Embed Size (px)
Citation preview

lable at ScienceDirect
American Journal of Infection Control 42 (2014) 405-11
Contents lists avai
American Journal of Infection Control
journal homepage: www.aj ic journal .org
American Journal of Infection Control
Major article
Preventing transmission of MRSA: A qualitative study of health careworkers’ attitudes and suggestions
Dorothy J. Seibert PhD, RN a,*, Karen Gabel Speroni PhD, RN b, Kyeung Mi Oh PhD, RN a,Mary C. DeVoe BSN, RN b, Kathryn H. Jacobsen PhD c
a School of Nursing, George Mason University, Fairfax, VAb Inova Fair Oaks Hospital, Fairfax, VAcDepartment of Global and Community Health, George Mason University, Fairfax, VA
Key Words:Health personnelInfection controlInpatientsHealth care associated infectionNursing personnel
* Address correspondence to Dorothy J. Seibert,George Mason University, 4400 University Dr, MS 3C
E-mail address: [email protected] (D.J. Seibert).Supported by a grant from the Epsilon Zeta cha
Honor Society of Nursing.Conflict of interest: None to report.
0196-6553/$36.00 - Copyright � 2014 by the Associahttp://dx.doi.org/10.1016/j.ajic.2013.10.008
Background: Health care workers’ (HCWs) perceptions and attitudes affect implementation of pre-cautions to prevent transmission of drug-resistant pathogens such as methicillin-resistant Staphylococcusaureus (MRSA). Identification of challenges and barriers to recommended practices is a critical compo-nent of promoting a safe clinical environment of care.Methods: Semistructured interviews addressed how MRSA affects HCWs, prevention of transmission,and challenges and barriers HCWs experience when entering a MRSA isolation room and performingappropriate hand hygiene.Results: The purposive sample of 26 acute care HCWs (16 registered nurses; 1 physician; 6 allied healthprofessionals; and 3 support staff) self-selected from 276 responding to a questionnaire on MRSA.Analysis identified 18 themes across seven categories. Most participants reported feeling responsible forpreventing transmission, and having the knowledge and desire to do so. However, many also reportedchallenges to following consistent hand hygiene and use of contact precautions. Barriers included patientcare demands, equipment and environmental issues such as availability of sinks, time pressures, thepractices of other HCWs, and the need for additional signs indicating which patients require contactprecautions.Conclusions: The HCWs reported a need for improved clarity of isolation protocols throughout patients’hospital journey, additional rooms and staff for isolation patients, improved education and communi-cation (including timely and appropriate signage), and an emphasis on involving all HCWs in reducingcontamination.
Copyright � 2014 by the Association for Professionals in Infection Control and Epidemiology, Inc.Published by Elsevier Inc. All rights reserved.
Recent qualitative studies in the United States provide insightinto developing strategies to successfully implement practices thatreduce health careeassociated infections (HAIs) related to medicaldevices.1-3 However, only limited qualitative research has evaluatedhealth care worker (HCW) attitudes and reports of barriers to handhygiene and contact precaution adherence in acute care. Interna-tional studies, mostly from Europe, have suggested thatmost HCWsfeel a strong responsibility to patients and a desire to prevent
PhD, RN, School of Nursing,4, Fairfax, VA 22030-4444.
pter of Sigma Theta Tau, the
tion for Professionals in Infection C
infections.4-7 They have also suggested that self-protectiondnotpatient protectiondis the primary cue to action for HCWs toimplement hand hygiene and contact precautions.4-8
Across studies, HCWs consistently report that barriers toadherence include workloads and time pressures,4-7,9 as well asinsufficient access to appropriate facilities and protective equip-ment.4,10-12 HCWs also report challenges in maintaining standardsduring emergent clinical situations, because taking time for contactprecautions may compromise patient safety.4-6 The present studybuilds on these previous qualitative studies by examining HCWs’attitudes about methicillin-resistant Staphylococcus aureus (MRSA),perceptions of challenges and barriers to MRSA prevention, andsuggestions for preventing the transmission of MRSA in acutehealth care settings.
ontrol and Epidemiology, Inc. Published by Elsevier Inc. All rights reserved.

D.J. Seibert et al. / American Journal of Infection Control 42 (2014) 405-11406
METHODS
Participants
This qualitative study is 1 of 3 components of a comprehensiveevaluation of MRSA prevention practices at an acute care hos-pital that includes quantitative, qualitative, and direct observationmethods. The methods and results from the quantitative and directobservation studies are reported elsewhere.13 A purposive sampleof 26 HCWs engaged in direct patient care or with jobs requiringentry into patient care areas were recruited for interviews. Out of atotal of 276 HCW survey participants, 42 volunteered to be inter-viewed for this study, and 26 completed the interview (24 femalesand 2 males). The participants represented a variety of health carefields (16 nurses, 1 physician, 6 allied health professionals, and 2support staff), a wide age range (3 age 18-25 years, 6 age 26-35years, 7 age 36-45 years, 4 age 46-55 years, and 6 age 56 years andolder), and varying employment status (22 full-time, 2 part-time,and 2 as needed).
Interview methods
Semistructured interviews approximately 30 minutes in lengthwere completed in the hospital during September and October2012. The following questions explored perceptions of MRSA andchallenges in reducing transmission in acute health care settings:
1. How do you feel MRSA affects you as a HCW?2. What are suggestions of ways to prevent transmission of MRSA?3. How are you challenged in your work task when you have to
enter an isolation room?4. What are other barriers that prevent implementing isolation
precautions or appropriate hand hygiene?
Data analysis
Interviews were audio recorded and transcribed into 27 pages ofverbatim responses by the lead author (D.J.S.). Comments wereimported into Excel and sorted by theme. The lead author and 2researchers (K.G.S. and M.C.D.) completed content analysis using adirected approach with an open and selective method of coding.Interviews were reviewed during transcription and categorizationto identify multiple unique elements from each conversation, andcomments were assigned to categories and themes.14 The reviewersused an iterative process to refine categories and achieve consensuson response categorization and theme coding. An a priori frame-work focused on interview question objectives: perceptions or at-titudes about MRSA prevention, challenges of adhering to contactprecautions for patients in isolation, and hand hygiene barriers. Thefinal categorization scheme also included time management,knowledge or education about MRSA, communication (includingsignage), and mechanisms of MRSA contamination (Table 1).
Within themes, keywords were identified and used as searchterms for a line-by-line analysis of interview transcripts (Table 2).15
The word processor “Find” function confirmed that all keywordswere identified and coded. Assignment of an observation was notrestricted to a single category; comments addressing multiplethemes were coded for relevant categories.
RESULTS
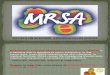
The final coding scheme consisted of 7 categories and 18 themes(Table 2). Figure 1 shows each core category and theme. Here,
emergent themes from each of the 7 main categories are presentedin the words of the study participants.
Perceptions and attitudes
Figure 1 lists the participants’ positive and negative perceptionsabout MRSA and its impact on their lives. The HCW’s responsibilityfor patient care was a common positive attitude that promotedMRSA prevention activities:
“First of all, I feel responsible for the person that I am dealingwith. That’s where it really impacts me. If I touch somebody andI haven’t washed my hands properly, then I am going to be thecarrier and trigger for that MRSA to go forward. And to thinkwhat happens to people! Especially, I work in joint replacement,and if they have some kind of joint infection, it’s epic” (nurse).
“It requires that we be much more careful in our registrations.Because.we’re responsible for alerting the clinical staff. So aspart of our job, we have to always be aware of an alert [and] topass the information on to the clinical staff” (support staff).
Negative prevention perceptions included concerns that per-sonal protection may adversely affect patient care and inhibithealing derived from physical contact with a caregiver:
“I think that at some point when a health care professionalknows that her patient is infectious, there is a barrier thathappens. A barrier to touch, just to provide comfort or a healingtouch or comfort touch.goes away when you have the barrierof the PPE [personal protective equipment] and just the ideathat the patient is infectious then. You want to protect yourselfand of course when you go home, you want to protect yourfamily” (nurse).
“I feel like I don’t make a connection and a contact [with] mypatient that I normally would if somebody was not on iso-lation...the gloved hands versus the skin-to-skin contact oftrying to make that connection with the patient” (nurse).
Some HCWs’ negative attitudes to contact precautions adher-ence could have significant repercussions for patient safety:
“I think the biggest things are that people either think, ’Well I’monly doing this one little task; it doesn’t matter,’ or ’I’m justgoing to pop in the room, and I just need to get this one formsignedddo I really need to put on and use all the isolation or allthe preventive things I should?’” (support staff).
Contact precautions
Among the comments related towork practices and challenges inwork practice, 15 reflected adherence to recommended practices ofgloving, gowning, and hand hygiene and 13 reflected nonadherence.Many participants expressed concern about nonadherence:
“My suggestion would be just better adherence to the system.Maybe a more strict, straightforward way of having people look atthe signage and the carts and gowning up and gloves and every-thing. I don’t feel like it is being adhered to as well” (allied health).
Adherence to contact precaution protocols raised concernsabout patient safety when time is critical. Donning and doffinggowns and gloves is a challenge “when there’s a safety issue andyou can’t just run right in,” as reported by nurses concerned aboutpatients at risk for falling and injuring themselves, among otherpossible threats to safety. Providing the same level of care to thepatient on isolation challenges the HCW who knows that “it just

Table 1Definitions of categories by order of frequency
Category Definition
Perceptions/attitudes (n ¼ 61) Positive comments such as responsibility in care, feelings, or opinions about awareness of MRSA, perceptions of barriers to patient care,concern for MRSA transmission, and empowerment related to MRSA prevention; expression of negative perceptions, such as contactprecautions being barriers to healing touch and comfort, lack of awareness, fear of MRSA, and nonadherence to MRSA prevention
Contact precautions (n ¼ 58) Challenges in the processes of caring for patients in isolation, equipment processing and cleaning, safety issues, barriers in gloving andgowning, and adherence to practice standards
Time (n ¼ 53) Time and contact precautions processes, time spent screening patients and researching patients’MRSA histories, time caring for patients,staffing issues, care planning and workflow, and planning assignments
Knowledge/education (n ¼ 41) Knowledge of MRSA, potential educational opportunities regarding MRSA, education about transporting patients and cleaning, methodsof education, and knowledge of patient MRSA status
Communication (n ¼ 33) Communication among HCWs and with patients, communication about MRSA status and MRSA screening, contact precautions signs forpatients with MRSA
Hand hygiene (n ¼ 28) Perceptions or attitudes about HCW adherence, responsibility for prevention, barriers related to facilities and equipment (eg, sinks,dispensers, and alcohol rubs)
Contamination (n ¼ 22) Contamination of the environment by MRSA, cross-contamination between patients and HCWs, contamination of equipment
D.J. Seibert et al. / American Journal of Infection Control 42 (2014) 405-11 407
takes more time to care for the patient” (nurse), but realizes that “Idon’t go into the patient’s [room] as frequently as I would nor-mally go into a room because of having to gown up” (nurse). “Tocome back to the room, regown, reglove, and go through thewhole thing is very time-consuming. So, I’ve noticed people whotake shortcuts” (allied health). Other HCWs identified concernsrelated to contaminated charts, stethoscopes, wheels, otherequipment removed from isolation rooms, and the time elementinvolved in cleaning. An allied health HCW mentioned an addi-tional barrier to use of contact precautions: “For one thing,wearing the gowns can be little overheating if I’m doing a lot ofphysical lifting of patients.”
Many HCWs questioned appropriate work environment pre-cautions. A registration staff worker noted that “a big challengefor us was [to determine] just what...we need to do.” According toa presurgical HCW, “I’m challenged in terms of the extra workthat needs to be done to find out if they [patients] still need to bekept on contact precautions when they come in for the surgery.”A surgical HCW stated, “Bacteria, not only MRSA, are justubiquitous and everywhere. There is always a risk of cross-contamination between patients, and any bacteria, not onlyMRSA, can certainly complicate any surgical procedure and onlymakes it worse...and without adequate staffing, the risk iscertainly increased.”
Time
Time issues were mentioned by HCWs as relating to contactprecautions/MRSA screening, patient care, staffing issues, andplanning and workflow. For example, time delays related to contactprecautions were reported by HCWs who review patient historiesfor MRSA colonization or infection before admission: “The chal-lenge that it has for me is that when I’m interviewing a patient andfind out that they’ve had a history of MRSA, it’s a lot of extrawork toresearch it out” (nurse). Isolation patients also create space de-mands: “It restricts the rooms that we can put patients in in theemergency department. It closes off rooms after the patient hasbeen moved out of the room” (nurse).
Other HCWs identified patient care- and equipment-relateddelays: “It adds an extra step when you’re on a busy unit. Youmay be bringing stuff in with you like Accu-checks. And it’s justalways those extra little steps that delay your efficiency. I guessthat’s the challenge” (nurse). “Time tends to be a barrier whenyou’re in a hurry and have a huge patient load. You find yourselfrunning in real quick to grab something before putting the gownon: ‘Oh, I’m just going to grab this out of the room’” (nurse). Anallied health staff member described the process involved in
entering and exiting isolation: “Getting gowned, gloved, washinghands before and washing hands after, [and] cleaning my equip-ment. So it definitely takes a lot of time.”
The HCWs acknowledged the challenges posed by the extratime needed to provide care and a lack of support staff to providesupplies and help with tasks. “Well, it definitely slows down theprocess. If you have a patient with MRSA, sometimes you will seethat patient last versus seeing them first” (nurse). “An isolationpatient really requires 2 people to care for them together. Youhave 1 considered contaminated and another clean” (nurse). Asfor delays in getting assistance, “I find that the patient needs a newbrief or they need new linens and it’s getting someone else, callingout of the room to get someone to bring in what we need” (alliedhealth).
Several participants who care for patients in isolation roomsreported ways to minimize the time burden of caring for MRSApatients and maximize patient safety: “Well, I don’t think it’s somuch of a challenge as remembering and positioning yourself in away that while you’re with a patient you don’t have to leave forother supplies” (allied health). “We do make a really strongconscious effort [to] always put the [MRSA] patient at the end of theday or the end of the cases” (nurse). Work planning contributes tothis success: “As the charge nurse making our patient.assign-ments, we certainly wouldn’t give a neutropenic patient or animmunocompromised patient to a nurse assigned to an activeMRSA case.”
Knowledge/education
Knowledge and educational opportunities were identified 23times for the HCWs and 18 times for patients, visitors, and thecommunity. A physician noted: “People knowwhat the right thing todo is. How do we help people do the right thing?.We have toremind people more constantly.” Interviewees emphasized the need“to make sure that all the employees understand what MRSA is”(nurse), to provide “a lot more education” (allied health), and to “getthe patients involved in prevention” (support staff). HCWs describedincidents of family members and visitors of patients with MRSAstrolling through the hospital corridors while wearing gowns andgloves as being “very oblivious to what was going on and thereasoning behind.wearing that stuff” (allied health). “Because lotsof people come from different countries, they do not understandwhat MRSA is” (nurse). Moreover, “lots of people don’t get that ed-ucation on a regular basis” (allied health). “I think it is all abouteducation, and I think we have to get buy-in from everybody.Everybody in the hospital, all those 42 people [that, on average, entera patient’s room over the course of a day] for 24 hours” (physician).

Table 2Interview content inductively developed categories and themes with characteristic response
Category Theme Key terms Characteristic interview response
Perceptions/attitudes(n ¼ 61)
Positive perception/attitude(n ¼ 44)
Feel, think, perceive,barrier, challenge
N: “Otherwise it’s just changing an individual’s mind andhabit. I just think.making MRSA visual and making aperson believe they actually can be empowered to stopthe transmission.”
Negative perception/attitude(n ¼ 17)
Feel, think, perceive,barrier, challenge
N: “You find yourself running in real quick to grabsomething before put, you know, not putting the gownon: ’Oh, I’m just going to grab this out of the room.’”
Contact precautions(n ¼ 58)
Challenges (n ¼ 30) Barriers, challenge N: “They need more; like their acuity is very high comparedto a nonisolation patient. I just feel like if I have lessisolation patients.I can follow all the standards thatthey require.”
Practice (adherence/nonadherence)(n ¼ 28)
Prevent transmission, challenge,contact precautions
N: “Making sure you do.wearing the gowns and gloveswhen we are in isolation for MRSA.”
AH: “I have seen health care workers walk into a roomungowned and hug an isolation patient.”
Time/work/planning(n ¼ 53)
Planning/workflow (n ¼ 22) Time, challenge, work, planning AH: “For me personally it means more time...gettinggowned and gloved, washing hands before and aftercleaning my equipment.”
Contact precaution/ screening(n ¼ 17)
Affect, challenge,contact precautions
N: “It’s the time, it’s the time. And you know you are doingthis in and out very quickly. It’s a lot of work to do itproperly. A lot of thought behind it.”
Caring for patients (n ¼ 7) Time, affect, challenge N: “Well it definitely slows down the process. Just the basicpatient care...”
Staffing (n ¼ 7) Barrier, challenge, staff N: “It’s easy to slip up because you’re so short staffed andyou’re going so fast.
Knowledge, education(n ¼ 41)
HCW, medical offices (n ¼ 23) Prevent, knowledge,barriers, education
N: “We’ve educated; we’ve done everything. I just think it’sjust continually, just the monitoring, continuallyeducating people, and keep hounding them.”
Patient/visitors/community(n ¼ 18)
Prevent, challenges,barriers, education
N: “I’ve actually told a lot of people, well this is what it is.Kind of like spread the word because a lot of peopleactually don’t know what it is.”
Communication(n ¼ 33)
General (n ¼ 13) Communicate, challenge, tell,educate, show
N: “They don’t understand. and they get very defensivewhen you go tell them that you cannot take this insidethe isolation rooms.”
Contact precaution signs(n ¼ 12)
Barrier, challenge,contact precautions
N: “Just the communication thing.the sign wasn’t up or wecan’t find a cart.and then people going in and not takingthe precautions that they should.”
MRSA status (n ¼ 8) Challenge, barrier, prevention, MD: “I think proper communication would be beneficial,not just here at our hospital but anywhere if a patient’sbeen flagged as being MRSA-positive. I think.follow-upshould be taken, like when a patient is discharged.”
Hand hygiene(n ¼ 28)
Perception/attitude (n ¼ 21) Feel, think, perceive, barrier,hand hygiene
N: “If I haven’t washedmy hands properly, then I’mgoing tobe the carrier and trigger for that MRSA to go forward.”
Barrier (n ¼ 7) Barrier, hand hygiene, sink MD: “I like the idea of washing them down the sink.trywhen you come out of the patient room and try andfigure out where the nearest sink is. They are behindartificial barriers.”
Contamination(n ¼ 22)
Environment (n ¼ 13) Clean, prevent, transmission AH: “We have to get the room that we take them intoterminally cleaned, so we’re not putting other patients atrisk.”
Patient/staff (n ¼ 5) Contamination, challenge N: “We have to make sure we don’t pass anything on topatients either, from patient to patient.”
Equipment (n ¼ 4) Affect, prevent transmission AH: “You come out and if there’s no bleach wipes readilyavailable, it’s hard to get everything [equipment] cleanedappropriately when you’re leaving the room.”
AH, allied health; MD, physician; N, nurse; SS, support staff.
D.J. Seibert et al. / American Journal of Infection Control 42 (2014) 405-11408
Communication
Communication received 33 mentions, including generalcomments, those related to contact precautions signs, and thoserelated to the patient’s MRSA status. Participants identifiedcommunication (or lack thereof) as a barrier preventing imple-mentation of recommended practices. “Make sure they areaware, the family is aware. The lack of communication can causelots of problems” (nurse). Eleven remarks emphasized theabsence of appropriate contact precautions signs: “Just too manytimes, [you] go to a new patient, then leave the room, come backin an hour, and all of a sudden the isolation signs are up” (alliedhealth).
Communication about the MRSA status of patients wasmentioned as a barrier, as a challenge, and as a means of pre-venting transmission of MRSA. “Sometimes it’s difficult to findout if the patient truly still has the infection. They may say theywere cleared by a doctor, not of this facility, but then they haveno documentation of it” (support staff). Communication of MRSAstatus was viewed as a challenge by one physician: “As soon asthey hit the hospital again, if they come, in the admission thingflags up as, MRSA-positive, and they get put into isolation. So wechanged our flow such that the patient gets informed. The pa-tient has a letter they can take to their primary care [provider].”One HCW reiterated the relationship between communicationand prevention: “Like I said, communication is the biggest. It

Fig 1. Categories and themes identified in 26 interview narratives.
D.J. Seibert et al. / American Journal of Infection Control 42 (2014) 405-11 409
[MRSA status] needs to be communicated right off the bat (alliedhealth).
Hand hygiene
Hand hygiene comment themes were classified as perceptions/attitudes (n ¼ 21) and barriers (n ¼ 7) in work practice. One nurserecognized the importance of handwashing as a team:
“All coworkers, all the people that work in the hospital. First theyhave to wash their hands, that’s the main thing. Before they go inthe patient’s room and even after. Wash their hands before usinggloves and after they take the gloves off; wash their hands.We justhave to make sure that everybody understands as a team” (nurse).
The challenges to hand hygiene generally related to placementof sinks:
“Well, I don’t think it is a barrier, but I think if you put a sink infront of someone, versus hiding it in every other place.... It
would probably be easier if the those sinks and places to washhands and things like that were right in your face so that youwould bump into it to get where you are going” (nurse).
Contamination
Contamination issues were related to the environment, pat-ients and staff, and equipment. The HCWs voiced concerns abouttransmission of bacteria in the environment and provided possiblesuggestions for preventing transmission:
“It’s certainly easy, even when wearing gloves, to touch acontaminated patient and then touch a countertop. Have any ofthe cleaning staff or any of the nursing staff, anyone actually,come in contact with that unknowingly and transmit bacteriafrom one place to another” (nurse).
“I think if we had more room basically, like having a secludedarea that we could just take them. Where the patient can be put

D.J. Seibert et al. / American Journal of Infection Control 42 (2014) 405-11410
in that room, registered there, wait there until the lab is ready todraw their blood” (allied health).
Related to equipment, a nurse identified concerns related to pa-tient care: “Weneed to do a better jobwithwiping down the surfacesof things we use all the time, like our pens, scissors, things like thatwe might touch while we are caring for the patient.” Cross-contamination between patients or staff to patients was identifiedas a concern: “So I know it affectsmy daily life here and I don’t want tobring anything home. And I’m aware we have to make sure we don’tpass anything on to patients either, from patient to patient” (nurse).
Eleven participants reported experiencing no barriers, and 7reported no challenges. A positive response was: “I don’t knowwhat barrier, I mean, they try to have sinks all over and the rightequipment for us to use” (nurse). Many HCWs identified no chal-lenges because they considered contact precautions and hand hy-giene to simply be standard practice: “I don’t see a challenge. Thebiggest challenge is getting the cart, and that’s not hard” (nurse).According to one managerial participant, the hospital’s adminis-tration had “worked so hard to remove any barriers.”
DISCUSSION
Qualitative studies provide a richer insight into HCWs’ percep-tions about prevention of MRSA and other HAIs than can be gainedby cross-sectional surveys and hand hygiene observations alone.16
The participants in this study generally had positive attitudesabout their ability and willingness to take action to reduce MRSAtransmission, along with a deep sense of responsibility to the patientand others that serves as a motivation for adherence to preventivepractices. In agreement with previous studies, the participantsexpressed ownership of professional responsibility to protect theirpatients and awareness that pathogen transmission is possible whenhand hygiene and contact precautions are neglected.4-6,12
HCWs and patients have voiced concerns that contact pre-cautions negatively affect the quality of patient care because HCWstend to visit isolated patients less often.17,18 Patients on contactprecautions receive fewer hourly visits than those not on contactprecautions and have less direct contact time with HCWs.18-20
Although this reduced time might not result in significant differ-ences in patient care quality or satisfaction,21,22 the perception thatHCWs check on isolated patients less often than nonisolated pa-tients was reported as a HCW stressor by this study’s participants.With appropriate staff and patient education on contact pre-cautions, it is possible to maintain patient care quality and patientsatisfaction at high levels.17,21
Isolated patients may be at increased risk for errors in care andadverse events,23 in part because adherence to contact precautionstakes time away from immediate patient care, and because caringfor a patient in isolation often requires 2 HCWs, so that 1 HCW canstay with the patient while the other retrieves extra equipment andassists with care. Improved staff-to-patient ratios when HCWs arecaring for patients on contact precautions may improve patientoutcomes.24,25 Higher staffing levels and greater total hours of careby registered nurses have been associated with reduced patientmortality and risk of HAIs.26-29
Knowledge and education of HCWs and the public are essentialfor preventing transmission of microorganisms in health caresettings. International studies have concluded that conventionaleducation to improve knowledge and skills will not sustainimprovement in hand hygiene campaigns.30,31 Strategies for main-taining compliance mentioned by this study’s participants and inprevious studies include continuous education, an organizationalcommitment to education; multimodal training components, suchas reminder signs and performance feedback; and the use of several
different teaching approaches in a variety of languages (given thatmany HCWs, patients, and visitors are multilingual) to reach targetaudiences in new ways.30-36 Our participants also suggested edu-cation of patients, visitors, and the public. Previous researchers havereported that patients with MRSA and their visitors often lack anunderstanding of MRSA transmission.17,37 Appropriate educationmay help patients and visitors to cope with their situation in thehospital, reduce anxiety and fear, improve patient and family satis-faction, and empower the patient to become an active participant inhelping reduce transmission of infectious agents.37-40 In addition,communication of patient isolation status and prompting of handhygiene and contact precautions is critical for reducing HAIs in acutecare facilities.
Several limitations of this study design require cautious inter-pretation of our results. First, the use of a self-selective sampleresulted in a participant list that drew disproportionately onnurses. This means that diverse medical, allied health, and supportstaff perspectives are not necessarily reflected in the transcripts. Inaddition, the self-selection of participants may mean that onlythose HCWs with concerns about MRSA or those with particularlyexemplary behaviors volunteered to be interviewed, and the in-clusion of HCWs from a single hospital limits the diversity ofbarriers encountered by participants seeking to engage in recom-mended hand hygiene and contact precautions. Second, some ofthe interviews were rushed because they occurred during workinghours or were conducted in noisy places like the hospital cafeteriathat did not lend themselves to extensive probing of responses. Thismeant that some participants did not have time to give longerexplanations of their thoughts and perceptions.
Strengths of the study include the participation of a diverse groupof HCWs, including support staff, and conducting interviews onsiteduring work shifts. The latter might have prompted better responsesfrom participants because they were interviewed in familiar andcomfortable places and could report on patient care issues that theyhad experienced immediately before their interviews.
Despite the study’s limitations, the main findings are clear:HCWs who perceive themselves as responsible for preventing thetransmission of MRSA and other pathogens report high motivationto adhere to hand hygiene and contact precautions, but timepressures and heavy workloads pose challenges to adherence. It isimportant for health care administrators and infection control staffto collaborate with patient care staff on identifying and removingbarriers to adherence and implementing positive cues to action.Organizational leadership strategies can help create a culture inwhich HCWs and others feel supported in their efforts to personallyengage in recommended behaviors and to encourage their co-workers to do the same.11,12,36,40,41
Our findings point to the importance of acknowledging the per-ceptions and attitudes of all HCWsdmedical, nursing, allied health,and support staffdand removing challenges to consistent adherenceto guidelines for contact precautions and hand hygiene. Multidisci-plinary (and, where appropriate, multilingual) educational in-terventions for staff, education of patients and visitors, effectivecommunication of isolation status and patient history of MRSA to allrelevant persons, empowerment of HCWs, and enforcement ofadherence to hand hygiene and contact precautions were all sug-gested by our participants as strategies for reducing MRSA trans-mission in acute care settings and should be seriously considered byinfection preventionists and others responsible for reducing HAIs.
References
1. Krein SL, Olmsted RN, Hofer TP, Kowalski C, Forman J, Banaszak-Holl J, et al.Translating infection prevention evidence into practice using quantitative andqualitative research. Am J Infect Control 2006;34:507-12.

D.J. Seibert et al. / American Journal of Infection Control 42 (2014) 405-11 411
2. Krein SL, Kowalski CP, Damschroder L, Forman J, Kaufman SR, Saint S. Pre-venting ventilator-associated pneumonia in the United States: a multicentermixed-methods study. Infect Control Hosp Epidemiol 2008;29:933-40.
3. Saint S, Kowalski CP, Forman J, Damschroder L, Hofer TP, Kaufman SR, et al.A multicenter qualitative study on preventing hospital-acquired urinary tractinfection in US hospitals. Infect Control Hosp Epidemiol 2008;29:333-41.
4. Erasmus V, Brouwer W, van Beeck EF, Oenema A, Daha TJ, Richardus JH, et al.A qualitative exploration of reasons for poor hand hygiene among hospitalworkers: lack of positive role models and of convincing evidence that handhygiene prevents cross-infection. Infect Control Hosp Epidemiol 2009;30:415-9.
5. Eveillard M, Bruna T, Kouatchet A, Dubé L, Poiroux L, Dabin E, et al. Using aqualitative study to understand the failure of a strategy implemented forimproving hand hygiene adherence in 4 intensive care units. Infect ControlHosp Epidemiol 2013;34:447-8.
6. Jang J, Wu S, Kirzner D, Moore C, Youssef G, Tong A, et al. Focus group study ofhand hygiene practice among healthcare workers in a teaching hospital inToronto, Canada. Infect Control Hosp Epidemiol 2010;31:144-50.
7. Lusardi G. Hand hygiene. Nurs Manag (Harrow) 2007;14:26-33.8. Morrow E, Griffiths P, Rao GG, Flaxman D. “Somebody else’s problem?” Staff
perceptions of the sources and control of meticillin-resistant Staphylococcusaureus. Am J Infect Control 2011;39:284-91.
9. Nichols A, Badger B. An investigation of the division between espoused andactual practice in infection control and of the knowledge sources that mayunderpin this division. Br J Infect Control 2008;9:11-5.
10. Cruz E, Pimenta F, Hayashida M, Eidt M, Gir E. Staphylococcus aureus detectionin the mouth of housekeepers. Rev Lat Am Enfermagem 2011;19:90-6.
11. Lines L. A study of senior staff nurses’ perceptions about MRSA. Nurs Times2006;102:32-5.
12. Randal JA, Clarke M. Infection control nurses’ perceptions of the code of hy-giene. J Nurs Manag 2011;19:218-25.
13. Seibert DJ, Speroni KG, Oh KM, DeVoe MC, Jacobsen KH. Knowledge, percep-tions, and practices of methicillin-resistant Staphylococcus aureus transmissionprevention among acute care setting health care workers. Am J Infect Control.2014 Jan 6. [Epub ahead of print.]
14. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. QualHealth Res 2005;15:1277-88.
15. Polit DF, Beck CT. Nursing research: principles and methods. 8th ed. Phila-delphia [PA]: Lippincott Williams & Wilkins; 2008.
16. Forman J, Creswell JW, Damschroder L, Kowalski CP, Krein SL. Qualitativeresearch methods: key features and insights gained from use in infectionprevention research. Am J Infect Control 2008;36:764-71.
17. Barratt R, Shaban R, Movie W. Behind barriers: patients’ perceptions of sourceisolation for methicillin-resistant Staphylococcus aureus (MRSA). Aust J AdvNurs 2010;28:53-60.
18. Evans HL, Shaffer MM, Hughes MG, Smith RL, Chong TW, Raymond DP, et al.Contact isolation in surgical patients: a barrier to care? Surgery 2003;134:180-8.
19. Masse V, Valiquette L, Boukhoudmi S, Bonenfant F, Talab Y, Carvalho J-C, et al.Impact of methicillin-resistant Staphylococcus aureus contact isolation units inmedical care. PLoS ONE 2013;8:e57057.
20. Morgan DJ, Pineles L, Shardell M, GrahamMM, Mohammadi S, Forrest GN, et al.The effect of contact precautions on healthcare worker activity in acute carehospitals. Infect Control Hosp Epidemiol 2013;34:69-73.
21. Gasink LB, Singer K, Fishman NO, Holmes WC, Weiner MG, Bilker WB, et al.Contact isolation for infection control in hospitalized patients: is patientsatisfaction affected? Infect Control Hosp Epidemiol 2008;29:275-8.
22. Morgan DJ, Day HR, Harris AD, Furuno JP, Perencevich EN. The impact ofcontact isolation on the quality of inpatient hospital care. PloS ONE 2011;6:e22190.
23. Stelfox H, Bates D, Redelmeier D. Safety of patients isolated for infection con-trol. JAMA 2003;290:1899-905.
24. Aiken L, Cimiotti J, Sloane D, Smith H, Flynn L, Neff D. Effects of nurse staffingand nurse education on patient deaths in hospitals with different nurse workenvironments. Med Care 2011;49:1047-53.
25. Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and healthcareeassociated infection. Am J Infect Control 2012;40:486-90.
26. Blegen M, Goode C, Spetz J, Vaughn T, Park S. Nurse staffing effects on patientoutcomes; Safety-net and nonesafety-net hospitals. Med Care 2011;49:406-14.
27. Needleman J, Buerhaus P, Mattke S, Stewart M, Zelevinsky K. Nurse-staffinglevels and the quality of care in hospitals. N Engl J Med 2002;346:1715-22.
28. Hugonnet S, Chevrolet J, Pittet D. The effect of workload on infection risk incritically ill patients. Crit Care Med 2007;35:76-81.
29. Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR, Harris M. Nursestaffing and inpatient hospital mortality. N Engl J Med 2011;364:1037-45.
30. Mathai E, Allegranzi B, Seto WH, Chraïti M-N, Sax H, Larson E, et al. Educatinghealthcare workers to optimal hand hygiene practices: addressing the need.Infection 2010;38:349-56.
31. Wilson S, Jacob CJ, Powell D. Behavior-change interventions to improve hand-hygiene practice: a review of alternatives to education. Crit Public Health 2011;21:119-27.
32. De Wandel D, Maes L, Labeau S, Vereecken C, Blot S. Behavioral determinants ofhand hygiene compliance in intensive care units. Am J Crit Care 2010;19:230-9.
33. Pittet D, Simon A, Hugonnet S, Pessoa-Silva CL, Sauvan V, Perneger TV. Handhygiene among physicians: performance, beliefs, and perceptions. Ann InternMed 2004;141:1-8.
34. Pittet D. The Lowbury lecture: behaviour in infection control. J Hosp Infect2004;58:1-13.
35. Eldridge NE, Woods SS, Bonello RS, Clutter K, Ellingson L, Harris MA, et al. Usingthe Six Sigma process to implement the Centers for Disease Control and Pre-vention guideline for hand hygiene in 4 intensive care units. J Gen Intern Med2006;21:S35-42.
36. Whitby M, McLaws M-L, Slater K, Tong E, Johnson B. Three successful in-terventions in health care workers that improve compliance with hand hy-giene: is sustained replication possible? Am J Infect Control 2008;36:349-55.
37. Skyman E, Sjöström H, Hellström L. Patients’ experiences of being infected withMRSA at a hospital and subsequently source isolated. Scand J Caring Sci 2010;24:101-7.
38. Alston C, Paget L, Halvorson G, Novelli B, Guest J, McCabe P, et al. Communi-cating with patients on health care evidence. Washington [DC]: Institute ofMedicine; 2012.
39. Hart R. The effects of a poster in informing and empowering patients ininfection prevention and control. J Infect Prev 2012;13:146-53.
40. Whitby M, Pessoa-Silva CL, McLaws M-L, Allegranzi B, Sax H, Larson E, et al.Behavioral considerations for hand hygiene practices: the basic building blocks.J Hosp Infect 2007;65:1-8.
41. Creedon S. Hand hygiene compliance: exploring variations in practice betweenhospitals. Nurs Times 2008;104:32.