Embed Size (px)
Citation preview

PREVENTION of SSIs
AUDIT TOOL INTRODUCTION April 30, 2015
Dr. Claude Laflamme Physician Lead for the Safer Healthcare Now! Surgical Site Infection Intervention Director of Cardiac Anesthesia, Sunnybrook Health Science Centre, Toronto, ON Assistant Professor, University of Toronto
Virginia Flintoft MSc BN Safer Healthcare Now! Manager, Central Measurement Team

French slides available during presentation
Links to:
a) English presentation slides and
b) English and French GSKs posted in chat box
Interested in using new data collection form?
Advance notice: SSI National Audit Fall 2015
Post questions in the chat box;
to “All Participants”
Using a MAC computer?
Before we get started

Welcome to our francophone attendees
Bienvenue à nos participants francophones Hélène Riverin Conseillère en sécurité et en amélioration Safety Improvement Advisor

Our Guest Speakers

Dr. Claude Laflamme
“Why should we care?”
Introduction to the SSI Audit Tool

Surgical Site Infection (SSI)
2-5% occurrence in inpatient surgery
60% preventable if evidence based guidelines
followed
Associated with 11 days increase LOS
SSI account for $3.5-$10 billion in United States
Double the mortality, 60% more time in ICU, and 5x
more likely to be re-admitted

SSI and Additional Hospital LOS

CPSI SSI Measurement 2006-2014
Figure 1: Incidence of Surgical Site Infections in patients undergoing clean and
clean contaminated surgery in Canada from 2006 to 2014


The SSI Audit Tool

The SSI Audit Tool
Each form will be for
one (1) patient

The SSI Audit Tool
Each question (A to L)
is one element of the
audit tool and rolls up
to an indicator

A. Type of Surgery
Type of surgery the patient underwent
Note Cardiac Surgery on and off pump
Pick only one

B. Surgical Class
NHSN definition of wound classifications
Clean - uninfected operative wound - no inflammation
Clean Contaminated - operative wound in which the respiratory,
alimentary, genital, or urinary tracts are entered under controlled
conditions and without unusual contamination
Contaminated - open, fresh, accidental wounds + operations
with major breaks in sterile technique or gross spillage from the
GI tract, and non–purulent inflammation
Dirty - Old traumatic wounds with retained devitalized
tissue + existing infection or perforated viscera..

C. Pre-Op Shower or bath with soap
or antiseptic agent
Soap: bar/bath soap
Antiseptic Agent: e.g. Chlorhexidine
Shower or Bath not required:
shower or bath is not required for the type of surgery
e.g. ophthalmologic or oral
No shower or bath –
a shower or bath was required but the patient did not have either
Not Recorded –
no evidence of having a shower or bath recorded in
the patient chart

D. Solution used for intra-op intact skin
cleansing…
2% Chlorhexidine in 70% alcohol –
has been demonstrated to be more effective as a surgical skin preparation
solution than other agents.
Chlorhexidine
Povidone-iodine with alcohol
Povidone-iodine –
remains the standard for head and neck procedures

D. Solution used for intra-op intact skin
cleansing…
Other – other solution used
Contraindicated –
i.e. skin sensitivity, allergy, rash, or contact with the eye, inner ear, mucosa
or meninges.
Not Applicable - i.e. ophthalmologic or oral
Not Recorded –
no evidence of having a shower or bath recorded in the patient chart

E. Prophylactic antibiotic administration
Within 60 minutes before incision
administration of antibiotic was completed within 0 to 60 minutes prior to
the first surgical incision time.
Within 120 minutes before incision for Vancomycin or
Fluoroquinolones
administered over 120 minutes and completed within 0 to 60 minutes
prior to the first surgical incision.
None of the above
gave antibiotics but did not meet the timing requirements above.
No antibiotics given

F. Dose of Cefazolin used as
prophylactic antibiotic
1 g (gram)
2g (grams)
3g (grams)
Other antibiotic used – any abx other than Cefazolin was
administered as the prophylactic antibiotic.
Not recorded – the type of prophylactic antibiotic given
was not recorded in the patient chart.

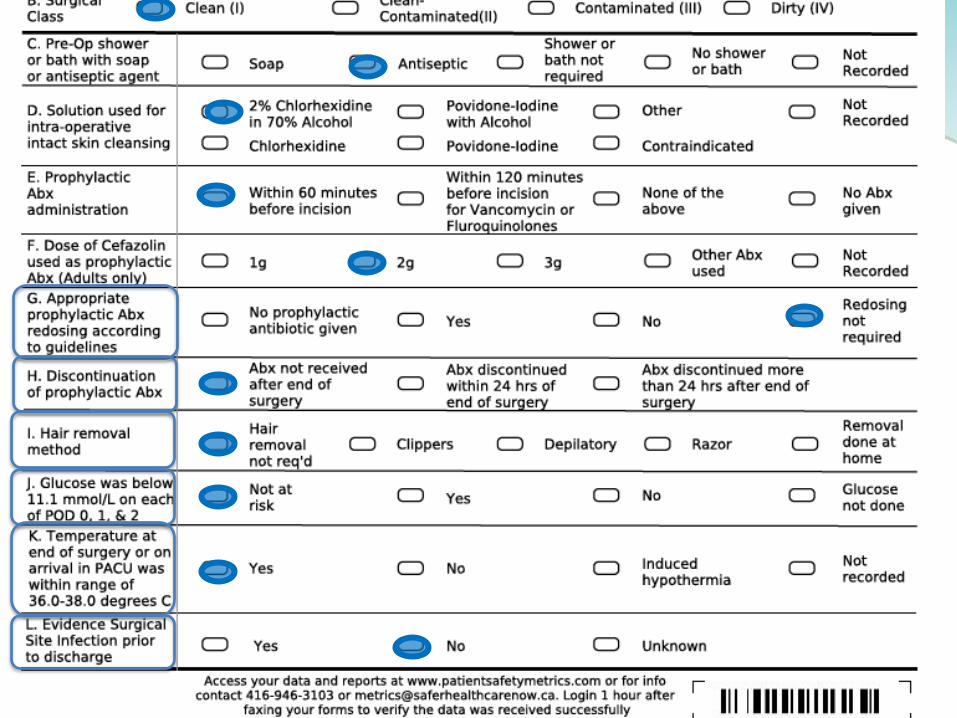
G. Appropriate prophylactic antibiotic
redosing according to guidelines
No prophylactic antibiotic given –
not administered prior to the 1st incision therefore even if an antibiotic
was delivered during the surgery it would not be considered ‘redosing’.
Yes –
given prior to the 1st incision + at least 1 other dose of the antibiotic
was given during the surgery - see recommended guidelines SSI GSK
No –
given prior to the 1st incision + length of surgery exceeds the
recommended intraoperative prophylactic antibiotic redosing interval but
no repeats dose of the antibiotic was given during the surgery.
Redosing was not required –
length of the surgery being less than redosing interval

H. Discontinuation of prophylactic abx
Antibiotic not received after end of surgery –
no prophylactic antibiotics were administered at any time following the
surgery.
Antibiotic discontinued within 24 hours of end of surgery -
prophylactic antibiotics were administered up to 24 hours following the
end of surgery.
Antibiotic discontinued more than 24 hours after end of
surgery
prophylactic antibiotics were administered more than 24 hours following
the end of surgery.

I. Hair removal method?
SSI Faculty recommends no hair removal prior to
surgery.
If hair removal is necessary, clippers (not razors) should
be used.
Ideally, hair removal should occur outside of the OR
theatre or procedure room, but inside of the operating
room department, within two hours of surgery.
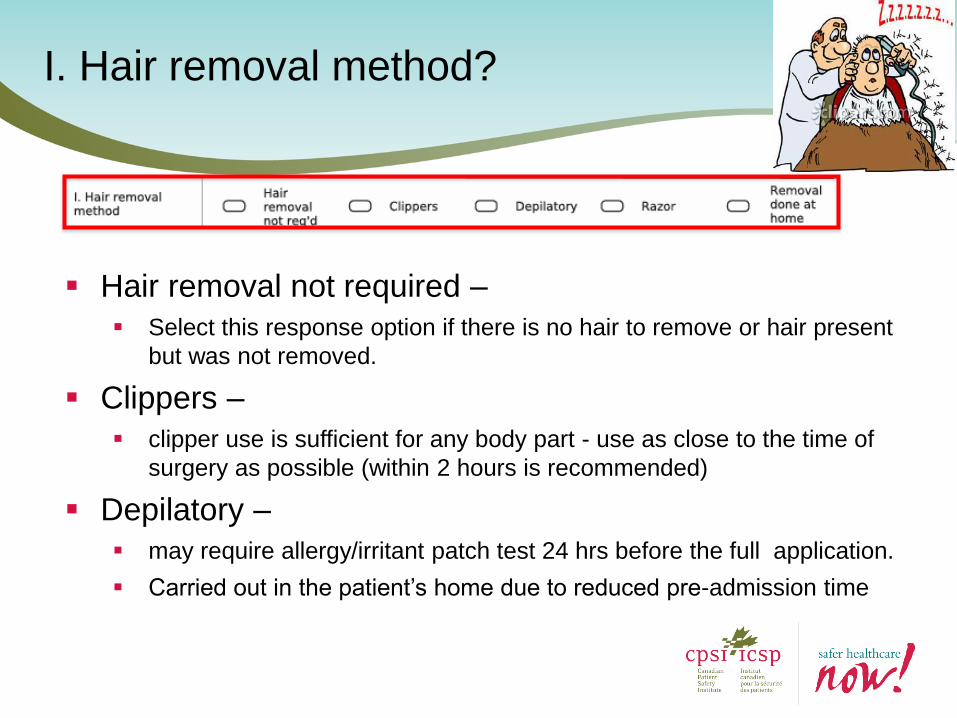
I. Hair removal method?
Hair removal not required –
Select this response option if there is no hair to remove or hair present
but was not removed.
Clippers –
clipper use is sufficient for any body part - use as close to the time of
surgery as possible (within 2 hours is recommended)
Depilatory –
may require allergy/irritant patch test 24 hrs before the full application.
Carried out in the patient’s home due to reduced pre-admission time

I. Hair removal method?
Razor –
razor use is not appropriate for any operative site
Removal done at home –
hair removal is not recommended.
patients should be educated not to shave the surgical site before
surgery.
Incorporate this message into the printed preoperative patient
information and surgeon’s office communication
X

J. Glucose was below 11.1 mmol/L
on each of POD 0, 1, & 2
Risk is defined as:
Diabetic
Pre-op HBA1C > 7%
Pre-op BG > 10mmol/L during their pre-op visit
Not at risk –
select this response option if the patient does not
meet any criterion for risk
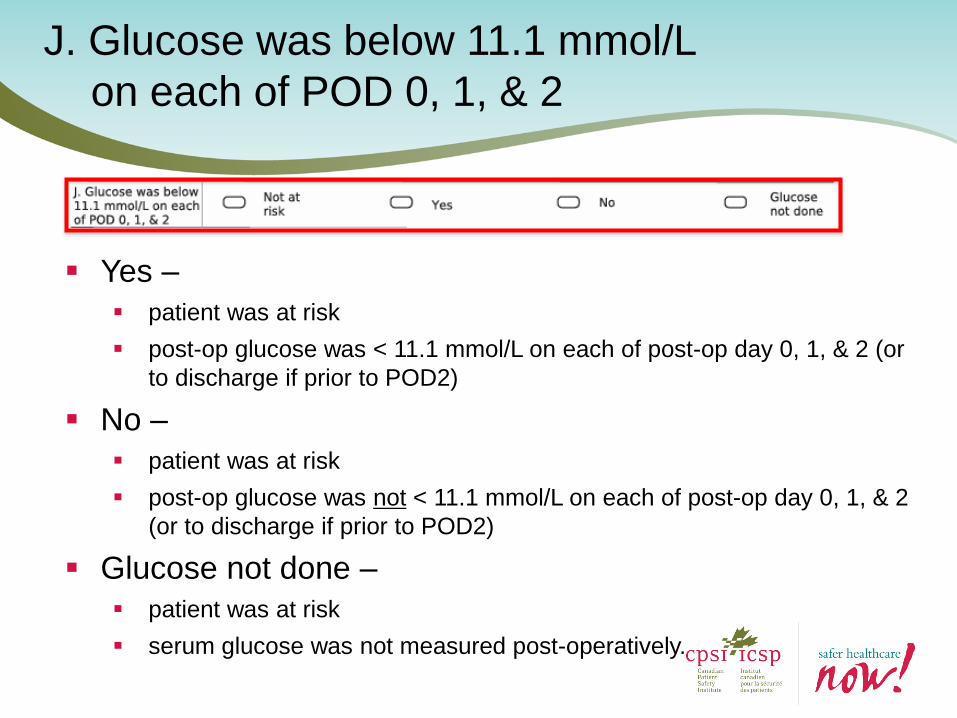
J. Glucose was below 11.1 mmol/L
on each of POD 0, 1, & 2
Yes –
patient was at risk
post-op glucose was < 11.1 mmol/L on each of post-op day 0, 1, & 2 (or
to discharge if prior to POD2)
No –
patient was at risk
post-op glucose was not < 11.1 mmol/L on each of post-op day 0, 1, & 2
(or to discharge if prior to POD2)
Glucose not done –
patient was at risk
serum glucose was not measured post-operatively.

Safer Healthcare Now! SSI Faculty recommend that
measures are taken to ensure that surgical patient’s core
temperatures remain between 36.0oC and 38.0oC pre-
operatively, intra-operatively, and in PACU.
K. Temp at end of surgery or on arrival in
PACU was w/i range of 36.0-38.0 oC

K. Temp at end of surgery or on arrival in
PACU was w/i range of 36.0-38.0 oC
Yes –
temp at the end of surgery or on arrival in PACU was within range of
36.0oC and 38.0oC
No –
temp at the end of surgery or on arrival in PACU was not within range of
36.0oC and 38.0oC i.e. higher or lower
Induced Hypothermia –
used as an organ protective strategy
Not Recorded –
temperature at the end of surgery or on arrival in PACU
was not recorded in the patient chart

L. Evidence of Surgical Site Infection
prior to discharge
Yes –
if there is documentation in the patient chart indicating evidence of a
surgical site infection prior to discharge
No –
if documentation in the patient chart indicates the incision is clean and
there is no evidence of a surgical site infection prior to discharge
Unknown –
there is no documentation in the patient chart regarding the state of the
surgical site incision prior to discharge
PREVENTION OF SSI
DATA COLLECTION FORM
Virginia Flintoft, MSc, BN and Alexandru Titeu, BA (Hons)
April 30, 2015

Brief introduction to PS Metrics
SSI Data Collection Methods and tools
Objectives

Features:
Free, cloud-based data collection and reporting tool
Available in English and French
User friendly and simple to navigate
Accessible from website with login details
Tracks >100 process and outcome measures over 14 interventions
Provides real time reporting and export of data to CSV/Excel
Reduces burden of data collection, entry and analysis
Roll Up or Drill Down Reports (i.e. Unit Organization Health Region Province National) with automated Run Charts
Capacity to customize measures and reports
Provides real time reporting and export of data to CSV/Excel
Patient Safety Metrics - Introduction

Data Collection (Audit) Forms - DCF
– Optical Mark Recognition – bubble form – e.g. ‘Lotto 6/49’
– Patient-level data (de-identified) – daily, weekly etc.
– Multiple data elements – e.g. 12 elements in Falls
– Automatic roll-up to Falls indicator Measurement Worksheets
– Data exportable to Excel
Measurement Worksheets (Falls Indicators)
– Aggregate data - monthly
– Numerator and Denominator
– Result automatically calculated
– Run chart created automatically
– Data exportable to Excel
Worksheets vs Data Collection Forms

SSI Audit Tool
Retrospective review of selected charts
Focus on processes
Measures for continuous improvement

Use of the Tool
Ideally an auditor(s) should:
o be someone familiar with the SSI
prevention process(es), forms used and
overall chart layout
o not audit their own work
o have some training or guidance provided (to
ensure consistency in application of org-
specific criteria)

SHN SSI Measures
Revised Measure From Audit tool

SHN SSI Measures
Revised Measure From Audit tool
New Measures

NEW SSI Scores
Revised Measure From Audit tool
New Measures


40
40
Computer generated
barcode identifies
your audit area/unit

Need this entered on every page So we may contact you if there is an error
10’s
units
Date is required on every form

43
43
SSI Infection
PRE-OP Score
SSI P
RE-
OP
ERA
TIV
E SC
OR
E (1
4)

44
44
SSI Infection
PERI-OP Score
SSI P
ERI-
OP
ERA
TIV
E SC
OR
E (1
5)

45
45
SSI Infection
POST-OP Score
SSI P
OST
-OP
SC
OR
E (1
6)

46
46
SSI Infection
Score
SSI I
NFE
CTI
ON
SC
OR
E (1
7)

DO … Colour inside the line - fill in bubble completely (Sharpie is best)
Avoid stacking forms when filling in bubbles to avoid bleed through
Use the void bubble for entry errors – avoid scratch out
Print new form each time - avoid photocopying
Avoid using 3-hole punch on forms
Keep form free from extra markings
Fax without a cover sheet
Fax form in FINE RESOLUTION - check setting on fax machine
Data Collection (Audit) tool- BE AWARE!
47

SSI Audit Form Instructions (2 pages)

Accessing Instructions from PSM

Start data collection
– Contact Virginia or Alex at the Central Measurement Team for help creating your forms (same day delivery!) [email protected]
Submit data monthly until you reach goal
Stay tuned for more information on the National SSI Audit Fall 2015 - Plan to participate
Next Steps
50

Questions?
51

Thank You / Merci

53
CPSI Central Measurement Team
Virginia Flintoft - 416-946-8350
Alexandru Titeu - 416-946-3103
CPSI Patient Safety Intervention Lead
Carla Williams
We are here to help!





























