Embed Size (px)
Citation preview
Department of Infectious Diseases and Neuroinfections, Medical University of Bialystok, Poland
Anna Moniuszko-Malinowska
Medical University of Bialystok
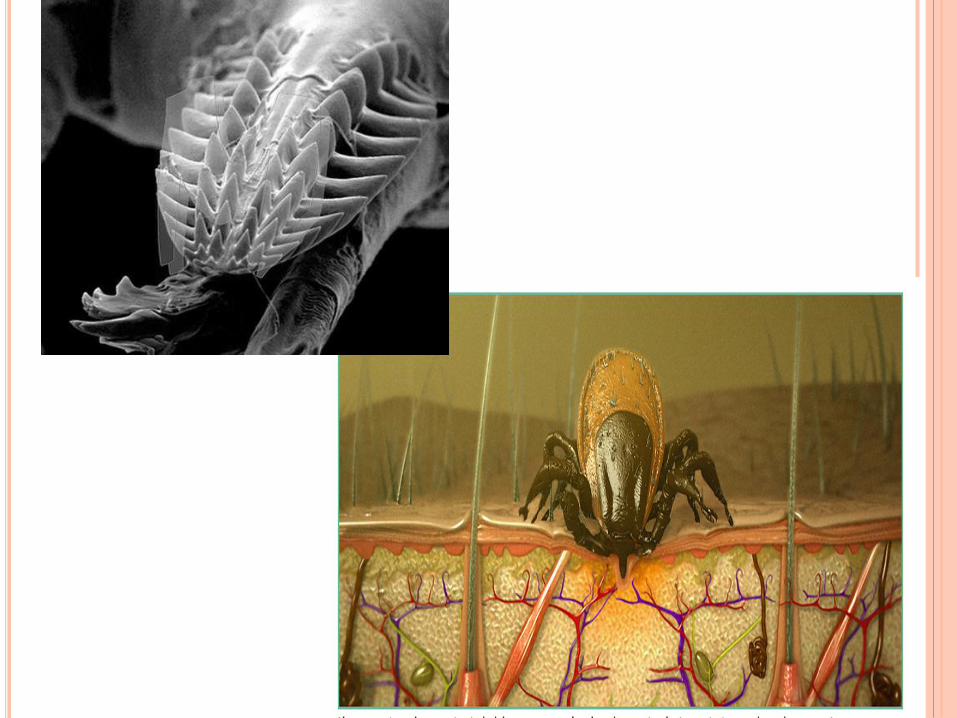
TICKS
Photo by Dr M. Kondrusik, Bialystok, Poland

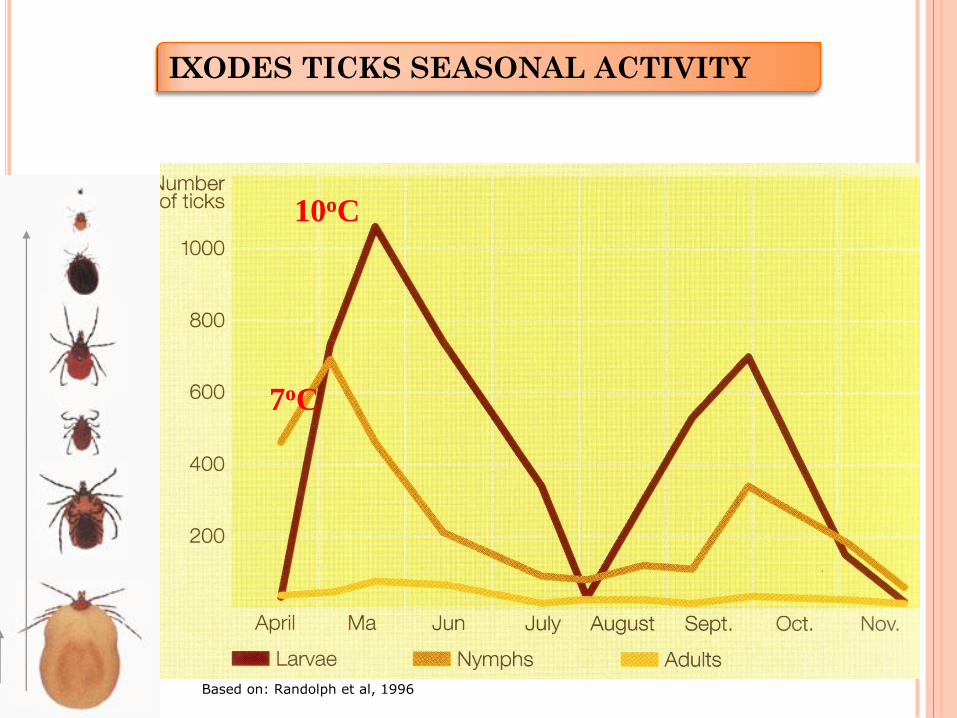
7oC
10oC
IXODES TICKS SEASONAL ACTIVITY
Based on: Randolph et al, 1996
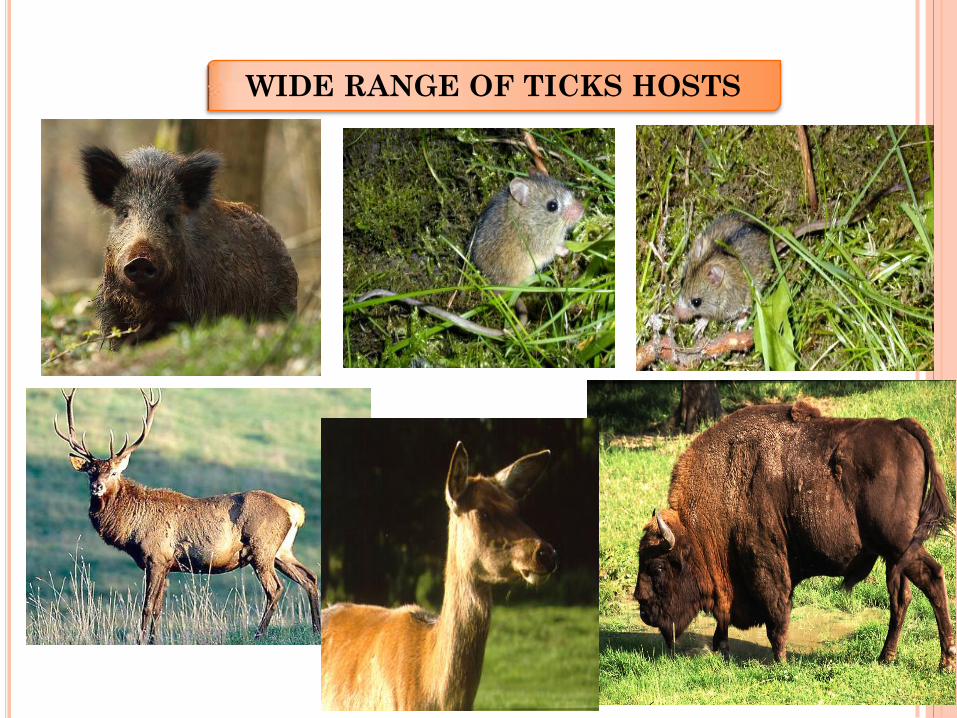
WIDE RANGE OF TICKS HOSTS
TBE virus
Flaviviridae (other close relatives: Omsk hemorrhagic fever virus,
Kyasanur forest disease virus, Louping ill virus, Langat virus,
Yellow Fever, West Nile, Japanese Encephalitis, Dengue viruses)
3 subtypes:
1.Western European subtype (formerly Central European
encephalitis virus, CEEV; principal tick vector: Ixodes ricinus)
2.Siberian subtype (formerly West Siberian virus; principal tick
vector: Ixodes persulcatus)
3.Far Eastern subtype (formerly Russian Spring Summer
encephalitis virus, RSSEV; principal tick vector: Ixodes persulcatus)
Mandl et al., 1997; Grard et al., 2007
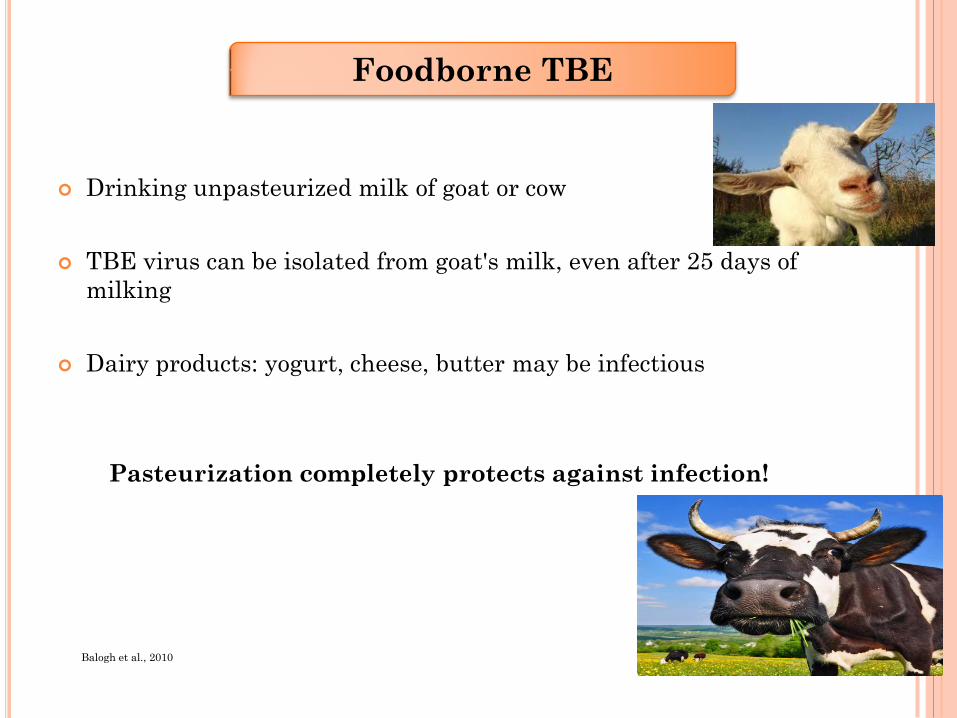
Drinking unpasteurized milk of goat or cow
TBE virus can be isolated from goat's milk, even after 25 days of
milking
Dairy products: yogurt, cheese, butter may be infectious
Pasteurization completely protects against infection!
Foodborne TBE
Balogh et al., 2010
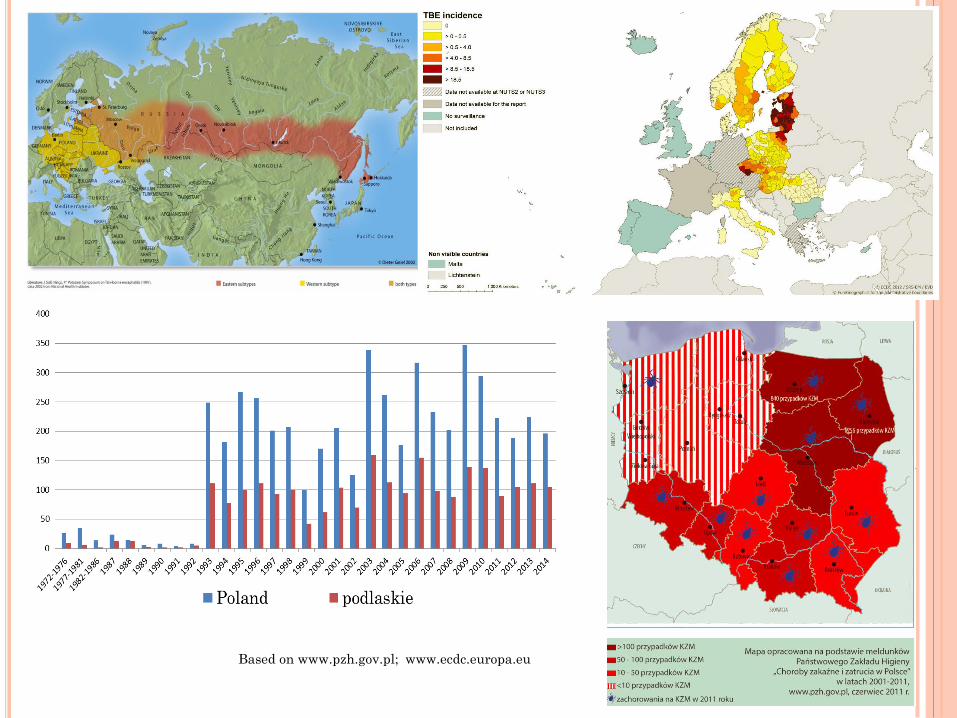
Based on www.pzh.gov.pl; www.ecdc.europa.eu
Forestry workers
National Parks employees
Mushrooms pickers
Berry pickers
Hunters
Dogs owners
RISK GROUPS
Depending on location of inflammatory process
neurologic phase of infection may take course of:
Meningitis
Meningoencephalitis
Meningoencephalomyelitis
Clinical presentation
Maximova et al., 2009
www.humanillnesses.com
0
10
20
30
40
50
60
70
80
90
100
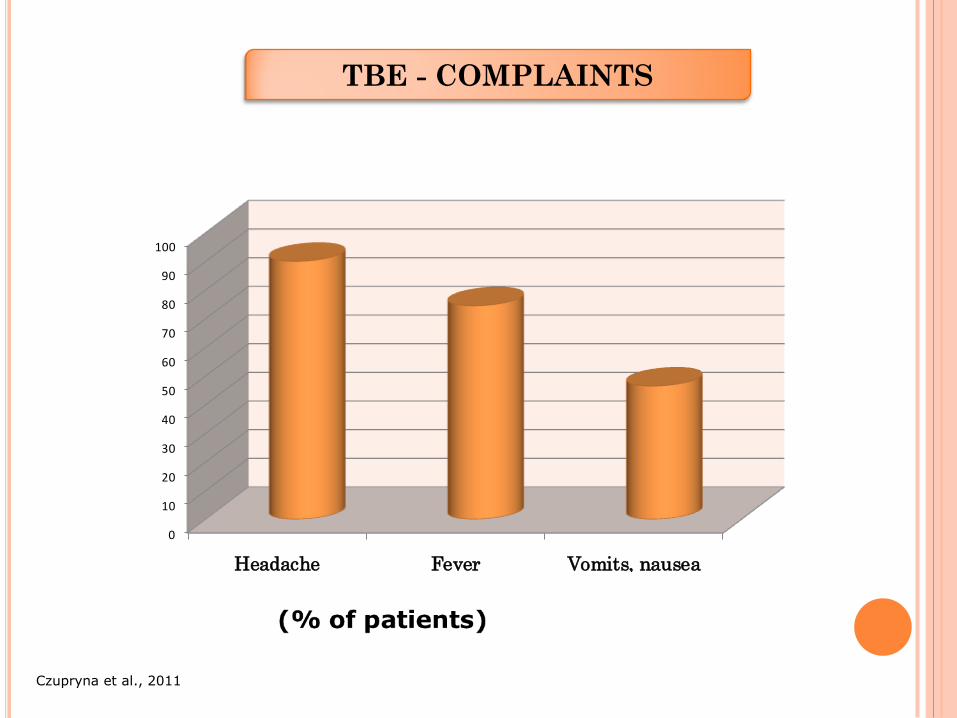
Headache Fever Vomits, nausea
TBE - COMPLAINTS
Czupryna et al., 2011
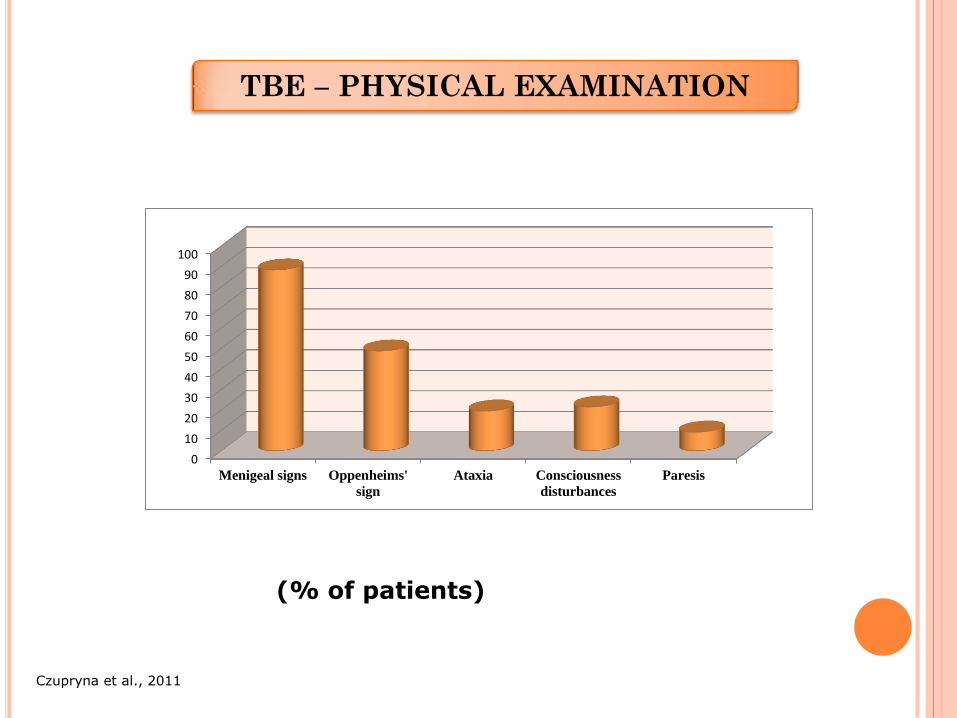
TBE – PHYSICAL EXAMINATION
0
10
20
30
40
50
60
70
80
90
100
Menigeal signs Oppenheims'
sign
Ataxia Consciousness
disturbances
Paresis
Czupryna et al., 2011
(% of patients)
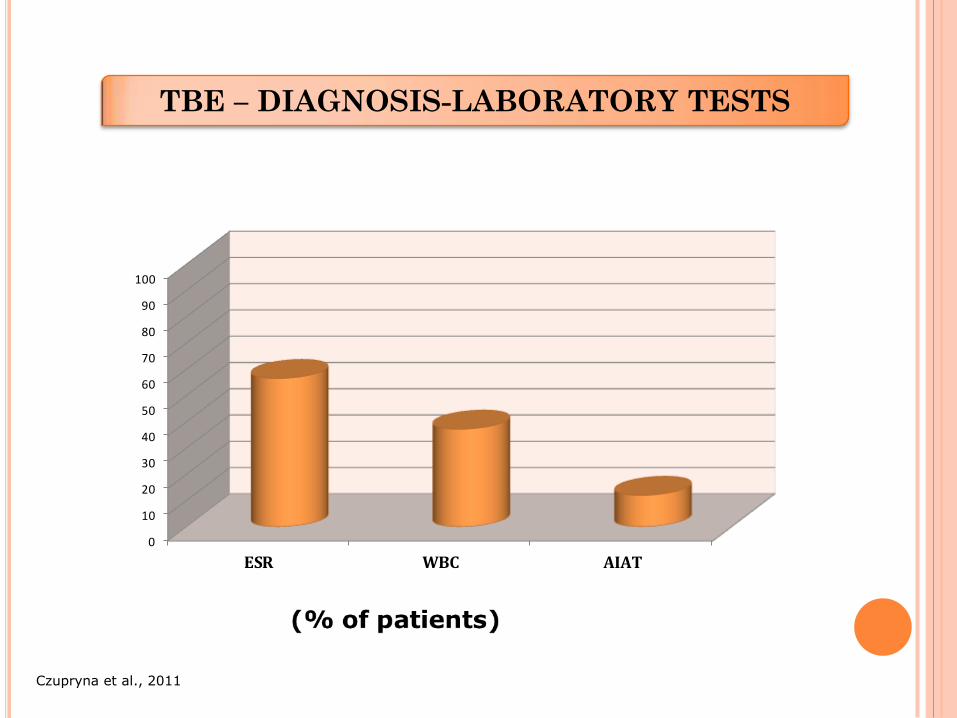
TBE – DIAGNOSIS-LABORATORY TESTS
0
10
20
30
40
50
60
70
80
90
100
ESR WBC AIAT
Czupryna et al., 2011
• Cerebrospinal fluid examinations
• Pleocytosis – 5 – 1000 cells/µl
• Lymphocytes predominate
• Protein concentration – normal or elevated
(>50 mg/ml)
• Glucose concentration - normal
TBE – LABORATORY TESTS
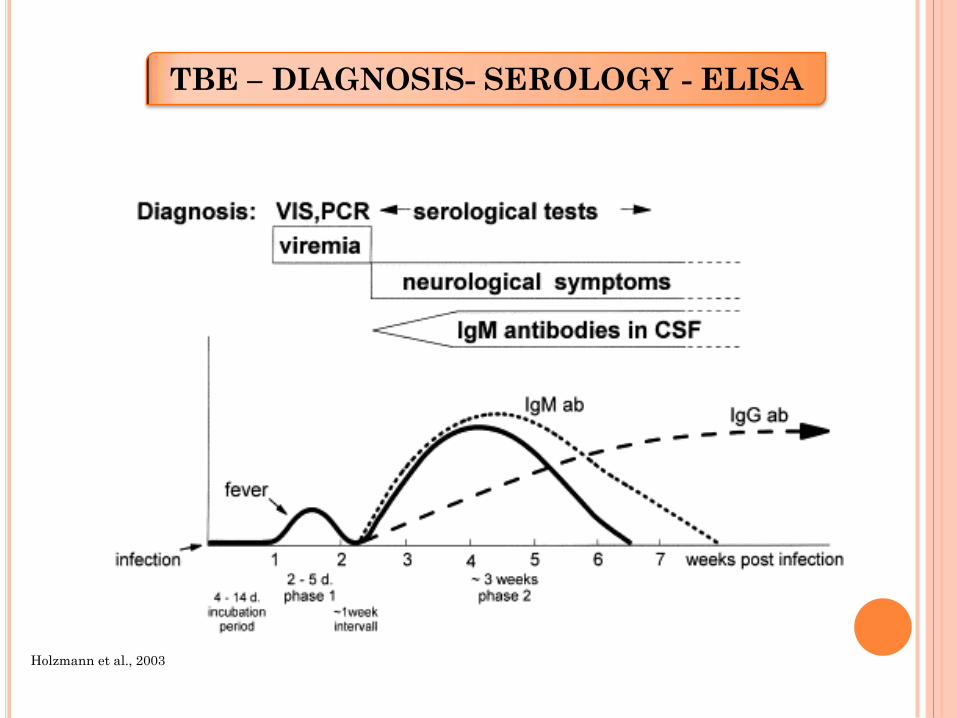
TBE – DIAGNOSIS- SEROLOGY - ELISA
Holzmann et al., 2003
a) no possibility of causative treatment
b) antioedematous drugs (mannitol, diuretics)
c) pain-killers
d) antinflammatory drugs (NSAID)
e) steroids (exceptional cases)
TBE – TREATMENT
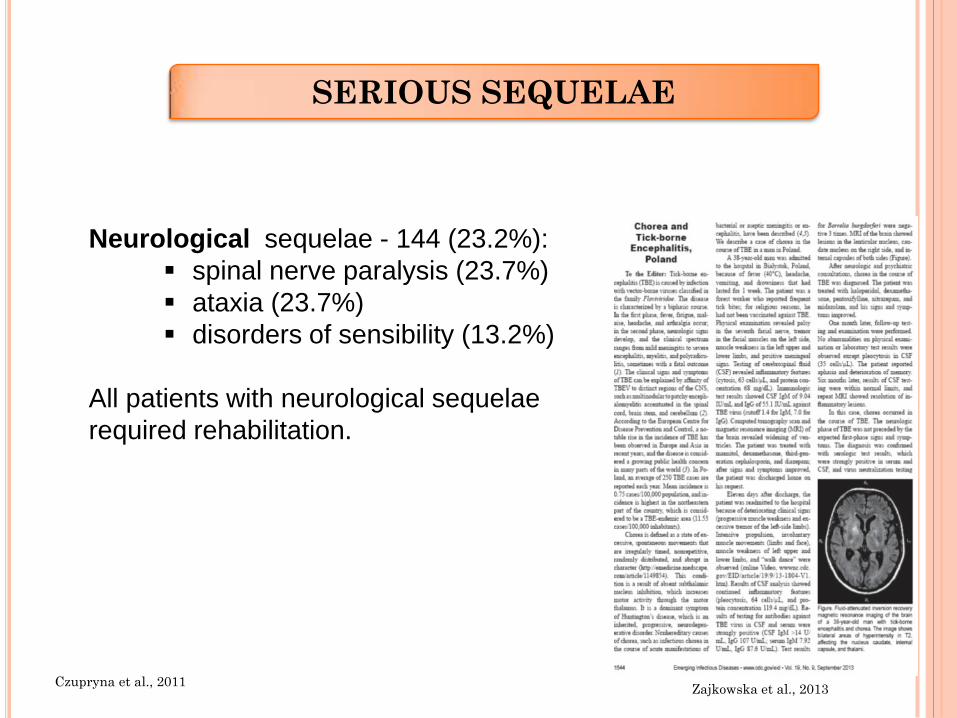
Neurological sequelae - 144 (23.2%):
spinal nerve paralysis (23.7%)
ataxia (23.7%)
disorders of sensibility (13.2%)
All patients with neurological sequelae
required rehabilitation.
SERIOUS SEQUELAE
Zajkowska et al., 2013 Czupryna et al., 2011
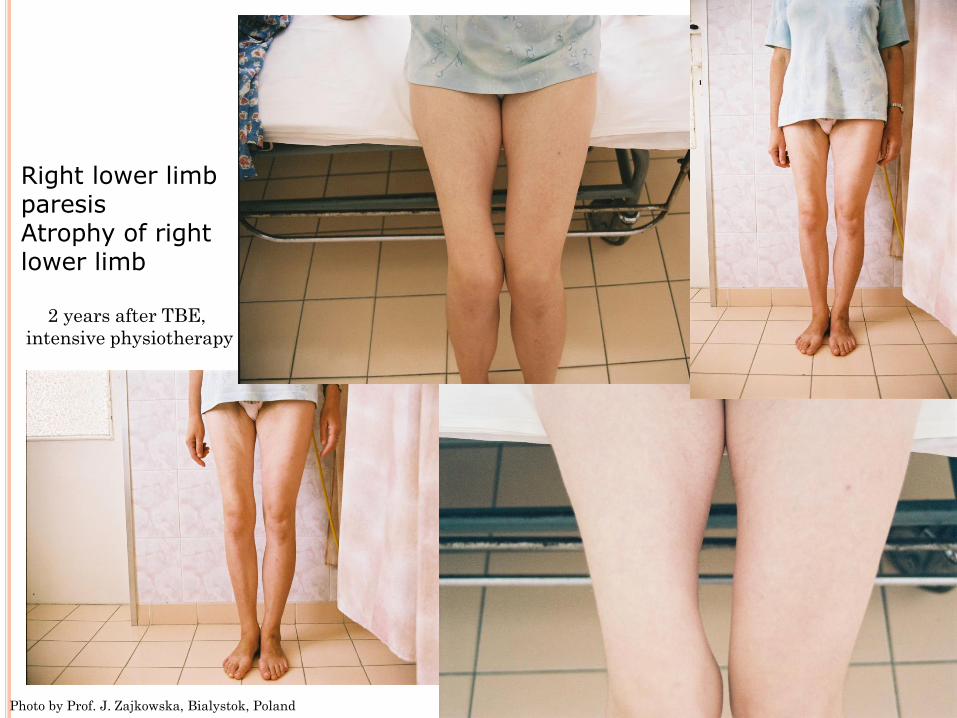
2 years after TBE,
intensive physiotherapy
Right lower limb paresis Atrophy of right lower limb
Photo by Prof. J. Zajkowska, Bialystok, Poland

Right brachial plexus paresis
Photo by Prof. J. Zajkowska, Bialystok, Poland
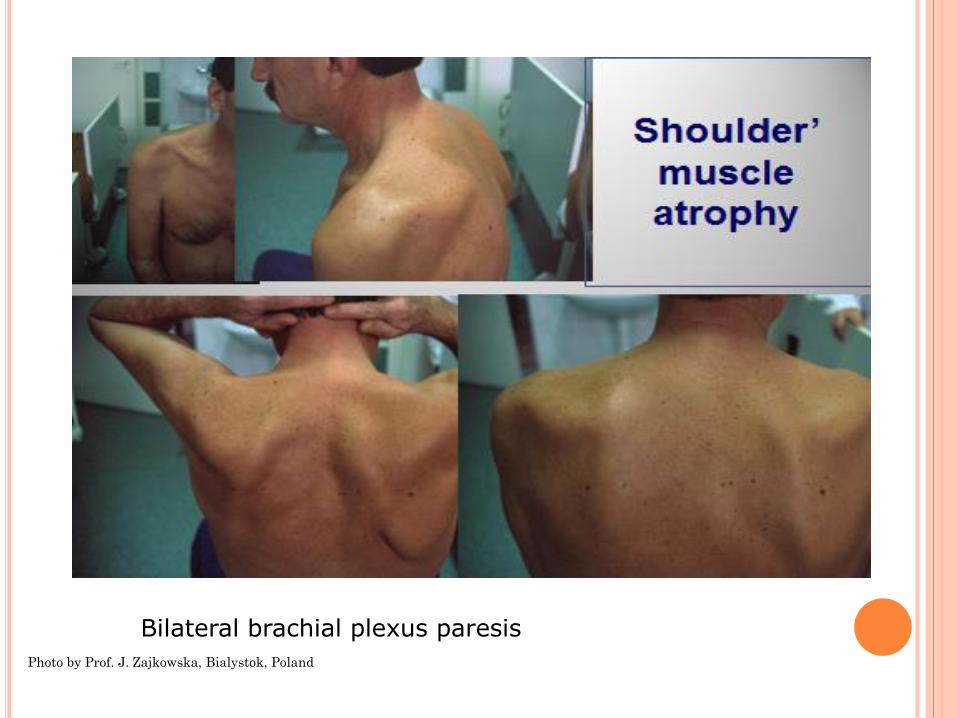
Bilateral brachial plexus paresis
Photo by Prof. J. Zajkowska, Bialystok, Poland
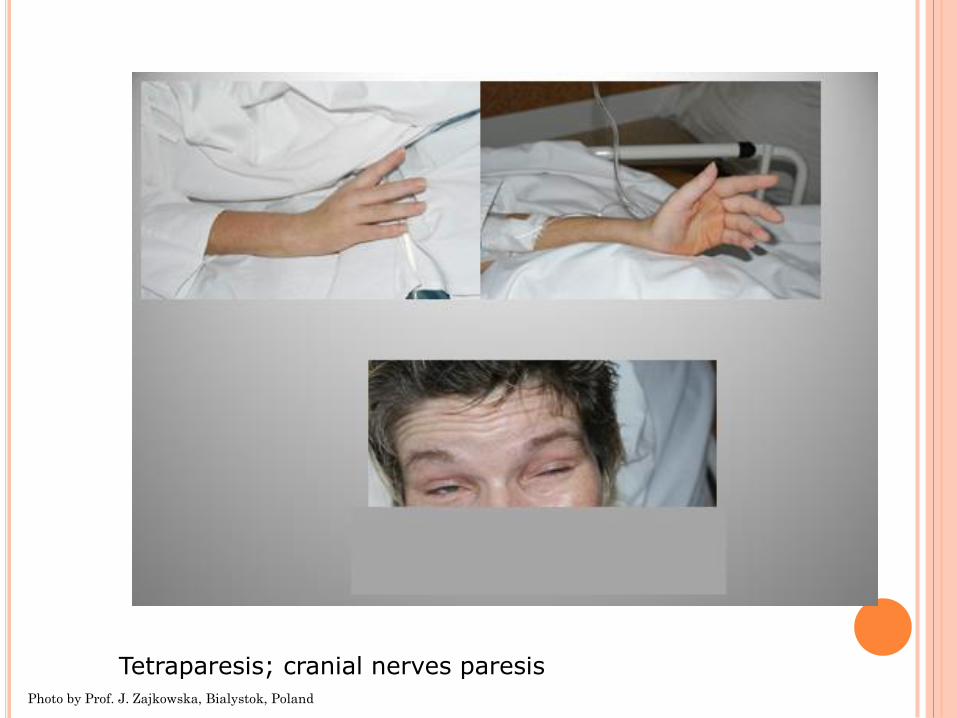
Tetraparesis; cranial nerves paresis Photo by Prof. J. Zajkowska, Bialystok, Poland
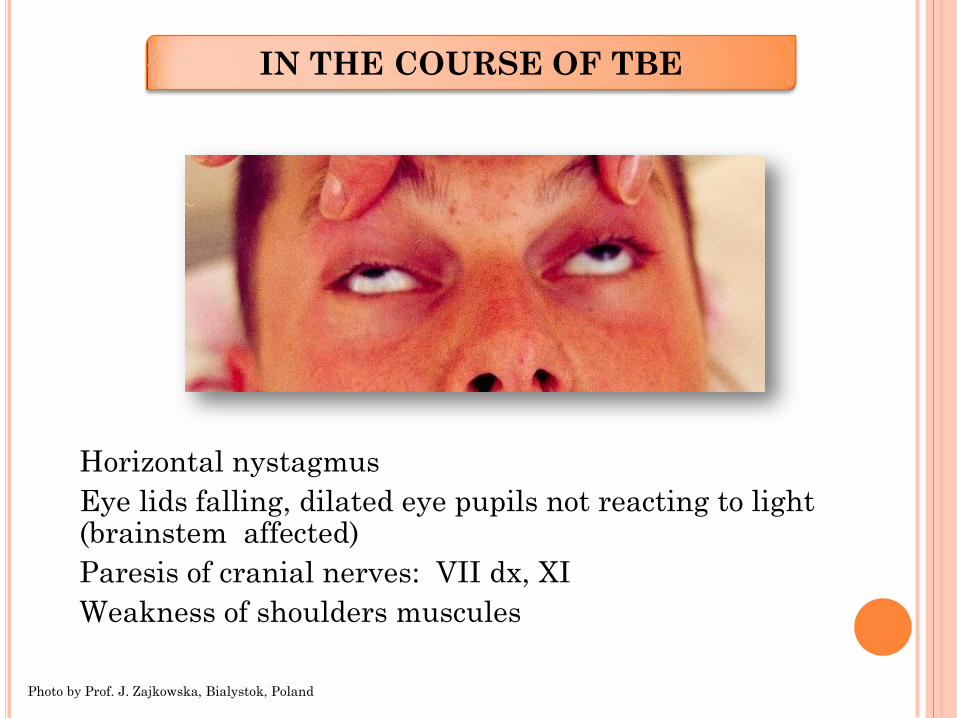
• Horizontal nystagmus
• Eye lids falling, dilated eye pupils not reacting to light (brainstem affected)
• Paresis of cranial nerves: VII dx, XI
• Weakness of shoulders muscules
IN THE COURSE OF TBE
Photo by Prof. J. Zajkowska, Bialystok, Poland
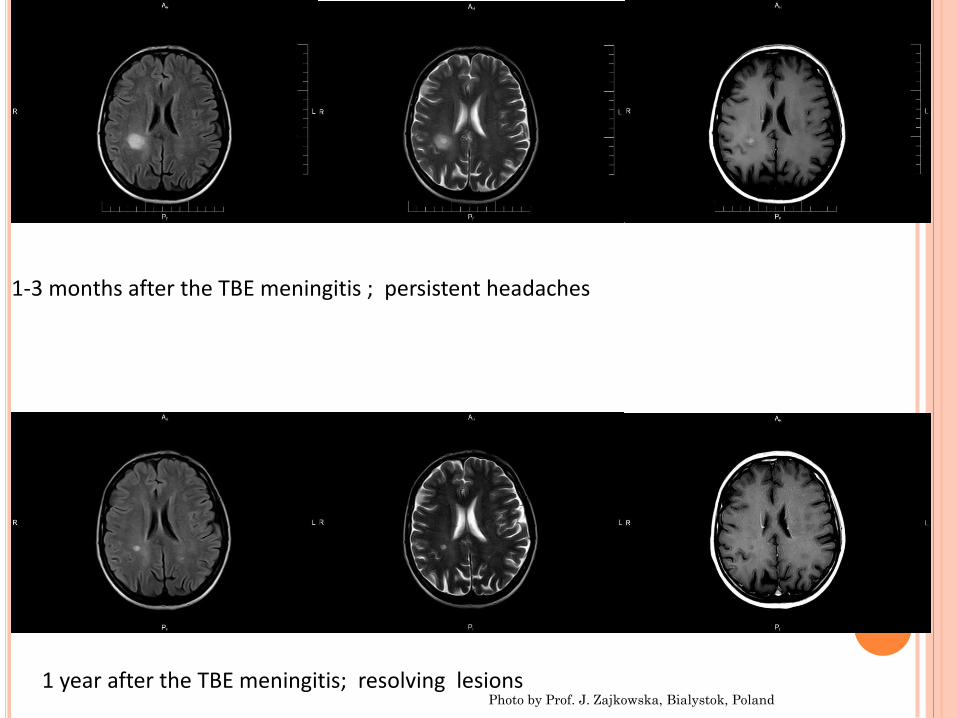
1 year after the TBE meningitis; resolving lesions
1-3 months after the TBE meningitis ; persistent headaches
Photo by Prof. J. Zajkowska, Bialystok, Poland
Daefness
Vision impairment
Vegetative (over 50% of patients): hyperactivity
irritability
mood changes
sweats
Intelectual problems: concentration (64%)
memory disorder (79%)
Psychiatric syndromes: neurasthenia (5.17%)
depression (15.1%)
psychoorganic (17.24%) Pancewicz et al., 2006
TBE – Sequelae
Psychiatric sequelae - 272
patients (43.8%):
cognitive disorders (42.1%) depression (28.9%) sleep disorders (13.2%) anxiety (10.5%)
Czupryna et al., 2011
• Mortality rate: 1-4%
• 68-years old female, coinfection with Listeria
monocytogenes
• 71-years old female for 20 years treated with steroids – RA
• 66- years old kidney transplant recipent
• 64-years old female, two years after renal transplant
• (on immunosupression)
TBE – LETHAL CASES
September 5, 2012 the European Commission published an official decision on the addition of TBE to the list of notifiable diseases in the European Union September 18, 2012 the ECDC published raport about: • Implementation of the standard case definition of TBE infection • Collecting standardized, comparable data at EU level • The need to develop recommendations for immunization of EU
citizens as well as for those traveling to areas endemic of this disease!
• Travel medicine!!!!!
1. Official Journal of the European Union, 5.9.2012, L 239/3, http://eurlex.europe.eu 2. Epidemiological situation of tick-borne encephalitis in the European Union and European Free Trade Association
countries, Technical Report, The European Centre for Disease Prevention and Control (ECDC), http://www.ecdc.europa.eu/en/publications/Publications/TBE-in- -EU-EFTA.pdf
3. World Health Organisation (WHO) Background Document on Vaccines and Vaccination against Tick-borne Encephalitis (TBE), 2011, http://www.who.int/immunization/sage/6_TBE_backgr_18_Mar_net_apr_2011.pdf
Non specific- avoiding tick bites, proper clothes in
nature, use of repelents
Specific- vaccination
TBE – PROPHYLAXIS
persons residing in areas with increased risk of the disease:
foresters
soldiers
firemen
border guards
farmers
trainees in forest areas
tourists, participants of colonies and camps
it is recommended when travelling to countries where the disease is endemic, especially if there is a risk of a tick bite
TBE – Vaccination -
Recommendation
Austria Albania Belarus Bosnia Croatia Czech Republic Denmark Estonia Finland France Greece Hungary Italy Lithuania Latvia Moldova Germany Norway Poland Romania Russia Serbia Slovakia Slovenia Sweden Switzerland Ukraine
Kollaritsch et al., 2010; WHO, 2010
1st Vaccine – 1970 - (Immuno AG Austria)
In Europe
FSME – IMMUN Baxter AG - Pfizer
Encepur - Novartis - GSK
Both vaccines – highly immunogenic
Antibodies, produced after vaccination, have cross-neutralizing response against various strains of the virus of TBE in Europe and Asia (including Siberian and Far Eastern subtype)
TBE – PROPHYLAXIS
Kunz et al., 1976; Heinz et al., 2007; Kunz, 2003
Administrated in 3-steps scheme - 0, 1-3 and 9-12
months; booster every 3- 5 years
If the need for rapid immunization (simlilar response):
1. For Encepur® a rapid immunization schedule is licenced with 3 vaccinations on
days 0-7-21 and a first booster after 12-18 months
2. For FSME-Immun® the rapid immunization (“modified or accelerated conventional
schedule”) consists of vaccinations on day 0 and 14 and an (early) third vaccination
after 5-12 months (for the adult formulation) and a booster after 12-18 months
TBE – Vaccination - Schedule
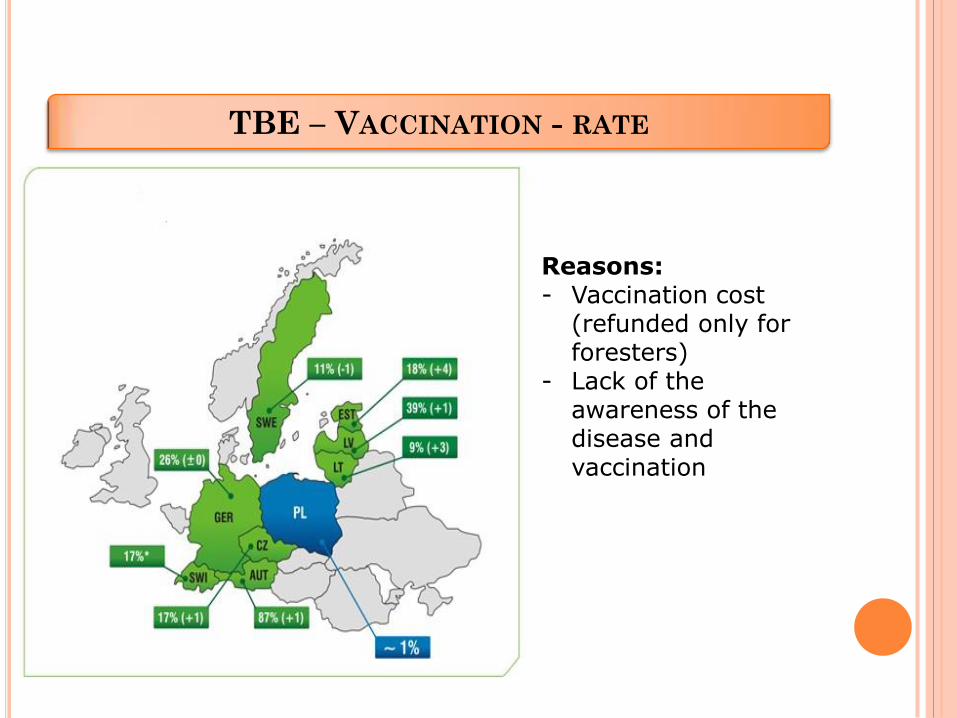
TBE – VACCINATION - RATE
Reasons: - Vaccination cost
(refunded only for foresters)
- Lack of the awareness of the disease and vaccination






























