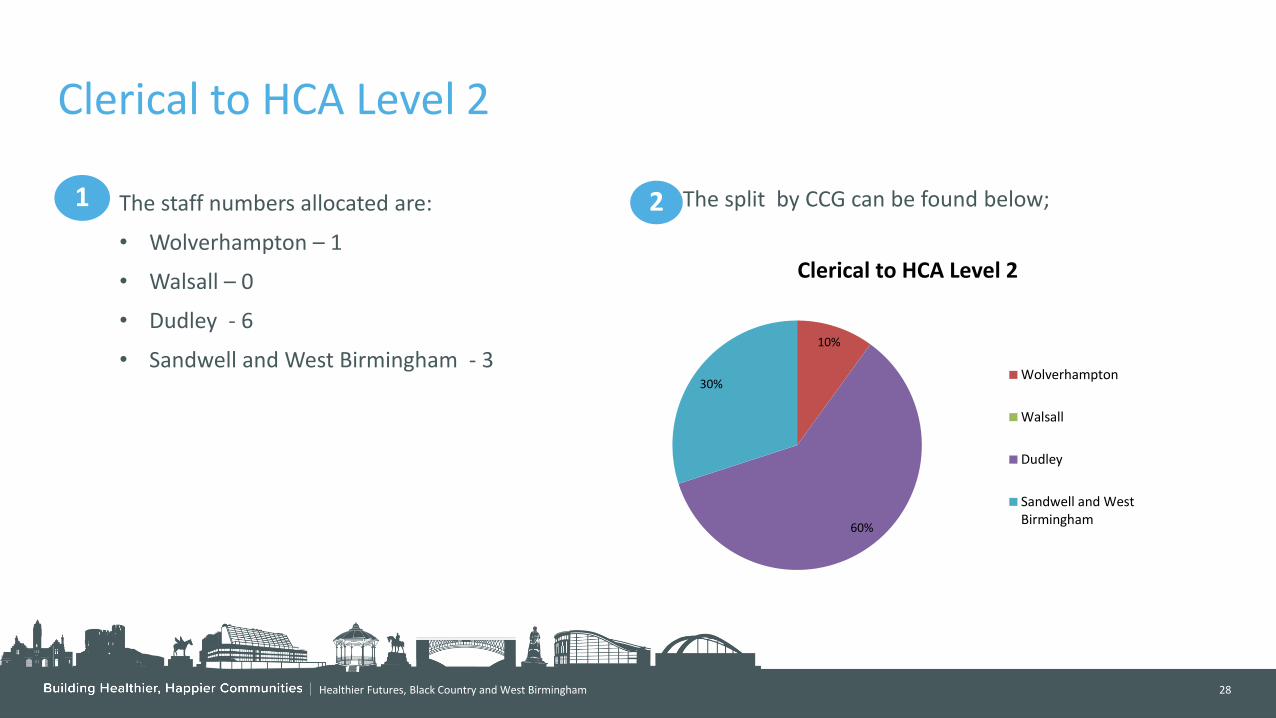
Healthier Futures, Black Country and West Birmingham 28
Clerical to HCA Level 2
2
The split by CCG can be found below;
1 The staff numbers allocated are:
• Wolverhampton – 1
• Walsall – 0
• Dudley - 6
• Sandwell and West Birmingham - 3 10%
60%
30%
Clerical to HCA Level 2
Wolverhampton
Walsall
Dudley
Sandwell and WestBirmingham
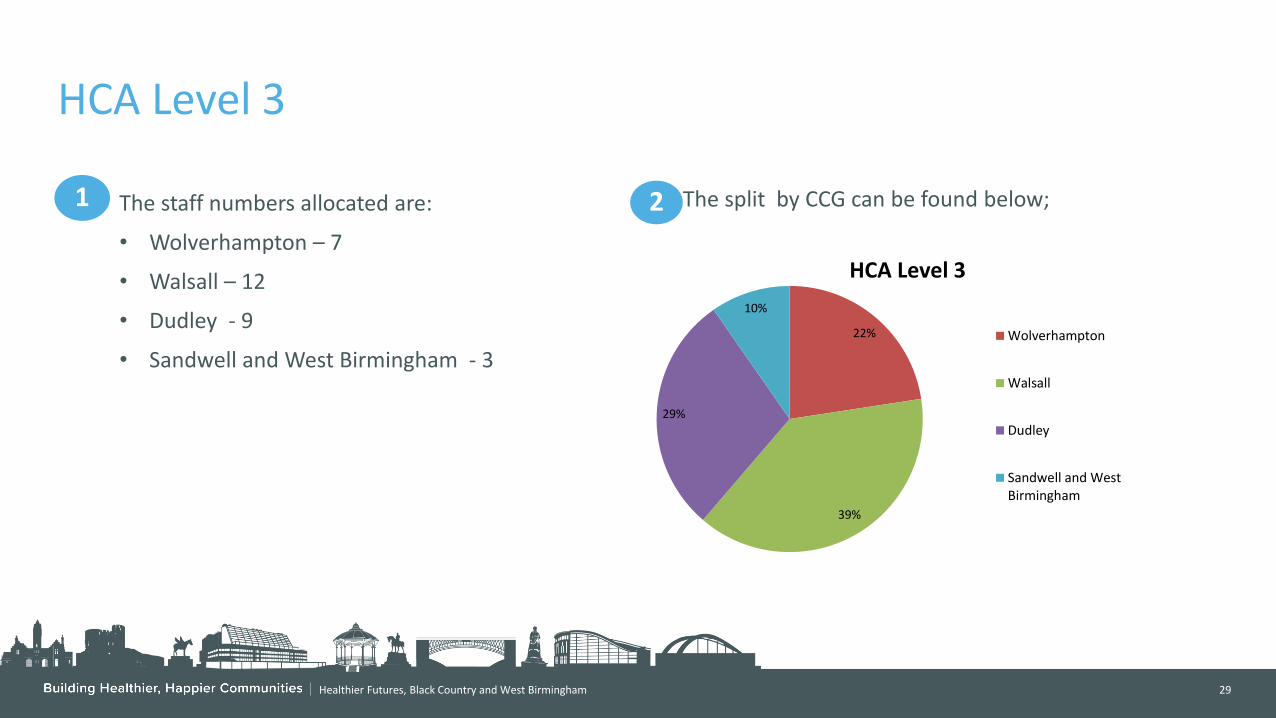
Healthier Futures, Black Country and West Birmingham 29
HCA Level 3
2
The split by CCG can be found below;
1 The staff numbers allocated are:
• Wolverhampton – 7
• Walsall – 12
• Dudley - 9
• Sandwell and West Birmingham - 3
22%
39%
29%
10%
HCA Level 3
Wolverhampton
Walsall
Dudley
Sandwell and WestBirmingham

Healthier Futures, Black Country and West Birmingham 30
Video Consultation
2
The split by CCG can be found below;
1 There have been 6 practices that have expressed an interest in video consultation.
3
4
Briefings have been offered which will be held before the training to allow practices to gain greater understanding
The dates for the training are being currently being arranged and will be confirmed shortly.
33%
17%
33%
17%
Video Consultataions
Wolverhampton
Walsall
Dudley
Sandwell and West Birmingham

Healthier Futures, Black Country and West Birmingham 31
PCN Analysis - Wolverhampton
0
1
2
3
Unity Limited- East Network Unity Limited - WestNetwork
Wolverhampton Total Health Wolverhampton NorthNetwork
Wolverhampton South EastCollaborative
Royal Wolverhampton Trust Wolverhampton CCG (noPCN Split Available)
Wolverhampton Analysis: Schemes PCNs Have Accessed
Physical Health Assessment Level 6 Non-Medical and Idependent Prescribing Course Clerical to HCA Level 2 HCA Level 3 Video Consultations

Healthier Futures, Black Country and West Birmingham 32
PCN Analysis - Walsall
0
1
2
3
4
North PCN South 1 PCN South 2 PCN East 1 PCN East 2 PCN West 1 PCN West 2 PCN Walsall CCG (no PCN SplitAvailable)
Walsall Analysis: Schemes PCNs Have Accessed
Non-Medical and Independent Prescribing Clerical To HCA Level 2 HCA Level 3 Video Consultations

Healthier Futures, Black Country and West Birmingham 33
PCN Analysis - Dudley
0
1
2
3
4
5
6
7
Dudley and Netherton Sedgley, Coseley and Gornal Brierley Hill Kingswinford Stourbridge, Wollescote andLye
Halesowen Dudley CCG (no PCN SplitAvailable)
Dudley Analysis: Schemes PCNs Have Accessed
Physical Health Assessment Level 6 Non-Medical and Independent Prescribing Clerical To HCA Level 2 HCA Level 3 Video Consultations
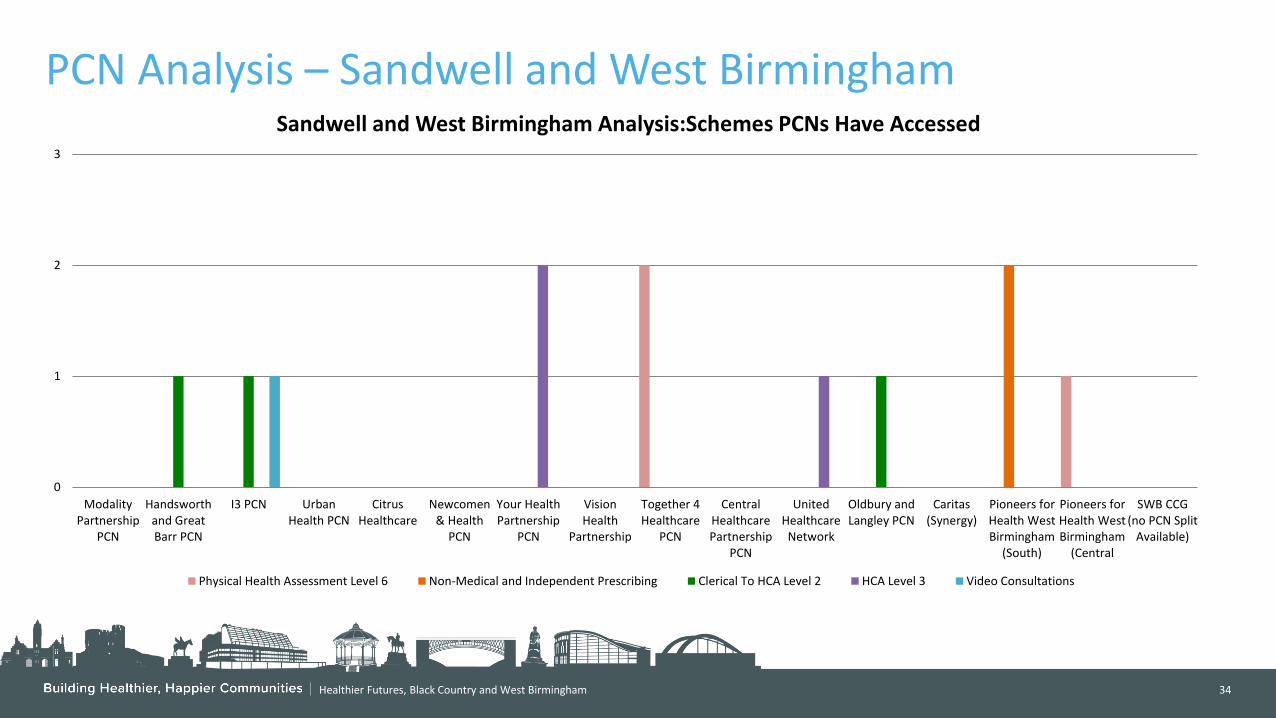
Healthier Futures, Black Country and West Birmingham 34
PCN Analysis – Sandwell and West Birmingham
0
1
2
3
ModalityPartnership
PCN
Handsworthand GreatBarr PCN
I3 PCN UrbanHealth PCN
CitrusHealthcare
Newcomen& Health
PCN
Your HealthPartnership
PCN
VisionHealth
Partnership
Together 4Healthcare
PCN
CentralHealthcarePartnership
PCN
UnitedHealthcare
Network
Oldbury andLangley PCN
Caritas(Synergy)
Pioneers forHealth WestBirmingham
(South)
Pioneers forHealth WestBirmingham
(Central
SWB CCG(no PCN Split
Available)
Sandwell and West Birmingham Analysis:Schemes PCNs Have Accessed
Physical Health Assessment Level 6 Non-Medical and Independent Prescribing Clerical To HCA Level 2 HCA Level 3 Video Consultations

Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Primary Care Operational Group (PCOG) Assurance Report

PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: Tuesday 25 August 2020 AGENDA ITEM: 16.0
Title of Report: Primary Care Operational Group (PCOG) Assurance Report
Purpose of Report: To provide assurance on Primary Issues to PCCCic
Author of Report: Carla Evans, Carol Marston, Julie Robinson, Gill Shelley
Management Lead/Signed off by: Sarah Southall
Public or Private: Public
Key Points:
Assurance on primary care issues provided from notes of Primary Care Operational Group Meetings from:
• Dudley CCG • Sandwell and West Birmingham CCG • Walsall CCG • Wolverhampton CCG
Recommendation: PCCCic accept the paper as assurance on primary care issues.
Conflicts of Interest: N/A
Links to Corporate Objectives:
Action Required: Assurance
Implications:
Financial N/A
Assurance Framework N/A
Risks and Legal Obligations N/A
Equality & Diversity N/A
Other N/A
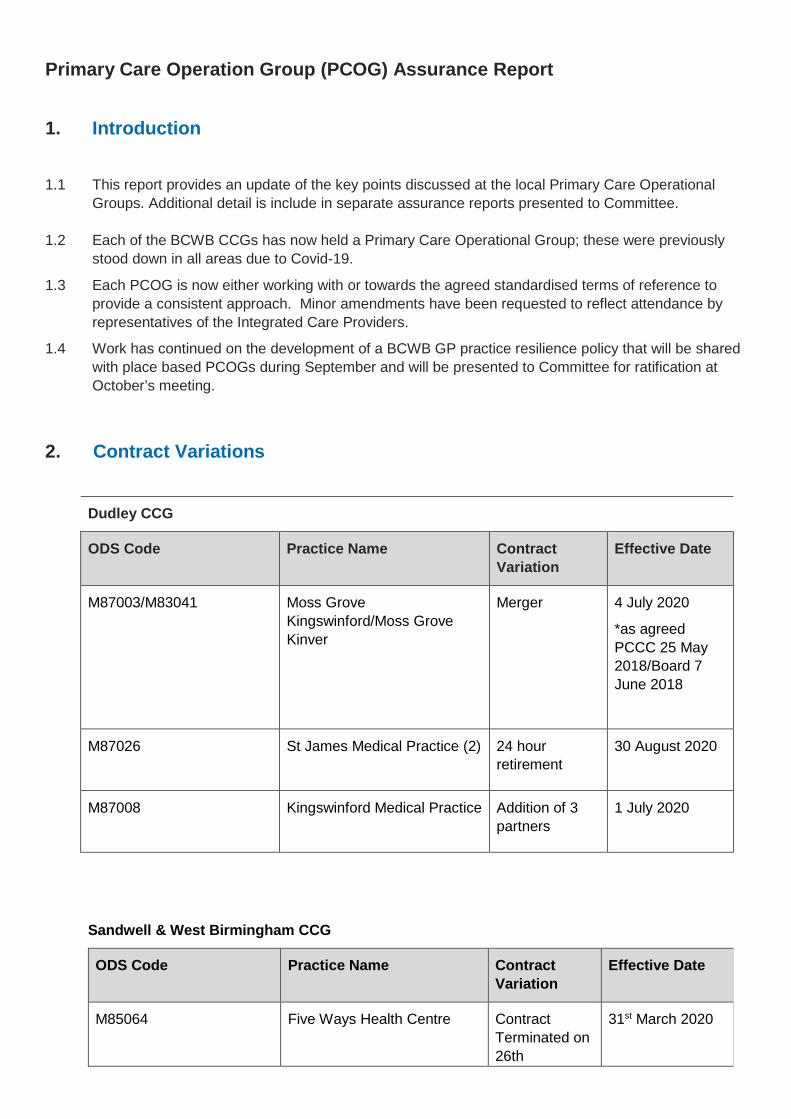
Primary Care Operation Group (PCOG) Assurance Report 1. Introduction 1.1 This report provides an update of the key points discussed at the local Primary Care Operational
Groups. Additional detail is include in separate assurance reports presented to Committee.
1.2 Each of the BCWB CCGs has now held a Primary Care Operational Group; these were previously stood down in all areas due to Covid-19.
1.3 Each PCOG is now either working with or towards the agreed standardised terms of reference to provide a consistent approach. Minor amendments have been requested to reflect attendance by representatives of the Integrated Care Providers.
1.4 Work has continued on the development of a BCWB GP practice resilience policy that will be shared with place based PCOGs during September and will be presented to Committee for ratification at October’s meeting.
2. Contract Variations
Dudley CCG
ODS Code Practice Name Contract Variation
Effective Date
M87003/M83041
Moss Grove Kingswinford/Moss Grove Kinver
Merger 4 July 2020
*as agreed PCCC 25 May 2018/Board 7 June 2018
M87026
St James Medical Practice (2) 24 hour retirement
30 August 2020
M87008
Kingswinford Medical Practice Addition of 3 partners
1 July 2020
Sandwell & West Birmingham CCG
ODS Code Practice Name Contract Variation
Effective Date
M85064 Five Ways Health Centre Contract Terminated on 26th
31st March 2020

September 2019. Caretakers in place until list dispersal completion
M85663 Bloomsbury Health Centre Contract terminated on 5th July 19 Caretaking Practice in place until list dispersal completion
31st March 2020
M88021 Dr S Jemahl
Newton Road Great Barr
Contract merger with:
M88024 Sundial Surgery
M88623 Park House Surgery
Clinical systems merger took place on 9th July and 15th July 2020 successfully.
The Practice is now known as Scott Arms Medical Centre and will relocate into a new build in September 2020.
The CCG now has 75 Practices operating from 99 sites.
1st July 2020
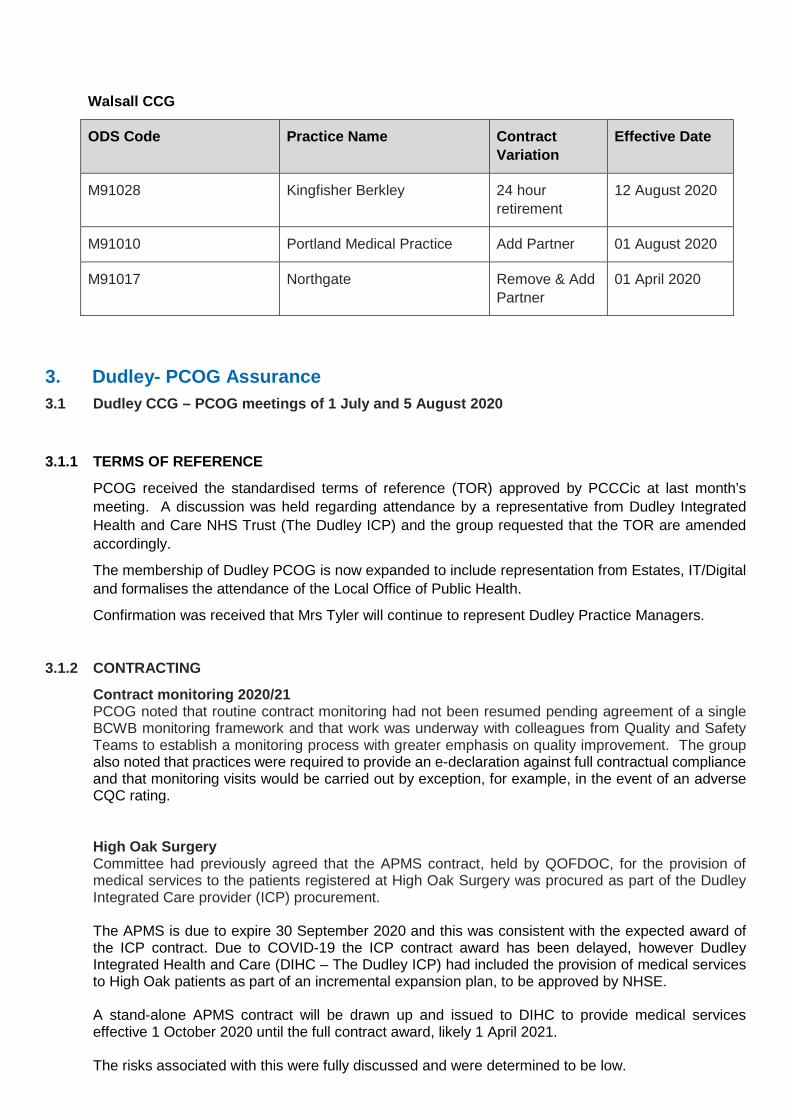
Walsall CCG
ODS Code Practice Name Contract Variation
Effective Date
M91028 Kingfisher Berkley 24 hour retirement
12 August 2020
M91010 Portland Medical Practice Add Partner 01 August 2020
M91017 Northgate Remove & Add Partner
01 April 2020
3. Dudley- PCOG Assurance 3.1 Dudley CCG – PCOG meetings of 1 July and 5 August 2020
3.1.1 TERMS OF REFERENCE
PCOG received the standardised terms of reference (TOR) approved by PCCCic at last month’s meeting. A discussion was held regarding attendance by a representative from Dudley Integrated Health and Care NHS Trust (The Dudley ICP) and the group requested that the TOR are amended accordingly.
The membership of Dudley PCOG is now expanded to include representation from Estates, IT/Digital and formalises the attendance of the Local Office of Public Health.
Confirmation was received that Mrs Tyler will continue to represent Dudley Practice Managers.
3.1.2 CONTRACTING
Contract monitoring 2020/21 PCOG noted that routine contract monitoring had not been resumed pending agreement of a single BCWB monitoring framework and that work was underway with colleagues from Quality and Safety Teams to establish a monitoring process with greater emphasis on quality improvement. The group also noted that practices were required to provide an e-declaration against full contractual compliance and that monitoring visits would be carried out by exception, for example, in the event of an adverse CQC rating.
High Oak Surgery Committee had previously agreed that the APMS contract, held by QOFDOC, for the provision of medical services to the patients registered at High Oak Surgery was procured as part of the Dudley Integrated Care provider (ICP) procurement.
The APMS is due to expire 30 September 2020 and this was consistent with the expected award of the ICP contract. Due to COVID-19 the ICP contract award has been delayed, however Dudley Integrated Health and Care (DIHC – The Dudley ICP) had included the provision of medical services to High Oak patients as part of an incremental expansion plan, to be approved by NHSE. A stand-alone APMS contract will be drawn up and issued to DIHC to provide medical services effective 1 October 2020 until the full contract award, likely 1 April 2021. The risks associated with this were fully discussed and were determined to be low.
Moss Grove Surgery PCOG was informed that Moss Grove Kinver transferred from NHS South East Staffordshire & Seisdon Peninsula CCG into Dudley CCG effective 1 April 2020 and that the merger with Kingswinford and Kinver had been completed, effective July 2020. Kinver is now a branch of Kingswinford.
There are some issues outstanding regarding the digital solution that require civil works to be carried out – assurance was provided that this is not causing the practice any problems and that an update would be provided at next month’s meeting.
3.1.3 PRIMARY CARE NETWORK DES (PCN DES)
PCOG noted that the PCN DES review group will be resurrected and that the terms of reference will
be reviewed to include the PCN manager as the first point of contact and that all Clinical Directors would not be required to be present for routine monitoring and assurance.
3.1.4 PRIMARY CARE COMMISSIONING Dudley Quality Outcomes for Health (DQOFH) A review of the indicators has been undertaken in respect of COVID-19 and the business rules amend accordingly. Guidance had been published by the diabetes society, this is being reviewed and amendments may be required to the relevant indicators. Practices have received assurance that income is protected during the pandemic, pending further guidance from NHSE. Any changes to DQOFH will be made in line with National QoF Two practices continue to deliver against the National QOF. Dudley Quality Outcomes for Health (DQOFH) reviews 14 Practices had been identified as requiring a review visit, 6 had been completed prior to COVID-19 and virtual meetings are being arranged for the remaining practices.
PCOG was assured that no significant issues had been found and that best practice guidance is being drawn up regarding exception reporting.
3.1.5 INTEGRATED CARE TEAMS Three virtual Integrated Care Team (ICT) meetings have now taken place in Halesowen and Stourbridge. The CCG has recruited 3 additional ICT GP leads who were expected to be in post from the 1 August 2020, but this has now been delayed until 1st September. A suggestion will be taken forward to develop specific paediatric ICT models in the future. Assurance had been received that all participants of the ICT meeting had access to all relevant IT equipment.
3.1.6 PRIMARY CARE QUALITY & SAFETY
PCOG received the primary care quality and safety matters and the following discussions were held. The items are set out in detail in the Quality and Safety report to Committee, key points discussed included:

Flu programme Discussion was held regarding the National guidance clarifying the expansion of patient cohorts and the national ambitions for the 2020/21 flu programme. PCOG was advised that a Dudley flu planning focus group had been established and was being clinically led by Dr Fiona Rose with management support provided by the local Quality and Safety Team. Challenges and feedback around issues such as funding and income protection, the transfer of vaccines and communication strategies were being feed into the West Midlands Regional Local Authority and flu leads meetings for escalation to national meetings.
CQC
The local CQC Inspector explained that CQC routine inspections and Annual Regulatory Reviews (ARRs) had been placed on hold due to Covid-19. However Emergency Support Framework (ESF) calls were being made to practices during this time. The group received an update regarding the progress of Dudley Wood Surgery.
Primary Care Analysis Tool
PCOG was advised that the full PCAT dataset will be presented to the group at the next meeting along with the findings from the GP patient survey.
IRIS (Identification and Referral to Improve Safety)
PCOG received a report that highlighted the breakdown of the number and types of referrals received and the support provided over Quarter 1 2020-2.
Special Allocation Scheme
PCOG requested that the review panel should be reinstated and this is now scheduled to be held on 25 August. There are currently 19 patients in the scheme.
Datix
The group was advised that discussions were on-going between Dudley CCG and Dudley Integrated Health and Care in relation to how incident management systems would be implemented going forward.
3.1.7 ESTATES
The group received an update and was assured about the progess being made regarding on-going projects in Dudley that will be presented to Committee in the estates section of the agenda.
3.1.8 DIGITAL
Dudley IT team has issued 400 laptops and associated VPN accounts to general practice to allow the workforce to work remotely. The team had also supported the Prescription Ordering Direct Team and a number of operatives are now enabled to work remotely.
It was noted that accuRx had been implemented within General Practice to assist with video consultations and that the desktop refresh programme had recommenced and is likely to be concluded by mid-September 2020.
An overview and update was provided in relation to FootFall (Silicon Practice) - an online digital solution for General Practice. FootFall is being rolled out to practices by PCN area with the expectation that Brierley Hill & Amblecote PCN will be live by 12 August 2020. Long term condition forms and templates are under development, practices will use a FootFall website that complies with all of the GMS contractual requirements.

3.2 Sandwell & West Birmingham CCG – PCOG meeting of 5th August 2020
3.2.1 Terms of Reference
The PCOG received the standardised terms of reference (TOR) approved by PCCCic at last month’s meeting. Given that we are still currently one statutory organisation with two places It was agreed with the Sandwell and West Birmingham Managing Directors that we would continue to operate a combined PCOG until it was deemed appropriate to run two separate place based meetings. Additional members in line with the revised TOR were welcomed to the meeting including the LMC GP, NHS England Primary Care Contracting and Training Hub representatives. Moving forward invitations will be extended to include public health colleagues, Health Watch, CQC and Local Pharmaceutical Committee representatives where appropriate together with a Practice Manager representative. It was noted that a process would need to be completed to appoint a Practice Manager representative to sit on the group given we do not currently have anyone acting in the capacity at present. It was queried that in previous PCOG meetings the group held delegated authority from SWB CCG PCCC to commit funding up to the value of £50K which was utilised to expedite decisions and progress work without delay. The group was in agreement to make a recommendation to continue this arrangement under the revised terms of reference.
3.2.2 Risk Register Review Members reviewed the Primary Care Risk Register to agree updates and recommendations. Recommendations were made to close the following risks: PC08_19 - There is a financial risk to the CCG if patients currently registered with one of our member practices choose to register with Babylon GP at Hand as under the current system the funding for these patients would transfer to Hammersmith and Fulham CCG PC11_17a - There is a risk we will not be able to recruit the workforce needed to meet future Primary Care Workforce requirements, missing the NHSE target (additional 129 w.t.e. GPs by 2020) and destabilising our member practices, risking the delivery of services. PC12_18c - If there are no resources identified to deliver the CCG social prescribing programme, then the CCG risks failing to deliver against its MOU as a Black Country Personalised Care Demonstrator site. PC19_11c - If practices don’t make use of complete functionality of the Health App in a timely manner as part of the proof of concept, there is a risk that the evaluation will not be robust and funding will not be utilised.
3.2.3 Finance Update PCOG members received an updated finance report, the detail of which will be covered in the Finance update provided at PCCCiC. Key points noted were as follows: As presented at the June Primary Care Committee in common Sandwell and West Birmingham CCG identified a cost pressure of £1.8m as part of the annual budget setting process.

During the current COVID-19 initial response phase an alternative financial regime is in place which ensures a short-term break-even position across these budgets, but this regime is currently only in place until the end of July. After this point these cost pressures must be addressed. In order to address this a management plan will be developed in conjunction with PCOG members to:
• Review spend in all areas • Review income and future allocations • Adhere to the principle of no new investment • Consider the use of contingency (if required)
3.2.4 Contracting Update Zero Tolerance Contract Extension Modality Enki Medical Centre gave notice to end the contract for the Zero tolerance scheme on 31st March 2020. However, as there was no interest from other practices to provide this service Modality agreed to extended to 30th September 2020. Since this, Modality have agreed to continue the service until 31st March 21 subject to the agreement of some additional costs. The current cost is £90,000 per annum and the new service cost has been agreed at £178, 000per annum. It was confirmed that BSOL CCG were approached and they have agreed to pay a proportion of the costs (£72,600). The cost to SWB CCG will therefore be £105,400, an additional cost of £15,400 above what was previously paid. Additional Roles Reimbursement Scheme An Additional roles reimbursement scheme tracker has been set up by the primary care contracting team to keep information updated for individual PCNs and to enable monitoring of spend against our overall allocation.
3.2.5 Primary Care Commissioning Primary Care Commissioning Framework (PCCF) Following approval at the June Primary Care Commissioning Committee in Common the revised PCCF for 20/21 went live on 1st July 2020. All of the corresponding changes to the searches, prompts and templates are in place and the Primary Care Development Managers have begun a series of virtual PCN support visits. Learning Disability (LD) Health Checks Commissioning responsibility for the LD Health Checks DES has now transferred over from the Senior Commissioning Manager for Learning Disabilities and Autism and will be led by the Head of Primary Care. In 2019/20 SWBCCG achieved 56% against a target of 75% so there is considerable work to be done to mobilise practices to increase the number of completed health checks this year. Work is already underway to map out the administrative process for recording completed health checks, ensuring correct coding is used and the process for uploading onto CQRS is fully understood by all practices. In addition, Dawn Garbett the Health Facilitation Lead - PAMHS (Promoting Access to Mainstream Services) at Black Country Healthcare NHS Foundation Trust is running training every month for both clinical and administrative staff covering the following aspects:
• Learning disability awareness

• Conducting annual health checks • How to deliver health checks the best way for the surgery • Referrals to BCH NHS Trust’s specialist LD team and how BCH NHS Trust can support
practice staff • Making reasonable adjustments • Syndrome specific health issues and tests required • Mental Capacity Act • Role of the PAMHS (Promoting Access to Mainstream Health Services) team
Moving forwards further analysis will be undertaken to look at performance at a PCN level to identify models of best practice and to share learning from those practices who achieve a high uptake of health checks. Flu Programme Discussion was held regarding the National guidance clarifying the expansion of patient cohorts and the national ambitions for the 2020/21 flu programme. In addition to the BCWB Strategic Flu Group a local SWB CCG Flu Leads group has been established with a representative from each PCN, Local Pharmaceutical Committee representatives and CCG officers. Locally, out of our 12 PCNs only 2 are planning on delivering flu vaccinations at a PCN level with the remaining networks planning on an individual practice basis. Given all of the additional complexities around delivering flu vaccinations this year further assurance will be sought from PCN Clinical Directors around contingency plans should a second wave prevent individual practice delivery. Historically, we have always struggled to hit the national targets for flu vaccination uptake across Sandwell and West Birmingham so this year it will be even more important to look at how we can ensure this is prioritised within practices. PCOG were informed that a BCWB dashboard is being compiled to monitor performance throughout the season and that this will be brought to future meetings.
3.2.6 Training Hub PCOG were informed that from April 2020, there has been a combined Training Hub offer across the Black Country and West Birmingham CCGs, covering all 5 places following previous arrangements which were divided between three then later two Training Hubs. The BCWB Training Hub will be transitioning towards a position of maturity by April 2021, delivering more functions currently aligned to universities and Health Education England. There is a full-time project co-ordinator covering both Sandwell and West Birmingham places. This mirrors the support for Wolverhampton and Walsall; however, the training hub is picking up support for Dudley without additional capacity. They will continue support for practices/PCNs and cultivate networks. Updates were also provided around each of the project coordinator led scheme including those available across the BCWB - nursing and clinician education, HCA virtual forums and vaccs and imms 2 day face to face training; and those commissioned specifically at a SWB place level including Active Sign Posting (Care Navigation), Spirometry training, Trainee Nurse Associates and the clinical update events run by Red Whale which are due to take place in the Autumn via virtual means.
3.2.7 Quality Update Primary Care Dashboard and Quality Assurance Tools PCOG members were informed of the work being undertaken across the BCWB to align the Primary Care Dashboards and quality assurance tools.
CQC PCOG was informed that following CQCs temporary suspension of inspections across the UK in March 2020, it is expected inspections would resume in again in September 2020 with a focus initially on practices with an inadequate rating. Further updates were provided around the status of Primary Care Centre West Bromwich, Swanpool, Stone Cross and Clifton Medical Centres. The detail of which can be found in the Quality and Safety Report.
3.2.8 Estates Update The group received an update and was assured about the progress being made regarding on-going projects in Sandwell and West Birmingham that will be presented to Committee in the estates section of the agenda. Great Barr Merger and Premises Relocation to a new build Scott Arms Medical Centre (Dr Jemhal, Sundial Surgery and Park House Surgery) PCOG were informed that requests have been received from two of the practices due to relocate into the Scott Arms Medical Centre for support for costs arising as a result of disposing of their current premises. One request is for support for costs arising from exiting the lease with confirmation given that the premises directions state we can support costs arising from penalties for early termination of a lease. The second request relates to support for a negative equity situation occurring due to a mortgage on the freehold premises. The premises directions state we can support this situation providing it is evidenced that genuine negative equity exists and is not bought about by partners borrowing from the practice. Further information from the practices concerned will be sought before a decision is made around the funding of these requests.
3.2.9 Digital Update Total Triage It was confirmed that the Sandwell and West Birmingham Health App had been successfully rolled out across 67 practices, with Modality practices opting to use e-Consult. As at 31st July only 1,973 patients were registered to use the system and utilisation figures for July showed only 224 completed uses of the interactive symptom checker. Statistics in the report relating to the number of patients receiving an outcome from the automated triage which triggered an urgent response (Urgent 111 or ring GP/Urgent/Immediate 999 or 111 and within 24hrs) totalled around 70% of all of the possible outcomes with only 30% related to self-help or routine GP. It was confirmed further work would be undertaken to look into the outcomes of the automated triage given such a high percentage of urgent outcomes. Technology deployed during covid-19 It was confirmed that during March - June 2020, the CCG had invested significantly in technology to support and enable remote working for general practices, in order to maintain delivery of patient care during the outbreak. This included: • Video technology • Hardware (tablets and laptops) • Applications for collaboration and communication • Patient monitoring tools
In order to capture the impact that these had within primary care, 4 case studies were presented to document the challenges that were being faced and the impact that they made.

3.2.10 Engagement Update It was confirmed that the engagement team has come together across the Black Country and West Birmingham in anticipation of management of change. The focus has been on the patient experience of Covid-19 to inform the restoration and recovery plans. This has been managed through patient experience surveys and also targeted workshops. 4 out of 5 stakeholder meetings have taken place around the merger conversation and they are working towards the member’s engagement with the PCNs.
3.3 Walsall CCG – PCOG meetings of 17 July and 11 August 2020
3.3.1 PCOG Terms of Reference PCOG will adopt the common terms of reference for CCG’s, agreed this is the way forward. Questions over some of the roles. PCOG Chair stated as Head of Primary care: until management of change is complete Dr Teoh will remain as Chair. It was agreed to change the date of PCOG to the second Tuesday in the month with the August meeting taking place on 11th August, and meetings going forward have been amended.
3.3.2 GP practice situation report Primary Care staff sickness/self-isolation continues to be fairly stable with around 37 clinical and non-clinical staff who are self-isolating and unable to work from home. Agreed the Primary Care team are contacting these practices to see if anything can be done to support staff to work from home. Green sites have now reduced from 8 to 3.
3.3.3 Standard Operating Procedure (SOP) for General Practice in Context of Covid-19 Updated SOP of 24 June sent out to general practice via the BCWB primary care bulletin with changes highlighted in yellow
3.3.4 Shielded Patients Following the pausing of shielding from 1 August 2020, clinicians were asked to continue to identify and record people who are extremely vulnerable to coronavirus and the individual made aware of this, so if shielding is reintroduced these people can be quickly identified.
3.3.5 GP Practice Risk Assessments The CCG required to submit practice risk assessment situation report until 31 July 2020. Practices were contacted and 100% achieved.
3.3.6 The NHS England letter of 9 July 2020 Letter discussed; further guidance awaited for some of the proposed revisions, particularly the relaxation of QOF. GP
General practice has been asked to continue with total triage and online consultations as standard unless there is good clinical reason otherwise. All practices must now deliver face to face care where clinically appropriate and ensure that patient know they are open.
3.3.7 AQP and LCS Payment Framework Work is ongoing between the CCG, GPs and LMC to agree a payment framework for AQP and LCSs.
3.3.8 PPE Portal GP practices asked to register with the national portal if not already done so and to start to place PPE orders.
3.3.9 Online Consultation
All 52 GP practices now offering online consultation. Patient utilisation is increasing, significantly higher in some practices than others: agreed to share benchmarked data with GP practices.
3.4 Wolverhampton CCG – PCOG meetings of 5 August 2020 3.4.1 Enhanced Care in Care Homes.
Work continues to take place around the above which is a requirement in the Network DES 2020/2, ready for the implementation October 2020.
3.4.2 Additional roles reimbursement scheme. The additional roles have been identified and it was noted there may be some training issues going forward.
These should be resolved by the training needs analysis workshop via the Training Hub.
3.4.3 Restoration & Recovery
Primary Care is now looking at introducing more services back into GP surgeries, increasing the number of patients seen in surgery and how to do this safely.
A ‘Phase 3 letter was received on Friday last which confirmed the Restoration and Recovery items that General Practices should be focusing on. Predominately each PCN has pulled together their own Restoration and Recovery Plan which will be discussed with Clinical Directors this week and next. These will be crossed referenced to ensure they marry up with the Phase 3 letter. There is a lot of focus on catching up with long term condition management; immunisations must continue with any the back log is to being dealt with. There is a great deal of emphasis on Flu planning season and the delivery of the Flu Planning Program.
Other Key issues are around Urgent Referrals, and referrals into the Acute Trust. A Restoration and Recovery meeting is taking place in Wolverhampton to discuss this further with the Trust. Annual Health Checks are a concern – they are priority to ensure that patients with a Learning Disability in particular are offered a telephone consultation to ensure that they are safe and well. With physical interventions taking place when it is safe to do so. There is a work stream for annual health checks for LD patients with an Action plan in place.
3.4.4 Point of Care Testing
An update was provided regarding the need to focus on a cohort of vulnerable patients and looking at a way to remove barriers around these patients accessing their health checks. Point of Care Testing is a finger prick test where the result is instant with patients will only needing to attend once.
The CCG is proposing buying more monitors for GP practices to support this approach. There is good evidence that this will reduce the DNA rate.
Practices will then be monitored on a monthly basis to review achievement. Feedback will be expected from each PCN regarding the distribution and success of the Project

3.4.5 Social Prescribing
This is currently rated at Amber due to the reduction in the number of referrals received from Primary Care. However this is not a concern as the reduction is in response to the Covid19 situation.
3.4.6 Primary Care Counselling at Amber due to the reduction in the number of referrals. This was expected however as this service is being wound down. This has been compared with the monitoring received from the IAPT service, i.e. ensuring that where one service decreases the other increases
3.4.7 Improving access
Showing at amber - the number was reduced due to Covid19. Close monitoring of Care Navigation is taking place to see how this is impacting, although there is now an increase in both Improving Access and Care Navigation.
3.4.8 Engagement with the public.
Some of the planned engagement work has been delayed: face to face meetings, market stall etc. due to Covid19 and currently these activities will not be possible.
PCNs have been asked to consider alternative plans and will include the review of websites. Other measures include:
• SMS (text) campaign • Letters sent by practices to those shielding • Telephone calls have been made by reception staff to check in on those patients.
It was noted that there are people who do not appear to know about Care Navigation and that further information should be supplied for clarity e.g. posters etc. and the need to be shared in different languages
3.4.9 Primary Care STP
The following was noted
• Still waiting funding confirmation for Primary Care Development – this funding was agreed a few weeks ago. It is likely to be around £1m for our STP area.
• The continued availability of the Dartmouth program was largely supported at the Clinical Director meeting.
• A constant approach to be agreed • Wolverhampton Clinical Director meetings continue to take place but have reduced to once a
fortnight. • Black Country leads still meet twice a week • the availability of new funding has been confirmed - which will be available up to the end of
September 2020. This is to be used for workforce and consumable items, such as items purchased to enable mass vaccination. A consistent approach will be needed across the Black Country – SS has approached Sally Roberts regarding this consistency being applied through the Strategic Blue Planning Group for clarity regarding what the funds can be used for- including notification regarding upper limits.
• PPE provision continues to be very well organized. All practices are being supported to access the National Framework provision; supplies will also continue to be made available through the Black Country PPE distribution centre.
• Restoration and Recovery, - ensuring that PCNs are all planning and have plans in place to demonstrate how they are restoring services – a Sitrep report will need to be developed regarding what services have been switched back on and when.
• The next Primary Care Commissioning Committee in Common is due to take place on 25 August 2020
• The Primary Care Resilience Policy is due to be completed, and ready for consideration, - once the Combined Quality Assurance Reporting is completed / confirmed. .
3.4.11 Resilience Funding
IH medical has shared evidence regarding Patient Satisfaction, Survey, with an increase in satisfaction in all areas and the new practice manager will continue to work at the practice permanently for 3 days per week.
3.4.12 Primary Care Contract Review Program
In the ‘second wave’ of practice visits all practices visited so far are showing improvement i.e. less actions identified
3.4.13 Practice visits
• The first visit taken place since Covid19 was completed virtually via teams with a successful outcome and positive feedback from the practice.
• The 2 next visits are booked in for August 2020.
3.4.14 Black Country Programme
The Black Country CCG’s are looking at unified Contracting Review Program and documentation along with a dashboard to assist in identifying those practices that need to be prioritised in the visiting program.
3.4.15 QOF+
Changes made to the QOF+ specification are:
• Now reduced to a 6 month program – due to the restrictions placed on Primary Care re Covid19 and p not being able to contact patients face to face
• The inclusion of 6 new indicators around Hypertension, End of Life, Carer Support, and Personalisation
• The draft has been adapted regarding Covid19.
It is expected the scheme will be shared with Practices in readiness for implementation from 01 September 2020.
3.4.16 Primary Care Quality Report
Highlights are noted below:
• There were no serious incidents • Quality Matters were quiet in June 2020 but are now (August 2020) increasing – there were 11
with 9 overdue; MB has been in contact with these Practices regarding a resolution/response. • IP audits are ongoing however due to Covid19 no visits took place in June 2020 • No MRSA reported within any practices in Wolverhampton in June 2020 • CAS alerts increased due to Covid19
• Complaints not expecting any further details until August 2020 • Friends and Family – no submissions due to Covid19 • Contacting Visits – from a Quality point of view this worked well especially the virtual aspect • CQC ratings – A practice recently inspected was rated as good.
3.4.17 Primary Care Finance/payments
• 2019/20 QOF+ about to be finalized. Final payout will be £1.83m - under spent by £270k. • Delegated Primary Care budgets - it was planned the budget would be £40.4m for 2020/21 But
due to Covid19 this is around £400k short on budget. Against the budget of £40.4m there is an un-committed balance of £520k mainly due to being unable to launch a full QOF+ scheme due to Covid19.
• Covid19 claims to end of June 2020 - paid £430k to Practices re Covid19 - all funds have been reimbursed by the Department of Health. July 2020 yet to be paid / reimbursed. At the end of June 2020 there were around 30 Practices who had not put in a claim.
• Additional Roles and Responsibilities. ARRs payments to PCNs to end of June 2020 have been reviewed - total £22k - an under-spend of £300k for April, May June 2020.
3.4.18 Premises/Estates
Infection Prevention Update
Audits are suspended due to the Covid19 situation but that these will be reinstated soon through RWT’s restoration and recovery programme.
GP debits/credit from rent payments
Two meetings have taken place with another due next week– There is a plan to forward figures to GPs in August 2020 with a view to meeting GPs in August 2020. A two pronged approach to encourage GPs to sign a Section 52 agreement– which enables CCGs to pay NHS PS direct on behalf of practices. This ten takes the GP debt away. Secondly there would then be an 18 month agreed recovery of GP debt via a Debt Recovery Program
3.4.19 Flu vaccination programme
A Black Country Planning group is in place with numerous meetings taking place over the last 2 months.
A letter was received 04 August 2020 from the Department of Health, with the primary focus for this year should still be on High Risk Patients – to focus on over 65’s. The plan is to:
• Extend to household contacts and those that are currently shielding /Children in year 7. • Greater emphases on Providers to ensure their staff are vaccinated. • Ensuring Commissioned Services are in place ie.GP Practices, Community Pharmacies, Care
Homes etc. • Ambitions for 2020/21 are to attain 75% of every group – this is going to be challenging given
social distancing still in place. • Lots of work is taking place locally in Wolverhampton but also at a Black Country level, -
developing a STP plan - this will be scrutinized by NHSE.
This is a big funding an issue for practices, i.e. if looking to deliver outside of practices. It is not clear how this will work in terms of whether there would be an up-lift on their DES payment or some other payment to compensate for this cost.
It was noted that now there is confirmation that funding is available from the Covid19 fund, a consistent approach will be needed re how to reimburse Practices/PCNs for the work required to enable mass vaccination. It was suggested this be discussed at a Clinical Directors meeting along with a list of suggested approaches for this mass vaccination. Currently it is not noted it is not clear what the Practices plans are as a collective and was suggested that each PCN has a Flu immunization management plan.
3.4.20 Training
Training Hub
A brief update regarding the Training Hub was provided:
• Working closely with the Flu Team to update any staff that needs an introduction to Vaccines – then moving on to the Flu training.
• Virtual Nurse Forums commenced on 07 May 2020 • Healthcare Professional feedback was received – who indicate they are pleased with Virtual
Training as it is now more accessible. They are also requesting further training topics which has been taken on board.
• Nine candidates have been put forward for non-Medical Prescribing for Wolverhampton – Placements will commence in September 2020
• Proposal been agreed for HCA Forums. Nurse Forums will be replicated for HCAs. • Discussion is taking place regarding replicating these Forums for Clinical Pharmacists and
Pharmacy Technicians. • Training for non-clinical staff is available regarding Conflict Management, Effective Calls and
Communications.
TEAM W
The CCG is looking at how September 2020 TEAM W session can be delivered, it should be possible to enable the development of a live Team’s event and individual videos. The CCG has a YouTube channel where it is planned snapshots of Program updates etc. could be viewed.

20-21 Seasonal Flu Programme | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Agenda Item 17.0
2020/21 Seasonal Flu Programme

Table of Contents 1 Introducution ................................................................................. Error! Bookmark not defined. 2 STP Strategic Flu Group………………………………………………………………………………………...3
3 National Flu Immunisation Programme 2020-21……………………………………………………………3
4 Current Position………………………………………………………………………………………………….3
5 Progress Against Plan…………………………………..………………………………………………….…..4
6 Summary…………………………………………………………………………………………………………..5
1. Introduction 1.1 STPs were asked to develop a local flu plan to supplement the NHS England and NHS Improvement
Regional Flu Plan which outlines the scope and ambitions of the National Flu Programme for 2020/21.
1.2 The primary purpose of the STP flu plan is to set out the Healthier Futures Partnership led approach to achieving the National Flu Programme for 2020/21 and the general NHS response to flu outbreaks. In addition, the plan describes the interface between NHSEI direct commissioning functions and local STP/ICS/CCG flu planning, setting out respective responsibilities and accountabilities [Appendix 1].
1.3 NHSEI required STPs to submit their plans by 31 July 2020. An innovation event to share local plans
was held on 11 August 2020: STPs may be required to provide another iteration of their plans following the event and issue of the NHSEI second flu letter on 4 August 2020.
2. STP Strategic Flu Group 2.1 A STP Strategic Flu Group has been set up for the purpose of developing the flu plan and managing the
interface between NHSEI direct commissioning functions and local STP/ICS/CCG flu planning, setting out respective responsibilities and accountabilities as set out in the terms of reference [Appendix 2].
2.2 The Group have met twice to date and will continue meet on a fortnightly basis with appropriate representation on the national and regional flu group. Each CCG flu group will continue to meet at place and be accountable for flu delivery in each area.
3. National Flu Immunisation Programme 2020/21 3.1 The first flu letter was issued on 14 May 2020 which recognised the delivery challenges because of the
impact of COVID-19 and confirmed that further guidance would be issued on how to manage the flu immunisation programme nearer the planned start date of September 2020 [Appendix 3].
3.2 The letter informed which groups were eligible for vaccination. Providers were asked to plan as usual
and urgently review the number of vaccines ordered to meet at least national ambitions and previous uptake rates, whichever was the highest.
3.3 A press statement was released on 24 July 2020 to report expansion of the flu programme to protect
vulnerable people and support the NHS with free vaccinations being made available to: • People aged 50-64 available later in the year • Households of those on shielded patient list eligible for free flu vaccinations • Year 7 – the first year of secondary school
https://www.gov.uk/government/news/most-comprehensive-flu-programme-in-uk-history-will-be-rolled-out-this-winter
3.4 The second flu letter was issued on 4 August 2020 reiterating that providers should focus on achieving
maximum uptake of the flu vaccine in existing eligible groups, as they are most at risk from flu or in the case of children transmission to other members of the community. The letter reaffirmed expansion of the programme as set out in 3.3 above [Appendix 4].
4.0 Current Position 4.1 There remains lack of clarity on funding, drawing down of additional vaccines procured by NHSE and
the use of an inactivated vaccine for BAME children whose parents refuse the normal vaccine due to porcine content.
4.2 The Department has/is:
• consulting on expansion of the workforce able to deliver flu vaccines during the summer; • developing a service specification for all Hospital Trusts to offer vaccinations to pregnant women
attending maternity appointments and to those clinically at risk eligible patients attending in- and out-patient appointments;
• expanded eligible health and social care worker groups to include Personal Assistants, employed through Direct Payment and/or Personal Health Budgets to deliver domiciliary care to patients and service users. This is intended to complement, not replace, any established occupational health schemes that employers have in place to offer flu vaccination to their workforce. Further guidance on how providers can ensure their employees get vaccinated will be published shortly.
• amended the Community Pharmacy Seasonal Influenza Advanced Service Framework to enable community pharmacies to vaccinate both residential care/nursing home residents and staff in the home setting in a single visit. GP practices are also able to vaccinate in residential/care home and residents and staff registered with the practice.
• confirmed MHRA rules on the transfer of flu vaccine between providers has not been relaxed: we are advised discussions are still ongoing.
5.0 Progress against the plan 5.1 CCGs are working with flu providers at place to quantify how many flu vaccines have been ordered to
establish the size of the problem; gaps and opportunities to improve the vaccine uptake by eligible groups.
5.2 Work is underway to develop a dashboard that provides timely data on vaccine uptake at CCG and GP
practice level measured against the number of people eligible, including the 50-64 year group who it is expected will be eligible later in the year if there are sufficient vaccines. NHSEI has not confirmed a provider for delivery to the 50-64 cohort but it may be an extension to the DES, we are still waiting for further information
5.3 CCGs are working with local stakeholders to look at innovative and collaborative delivery models
including mass vaccination. A Local Commissioned Service (LCS) specification is being developed to support the delivery by PCNs/other providers in addition to the national seasonal flu DES and Pharmacy Framework. This will be subject to the ability to obtain a supply of vaccines and/or draw down from the NHSEI procured vaccines to support flu programme expansion. Estates are working to identify suitable locations and the sourcing of equipment is being explored.
5.4 The school service providers have been asked to provide the year 7 vaccines subject to contract
negotiation. 5.5 The additional supply of PPE is being sourced to support delivery of the programme. New infection
control guidance is expected around the changing of gloves after every patient. 5.6 CCG clinical staff have been identified and training organised so they are available to support delivery
of the flu programme. 5.7 At the time of writing this report there is no DES income protection for GP practices although
negotiations are going on behind the scenes. The RCGP has confirmed vaccine administration will take twice as long because of social distancing and infection control prevention and it is unclear whether the relaxation of QOF will free up additional vaccinators at practice level to support delivery.
5.8 All Hospital Trusts will be asked to offer vaccinations to pregnant women attending maternity
appointments and to those clinically at risk eligible patients attending in- and out-patient appointments. National service specifications will be developed to support the standardised commissioning of these services. Locally all heads of midwifery have been asked to look at every opportunity to vaccinate and will be producing plans to support delivery.
5.9 Work is underway to provide vaccinations to care homes and their staff and a plan will be produced to support delivery.
5.10 Communications are working on a winter plan which includes seasonal flu. Providers will be expected
to promote flu vaccination to patients. Public Health are assisting with messaging to school children: the flu fighter campaign will continue and a school toolkit is being produced.
6.0 Summary 6.1 A lot of work is being undertaken to ensure that vulnerable people are protected from the risk of flu this
winter is made more challenging by the circulation of COVID-19 and the additional measures that have to be taken to protect the safety of patients, their families and/or carers and staff delivering the services.
6.2 The lateness or lack of advice from the centre is not helping with the planning process. Notwithstanding
this the system is looking at how they can work together collaboratively to achieve maximum uptake of flu in existing eligible groups, whilst still planning for how to deliver mass vaccinations to the 50-64 year group later in the season.
6.3 It is expected that additional resources will need to be made available to support delivery this year. The
Group will be working with finance and service leads to agree any additional requirements.
APPENDICES
1. STP Flu Plan 2. STP Flu Group Terms of Reference 3. NHSEI Letter of 14 May 2020 4. NHSEI Letter of 8 August 2020
BCWB Seasonal Flu Plan Draft 2020/21 | 0
Appendix 1
Black Country & West Birmingham STP
Seasonal Flu Plan (Draft) 2020/21
7/30/2020

BCWB Seasonal Flu Plan 2020/21 | 1
Contents 1. Introduction ......................................................................................................................... 3
2. Governance and planning arrangements within the Healthier Futures Partnership. 3
3. Assurance processes and findings around: ................................................................... 3
3.1 Sufficient and correct flu vaccines ordered .........................................................................................3
3.2 Clarity on which GP Practices are operating as green/amber/red ..................................................3
3.3 Clarity of PPE requirements and provision .........................................................................................4
3.5 Additional staffing requirements ...........................................................................................................5
3.6 Additional venue requirements .............................................................................................................5
3.7 Domiciliary service for shielded patients .............................................................................................5
3.8 Cold chain storage requirements ..........................................................................................................5
3.9 Enhanced call/recall requirements .....................................................................................................6
4 Practice support .................................................................................................................. 6
4.1 Plan for low performers from last year .................................................................................................6
4.2 Monitoring vaccine orders and transfers .............................................................................................6
4.3 Immunisation training provision and assurance .................................................................................6
4.4 Managing performance through the season .......................................................................................7
4.4.1 Weekly/monthly uptake reports .................................................................................................................... 7
4.4.2 ImmForm submission ..................................................................................................................................... 7
5 Review of local priorities ................................................................................................... 7
5.1 Demographic description and identification of vulnerable groups ....................................................7
5.2 Review of last years’ uptake ............................................................................................................... 10
5.3 Approach to health inequalities .......................................................................................................... 11
6 Local arrangements .......................................................................................................... 12
6.1 Maternity ................................................................................................................................................ 12
6.2 Inpatient/Outpatient ............................................................................................................................. 13
6.3 School Age Immunisation Service (SAIS) ........................................................................................ 13
7 Outbreak management – Linking in with local EPRR arrangements ........................ 14
7.2 Swabbing ............................................................................................................................................... 15
7.3 Treatment – use of antivirals .............................................................................................................. 15
8 Requests to NHSE for local commissioning ................................................................. 15
8.1 Care Home hit squads ......................................................................................................................... 15
8.2 PCN proposals ..................................................................................................................................... 16

BCWB Seasonal Flu Plan 2020/21 | 2
9 Communications and engagement ................................................................................ 16
9.1 Staff communications ......................................................................................................................... 17
10 IT/Digital ............................................................................................................................................... 18
11 Action Plan ........................................................................................................................... 18

BCWB Seasonal Flu Plan 2020/21 | 3
1. Introduction This is the Black Country and West Birmingham Sustainability and Transformation Partnership (Healthier Futures Partnership) Flu Plan. It supplements the NHS England and NHS Improvement Regional Flu Plan which outlines the scope and ambitions of the National Flu Programme for 2020/21. The primary purpose of this plan is to set out the Healthier Futures Partnership led approach to achieving the National Flu Programme for 2020/21 and the general NHS response to flu outbreaks. In addition, this plan will describe the interface between NHSE/I direct commissioning functions and local STP/ICS/CCG flu planning, setting out respective responsibilities and accountabilities. In the Black Country and West Birmingham area there are 279 care homes across the system. 4 CCGs, 210 GP Practices organised within 34 Primary Care Networks (PCNs)
2. Governance and planning arrangements within the Healthier Futures Partnership
The Black Country and West Birmingham system flu plan works across our 5 places; Dudley, Sandwell, Walsall, West Birmingham and Wolverhampton. This plan has been developed through place based teams, culminating into one plan. The flu plan will be overseen at each local place through the health protection forums. In addition the primary care response to flu will be reported through the primary care commissioning committee in common for BC&WB system. As such local governance arrangements are in place and the overall plan has been reported to the Healthier Futures Partnership Board. There is a STP strategic flu planning group set up to pull the 5 place plans together and provide an overall system plan for flu. Progress on delivery is reported to the healthier futures partnership board. A Healthier Futures Partnership representative will attend the NHS England Regional Flu Board. The Healthier Futures Partnership Strategic Planning Group membership and frequency are set out in the terms of reference [Appendix 1].
3. Assurance processes and findings around: 3.1 Sufficient and correct flu vaccines ordered
GP practices have been asked to provide confirmation that sufficient vaccines have been ordered to deliver this year’s flu programme to meet at least previous uptake rates, recognising the additional cohorts from the flu expansion will now require additional vaccines. Each place is establishing the additional vaccines requirements given the recent announcement and is awaiting further guidance on how these will be accessed. With respect to delays and shortages, in previous years, manufacturers and NHSE/DoH have issued information regarding shortages and guidance on using alternatives where available, this has been shortly followed by MHRA issuing guidance on allowing transfer of vaccines between providers. The understanding is this would be replicated this year, should we face shortages again.
3.2 Clarity on which GP Practices are operating as green/amber/red
Primary care is now in phase 2 and working on the restoration of services. Many GP practices continue to see their own patients as amber sites; some are operating as green sites with their patients seen at a neighbouring practice and COVID-19 symptomatic patients are seen at red sites [Appendix 2].

BCWB Seasonal Flu Plan 2020/21 | 4
3.3 Clarity of PPE requirements and provision The Healthier Futures Partnership put in place a central procurement hub to secure and maintain appropriate levels of Personal Protection Equipment (PPE) for all GP practices. A process for collating GP practice requirements was put in place with regular direct delivery of supplies to practices. This approach has ensured sufficient PPE is available to maintain service delivery and will continue to provide resilience through the revised arrangements described below
The West Midlands Local Resilience Forum (WMLRF) has communicated with all Healthier Futures Partnership GP practices detailing the increases in quantities of PPE available through the online PPE Portal. Practices are being encouraged to register and to start using the PPE Portal as soon as possible. There is work in progress on standing down the WMLRF PPE support in the near future and we are actively working towards the full utilisation of the online PPE portal by all GPs in the Black Country and West Birmingham area. This mirrors work underway across the rest of the West Midlands and indeed the country.
The Black Country & West Birmingham PPE Logistics Cell (BCWBPPE) is currently working with Primary Care Teams and the Local Resilience Forum (LRF) to progress GPs across the BC&WB to register and purchase PPE via the online PPE Portal. At present there is a ‘soft’ end date for the end of August to get this completed, however, at this moment in time, there are no plans to stand down the support of PPE from the PPE cell, until such time that all GPs are fully supported by the online PPE portal and there is confidence across the system that no further support from the PPE Cell is required to GPs or any other service. This status will be reviewed regularly by the LRF & CCGs.
The Healthier Futures Partnership recognises the PPE requirement for other providers i.e. community pharmacies, care home providers etc. in supporting the administration of flu vaccinations. Work is underway to establish the demand and contingency has been built into the local PPE distribution arrangements
3.4 Monitoring how long it takes to administer a flu vaccine due to COVID requirements
The Royal College of General Practitioners (RCGP) guidance on delivering mass vaccinations during COVID https://www.rcgp.org.uk/-/media/Files/Policy/A-Z-policy/2020/covid19/RCGP-guidance/RCGP-Mass-Vaccination-at-a-time-of-COVID-V15.ashx?la=en has reported that under normal circumstances, well organised, properly supported flu clinics may be able to vaccinate patients at rates as high as one patient per vaccinator every one to three minutes, as part of a patient journey around 15 minutes in length. In these altered circumstances, it is estimated that the actual vaccination process may take at least four minutes, and potentially five to six minutes depending on the PPE requirements. This is in comparison with a normal GP throughput of between 1-3 minutes per seasonal flu vaccination.
The RCGP say additional time will be needed to allow for staff breaks. Other elements of the process (registration, queuing etc.) will add to the length of the patient journey, but it likely that the vaccination itself will be the limiting factor.
BCWB Seasonal Flu Plan 2020/21 | 5
3.5 Additional staffing requirements Unless the number of vaccinators is also increased, this will have significant implications for the time taken to vaccinate a population (Table 2, page 5 RCGP Guidance).
As vaccinations will take longer this year than in previous years due to social distancing and enhanced standards of infection prevention and control, there will be a requirement for additional staff and services to be made available to support a system wide approach. The Healthier Futures Partnership recognises there may be challenges facing the wider workforce required with regards to indemnity, training and governance. The Healthier Futures Partnership workforce group are currently considering a system approach supporting these arrangements. In addition we await further guidance from NHSEI.
3.6 Additional venue requirements
Existing premises used to deliver flu vaccinations are likely to be impacted by social distancing i.e. GP surgeries, pharmacies, schools. To achieve the high throughput to vaccinate large numbers of patients and to maintain social distancing larger spaces will be required. An options appraisal is underway to determine the requirement for additional venues. This will be carried out in conjunction with Local Authority and Estate Management colleagues at each place. We recognise additional venues beyond GP practices will need to represent local need and demography, specifically with regards hard to reach communities and those areas of highest deprivation.
3.7 Domiciliary service for shielded patients
Recognising the shortfalls in primary care capacity to support those shielding the STP will be working with primary care leads at each place to develop a locally enhanced service. It is envisaged this service will be multidisciplinary and will include delivery via community services, Public health services, community pharmacies as well as primary care. This service will complement the enhanced community services already in place. Recognising the vulnerability of this cohort of patients, families and carers will also be included and patients will be stratified to ensure all shielded patients are prioritised.
3.8 Cold chain storage requirements
All options considered will be cognisant of Cold chain storage requirements as noted in the Green Book https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/223753/Green_Book_Chapter_3_v3_0W.pdf We recognise the requirement for additional refrigeration to be made available for off-site administration as well as validated cooler boxes. Access to electricity, running water, waste disposal and secure refrigeration is required. Arrangements for sourcing these are underway.
BCWB Seasonal Flu Plan 2020/21 | 6
3.9 Enhanced call/recall requirements In line with the DES requirements practices will ensure a proactive call and recall basis, if considered at-risk and a proactive call basis, if not considered at-risk with the aim of maximising uptake in at-risk patients. Methods for call and recall will include letters, text messages and phone calls.
4 Practice support 4.1 Plan for low performers from last year
The Regional Immunisation Team directly emails GP practices with uptake rates. CCG Primary Care Operational Groups regularly review local GP practice immunisation achievement and agree targeted action where there are areas of concern. The approach is supportive, seeking assurance that plans are in place to improve uptake. Performance will be monitored on a very regular basis to ensure appropriate uptake. Where there are issues relating to performance these will be escalated rapidly through existing governance channels. Practices have been sent top tips on improving uptake from intelligence gathered from our practices with the highest uptake in previous years.
We are currently reviewing all of previous data and will be targeting specifically those areas where performance was challenged to support rectification plans for improvement this year. The Healthier Futures Partnership will also be supporting the development of a local performance dashboard that can be monitored regularly and remedial actions out in place if required. CCGs will be requesting direct access to IMFORM to ensure latest performance data is available and tracked. We await the decision from NHSE/I as to the availability of a local dashboard too.
4.2 Monitoring vaccine orders and transfers GP practices received the NHS England letter of 19 December 2019 regarding flu vaccine ordering.
GP practices received the NHS England letter of 14 May asking them to continue to plan for the flu programme as usual and to ensure sufficient stocks of adult flu vaccines have been ordered for eligible patients. NHS Trusts and ICPs were also asked to review vaccine orders to ensure the number of vaccines ordered meets the requirement for the vaccination programme to cover all front line healthcare workers.
CCGs were required to submit a report by 22 May 2020 to ensure the number of vaccines ordered met at least national ambitions or previous uptake rates, whichever is the highest.
We know that in previous years most practices end up disposing unused vaccines. If the rules allow, we will consider how PCNs could transfer vaccines between practices to ensure all ordered vaccines are administered and there is no waste. Local protocols will support this arrangement and will also include the process for ordering of additional vaccines if the programme is expanded as expected.
4.3 Immunisation training provision and assurance
The Healthier Futures Partnership has commissioned the Training Hub to provide the following immunisation training:

BCWB Seasonal Flu Plan 2020/21 | 7
• Flu updates for the flu vaccination programme 20/21 including any changes to adult pneumococcal and shingles programmes. Virtual and face to face training sessions will run during August and September.
• Immunisation training for HCA who are new to vaccinations, adhering to the national minimum standards for immunisations including flu, pneumococcal and shingles during August.
• A free flu e-learning package is also available from e-Learning for Healthcare.
The STP workforce group are currently considering a system approach supporting these training arrangements. In addition we await further guidance from NHSEI.
4.4 Managing performance through the season
4.4.1 Weekly/monthly uptake reports The Regional Immunisations Team provide GP vaccination reports that can be used by CCGs to monitor vaccination uptake and look at unwarranted variation for targeted action as appropriate. The Healthier Futures Partnership flu group will receive performance monitoring reports on a weekly basis, which will represent flu vaccination across the region. Where there are issues regarding performances these will be addressed through local governance arrangements.
4.4.2 ImmForm submission GP practices are expected to deliver the arrangements set out in the DES which includes monitoring and reporting all activity information via ImmForm on a monthly basis as per the national uptake surveys for influenza and PPV uptake. This information will be reported in the Regional flu vaccination reports made available to CCGs for monitoring as detailed in 4.4.1 above.
4.4.3 PharmOutcomes Local IM&T teams are ensuring the correct emails are in place to enable more efficient transfer of information regarding flu vaccinations administered in community pharmacies. This will enable community pharmacy to report flu vaccinations in a timely fashion.
5 Review of local priorities
5.1 Demographic description and identification of vulnerable groups The Healthier Futures Partnership footprint has a diverse population with varied and
significant health care needs. Wider determinants of health such as poor education, housing, work and unemployment, all affect our resident’s experience of wellbeing and health. Differences in lifestyles, such as smoking, binge drinking, insufficient exercise and lack of five-a-day fruit and vegetable consumption lead to much poorer health experiences for those living in some areas of our partnership. This translates into real differences in health outcomes for the people living in these areas, including higher morbidity from coronary heart disease and diabetes.

BCWB Seasonal Flu Plan 2020/21 | 8
It is predicted that the population age structure will change shape as the population ages. This suggests that the care needs of the frail elderly will increase in the future and with this the development of associated long term Conditions. The areas have become increasingly diverse since 2001, for example in Wolverhampton 16.4% of the population in 2011 born outside of the UK. Whilst 10% of the population at 2011 spoke a non-English 1st language, local interpreting data highlights an increased demand for interpreting in Kurdish and central and eastern European languages. 2014 saw a significant arrival of Romanian nationals, noticeable in school admission and National Insurance Number data. This group includes a high proportion of the Czech and Slovak Roma community. In terms of ethnic groups these include: Indian, Black African, White other, Asian and Chinese. In Sandwell and West Birmingham (SWB) the total registered GP population is 578,140 (January 2020). The population is younger than most areas of England, particularly West Birmingham where 64.8% of the population is under 45 years of age. The proportion of older people (aged 65 years and over) in the CCG is lower than England average. The majority of the SWB population live in areas deemed to be amongst the most disadvantaged in England with the population representing of the most diverse multi-racial, ethnic and cultural populations in England. 50% of our population are British White compared to 86% for West Midlands and 87% for England. The main Black and Minority Ethnic (BME) groups are: 12% Asian Indian, 8% Asian Pakistani and 6% Black British / Caribbean. BME classification alone does not highlight the true diversity of the population. Analysis of interpretation requests in primary care shows a total of 46 languages and dialects were utilised originating from many parts of the world including Asia, Africa and Europe. The birth rate for live births is higher in the SWB population than England. The proportion of women who are of child-bearing age is higher than in other populations, however this does not explain the higher birth rate. In 2014 over 60% of live births in West Birmingham were to first generation migrant mothers. Dudley’s population is, on average, older than that for England, with a higher proportion of the population aged over 45. The five townships all have a variety of age profiles: • Dudley Central has a younger population than the Borough average with a greater proportion of the population in the age groups under 35; • Dudley North, Brierley Hill and Stourbridge all have resident populations with older age profiles than the Borough. • Halesowen’s population has an age profile very similar to that for the Borough as a whole. The proportion of the Dudley population represented by the 0-19 age group has been broadly stable, with some marginal changes at the township level. Dudley Central township has the largest population aged under 20, both in total numbers (more than 20,000) and as a proportion of the total (27.3%). Dudley North and Stourbridge townships both have a relatively small proportion of their populations in the 0-19 age group (22.3% in each case).

BCWB Seasonal Flu Plan 2020/21 | 9
The working age group (16-64) is falling as a proportion of the total population at a Borough-wide level as well as in all five townships. It also represents a smaller part of the population in Dudley than for England as a whole. Dudley Central township has the largest population aged 16-64, both in total numbers (more than 45,500) and as a proportion of the total (62.2%). At fewer than 31,000 and less than 60% of the total population, Dudley North has the smallest working age population of any of the five townships. The population of the Borough aged 65 and over is increasing as a proportion of the total, and this is true for all but one of the five townships. The proportion over 65 is also higher in Dudley than it is in England as a whole. In proportion to its population, the Dudley North township has the largest proportion of retirement age, and in some parts of Gornal and Sedgley more than a third of the population is 65 or older. Dudley Central township has a much smaller proportion of its population in this older age group (15.4%) than any of the other townships. By 2031 the Dudley population is expected to increase by 13,990 (4.4%). Most of this increase is accounted for by the rise in the 65 and over age group, with the 85+ ages increasing by nearly 70%.The only age group projected to decline is that between the ages of 45 and 64. This group could see more than a 5% reduction in size by 2031. The population of England is expected to grow 10.2%, a faster growth than Dudley. In England, BME residents represented 20.9%, nearly double the Dudley rate. Compared to Dudley, England had a higher rate of all Broad BME groups. Ethnic diversity varies across the Borough, with Dudley Central township having the largest rate of BME of 20.2%, with the Pakistani, Indian, Black Caribbean groups being prominent. At 5.5%, Dudley North township had the lowest proportion of BME residents in this age group. Walsall has an estimated population of 285,500 (ONS 2019 Mid-Year Estimates), comprised of approximately 21.7% children 0-15 (62,100), 60.7% working-aged 16-64 (173,300), and 17.6% 65 years & over (50,100), giving a dependency ratio of 0.65 dependents to every 1 working age adult. In terms of density, this equates to around 2,745 people per square kilometre. The population has seen a 7.8% increase over the past decade, from 264,800 in 2009: most of this increase has been under 16s & over 65s, both groups seeing approximately 12% increases, contrasted to a working age (16-64 years) increase of around 5% (2019 & 2009 ONS Mid-Year Estimates).
Walsall is expected to see continued & consistent population growth, projected to increase by 7% to an estimated 304,400 by 2030 & further by 13% to an estimated 320,400 by 2040 (2020 ONS, 2018-based projections). The largest increases are expected within older age groups; the population over 65 years of age will increase their share of the population from approximately 18% to 20% by 2040 (around a 1% decline in population share for both children & working-age adults). There has already been an 8.8% increase in births in Walsall between 2004 and 2014, and the number of Walsall of reception pupils in Walsall schools has increased 11.34% between 2012 and 2017.

BCWB Seasonal Flu Plan 2020/21 | 10
Therefore, planning to meet the needs of a growing number of a younger population as well as a growing number of older people is incorporated within our key strategic priorities, while recognizing that the proportion of residents likely to be economically active is projected to fall.
5.2 Review of last years’ uptake
Please see below the Final Seasonal Influenza Vaccination Summary Uptake Tables:
The practice level uptake has been shared GP Practices, the email send in attached in Appendix 3
School Age
GP Practice Flu Immunisation uptake up to the end of February 2020
65 and overUnder 65 (at-
risk only)All Pregnant
WomenAll Aged 2 All Aged 3
ENGLAND 72.4% 44.9% 43.7% 43.4% 44.2%Q77 West Midlands DCO 71.1% 45.0% 41.9% 39.8% 41.8%05C NHS Dudley CCG 71.7% 48.5% 48.0% 45.7% 49.4%05L NHS Sandwell and West Birmingham CCG 63.3% 38.6% 34.8% 33.1% 33.6%05Y NHS Walsall CCG 71.0% 47.6% 41.8% 36.9% 38.8%06A NHS Wolverhampton CCG 67.9% 42.4% 40.5% 37.1% 42.7%
CCG Code Org NameSummary of Flu Vaccine Uptake %
GP Practice Flu Immunisation uptake up to the end of February 2019
65 and overUnder 65
(at-risk only)All Pregnant
WomenAll Aged 2 All Aged 3
ENGLAND 72.0% 48.0% 45.2% 43.8% 45.9%Q77 West Midlands DCO 70.8% 47.9% 43.2% 41.9% 44.7%05C NHS Dudley CCG 71.0% 50.4% 47.8% 49.5% 50.5%05L NHS Sandwell and West Birmingham CCG 64.5% 43.1% 38.4% 36.0% 36.4%05Y NHS Walsall CCG 69.9% 47.7% 44.6% 35.2% 40.3%06A NHS Wolverhampton CCG 67.8% 46.6% 43.9% 40.9% 44.7%
CCG Code Org NameSummary of Flu Vaccine Uptake %
Percentage Change in uptake for February 2020 compared to February 2019
65 and overUnder 65 (at-
risk only)All Pregnant
WomenAll Aged 2 All Aged 3
ENGLAND 0.4% -3.1% -1.5% -0.4% -1.7%Q77 West Midlands DCO 0.3% -2.9% -1.3% -2.1% -2.9%05C NHS Dudley CCG 0.7% -1.9% 0.2% -3.8% -1.1%05L NHS Sandwell and West Birmingham CCG -1.2% -4.5% -3.6% -2.9% -2.8%05Y NHS Walsall CCG 1.1% -0.1% -2.8% 1.7% -1.5%06A NHS Wolverhampton CCG 0.1% -4.2% -3.4% -3.8% -2.0%
CCG Code Org NameSummary of Flu Vaccine Uptake %
GP Practice Flu Immunisation uptake up to the end of January 2020
ReceptionSchool Year
OneSchool Year
TwoSchool Year
ThreeSchool Year
FourSchool Year
FiveSchool Year
SixENGLAND 64.2% 63.5% 62.6% 60.6% 59.6% 57.2% 55.1%
48.4% 46.7% 46.9% 45.7% 45.3% 41.4% 40.3%72.4% 69.6% 69.3% 69.0% 67.0% 62.4% 60.9%59.7% 55.7% 60.6% 58.1% 57.8% 58.2% 52.8%59.7% 57.0% 56.9% 53.8% 55.3% 50.4% 50.7%72.7% 68.7% 66.3% 65.8% 66.4% 65.0% 62.1%
Org NameCCG Code
Wolverhampton Local AuthorityWalsall Local AuthoritySandwell Local AuthorityDudley Local Authority
Summary of Flu Vaccine Uptake %
Birmingham Local Authority

BCWB Seasonal Flu Plan 2020/21 | 11
Overall flu vaccination uptake has increased across school-age children in all areas when comparing January 2020 and January 2019 uptake data by Black Country local authorities (Birmingham LA is included as there is currently no split for West Birmingham). However, there are areas that require a more targeted approach especially around school year one uptake across most areas.
Trust Staff Flu Vaccine Uptake
5.3 Approach to health inequalities
There is a strong correlation between the uptake of flu vaccination (65+ and at risk individuals) and deprivation (IMD 2019). Deprivation is measured using Index of Multiple Deprivation – this is a composite measure and is informed by or correlated with other factors that lead to health inequalities (socio-economic factors, geography – urban/ rural, protected characteristics including ethnicity and socially excluded groups). Therefore in the first instance we will focus on deprivation in our approach to health inequalities with an additional focus on ethnicity.
The Healthier Futures Partnership is one of the most deprived STPs in England (second only to BSOL STP). There is variation in levels of deprivation between PCNs and places in the Healthier Futures Partnership.
GP Practice Flu Immunisation uptake up to the end of January 2019
ReceptionSchool Year
OneSchool Year
TwoSchool Year
ThreeSchool Year
FourSchool Year
FiveSchool Year
Six
ENGLAND 63.9% 63.4% 61.4% 60.2% 58.0% 56.2%Q77 West Midlands DCO 62.0% 61.7% 60.2% 59.5% 57.4% 55.1%
48.4% 48.1% 47.0% 45.9% 43.3% 40.4%67.9% 65.0% 64.9% 62.4% 58.8% 57.7%59.2% 60.9% 59.2% 58.7% 58.0% 54.2%54.8% 64.2% 51.4% 51.5% 49.7% 48.9%73.3% 73.8% 72.7% 70.5% 69.8% 68.9%
CCG Code Org Name
Walsall Local Authority
Summary of Flu Vaccine Uptake %
Sandwell Local AuthorityDudley Local AuthorityBirmingham Local Authority
Wolverhampton Local Authority
Percentage Change in uptake for January 2020 compared to January 2019
ReceptionSchool Year
OneSchool Year
TwoSchool Year
ThreeSchool Year
FourSchool Year
FiveSchool Year
Six
ENGLAND 0.3% 0.1% 1.2% 0.4% 1.6% 1.0%0.0% -1.4% -0.1% -0.2% 2.0% 1.0%4.5% 4.6% 4.4% 6.6% 8.2% 4.7%0.5% -5.2% 1.4% -0.6% -0.2% 4.0%4.9% -7.2% 5.5% 2.3% 5.6% 1.5%-0.6% -5.1% -6.4% -4.7% -3.4% -3.9%Wolverhampton Local Authority
Walsall Local AuthoritySandwell Local AuthorityDudley Local Authority
Summary of Flu Vaccine Uptake %
Birmingham Local Authority
CCG Code Org Name
Number of HCWs
involved with direct patient
care
Seasonal Flu doses given
since 1 September
2019
Vaccine uptake (%)
CQUIN payment indicators
Number of HCWs involved with
direct patient care
Seasonal Flu doses given
since 1 September
2018
Vaccine uptake (%)
RYK DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST 879 729 82.9 100 856 656 76.6
RXK SANDWELL AND WEST BIRMINGHAM HOSPITALS NHS TRUST 5,357 4,454 83.1 100 4,512 3,687 81.7
RNA THE DUDLEY GROUP NHS FOUNDATION TRUST 4,877 3,959 81.2 100 4,525 3,477 76.8
RL4 THE ROYAL WOLVERHAMPTON NHS TRUST 6,810 4,366 64.1 20.6 6,789 4,283 63.1
RBK WALSALL HEALTHCARE NHS TRUST 2,785 2,511 90.2 100 3,157 2,552 80.8
Org Code Trust Name (2019/20)
2019/20 2018/19
Seasonal Flu Vaccine Uptake (Frontline Healthcare Workers - all NHS England Trusts, Local Teams and old Area Teams) 2019/20February 2020 (Cumulative data from 1 Sep 2019 to 29 Feb 2020)
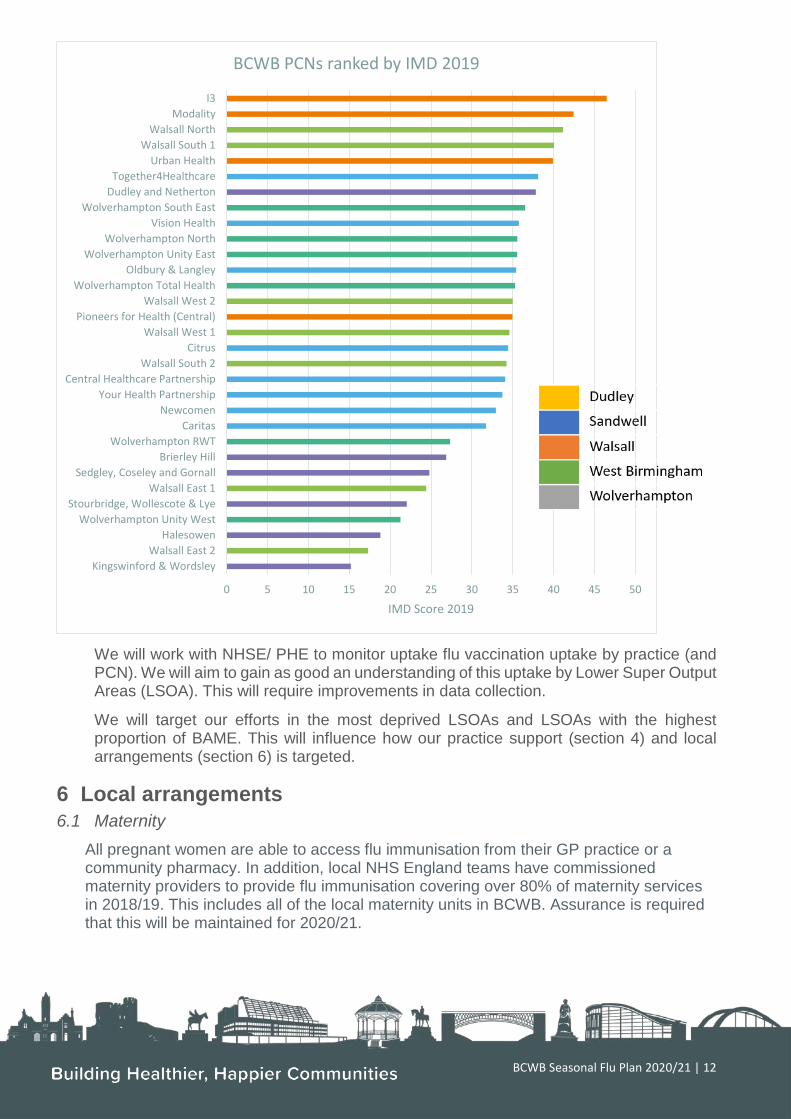
BCWB Seasonal Flu Plan 2020/21 | 12
We will work with NHSE/ PHE to monitor uptake flu vaccination uptake by practice (and PCN). We will aim to gain as good an understanding of this uptake by Lower Super Output Areas (LSOA). This will require improvements in data collection.
We will target our efforts in the most deprived LSOAs and LSOAs with the highest proportion of BAME. This will influence how our practice support (section 4) and local arrangements (section 6) is targeted.
6 Local arrangements 6.1 Maternity
All pregnant women are able to access flu immunisation from their GP practice or a community pharmacy. In addition, local NHS England teams have commissioned maternity providers to provide flu immunisation covering over 80% of maternity services in 2018/19. This includes all of the local maternity units in BCWB. Assurance is required that this will be maintained for 2020/21.
0 5 10 15 20 25 30 35 40 45 50
Kingswinford & WordsleyWalsall East 2
HalesowenWolverhampton Unity West
Stourbridge, Wollescote & LyeWalsall East 1
Sedgley, Coseley and GornallBrierley Hill
Wolverhampton RWTCaritas
NewcomenYour Health Partnership
Central Healthcare PartnershipWalsall South 2
CitrusWalsall West 1
Pioneers for Health (Central)Walsall West 2
Wolverhampton Total HealthOldbury & Langley
Wolverhampton Unity EastWolverhampton North
Vision HealthWolverhampton South East
Dudley and NethertonTogether4Healthcare
Urban HealthWalsall South 1
Walsall NorthModality
I3
IMD Score 2019
BCWB PCNs ranked by IMD 2019

BCWB Seasonal Flu Plan 2020/21 | 13
Midwives are able to explain the benefits of flu vaccination to pregnant women and offer them the vaccine, or signpost women back to their GP or community pharmacy if they are unable to offer the vaccine.
The BCWB LMNS is supporting local maternity units to administer flu vaccinations in a consistent and accessible way. Working with MVPs in each local system to raise the profile for flu vaccination will be a supported principle of the local LMNS and resource to further enhance this performance will be supported through the LMNS.
Where maternity providers provide the flu vaccine, they are required to inform the patient’s GP practice within 48 hours so their records can be updated accordingly, and included in vaccine uptake data collections. Maternity providers are required to inform GPs when a woman is pregnant or no longer pregnant.
The pharmacy contractor will ensure that a notification of the vaccination is sent to the patient’s GP practice on the same day the vaccine is administered or on the following working day. This can be undertaken via post, hand delivery, secure email or secure electronic data interchange. If an electronic method to transfer data to the relevant GP is used and a problem occurs with this notification platform, the pharmacy contractor should ensure a copy of the paperwork is sent or emailed to the GP practice. Where the notification to the GP practice is undertaken via hardcopy, the national GP Practice Notification Form should be used.
6.2 Inpatient/Outpatient
Within Black Country Healthcare NHS Foundation Trust, guidance will be provided to inpatient services to support offering flu vaccinations to eligible in patients who fall into risk categories for flu. Checks will be made on admission to establish if patients have already been vaccinated through other routes. Patients will be provided with written and verbal information so that they can make an informed decision wherever possible. The vaccines will be prescribed by the clinical team, supplied through pharmacy dispensary and administered through clinical staff trained as vaccinators. Information will then be shared with the patients GP. Admission will be used as an opportunity to remind patients of the importance of vaccination and other healthy life style options and services available to them within primary care. Vaccinations are not provided to patients who are outpatients. They are required to access these through their GP or Community Pharmacists. Opportunities to encourage patients to have their flu vaccine will be taken within health promotion work through physical health clinics.
6.3 School Age Immunisation Service (SAIS)
VUK are commissioned to deliver the flu programme in all schools in Dudley, Walsall and Wolverhampton area and from September 2020 also in Sandwell. Children from Reception to Year 6 are currently eligible for this vaccination. However, in the 2020 programme eligibility will be extended to include year 7 pupils. In addition, we will be delivering the programme to students in special schools. The vaccine offered is Fluenz Nasal spray to pupils below the age of 18 and those with no contraindications. The

BCWB Seasonal Flu Plan 2020/21 | 14
majority of vaccination activity will take place in schools but we will supplement these sessions with community clinics to ensure several opportunities to access our service. The programme will begin at the start of October with Special Schools being prioritised. All schools will receive first visits from our team by the 12th December with catch up sessions being run throughout January in order to maximise uptake and meet national targets. BCHC are delivering services via schools where accessible from September, and currently delivering immunisations through additional local clinic provision developed across the city for CYP / Families throughout the summer break. We are also in the process of developing a mobile option to support access where schools are struggling with on-site space to support vaccination delivery from September. We are currently working through the backlog of vaccinations (due to COVID 19) plus preparing for mobilisation of new Birmingham and Solihull service model to commence September onwards. Over the next 12 months (academic year) we will be delivering the core programmes including additional flu delivery in year 7 and on-going mop up of backlog of vaccinations (as per PHSE and NHSE commissioner guidance).
6.4 Community Pharmacy
Community Pharmacists contribute significantly to the overall number of flu vaccinations and provide a welcome alternative for many patients.
This year, as never before, vaccines are in everyone's mind and it is likely public demand will be at an all-time high for both flu and COVID vaccination should it become available. The Pharmoutcomes IT platform should facilitate easier data transfer to the patients' GP this year.
Vaccination in Community Pharmacy is well established and can help to support a coordinated approach to cover as many people as possible across the geography, especially the vulnerable and higher-risk groups. To ensure community pharmacy uptake is maximised a collaborative partnership between practices and pharmacies will be required. Community pharmacy PCN leads and PCN Clinical Directors need to have regular communication so collaboration between the professions delivers significantly higher uptake in all target flu categories.
7 Outbreak management – Linking in with local EPRR arrangements
7.1 CCGs commission outbreak management services from local providers
In February 2020 BC&WB CCGs enacted their EPRR processes and established a Healthier Futures Partnership wide Incident Coordination Centre (ICC) which continues to operate and co-ordinate the response to COVID-19 under its agreed governance arrangements. The ICC operates 8am to 5pm Monday to Friday and 8am to 4pm Saturday and Sunday, as directed by NHS England. The ICC team continue to directly support the coordination of the STP’s Pillar 1 COVID-19 staff testing; this has reduced in service offer as the national programme had become established. The CCG also
BCWB Seasonal Flu Plan 2020/21 | 15
continue to support swabbing for in care homes, staff testing facilitated through the ICC team and Mobile Testing Unit programme coordinated by the West Midlands IU&EC Team. The Primary Care Testing Cell has been decommissioned as demand from the GP staff switched to the government online offering. All of the above measures can be flexed / stood-up to support outbreaks as and when required.
In the event of a local or regional outbreak the EPRR have representation from each Local Authority, normally Emergency Planners, who have regular and direct links with the Local DPHs. Through this a local response can be instigated and co-ordinated. Routinely EPRR representatives attend local Health Protection Forums where local and regional Health Protection related issues, such as flu, are discussed, planned and assurances obtained.
7.2 Swabbing
Each local authority place has an outbreak management plan in place that is managed and overseen through the health protection forum at each place. Swabbing activity will be supported through the operationalisation of any outbreak plan when needed. Arrangements are in place for the provision of community swabbing teams through local health provision.
7.3 Treatment – use of antivirals
The Department of Health & Social Care will inform prescribers when they can prescribe antivirals. These are provided by a patient’s GP ‘in season’ and a local provider ‘out of season’.
8 Requests to NHSE for local commissioning
8.1 Care Home hit squads
The optimal position will be for vaccinations to be administered to both residents and staff members by the registered GP practice in line with the DES. However, it is recognised that due to inevitable complexities that arise from registrations with multiple practices, timely attendance by staff at practices, availability of night staff to name but a few, this may not always be feasible. This does create issues with funding streams and how these may be addressed. To this extent, we will take a blended approach to reach maximum contacts including;
• District nurse cover for those patients registered on the DN caseload on a cross border basis, but registered with a GP practice
• Pop up clinics within care homes where the number of vaccinations to be administered is greater than 10 (for both residents and staff)
• Care home nurses trained with the governance infrastructure to carry out vaccinations of residents that includes the use of PSD and ensures the correct and appropriate storage of the vaccines in the home

BCWB Seasonal Flu Plan 2020/21 | 16
The Healthier Futures Partnership would also like to request of NHSE/I to commission either community pharmacy or the Primary Care Network and/or practice aligned to a care home to carry out vaccinations for care home staff (including agency), although funding streams in order to meet this pathway would need to be addressed with the provision of a LIS.
It is noted that there could be risk in the availability of sufficient vaccines for care home staff, as such the Healthier Futures Partnership will need to be assured of the sourcing of additional vaccines for this group, as practices have already placed their orders and would not have included care home staff within these numbers. Care home staff who move between different homes should also be included.
Significant investment is also required in obtaining resident consent prior to the launch of any flu vaccination programme, including, but not restricted to those without capacity to consent. NHSE/I and each respective CCG will need to be supporting practices aligned to care homes to encourage commencement of this process now so that when the vaccines are delivered, delivery of vaccinations can commence with immediate effect in a single visit.
We will work with Local authority commissioning and public health colleagues to promote vaccination in care home staff and target those care homes where uptake is poor
Finally, given the immense success of the drive-thru swabbing service in Wolverhampton, provision of (a) replica version(s) for flu vaccinations may be deliberated as a failsafe contingency position. However, additional funding for operationalisation of such a service will be required.
8.2 PCN proposals Care Homes in each place have been geographically aligned to PCNs who are already working as part of an MDT to deliver the COVID Care Home service until 30 September 2020 and the PCN Enhanced Healthcare in Care Homes service operational from 1 October. PCNs are well placed to be incentivised to deliver mass flu vaccinations if the regulations allow this level of flexibility. Flu delivery would be dependent upon an appropriate supply of vaccines and funding for additional vaccinators. PCNs have made progress with the sharing of patient records which would support timely recording of vaccine uptake.
9 Communications and engagement An integrated national communications strategy will be introduced for the national flu immunisation programme in 2020/21. The strategy will be led by PHE and will provide communications colleagues in other organisations with information and resources to assist the delivery of the programme. In the Black Country and West Birmingham, we will use national content, but will localise it with Black Country and West Birmingham activity and information. As in previous years, a Healthier Futures Partnership Winter Communications Plan will be produced for 2020/21 and will incorporate flu activity as a key component. The communications lead for this activity will be Sophie Powers. Insight to inform this
BCWB Seasonal Flu Plan 2020/21 | 17
communications plan will be gathered at a communications planning meeting on 24 August 2020, with attendees to include communications leads from STP organisations.
Coronavirus means we have to deliver things differently this year and therefore there is an important role for communications and engagement to play. Flu immunisation has never been more important. We must:
• Encourage all those in at risk groups to have the vaccination
• Support vulnerable and shielding patients – making it easier for them to receive the vaccination in an environment that is as safe as possible for them
• Encourage vaccination to be equitable – those who identify as BAME, those from areas of deprivation, homeless people…
• Encourage our workforce to set an example by having the vaccine
• Find more creative and innovative ways of giving the vaccine to increase uptake and to meet safety requirements.
There are additional considerations that will need to be factored into the communications plan in light of the Covid-19 pandemic. With the expansion to the routine flu vaccination programme, communications activity to promote uptake of the flu will need to adapt to target new groups. Additionally, the national team is looking at how Covid-19 vaccination messaging could run alongside flu messaging should a vaccine be ready for delivery this winter period. Should this be the case, we will respond to this requirement on a local basis.
The flu activity this year will also link into our restoration and recovery communications activity, which aims to ensure that people feel safe in using NHS services, as patients will need to be reassured that accessing the flu vaccination is safe.
One example of communications activity that will be run locally is the ‘Flu Fighters’ campaign developed by the City of Wolverhampton Council’s Communications and Public Health teams and the communications teams at Wolverhampton Clinical Commissioning Group and the Royal Wolverhampton NHS Trust. The campaign – which centres on a free children’s storybook distributed to primary aged pupils – was successfully run in Wolverhampton in 2019 and will be extended across all of the Healthier Futures Partnership local authority areas this year to encourage uptake amongst children.
9.1 Staff communications
Staff-facing collateral for the flu is expected to become available in August. The Healthier Futures Partnership organisations will have access to this collateral and campaign materials for their internal, staff communications. Individual organisations will be responsible for planning and delivering their own internal communications plans around flu. However, the Healthier Futures Partnership communications group will use its regular meetings to review and share staff communications activity. These regular meetings will allow for the identification of issues and the sharing of best practice across organisations so that organisations with low uptake are identified and communications activity can be adapted.

BCWB Seasonal Flu Plan 2020/21 | 18
Staff communications will consider hard-to-reach staff, including staff outside the NHS family, to ensure that messages reach the right stakeholders and that all staff are able to and encouraged to access the flu vaccination.
We will encourage our workforce to set an example by having the vaccine and we organisations will be encouraged to use their leadership to highlight the importance of staff uptake of the vaccine.
9.2 At risk groups
With the expansion to the routine flu vaccination programme, communications activity to promote uptake of the flu will need to adapt to target new groups. In addition to targeting these new groups, we will focus our activity on key cohorts where uptake is lower including: people with long-term conditions, pregnant women, parents of 0-3s and carers.
It will be important to make every contact count. Staff, including GPs, will be encouraged to think about the flu vaccine even with patients not ‘at risk’. Flu vaccination should become routine vocabulary at every opportunity to encourage uptake.
The Healthier Futures Partnership communications group will use its regular meetings to review communications activity and identify issues and areas of lower uptake. In these instances, we will flex our plans to amend our communications activity to improve uptake. This may include the production of new localised materials or the use of different channels.
10 IT/Digital 10.1 Clinical IT
Consideration needs to be made regarding the recording of accurate, timely information into appropriate clinical systems. The default IT system for recording influenza vaccinations is the GP Practice clinical system. This is not a new requirement and so the local systems are not a problem to be solved however, with remote clinics or open access clinics problems are posed with regard to data capture. There is a dependency upon agreeing the model of delivery which will then identify the issues to be resolved and so the CCG digital team have mobilised to work with commissioners and GPs to create robust solutions: • Planning in progress to support multiple practice clinics • Clinical system specialists are reviewing plans with PCNs • Barcoded Flu Clinics are being considered as a good practice example • Consideration is being made around the recording of patient immunisations
administered in other settings such as pharmacy – how these are recorded in GP clinical systems
11 Action Plan A system flu group has now commenced and now developing the action plan
Appendix 2
STP BCWB Strategic Flu Plan Terms of Reference | 1
Terms of Reference PURPOSE
The primary purpose of the Healthier Futures Partnership strategic Flu Planning Group is to develop a flu plan that sets out the Healthier Futures Partnership led approach to achieving the National Flu Programme for 2020/21 and the general NHS response to flu outbreaks. The plan will describe the interface between NHSE/I direct commissioning functions and local STP/ICS/CCG flu planning, setting out respective responsibilities and accountabilities.
MEMBERSHIP STP Lead – Chair: Sally Roberts, BCWB Healthier Futures Partnership CCG Flu Leads: Carol Marston, Walsall CCG
Marcia Minnott, Dudley CCG
Carla Evans, Sandwell & West Birmingham CCG
Hemant Patel, Wolverhampton CCG
STP Finance Lead/Representative: Stacey Dixon, Dudley CCG
STP Communications Lead: Sophie Powers, BCWB Healthier Futures Partnership
STP Medicines Management Representative: Hemant Patel, Wolverhampton CCG
STP IM&T Lead: Mike Hastings, Black Country and West Birmingham CCG & BCWB Healthier Futures Partnership
STP Estates Lead: Andrew Lawley, BCWB Healthier Futures Partnership
STP Performance Lead: Martin Stevens, BCWB Healthier Futures Partnership
CCG Medicines Management Leads: Jonathan Boyd, Sandwell and West Birmingham CCG
Hannah Peach, Sandwell and West Birmingham CCG
Jyoti Saini, Walsall CCG
Duncan Jenkins, Dudley CCG Local Authority Flu Leads: Uma Viswanathan, Walsall Local Authority
Valerie Unsworth, Sandwell Local Authority
Barry Jones, Dudley Local Authority
Sophie Pagett, Wolverhampton Local Authority
Riva Eardley, Wolverhampton Local Authority Community Health Representative:
Professor Ann-Marie Cannaby, The Royal Wolverhampton NHS Trust
Tracie Wilson, Walsall CCG Community Pharmacy Facilitator: Hema Patel, Walsall CCG and Walsall Public Health
West Midlands Ambulance Service Flu Lead: Kim Nurse, WMAS
document name | 2
Acute Trust Representatives:
Mary Sexton, Dudley Group, NHS Foundation Trust
Professor Ann-Marie Cannaby, The Royal Wolverhampton NHS Trust
Kate Horton, Walsall NHS Trust
Karen Hanson, Dudley Foundation Trust
Dr Tranprit Salujia, Sandwell and West Birmingham Trust Mental Health, Learning Disabilities and Family services: Rebecca Purcell-Temple, Black Country Healthcare NHS Foundation Trust GP Representative:
Salma Reehana, Wolverhampton CCG
Dr Anand Rishie, Walsall CCG LMC Member: Dr Kewal Krishan, Wolverhampton LMC
Local Pharmacy Committee Member: Jeff Blankley, Wolverhampton, Birmingham & Solihull LPC
Ali Din, Sandwell LPC
Infection Prevention & Control Representatives: Barry Jones, Dudley Local Authority
Kim Corbett, The Royal Wolverhampton NHS Trust School Age Immunisation Program Representatives: James Hart – Vaccination UK
Fiona Nichols/David Coles, Birmingham Community Healthcare Trust Primary Care Representative: Lucy Sherlock, Wolverhampton CCG Project Support Representative: Raj Kular, BCWB Healthier Futures Partnership
If a member is unable to attend then a nominated deputy may attend on their behalf. Other staff members or stakeholders may be co-opted on to the Group as required for the Group to achieve its key objectives.
FREQUENCY
The Group will meet every four weeks.
SCOPE
This plan relates to: • NHS England and Improvement commissioned flu immunisations in the BCWB region for the elderly,
at-risk population, pregnant women, eligible healthy children, Healthcare Workers (HCWs) and Social Care Workers.
• Flu immunisations in health and social care workers organised by employers who remain responsible for offering and promoting flu uptake
• Roles and responsibilities for NHS England, CCGs, Local Authorities, immunisation providers, health and social care workers and other stakeholders.

document name | 3
OBJECTIVES
Develop and agree a STP seasonal flu plan for 2020/21 that includes:
• Governance arrangements for planning, implementation and monitoring – details of local groups including membership and frequency of meetings.
• Review of last year’s performance and identification of local priorities and initiatives • Review of population based data to identify local health inequalities for targeted action • Details of local assurance processes for ensuring practices order enough vaccine of the correct type
including processes for redistributing vaccine if required and allowed by any relaxation in MHRA regulations when announced
• Assurances processes and findings around: - Sufficient and correct flu vaccines ordered - Clarity on which GP Practices are operating as hot/cold sites - Clarity of PPE requirements and provision - Monitoring how long it takes to administer a flu vaccine due to Covid requirements - Additional staffing requirements - Additional venue requirements - Domiciliary service for shielded patients - Cold chain storage requirements - Enhanced call/recall requirements - PCN arrangements for flu immunisations
GOVERNANCE
The Black Country and West Birmingham system flu plan works across our 5 places; Dudley, Sandwell, Walsall, West Birmingham and Wolverhampton. This plan has been developed through place based teams, culminating into one plan. The flu plan will be overseen at each local place through the health protection forums. In addition the primary care response to flu will be reported through the primary care commissioning committee in common for BC&SW system. As such local governance arrangements are in place and the overall plan has been reported to the Healthier Futures Partnership Board. There is a STP strategic flu planning group set up to pull the 5 place plans together and provide an overall system plan for flu. Progress on delivery is reported to the healthier futures partnership board. A Healthier Futures Partnership representative will attend the NHS England Regional Flu Board.

1 PHE Gateway Ref: GW-1266 NHS England Publishing Approval Reference: 001638
Thursday 14 May 2020
Dear Colleague,
The national flu immunisation programme 2020/21 1. Thank you for all the hard work everyone is doing as part of the NHS response to the
global COVID-19 pandemic. It is more important than ever that we have effective plans in place for the 2020/21 flu season to protect those at risk, prevent ill-health and minimise further impact on the NHS and social care.
2. We recognise that delivering the flu immunisation programme is likely to be more challenging because of the impact of COVID-19 on our health and social care services. Further guidance will be issued about how to manage the immunisation programme to reflect circumstances nearer the planned start of the progamme in September 2020. Discussions to consider expansion of the flu programme for this autumn are underway, and we will write again with any changes in due course.
3. In the meantime, you should continue to plan for the programme as usual. This letter is to inform you which groups are eligible for flu vaccination this autumn and sets out actions that you can take now to prepare for this autumn’s vaccination campaign.
4. In particular, this season it will be more important than ever to ensure that sufficient
stocks of the recommended adult flu vaccines have been ordered for your eligible patients. In light of COVID-19, we ask Primary Care providers (General Practices and Community Pharmacies) to urgently review your vaccine orders now to make sure the number of vaccines ordered meet at least national ambitions and previous uptakes rates, whichever is highest. Please do so across your local Primary Care Network ensuring that the Clinical Commissioning Group flu lead is fully appraised of the position. If necessary, you may need to adjust your orders with suppliers.
5. For NHS Trusts and across Integrated Care System arrangements, please review your vaccine orders now to make sure the number of vaccines ordered meets your requirements for a vaccination programme to cover all frontline healthcare workers.

The national flu immunisation programme 2020 to 2021
2
Eligibility
6. In 2020/21 groups eligible for the NHS funded flu vaccination programme are the same as last year, although this may change if the programme is expanded, and include:
• all children aged two to ten (but not eleven years or older) on 31 August 2020
• those aged six months to under 65 years in clinical risk groups • pregnant women • those aged 65 years and over • those in long-stay residential care homes • carers • close contacts of immunocompromised individuals • health and social care staff employed by a registered residential
care/nursing home, registered domiciliary care provider, or a voluntary managed hospice provider.
7. We expect universal vaccination of health and care workers and further guidance will be published in due course.
Prioritising flu vaccine uptake
8. Flu vaccination is one of the most effective interventions we have to reduce pressure on the health and social care system this winter. We are currently seeing the impact of COVID-19 on the NHS and social care, and this coming winter we may be faced with co-circulation of COVID-19 and flu. We understand that planning this year is more challenging with the uncertainties of staff absences, and how long policies around social distancing and school closures will remain in place. However, it is more important than ever to make every effort to deliver flu vaccination.
9. Those most at risk from flu are also most vulnerable to COVID-19. We must do all we can to help protect them this winter. We anticipate that concerns about COVID-19 may increase demand for flu vaccination in all groups this year, and some in at risk groups may have concerns about maintaining social distancing when being given the vaccine.
10. All those eligible should be given flu vaccination as soon as possible so that individuals
are protected when flu begins to circulate. Providers should aim to schedule their immunisation services to match vaccine supply, usually from September, and complete vaccination by the end of November, where possible.

The national flu immunisation programme 2020 to 2021
3
Service specifications
11. The Directed Enhanced Service (DES) specification for seasonal influenza and pneumococcal immunisation sets out all eligible groups for vaccination (apart from those aged two and three on 31 August 2020). It includes eligible frontline health and care workers working in residential care and nursing homes, domiciliary care providers and the voluntary managed hospice sector. The DES can be found at: www.england.nhs.uk/gp/investment/gp-contract/
12. There is a separate Enhanced Service (ES) specification for the childhood seasonal influenza vaccination programme, covering the vaccination of children aged two and three years on 31 August 2020. The ES can be found at: www.england.nhs.uk/gp/investment/gp-contract/
13. General practices are reminded that both the DES and ES specifications require a
proactive call and recall system to contact all at risk patients. Various methods for this should be considered such as letter, email, phone call, text or social media and during face to face interactions if the opportunity arises, to encourage people to attend for their vaccination.
14. GP practices should also proactively call two and three year olds. This year the
national Childhood Health Information System (CHIS) service specification has been revised to include issuing an early communication to advise parents/carers of all eligible two and three years olds that they should access the flu vaccination from their GP practice. These communications are designed to support local call and recall initiatives. It is important that all children are given early protection through the flu vaccine, and GP practices should aim to complete flu vaccination by the end of November at the latest.
15. Community pharmacies offering a flu vaccination service for adults will be required to
do so in accordance with the Community Pharmacy Seasonal Influenza Vaccination Advanced service specification for 2020/21 which will be published at: www.england.nhs.uk/publication/community-pharmacy-seasonal-influenza-vaccine-service/
16. Planning for the school age programme should continue in the context of the current
constraints of school closures and staff redeployment. The school age immunisation service specification has a requirement that, to provide early protection, the provider will complete the flu vaccination as early as possible after the flu vaccine becomes available and at the latest by 15 December for all eligible children. School aged vaccination services must actively invite 100% of eligible children. Providers will be required, if asked, to demonstrate that such an offer has been made.
The national flu immunisation programme 2020 to 2021
4
Recommended vaccines for the national flu immunisation programme
17. Flu viruses change continuously and the World Health Organization (WHO) monitors the epidemiology of flu viruses throughout the world making recommendations about the strains to be included in vaccines. For further information on the strains for 2020/21 see the WHO website: www.who.int/influenza/vaccines/virus/recommendations/2020-21_north/en/
18. Providers should ensure that they have ordered adequate supplies of the recommended vaccines for their different patient groups, as set out in the letter from NHS England in December 2019: www.england.nhs.uk/wp-content/uploads/2019/12/NHS-England-JCVI-advce-and-NHS-reimbursement-flu-vaccine-2020-21.pdf
19. In summary these are:
• for those aged 65 and over – the adjuvanted trivalent influenza vaccine (aTIV) (with the cell-based quadrivalent influenza vaccine (QIVc) offered if aTIV is unavailable)
• for under-65s at risk, including pregnant women, offer QIVc or, as an alternative, the egg-grown quadrivalent influenza vaccine (QIVe)
20. The live attenuated influenza vaccine (LAIV) for children should be ordered through ImmForm from centrally purchased supplies and QIVe will be available to order for children in at risk groups aged less than 9 years old who are contraindicated to receive LAIV, in accordance with the letter referred to in paragraph 18. See: www.immform.dh.gov.uk
21. Children in at risk groups who are contraindicated to LAIV aged 9 years and over who access the vaccine through general practice should ideally be offered the QIVc from the practice’s locally procured vaccine stocks. GP practices offering QIVc to these children will be reimbursed by NHS England and NHS Improvement (NHSE/I). Where QIVc vaccine is unavailable, practices can either offer QIVe ordered through ImmForm from centrally purchased supplies (which will not be reimbursed), or their own locally procured QIVe which will be reimbursed by NHSE/I.
22. The DES and ES specifications state that in order for practices to receive payment for administration and reimbursement of vaccine they will need to use the specific flu vaccines recommended in the NHSEI guidance.
23. The Community Pharmacy Seasonal Influenza Vaccination Advanced Service specification sets out the requirements under which community pharmacies may provide flu vaccinations to eligible adult patients, including detailing the specific flu vaccines which are recommended by NHSE and are reimbursable under this service.
The national flu immunisation programme 2020 to 2021
5
Information and training resources for health professionals and PGDs
24. Healthcare practitioners should refer to the influenza chapter in ‘Immunisation against infectious disease’ (the “Green Book”) for further detail about clinical risk groups advised to receive flu immunisation and advice on contraindications and precautions for the flu vaccines. This can be found at: www.gov.uk/government/collections/immunisation-against-infectious-disease-the-green-book
25. Information for healthcare practitioners about the childhood flu programme and the inactivated flu vaccines, and links to training slide sets and flu e-learning programme will be available from: www.gov.uk/government/collections/annual-flu-programme and www.e-lfh.org.uk/programmes/flu-immunisation/
26. PHE will develop PGDs that will be available prior to commencement of the programme from: www.gov.uk/government/collections/immunisation-patient-group-direction-pgd and www.england.nhs.uk/publication/community-pharmacy-seasonal-influenza-vaccine-service/
Conclusion
27. We would like to take this opportunity to thank you all for your hard work in delivering the flu immunisation programme. Your continued efforts mean that we have some of the best flu vaccine uptake rates in Europe. This winter, more than ever, it is going to be a key intervention to reduce pressure on the NHS and social care.
28. We thank you for all your hard work in the most challenging of circumstances.
Yours sincerely, Prof Chris Whitty Prof Yvonne Doyle Prof Stephen Powis Chief Medical Officer Public Health England NHS England & NHS & Department of Medical Director & Improvement, National Health & Social Care Director for Health Medical Director Chief Scientific Adviser Protection Any enquiries regarding this publication should be sent to: [email protected] For operational immunisation queries, providers should contact their local screening and immunisation team.

The national flu immunisation programme 2020/21
6
Distribution list
General practices Community pharmacies Clinical commissioning groups clinical leaders Clinical commissioning groups accountable officers General Practitioners Committee NHS England & NHS Improvement regional directors NHS England & NHS Improvement regional directors of commissioning NHS England & NHS Improvement regional directors of primary care & public health NHS England & NHS Improvement heads of public health NHS England & NHS Improvement heads of primary care Sustainability and Transformation Partnership (STP) leads PHE centre directors PHE Screening and immunisation leads NHS foundation trusts chief executives NHS trusts chief executives Heads of nursing of NHS trusts Heads of midwifery of NHS trusts Chief pharmacists of NHS trusts Chief pharmacists of NHS Foundation trusts Directors of public health Local authority chief executives Chairs of health and wellbeing boards For information: Allied Health Professionals Federation Community Practitioners and Health
Visitors Association Nursing and Midwifery Council Royal College of Midwives Royal College of Nursing Academy of Medical Royal Colleges Royal College of Anaesthetists Royal College of Physicians Royal College of Surgeons Royal College of Obstetricians and
Gynaecologists Royal College of General Practitioners College of Emergency Medicine Faculty of Occupational Medicine Royal College of Pathologists Royal College of Ophthalmologists Royal College of Paediatrics and Child Health British Medical Association Royal Pharmaceutical Society Association of Pharmacy Technicians UK Company Chemist’s Association National Pharmacy Association
Pharmaceutical Services Negotiating Committee
Local Government Association Association of Directors of Adult Social
Services Council of Deans of Health General Medical Council General Pharmaceutical Council Faculty of Public Health Association of Independent Multiple Pharmacies UK Homecare Association (UKHCA) Skills for Care Association of Directors of Adult Social Services Care Association Alliance Care Provider Alliance Hospice UK Voluntary Organisations Disability Group National Care Forum (NCF) National Care Association (NCA) Care England ADASS (Association of Directors of Adult Social Services) Local Government Association Unison

The national flu immunisation programme 2020/21
7
Summary table of which influenza vaccines to offer
Eligible group Type of flu vaccine
At risk children aged from 6 months to less than 2 years
Offer QIVe.
LAIV and QIVc are not licenced for children under 2 years of age.
At risk children aged 2 to under 18 years
Offer LAIV If LAIV is contraindicated offer: • QIVe to children less than 9 years of age. • QIVc should ideally be offered to children aged 9 years and
over who access the vaccine through general practice. Where QIVc vaccine is unavailable, GPs should offer QIVe.
• It is acceptable to offer only QIVe to the small number of children contraindicated to receive LAIV aged 9 years and over who are vaccinated in a primary school setting.
Aged 2 and 3 years on 31 August 2020
All primary school aged children (aged 4 to 10 on 31 August 2020)
Offer LAIV
If child is in a clinical risk group and is contraindicated to LAIV (or it is otherwise unsuitable) offer inactivated influenza vaccine (see above).
At risk adults (aged 18 to 64), including pregnant women
Offer: • QIVc • QIVe (as an alternative to QIVc)
Those aged 65 years and over
Offer: • aTIV* should be offered as it is considered to be more effective than
standard dose non-adjuvanted trivalent and egg-based quadrivalent influenza vaccines.
• QIVc is suitable for use in this age group if aTIV is not available.
* It is recommended that those who become 65 before 31 March 2021 are offered aTIV ‘off-label’.
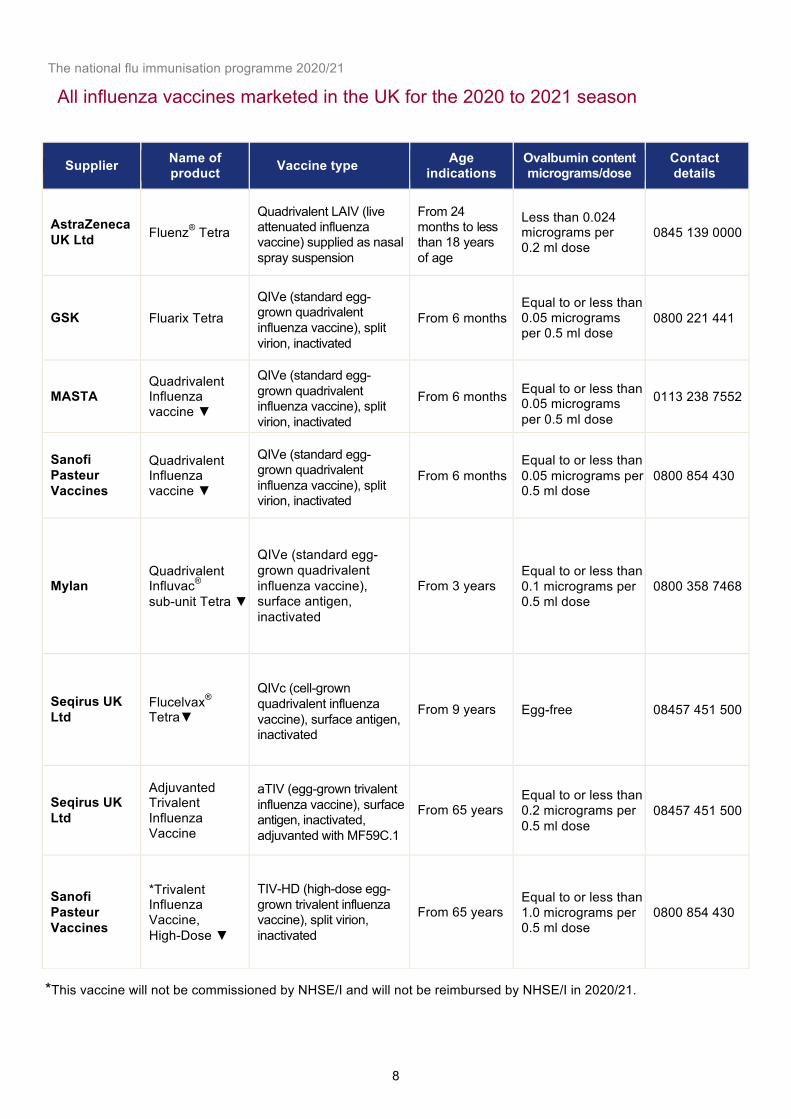
The national flu immunisation programme 2020/21
8
All influenza vaccines marketed in the UK for the 2020 to 2021 season
*This vaccine will not be commissioned by NHSE/I and will not be reimbursed by NHSE/I in 2020/21.
Supplier Name of product Vaccine type Age
indications Ovalbumin content micrograms/dose
Contact details
AstraZeneca UK Ltd Fluenz® Tetra
Quadrivalent LAIV (live attenuated influenza vaccine) supplied as nasal spray suspension
From 24 months to less than 18 years of age
Less than 0.024 micrograms per 0.2 ml dose
0845 139 0000
GSK Fluarix Tetra QIVe (standard egg- grown quadrivalent influenza vaccine), split virion, inactivated
From 6 months Equal to or less than 0.05 micrograms per 0.5 ml dose
0800 221 441
MASTA Quadrivalent Influenza vaccine ▼
QIVe (standard egg- grown quadrivalent influenza vaccine), split virion, inactivated
From 6 months
Equal to or less than 0.05 micrograms per 0.5 ml dose
0113 238 7552
Sanofi Pasteur Vaccines
Quadrivalent Influenza vaccine ▼
QIVe (standard egg- grown quadrivalent influenza vaccine), split virion, inactivated
From 6 months Equal to or less than 0.05 micrograms per 0.5 ml dose
0800 854 430
Mylan Quadrivalent Influvac® sub-unit Tetra ▼
QIVe (standard egg- grown quadrivalent influenza vaccine), surface antigen, inactivated
From 3 years Equal to or less than 0.1 micrograms per 0.5 ml dose
0800 358 7468
Seqirus UK Ltd
Flucelvax® Tetra▼
QIVc (cell-grown quadrivalent influenza vaccine), surface antigen, inactivated
From 9 years Egg-free 08457 451 500
Seqirus UK Ltd
Adjuvanted Trivalent Influenza Vaccine
aTIV (egg-grown trivalent influenza vaccine), surface antigen, inactivated, adjuvanted with MF59C.1
From 65 years Equal to or less than 0.2 micrograms per 0.5 ml dose
08457 451 500
Sanofi Pasteur Vaccines
*Trivalent Influenza Vaccine, High-Dose ▼
TIV-HD (high-dose egg- grown trivalent influenza vaccine), split virion, inactivated
From 65 years Equal to or less than 1.0 micrograms per 0.5 ml dose
0800 854 430
1 PHE Gateway Ref: 2020153 NHS England Publishing Approval Reference: B0096
Tuesday 4 August 2020
Dear Colleague,
The national flu immunisation programme 2020 to 2021- update 1. We write with more information about this year’s programme, further to the letter
published on 14 May1.
Expansion of the programme
2. In light of the risk of flu and COVID-19 co-circulating this winter, the national flu immunisation programme will be absolutely essential to protecting vulnerable people and supporting the resilience of the health and care system.
3. As indicated in our letter of 14 May, providers should focus on achieving maximum uptake of the flu vaccine in existing eligible groups, as they are most at risk from flu or in the case of children transmission to other members of the community. Appendix A provides the full list of those eligible in 2020/21 as part of the NHS funded flu vaccination programme. This includes individuals meeting existing flu eligibility criteria.
4. This year as part of our wider planning for winter, and subject to contractual negotiations, this season flu vaccination will be additionally offered to:
• household contacts of those on the NHS Shielded Patient List. Specifically individuals who expect to share living accommodation with a shielded person on most days over the winter and therefore for whom continuing close contact is unavoidable.
• children of school Year 7 age in secondary schools (those aged 11 on 31 August 2020).
• health and social care workers employed through Direct Payment (personal bugets) and/or Personal Health Budgets, such as Personal Assistants, to deliver domiciliary care to patients and service users
5. We aim to further extend the vaccine programme in November and December to include the 50-64 year old age group subject to vaccine supply. This extension is being phased to allow you to prioritise those in at risk groups first. Providers will be
1https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/885281/The_national_flu_immunisation_programme_2020_to_2021.pdf
The national flu immunisation programme 2020 to 2021
2
given notice in order to have services in place for any additional cohorts later in the season.
6. Department of Health and Social Care (DHSC) is exploring options to expand the workforce that is able to administer vaccinations as part of the COVID-19 response. Key stakeholders and the public will be consulted on the proposed changes over summer, including via stakeholder meetings. In line with the government’s consultation
principles, the consultation will be published on gov.uk in due course and will clearly set out the policy proposals.
7. Building on good practice from previous flu seasons and to reflect the need to achieve maximum coverage this year, all Hospital Trusts will be asked to offer vaccinations to pregnant women attending maternity appointments and to those clinically at risk eligible patients attending in- and out-patient appointments. National service specifications will be developed to support the standardised commissioning of these services.
8. In addition, this season an inactivated vaccine may be offered to those children whose parents refuse the live attenuated influenza vaccine (LAIV) due to the porcine gelatine content, in order to prevent localised outbreaks this year. Providers of children’s
vaccination services will receive further instruction on the offering of this service in due course.
9. It is essential to increase flu vaccination levels for those who are living in the most
deprived areas and from BAME communities. We need to ensure equitable uptake compared to the population as a whole and help protect those who are more at risk if they are to get COVID-19 and flu. It will therefore require high quality, dedicated and culturally competent engagement with local communities, employers and faith groups.
10. Providers are expected to ensure they have robust plans in place for tackling health
inequalities for all underserved groups to ensure equality of access.
11. Individuals eligible for flu vaccine this season should be offered a vaccine recommended for them according to their age, as detailed in Appendix B.
Frontline health and social care workers
12. All frontline health and social care workers should receive a vaccination this season. This should be provided by their employer, in order to meet their responsibility to protect their staff and patients and ensure the overall safe running of services. Employers should commission a service which makes access easy to the vaccine for all frontline staff, encourage staff to get vaccinated, and monitor the delivery of their programmes.

The national flu immunisation programme 2020 to 2021
3
13. For healthcare workers providers should use the current definition as set out in chapter 12 of the Green Book. https://www.gov.uk/government/publications/immunisation-of-healthcare-and-laboratory-staff-the-green-book-chapter-12
14. NHS Trusts should complete a self-assessment against a best practice checklist which has been developed based on five key components of developing an effective flu vaccination programme. The completed checklist should be published in public board papers at the start of the flu season. See Appendix C.
15. NHS England and Improvement (NHSEI) will continue to support vaccination of social care and hospice workers employed by registered residential or domiciliary care providers. The eligible groups have been expanded this year to include those health and social care workers, such as Personal Assistants, employed through Direct Payment and/or Personal Health Budgets to deliver domiciliary care to patients and service users. Vaccination will be available through community pharmacy or their registered general practice. This scheme is intended to complement, not replace, any established occupational health schemes that employers have in place to offer flu vaccination to their workforce. Further guidance on how providers can ensure their employees get vaccinated will be published shortly.
16. The Community Pharmacy Seasonal Influenza Advanced Service Framework will be
amended to enable community pharmacies to vaccinate both residential care/nursing home residents and staff in the home setting in a single visit to increase uptake rates and offer further protection to this vulnerable group of patients. GP practices are also able to vaccinate in the residential/care home, residents and staff who are registered with the practice.
17. Good practice guidance along with a range of resource material can be found here:
www.england.nhs.uk/increasing-health-and-social-care-worker-flu-vaccinations/. Further updates are underway to include additional resources which will be made available ahead of the flu season this year.
Vaccine supply
18. As usual, providers will have ordered flu vaccine directly from manufacturers. This season, we are expecting increased demand for flu vaccine across all cohorts and we are also expanding the flu programme. To support this, the Department of Health and Social Care (DHSC) has procured additional national supply of the adult vaccine and will issue guidance in September on how and when this can be accessed.
19. Two of the vaccines for use in the children’s programme have been procured by Public
Health England (PHE) and PHE has procured additional stock for this season.These are the live attenuated influenza vaccine (LAIV) administered as a nasal spray and

The national flu immunisation programme 2020 to 2021
4
suitable for use in children aged 2 to less than 18 years except where contraindicated, and the injectable egg-grown Quadrivalent Influenza Vaccine (QIVe) for children in clinical risk groups for whom LAIV is unsuitable due to contraindication or age. These vaccines can be accessed through Immform at https://portal.immform.phe.gov.uk.
20. For eligible children from 9 years of age unable to receive LAIV, locally procured QIVc
and QIVe are alternatively able to be given. For further information see Appendix E and www.england.nhs.uk/wp-content/uploads/2019/12/NHS-England-JCVI-advce-and-NHS-reimbursement-flu-vaccine-2020-21.pdf
Flu vaccine uptake ambitions
21. This year, we are asking for a concerted effort to significantly increase flu vaccination coverage and achieve a minimum 75% uptake across all eligible groups. Where possible, we expect uptake will be higher than this and a national supply of stock has been procured to ensure demand does not outstrip supply.
22. Many of the groups who are vulnerable to flu are also more vulnerable to COVID-19. Not only do we want to help protect those most at risk of flu, but also protect the health of those who are vulnerable to hospitalisation and death from COVID-19 by ensuring they do not get flu. The table below sets out the ambitions for 2020/21:
Table 1: Vaccine uptake ambitions in 2020 to 2021 Eligible groups
Uptake ambition
Aged 65 years and over At least 75%
In clinical at risk group At least 75%
Pregnant women At least 75% Children aged 2 and 3 year old At least 75% All primary school aged children and school year 7 in secondary school
At least 75%
Frontline health and social care workers
100% offer
23. Household contacts of people on the NHS Shielded Patient list will not be subject to call and recall arrangements but will be offered the vaccine opportunistically, with the aim to offer to all identified.
24. NHSEI are developing a national call and recall service to support localised call and recall provision and ensure that all eligible patients are informed of their eligibility and are encouraged to get vaccination this season. This service is intended to supplement not replace local call and recall mechanisms that are already in place contractually.
The national flu immunisation programme 2020 to 2021
5
Delivering the programme during the pandemic
25. Patients will, need reassurance that appropriate measures are in place to keep them safe from COVID-19, as it is likely to be co-circulating with flu. This reassurance will be especially important for those on the NHS Shielded Patient List.
26. Providers will be expected to deliver the programme according to guidelines on social distancing that are current at the time. Standard operating procedures in the context of COVID-19 have been issued for General Practice, community pharmacy, and community health services:
www.england.nhs.uk/coronavirus/publication/managing-coronavirus-covid-19-in-general-practice-sop/
www.england.nhs.uk/coronavirus/publication/standard-operating-procedure-community-pharmacy/
www.england.nhs.uk/coronavirus/publication/covid-19-prioritisation-within-community-health-services-with-annex_19-march-2020/
www.england.nhs.uk/coronavirus/publication/novel-coronavirus-covid-19-standard-operating-procedure-community-health-services/
27. For guidance on immunisation during COVID-19, including personal protective equipment, see: ‘Clinical Guidance for Healthcare professionals on maintaining
immunisation programmes during COVID-19’ at: www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/06/clinical-guidance-for-hcps-on-imms-for-covid-19.pdf
28. These procedures and guidance mean that a range of different ways of delivering the flu immunisation programme this year should be considered including the following:
• careful appointment planning to minimise waiting times and maintain social distancing when attending
• providing patients with information in advance of their appointment to explain what to expect
• recalling at risk patients if they do not attend in line with contract requirements
• social distancing innovations such as drive in vaccinations and ‘car as
waiting room’ models, if possible • for those on the Shielded Patient List who are high risk for COVID-19
consider the use of domiciliary visits
29. For the overall schools vaccination programme social distancing measures will create additional challenges, and where possible we still expect the school estate to be used in the event of any local school closures.
30. Providers need to be prepared to make adjustments to the programme in the face of any local restrictions to ensure those at highest risk can continue to be vaccinated.
The national flu immunisation programme 2020 to 2021
6
31. We are also considering supporting delivery through standing up alternative delivery
approaches, to maximise coverage of the vaccine this winter.
Infection prevention and control when administering vaccines
32. Individuals should attend for vaccination at premises that are following the recommended infection prevention and control (IPC) guidance. www.england.nhs.uk/coronavirus/primary-care/infection-control/
33. Those displaying symptoms of COVID-19, or who are self-isolating because they are confirmed COVID-19 cases or are contacts of suspected or confirmed COVID-19 cases, should not attend until they have recovered and completed the required isolation period.
34. Further information regarding infection prevention and control measures can be found
in the ‘Information for Healthcare Practitioner’ documents, which will be updated prior
to and during the season as required, and are available at: www.gov.uk/government/collections/annual-flu-programme
35. Healthcare professionals administering the vaccine will need to wear the recommended
personal protective equipment that is in line with the current advice from the government: www.gov.uk/government/publications/wuhan-novel-coronavirus-infection-prevention-and-control/covid-19-personal-protective-equipment-ppe
Communications and Marketing
36. The flu vaccination programme will be supported with a major new public facing marketing campaign to encourage take up amongst eligible groups for the free flu vaccine, due to launch in October. More detailed plans will be shared as these are developed.
37. PHE will make available a toolkit of adaptable campaign assets, highlighting the protective benefits of the flu vaccination, for NHS Trusts and social care organisations to use in their own staff vaccination campaigns.
38. Resources for both campaigns will be available to download and order from the PHE
Campaign Resource Centre at: https://campaignresources.phe.gov.uk/resources/

The national flu immunisation programme 2020 to 2021
7
List of appendices
39. Detailed planning information is set out in the following appendices:
Appendix A: Groups included in the national immunisation programme page 9 Appendix B: Summary table of which influenza vaccines to offer page 11
Appendix C: Healthcare worker best practice management checklist page 12
Appendix D: Children’s flu vaccination programme page 14
Appendix E: Vaccine ordering for children’s programme page 16
Appendix F: General Practice system supplier searches page 17
Appendix G: Data collection page 19
Appendix H: Antiviral medicines page 21
Conclusion
40. This year, more than ever, we need to protect those most at risk from flu. Thank you for all your hard work in these very challenging times.
41. This Annual Flu Letter has the support of the Chief Pharmaceutical Officer, the NHS Chief Nursing Officer for England and the Public Health England Chief Nurse.
Yours sincerely, Prof Chris Whitty Prof Yvonne Doyle Prof Stephen Powis Chief Medical Officer Public Health England NHS England & NHS for England Medical Director & Improvement, National Director for Health Medical Director Protection Any enquiries regarding this publication should be sent to: [email protected]. For operational immunisation queries, providers should contact their local screening and immunisation team.
The national flu immunisation programme 2020 to 2021
8
Distribution list
General practices Community pharmacies Clinical commissioning groups clinical leaders Clinical commissioning groups accountable officers General Practitioners Committee NHS England & NHS Improvement regional directors NHS England & NHS Improvement regional medical directors NHS England & NHS Improvement regional chief nurses NHS England & NHS Improvement regional directors of commissioning NHS England & NHS Improvement regional directors of primary care & public health NHS England & NHS Improvement heads of public health NHS England & NHS Improvement heads of primary care Sustainability and Transformation Partnership (STP) leads PHE centre directors PHE Screening and immunisation leads NHS foundation trusts chief executives NHS trusts chief executives Heads of nursing of NHS trusts Heads of midwifery of NHS trusts Chief pharmacists of NHS trusts Chief pharmacists of NHS Foundation trusts Directors of public health Local authority chief executives Chairs of health and wellbeing boards For information: Allied Health Professionals Federation Community Practitioners and Health
Visitors Association Nursing and Midwifery Council Royal College of Midwives Royal College of Nursing Academy of Medical Royal Colleges Royal College of Anaesthetists Royal College of Physicians Royal College of Surgeons Royal College of Obstetricians and
Gynaecologists Royal College of General Practitioners College of Emergency Medicine Faculty of Occupational Medicine Royal College of Pathologists Royal College of Ophthalmologists Royal College of Paediatrics and Child Health British Medical Association Royal Pharmaceutical Society Association of Pharmacy Technicians UK Company Chemist’s Association National Pharmacy Association Pharmaceutical Services Negotiating
Committee
Local Government Association Association of Directors of Adult Social
Services Council of Deans of Health General Medical Council General Pharmaceutical Council Faculty of Public Health Association of Independent Multiple Pharmacies UK Homecare Association (UKHCA) Skills for Care Association of Directors of Adult Social Services Care Association Alliance Care Provider Alliance Hospice UK Voluntary Organisations Disability Group National Care Forum (NCF) National Care Association (NCA) Care England ADASS (Association of Directors of Adult Social Services) Local Government Association Unison

The national flu immunisation programme 2020 to 2021
9
Appendix A: Groups included in the national flu immunisation programme
1. In 2020/21, flu vaccinations will be offered under the NHS flu vaccination programme to the following groups:
• all children aged two to eleven (but not twelve years or older) on 31 August 2020
• people aged 65 years or over (including those becoming age 65 years by 31 March 2021)
• those aged from six months to less than 65 years of age, in a clinical risk group such as those with: o chronic (long-term) respiratory disease, such as severe asthma,
chronic obstructive pulmonary disease (COPD) or bronchitis o chronic heart disease, such as heart failure o chronic kidney disease at stage three, four or five o chronic liver disease o chronic neurological disease, such as Parkinson’s disease or motor neurone
disease, o learning disability o diabetes o splenic dysfunction or asplenia o a weakened immune system due to disease (such as HIV/AIDS) or treatment
(such as cancer treatment) o morbidly obese (defined as BMI of 40 and above)
• all pregnant women (including those women who become pregnant during the flu season)
• household contacts of those on the NHS Shielded Patient List, or of immunocompromised individuals, specifically individuals who expect to share living accommodation with a shielded patient on most days over the winter and therefore for whom continuing close contact is unavoidable
• people living in long-stay residential care homes or other long-stay care facilities where rapid spread is likely to follow introduction of infection and cause high morbidity and mortality. This does not include, for instance, prisons, young offender institutions, university halls of residence, or boarding schools (except where children are of primary school age or secondary school Year 7).
• those who are in receipt of a carer’s allowance, or who are the main carer of an older or disabled person whose welfare may be at risk if the carer falls ill
• health and social care staff, employed by a registered residential care/nursing home or registered domiciliary care provider, who are directly involved in the care of vulnerable patients/clients who are at increased risk from exposure to influenza.
The national flu immunisation programme 2020 to 2021
10
• health and care staff, employed by a voluntary managed hospice provider, who are directly involved in the care of vulnerable patients/clients who are at increased risk from exposure to influenza.
• health and social care workers employed through Direct Payments (personal budgets) and/or Personal Health Budgets, such as Personal Assistants, to deliver domiciliary care to patients and service users.
2. Additionally, in 2020/21, flu vaccinations might be offered under the NHS flu
vaccination programme to the following groups:
• individuals between 50-64 years, following prioritisation of other eligible groups and subject to vaccine supply
3. Organisations should vaccinate all frontline health and social care workers, in order to meet their responsibility to protect their staff and patients and ensure the overall safe running of services.
4. The list above is not exhaustive, and the healthcare professional should apply clinical judgement to take into account the risk of flu exacerbating any underlying disease that a patient may have, as well as the risk of serious illness from flu itself.
5. Healthcare practitioners should refer to the influenza chapter in ‘Immunisation against
infectious disease’ (the “Green Book”) for further detail about clinical risk groups advised to receive flu immunisation and for full details on advice concerning contraindications and precautions for the flu vaccines. This can be found at: www.gov.uk/government/collections/immunisation-against-infectious-disease-the-green-book
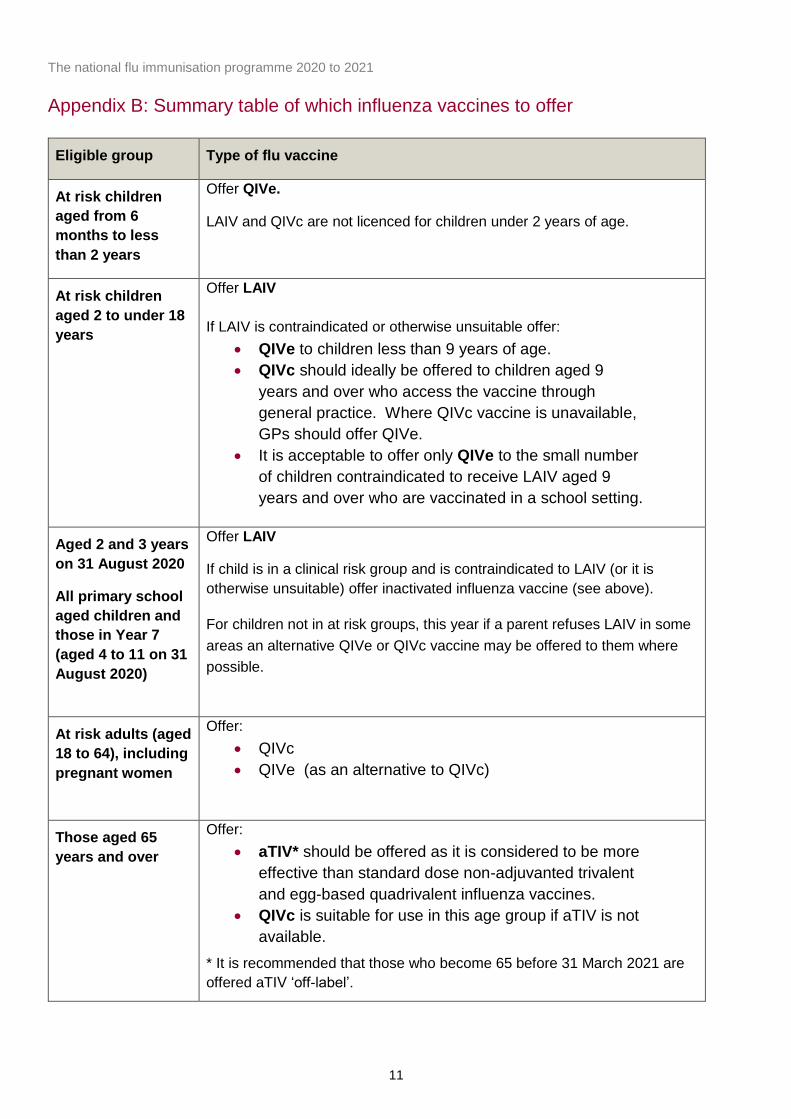
The national flu immunisation programme 2020 to 2021
11
Appendix B: Summary table of which influenza vaccines to offer
Eligible group Type of flu vaccine
At risk children aged from 6 months to less than 2 years
Offer QIVe.
LAIV and QIVc are not licenced for children under 2 years of age.
At risk children aged 2 to under 18 years
Offer LAIV If LAIV is contraindicated or otherwise unsuitable offer:
• QIVe to children less than 9 years of age. • QIVc should ideally be offered to children aged 9
years and over who access the vaccine through general practice. Where QIVc vaccine is unavailable, GPs should offer QIVe.
• It is acceptable to offer only QIVe to the small number of children contraindicated to receive LAIV aged 9 years and over who are vaccinated in a school setting.
Aged 2 and 3 years on 31 August 2020
All primary school aged children and those in Year 7 (aged 4 to 11 on 31 August 2020)
Offer LAIV
If child is in a clinical risk group and is contraindicated to LAIV (or it is otherwise unsuitable) offer inactivated influenza vaccine (see above).
For children not in at risk groups, this year if a parent refuses LAIV in some areas an alternative QIVe or QIVc vaccine may be offered to them where possible.
At risk adults (aged 18 to 64), including pregnant women
Offer: • QIVc • QIVe (as an alternative to QIVc)
Those aged 65 years and over
Offer: • aTIV* should be offered as it is considered to be more
effective than standard dose non-adjuvanted trivalent and egg-based quadrivalent influenza vaccines.
• QIVc is suitable for use in this age group if aTIV is not available.
* It is recommended that those who become 65 before 31 March 2021 are offered aTIV ‘off-label’.
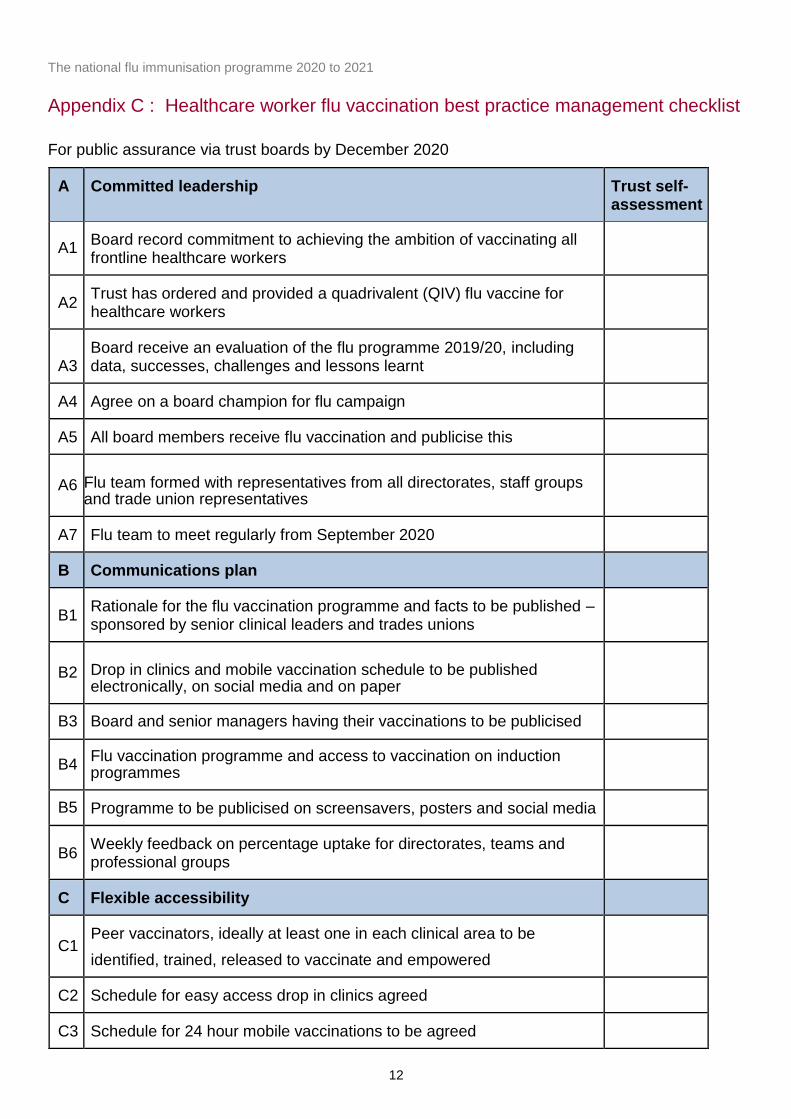
The national flu immunisation programme 2020 to 2021
12
Appendix C : Healthcare worker flu vaccination best practice management checklist
For public assurance via trust boards by December 2020
A Committed leadership Trust self- assessment
A1 Board record commitment to achieving the ambition of vaccinating all frontline healthcare workers
A2 Trust has ordered and provided a quadrivalent (QIV) flu vaccine for healthcare workers
A3 Board receive an evaluation of the flu programme 2019/20, including data, successes, challenges and lessons learnt
A4 Agree on a board champion for flu campaign
A5 All board members receive flu vaccination and publicise this
A6 Flu team formed with representatives from all directorates, staff groups and trade union representatives
A7 Flu team to meet regularly from September 2020
B Communications plan
B1 Rationale for the flu vaccination programme and facts to be published – sponsored by senior clinical leaders and trades unions
B2 Drop in clinics and mobile vaccination schedule to be published electronically, on social media and on paper
B3 Board and senior managers having their vaccinations to be publicised
B4 Flu vaccination programme and access to vaccination on induction programmes
B5 Programme to be publicised on screensavers, posters and social media
B6 Weekly feedback on percentage uptake for directorates, teams and professional groups
C Flexible accessibility
C1 Peer vaccinators, ideally at least one in each clinical area to be identified, trained, released to vaccinate and empowered
C2 Schedule for easy access drop in clinics agreed
C3 Schedule for 24 hour mobile vaccinations to be agreed

The national flu immunisation programme 2020 to 2021
13
D Incentives
D1 Board to agree on incentives and how to publicise this
D2 Success to be celebrated weekly
The national flu immunisation programme 2020 to 2021
14
Appendix D: Children’s flu vaccination programme
1. A recommendation to extend flu vaccination to children was made in 2012 by JCVI to provide both individual protection to the children themselves and reduce transmission across all age groups2. Implementation of the programme began in 2013 with pre-school children offered vaccination through GP practices and pilots for school aged children. In 2015/16 the programme began nationally in a phased roll-out starting with the youngest school-aged children first and was fully implemented for all primary school aged children in 2019/20.
2. This year as part of our wider planning for winter, in case we see flu and COVID-19 both circulating at the same time, PHE have secured additional vaccine to enable the programme to be extended into Year 7 in secondary schools in 2020/21. Although it is the first time Year 7 pupils will be offered the vaccine nationally, these children will have been offered the flu vaccine when they were in primary school so both they and their parents will be familiar with the programme.
3. In 2020/21 children will be offered vaccination in general practice or through a schools provider as follows:
• all those aged two and three years old on 31 August 2020 (date of birth on or after 1 September 2016 and on or before 31 August 2018) will be offered vaccine in general practice.
• all primary school children and Year 7 in secondary school (date of birth on or after 1 September 2008 and on or before 31 August 2016) will be offered through a school age immunisation service3
4. Research into the first three years of the childhood programme compared the differences between pilot areas, where the entire primary school age cohort was offered vaccination, to non-pilot areas. These include reductions in: GP consultations for influenza-like illness, swab positivity in primary care, laboratory confirmed hospitalisations and percentage of respiratory emergency department attendances4.
5. At risk children who are eligible for flu vaccination via the school-based programme because of their age will be offered immunisation at school. However, these children are also eligible to receive vaccination in general practice if the school session is late in the season, parents prefer it, or they missed the session at school. GP practices should invite
2 Joint committee on Vaccination and Immunisation. Statement on the annual influenza vaccination programme – extension of the programme to children. JCVI (2012). 25 July 2012. www.gov.uk/government/uploads/system/uploads/attachment_data/file/224775/JCVI-statement-on-the-annual-influenza-vaccination-programme-25-July-2012.pdf 3 Some children might be outside of these date ranges (e.g. if a child has been accelerated or held back a year). It is acceptable to offer and deliver immunisations to these children with their class peers. 4 Pebody, R. et al. 21 June 2018. Uptake and impact of vaccinating primary school-age children against influenza: experiences of a live attenuated influenza vaccine programme, England, 2015/16. Eurosurveillance. Volume 23, Issue 25. www.eurosurveillance.org/content/10.2807/1560-7917.ES.2018.23.25.1700496

The national flu immunisation programme 2020 to 2021
15
children in at-risk groups for vaccination, so that parents understand they have the option of taking up the offer in general practice.
6. Children in at risk groups for whom LAIV is contraindicated or unsuitable will be offered inactivated influenza vaccine.
7. As in previous years LAIV will be the vaccine offered to the routine age cohorts for the childhood flu vaccination programme as this is the most effective vaccine for this programme. However for 2020/21, consideration is being made to offer an injectable vaccine to those children whose parents object to the porcine gelatine in LAIV, to provide additional resilience against flu in what could be a challenging year. If the parent of a child eligible for the routine childhood immunisation programme refuses LAIV (and they understand that it is the most effective product) and they request an alternative vaccine, this will be offered to them where possible. Providers of childrens vaccination services will receive further instruction on the offering of this service, including vaccine supply arrangements, in due course.
8. Arrangements should be made to ensure that children who missed out on vaccination during
the school session are recalled and offered subsequent opportunities to attend. Precise arrangements for achieving this are for local determination. Children of primary school age who are home educated should also be offered vaccination. Local NHS England/Improvement Public Health Commissioning teams should be consulted for details about local arrangements. Contact details can be found at: www.england.nhs.uk/about/regional-area-teams/
The national flu immunisation programme 2020 to 2021
16
Appendix E: Vaccine ordering for children’s programme
1. The live attenudated influenza vaccine (LAIV) and the egg-grown Quadrivalent Influenza Vaccine (QIVe) are procured and supplied by Public Health England (PHE). For full details of the arrangements on which vaccines to use for children in risk groups who are unable to receive LAIV due to age or contraindications see www.england.nhs.uk/wp-content/uploads/2019/12/NHS-England-JCVI-advce-and-NHS-reimbursement-flu-vaccine-2020-21.pdf. Centrally supplied children’s vaccines
can be ordered through the ImmForm website: https://portal.immform.phe.gov.uk.
2. PHE ask that timing of vaccine availability is taken into account when earlier vaccination sessions are being arranged, to reduce the risk of disruption to planned activity. Vaccine availability will not be finalised until late summer. The latest and most accurate information on centrally supplied flu vaccines for the children’s programme is
available on the ImmForm news page.
3. As in previous years, ordering controls will be in place for Fluenz® Tetra in 2020/21 to enable PHE to manage vaccine availability and demand appropriately across the programme. The latest information on ordering controls and other ordering advice for PHE supplied flu vaccines is featured on the ImmForm news page both prior to and during the flu vaccination period. Information will also be featured in Vaccine Update www.gov.uk/government/collections/vaccine-update and disseminated via the National Immunisation Network as appropriate. It is strongly advised that all parties involved in the provision of flu vaccines to children ensure they remain up to date with this information.
The national flu immunisation programme 2020 to 2021
17
Appendix F: General practice system supplier searches for the 2020 to 2021 flu programme
1. Achieving the influenza vaccine uptake ambitions are a high priority within public health policy every year. In the current context of COVID-19, improving uptake and reducing the impact of flu on the wider health and social care system this priority cannot be understated in 2020/21.
2. GP practices are reminded that the Directed Enhanced Service requires that a proactive call and recall system is developed to contact all at-risk patients through mechanisms such as by letter, e-mail, phone call, or text. Any automated call and recall list should be subject to clinical review. Template letters for practices to use will be available at www.gov.uk/government/collections/annual-flu-programme nearer the time. Practices should also operate a proactive call system for patients not considered at-risk.
3. Public Health England (PHE) commission the PRIMIS team to provide the SNOMED CT code specifications to the general practice system suppliers. Your general practice system suppliers will then provide system searches using these codes to enable vaccine uptake monitoring.
4. It is essential that the general practice system searches are used for vaccine uptake monitoring
and NOT amended in any way by business support teams locally. This standard must be implemented to ensure accurate general practice system searches.
5. This approach will enable practices and support the collection of high quality, robust and timely
data on vaccine uptake throughout the delivery of the programme. This will also support GP practices and other providers to act to address issues relating to uptake.
6. Each year Public Health England (PHE) are required to collect data to monitor uptake and
coverage of the seasonal flu vaccination programme. This is done via two Seasonal Influenza Vaccine Uptake Surveys (approved by the Data Coordination Board, NHS Digital) with data obtained via automated data returns from general practice system suppliers on behalf of GP practices.
7. GP practices should also note that upon receipt of notification of vaccinations given by another
provider e.g. pharmacist/midwife, the vaccination should be recorded in the patients' electronic GP practice record in a timely manner. Any data extraction/uploads will only include patients vaccinated outside the GP practice if the information has been returned and appropriately recorded in the patients' GP practice record using the specified codes.
8. If you feel there are additional training requirements to carry out this approach arising from:
• practice staff turnover, new staff; • refresher training; and/or • new system functionality;
then you are advised to discuss these with your CCG who have a responsibility for training within the overarching general practice IT operating framework.

The national flu immunisation programme 2020 to 2021
18
9. The above is separate to the CQRS payment system, therefore your normal payment
mechanisms should be used to claim for vaccines given by the GP practice.
The national flu immunisation programme 2020 to 2021
19
Appendix G: Data collection
Introduction
1. As in previous years, data will be collected on the uptake of the vaccination. Currently, it is intended that these data collections will follow established processes. Flu vaccine uptake data collections will be managed using the ImmForm website https://portal.immform.phe.gov.uk. PHE coordinates the data collection and will issue details of the collection requirements and guidance on the data collection process. This guidance and flu vaccine uptake data will be available at: www.gov.uk/government/collections/vaccine-uptake
2. In addition to the established ImmForm data collection, further work is currently being undertaken by Public Health England, NHSx, NHS Digital and NHS England to improve the coverage and timeliness of these data collections as well as reducing the burden from data collections. As and when this further work matures, further information will be provided and may modify the data collection processes outlined below.
3. Queries concerning data collection content or process should be emailed to [email protected]. Queries concerning ImmForm login details and passwords should be emailed to [email protected].
Reducing the burden from data collections
4. Considerable efforts have been made to reduce the burden of data collections on GP practices by increasing the number of automated returns that are extracted directly from general practicesystem suppliers. Over 95% of GP practices benefited from using automated IT data returns for flu vaccine uptake for the final 2019/20 survey. GP practices that are not able to submit automated returns should discuss their arrangements with their general practice system supplier. If automated returns fail for the monthly data collection GP practices will be required to submit the mandatory data manually on to ImmForm to meet contractual obligations.
Data collections for 2020 to 2021
5. Monthly data collections will take place over five months during the 2020/21 flu immunisation programme. Subject to the approval from the Data Coordination Board the first data collection will be for vaccines administered by the end of October 2020 (data collected in November 2020), with the subsequent collections monthly thereafter, and with the final data collection for all vaccines administered by the end of February 2021 (final data collected in March 2021).
The national flu immunisation programme 2020 to 2021
20
6. Data will be collected and published monthly at national level, clinical commissioning group (CCG) level, local authority (LA) level, NHS Sustainable Transformation Partnerships and by 2019 NHS England local team level.
7. During the data collection period, those working in the NHS with relevant access rights
are able, through the ImmForm website, to: • see their uptake by eligible groups • compare themselves with other anonymous general practices or areas • validate the data on point of entry and correct any errors before data submission • view data and export data into Excel, for further analysis • make use of automated data upload methods (depending on the general practices
system supplier used at GP practices) • access previous years' data to compare with the current performance
These tools can be used to facilitate the local and regional management of the flu vaccination programme.
Monitoring on a weekly basis
8. Weekly uptake data will be collected from a group of GP practices that have fully automated extract and upload facilities provided by their general practice system suppliers. These data will be published in the PHE weekly flu report available throughout the flu season at: www.gov.uk/government/statistics/weekly-national-flu-reports.
9. During the data collection period, those working in the NHS with relevant access rights are able, through the ImmForm website to view this data as per the monthly collections.

The national flu immunisation programme 2020 to 2021
21
Appendix H: Antiviral medicines
1. Antiviral medicines (AVMs) have an important role to play in managing symptoms of flu for specified groups of patients, especially for people who may not get vaccinated against seasonal flu.
2. AVMs can only be prescribed by GPs and non-medical prescribers in primary care during the flu season, once a Central Alerting System (CAS) Alert has been cascaded to GP practices and community pharmacies by the Chief Medical Officer (CMO) and Chief Pharmaceutical Officer authorising the prescribing and supply of antiviral medicines AVMs at NHS expense, informed by surveillance data from Public Health England (PHE), that indicates that flu activity has risen above baseline levels, across a number of indicators.
3. Antiviral medicines may be prescribed for patients in “clinical at-risk groups” as well as
individuals who are at risk of severe illness and/or complications from influenza if not treated.
4. Information on clinical at risk groups and patients eligible for treatment in primary care at NHS expense with either oseltamivir or zanamivir is available from: www.gov.uk/government/publications/influenza-treatment-and-prophylaxis-using-anti-viral-agents
5. Once PHE informs DHSC that the level of seasonal flu activity is below threshold levels at the end of the flu season, another CMO CAS Alert is cascaded to stop the prescribing and supply of AVMs.
6. The statutory prescribing restrictions that apply to primary care do not apply in secondary care.
Hospital clinicians can continue to prescribe antiviral medicines for patients whose illness is confirmed or clinically suspected to be due to influenza, in accordance with PHE guidance for the treatment of complicated influenza.
7. The Department of Health and Social Care works with manufacturers of antiviral medicines
from summer and throughout the flu season to monitor supplies of antiviral medicines to ensure adequate stocks are available in the supply chain to meet demand.

PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: 25.8.2020 AGENDA ITEM:18.0
Title of Report: Estates Update
Purpose of Report: To update committee on approved projects, and Black Country estates issues.
Author of Report: Stephen Howells Management Lead/Signed off by: Andrew Lawley
Public or Private: Public
Key Points: Report summarises the status of approved projects and Black Country operational estates issues for the purposes of information.
Recommendation: Committee review the attached update for assurance and information.
Conflicts of Interest: None identified.
Links to Corporate Objectives:
Action Required: Assurance Approval For Information
Implications:
Financial
Assurance Framework
Risks and Legal Obligations
Equality & Diversity
Other

1
ESTATES UPDATE
August 2020
1. APPROVED PROJECTS 1.1 Carters Green (SWB CCG) The project comprises of a new building on the Sandwell General Hospital Site which involves the relocation of existing GP premises to address significant capacity and quality issues. The scheme is being led by Sandwell and West Birmingham Hospitals Trust. The ETTF allocation of £2.2m has been delayed by NHSEi awaiting resolution of other financial matters. The project was due for occupation February 2021, however there is now significant slippage due to suspension of construction during the period of COVID-19 lock down. Project Lead – Andrew Lawley Project Support – Anita Kumari 1.2 St Pauls (SWB CCG) A new Development Hub led by the GP to overcome significant over capacity issues within the Smethwick area. The new building will be located on Council land (Chatwin Street). The Practice continues to work through a complex land purchase with SMBC. A legal challenge regarding sale of the land is currently being defended by SMBC’s lawyers. It is hopeful that the land sale will be back on track August / September 2020. This along with programme delay due to COVID-19 will result in construction delays moving the delivery date from mid-2021 to late 2021. Project Lead – Andrew Lawley Project Support – Anita Kumari 1.3 Stoney Lane (SWB CCG) An ETTF funded project to provide an extension to the existing premises to improve capacity and quality which will lead to an increase in the number of consulting rooms and improve the overall flow of the building. The timeline had slipped due to COVID-19 creating delays of approximately 2 months due to the availability of materials. There is good progress being made, and all works (excluding a planned extension to the car park) should be finished around the middle of August.
2
The practice has successfully secured additional land to provide an improved car parking layout (improved access and additional spaces) subject to District Valuer CMR (current market rent). Project Lead – Hayley Haworth Project Support – Andrew Lawley 1.4 Newtown Medical Centre (SWB CCG) This project involves the relocation of GP’s from an existing NHS PS premises into a new GP led development to improve capacity and quality of environment and services for patients in the area. Following a period of site closure due to COVID-19 restrictions, works have recommenced, with an anticipated two-month delay to the programme the expected completion date is Oct / Nov 2020. Project Lead – Andrew Lawley Project Support – Hayley Haworth 1.5 Great Barr Group Practice (SWB CCG) Development of a new building on SMBC owned land at Queslade Close to accommodate co location of three GP Practices, resulting in considerable service improvement for patients in the area. The expected date for practical completion is 14th August 2020 with the earliest date for occupation being the 24th August (to provide solicitors time to complete the leases). Project Lead – Andrew Lawley Project Support – Hayley Haworth 1.6 156 Crankhall Lane (SWB CCG) Relocation of the existing 156a Crankhall Lane Medical Centre to a nearby site already owned by the practice (Friar Park) and for the redevelopment of the site which was previously a health facility. COVID-19 continues to cause a pause to this project. Project Lead - Hayley Haworth / Andrew Lawley Project Support - Anita Kumari 1.7 East Park Medical Practice (Wolverhampton CCG) A GP led ETTF scheme, comprising of a considerable proposed extension and reconfiguration to the existing premises creating additional Consulting Rooms and a refurbishment with additional car parking on the adjacent land currently on site and under construction, however works have been suspended on site due to the current COVID-19 situation. Project Lead – Steve Howells
3
Project Support – Hayley Haworth 1.8 (Sai) Forester Street Medical Centre (Walsall CCG) A project which is the result of the APMS procurement process, and is being delivered by NHS PS. Following the recent shut down of site activity due to Covid-19 works have yet to recommence on site to Phase 3. A pre-start meeting has been scheduled 13th July with a view to starting works on site 4th August. There has been an indicative completion date of 29th November which is currently being challenged by NHS PS who are seeking clarification and justification as to the longer programme, notwithstanding the COVID-19 affect. Project Lead – Steve Howells Project Support – Hayley Haworth 1.9 St Johns Surgery (Walsall CCG) A proposed Landlord/GP led extension which will be accompanied with a substantial refurbishment program that will also increase the number of clinical rooms within the existing building. The proposal received support and approval at the Walsall PCCC meeting 17/10/19. Planning Permission has been granted, the legal documents in terms of lease are complete pending signature. The building contract tenders are due back at the end of July, it is anticipate that works will start on site towards the end of August with a projected completion of March 2021 all subject to the signed documents being in place. A copy of the detailed documents and programme will be shared with the EDU once the contractor has been appointed and the legal documents signed. It should be noted that the project has suffered a delay due to COVID. Project Lead – Steve Howells Project Support – Hayley Haworth 1.10 Walsall Town Centre (Walsall CCG) A Town Centre Hub GP led project with ETTF funding. The FBC was approved at the PCCCic meeting by Walsall CCG members at the 23rd June 2020 meeting. NHSI/E are in the process of securing FBC sign off and approval which is imminent. All legal documents are due for completion by 3rd July including the formal planning consent and section 106/111 and the land sale. The proposed start on site is proposed for 11th September 2020 and completion for handover on 11th September 2022. Project Lead – Steve Howells / Andrew Lawley Project Support – Hayley Haworth 1.11 Rushall Medical Practice (Walsall CCG) The Practice have undertaken the creation of four additional consulting rooms and to move the reception by way of internal reconfiguration to improve the flow of the building and address the current patient confidentiality issues. The project is due to be complete
4
by the end of July 2020 however, the timeframe has been longer than anticipated due to COVID-19. Project Lead – Steve Howells Project Support – Hayley Haworth 1.12 Three Villages – Stourbridge Health and Social Care Centre (Dudley CCG) These works are to convert under-utilised administration space into clinical space, four clinical rooms, to improve the efficiency and effectiveness of the existing facility. This allows the closure of the Wollaston Branch absorbing the practice list size within the same demise area proving a more sustainable practice able to meet future housing increasing within the area and to also provided a broader range of clinical services. This is line with the CCG Health Infrastructure Strategy and BC STP to deliver enhanced services in the community health and social care buildings. Works have now commenced on site and is predicted for completion on 29th September 2020 (16 wks.). The construction phase plan recognises COVID as a risk. Project Lead – Mike Nicklin Project Support – Andrew Lawley 2. UPCOMING PROJECTS There are several projects in early development that will come forward into the public meeting at the appropriate time. This includes the following numbers projects in the respective CCG’s: Sandwell and West Birmingham CCG – two projects in the approval process, four projects in the early development process. Walsall CCG – two projects in the approval process, two projects in the early development process. Wolverhampton CCG – five projects in the approval process, four projects in the early development process. Dudley CCG – one project in the approval process, three projects in the early development process. 3. BLACK COUNTRY ESTATE 3.1 Planning Applications The EDU and Estates Team are now regularly receiving from the Local Councils, Planning Departments weekly Planning Application notifications from: Sandwell, Wolverhampton, West Birmingham and Walsall, in order to assess all new Major Planning Applications for Residential development against the impact of the existing Primary Care Estate. The purpose being that the Estates Team can assess the housing growth effects on existing premises in terms of capacity, condition and the potential for accommodating an increase in population growth and patient numbers. This

5
assessment will also enable the Estates Team to eventually negotiate contributions from Private Housing Developers by way of Capital Receipt, Physical Building (extension or new buildings) and Land Assembly or Transfer through entering into Section 106 Legal Agreements (also known as Planning Obligations). 3.2 NHS PS Leases The review of premises by the Estates Team is ongoing where NHS PS are sitting as a Head Lease Holder. Progress is being made on several sites, however this process can become protracted due to the legal due diligence and resolution of debt. The reasons are to consider the benefits of leases being direct between the Occupant/Provider and the Landlord. The premises being reviewed at present are where the Council are the Landlord, NHS PS are sitting in a Head Lease position and the Trust and/or GP’s are the tenant. The criteria for this process to be successful are: 1 – Where a lease has expired, 2 – Where a lease break is immanent, 3 – Where NHS PS add no value to the position, however all of the above criterion is subject to DHSC approval.
Further work is being down around the ability for NHS PS to provide TIR leases in lieu of the NHS PS preferred default FRI lease, however this proposal is subject to further scrutiny by NHS PS. Leases in general do remain an issue for GP’s and NHS PS in
particular the high number of Practices that are not in a current lease position. The Estates Team continue to monitor any changes to this situation as it becomes known.
3.3 Section 106 and CIL The Estate Team are continuing to work up the National Planning Policy Framework, Local Plan Policy relating to Section 106 and CIL, whereby the NHS economy can receive developer contributions into the NHS economy where largescale new housing developments are planned. The team are working with Council Planning and Policy Departments and the Black Country Core Plan team to approve and adopt the Planning Policy originally written by the Estates Team and now edited by the Local Council’s Planning Policy Teams. The final draft of the policy has now been agreed by the EDU and Councils, this will now go to future formal approval and future adoption. The EDU are now embarking on authoring a Supplementary Planning Document which will focus on the local detail relative to each Council in the Black Country. The EDU is also working across border with Staffordshire Council and Birmingham City Council to understand the impact of housing growth close to the BCWB CCG boundary. 3.4 Optispace The EDU are working on plans to implement the Optispace booking system across Black Country and West Birmingham CCG office accommodation to replicate what is already in operation at SWBCCG. This system will allow staff to book desks in order to facilitate social distancing in offices.
The EDU have been working up a solution to the vacant spaces in NHS PS and CHP premises which are currently being paid for by the CCG as void. This includes
6
categorizing space as Clinical or Office/Admin and added to the Optispace Booking System for NHS staff to access.
4. STP ESTATES The Black Country Estates Checkpoint document was submitted to NHSI’s coordinator in July 2019, and the Black Country STP retained its strong category rating. The EDU are continuing to review the Black Country STP priorities for future capital investment. It was agreed to update our register of STP NHS partners headline capital priorities to ensure we are prepared if any further opportunities to bid for finding arise in the immediate future. The work has been ongoing with further input required from the Black Country Partnership to understand the requirements of the emerging strategy. 5. ESTATES COMPLIANCE The CCG’s Estates team continues to work with both property companies NHS PS and CHP to monitor their management of statutory compliance. Both companies have satisfactory monitoring processes in place.
Document name goes here, document name goes here | 1 NHS Dudley Clinical Commissioning Group
NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Falsified Medicines Directive (FMD)
PRIMARY CARE COMMISSIONING COMMITTEES IN COMMON
DATE OF MEETING: AGENDA ITEM: 19.0
Title of Report: Falsified Medicines Directive (FMD)
Purpose of Report: Approval
Author of Report: Graham Westgate
Management Lead/Signed off by: Head of Medicines Management
Public or Private: Public
Key Points:
The purpose of this paper is to outline the Falsified Medicines Directive (FMD), to seek approval to form an appropriately represented working group and request funding to procure a solution for deployment to constituent GP practices within Black Country and West Birmingham CCGs.
The Directive introduces tougher rules to ensure medicines are safe and that the trade in medicines is rigorously controlled. This is a reaction to a reported significant increase of false medicinal products detected within the legal supply chain of the Member States.
Counterfeiting high-price medicines is perceived as a growing illegal business and a threat to public health worldwide.
Although legislation was effective from the 9th February 2019, the implementation of this was not immediate. At the time, the risk of a no deal Brexit meant that the UK would come out of the European Union without access to the drugs database that is used to verify falsified medicines.
Although no assurances are still given, we are required to work towards having a solution in place for FMD.
The Directive will impact on all healthcare bodies in the supply chain including dispensing and non-dispensing GPs, and will need to be considered by manufacturers, wholesalers and dispensers with an aligned approach.
More specifically, the legislation will require all prescription medicines for sale to carry a unique and randomised serial number encoded in a 2D-barcode and a visible anti-tampering device.
On supply to the patient, the unique identifier must be ‘decommissioned’ via a scan from the FMD system, to prevent any duplication of a legitimate identifier for use on a falsified medicine. This will be checked against data in the national repository.
All practices will need to have the infrastructure and processes in place to decommission medicines, even non-dispensing practices that prescribe and administer vaccines.
Recommendation: To set up a working group with the purpose of scoping and supporting the procurement, to confirm the correct route to procurement and validating the Black Country and West Birmingham GP practices to be included.
To procure as Black Country and West Birmingham CCGs to identify other providers for this solution which may fulfil the requirements of this directive.
To secure funding to enable compliance with the FMD directive for all Black Country and West Birmingham CCGs.
Conflicts of Interest: None identified
Links to Corporate Objectives:
Action Required: Assurance Decision
Implications:
Financial N/A
Assurance Framework N/A
Risks and Legal Obligations Non-compliance with the directive
Equality & Diversity N/A
Other N/A

NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Falsified Medicines Directive

Falsified Medicines Directive | 2 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Table of Contents 1 Purpose ..................................................................................................................................... 3
2 Background .............................................................................................................................. 3
3 Project ....................................................................................................................................... 4
3.1 FMD Solution EGTON/ EMIS – ...................................................................................................... 4
3.2 Additional Opportunities .............................................................................................................. 5
3.3 Costs (Egton indicative costs from Oct. 2019) ........................................................................... 6
4 Recommendations ................................................................................................................... 6
5 Committee Actions .................................................................................................................. 7
APPENDIX A – Original Falsified Meds Directive ........................................................................ 8
APPENDIX B – EGTON/ EMIS Quote ............................................................................................. 8

Falsified Medicines Directive | 3 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
1 Purpose The purpose of this paper is to outline the Falsified Medicines Directive (FMD), to seek approval to form an appropriately represented working group and request funding to procure a solution for deployment to constituent GP practices within Black Country and West Birmingham CCGs.
2 Background Following adoption by the Council and the European Parliament, the Falsified Medicines Directive (FMD) (Directive 2011/62/EU) was published on 1 July 2011 (Appendix A) in the Official Journal of the European Union. The Falsified Medicines Directive had to be transposed by member states by 2nd January 2013.
The Directive introduces tougher rules to ensure medicines are safe and that the trade in medicines is rigorously controlled. This is a reaction to a reported significant increase of false medicinal products detected within the legal supply chain of the Member States.
Counterfeiting high-price medicines is perceived as a growing illegal business and a threat to public health worldwide.
In order to tackle the problem a number of measures are proposed:
• The introduction of safety features to ensure full traceability of any prescription item, so identifying more easily false representations of medicinal products
• Improving the control at the EU external borders through which false medicinal products could enter; and
• Ensuring the active pharmaceutical ingredients are of a high quality standard and not falsified.
This is a significant change that will affect all those in the pharmaceutical supply chain.
The Government agreed to adopt the Directive, which meant practices should be preparing for implementation and be able to demonstrate compliance with the Directive.
Although legislation was effective from the 9th February 2019, the implementation of this was not immediate. At the time, the risk of a no deal Brexit meant that the UK would come out of the European Union without access to the drugs database that is used to verify falsified medicines.
Although no assurances are still given, we are required to work towards having a solution in place for FMD.
The Directive will impact on all healthcare bodies in the supply chain including dispensing and non-dispensing GPs, and will need to be considered by manufacturers, wholesalers and dispensers with an aligned approach.
More specifically, the legislation will require all prescription medicines for sale to carry a unique and randomised serial number encoded in a 2D-barcode and a visible anti-tampering device.
The unique identifier comprises:
• a product code, which allows the identification of at least the name of the medicine, the common name, the pharmaceutical form, the strength, the pack size and the pack type
Falsified Medicines Directive | 4 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
• a serial number which is a numeric or alphanumeric sequence of a maximum of 20 characters randomly generated
• a batch number
• an expiry date
It will be the responsibility of manufacturers to upload the serial numbers to a system of national databases linked by a European hub (although only 15% of products are expected to be compliant from February), while country-based national data repositories will allow verification at different times and final decommissioning when each pack is dispensed to a patient.
At each stage of the supply chain, the product will be inspected to ensure it has not been tampered with, has not previously been dispensed and that the packaging remains intact. Additionally, goods distribution practice guidelines will require the individual product to be scanned to record the batch number and expiry date. This check will indicate whether the product is authentic and bring up information such as whether the product has been subject to a recall.
On supply to the patient, the unique identifier must be ‘decommissioned’ via a scan from the FMD system, to prevent any duplication of a legitimate identifier for use on a falsified medicine. This will be checked against data in the national repository.
All practices will need to have the infrastructure and processes in place to decommission medicines, even non-dispensing practices that prescribe and administer vaccines. They will also need to decide whether they decommission medicines at the point of dispensing or in advance, although practices should take into consideration the proposed 10-day window in which they will be able to recommission the medication into the system.
3 Project In response to the directive a project was requested of WHT IT services by the Walsall CCG, Heads of Meds Management, in 2019/20 Q1 to meet the requirements of the directive, though has made limited progress due to the directive being placed on hold, uncertainties regarding Brexit and the recent COVID-19 pandemic.
However, during that period, the EGTON/ EMIS FMD solution was investigated and a demonstration of the Egton/ EMIS FMD solution was provided in 2019/20 Q3 to Black Country CCGs IT Meds Management and IT leads. As a significant proportion of Black Country CCGs utilise EMIS as their principle clinical system, it was agreed a standardised approach across the Black Country would be beneficial and a quotation was provided for consideration. See appendix B.
3.1 FMD Solution EGTON/ EMIS – Regardless of a GP practice dispensing status, the FMD will mean that staff will have to decommission vaccines and medication at the point of administration or issue and practices will require hardware and software to fulfil Falsified Medicines Directive requirements.
Falsified Medicines Directive | 5 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Practices will be expected to verify medication upon receipt and require the capability to decommission medicines.
• For dispensing practices, there will be a requirement to decommission packs of medication at the point of being issued to the patient.
• For non-dispensing practices, there’s a requirement to decommission vaccines once administered to patients.
The EGTON/ EMIS FMD Authenticator is a stand-alone internet-based application that can be accessed on any device that has a connection to the internet. The use of FMD Authenticator has the capability to spot counterfeit medications and identify which medications are most suitable for patients, greatly improving patient safety.
By scanning medication packages using the FMD Authenticator solution, the validity of medications can be verified as well as recommission or decommission relevant packages. Medications can be marked as ‘Sample’ or ‘Destroyed’ to effectively track medicines and stock.
Every item scanned is checked against the register within the National Medicine Verification System (NMVS). NMVS will instantly respond with the status of the item(s), and alert them as to whether the medicine is valid or not. The user then determines whether it is appropriate to administer the medication based on the response they receive.
Whilst the solution doesn’t currently integrate with EMIS Web, i.e. the system cannot be launched from within EMIS, it may integrate with the future version of EMIS (EMIS X). It is important to note that no other solutions integrate with EMIS and at the time of writing this report there are no plans for them to do so.
3.2 Additional Opportunities The deployment of the Egton solution would also provide an opportunity in the future to implement the EMIS dispensing module to respective practice potentially introducing further efficiencies to associated processes. However, the procurement across the CCGs will identify the most appropriate solution for FMD.

Falsified Medicines Directive | 6 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
3.3 Costs (Egton indicative costs from Oct. 2019) Year Description Cost per
practice location
GP Practice Locations (incl. branch
sites)
Net Total VAT Total
2020/21 Scanner, support & maintenance costs, delivery
£409 260 £106,340 £21,268 £127,608
2021/22 Annual Support & maintenance
£150 260 £39,000 £7,800 £46,800
2022/23 Annual Support & maintenance
£150 260 £39,000 £7,800 £46,800
Total cost over 3 years £184,340 £36,868 £221,208
Additional costs are expected to be confirmed through the procurement from supplier responses including project management and business change resources.
4 Recommendations
To procure as Black Country and West Birmingham CCGs to identify other providers for this solution which may fulfil the requirements of this directive.
To secure funding to enable compliance with the FMD directive for all Black Country and West Birmingham CCGs.
To set up a working group with the purpose of scoping and supporting the procurement, to confirm the correct route to procurement and validating the Black Country and West Birmingham GP practices to be included.
Suggested working group members /roles;
• Medicines Management Leads
• Primary care digital
• GP leads/ advisors
• Primary Care Commissioners
• IT service provider
• Contracting leads
Falsified Medicines Directive | 7 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
Approval and support has also been gained from The Black Country and West Birmingham STP Digital Programme Board and the STP Pharmacy Leadership Group.
5 Committee Actions The Committee are invited to:
• To note the report
• To agree to setting up a working group
• To agree to funding that is required to enable compliance with the FMD directive.

Falsified Medicines Directive | 8 NHS Dudley Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Walsall Clinical Commissioning Group NHS Wolverhampton Clinical Commissioning Group
APPENDIX A – Original Falsified Meds Directive https://www.gov.uk/guidance/implementing-the-falsified-medicines-directive-safety-features
APPENDIX B – EGTON/ EMIS Quote
Egton Quote 69288 - 17 October 2019 1323