Embed Size (px)
DESCRIPTION
Prevention and Management of Pressure Ulcers for nursing homes
Citation preview
Leeds Community Healthcare is responsible for providing NHS services in the Leeds area and is hosted by NHS Leeds Primary Care Trust.
The Prevention and Management of Pressure Ulcers
in the Community
Authors
Jackie Dawson Tissue Viability Nurse Specialist Nikki Stubbs Clinical Team Leader Tissue Viability Tissue Viability Service
Corporate Leads
NHS Leeds Community Healthcare Angie Clegg Acting Director of Nursing and Allied Health Professionals Dr Amanda Thomas Medical Director
Date Ratified at C-GaP
26th January 2010
Status
Final
Date Approved by Quality Governance and Risk Committee
12th March 2010
Review Date
March 2013
Guideline Number
PL182
The Prevention and Management of Pressure Ulcers in the Community
Page 1 of 24
CONTENTS
1. Purpose .........................................................................................................................................2
2. Scope .............................................................................................................................................2
3. Equality Impact Assessment (EIA) ........................................................................................2
4. Objectives .....................................................................................................................................2
5. Client Group – Inclusion...........................................................................................................2
6. Client Group – Exclusion..........................................................................................................2
7. Staff Requirements ....................................................................................................................2
9. Mental Capacity Act (MCA 2005 Code of Practice)............................................................3
10. Risk Assessments....................................................................................................................3
11. Audit and Monitoring...............................................................................................................4
Guidelines ...........................................................................................................................................
References......................................................................................................................................11
Appendix 1: Equality Impact Assessment – Relevance Screening.................................13
Appendix 2: Glossary of Terms and Risk Factors ...............................................................13
Appendix 3: Signs to observe when inspecting the skin ...................................................16
Appendix 4: Equipment Selection............................................................................................17
Appendix 5: Pressure Ulcer Care Pathway for Screening and Assessment ................19
Appendix 6: Pressure Relieving/Reducing Equipment ......................................................20
Appendix 7: NPUAP/EPUAP (2009) Pressure Ulcer Classification System ..................21
Appendix 8: 30º Tilt Leaflet.........................................................................................................23
Clinical Guideline Consultation Process................................................................................24
The Prevention and Management of Pressure Ulcers in the Community
Page 2 of 24
1. Purpose
The purpose of this guideline is to enable staff to take the necessary actions to prevent, detect and manage pressure ulceration. The actions and rationales detailed in this guideline include the key NICE (2005) recommendations. Additional NICE (2005) information can be found in Appendix 1. NICE has agreed that the use of clinical judgement and the use of a pressure ulcer risk assessment tool facilitates accuracy when identifying whether a patient is at risk of pressure ulcers. This guideline examines all the processes and stages required to identify and manage patients’ individual risk of pressure ulceration. 2. Scope This guideline sets out the standards and procedures for any member of staff in Leeds PCT, irrespective of age, race, colour, religion, disability, nationality, ethnic origin, gender, sexual orientation or marital status, domestic circumstances, social and employment status, HIV status, gender reassignment, political affiliation or trade union membership. This guideline is for all health professionals caring for patients at risk of or with existing pressure damage. 3. Equality Impact Assessment (EIA) An equality impact assessment of this guideline was completed, and was screened at low. Ethnicity data is collected on the referral form to the Tissue Viability Service. 4. Objectives For all staff in Leeds PCT to prevent, detect and manage pressure ulcers. A pressure ulcer is an area of localised damage to the skin and underlying tissue caused either by pressure, friction and shear, or a combination of these, (E.P.U.A.P. 2003). Pressure ulcers are graded 1-4, according to level of severity, using the European Pressure Ulcer Advisory Panel scoring system. Usually pressure ulcers occur on areas of bony prominences, hips, heels, sacrum, elbows, shoulder blade, spine, back of the head, ear lobe. 5. Client Group – Inclusion All adults and children 6. Client Group – Exclusion None. 7. Staff Requirements All nurses both registered and non registered. All registered nurses will be expected to attend the Tissue Viability Service Pressure Ulcer study day. Health support workers will be expected to complete the Tissue Viability workshop incorporated into the competency framework for health support workers.
The Prevention and Management of Pressure Ulcers in the Community
Page 3 of 24
8. Resources and Equipment Patient records Pressure Ulcer Care Plan Braden Scale Practice Guidelines for the Provision of Equipment First Choice Dressing List EPUAP Classification System Generic Wound assessment form LCES Justification form/LES 2 9. Mental Capacity Act (MCA 2005 Code of Practice) This Act applies to all PCT employees who provide care and/or treatment to persons over the age of 16 who are judged to lack capacity to consent or withhold consent to acts, which are considered by health and social care professionals to be in the best interests of their welfare and health. This guidance in the Mental Capacity Act 2005 Code of Practice is designed specifically to assist carers, health and social care practitioners in the assessment of mental capacity and, where necessary, making decisions on behalf of individuals who lack capacity, in their best interests. Detailed guidance is available in the Mental Capacity Act 2005 Code of Practice (http://www.dca.gov.uk/legal-policy/mental-capacity/mca-cp.pdf ) The Code provides guidance on when a general power of authority for day to day decisions on health and welfare needs can be used and when a formal assessment of capacity and decision making will be required. It provides guidance on professional responsibility for assessing capacity and making best interest decisions. It provides guidance on recording mental capacity assessments and an understanding of what constitutes best interests and how to conduct and record a best interests assessment and decision. This includes actions to be taken in cases of conflict, dispute or when a second opinion or assessment is required. The Code provides guidance for staff regarding the legal position of Advanced Decisions, Lasting Powers of Attorney and the Court of Protection in relation to adults who lack capacity. It will enable staff to recognise when and in which circumstances there is a legal duty to refer to an Independent Mental Health Advocate (IMCA) and their statutory role. The Code provides guidance for staff on the limits of actions that can be taken on behalf of a person who lacks capacity and the protection afforded to staff and patients under Section 5 of the Mental Capacity Act 2005. 10. Risk Assessments All patients must be screened for risk of pressure ulceration. This must recorded, on RIO for one off visits, and in the district nursing core documents, for patients requiring longer interventions. Patients at risk must have a completed pressure ulcer prevention care plan. All patients with classification 2 and above pressure ulcers must have an IR1 completed.
The Prevention and Management of Pressure Ulcers in the Community
Page 4 of 24
11. Audit and Monitoring Audits will be carried out yearly in conjunction with Essence of Care work, to determine concordance of guidelines. Additionally, data collected from the reporting of incidents of pressure ulcers will be analysed to identify where adjustments need to be made to practice.
The Prevention and Management of Pressure Ulcers in the Community
Page 5 of 24
Action ? Rationale Risk Assessment - When All patients must be screened for their risk of developing pressure ulcers. It is the responsibility of all health professionals to undertake the initial and any necessary ongoing assessment. Screening needs to be recorded as a RiO activity and where patient held records are being completed recorded in the skin section of the nursing assessment form A risk assessment must be conducted at initial assessment by health professionals if the initial screening identifies risk f the patient is an in patient on one of the community wards e.g. Community Rehabilitation Unit /V Ward the patient must be screened and if required assessed for risk within 6 hours of admission Risk assessment –What A Braden Risk assessment must be completed for all patients screened and identified as at risk of pressure ulceration. In Leeds PCT the recommended tool is the Braden (1994) score. This must be completed at initial assessment, then repeated monthly or as a patient’s condition changes.(see appendix 1 )
à
Screening patients enables the health professional to identify patients at risk of developing pressure ulcers and to identify those with ongoing risk needs. It also enables the nurse to screen out those patients at no or very low risk. To demonstrate concordance with NICE, (2005) and Essence of Care, (2003) recommendations, Supports clinical decision making and resource allocation In order to ensure that patients risk is identified and measures are put in place to address this. Carrying out the assessment within these time scale enables an immediate preventative care plan to be devised, implemented and documented to reduce pressure damage occurring. This is in line with the NICE (2005) and Essence of Care benchmark for pressure ulcers,(DOH 2003). This is in line with The Tissue Viability Service’s recommendations. Research evidence exists to support the sensitivity and specificity of the Braden tool. Reassessment of risk enables the nurse to recognise when a patients’ pressure needs have changed. Adjustments to the care plan can then be made immediately to reduce the likelihood of pressure damage.
The Prevention and Management of Pressure Ulcers in the Community
Page 6 of 24
Action ? Rationale Extrinsic Factors Direct Pressure Patients unable to change their own position need to have a repositioning regime developed and documented which supports risk management .The frequency of repositioning will be based upon their individual skin response to pressure(appendix 3) Friction/Shear Clinicians need to implement measures to reduce the impact of friction and shear. This can occur as a result of frequent skin washing and incorrect moving and handling techniques. Use of slide sheets and correct profiling of patients should be implemented to minimise risk Intrinsic Factors Immobility and /or Sensory Impairment Assessment should consider the patients ability to change their own position and any equipment provided should maximise patients’ independent movement Patients with some mobility should be made aware of the need to reposition themselves in accordance with their individual response to pressure Clinicians need to record the frequency of repositioning on the pressure ulcer prevention plan and on the patients care plan
à
In order to minimise the impact of prolonged, sustained pressure In order to minimise the impact of skin stripping from frequent skin cleansing and the impact of friction and shear from incorrect moving and handling To maximise patients independence To encourage patients to take ownership of their risk of pressure damage To facilitate communication of the patient’s risk and the management plan for that risk. To encourage ownership of risk
NB This is particularly important in patients with impaired sensation as their inability to feel pressure/pain can result in an underestimation of their risk Patients should be provided with an ‘Are you at Risk’ – your guide to preventing pressure sores document (available from the TV service Additional information can be sought on www.nice.org.uk, patient information link
à
To encourage ownership of risk To educate the patients with regard to their risk
The Prevention and Management of Pressure Ulcers in the Community
Page 7 of 24
Action ? Rationale Change in consciousness level Acute, chronic or terminal illness affecting a patient’s level of consciousness should initiate a re-assessment of individual risk of pressure ulcers
à
A drop in conscious level and health status increases risk
Previous pressure damage Assessment of the patients skin to identify previous scar tissue from pressure ulceration and a history of previous skin damage needs to be documented in skin section of the core document
à
Patients who have developed pressure ulcers in the past have an 80% increased chance of the pressure ulcer reoccurring, (N.I.C.E. 2005).
Nutrition and hydration status If nutrition is identified as a risk factor for the individual, the nurse must support the pressure ulcer risk assessment with a nutritional screening tool, then document on the Tissue Viability Service Preventative Care plan that it has been undertaken. Assessment of the patient’s hydration level must be made. Acute dehydration increases the incidence of pressure ulceration.
à
To identify patients who are at risk of malnutrition(either over or under weight) as this is known to increase the risk of developing pressure ulcers
Moisture to the skin For those patients with incontinence, measures such as catheterisation/pad usage need to be considered in order to minimise the impact of moisture on the skin. Need to consider that the use of pads/incontinence sheets between the patient and a pressure relieving mattress/cushion may reduce the benefits of the equipment
• Also need to consider patients with excessive sweating or exudate leakage from wounds
à
Moisture to the skin increases the risk of pressure damage
Skin inspection/repositioning In addition to carrying out an individual assessment of patient’s skin response to pressure, the patient’s skin needs to be assessed for evidence of pressure damage e.g non blanching erythema
à
To facilitate the identification of non blanching erythema /skin damage
A film dressing such as tegaderm / c view should be applied to the area of non blanching erythema
à
To protect the damaged tissue
The Prevention and Management of Pressure Ulcers in the Community
Page 8 of 24
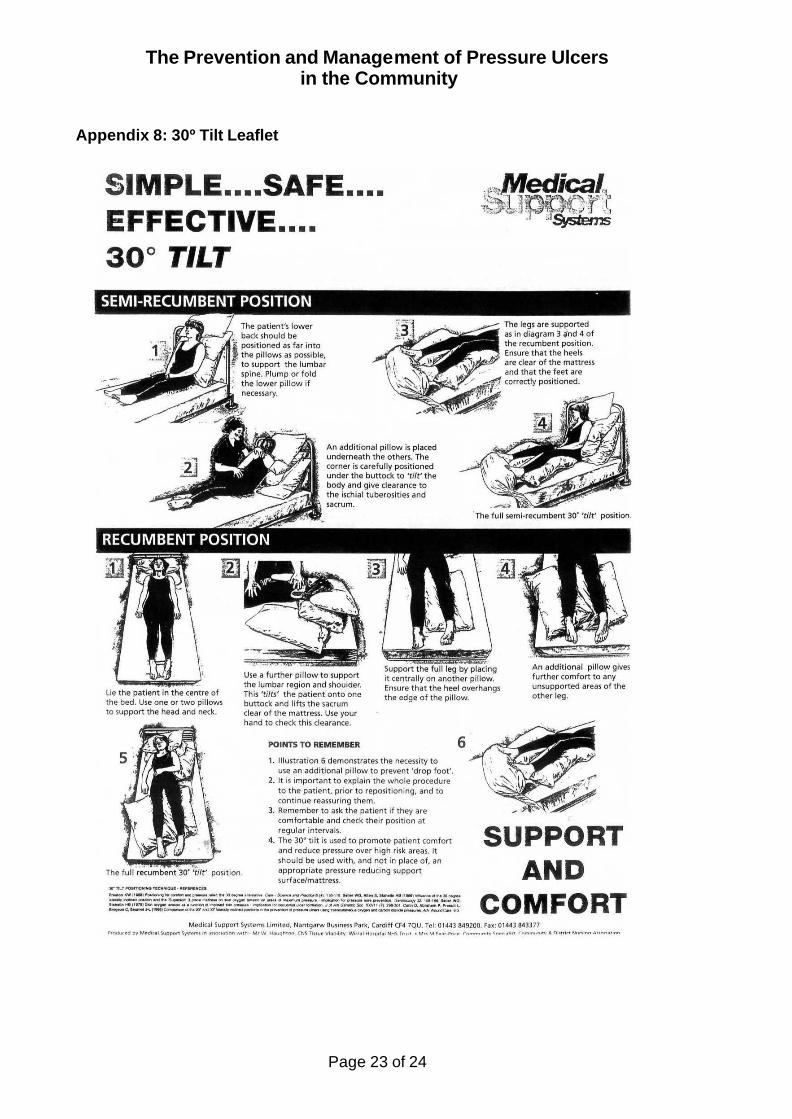
Action ? Rationale Patients should not be repositioned directly onto pressure ulcers or bony prominences where possible (NICE 2005). NB. The 30 degree tilt can be used as a repositioning alternative for vulnerable patients, ( see appendix 8).
à
Due to increased risk of further pressure. The 30 degree tilt can enable pressure relief without excessive positional change in patients in pain, with existing pressure damage or with limb contractures where repositioning is difficult
Assessment should include the repositioning needs of patients seated in both chairs and wheelchairs. If a patient is identified to be at risk of pressure damage, the time spent sat should be restricted to 2 hours maximum (NICE 2005)
à
Patients who spend long periods seated are at increased risk of developing pressure ulcers, (Anton 2005).
Clinicians should encourage patients to change their own position and demonstrate to the patient how to redistribute weight/relieve pressure whilst in bed or chair
à
To reduce risk and facilitate concordance.
Equipment Pressure relieving/reducing equipment should be provided which is appropriate to the patients level of risk
à
To manage the identified risk
‘The Leeds Community Equipment Service practical guidelines for the provision of equipment‘ should be referred to in order to facilitate appropriate equipment selection for patients’ level of risk. See appendix 4 for list of factors to consider when selecting equipment. Equipment should be ordered on a LES 2 and supported with a justification form which justifies why the equipment is appropriate for the patient including their medical condition, patient carer needs, moving and handling issues
à
In order to identify equipment which is readily available and fit for purpose from LCES In order to ensure that the Budget Management Group at LCES are able to allocate resources appropriately
When prescribing equipment, always consider the safety implications and the impact of equipment on the patients’ independent repositioning and transfers. For example does the patient require cot sides and how will that reduce/increase risk of entrapment, or if a patient now is unable to transfer due to the provision of an alternating mattress
à Ensuring that the equipment provided does not increase patient risk. There are clear MDA recommendations around the provision of equipment. If unsure, contact the Tissue Viability Service or LCES for advice.
The Prevention and Management of Pressure Ulcers in the Community
Page 9 of 24
Action ? Rationale Pressure Ulcer –wound assessment All patients with a pressure ulcer must have a generic wound assessment form completed . This must be completed on initial assessment and re-evaluated monthly or if any change occurs NB for wound assessment and management see separate guidelines Hyperlink to Leeds health pathways Wound Management: http://nww.lhp.leedsth.nhs.uk/common/guidelines/other_versions/1102v2.pdf Aseptic Technique: Wound Cleansing Guideline - Leeds PCT MRSA:http://nww.lhp.leedsth.nhs.uk/common/guidelines/other_versions/684.pdf
à Clearly documenting the wound assessment provides baseline information about the cause of the ulcer, an accurate description of the ulcer, effectiveness of treatments and repositioning regimes, (Stephen-Haynes 2006).
NICE states that the assessment must be supported by maps detailing the wound dimensions. If available, a photograph can be taken to support documentation. Where photography is used, a consent form must be completed (see consent guideline).
à
To monitor deterioration/improvement in wound size
All ulcers must be classified using the European Pressure Ulcer Advisory Panel 1-4 classification system, (see appendix 7 for clarification)
à
In line with NICE (2005).
Pressure ulcers must not be reversed graded as they heal.
à
To ensure that the original degree of damage is taken into consideration for future management/risk.
All pressure ulcers classified 2 and above must be reported as a clinical incident on an IR1 form, in line with the PCT incident reporting guidance. NB see the flow chart in appendix 6 for guidance on pressure ulcer incident reporting
à
In line with NICE (2005) and PCT recommendations.
If patients are to be transferred to another care setting or admitted to hospital, a written record of the patients risk, severity of wounds and management plan should be communicated.
à
To ensure continuity of care and management of risk
The Prevention and Management of Pressure Ulcers in the Community
Page 10 of 24
Action ? Rationale Referral to other professionals Patients with non healing /deteriorating pressure ulcers should be referred, in writing, to the Tissue Viability team. Patients who fail to respond to conservative measures may need referral to a plastic surgeon for possible surgery (NICE 2005)
à
To ensure all risk factors have been addressed To ensure that patients receive specialist care if needed To ensure that all treatment options are considered
The Prevention and Management of Pressure Ulcers in the Community
Page 11 of 24
References The following guideline is evidenced based. The Tissue Viability Service uses the grading system adapted from the Scottish Intercollegiate Guidelines Network, (SIGN 50). The grading system of A,B,C, D, or GPP, (Good Practice Point) Anton L. (2006) Pressure ulcer prevention in older people who sit for long periods, Nursing Older People 18 4 29-35 GPP Bale, S. Cameron, J. Meaume, S.(2006) Skin Care in Aetiology and Risk Factors in Science and Practice of Pressure Management, Springer-Verlag London GPP Bliss, M. Gebharat K, (1994) Preventing pressure ulcers in orthopaedic patients is prolonged chair nursing detrimental? Journal of Tissue Viability 4 (2) 51-55 GPP Braden B. J. Bergstrom N. (1994) Predictive validity of the Braden score for pressure sore risk in the nursing home population. Resident Nursing Health 17 459-470 C Collier M. Moore Z. (2006) Aetiology and Risk Factors in Science and Practice of Pressure Management, Springer-Verlag London. Defloor T. De Bacquer D. Grypdonck M. (2005) the effect of various combinations of turning and pressure reducing devises on the incidence of pressure ulcers. International Journal of Nursing Studies 42 37-46 C Department of Health (2007) Improving Nutritional Care A joint action plan from the Department of Health and Nutrition Summit stakeholders .A Department of Health (2003) Essence of Care Benchmarks for Pressure ulcers. A EPUAP/NPUAP (2009) Pressure ulcer treatment guidelines A Fernandos T. (2007) Preventing pressure ulcers selecting the right equipment International Journal of Therapy and Rehabilition.14 5 235-237 GPP Langemo D. Brown G. (2006) Skin fails too: Acute, chronic and end stage skin failure. Advances in Skin and Wound Care 19 4 206-211 GPP Langemo D. (2006) when the goal is Palliative Care. Advances in Skin and Wound care 19 3 148- 153 GPP Stephen- Haynes J. (2006) NICE pressure ulcer guideline: summary and implications for practice British Journal of Nursing Sep, 11 9 S18-24 GPP McManus J. (2007) Principles of skin and wound care: the palliative approach End of Life 1 1 8-19 GPP National Institute of Clinical Excellence (2005) Guideline GC29 The prevention and management of pressure ulcers A

The Prevention and Management of Pressure Ulcers in the Community
Page 12 of 24
References continued National Institute of Clinical Excellence (2006), Guideline CG32, Nutritional Support, enteral tube feeding and parental nutrition, A Nixon, J. Cranny, G. Bond, S. (2007) Skin alterations of intact skin and risk factors associated with pressure ulcer development in surgical patients. A cohort study. International Journal of Nursing studies 44 655-663 B
The Prevention and Management of Pressure Ulcers in the Community
Page 13 of 25
Appendix 1:
Equality Impact Assessment – Relevance Screening 1. Name of the policy/strategy/project or service
Clinical Guideline for the Prevention and Management of Pressure Ulcers in the Community
2. What are the main aims and objectives of the policy/strategy/project or service?
To ensure wounds are assessed in a systematic way in order that suitable wound care products are prescribed. To determine wound progress in an objective manner. To accurately document wound assessment and progress wound.
Yes No 3. Is this a key strategic document or a major project/programme
X
High Medium Low Don’t know 4. What impact will this policy/strategy/project or service have on the public or staff? X
Please explain: This guideline will have a low impact on Equality and Diversity as: a) It is not selective of the client group, therefore the potential for discrimination is removed,
service equality impact assessments will have been completed by services utilising these guidelines.
b) Access to treatment is open to all client groups c) Care is delivered across various venues.
Yes No Don’t Know
5. Is there any evidence, or other reason to believe, that different groups have different needs, experiences, issues and priorities in respect of this particular policy/strategy project or service etc?
x
Please explain: Access to the interpretation service is available to NHS Community Healthcare Staff and staff should be aware of when and how to refer to this service. NHS Community Healthcare staff should have attended Equality and Diversity training and regularly receive updates through staff briefing and formal channels. NHS Community Healthcare Staff should be aware of the ethnicity of patients and of any specific individual requirements required prior to visiting patients and where necessary specific arrangements made. If you have answered Yes to question 3, you should move straight on to a Stage Two Assessment. If, for question 4 you have answered Low, there is no need to continue to an Equality Impact Assessment. If for question 4 you have answered Medium and No for question 5, there is no need to continue to an Equality Impact Assessment. If, for question 4 you have answered Medium or Don’t Know, and have answered Yes or Don’t Know for question 5 you should move on to a Stage One Equality Impact Assessment. If, for question 4 you have answered High, you should consider whether you need to undertake a Stage One Impact Assessment or move straight to a Stage Two Impact Assessment. Stage One Stage Two None 6. Based this screening please indicate if this policy/strategy/project or service should proceed to a Stage One or Stage Two assessment?
X
Signed: J Dawson Signed: ……………………………. Lead Officer
The Prevention and Management of Pressure Ulcers in the Community
Page 14 of 24
Appendix 2: Glossary of Terms and Risk Factors A risk factor is either a health problem or illness that could make the patient more susceptible to pressure ulcers, (Collier/ Moore 2006) The guidance of NICE, (2005) recommends that the following are key indicators of pressure ulcer development. Identification and minimising risks can reduce pressure damage occurring. Direct Pressure damage occurs when the oxygen supply to the tissues of the skin becomes deprived. Usually this occurs when a patient has spent long periods either sat or laid, in one position. Friction, is the action of two surfaces sliding across one another. For example, when incorrectly repositioning a patient. Shearing, occurs when strain is placed on the skin and upper layers, consequently they are pulled away from the deep skin. An example of this is when a patient either slides or is dragged down the bed. Mobility: This must include whether the patient can change their position, how much assistance is required. Level of understanding, patient compliance. Crucially, patients who spend long periods in the chair are also at very high risk of developing pressure ulcers. Sensory Impairment: Patients with medical conditions such as diabetes and spinal injuries have reduced sensation/ feeling. They are unable to feel pain or discomfort when sat or laid for long periods. Therefore need prompting or assistance to relieve pressure.
Level of consciousness a patient whose consciousness is impaired through illness or medication will require assistance to reposition. Acute illness such as a chest infection, myocardial infarction, Cerebral Vascular Accident, reduces the blood supply to the skin, consequently, causing the skin to be vulnerable to pressure damage, (Langemo and Brown 2006). Chronic illness, the skin of patients with chronic diseases such as diabetes, heart failure and Chronic Pulmonary disease gradually becomes more vulnerable to ulceration. Specifically, the skin gradually begins to fail due to a limited oxygen supply. Furthermore, pressure damage can occur more rapidly due the reduced level of capillary closure. Additionally, patients with these illnesses often have other associated risk factors such as restricted nutritional and hydration intake impaired level of mobility. Terminal Illness, multiple failure of organs, and catabolism ( wasting of tissue ) occurs in end of life diseases therefore the skin of this group of patients is less tolerant and increasingly vulnerable to pressure ulcers, (Langemo 2006, McManus 2007). Posture: Certain medical conditions, specifically neurological illnesses, such as Multiple Sclerosis, can cause fixed muscle contractures which if uncorrected affect posture.
The Prevention and Management of Pressure Ulcers in the Community
Page 15 of 24
Appendix 2: Glossary of terms and risk factors continued Additionally patients also at risk are those who sit slumped in the chair. Consideration should be made for the type of chair the patient is sat in. Is it too high, too small, or is the width restrictive Inadequate seating posture places increasing strain on the skin and causes an uneven distribution of pressure. Most specifically, to the ischial tuberosities, heels and sacrum, (Anton, 2006). Furthermore, certain groups of patient have poor posture stability due to the anatomy of their pelvis. Additional expert advice should also be sought from occupational therapy. Cognition, psychological status: The mood and motivation of patients with anxiety, depression and other psychological health problems will impact on their assistance to change their position. Expert advise and management should be sought from the mental health team. Extremes of Age: The ageing process affects the structure of the skin; firstly the epidermis and dermis become much thinner. Secondly, collagen production is reduced by 1% (Langemo and Brown 2006). Thirdly, the subcutaneous tissue also diminishes, removing the layer of protective padding to the skin. Finally, the skin becomes drier and friable consequently, the skin becomes susceptible to damage. Considerations of the fragile nature of the skin of children should be made. Pressure damage to this patient group usually occurs to the occipital region. Nutrition and Hydration Status: Patients both underweight and overweight are at risk of developing pressure ulcers. Furthermore dehydration, reduced calorie intake and a low serum albumin level affect the ability of the skin to manage pressure, friction and shear (N.I.C.E.2005). Undertaking a nutritional screening assessment identifies those patients who are at risk of malnutrition, (NICE 2006, DoH, 2007) Additional expert advise and management should be sought from the dieticians. Moisture to the Skin: Moisture can be from excessive sweating from pyrexia, urinary incontinence and high levels of wound exudate. Excoriation and maceration of the skin increase the risk of friction. Urine and faeces alters the pH level of the skin (Bale, Cameron, and Meaume 2006). For those patients with incontinence a continence assessment should be completed to assess for appropriate treatment options, measures such as catheterisation/pad usage. Referral to the Urology and Colorectal service maybe indicated should the incontinence be problematic.
The Prevention and Management of Pressure Ulcers in the Community
Page 16 of 24
Appendix 3: Signs to observe when inspecting the skin Blanching erythema: (When light finger pressure is applied to the area of redness on release the skin is white/ pale, then quickly recovers it’s normal colour). Non blanching erythema (When light finger pressure is applied to the area of redness and the skin remains red on the release of the finger pressure, Bliss, 1994) The presence of non- blanching erythema, with or without other skin signs such as heat, oedema, is an indicator that pressure damage will subsequently follow, (Nixon 2007). Therefore it is crucial that the patient who has signs of non- blanching erythema is closely assessed for pressure ulcers developing Purplish/ bluish localised areas: Patients, in particular those with darker skins, will present with a purplish/bluish skin change this will indicate early pressure damage. If the skin becomes pale, this usually suggests lack of blood supply and predisposes to necrosis. Black discolouration is usually due to advanced necrosis (tissue death and dehydration). Blisters are a result of separation of the epidermis and dermis which can then becomes fluid filled. They are commonly associated with friction damage but can be found where significant acute oedema has occurred. Other signs of friction damage may be scuffing of the skin. Temperature changes: Local changes to temperature over the pressure point may indicate damage: localised heat suggests inflammation and may be an early indicator, coldness will indicate lack of blood supply and is associated with early necrosis. Tissue texture :Localised oedema will occur due to the inflammatory changes of early pressure damage this may be felt as induration (hardness). Deep tissue damage which is not visible on the skin may present as induration. If deep tissue damage has been occurring over a long period of time e.g. where internal shearing of tissues has occurred( a patient has been sliding in the bed or chair) and autolysis is taking place, then a collection of fluid may be developing, similar to an abscess. The presence of fluid may be felt through the skin i.e.fluctuant.
The Prevention and Management of Pressure Ulcers in the Community
Page 17 of 24
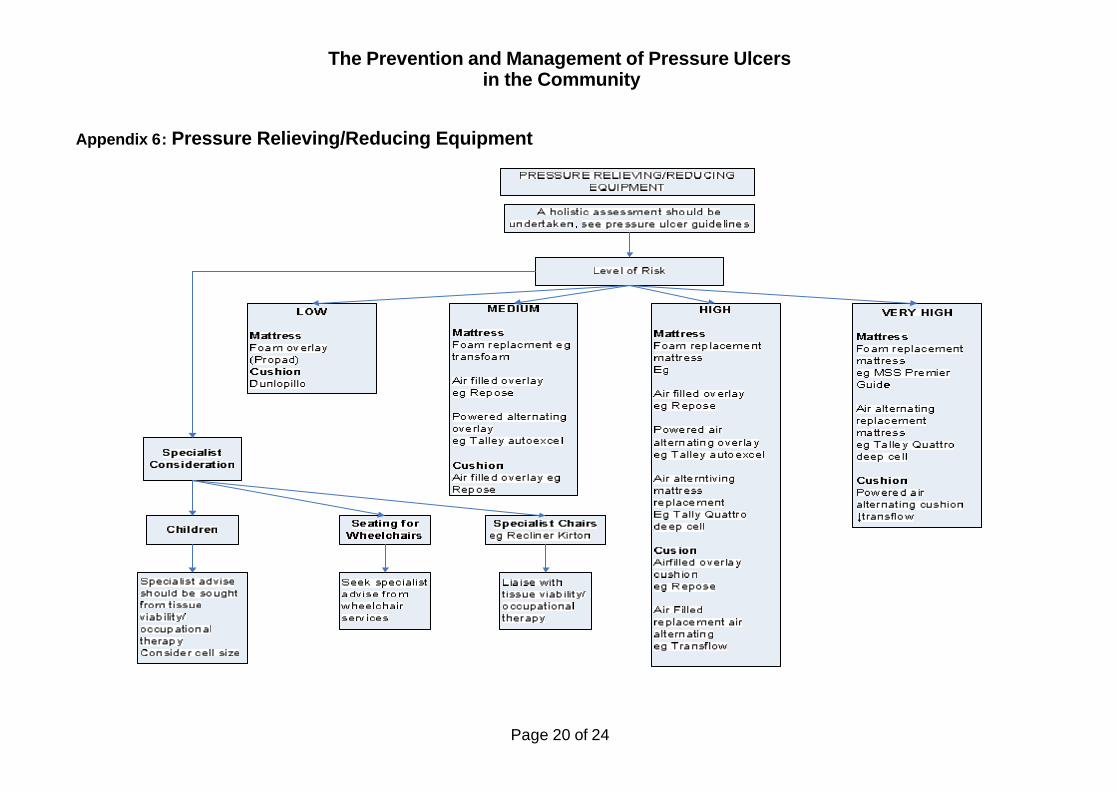
Appendix 4: Equipment Selection NICE (2005) consensus is that no one pressure support system is more superior to another. Therefore the following criteria and clinical judgement must be used. Additionally, the flow chart in appendix 4 for mattress/ equipment selection can be used in conjunction with the LCES, practice guidelines for the provision of equipment. Level of risk, or severity of pressure ulcer: The severity of a pressure ulcer will require more frequent repositioning. Location and cause of pressure ulcer: Determining what has caused the pressure damage, will impact on the choices `made regarding equipment. Availability of carer/ health care professional to reposition the patient: Equipment selection should consider the frequency of both carer and health professional visits. This should include training and knowledge of equipment prescribed. Skin Assessment: The condition of the skin will determine the level of risk the patient has and consequently will determine the type of mattress used. General Health: Certain medical conditions such as breathlessness, neurological conditions, will impact on the equipment used. For example patients with Multiple sclerosis may experience increasing muscle spasm on air alternating systems. Patients with amputations will find soft mattress surfaces affect their balance. Lifestyle and Abilities: The prescribed equipment must compliment the lifestyle of the patient and not restrict. For example enable the patient to sit up to eat their meals, safely. Critical Care: This specifically relates to patients who are at risk of cardiac arrest and are on long term ventilation. Equipment Acceptability and Comfort: Explain to the patient the rationale for equipment, the benefits. Consider patient choice, the noise of air alternating systems is not acceptable to some patients. Certain patients may prefer a hard or a soft mattress. Also consider is there enough space in the patients home. Are there any trailing electrical wires/ leads, carers/ health professionals could trip over. Repose mattresses and cushions are vulnerable, rips and tears can occur when used in environments where cats and smokers are present.
The Prevention and Management of Pressure Ulcers in the Community
Page 18 of 24
Appendix 4: Equipment Selection continued Patients’ Weight : Always check the weight restrictions of each piece of equipment. See the Leeds Equipment Manual for additional guidance Cost Consideration: Specialist equipment, non stock equipment will need justification forms to be completed and advice from the Tissue Viability service Safety: When prescribing equipment always considers the safety implications. Ensure that the mattress or cushion is not too high, increasing the patients’ risk of falling. Pressure relieving mattresses and profiling beds must be compatible, both supplied by same company
An MDA alert informed that there could be potential fatalities if equipment was not compatible.
Risk Assessment: A risk assessment must be completed of the potential safe use of all pressure relieving equipment, and cot sides. This must be clearly documented in the nursing notes.
The Prevention and Management of Pressure Ulcers in the Community
Page 19 of 24
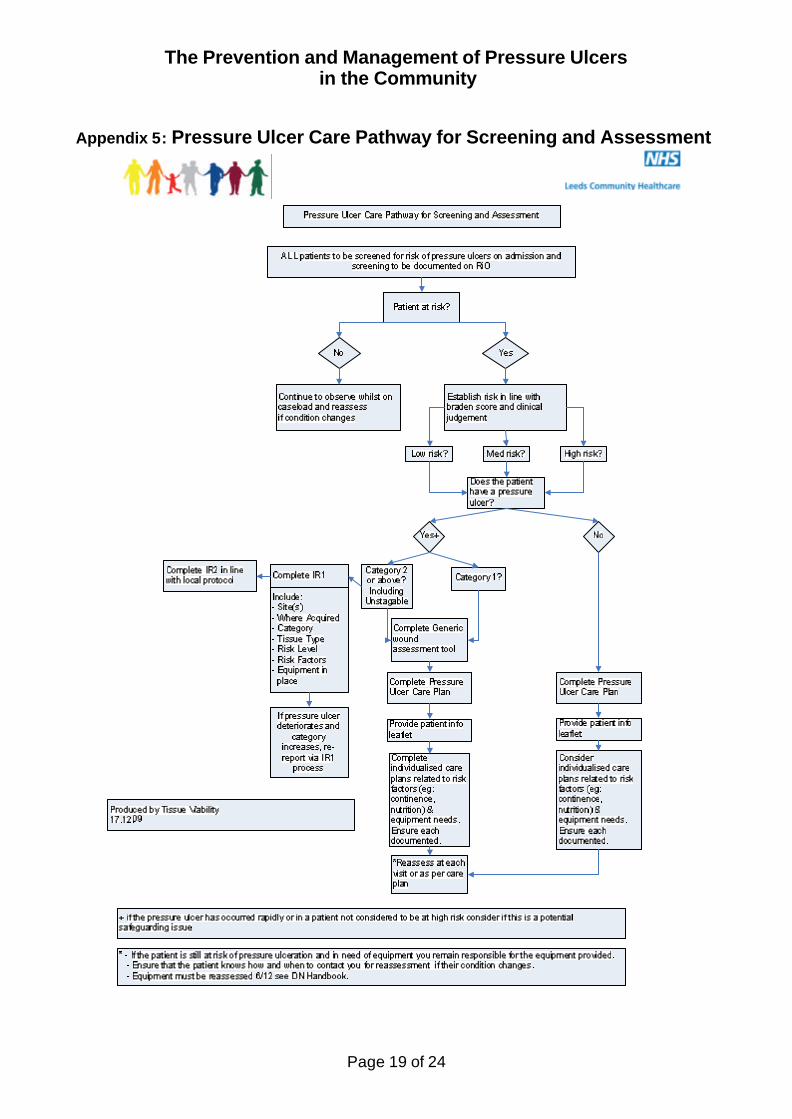
Appendix 5: Pressure Ulcer Care Pathway for Screening and Assessment
The Prevention and Management of Pressure Ulcers in the Community
Page 20 of 24
Appendix 6: Pressure Relieving/Reducing Equipment
The Prevention and Management of Pressure Ulcers in the Community
Page 21 of 24
Appendix 7: NPUAP/EPUAP (2009) Pressure Ulcer Classification System
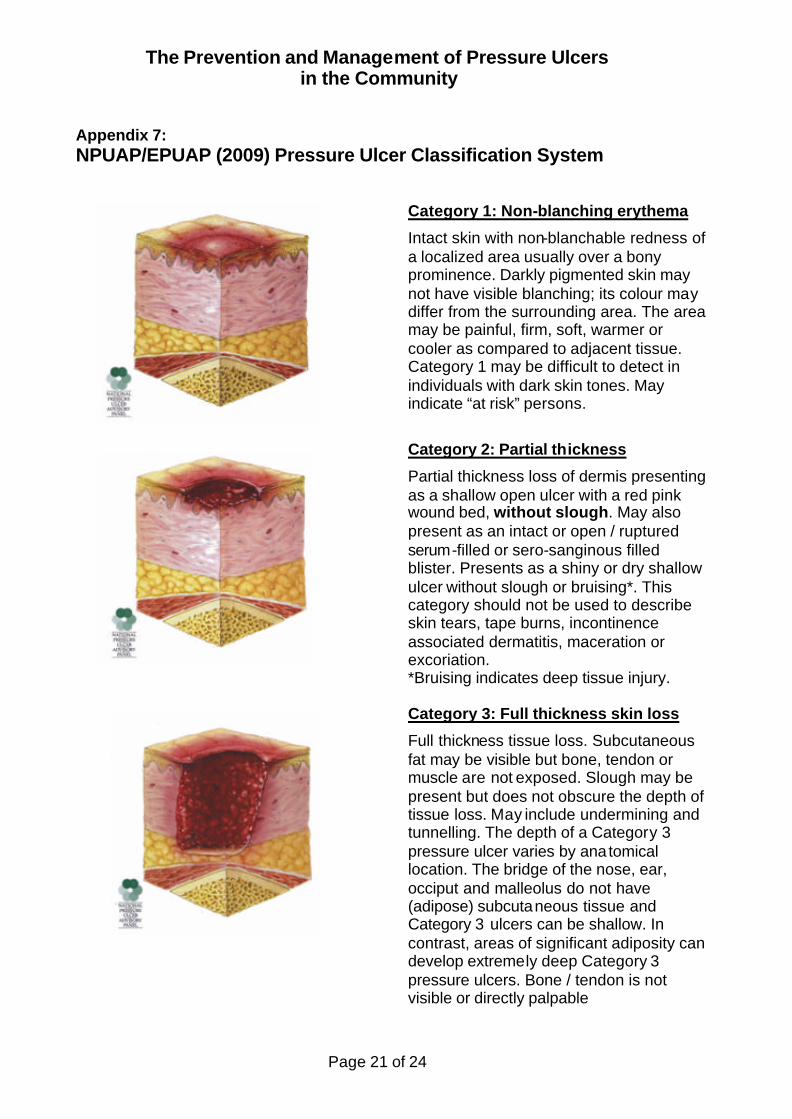
Category 1: Non-blanching erythema
Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its colour may differ from the surrounding area. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Category 1 may be difficult to detect in individuals with dark skin tones. May indicate “at risk” persons.
Category 2: Partial thickness
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open / ruptured serum-filled or sero-sanginous filled blister. Presents as a shiny or dry shallow ulcer without slough or bruising*. This category should not be used to describe skin tears, tape burns, incontinence associated dermatitis, maceration or excoriation. *Bruising indicates deep tissue injury.
Category 3: Full thickness skin loss
Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunnelling. The depth of a Category 3 pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and Category 3 ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep Category 3 pressure ulcers. Bone / tendon is not visible or directly palpable
The Prevention and Management of Pressure Ulcers in the Community
Page 22 of 24
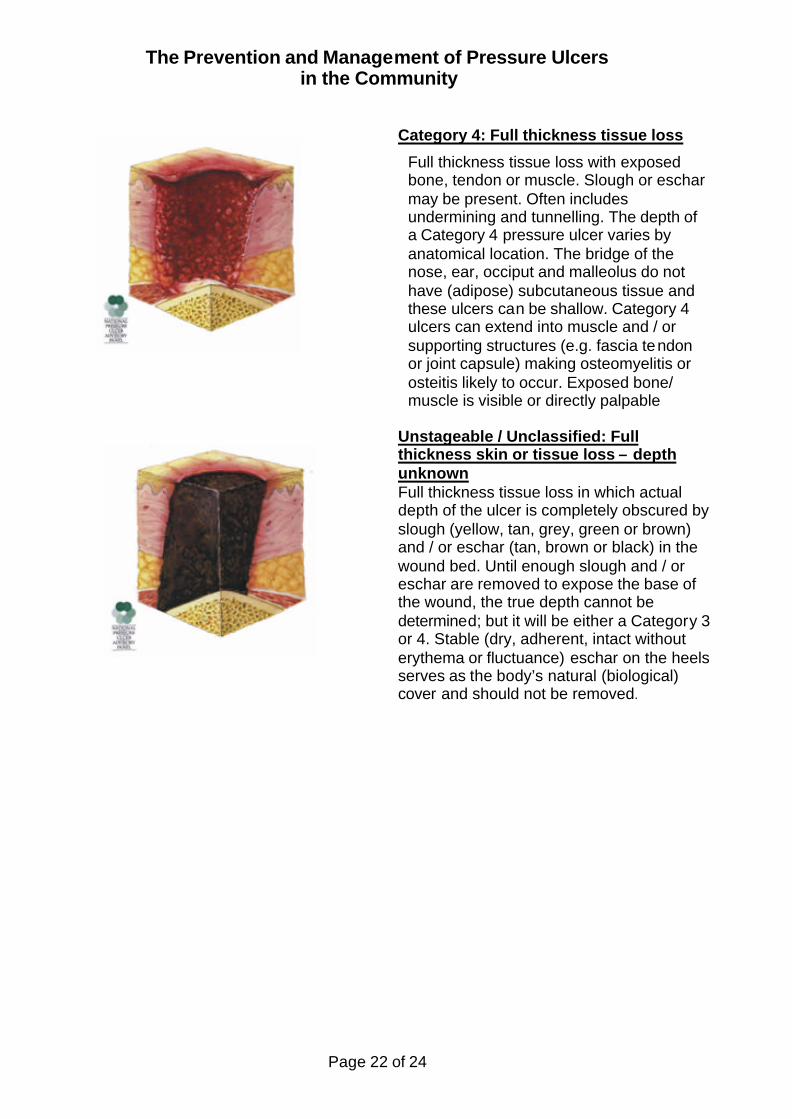
Category 4: Full thickness tissue loss
Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present. Often includes undermining and tunnelling. The depth of a Category 4 pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and these ulcers can be shallow. Category 4 ulcers can extend into muscle and / or supporting structures (e.g. fascia tendon or joint capsule) making osteomyelitis or osteitis likely to occur. Exposed bone/ muscle is visible or directly palpable
Unstageable / Unclassified: Full thickness skin or tissue loss – depth unknown Full thickness tissue loss in which actual depth of the ulcer is completely obscured by slough (yellow, tan, grey, green or brown) and / or eschar (tan, brown or black) in the wound bed. Until enough slough and / or eschar are removed to expose the base of the wound, the true depth cannot be determined; but it will be either a Category 3 or 4. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as the body’s natural (biological) cover and should not be removed.
The Prevention and Management of Pressure Ulcers in the Community
Page 23 of 24
Appendix 8: 30º Tilt Leaflet
The Prevention and Management of Pressure Ulcers in the Community
Page 24 of 24
Clinical Guideline Consultation Process
Title of Document The Prevention and Management of Pressure Ulcers in the Community
Document Type Guideline
New/ Revised Document Revised
If the document is revised what revisions were required and for what reasons e.g. change in medical procedures or change in legislation
NICE made new recommendations in 2005 regarding the prevention and management of pressure ulcers.
Lists of persons involved in developing the policy (names, job titles and organisations)
Jackie Dawson Tissue Viability Nurse Specialist Nikki Stubbs Clinical Team Leader Tissue Viability
List of persons involved in the consultation process
(names, job titles and organisations)
Members of the Tissue Viability Service, NHS Leeds Elizabeth McGinnis, Nurse Consultant Tissue Viability, Leeds Teaching Hospital Trust Citywide Wound Care Group - Bev Cole, Martin Sylvester, Elaine Dickinson, Linzi Bailey, all Staff Nurses Sheila Barnett, Clinical Specialist Occupational Therapist, Continuing Care Team Elaine Lane, Dietitian, Leeds PCT Nicola Cox, Nurse Specialist Community Urology and Colorectal Service Alison Dickinson, NICE Effectiveness Manager Gill Armstrong, Practice and Professional Development Lead for Quality Alex Gordon, District Nurse, Yeadon Health Centre Janet Lee, Deputy Manager, Ghyll Royd House Nursing Home Sheila Hinchcliffe, Manager, Grove Court Care Home Community Matrons, North West wedge Doreen Escolme Clinical Services Manager, Children’s Community Nursing Service Caroline Millward Senior Nurse ICT , East wedge Jan O’Hara, Paediatric Nurse, NHS Leeds Stanley Cutcliffe, Infection Control Nurse Specialist,
List any declarations of interest from commercial sponsors (if applicable)
No input from commercial sponsors.