Embed Size (px)
Citation preview

Prevention and Treatment of Prevention and Treatment of Urinary Stone DiseaseUrinary Stone Disease


Occurrence of Urolithiasis during Last Century
0
10
20
30
40
50
60
70
80
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990Year
Norway
UK
3.2
2.4
1.6
0.8
0
Ston
e C
ases
per
1,0
00 P
atie
nts
(Nor
way
)
Dis
char
ge fo
r Sto
nes
per 1
0,00
0 Po
pula
tion
in U
K
WW I
WW II
Oil crisis
Depression

0
20
40
60
80
100
0 5 10 15 20 25 30
Williams (1963)
Blacklock (1968)
Marshall et al (1975) (males)
Marshall et al (1975) (females)
Cum
ulat
ive
Recu
rren
ce (%
)
Years since first stone
Cumulative Recurrence of Stone-Formation in UK

Stone Recurrence Rates 3 Years After Various Urological Procedures for Stone Management
0
10
20
30
40
50
60
OpenSurgery
PCNL ESWL HM3
ESWL 2 & 3
NewStones
New +ResidualStonesPe
rcen
tage

Age at Onset of Stones in Males
0
5
10
15
20
25
30
35
0 10 20 30 40 50 60 70 80
London (1975)
Leeds (1985)
London (2001)
Age at Onset (years)
Perc
enta
ge (%
)
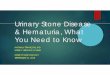
Age at Onset of Stones in Females
0
5
10
15
20
25
30
35
0 10 20 30 40 50 60 70 80
Age of Onset (years)
London (1975)
Leeds (1985)
London (2001)
Perc
enta
ge (%
)

Life-Time Expectancy of Stone-Formation in Men Aged 60-70 in Various Countries
0
5
10
15
20
25Ch
ina
UKGer
man
ySw
eden
Japa
nCa
nada
USA
UAE
KSA
Perc
enta
ge (%
)

URINARY STONES
MINERAL (90%) WATER (7%) ORGANIC MATRIX 3%)
Calcium oxalateCalcium phosphateMagnesium ammonium phosphateUric acid/uratesCystineXanthine2,8-DihydroxyadenineSilicaInsoluble drugs (eg Indinavir, Triamterene etc)
MucoproteinProtein

Predominant KSA USA UK KSA/UK* Mineral (%) (%) (%) Ratio
Uric acid 14.6 10.1 4.5 5.1
CaOx 71.3 58.8 53.8 2.1
CaP 7.6 20.3 30.9 0.4
MAP 3.7 9.3 9.6 0.6
Rare 2.8 1.5 1.7 2.6
* Including overall Saudi/UK prevalence ratio in adults of 1.6:1
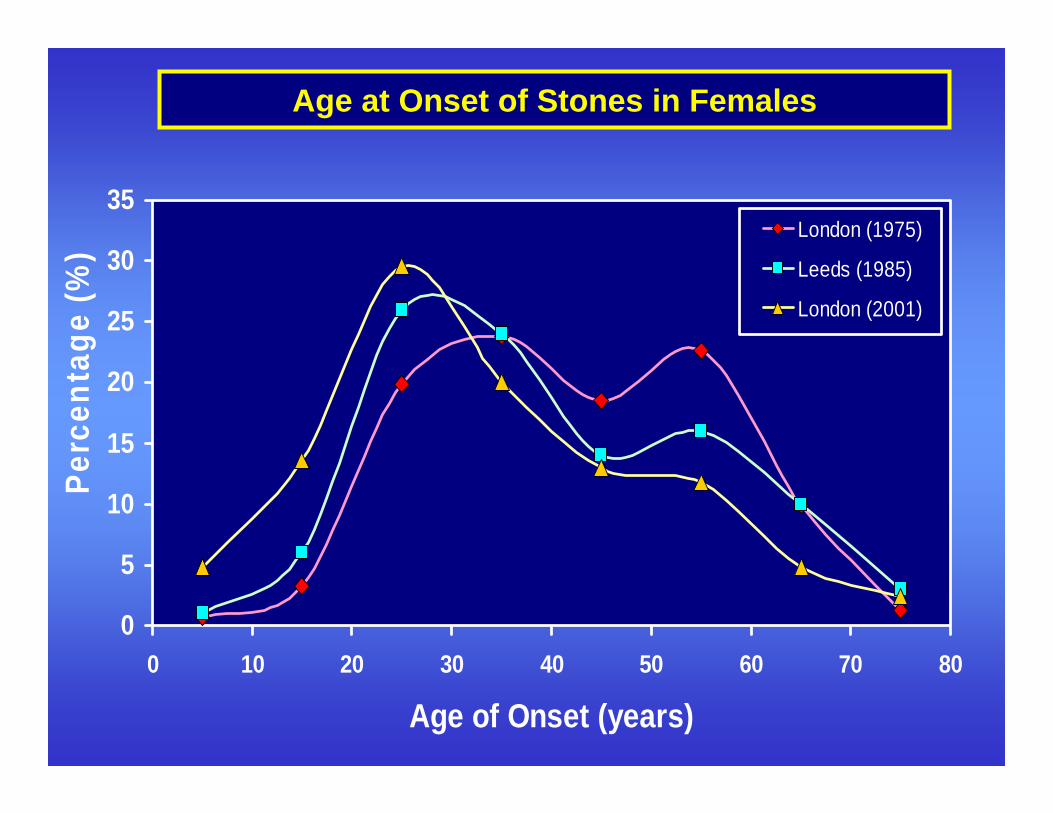
Mineral Solubilities in Water at 37ºC and pH 6
Mineral Maximum Solubility (g/litre)
Calcium oxalate 0.0071
Calcium phosphate 0.08
Magnesium ammonium phosphate 0.36
Uric acid 0.08
Cystine 0.17
Calcium sulphate 2.1
Calcium citrate 2.2
Magnesium sulphate 293
Calcium chloride 560

Simplest Model of Urinary Stone-Formation
Free-Particle Model
1. Crystal nucleation
2. Crystal growth and agglomeration
3. Retention of critically-sized particle
4. Growth of trapped particle into stone

CaOx Crystals and Aggregates Growing in Urine
20µm 20µm 100µm

Calcium Oxalate Microstone
100 µm

Diagram of Kidney
Stylised nephron

Urine containing
crystals flowing down collecting
tubules
Free-Particle Model of
Stone Initiation
Fixed-Particle Model of
Stone Initiation
Crystals growing and
agglomerating
Critical particle
trapped in tubule
Particle adheres to damaged site on tubule wall and other crystals
agglomerate with it

Supersaturation of Urine
-0.5
0
0.5
1
1.5
Incr
easi
ng S
uper
satu
ratio
n
Formation Product
Solubility Product
UNDERSATURATED ZONE: Crystal dissolution
METASTABLE ZONE: Heterogeneous Nucleation
Crystal Growth
UNSTABLE ZONE: Spontaneous Nucleation

↓ Tubularreabsorption
of cystine
Possiblemetabolic
factors
↑ Urinarycystine
↑ Cystinesupersaturation
Abnormalcrystalluria
Cystinestone
Risk Factor Model of Cystine Stone-Formation

Cystine Stone-Formation
Stone: Cystine (+calcium phosphate)Occurrence: ~1%Age: Child and adultGender: Male and female
Abnormal Normal
24-h Urine cystine ↑↑ Calcium metabolism24-h Urine lysine ↑↑, MSUarginine ↑↑, ornithine ↑↑

Risk Factors for Uric Acid Stone Disease
Pre-Urinary Urinary
↓ Renal NH3 production ↓ pH Ileostomy Gout ↑ Uric acid ↑ Purine intake Glycogen storage disease Lesch-Nyhan syndrome Neoplastic disease ↑ Percutaneous loss of fluid ↓ Volume Diarrhoea Ileostomy

Uric Acid Stone-Formation
Stone: Uric acid (+calcium oxalate)Occurrence:~5%Age: 30 - 70Gender: Male > female
Abnormal NormalPlasma uric acid ↑ Calcium metabolism24-h Urine uric acid ↑, MSU24-h Urine pH ↓24-h Urine volume ↓
Other FeaturesIleostomy

AgeSex (M > F)Genetic disordersMetabolic disorders↑ Dietary purine
↓ Renal NH3production↑ Dietary acid
↑ Urinaryuric acid
↑ Uric acid supersaturation
Abnormalcrystalluria
Uric acid
stone↓ Urinary
pH
↓ Urinaryvolume
↓ Fluid intake↑ Fluid loss↑ Ambient
temperature
Risk Factor Model of Uric Acid Stone-Formation

Additional Features of Infected Stone-Formation
• There is a metabolic abnormality in > 50% of patients with infection stones
• Any anatomical abnormality may lead to infection
• Ammonia may cause damage to protective GAG layer
• Recurrence in 10% of patients after complete removal
• Recurrence in 85% of patients if fragments remain
• Antibiotics may suppress bacteriuria and afford symptomatic relief but rarely totally eliminate infection in the presence of calculi

Calcium Stone-Formation
0
20
40
60
80
100
Idiopathic Hyper-Parathyroid
Others
FemaleMale
dRTA
Hyperoxaluria
MSK
Steroids
Hypervitaminosis D
Immobilisation
Milk-Alkali Syndrome

Inhibitors and Promoters of Crystallisation in Urine
INHIBITORSCitrate, Pyrophosphate, Magnesium, ADP, ATP, Phosphocitrate, Glycosaminoglycans, Tamm-Horsfall Mucoprotein, Uromodulin, (Osteopontin), α-1-Microglobulin, β-2-Microglobulin, Urinary Prothrombin Fragment 1, Inter-α-Inhibitor
PROMOTERSUromucoid (Polymerised THM), Matrix Substance A

Normal Subjects RSF RSF
Recurrent CaOx Stone-Former (RSF)

0
0.5
1
1.5
2
2.5
0 10 20 30 40
Basal
+ Orthophosphate
Percentage of large crystals (>12 µm in diameter)
Ston
e ep
isod
es/y
ear
Severity of Calcium Stone Disease and Crystalluria

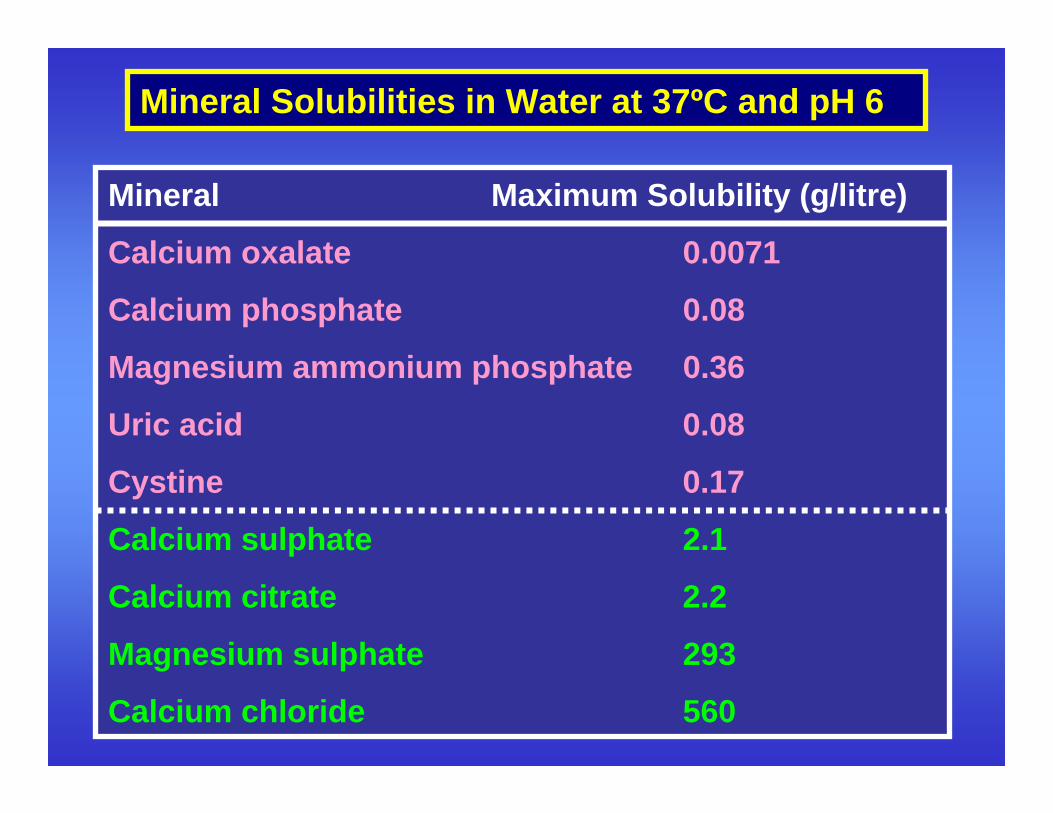
Risk Factor Model of Calcium Stone-Formation
Abnormal Crystalluria
Stone
↑Supersaturation
↓ Inhibitors
↑ Promoters

Urinary Risk Factors for Calcium Stone-Formation
• Low urine volume
• Mild hyperoxaluria
• Increased urinary pH
• Hypercalciuria
• Hypocitraturia
• Hyperuricosuria
• Hypomagnesiuria

Urinary Risk Factors in Stone-Formers and Normals
Volume (litres)
Calcium (mmol) Oxalate (mmol) pH
Citrate (mmol) Uric Acid (mmol) Magnesium (mmol)
SF SF SF SF
SF SF SF
N N N N
N N N
1 2 3 5 10 15 0.2 0.4 0.6 . 5.0 6.0 7.0
25
50
25
50
Freq
uenc
y (%
)
Log RS (Uric Acid)
SF
N
l l l l l l l l l l l l l l l
0 2 4 0 2 4 6 0 3 6 9 -1 0 1 2

0
5
10
15
20
-3 -2 -1 0 1 2 3 4
Oxalate
pH
Calcium
Uric Acid
Volume
Citrate
Magnesium
SD Units from Mean Value in Normal Population
Rel
ativ
e R
isk
Fact
or (α
= SF
/N)
Risk Curves for Urinary Risk Factors for Stone-Formation

0
1
2
3
4
5
6
7
8
2 3 4 5 6 7 8
0.001 0.01 0.1 0.5 0.9 0.99 0.999
Relative Probability (PSF)
Ston
e Ep
isod
e R
ate
(No/
year
) Severity of Stone-Formation

Example of Risk Accumulation in a "Normal-Looking" Urine from a CaOx/CaP Stone-Former Compared with that of a Normal
Patient (AGW) Normal (JHT)Volume (litre/day) 1.50 1.65pH 6.10 6.00Calcium (mmol/day) 5.98 5.50Magnesium (mmol/day) 3.62 4.50Oxalate (mmol/day) 0.40 0.35Uric acid (mmol/day) 3.66 3.20Citrate (mmol/day) 2.11 2.50
PSF(CaOx) 0.85**** 0.35PSF(CaOx/CaP) 0.90***** 0.36PSF(CaP) 0.67** 0.42

Idiopathic Calcium Stone-Formation
Stone: Calcium oxalate and/or calcium phosphate or uric acid
Occurrence: 70%Age: 15 - 75Gender: Male > female (3:1)
Abnormal Normal24-h Urine volume ↓ Plasma Ca, Pi, PTH24-h Urine pH ↑ MSU24-h Urine calcium ↑24-h Urine oxalate ↑24-h Urine uric acid ↑24-h Urine citrate ↓24-h Urine magnesium ↓
Risk Factor Model of Calcium Stone-Formation
Abnormal Crystalluria
Stone
↑ Calcium
↑ Oxalate
↑ pH
↓ Volume
↓ Citrate
↓ Magnesium
↑ Uric acid
↑Supersaturation
↓ Inhibitors
↑ Promoters

AgeGenderSeasonClimate
Fluid IntakeStress
OccupationAffluence
DietMetabolic disordersGenetic disorders
Epidemiological Risk Factors for Calcium Stone-Formation

0
2
4
6
8
10
12
2.00 2.50 3.001.5
2.0
2.5
3.0
3.5
2.10 2.20 2.30 2.40 2.50
1.5
2.0
2.5
3.0
3.5
2.10 2.20 2.30 2.40 2.500
5
10
15
20
0 1000 2000 3000 4000 5000
Leeds 1971-73i
ii
iiii
vv
UK Regions 1971-73
Sc
WM
EM
NNW
SW
YHSE
EAWa
InP
T EgIs ItJIrl F A
UK
N
NZ
NLAus
D S
Can
KSA
USA
UAE
Ann
ual D
isch
arge
s fo
r Sto
nes/
104
Popu
latio
n
Weekly Food Expenditure (£) Gross National Product ($)
UK 1958-73 World
Arg
Stones and Affluence

40
45
50
55
2.00 2.50 3.0042
44
46
48
2.10 2.20 2.30 2.40 2.50
42
44
46
48
2.10 2.20 2.30 2.40 2.500
20
40
60
80
100
0 1000 2000 3000 4000 5000
Leeds 1971-73i
iiii
iivv
UK Regions 1971-73
Sc
WM
EMN
NW
SW
YH
SE
EAWa
InP
T Eg
Is ItJ
Irl FA
UK
N
NZ
NL
Aus D S
Can
KSA
USA
UAE
Ani
mal
Pro
tein
Con
sum
ptio
n (g
/day
)
Weekly Food Expenditure (£) Gross National Product ($)
UK 1958-73 World
Arg
Animal Protein Intake and Affluence

0
2
4
6
8
10
12
42 46 50 541.5
2.0
2.5
3.0
3.5
42 44 46 48
1.5
2.0
2.5
3.0
3.5
42 44 46 480
5
10
15
20
0 20 40 60 80 100
Leeds 1971-73i
ii
iiii
vv
UK Regions 1971-73
Sc
WM
EM
N NW
SW
YH SE
EAWa
InP
T EgIsIt
J
IrlF
AUK
N
NZ
NLAus
D S
Can
KSA
USA
UAE
Ann
ual D
isch
arge
s fo
r Sto
nes/
104
Popu
latio
n
Animal Protein Intake (g/day)
UK 1958-73 World
Arg
Stones and Animal Protein Intake

0
2
4
6
8
10
12
14
16
18
20
0 20 40 60 80 100
KSA
UAE
USA (1975)
USA (1950)
Can
NZS
It (1978)
ArgAus
D
NL
It (1954)
N J (1990)
J (1960)
UK (1979)UK (1958)
AIrl
F
Is
Eg
PIn
World
Animal Protein Intake (g/day)
Adm
issi
ons
for S
tone
/104
Adu
lt Po
pula
tion

050
100150200250
1965 1970 1975 1980 1985
0
5
10
15
20
1 9 6 5 1 9 7 0 1 9 7 5 1 9 8 0 1 9 8 5
Year
Uric acid
Cystine
Calcium
Infection
Ston
es R
ecei
ved
for A
naly
sis
(no/
year
)

0
1
2
3
4
5
Leeds Study(1980)
Vegetarians SecondaryStones
Prev
alen
ce (%
)Prevalence of Urinary Stone Disease in Men

Other Dietary Factors Influencing Urinary Stone-Formation
↑ Calcium - ↑ Urinary calcium
↓ Calcium - ↑ Urinary oxalate
↑ Oxalate - ↑ Urinary oxalate
↑ Sodium - ↑ Urinary calcium
↑ Refined sugars - ↑ Urinary calcium
↓ Fibre - ↑ Urinary calcium
↑ Fibre - ↓ Urinary volume
↓ Magnesium - ↓ Urinary magnesium

0
1
2
3
4
5
6
7
8
9
1 0
0 1 2 3 4Urine Volume (litre/day)
0.5
0.01
0.1
0.999
0.9999
0.99
0.9
0.0010.0001
Rel
ativ
e Pr
obab
ility
(PSF
)Normal Subjects
Low fluid intake
Normal fluid intake
High fluid intake

Occupation, Low Urine Volume and Urolithiasis
Occupation Percent of Male Stone-Formers
Urine Volume
(litre/day) Taxi-Drivers, Chauffeurs
5.6
1.42 ± 0.27
Chefs, Kitchen-Workers
6.3
1.31 ± 0.34

Dietary Risk Factors for Stones in Saudi Arabia
Dietary Constituent UK USA KSA
Animal protein (g/day) 61 85 87
Calcium (mmol/day) 24.5 25.0 13.0
Oxalate (mmol/day) 1.4 - 3.8
Purine (mg/day) 150 257 265
Oxalate/Calcium 0.06 - 0.29

0
5
10
15
20
25
0 2 4 6 8 10 12 14 16 18 20Urine Calcium (mmol/day)
Freq
uenc
y (%
)
0
2
4
6
8
10
12
14
Cal
cium
Ris
k C
urve
Normals
Stimulated
Risk curve
Effect of Small Increase in Urinary Calcium Excretion in the Population
Mean 6.2 mmol/day
Mean 6.5 mmol/day

Medical Management of Urolithiasis
• To identify the particular risk factors for stone-formation in the patient concerned
• To reduce the supersaturation of urine with respect to the stone-forming mineral concerned in order to minimise the risk of forming abnormal crystals and aggregates in urine
• This may be achieved by means of dietary and/or medical treatment
Objectives:

Medical Management of Non-Calcium-Containing Stones
Stone Treatment
2,8-DHA Very high fluids + allopurinolXanthine Hereditary: High fluid intake + alkali (pH >7.4)
Iatrogenic: Withdraw allopurinolCystine Very high fluids + alkali (pH >7.5) or
D-penicillamine or α-mercaptopropionylglycineUric acid High fluids + alkali (pH >6.2) or reduce purine
intake or allopurinolInfected Antibiotics + high fluids + oral acid (pH <6.2)
Iatrogenic Discontinue drug concerned and replace withalternative treatment + high fluids

Medical Management of Calcium Stones
Patient Type TreatmentIdiopathic High fluids + relevant dietary advice or
thiazides or phosphate or magnesiumsupplements or potassium citrate (K3Cit)
Hyperparathyroid Parathyroidectomy or high fluid + acids1° Hyperoxaluric High fluids + pyridoxine2° Hyperoxaluric High fluids + low Ox + high Ca or K3CitDistal RTA High fluids + thiazides or K3CitMSK Treat as for idiopathicCorticosteroid Discontinue steroids; treat as idiopathicMilk-alkali syndrome Discontinue alkali; reduce Ca + fluidsVit D intoxication Discontinue vitamin D supplements

Problems in the Medical Management of Patients with Urinary Stones
• It is impossible to treat stone patients satisfactorily without proper biochemical screening and this has been abandoned by many hospitals world-wide
• Most stone patients feel well most of the time apart from the occasions when they have renal colic
• It is difficult to motivate them to keep to their dietary or medical treatment over a long period and their biochemical risk of forming stones increases (the Anti-"Stone Clinic Effect")

0
5
10
15
20
0 4 8 12 16 20 24Time (weeks)
Urin
e C
alci
um (m
mol
/day
)
0
0.2
0.4
0.6
0.8
0 4 8 12 16 20 24Time (weeks)
Urin
e O
xala
te (m
mol
/day
)
The Anti-"Stone Clinic Effect"
Colic
Colic




















![Urinary Stone Management [Dr. Edmond Wong]](https://img.pdfslide.us/doc/110x75/55d4fd91bb61eba4528b46ca/urinary-stone-management-dr-edmond-wong.jpg)