Embed Size (px)
DESCRIPTION
Luis F. Moreno. Preventive Profile. Patient History. Age: 63 Sex: Female Race: Caucasian Occupation: Accountant Marital status: Married . Medical History. Past medical history: Menopause Past medications or drugs: June 1997: - PowerPoint PPT Presentation
Citation preview
PREVENTIVE PROFILE
Luis F. Moreno
Patient History Age: 63 Sex: Female Race: Caucasian Occupation: Accountant Marital status: Married
Medical History Past medical history: Menopause Past medications or drugs: June 1997: Premarin: treatment of moderato-to-severe vasomotor
symptoms associated with menopause. No dental implications.
Provera: estrogen replacement in postmenopausal women. Provera may predispose the patient to gingival bleeding.
May 2003: Advil: inflammatory diseases and rheumatoid disorders,
mild-to-moderate pain, fever. No dental implications, but Advil may counteract the effect of baby aspirin and hinder its benefits as a preventive cardiovascular medication.
Family History Heart disease Diabetes Cancer
General Health
Excellent
Review of systems Neurological: None Psychological: None Functional: None Respiratory: None Cardiovascular: None Dermatological: None Gastrointestinal: None Sexual: None Hematological: None Endocrine: None Immunological: None
Current medications Aspirin 81 mg, (a.k.a. baby aspirin),
1 tablet/day.
Implications: Aspirin is a blood thinner.
Dental concerns: There may be
excess bleeding during dental procedures, such as scaling and root planings.
Baseline vitals First visit: BP: 124/80 P: 60 R: 14
Second visit: BP: 114/80 P: 52 R: 14
Third visit: BP: 118/80 P: 55 R: 14
ASA status: II
Rationale: Patient takes baby aspirin daily as a preventive measure.
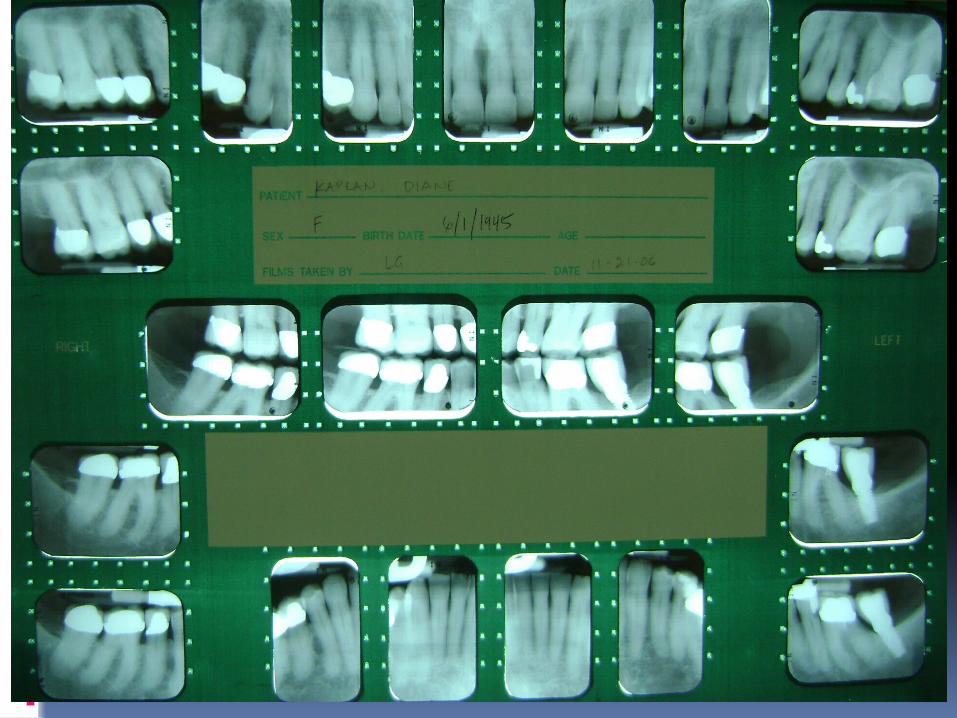
Dental history Last dental exam: 8/2008 Last dental hygiene care: 10/2008 Last FMX: 10/2006 Dental Hygiene intervals every six months. Third molars extracted at age 23. Orthodontic treatment at age 26. Molar # 18 extracted in June 2005. Failed root canal
treatment. Tooth # 18 replaced with an implant in 2007. Patient has been a patient of record at UCLA since
1973. Patient has had most of her dental work done at UCLA.
Present status Patient admits to grinding her teeth
at night.
Patient wears a hard acrylic night guard.
Patient is aware of severe gingival recession in localized areas.
Clinical examination (pre-treatment)
Symmetry: WNL Skin: WNL Lymph nodes: WNL Trachea: WNL Thyroid: WNL TMJ: WNL Tonsils: WNL
Extraoral findings
Clinical examination (pre-treatment) Intra-oral findings Lips: WNL Labial/buccal mucosa:
Bilateral linia alba and bite marks on left side buccal mucosa.
Vestibules: WNL Mucobuccal folds: WNL Frena: WNL Alveolar bone: WNL Hard palate: WNL Soft palate: WNL Tongue: WNL Floor of the mouth: WNL
Salivary glands: WNL Tonsils: WNL Occlusion: Unclassified
clusion. Anterior bite: 2mm
overbite, over jet from 2-6mm.
Maximum opening : 52mm.
Attrition: Normal wear. Erosion: None Abfraction: None

Intraoral findings
Linia alba Bite marks
Gingival description Maxillary attached: pink, firm, stippled
with moderate generalized recession areas of 1-2mm.
Maxillary free: pink, firm, scalloped, smooth.
Mandibular attached: pink, firm, stippled with mild generalized and severe localized recession.
Mandibular free: pink, firm, scalloped, smooth.
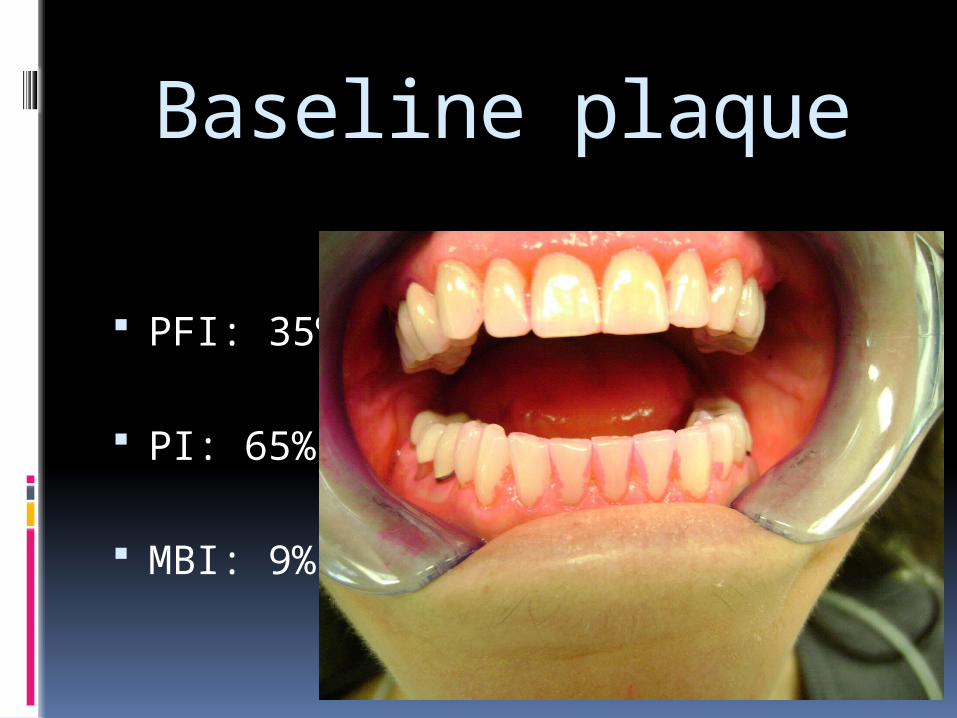
Baseline plaque
PFI: 35%
PI: 65%
MBI: 9%
Baseline periodontal record Pocket depth: Generalized 2-3.
Localized 4 on teeth # 4,14,15,31. BOP: #3 B, #3 DL, #14 Ml, #29 L. Mobility: None Furcations: None Recession: Generalized 1-2 mm with
severe areas up to 5mm on buccal surface of teeth #19 and 30.
Description of calculus
LtM 3
Perpetuating factors Restorations: Patient has several crowns
in her mouth. Most of them fit well; nonetheless, they are a contributing factor to plaque accumulation.
Occlusion: Patient presents with problematic occlusion.
Hormonal activity: Hormonal fluctuation 10-12 years ago may have contributed to systemic gingival inflammation and recession.
Etiology
Plaque
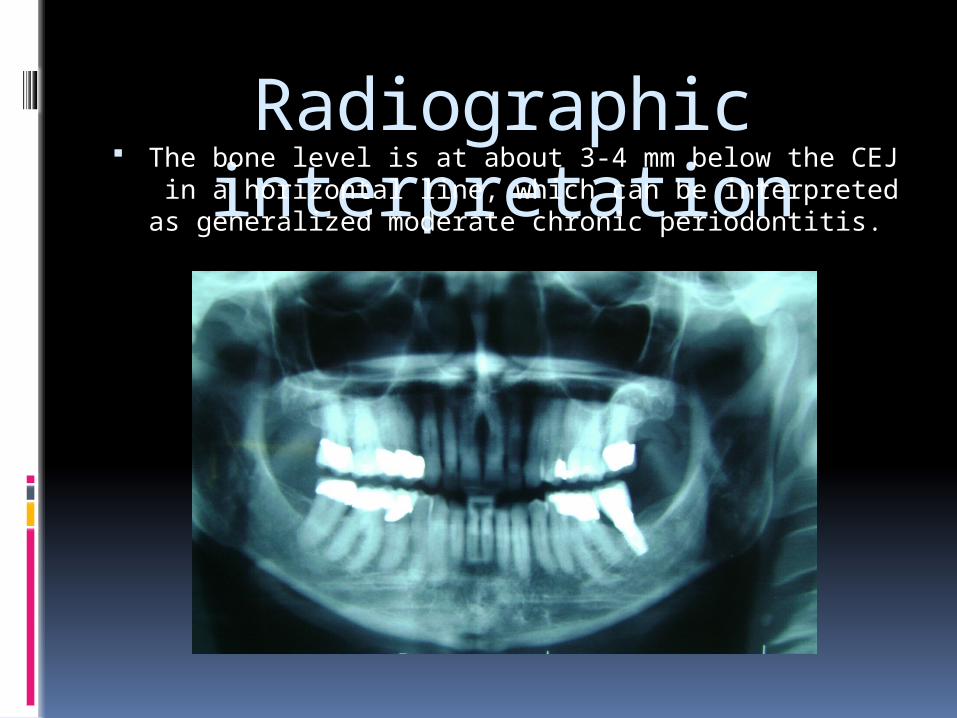
Radiographic interpretation The bone level is at about 3-4 mm below the CEJ in a
horizontal line, which can be interpreted as generalized moderate chronic periodontitis.
Periodontal diagnosis (AAP)
Generalized Moderate Chronic Periodontitis with Localized Severe Chronic Periodontitis
Oral hygiene evaluation
(pre-treatment) Patient’s Skill Level: Fair Patient’s Knowledge and awareness of dental
and periodontal disease: Fair Objectives developed during OHI: Better
plaque control. Oral Hygiene Instruction:
a) Flossing.b) Modified Bass and Roll brushing technique.c) Interproximal Brushing.
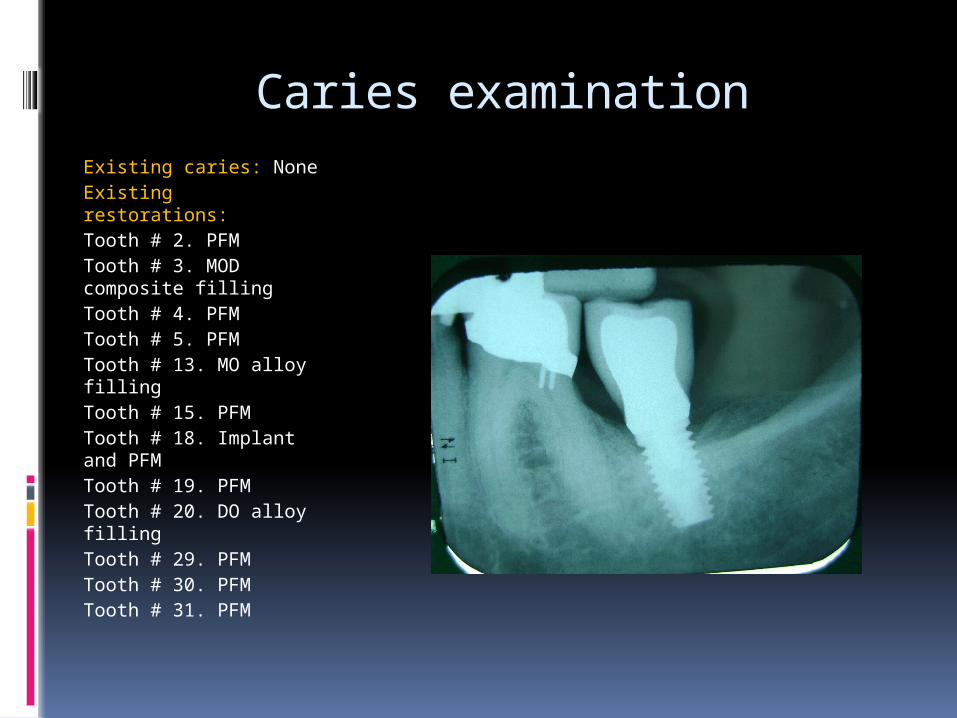
Caries examinationExisting caries: NoneExisting restorations:Tooth # 2. PFMTooth # 3. MOD composite fillingTooth # 4. PFM Tooth # 5. PFMTooth # 13. MO alloy fillingTooth # 15. PFMTooth # 18. Implant and PFMTooth # 19. PFMTooth # 20. DO alloy fillingTooth # 29. PFMTooth # 30. PFMTooth # 31. PFM
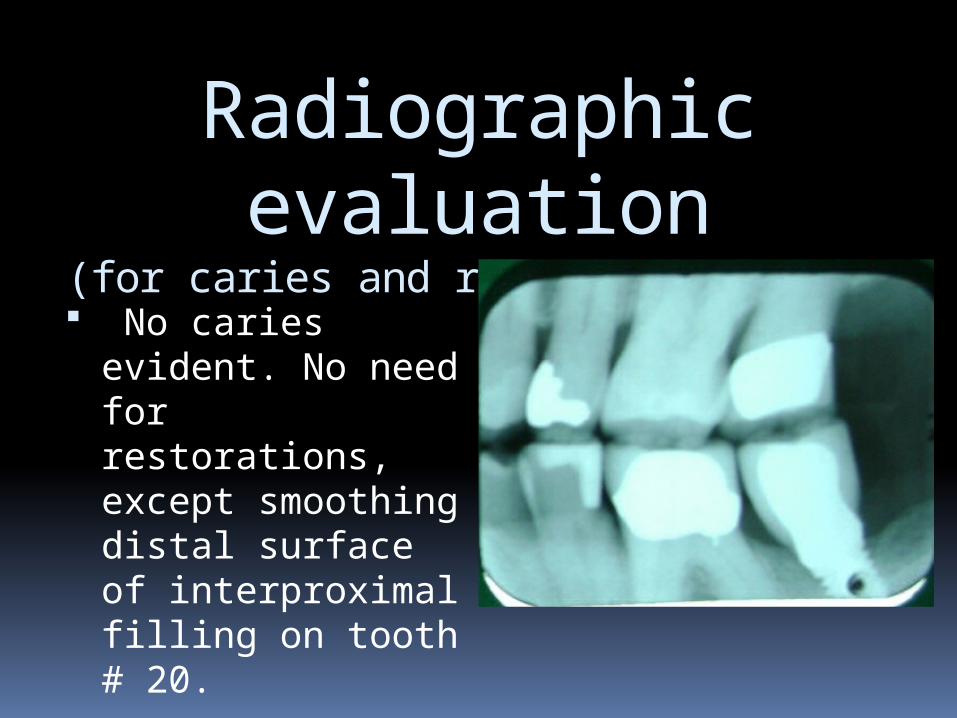
Radiographic evaluation
(for caries and restoration needs) No caries evident.
No need for restorations, except smoothing distal surface of interproximal filling on tooth # 20.
Nutritional analysis
Patient filled out a 3-day food diary I prepared a dietary analysis @ My
Pyramid.gov A carbohydrate intake analysis was
made based on the 3-day food diary A nutritional counseling was done on
the last appointment stressing the importance of proteins and milk products for a healthy diet
Fluoride analysis Current usage of fluoride: Patient uses Crest Pro Health daily, which
contains 0.454% Stanous Fluoride Patient cooks with tap water Patient drinks tap water Patient lives in the Beverly Hills area
where the water has a fluoride concentration of 0.8 ppm.
I recommended fluoride varnish, but patient was not interested.
Dental Hygiene treatment plan Appointment 1: RMH, Vitals, EO & IO,
Probing, PFI, BI, OHI, Gather data. Appointment 2: RMH, Vitals, EO & IO, Spot
probing, Full Mouth Scaling, Selective Polishing.
Appointment 3: RMH, Vitals, EO & IO, Probing, PFI, BI, OHI, Gather data, Re-asses oral health and discuss nutritional analysis in order to make recommendations
Re-care: Every 6 months.
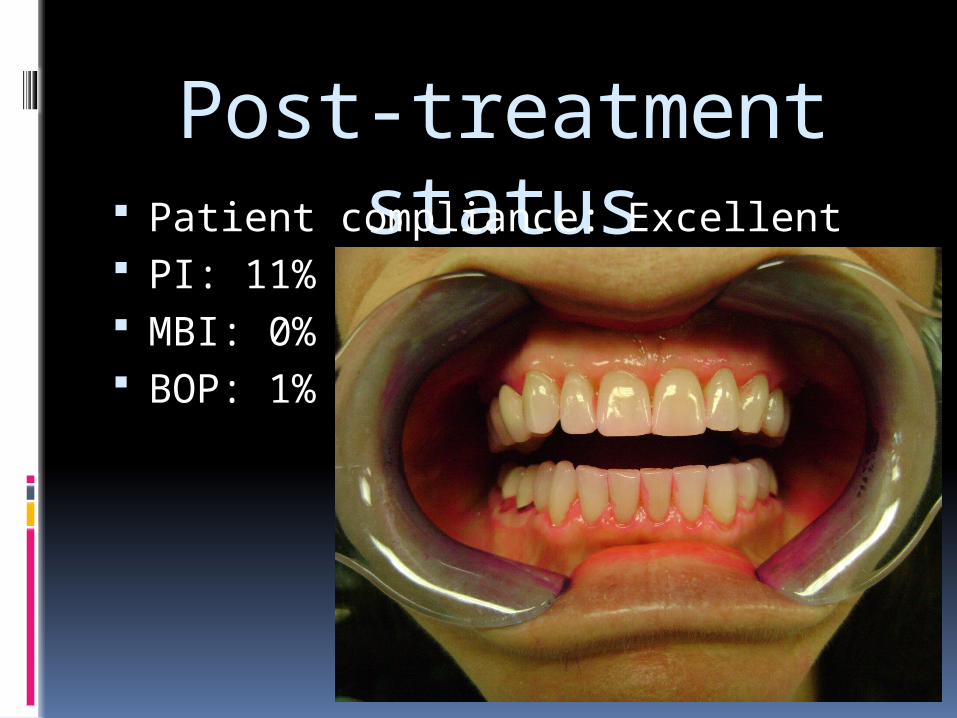
Post-treatment status Patient compliance: Excellent
PI: 11% MBI: 0% BOP: 1%
References Banihashemrad S, Fatemi K, Najafi M (2008). Effects of Smocking
on Gingival Recession. Dental Research Journal. Retrieved May 10, 2009 from: http://journals.mui.ac.ir/drj/article/viewFile/2882/1107
Remya V, Kishore K, Sabitha S, Arun DV (2008). Free gingival graft
in the treatment of class IIIgingival recession. Indian Journal of Dental Research. Retrieved May 10, 2009 from http://www.ijdr.in/temp/IndianJDentRes193247-5866461_161744.pdf
Moawia M, Kassab and Robert E, Cohen (2008). The etiology and
prevalence of gingival recession. The Journal of the American Dental Association. Retrieved may 10, 2009 from http://jada.ada.org/cgi/reprint/134/2/220.pdf