Embed Size (px)
Citation preview

Prevention and early diagnosis of frailty and functional decline
Tomasz Kostka Medical University of Lodz, Poland

CONFLICT OF INTEREST DISCLOSURE
I have no potential conflict of interest to report
Tomasz Kostka Medical University of Lodz, Poland

Definitions
Early diagnosis
Prevention
Prof. Tomasz Kostka
EUGMS, Nice, 20-22.09.2017

Definitions
Functional decline
Frailty
Prof. Tomasz Kostka
EUGMS, Nice, 20-22.09.2017
Physical performance (fitness)
1. Cardiorespiratory fitness, cardiorespiratory endurance, aerobic power, aerobic capacity, stamina
2. Muscle strength, power and endurance (muscular fitness)
3. Speed
4. Flexibility, balance…
Body composition (% body fat, BMI, WHR)
Age-related functional decline:
- physiological changes with ageing
- concomitant diseases
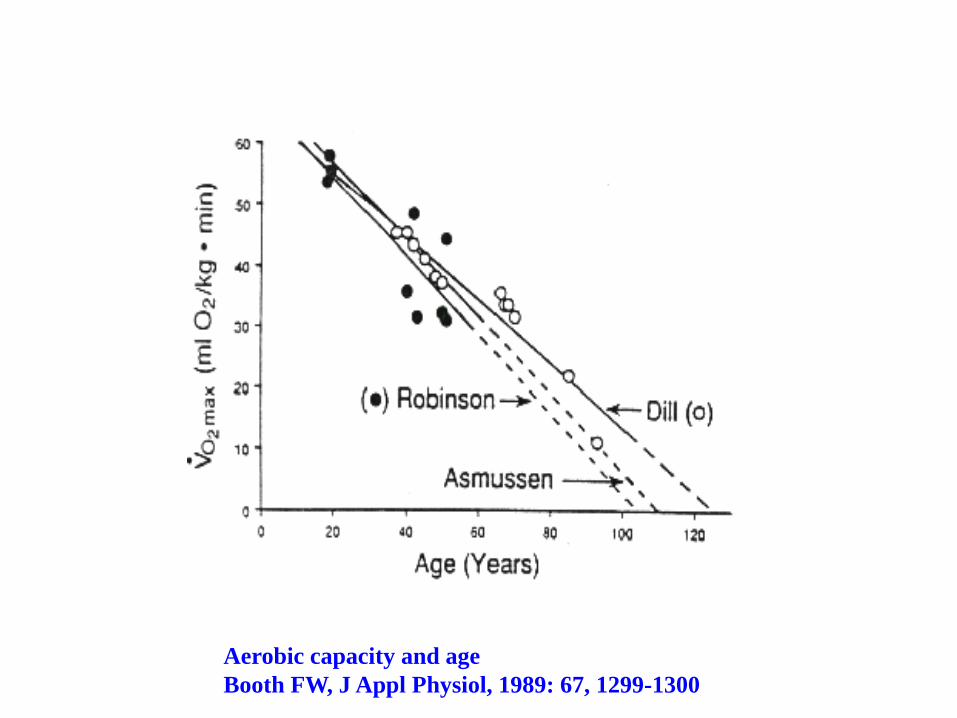
Aerobic capacity and age
Booth FW, J Appl Physiol, 1989: 67, 1299-1300

Handgrip and age in 847 men aged 20-100 years.
Kallman et al., J Gerontol MED SCI 1990: 45, M82-M88.

Age (years)
Pm
ax (
W)
200
400
600
800
1000
1200
20 30 40 50 60 70 80 90
r2 = 54.4 p < 0.001
Kostka T., Eur. J. Appl. Physiol.
2005, 95, 140-145

Velocity (rpm)
Pow
er
(W
)
0
200
400
600
800
20 60 100 140 180
young
old
Bonnefoy et al., Eur. J. Appl.
Physiol. 1998, 77, 182-188

Aerobic power
Anaerobic power
Age
Po
we
r (W
)
20 30 40 50 60 70 80 90
0
200
400
600
800
1000
1200
Kostka et al. Int J Sports Med. 2009

Correlations between functional status variables and muscle
strength, power and nopt
baseline
Quantitative
variable Fext·kg−1 Pmax·kg−1 υopt
ADL
(points)
r=0.08 r=0.41* r=0.27
TUG test (s) r=-0.32 r=-0.66*** r=-0.61***
Tinetti test
(points)
r=0.26 r=0.64*** r=0.55**
6-MWT (m) r=0.32 r=0.76*** r=0.59***
after rehabilitation
Quantitative
variable Fext·kg−1 Pmax·kg−1 υopt
ADL (points) r=0.11 r=0.47* r=0.46*
TUG test (s) r=-0.52** r=-0.83*** r=-0.77***
Tinetti test
(points)
r=0.22 r=0.60** r=0.69***
6-MWT (m) r=0.38* r=0.73*** r=0.71***
Kostka J, Czernicki J, Kostka T: Association of muscle strength, power and optimal shortening velocity
with functional abilities of women with chronic osteoarthritis participating in a multi-modal exercise
program. J Aging Phys Act. 2014 Oct;22(4):564-70.

Major age-related diseases leading
to functional decline and disability
Hypertension, CHD, CHF
Stroke
Diabetes
COPD, asthma
Osteoporosis, osteoarthritis
Dementia. AD, PD
Other…

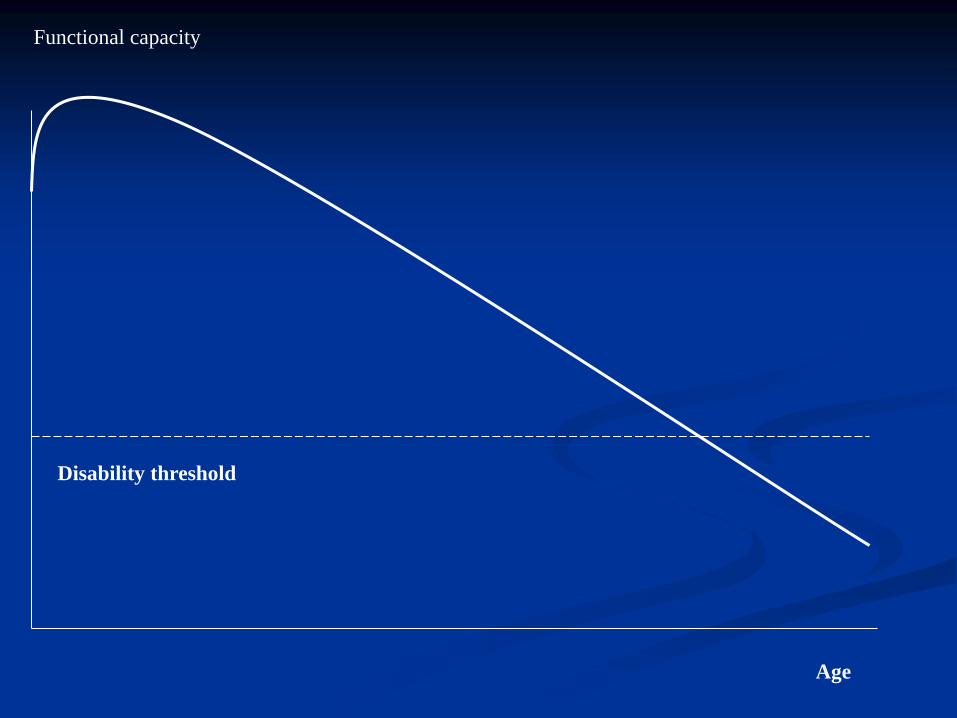
Functional capacity
Age

Functional capacity
Disability threshold
Age
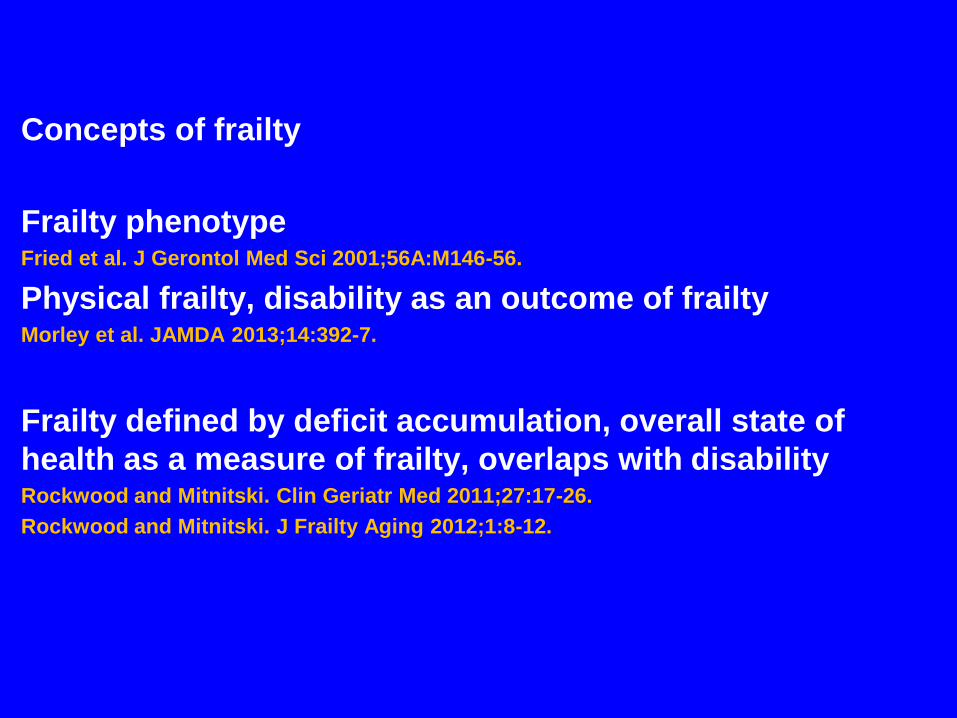
Concepts of frailty
Frailty phenotype Fried et al. J Gerontol Med Sci 2001;56A:M146-56.
Physical frailty, disability as an outcome of frailty Morley et al. JAMDA 2013;14:392-7.
Frailty defined by deficit accumulation, overall state of
health as a measure of frailty, overlaps with disability Rockwood and Mitnitski. Clin Geriatr Med 2011;27:17-26.
Rockwood and Mitnitski. J Frailty Aging 2012;1:8-12.
Sarcopenia as the central biological substrate of physical
frailty
PF & sarcopenia (PF&S) syndrome
Operationalization of the theoretical concept of PF&S
Landi F, Calvani R, Cesari M, et al. Sarcopenia as the biological substrate of physical frailty. Clin
Geriatr Med. 2015;31(3):367–374.
Marzetti E, Calvani R, Cesari M, et al. Operationalization of the physical frailty & sarcopenia
syndrome: rationale and clinical implementation. Translational Medicine @ UniSa. 2015;13:29-32.
Cesari et al. Rationale for a preliminary operational definition of physical frailty and
sarcopenia in the SPRINTT trial. Aging Clin Exp Res. 2017 Feb;29(1):81-88.
Functional capacity
Disability threshold
Age
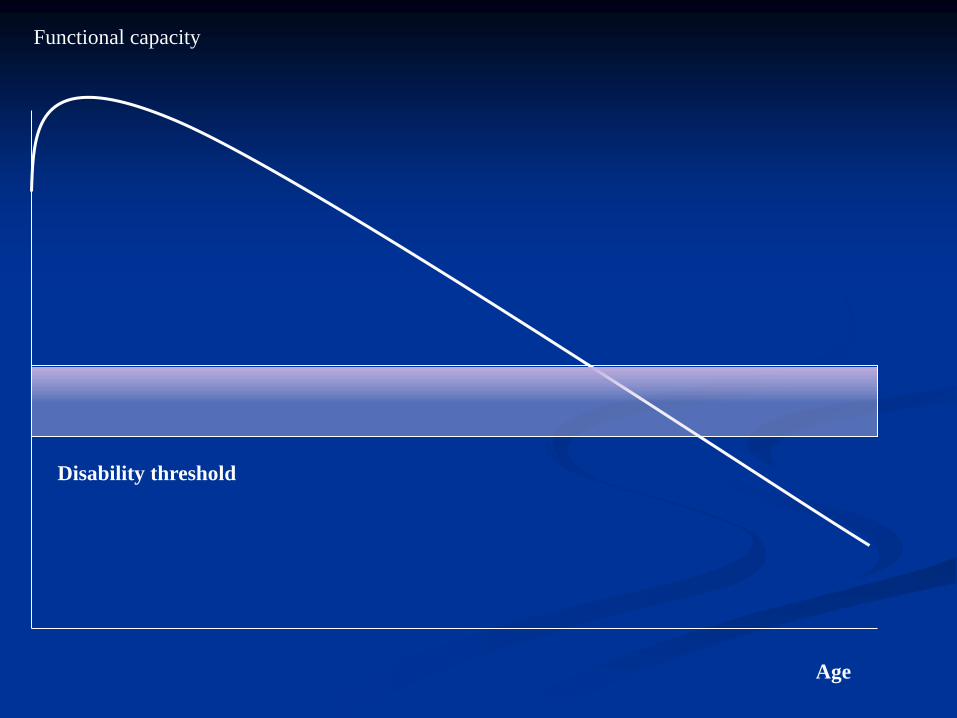
Functional capacity
Disability threshold
Age
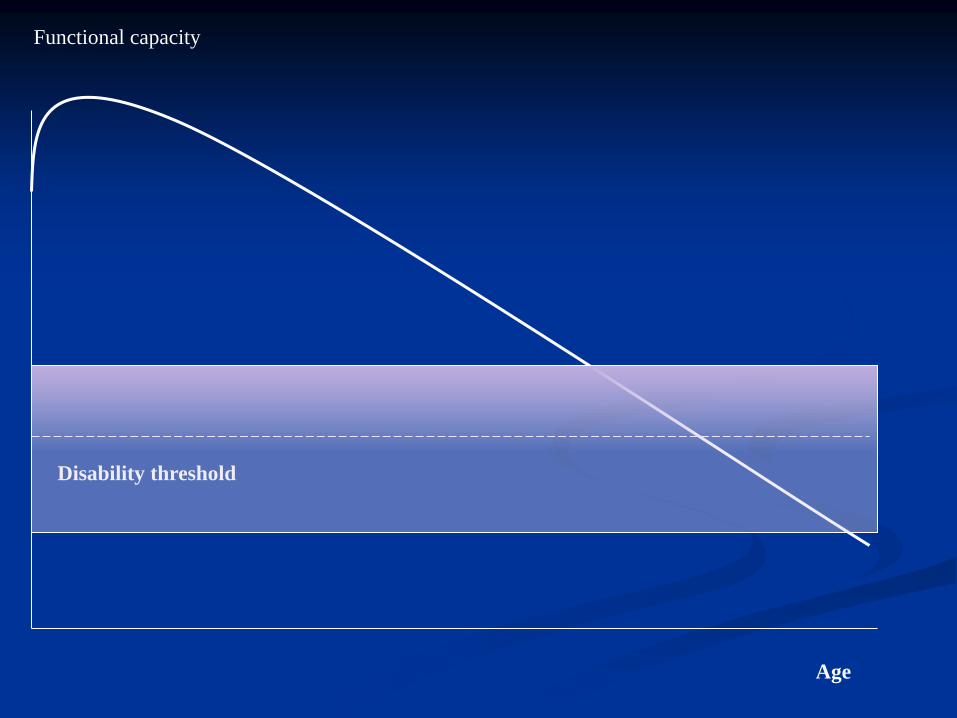
Functional capacity
Disability threshold
Age

Definitions
Early diagnosis
Prevention
Prof. Tomasz Kostka
EUGMS, Nice, 20-22.09.2017

Functional capacity
Disability threshold
Age
Early detection/assessment of:
- physical/biological (at the physiological and molecular level)
- psychological
- sociodemographic
- lifestyle
biomarkers/risk factors/subclinical changes/deficits
is a prerequisite to the primary prevention of frailty

Appendicular lean body mass (ALM) cutpoints (ALM
<19.75kg in men and <15.02kg in women) derived from a large,
diverse sample of older adults identified lean mass thresholds
below which older adults had a higher likelihood of weakness
(defined as grip strength <26kg in men and <16kg in women).
Cawthon et al. Cutpoints for low appendicular lean mass that identify older adults with clinically
significant weakness. J Gerontol A Biol Sci Med. Sci 2014;69(5):567-575.

Cut-points for low grip strength (<26kg men and <16kg women),
low grip strength-to-body mass index (BMI) ratio (<1.00 men and
<0.56 women) and low appendicular lean body mass (ALM)-to-
BMI ratio (<0.789 men and <0.512 women) as candidate criteria
for clinically relevant weakness and low lean mass for incident
mobility impairment (gait speed ≤ 0.8 m/s).
McLean et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal
association with incident mobility impairment and mortality: the foundation for the National
Institutes of Health (FNIH) sarcopenia project. J Gerontol A Biol Sci Med Sci 2014;69(5):576-583.
Established Populations for the Epidemiologic Study of the
Elderly (EPESE) performance battery: tests of balance, time
to walk 8 ft, and time to rise from a chair 5 Times
Performance tests of lower extremity function accurately
predict disability
Both the summary score and the gait speed alone allow for
the estimation of risk of disability
Guralnik et al. Lower extremity function and subsequent disability: consistency across studies,
predictive models, and value of gait speed alone compared with the short physical performance
battery. J Gerontol A Biol Sci Med Sci. 2000 Apr;55(4):M221-31.

A gait speed <0.8m/s; a timed-up-and-go test >10s; and a
score of ≥3 on the PRISMA 7 questionnaire can indicate
frailty.
Turner G, Clegg A; British Geriatrics Society; Age UK; Royal College of General Practitioners. Best
practice guidelines for the management of frailty: a British Geriatrics Society, Age UK and Royal
College of General Practitioners report. Age Ageing. 2014 Nov;43(6):744-7.
Clegg A, Rogers L, Young J. Diagnostic test accuracy of simple instruments for identifying frailty in
community-dwelling older people: a systematic review. Age Ageing. 2015 Jan;44(1):148-52.

Highlights
Frailty tool proliferation (identified 67 frailty instruments) is a
challenge for selecting an assessment instrument.
Instruments most used were frailty phenotype, deficit accumulation
index, and VES-13.
Buta et al. Frailty assessment instruments: Systematic characterization of the uses
and contexts of highly-cited instruments, Ageing Research Reviews 2016; 26: 53-61.

Gender
□M
□F
□ Yes
□ Yes
□ Yes
□ Yes
□ Yes
□ Yes
□ Yes
□ Yes
9. Have you had any financial difficulties in
facing dental care and health care costs
during the last year? □ No
6. Have you experienced memory decline
during the last year? □ No
7. Do you feel lonely most of the time? □ No8. In case of need, can you count on
someone close to you? □ No
3. Your physical state made you walking less
during the last year? □ No4. Have you been evaluated by your GP
during the last year? □ No5. Have you fallen 1 or more times during
the last year? □ No
Questions1. Do you regularly take 5 or more
medications per day? □ No
2. Have you recently lost weight such that
your clothing has become looser? □ Yes □ No
BENEFICIARIES
Age
□75-85
Level of education
□ Low (Without studies,
Primary School)
□Medium (Secondary school,
or vocational degree)
□ High (University, Master or
PhD degree)
□65-74
Professional
□ Nurse □ GPs □ Other Professionals
□ Social Worker □ Community Actor □ Caregiver
QUESTIONNAIRE NUMBER ID
Date and place
PROFESSIONALS
Sunfrail Tool

Kroc Ł, Socha K, Sołtysik BK, Cieślak-Skubel A, Piechocka-Wochniak E, Błaszczak R, Kostka T: Validation of the
Vulnerable Elders Survey-13 (VES-13) in hospitalized geriatric patients. Eur Geriatr Med 2016; 7: 449-453.
The quickly and easily administered MNA-SF appears
to be a good tool for predicting both under-nutrition and
frailty in elderly hospitalised people.
Dent et al. Use of the Mini Nutritional Assessment to detect frailty in hospitalised older
people. J Nutr Health Aging. 2012;16(9):764-7.

Risk factors/biomarkers of frailty
Routine blood tests and standard physical measures (blood pressure) Rockwood et al.JAMDA 2015;16:842-7.
Routine blood and urine tests
Ritt et al. Clin Interv Aging 2017;12:1029-40.
Higher TSH in men and lower TSH in women aged≥65 years Veronese et al. Rejuvenation Res 2017;20:3.
Routine blood and special blood tests (eg, DNA) Mitnitski et al. BMC Med 2015;13:161.
“Omics”-based laboratory biomarkers Rodrígues-Mañas L. JFA 2015;4:125-8.
673 significant differentially expressed genes
(128 upregulated and 545 downregulated)
in sarcopenia patients of over 60 years of age.
Most of the upregulated genes were involved in metabolic
processes.
Jeong et al. DETERMINATION OF THE MECHANISMS THAT CAUSE SARCOPENIA
THROUGH cDNA MICROARRAY. J Frailty Aging 2017;6(2):97-102.

The pooled OR of frailty for the lowest versus the
highest level of vitamin D was 1.27 (95% CI=1.17-1.38,
I(2)=59%), suggesting that low level of vitamin D was
significantly associated with the risk of frailty.
Zhou et al. Association of vitamin D deficiency and frailty: A systematic review and
meta-analysis. Maturitas. 2016 Dec;94:70-76.
After adjusting for BMI, the relationship of 25(OH)D < 10
ng/mL (vs ≥30 ng/mL) with incident frailty persisted, but
was attenuated after further accounting for
cardiometabolic diseases.
Buta et al. The Association of Vitamin D Deficiency and Incident Frailty in Older
Women: The Role of Cardiometabolic Diseases. J Am Geriatr Soc. 2017
Mar;65(3):619-624.
"inflamm-aging"
High levels of interleukin (IL)-6, IL-1, tumor necrosis
factor-α, and C-reactive protein are associated in the older
subject with increased risk of morbidity and mortality.
The low-grade inflammation characterizing the aging
process notably concurs at the pathophysiological mechanisms
underlying sarcopenia.
Michaud et al. Proinflammatory cytokines, aging, and age-related diseases. J Am Med Dir
Assoc. 2013 Dec;14(12):877-82.

Higher serum levels of anti-inflammatory markers,
and in particular IL-4 and IL-13, may play a protective role
on FFM and performance maintenance in elderly subjects.
Rossi et al. Role of Anti-Inflammatory Cytokines on Muscle Mass and Performance Changes in Elderly
Men and Women. J Frailty Aging. 2017;6(2):65-71.
Frail subjects have lower levels of serum IGF-I and DHEA-S and
higher levels of IL-6 than do non-frail, age-matched individuals.
Leng SX, Cappola AR, Andersen RE, et al. Serum levels of insulin-like growth factor 1 (IGF-1) and
dehydroepiandrosterone sulfate (DHEAS), and their relationships with serum interleukin-6, in the geriatric
syndrome of frailty. Aging Clin Exp Res 2004; 16:153–157.
Higher baseline levels of differential white cell counts (WCC), lower
levels of dehydroepiandosterone sulphate (DHEAS) and higher
cortisol:DHEAS ratio were all significantly associated with increased
odds of frailty at 10-year follow-up.
Baylis et al. Immune-endocrine biomarkers as predictors of frailty and mortality: a 10-year
longitudinal study in community-dwelling older people. Age (Dordr). 2013 Jun;35(3):963-
71.
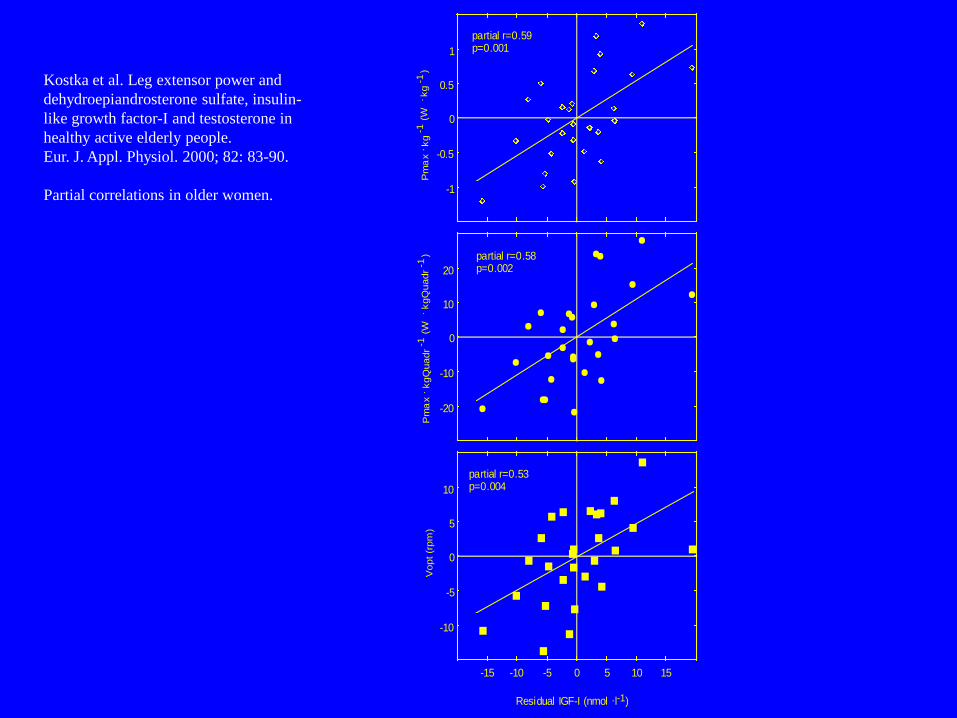
Residual IGF-I (nmol .l-1)
-20
-10
0
10
20
-1
-0.5
0
0.5
1
-10
-5
0
5
10
-15 -10 -5 0 5 10 15
partial r=0.59 p=0.001
partial r=0.58 p=0.002
partial r=0.53 p=0.004
Pm
ax .
kg
-1 (W
. kg
-1)
Pm
ax .
kgQ
uadr
-1 (W
. kgQ
uadr
-1)
Vopt (r
pm
)
Kostka et al. Leg extensor power and
dehydroepiandrosterone sulfate, insulin-
like growth factor-I and testosterone in
healthy active elderly people.
Eur. J. Appl. Physiol. 2000; 82: 83-90.
Partial correlations in older women.

-10
-5
0
5
10
-1.51 -0.58 0 0.58 1.51
-20
-10
0
10
20
-1
-0.5
0
0.5
1
Residual DHEAS ( mol.l-1)
partial r=0.54 p=0.003
partial r=0.58 p=0.002
partial r=0.34 p=0.08
Vop
t (r
pm
)P
max .
kgQ
uad
r-1
(W
. kgQ
uad
r-1
)P
max .
kg
-1 (W
. kg
-1)
Kostka et al. Leg extensor power and
dehydroepiandrosterone sulfate, insulin-
like growth factor-I and testosterone in
healthy active elderly people.
Eur. J. Appl. Physiol. 2000; 82: 83-90.
Partial correlations in older women.
Higher serum IGF-1 was independently associated with
more muscle mass, higher BMD, and better handgrip
performance in both genders.
Chen et al. Association Among Serum Insulin-Like Growth Factor-1, Frailty, Muscle Mass,
Bone Mineral Density, and Physical Performance Among Community-Dwelling Middle-Aged
and Older Adults in Taiwan. Rejuvenation Res. 2017 May 9. doi: 10.1089/rej.2016.1882.

Schwenk et al. Frailty and Technology: A Systematic Review of Gait Analysis in
Those with Frailty. Gerontology 2014;60:79-89.
Greene et al. Frailty status can be accurately assessed using inertial sensors and the
TUG test. Age and Ageing 2014; 43:406–11.
Martinez-Ramirez A, Martinikorena I, Gomez M, Lecumberri P, Millor N,
Rodriguez-Manas L et al (2015) Frailty assessment based on trunk kinematic
parameters during walking. J Neuroeng Rehabil 12:48.
Mohler MJ, Wendel CS, Taylor-Piliae RE, Toosizadeh N, Najafi B (2016) Motor
performance and physical activity as predictors of prospective falls in community-
dwelling older adults by frailty level: application of wearable technology.
Gerontology 2016;62: 654-64.
Dasenbrock et al. Technology-based measurements for screening, monitoring and
preventing frailty. Z Gerontol Geriatr. 2016;49:581-95.
Definitions
Early diagnosis
Prevention
Prof. Tomasz Kostka
EUGMS, Nice, 20-22.09.2017

Lifelong prevention
Midlife prevention
of age-related functional decline
Prof. dr hab. med. Tomasz Kostka
EUGMS, Nice, 20-22.09.2017
Prevention of frailty and functional decline:
1. Physical activity
2. Nutrition
3. Prevention and treatment of concomitant disorders
Prevention of frailty and functional decline:
1. Physical activity
2. Nutrition
3. Prevention and treatment of concomitant disorders
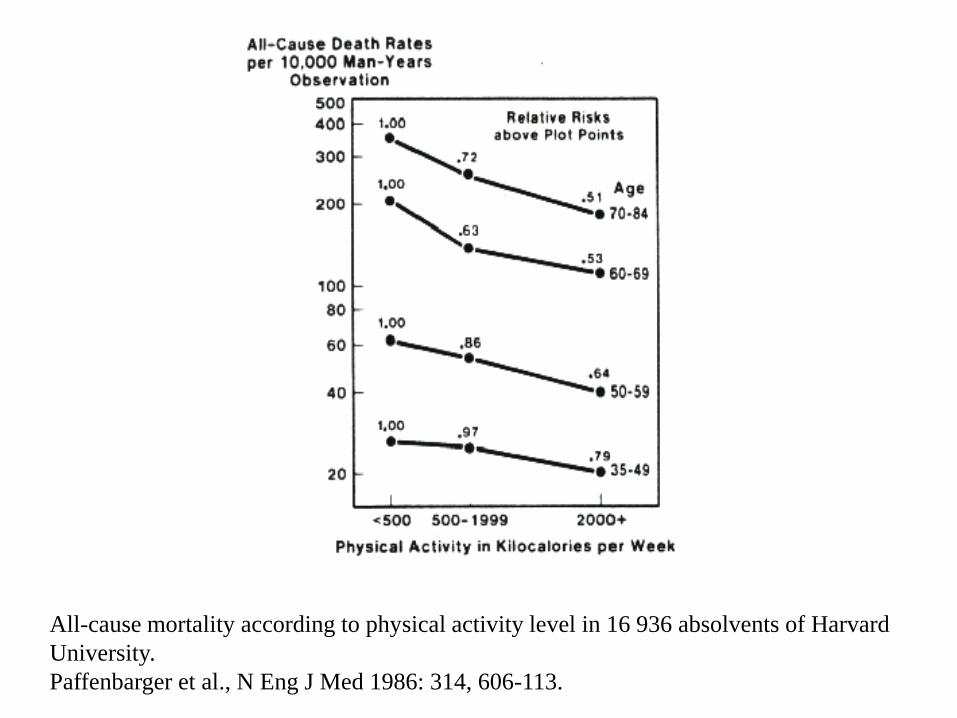
All-cause mortality according to physical activity level in 16 936 absolvents of Harvard
University.
Paffenbarger et al., N Eng J Med 1986: 314, 606-113.

Pahor et al. Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE Study randomized clinical
trial. JAMA. 2014;311(23):2387-2396.

1. The WHO guidelines for promoting physical
activity among older persons. J. Aging Phys.
Activity 5:1-8, 1997.
2. American College of Sports Medicine position
stand. Exercise and physical activity for older
adults. Med. Sci. Sports Exerc. 30:992-1008, 1998.
3. King, A. C., W. J. Rejeski, and D. M. Buchner.
Physical activity interventions targeting older
adults: a critical review and recommendations. Am.
J. Prev. Med. 15:316-333, 1998.
4. Evans, W. J. Exercise training guidelines for the
elderly. Med. Sci. Sports Exerc. 31:12-17, 1999.

Physical Activity and Public Health in Older Adults
Recommendation From the American College of Sports Medicine and the American Heart Association
Miriam E. Nelson, PhD, FACSM; W. Jack Rejeski, PhD; Steven N. Blair, PED, FACSM, FAHA; Pamela W. Duncan, PhD; James O. Judge, MD; Abby C. King, PhD, FACSM, FAHA; Carol A. Macera, PhD, FACSM; Carmen Castaneda-Sceppa, MD, PhD
Circulation 2007;116;1094-1105; originally published online Aug 1, 2007;
WHO 2010
Recommended levels
of physical activity for health
for 65 years old and above

Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults.Med Sci Sports Exerc. 2009 Jul;41(7):1510-30
Summary of ACSM/AHA physical activity recommendations for older adults.
Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults.Med Sci Sports Exerc. 2009 Jul;41(7):1510-30
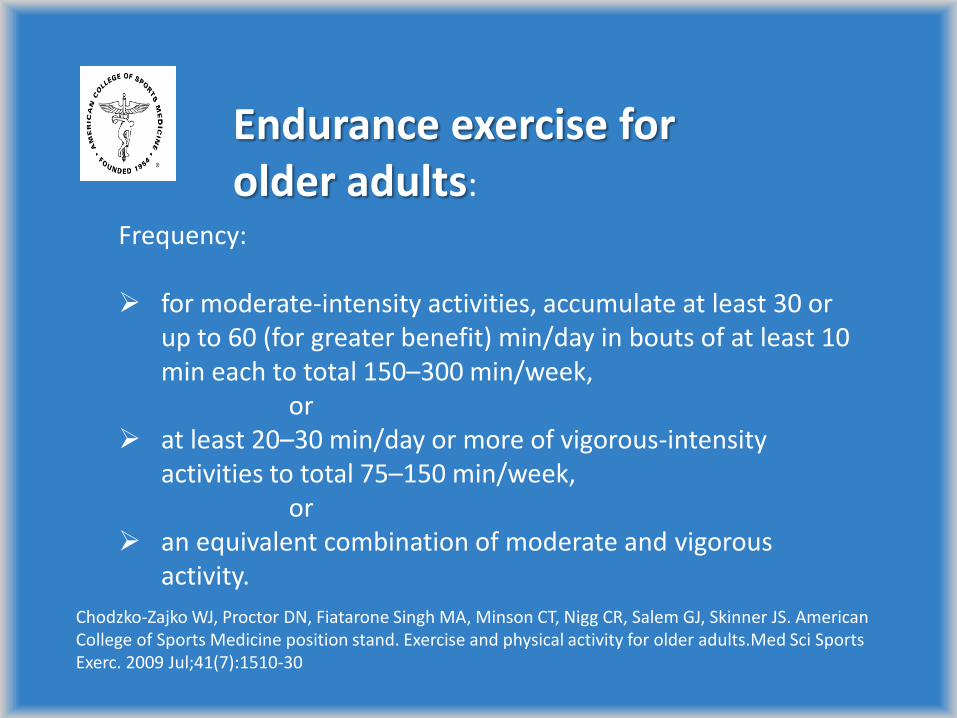
Endurance exercise for older adults:
Frequency: for moderate-intensity activities, accumulate at least 30 or
up to 60 (for greater benefit) min/day in bouts of at least 10 min each to total 150–300 min/week,
or at least 20–30 min/day or more of vigorous-intensity
activities to total 75–150 min/week, or an equivalent combination of moderate and vigorous
activity.

Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults.Med Sci Sports Exerc. 2009 Jul;41(7):1510-30
Frequency: At least 2 days/week Intensity: Between moderate- (5–6) and vigorous- (7–8) intensity on a scale of 0 to 10 Type: Progressive weight training program or weight bearing calisthenics (8–10 exercises involving the major muscle groups of 8–12 repetitions each), stair climbing, and other strengthening activities that use the major muscle groups
Resistance exercise for older adults

Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults.Med Sci Sports Exerc. 2009 Jul;41(7):1510-30
Frequency: At least 2 days/week Intensity: Moderate (5–6) intensity on a scale of 0 to 10 Type: Any activities that maintain or increase flexibility using sustained stretches for each major muscle group and static rather than ballistic movements.
Flexibility exercise for older adults:
Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults.Med Sci Sports Exerc. 2009 Jul;41(7):1510-30
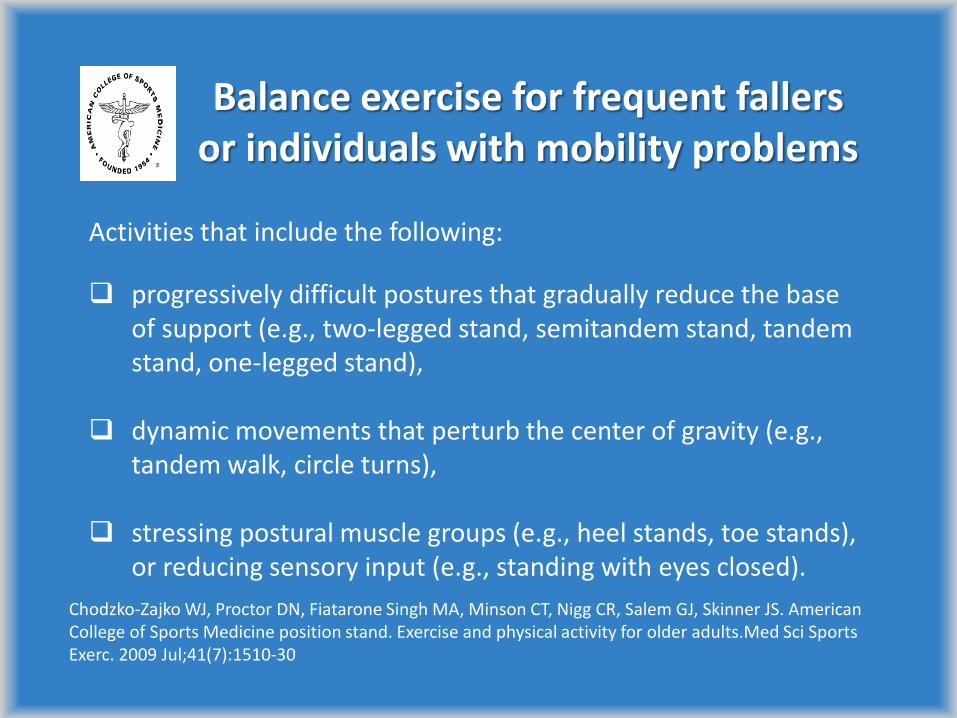
Activities that include the following:
progressively difficult postures that gradually reduce the base of support (e.g., two-legged stand, semitandem stand, tandem stand, one-legged stand),
dynamic movements that perturb the center of gravity (e.g.,
tandem walk, circle turns),
stressing postural muscle groups (e.g., heel stands, toe stands), or reducing sensory input (e.g., standing with eyes closed).
Balance exercise for frequent fallers or individuals with mobility problems
American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009 Mar;41(3):687-708.
There is support for the inclusion of power training for the healthy older adult. Muscle atrophy results from fiber denervation with loss of some fibers and atrophy of others, that is, especially fast twitch, with aging and inactivity. Age-related muscle atrophy is associated with reductions in strength and power, and reductions in power exceed decreases in maximal strength. Although most studies in the elderly examined heavy RT programs, power training may optimize functional abilities…
Physical exercise has beneficial effects for frail elderly on gait
speed, physical functioning, mobility, falls, functional abilities,
muscle strength, body composition, and frailty.
Gine-Garriga et al. Physical exercise interventions for improving performance-based
measures of physical function in community-dwelling, frail older adults: a systematic review
and meta-analysis. Arch Phys Med Rehabil. 2014;95(4):753.e3–769.e3.
de Labra et al. Effects of physical exercise interventions in frail older adults: a systematic
review of randomized controlled trials. BMC Geriatr. 2015;15:154.

The multi-component exercise intervention composed by strength,
endurance and balance training seems to be the best strategy to improve
rate of falls, gait ability, balance, and strength performance in physically
frail older adults.
Cadore et al. Effects of different exercise interventions on risk of falls, gait ability,
and balance in physically frail older adults: a systematic review. Rejuvenation Res.
2013;16:105-14.
Routine multicomponent exercise intervention should be prescribed to
nonagenarians because overall physical outcomes are improved in this
population.
Cadore et al. Multicomponent exercises including muscle power training enhance
muscle mass, power output, and functional outcomes in institutionalized frail
nonagenarians. Age (Dordr). 2014 Apr;36(2):773-85.

Gardening as the dominant leisure time physical activity (LTPA) of older adults from
a post-communist country. The results of the population-based PolSenior Project
from Poland Rafal Rowinski a, Andrzej Dabrowski b, Tomasz Kostka c,
a Faculty of Physical Education, Jozef Pilsudski University of Physical Education in Warsaw, Marymoncka 34, Warsaw, Poland
b Faculty of Physical Education and Sport in Biala Podlaska, Jozef Pilsudski University of Physical Education in Warsaw, Marymoncka 34, Warsaw, Poland
c Department of Geriatrics, Medical University of Lodz, Pl. Hallera 1, Lodz, Poland
Corresponding author at: Department of Geriatrics, Medical University of Lodz, Pl. Hallera 1, Lodz, Poland. Tel.: +48 42 639 3215; fax: +48 42 639 3218. [email protected]
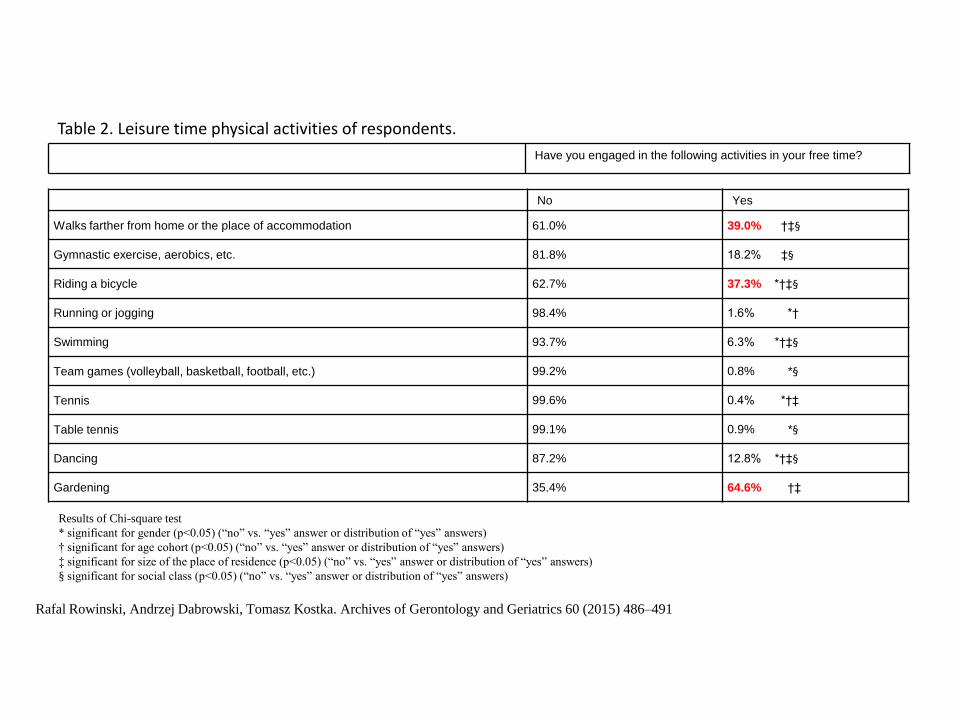
Table 2. Leisure time physical activities of respondents. Have you engaged in the following activities in your free time?
No Yes
Walks farther from home or the place of accommodation 61.0% 39.0% †‡§
Gymnastic exercise, aerobics, etc. 81.8% 18.2% ‡§
Riding a bicycle 62.7% 37.3% *†‡§
Running or jogging 98.4% 1.6% *†
Swimming 93.7% 6.3% *†‡§
Team games (volleyball, basketball, football, etc.) 99.2% 0.8% *§
Tennis 99.6% 0.4% *†‡
Table tennis 99.1% 0.9% *§
Dancing 87.2% 12.8% *†‡§
Gardening 35.4% 64.6% †‡
Results of Chi-square test
* significant for gender (p<0.05) (“no” vs. “yes” answer or distribution of “yes” answers)
† significant for age cohort (p<0.05) (“no” vs. “yes” answer or distribution of “yes” answers)
‡ significant for size of the place of residence (p<0.05) (“no” vs. “yes” answer or distribution of “yes” answers)
§ significant for social class (p<0.05) (“no” vs. “yes” answer or distribution of “yes” answers)
Rafal Rowinski, Andrzej Dabrowski, Tomasz Kostka. Archives of Gerontology and Geriatrics 60 (2015) 486–491

Prevention of frailty and functional decline:
1. Physical activity
2. Nutrition and pharmacological
interventions
3. Prevention and treatment of concomitant disorders

High Prevalence of Physical Frailty Among Community-Dwelling Malnourished Older
Adults–A Systematic Review and Meta-Analysis
Sjors Verlaan, MSc, Gerdien C. Ligthart-Melis, PhD, Sander L.J. Wijers, PhD, Tommy Cederholm, MD, PhD, Andrea B. Maier, MD, PhD,
Marian A.E. de van der Schueren, PhD
Journal of the American Medical Directors Association
Volume 18, Issue 5, Pages 374-382 (May 2017) DOI: 10.1016/j.jamda.2016.12.074
CONCLUSIONS:
The systematic review and meta-analysis revealed that malnutrition and physical frailty
in community-dwelling older adults are related, but not interchangeable geriatric
syndromes. Two out of 3 malnourished older adults were physically frail, whereas
close to 10% of the physically frail older adults was identified as malnourished.
Copyright © 2017 AMDA – The Society for Post-Acute and Long-Term Care Medicine Terms and Conditions

Nutritional supplementation is effective in the treatment of sarcopenia in
old age, and its positive effects increase when associated with physical
exercise.
Malafarina V(1), Uriz-Otano F, Iniesta R, Gil-Guerrero L. Effectiveness of nutritional supplementation on
muscle mass in treatment of sarcopenia in old age: a systematic review. J Am Med Dir Assoc. 2013
Jan;14(1):10-7.
Physical, nutritional, and cognitive interventional approaches were
effective in reversing frailty among community-living older persons.
Ng et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among
Older Adults: A Randomized Controlled Trial. Am J Med. 2015 Nov;128(11):1225-1236.e1.
Multicomponent exercise intervention reverses frailty and improves
cognition, emotional, and social networking in a controlled population of
community-dwelling frail older adults.
Tarazona-Santabalbina et al. A Multicomponent Exercise Intervention that Reverses Frailty and
Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A
Randomized Clinical Trial. J Am Med Dir Assoc. 2016 May 1;17(5):426-33.
European Union Geriatric Medicine Society (EUGMS), in cooperation with
other scientific organizations, appointed an international study group to
review dietary protein needs with aging (PROT-AGE Study Group).
To help older people (>65 years) maintain and regain lean body
mass and function, the PROT-AGE study group recommends average
daily intake at least in the range of 1.0 to 1.2 g protein per kilogram of
body weight per day.
Both endurance- and resistance-type exercises are
recommended at individualized levels that are safe and tolerated, and
higher protein intake (ie, ≥ 1.2 g/kg body weight/d) is advised for those
who are exercising and otherwise active.
Most older adults who have acute or chronic diseases need even
more dietary protein (ie, 1.2-1.5 g/kg body weight/d). Older people with
severe kidney disease (ie, estimated GFR <30 mL/min/1.73 m(2)), but who
are not on dialysis, are an exception to this rule; these individuals may
need to limit protein intake.
Bauer et al. Evidence-based recommendations for optimal dietary protein intake in older people: a
position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013 Aug;14(8):542-59.

Deutz et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clinical Nutrition 2014;33:929-936
European Society for Clinical Nutrition and Metabolism (ESPEN) recommendations:
(a) for healthy older people, the diet should provide at least 1.0-1.2 g protein/kg body weight/day,
(b) for older people who are malnourished or at risk of malnutrition because they have acute or chronic illness, the diet should provide 1.2-1.5 g protein/kg body weight/day, with even higher intake for individuals with severe illness or injury,
(c) daily physical activity or exercise (resistance training, aerobic exercise) should be undertaken by all older people, for as long as possible.

Muscle protein synthesis enhancement:
Daily protein intake of 1.2-1.5 g/kg (0.4-0.5 g/kg per meal)
Increased proportion of leucine in a given dose of protein
Supplementation with n=3 polyunsaturated fatty acids
Physical activity prior to protein intake Witard et al. Biogerontology 2016;17:529-546.

Supplementation
Vitamin D
BCAA
Leucine
β-hydroxy-β-methylbutyrate (HMB)
Creatine

Summary of the effect of nutrition on sarcopenia in randomised,
controlled studies meeting the inclusion criteria
Refe
rence Popula
tion Num
ber
Age, years,
mean (SD)
[range]
PED
ro
Score
Intervention
(duration) Outcomes
measured Main results
Flakoll et
al. [34]
Communit
y-dwelling
57
(0/57)
76.7
[62–90] 8
ARG + HMB +
LYS; PLA (12
weeks)
MM (BIA), MS
(isometric leg
strength, HS), PP
(get up and go)
MS (P ≤ 0.05) and PP (P = 0.002) significantly improved
with ARG + HMB + LYS versus PLA
ARG + HMB + LYS did not significantly improve MM
versus PLA
Deutz et
al. [32]
Healthy
individual
s on bed
rest
19
(4/15)
PLA: 67.1
(±1.7)
HMB: 67.4
(±1.4)
[60–76]
10
HMB; PLA
Bed rest (10
days) +
rehabilitation (8
weeks)
MM (DEXA), MS
(KE, leg press), PP
(SPPB, get up and
go, 5-item PPB)
Bed rest caused a significant decrease in MM (P = 0.02)
in the PLA group, but MM was preserved in the HMB
group
Changes in MS and PP were not significant for HMB
versus PLA
Stout et
al.[36]
Communit
y-dwelling
98
(49/4
9)
73 (±1 SEM)
[≥65] 9
Phase I: HMB;
PLA (24 weeks)
Phase II: PLA +
RET; HMB +
RET (24 weeks)
MM (DEXA), MS
(isokinetic leg
strength, HS), PP
(get up and go)
HMB alone significantly improved some, but not all
measures of MS versus PLA. No significant changes
were found in MM and PP with HMB versus PLA
Adding HMB to RET did not improve any parameters
over RET alone
Vukovich
et al. [39]
Communit
y-dwelling
31
(15/1
6)
70 (±1) 10
HMB + RET;
PLA + RET (8
weeks)
MM (DEXA, CT
scan), MS (misc.
upper and lower
body strength press,
flexion and extension
measurements)
MM improved with HMB + RET versus PLA + RET, but
not significantly (P = 0.08)
MS did not improve with HMB + RET versus PLA +
RET
Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS), 2014

Summary of studies involving creatine supplementation in
older adults (Candow, 2011)
Study Population Dosage Findings
Bermon et al.1998 Male/female (70 years)
CR: 16; PL: 16
CR: 20 g for 5 days
Maintenance: 3 g for 47 days ↔ lower-limb muscle volume
Brose et al. 2003 Male/female (68 years)
CR: 14; PL: 14 CR: 5 g, 98 days ↑ fat-free mass
Candow et al.2008 Male (66 years)
CR: 23; PL: 12 CR: 0.1 g kg−1, 30 days ↑ muscle hypertrophy
Chrusch et al.2001 Male (71 years)
CR: 16; PL: 14
CR loading: 0.3 g kg−1 for 5 days
Maintenance: 0.07 g kg−1 79 days ↑ fat-free mass, strength
Eijnde et al.2003 Male (64 years)
CR: 23; PL: 23 CR: 5 g for 1 year ↔ fat-free mass
Gotshalk et al.2008 Female (63 years)
CR: 15; PL: 12 CR: 0.3 g kg−1 for 7 days ↑ fat-free mass, strength
Gotshalk et al. 2001 Male (65 years)
CR: 10; PL: 8 CR: 0.3 g kg−1 for 7 days ↑ fat-free mass
Jakobi et al.2001 Male (72 years)
CR: 7; PL: 5 CR : 20 g for 5 days ↔ force production
Rawson et al.1999 Male (74 years)
CR: 10; PL: 10
CR: 20 g for 10 days
Maintenance: 4 g for 20 days ↔ fat-free mass
Tarnopolsky et al.
2007
Male/female (70 years)
CR: 21, PL: 18 CR: 5 g/days for 6 months ↑ fat-free mass, strength
CR creatine,
PL placebo

Creatine vs. chest press strength
Candow, 2014

Creatine and carbohydrates
Carbohydrate coingestion is important to
optimize creatine effects on body composition,
strength, and functional performance in older
adults
Creatine should be coingested with a carbohydrate
drink (for example with juice)
Devries MC, Phillips SM. Creatine supplementation during resistance training in older adults-a meta-analysis.
Med Sci Sports Exerc. 2014 Jun;46(6):1194-203.
Pharmacological interventions targeting the underlying biology of
sarcopenia
GH/IGF-1
DHEAS
Testosterone/androgens
Selective Androgen Receptor Modulators (SARMs)
TGFβ family members: myostatin, follistatin and GDF11
Myostatin antagonists

Becker et al. reported the improvement of power-demanding
performance measures (stair climbing, five-chair rise, fast gait speed)
in the older individuals after the treatment with the humanized
monoclonal antibody LY2495655.
For less power-intensive performance-based measures (6-min
walking distance, usual gait speed) and muscle strength no important
treatment effects were observed.
Becker et al. Myostatin antibody (LY2495655) in older weak fallers: a proof-of-concept,
randomised, phase 2 trial. Lancet Diabetes Endocrinol, 2015;3: 948-57.
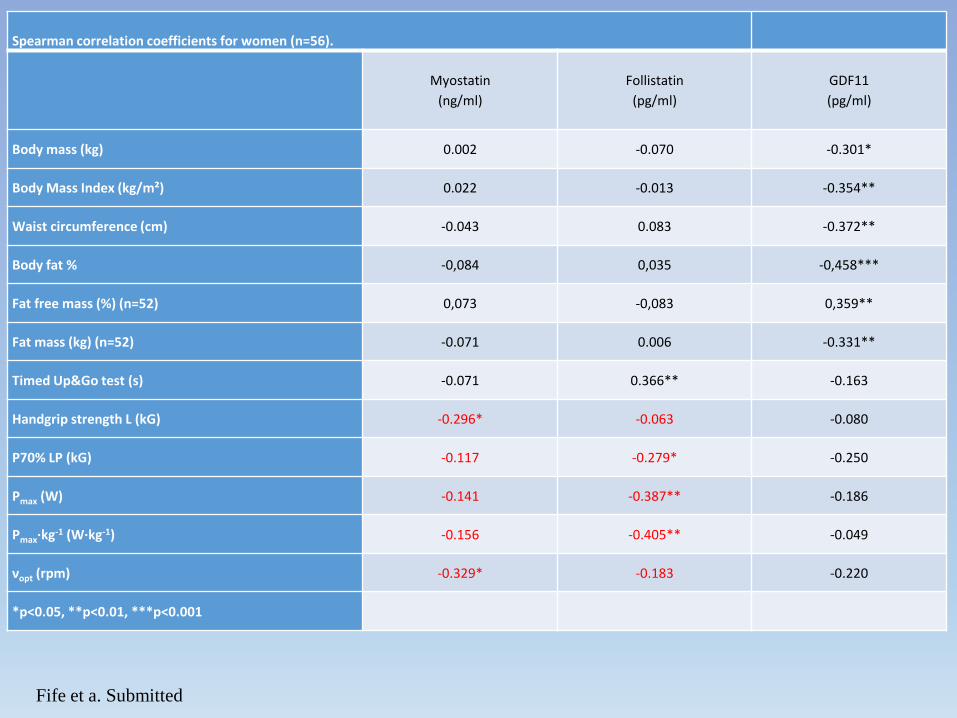
Spearman correlation coefficients for women (n=56).
Myostatin
(ng/ml)
Follistatin
(pg/ml)
GDF11
(pg/ml)
Body mass (kg) 0.002 -0.070 -0.301*
Body Mass Index (kg/m²) 0.022 -0.013 -0.354**
Waist circumference (cm) -0.043 0.083 -0.372**
Body fat % -0,084 0,035 -0,458***
Fat free mass (%) (n=52) 0,073 -0,083 0,359**
Fat mass (kg) (n=52) -0.071 0.006 -0.331**
Timed Up&Go test (s) -0.071 0.366** -0.163
Handgrip strength L (kG) -0.296* -0.063 -0.080
P70% LP (kG) -0.117 -0.279* -0.250
Pmax (W) -0.141 -0.387** -0.186
Pmax·kg-1 (W·kg-1) -0.156 -0.405** -0.049
νopt (rpm) -0.329* -0.183 -0.220
*p<0.05, **p<0.01, ***p<0.001
Fife et a. Submitted

Prevention of frailty and functional decline:
1. Physical activity
2. Nutrition
3. Prevention and treatment
of concomitant disorders
Frail and pre-frail older people corresponded to a substantial proportion of those
with more CVD risk factors, especially diabetes mellitus, highlighting the need
for preventive strategies in order to avoid the co-occurrence of CVD and frailty.
Ricci NA et al.: Frailty and cardiovascular risk in community-dwelling elderly: a population-based study.
Clinical Interventions in Aging 2014:9 1677–1685
Abdominal obesity, insulin resistance, and inflammation were significantly associated
with frailty, and the effect was independent of functional measurement and decline of
skeletal muscle mass.
Hwang et al. Association of Frailty and Cardiometabolic Risk Among Community-Dwelling Middle-Aged
and Older People: Results from the I-Lan Longitudinal Aging Study. Rejuvenation Res. 2015
Dec;18(6):564-72.

Cardiometabolic risk assessment:
- diet, smoking status, family history,
- fasting lipids (TC, triglycerides, HDL cholesterol, LDL Cholesterol,
TC/HDL ratio)
- glucose
- blood pressure
- weight, height, waist and hip circumference (BMI, WHR)
- blood count, electrolytes, creatinine, eGFR, microalbuminuria

ACE inhibitor treatment may halt or slow decline in muscle
strength in elderly women with hypertension and without
CHF.
Onder G, et al. Relation between use of angiotensin-converting enzyme inhibitors and muscle
strength and physical function in older women: an observational study. Lancet.
2002;359(9310):926-30.
The I/I ACE genotype is associated with a lower risk of frailty
and a lower frailty level relative to the D-carrying genotypes
among older Han people.
Chen et al. Association between Angiotensin-converting enzyme insertion/deletion polymorphisms and
frailty among chinese older people. J Am Med Dir Assoc. 2015 May 1;16(5):438.e1-6.

J Kostka, J Sikora, T Kostka: Relationship of quadriceps muscle power and optimal shortening velocity with angiotensin converting enzyme activity in older women. Clinical Interventions in Aging– in press.
Women taking
ACEI
N=22
Women taking
ARBs or ARBs
+ACEI
N=12
Women taking
MCRA or
MCRA+ACEI or
MCRA +ARB
N=10
Women taking no
ASBMs
N=51
mean±SD
mean±SD mean±SD mean±SD
Age 73.6±4.7 70.8±4.4 73.1±3.9 71.5±4.4
Hand grip strength – left (kgf) 24.2±9.8 23.3±7.8 18.1±5.3 23.5±7.8
Hand grip strength – right (kgf) 25.6±9.1 24.4±7.0 22.7±6.5 25.5±7.9
Pmax (W) 217±88 221±52 233±44 230±65
Pmax (W·kg-1) 3.11±1.20 3.25±0.88 3.38±0.95 3.49±1.05
Ʋopt (rep/min) 65.2±11.7 69.6±8.4 67.0±13.3 69.2±9.1
ACE (U/L) 27.4±13.4 38.9±12.9 37.1±12.3 46.2±17.5*
The influence of Angiotensin System Blocking Medications (ASBMs) blockers on muscle function and Angiotensin Converting Enzyme (ACE) activity

J Kostka, J Sikora, T Kostka: Relationship of quadriceps muscle power and optimal shortening velocity with angiotensin converting enzyme activity in older women. Clinical Interventions in Aging– in press.
The relationship between optimal shortening velocity (Ʋopt) and angiotensin converting enzyme activity in women not taking any ASBMs
rho = - 0.37 p=0.01
ACE activity (U/L)
Vo
pt
(re
p/m
in)
0 20 40 60 80 100 120
47
57
67
77
87
97
Other diseases, e.g.:
Michel JP et al. Advocating vaccination of adults aged 60 years and
older in Western Europe:statement by the Joint Vaccine Working
Group of the European Union Geriatric Medicine Society and the
International Association of Gerontology and Geriatrics-European
Region. Rejuvenation Res. 2009 Apr;12(2):127-35.
Liljas AEM et al. Self-Reported Hearing Impairment and Incident
Frailty in English Community-Dwelling Older Adults: A 4-Year
Follow-Up Study. J Am Geriatr Soc. 2017 May;65(5):958-965.
COPD, dementia, depression…

Acute care of frail elderly patients in a CGA unit was
independently associated with lesser loss of functional
ability and lesser increase in frailty after 3 months. Ekerstad et al. Clin Interv Aging 2017;12:1239-49.
Prevention of hospital-associated functional decline:
appropriate nutrition, early mobilisation, care of
comorbidities (incontinence, decubitus) Zisberg et al. JAGS 2015;63:55-62.
Benefits of early rehabilitation in hospitalised older subjects Kosse et al. BMC Geriatr 2013;13:107.

Summary
Early diagnosis and prevention of frailty
and functional decline:
1. Building-up physiological potential throughout
the lifetime
2. Identification of people at risk.
3. Identification and combatting of risk factors
4. Prevention and treatment of concomitant
disorders

Thank you for your attention




























![Frailty pathway [970kb]](https://img.pdfslide.us/doc/110x75/588da5761a28ab737b8b4e2c/frailty-pathway-970kb.jpg)