Embed Size (px)
Citation preview
Prevention and Management of medical emergencies.
ByDr: Waleed A Aabdulaah
Bds, Msc, PhdAssistant professor
of maxilofacial surgery King Saud University
Preparation for medical emergencies
_ Personal continuing education
-- auxiliary staff education
--- establishment and periodic testing of a system to access medical assistance
----equipping office with supplies necessary for emergency care
Basic life support
Abcs:
A: air way
B: breathing
C: circulation
Emergency supplies for the dental office:
-Establishing and maintenance of iv access.
-- high-volume suction
--- drug administration
----Oxygen administration
Hypersensitivity Reactions
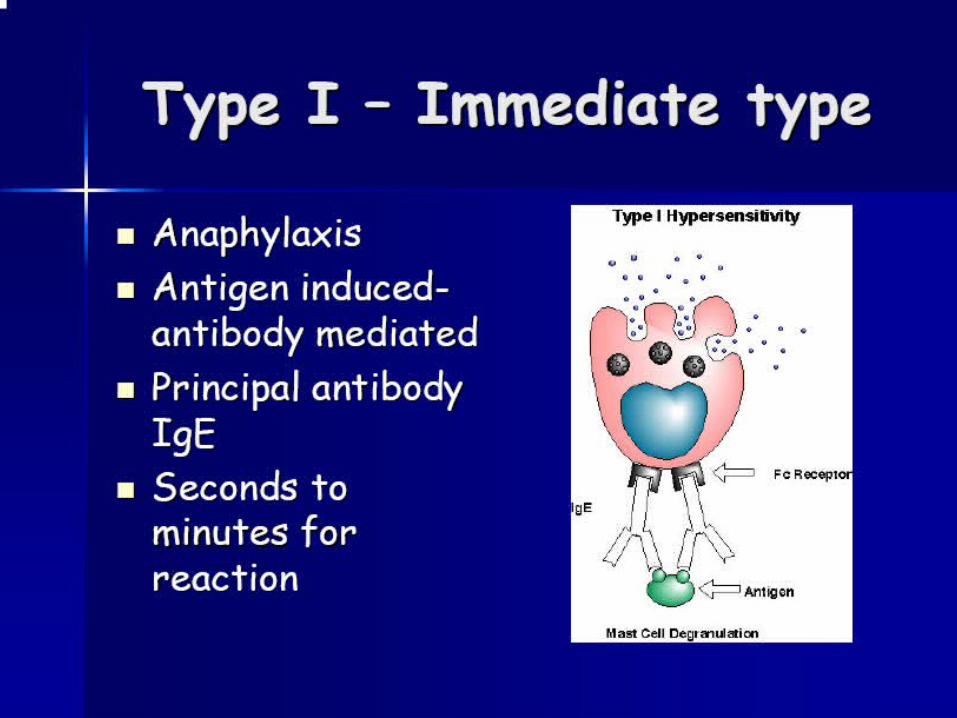
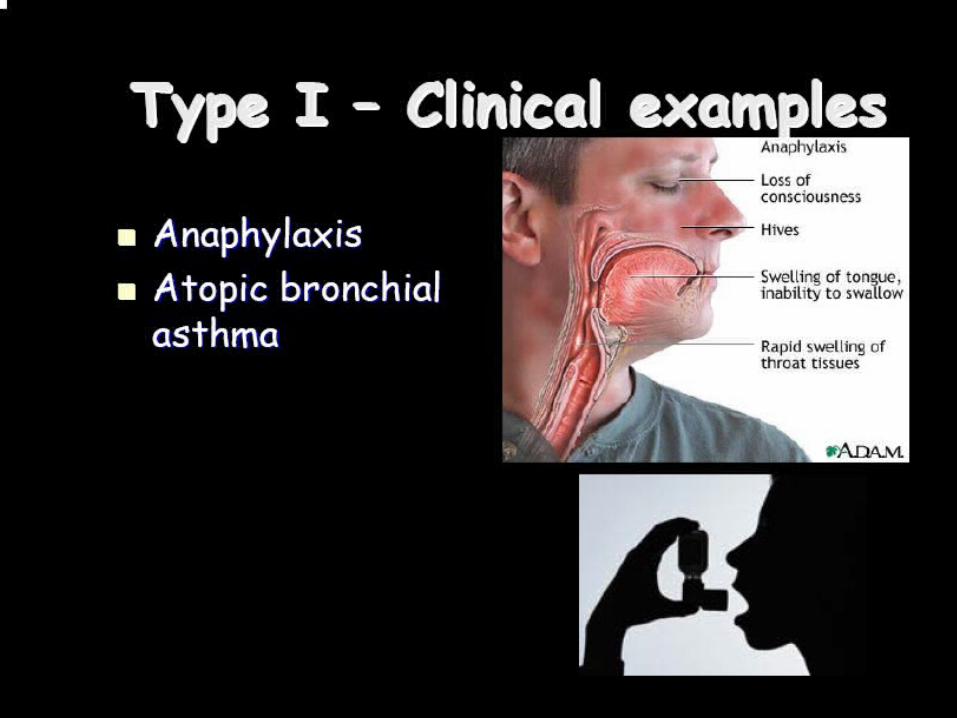
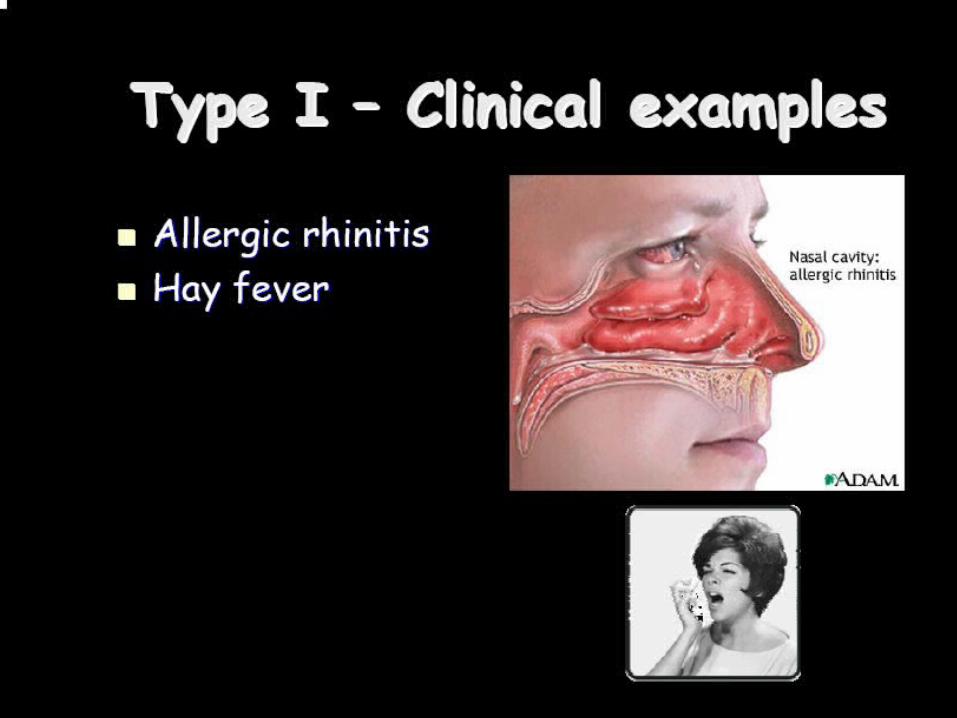
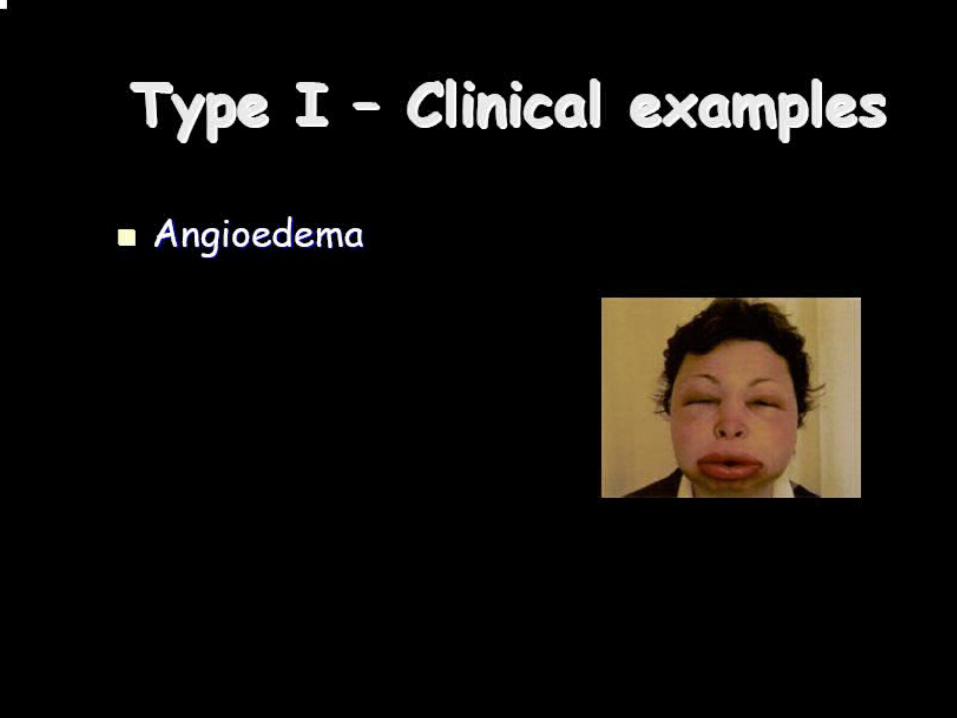
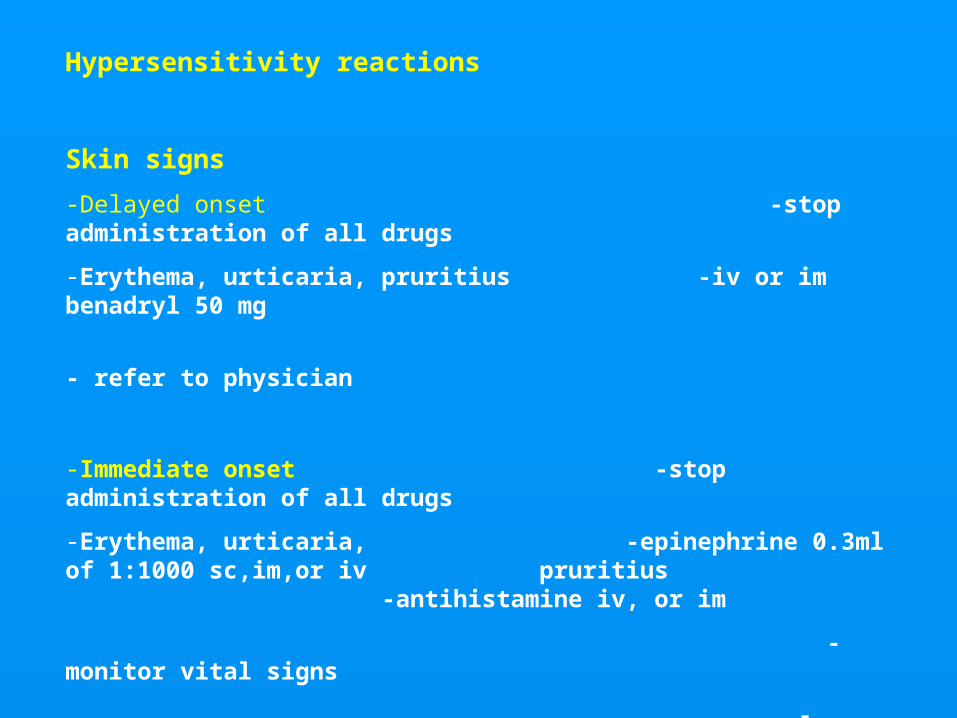
Hypersensitivity reactions
Skin signs
-Delayed onset -stop administration of all drugs
-Erythema, urticaria, pruritius -iv or im benadryl 50 mg
- refer to physician
-Immediate onset -stop administration of all drugs
-Erythema, urticaria, -epinephrine 0.3ml of 1:1000 sc,im,or iv pruritius -antihistamine iv, or im
-monitor vital signs
- consult physician
Respiratory tract signs with or without cardiovascular or skin signs
Wheezing, mild dyspnea -stop administration of all drugs
-place the patient in sitting position
- epinephrine
- iv access
- consult physician or emergency
Stridorous breathing -stop administration of all drugs
Moderate to sever dyspnea -sit thee patient upright
- epinephrine
- oxygen by face mask (6l/m)
-- iv access, monitor vital signs
- antihistaminic
- consult physician
Anaphylaxis ( with or without skin signs)
Malaise, wheezing, moderate to -stop administration of all drugs
Sever dyspnea, cyanosis, total -position patient supine on - floor
air way obstruction, nausea and - epinephrine
vomiting, abdominal cramps, - BLS, and monitoring
tachycardia, hypotension, - cricothyrotomy
Cardiac dysrhythmias, - iv access
Cardiac arrest - oxygen 6 l/m
- antihistaminic im or iv
- prepare for transport


Chest Discomfort
Chest Discomfort
Differential diagnosis of acute onset chest pain:
Common causes:-
CVS: Angina pectoris, MI.
GIT : Gastric ulcers, reflux eosphagitis, dyspepsia.
M SK S: Intercostal muscle spasm, rib or muscle contusion.
Psychogenic: Hyperventilation.
Uncommon causes:-
CVS : Pericarditis.
GIT : Esophageal rupture.
M SK S: Osteocondritis.
RESP S: Pulmonary embolism, pleuritis, mediastinitis, pneumothorax.
Psychogenic: imagined chest pain
Clinical characteristics of chest pain caused by myocardial ischemia or infarction:
Pain or discomfort described by the patient:
1- Squeezing, pressing, burning, choking, or crushing in character
( not typically sharp or stabbing in quality)
2- Substernally located with variable radiation to :
left shoulder, arm, left side, or combination of these areas with neck and mandible..
3- Frequently associated with:
exertion, heavy meal, anxiety, or assuming horizontal position.
4- Relived with vasodilator (nitroglycrin), or rest (as in angina).
5- accompanied by dyspnea, nausea, weakness,, palpitations
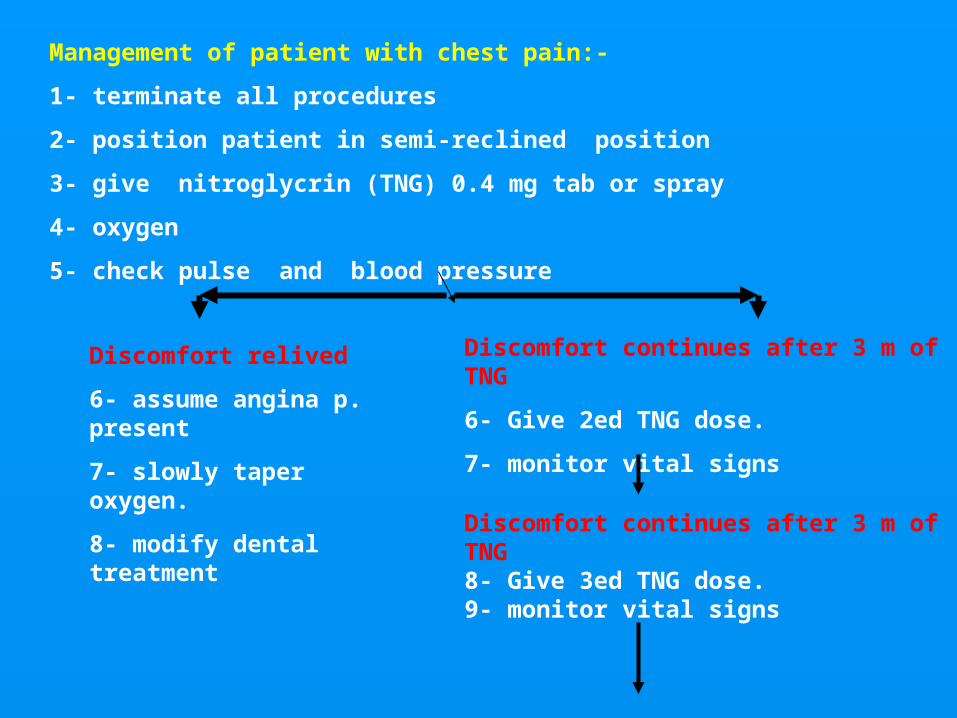
Management of patient with chest pain:-
1- terminate all procedures
2- position patient in semi-reclined position
3- give nitroglycrin (TNG) 0.4 mg tab or spray
4- oxygen
5- check pulse and blood pressure
Discomfort relived
6- assume angina p. present
7- slowly taper oxygen.
8- modify dental treatment
Discomfort continues after 3 m of TNG
6- Give 2ed TNG dose.
7- monitor vital signs
Discomfort continues after 3 m of TNG8- Give 3ed TNG dose.9- monitor vital signs
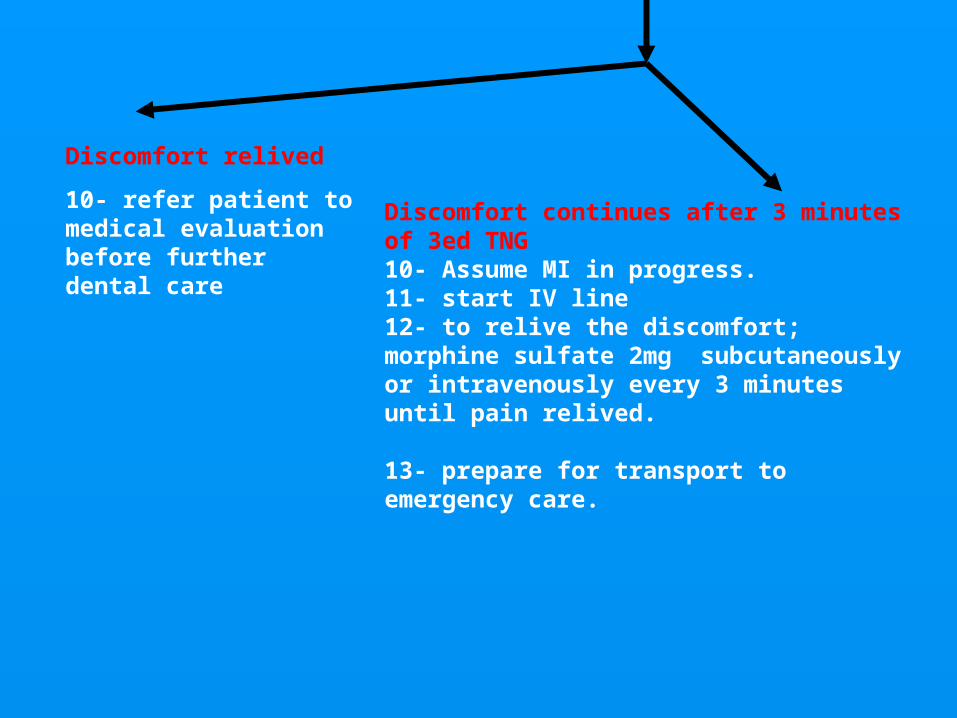
Discomfort relived
10- refer patient to medical evaluation before further dental care
Discomfort continues after 3 minutes of 3ed TNG10- Assume MI in progress.11- start IV line12- to relive the discomfort; morphine sulfate 2mg subcutaneously or intravenously every 3 minutes until pain relived.
13- prepare for transport to emergency care.

Respiratory Difficulty
Respiratory Difficulty:
-Asthma
-Hyperventilation
-Foreign-body aspiration
Manifestations of acute asthmatic episode
Mild to moderate:-WheezingDyspneaTachycardiaCoughingAnxiety
Asthma
Sever:
-Intense dyspnea ( with flaring of the nostrils, and use of accessory muscles of respiration.
-Cyanosis
-Minimal breath sound.
-flushing of the face
-Mental confusion
- prespiration.
Management:
1- terminate the procedures
2- patient in fully sitting position.
3-bronchodilator (isoproterenol).
4- oxygen.
5- monitor vital signs
Relived:
6- STILL monitoring
7- DC IV lines.
8-no dental ttt until consultation.
Not relived:
6- Epinephrine 0.3ml of 1/1000 IM or Sc
7-IV line with crystalloid solution 30ml/h
8-monitor vital signs
Not relived:
9- Theophylline 250 mg IV, and cortisone 100mg IV
10- Prepare for transport to emergency care
Hyperventilation syndrome
Manifestations of hyperventilation syndrome:
Neurologic;
Dizziness
Numbness of fingers, toes, lips
syncope
Respiratory;
Increase rate and depth of breath
Feeling of shortness of breath
Chest pain
xerostomia
Cardiac;
Palpitations, tachycardia
Musculoskeletal;
Myalgia, muscle spasm , tremor, tetany
Psychologic;
anxiety
Management:
1- terminate all procedures’
2-Patient in almost fully upright position.
3-verbally calm the patient
4- patient breath Co2 enriched air, such as in a small bag.
Symptoms persist ;
5-diazebam 10mg IM or slowly IV until anxiety relived.
6- monitor vital sings
7- perform all further dental procedures using anxiety reducing measures
Foreign- body aspiration

Foreign-body aspiration
Manifestations
Large foreign body
-coughing
-choking sensation
-stridorous breathing
-dyspnea
-Feeling something caught in throat
-Inability to breath
-Cyanosis
-Loss of consciousness
Gastric content
-coughing
-stridorous breathing
-wheezing
-tachycardia
-hypotension
-dyspnea
-cyanosis
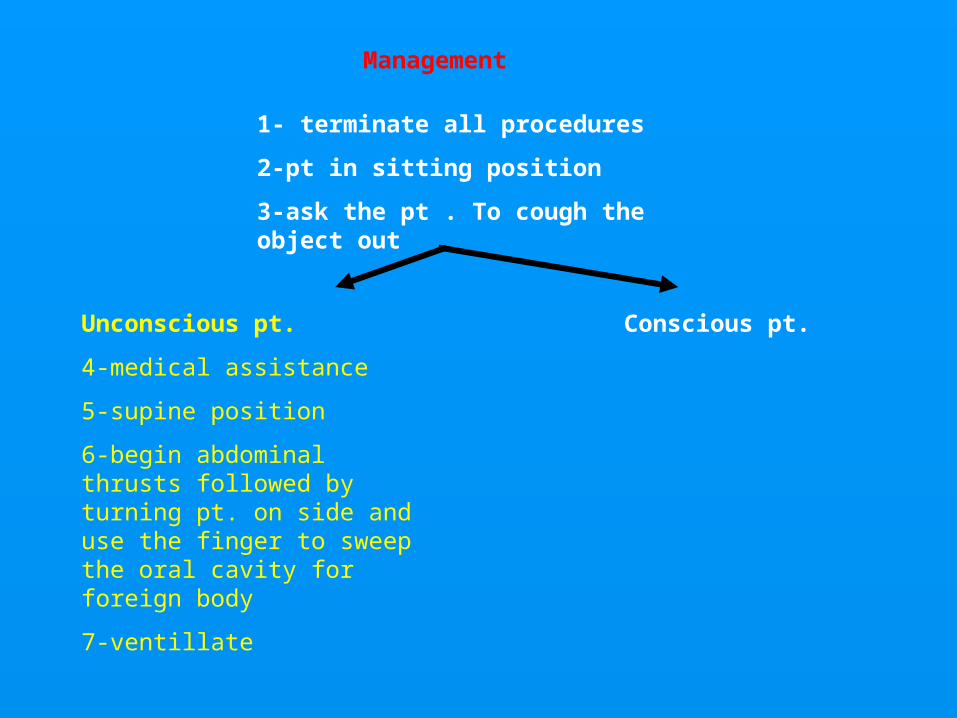
Management
1- terminate all procedures
2-pt in sitting position
3-ask the pt . To cough the object out
Unconscious pt.
4-medical assistance
5-supine position
6-begin abdominal thrusts followed by turning pt. on side and use the finger to sweep the oral cavity for foreign body
7-ventillate
Conscious pt.
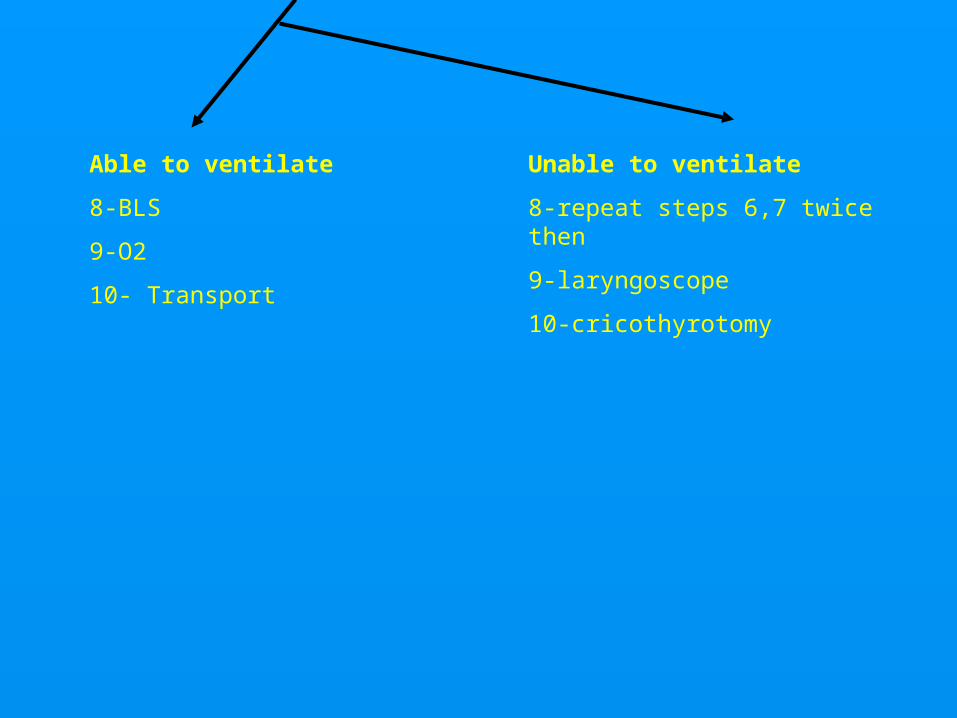
Able to ventilate
8-BLS
9-O2
10- Transport
Unable to ventilate
8-repeat steps 6,7 twice then
9-laryngoscope
10-cricothyrotomy
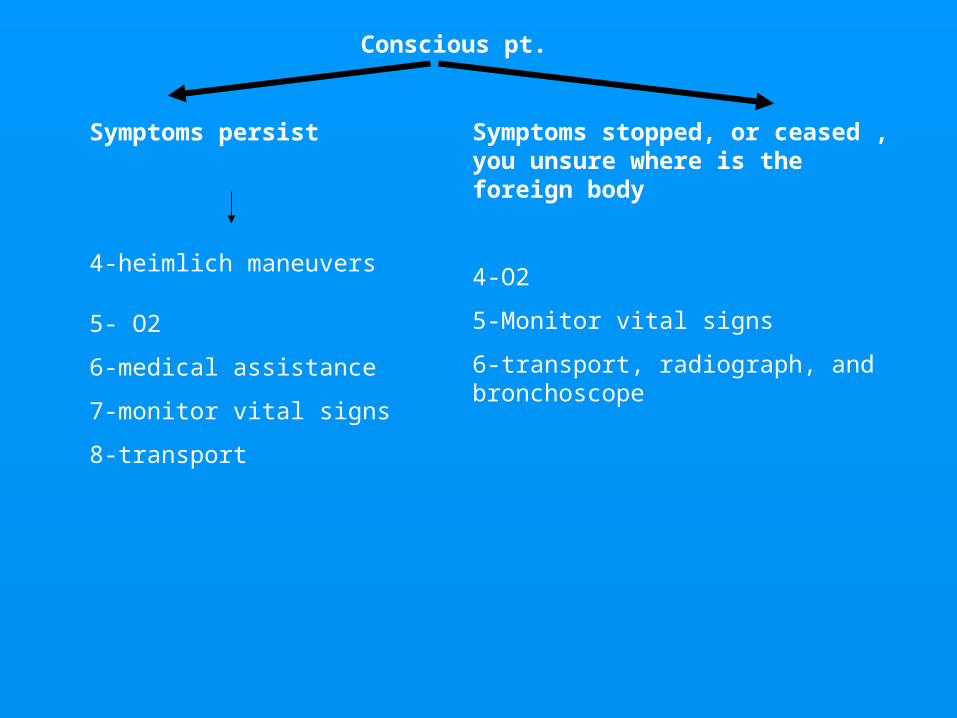
Conscious pt.
Symptoms persist
4-heimlich maneuvers
Symptoms stopped, or ceased , you unsure where is the foreign body
4-O2
5-Monitor vital signs
6-transport, radiograph, and bronchoscope
5- O2
6-medical assistance
7-monitor vital signs
8-transport

Altered Consciousness
Altered consciousness:
Vasovagal syncope.
-Orthostatic hypotension.
-Seizure
-Local anesthetic toxicity
-Diabetes mellitus.
-Thyroid dysfunction
-Adrenal insufficiency
- Cerebrovascular compromise
Vasovagal syncope
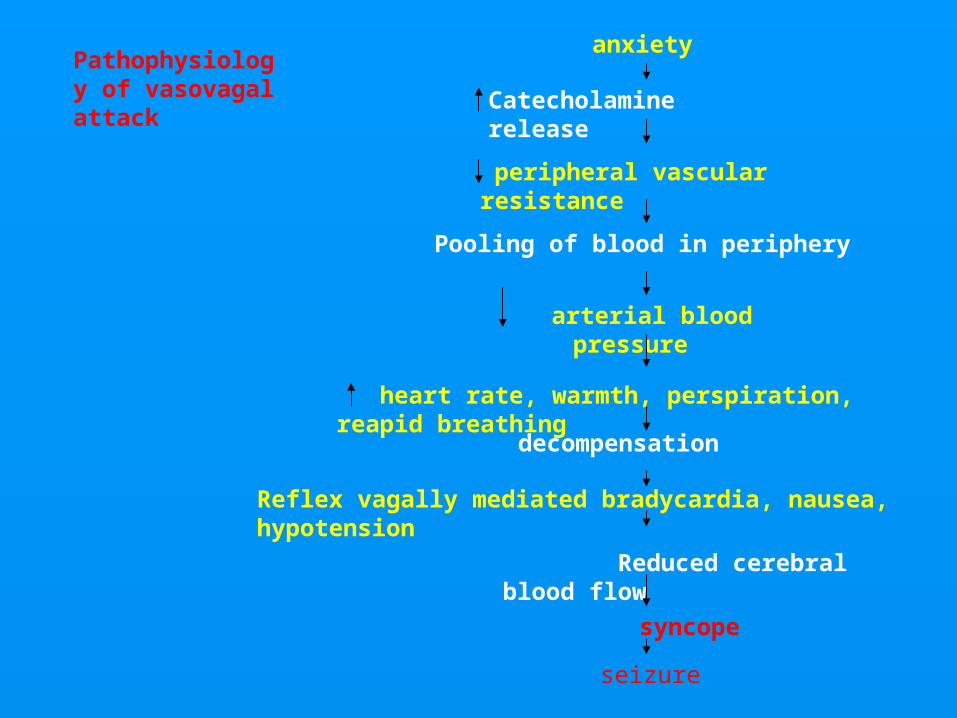
Pathophysiology of vasovagal attack
anxiety
Catecholamine release
peripheral vascular resistance
Pooling of blood in periphery
arterial blood pressure
heart rate, warmth, perspiration, reapid breathing
decompensation
Reflex vagally mediated bradycardia, nausea, hypotension
Reduced cerebral blood flow
syncope
seizure
Management:
Prodrome;
1- terminate all procedures.
2-supine position, legs elevated
3-calm the patient
4-place cool towel on patient forehead
5-monitor vital sings.
Syncope:
1- terminate all procedures
2-supine position and legs elevated.
3-check for breathing
If absent;
4-start basic life support
5- search medical assistance
6-consider other causes of syncope
If present;
4- ammonia under nose
5- O2
6- monitor vital signs
7- anxiety control measures during future dental ttt.
Orthostatic hypotension
Orthostatic hypotension
Management:
1- Terminate all procedures
2- patient in supine position with legs elevated
3-monitor vital ssigns
4-once blood pressure improves, slowly return patient to sitting position.
5-discharge to home once vital sings are normal
6- medical consultation before any future dental treatment.
Seizure
Seizures
Manifestations
(I) Isolated, brief seizure
Tonic-clonic movements of trunk and extremities, loss of consciousness, vomiting, air way obstruction, loss of anal and urinary sphincter control Acute management
1- terminate all dental procedures
2-place in supine possition
3-protect from nearby objects
After seizure
Unconscious pt.
4- medical assistance
5-pt. on side and suction air way
6-monitor vital signs
7-basic life support
8-O2
9-transport to emergency care
Conscious pt.
4-Suction air way
5-monitor vital signs
6-O2
7-consult physician
(II) Repeated or sustained seizures ( status epilepticus)
Acute management;
1- diazepan 5mg/min IV up to 10 mg or midazolam 3mg/min up to 6 mg.
2-medical assistance
3-protect patient from nearby objects
Once seizures ceases;
4- pt. on side, and suction air way.
5-monitor vital signs.
6-Basic life support.
7-O2
8-transport to emergency care.
Local anesthetic toxicity
Local anesthetic toxicity
Manifestations;
Mild toxicity:
talkativeness, anxiety,
slurred speech, confusion
Management;
-Stop administration of local anesthesia
-Monitor all vital signs
-Observe for 1 h
Moderate toxicity;
Stuttering speech, headache,dizziness, blurred vision, drowsiness
Management;-Stop administration of local anesthesia- Supine position-Monitor all vital signs- O2-Observe for 1 h
Sever toxicity;
Seizure, cardiac dysrhythmia or arrest
Management;-supine position-protect from nearby objects-Suction oral cavity if vomiting occur-Medical assistance-Monitor all vital signs-O2- Start IV-DIAZEPAM 5-10 mg slowly or midazolam 2-6 mg-Basic life support-Transport to emergency care
Diabetes Mellitus
Diabetes Mellitus
Manifestations off acute hypoglycemia
Mild
Hunger
Nausea
Mood change
weakness
Moderate
Tachycardia
Prespiration
Pallor
Anxiety
Behavior change;
Confusion
uncooperativness
Sever
Hypotension
Unconsciousness
seizures
Mangement;
Mild hypoglycemia;
-glucose source like sugar or fruit by mouth
-monitor vital signs
-consultation before future dental treatment
MODERATE HYPOGLYCEMIA
-glucose source like sugar or fruit by mouth-monitor vital signs
-If symptoms do not improve, administer 50 ml 50% glucose or 1 mg glucagon IV or IM
- Consultation
Sever hypoglycemia
-50 ml of 50% glucose IV, or IM, or 1mg glucagon
-Medical assistance
-Monitor vital signs
-O2
-Transport to emergency care
Thyroid dysfunction
Thyroid dysfunction
Manifestations
-hyperpyrexia
-tachycardia
-nervousness
-tremor
-weakness
-palpitations
-cardiac dysrhythmias
-nausea and vomiting
-abdominal pains
-Partial or complete loss of conciousness
Management
-Terminate all procedures
-Medical assistance
-O2
-Monitor vital signs
-BLS
-IV line with crystalloid solution
-Transport to medical emergency care
Adrenal insufficiency
Adrenal insufficiency
Manifestations
-weakness
-feeling of extreme fatigue
-confusion
-hypotension
-nausea
-abdominal pain
-myalgias
-partial or total loss of consciousness
Management;
-terminate all procedures
-supine position with legs elevated
-medical assistance
-corticosteroids (100mg of hydrocortisone IM or IV
-O2
-monitor vital signs
-IV line
-BLS
--transport to emergency care
Cerebrovascular compromise
Cerebrovascular compromise
Manifestations;
-headache
-unilateral weakness or paralysis of extremities or facial muscles or both.
-slurring of speech or inability to speak
-difficulty of breathing or swallowing or both
-loss of bladder control
-seizures
-visual disturbance
-dizziness
-partial or total loss of consciousness
Management;
-terminate all procedures
-medical assistance
-supine position with head slightly raised
-monitor all vital signs
-If loss of consciousness; O2, BLS.
-Transport to emergency care
Thank You