Embed Size (px)
Citation preview

Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
Prof. Sverre E. Kjeldsen, MD, PhD
Department of Cardiology, Oslo University Hospital, Ullevaal, Oslo, Norway
The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion or Treatment of Patients With Established Heart Disease

Prevalence of HT in AF Trials
Manolis AJ et al. ESH Position Paper. J Hypertens 2011; 30: 239-252.

0 5 10 15 20 25 30 35
Observation time (Years)
Q1 (88-116)
Q2 (118-126)
Q3 (128-138)
Q4 (140-220)
60%
70%
80%
90%
100%
Free
from
atria
l fibr
illatio
n
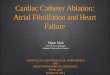
Kaplan-Meier Curves Showing Participants Free From AF Related to Quartiles of Systolic BP (N=2014)
Grundvold I, Kjeldsen SE et al. J Hypertension 2012; 59: 198-204
High normal SBP predicts incident atrial fibrillation
N=272 detected with new onset atrial fibrillation.

4
Diuretic and beta-blocker treatment mainly
Prevention of Heart Failure and LVH in Hypertension Strongly Suggests Similar Prevention of Atrial Fibrillation

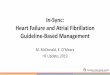
Possible Preventive Mechanisms of ARBs in Atrial Fibrillation
Aksnes TA, Flaa A, Strand A, Kjeldsen SE. J Hypertens 2007;25:15-23


Study Treatment Control OR (random) Weight OR (random) or sub-category n/N n/N 95% CI % 95% CI
Hypertension studies Hansson (CAPPP) 117/5456 135/5459 6.39 0.86 [0.67, 1.11] Hansson (STOP-2) 200/2088 357/4215 6.97 1.14 [0.95, 1.37] Wachtell (LIFE) 150/4298 221/4182 6.73 0.65 [0.52, 0.80] Salehian (HOPE) 86/4291 91/4044 5.95 0.89 [0.66, 1.20] Schmieder (VALUE) 252/6872 299/6888 7.06 0.84 [0.71, 1.00] Yusuf (TRANSCEND) 182/2844 180/2857 6.72 1.02 [0.82, 1.26] Subtotal (95% CI) 25849 27645 39.82 0.89 [0.75, 1.05] Total events: 987 (Treatment), 1283 (Control) Test for heterogeneity: Chi² = 17.98, df = 5 (P = 0.003), I² = 72.2% Test for overall effect: Z = 1.39 (P = 0.17)
Post-MI studies Pedersen (TRACE) 22/790 42/787 3.99 0.51 [0.30, 0.86] Pizzetti (GISSI-3) 665/8865 721/8846 7.45 0.91 [0.82, 1.02] Subtotal (95% CI) 9655 9633 11.45 0.72 [0.41, 1.27] Total events: 687 (Treatment), 763 (Control) Test for heterogeneity: Chi² = 4.59, df = 1 (P = 0.03), I² = 78.2% Test for overall effect: Z = 1.13 (P = 0.26)
Heart Failure studies Vermes (SOLVD) 10/186 45/188 2.80 0.18 [0.09, 0.37] Ducharme (CHARM) 177/3191 215/3188 6.78 0.81 [0.66, 1.00] Maggioni (Val-HeFT) 113/2205 174/2190 6.44 0.63 [0.49, 0.80] Subtotal (95% CI) 5582 5566 16.03 0.52 [0.31, 0.87] Total events: 300 (Treatment), 434 (Control) Test for heterogeneity: Chi² = 16.40, df = 2 (P = 0.0003), I² = 87.8% Test for overall effect: Z = 2.48 (P = 0.01)
Post-cardioversion studies Van den Berg 2/7 7/11 0.51 0.23 [0.03, 1.77] Madrid 9/79 22/75 2.22 0.31 [0.13, 0.73] Ueng 18/70 32/75 2.88 0.47 [0.23, 0.94] Madrid 2 8/30 14/30 1.55 0.42 [0.14, 1.23] Grecu 10/16 16/20 0.90 0.42 [0.09, 1.85] Tveit 48/68 45/69 2.80 1.28 [0.62, 2.63] Belluzzi 3/31 10/31 1.00 0.23 [0.06, 0.92] GISSI-AF 371/722 375/720 6.77 0.97 [0.79, 1.20] Subtotal (95% CI) 1023 1031 18.64 0.55 [0.34, 0.89] Total events: 469 (Treatment), 521 (Control) Test for heterogeneity: Chi² = 18.59, df = 7 (P = 0.010), I² = 62.3% Test for overall effect: Z = 2.44 (P = 0.01)
Medical Therapy studies Yin 25/118 24/59 3.00 0.39 [0.20, 0.78] Fogari 1 13/111 39/111 2.92 0.24 [0.12, 0.49] Fogari 2 42/246 46/123 4.23 0.34 [0.21, 0.56] Fogari 3 28/148 48/148 3.91 0.49 [0.28, 0.83] Subtotal (95% CI) 623 441 14.06 0.37 [0.27, 0.49] Total events: 108 (Treatment), 157 (Control) Test for heterogeneity: Chi² = 2.45, df = 3 (P = 0.49), I² = 0% Test for overall effect: Z = 6.73 (P < 0.00001)
Total (95% CI) 42732 44316 100.00 0.67 [0.57, 0.78] Total events: 2551 (Treatment), 3158 (Control) Test for heterogeneity: Chi² = 100.83, df = 22 (P < 0.00001), I² = 78.2% Test for overall effect: Z = 5.24 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10 Favours treatment Favours control
CAPPP – adverse event reports STOP-2 adverse event reports LIFE – secondary endpoint and annual ECGs – first HT study HOPE – not a hypertension study VALUE – secondary endpoint and annual ECGs – second HT study TRANSCEND – not a hypertension study
Prevention of Atrial Fibrillation by RAAS-Inhibtion (JACC 2010)

Primary Prevention of Atrial Fibrillation in the Treatment of Hypertension
• Need hypertensive population with high risk of incidental atrial fibrillation
• Need pre-specified protocol • Need AF detection from systematic taking of
ECGs and central ECG readings • Need double-blinded head-to-head randomized
comparison • Two trials fullfil these criteria – LIFE and VALUE

LIFE Baseline Characteristics-1n=9193
Age, years 66.9 (7.0)Female, n 4963 (54%)Body mass index, kg/m2 28.0 (4.8)Blood pressure, mmHg 174.4/97.8 (14.3/8.9)Heart rate, bpm 73.8 (11.1)Cornell product, mm·msec 2828.8 (1049.5)Sokolow-Lyon, mm 30.0 (10.5)Framingham risk score 0.224 (0.096)Smokers, n 1499 (16%)
Values are mean (SD) or n (%) when indicated.


10 %
22 %68 %
LIFE: Patient Recruitment ECG-Criterion (n=9192)
Both Cornell Product
Sokolow-Lyon
Dahlöf B, Kjeldsen SE et al. Hypertension 1998;32:989-997.


13
0 6 12 18 24 30 36 42 48 54 60 660
1
2
3
4
5
6
7
8LosartanAtenolol
Time (months)
Prop
ortio
n of
pat
ient
sw
ith fi
rst e
vent
(%)
RR: 0.70 [95% CI: 0.58-0.85], p<0.001.
LIFE Atrial Fibrillation: Losartan vs. Atenolol Reduces New Onset AF/Flutter
Wachtell, Kjeldsen SE et al.: J Am Coll Cardiol 2005;45:712-719.

14
LIFE Atrial Fibrillation: Stroke in Patients with and without AF
Strokes in Losartan-Treated
Patients
Strokes in Atenolol-Treated
Patients
Hazard Ratio (95%
CI)
Patients with Pre-existing AF (n=342)
18 38 0.55 (0.31-0.97)
p=0.039
Patients with New-onset AF (n=371)
19 (n=150 with new AF)
38 (n=221 with new AF)
0.49 (0.29-0.86)
p=0.01
Patients with No AF (n=8480)
195 233 0.81 (0.67-0.99)
p=0.04
Wachtell K, Kjeldsen SE et al.: J Am Coll Cardiol 2005;45:705-711 and 712-719.

Circ Arrhythm Electrophysiol 2013;6:243-251.

16
Regression of Cornell Product LVHwith Losartan vs Atenolol Treatment
-400
-300
-200
-100
0
LosartanAtenolol
p<0.001
p<0.001
p<0.001 p<0.001
-67
6 Months 1-Year 2-Year 3-Year 4-Year 5-Year Last
p<0.001p<0.001
p<0.001
-202
-256
-109
-319
-169
-314
-171
-306
-162
-327
-182
-290
-124
∆ C
orne
ll Pr
oduc
t (m
m•m
sec)
Dahlöf B, Devereux RB, Kjeldsen SE et al. Lancet 2002.

23* n= number of patients in each group at baseline, 2 and 4 years of LIFE
New Onset of AF According to the Presence or Absence ofECG LVH by Time-Varying Cornell Voltage-Duration Product
0 10 20 30 40 50 60Follow-Up (Months)
0.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
New
-Ons
et A
F R
ate
<= 2440 (n=2931, 3950, 3832)>2440 (n=5604, 4156, 3641)
Adapted from Okin et al.: JAMA 2006;296:1242-1248.

18
Incidence of Atrial Fibrillation in Relation to Changing Heart Rate Over Time in Hypertensive Patients. The LIFE Study.
Okin PM, Wachtell K, Kjeldsen SE et al. Circ Arrhythmia Electrophysiol 2008; 1: 337-343

HF: Framingham Criteria
Major Criteria Clinical Findings Diagnostic Findings
Minor Criteria* Clinical Findings Diagnostic Findings
Minimum requirement
• 2 major findings, or • 1 major finding plus 2 minor findings In both cases at least
• 1 clinical finding, and • 1 diagnostic finding
* Minor findings are accepted only if they cannot be attributed to another disease process

LIFE: Criteria for Heart Failure MAJOR CRITERIA CLINICAL Paroxysmal nocturnal dyspnea or orthopnea Jugular venous distention Pulmonary rales Ventricular S3 gallop Hepatojugular reflux Diuresis 10 lbs/5kg in response to diuretic;
clinical improvement in congestive symptoms
DIAGNOSTIC Acute pulmonary edema on chest x-ray PCWP ≥ 20 mmHg LVEF ≤ 35 CI < 2,0 Evidence of severe valvular heart disease Pulmonary edema or visceral congestion on
autopsy
MINOR CRITERIA* FINDINGS Night cough Dyspnea on ordinary exertion Bilateral ankle edema Hepatomegaly
FINDINGS Pleural effusion or pulmonary vascular engorgement or redistribution on x-ray PCWP 16-19 mmHg LVEF 36-44 CI 2,0 – 2,4 Evidence of moderate valvular heart
disease
* Minor criteria will be accepted only if they can not be attributed to another disease process

147:311-319.

147:311-319.
*

Electrocardiographic Strain Pattern and Prediction of New-Onset Congestive Heart Failure in Hypertensive
Patients: The LIFE Study
Okin P, Kjeldsen SE et al. Circ 2006; 113: 67-73.

Okin P, Kjeldsen SE et al. Circ 2009; 119: 1883-1891

Pulse Pressure and Incident Atrial Fibrillation in LIFE
Larstorp AC, Kjeldsen SE et al. Hypertension 2012; 60: 347-353.

Hypertension 2015; 66: 368-373.

27
Summary – New Atrial Fibrillation in LIFE
1) LIFE included n=9193 patients with ECG-LVH 2) In LIFE, losartan reduced new AF with 30% compared to
atenolol 3) In LIFE, regression of ECG-LVH was strongly related to
less new AF. Lower heart rate was also related to less new AF suggesting HR lowering therapy (ivabradin study)
4) In LIFE, prevention of new AF was related to less stroke 5) In LIFE, new AF predicted sudden cardiac death and
incident heart failure 6) In LIFE, baseline BP predicts new AF despite treatment
and lower achieved BP (in-treatment BP) gives less AF

Kjeldsen SE, Julius S et al. Blood Press. 2001;10:83–91.
VALUE: Patient Characteristics
Patients (%)
Associated Risk Factors Associated Diseases
0 10 20 30 40
Increased serum creatinine
LVH
Proteinuria
Active smoker
Diabetes
High Cholesterol
0 10 20 30 40 50
LVH with
Strain
PAD
Stroke
CAD
LVH = left ventricular hypertrophy. PAD = peripheral artery disease; CAD = coronary artery disease.
33.3
22.5
31.6
24.0
12.2
3.6
45.8
19.8
13.9
6.1
Patients (%)



Reduced First Occurence of Incident Atrial Fibrillation With ARB: the VALUE Trial
Schmieder RE, Kjeldsen SE, Julius SE et al. J Hypertens 2008; 26: 403-411.

Reduced First Occurence of Persistent Atrial Fibrillation With ARB: the VALUE Trial
Schmieder RE, Kjeldsen SE, Julius SE et al. J Hypertens 2008; 26: 403-411.

Importance of Incident Atrial Fibrillation for Primary Cardiac Endpoint: the VALUE Trial
Schmieder RE, Kjeldsen SE, Julius SE et al. J Hypertens 2008; 26: 403-411.

Never DM (8697)
New-onset DM (1298)
Baseline DM (5250)
Age (years) 67.5 ± 8.3 65.6 ± 8.0‡ 67.1± 7.9†
Gender (% male) 57.8 % 63.1%† 55.9%*
Caucasian 91.8 % 86.8 %‡ 85.9 %‡
BMI (kg/m²) 27.7 ± 4.6 29.6 ± 5.1‡ 29.9 ± 5.4‡
SBP (mmHg) 153.9 ± 19.0 154.4 ± 19.0 156.0 ± 18.9‡
DBP (mmHg) 87.8 ± 10.8 87.9 ± 10.8 86.9 ± 10.8‡
HR (bpm) 71.1 ± 10.5 72.9 ± 11.1‡ 74.2 ± 10.8‡
Glucose (mmol/L) 5.38 ± 0.60 5.88 ± 0.67‡ 9.25 ± 3.26‡
Potassium (mmol/L) 4.36 ± 0.45 4.32 ± 0.44† 4.43 ± 0.46‡
Pair-w ise comparison w ith never DM; *0.01≤ p-value<0.05, †0.0001≤ p-value<0.01, ‡ p-value <0.0001
VALUE: Baseline Characteristics Aksnes TA, Kjeldsen SE, et al. Hypertension 2007; 50: 467-73.



20
15
10
5
0
Patients Developing Atrial Fibrillation Have More Heart Failure
Heart failure (%)
Never DM New-onset DM Baseline DM
No Atrial Fibrillation New Atrial Fibrillation
2.8 11.3 15.8 3.6 6.9 22.6
Aksnes TA, Kjeldsen SE et al. Am J Cardiol 2008; 101: 634-8.

LVH
Systolic dysfunction
Diastolic dysfunction
HEART FAILURE
Obesity Diabetes
BP
Myocardial ischemia
Atrial Fibrillation


2013 ESH/ESC Hypertension Guidelines

ATRIAL FIBRILLATION HYPERTENSION
ACEI
ARB
CCB Diuretic
BB*
MRA*