Embed Size (px)
Citation preview

Preventing perinatal depression in community health settings
Huynh-Nhu Le, Ph.D.George Washington University
DHHS/HRSA/Maternal and Child Health Bureau/Division of Research,Training and EducationR40 MC 02497

Overview
Prevention of perinatal depression The Mothers and Babies: Mood and
Health ProjectInterventionPreliminary findings
Practice and policy implications

Prevention(of new cases, i.e., before onset
of disorder)
Treatment(for individuals with disorder)
Maintenance (of normal mood after
recovery)

Postpartum Depression Prevention Trials
No significant prevention effects:
Stamp, Williams, & Crowther (1995) Brugha et al. (2000)
Significant effects:
Elliott et al. (2000): groups for first-time mothers
Zlotnick et al. (2001, 2006): interpersonal approach with low-income women
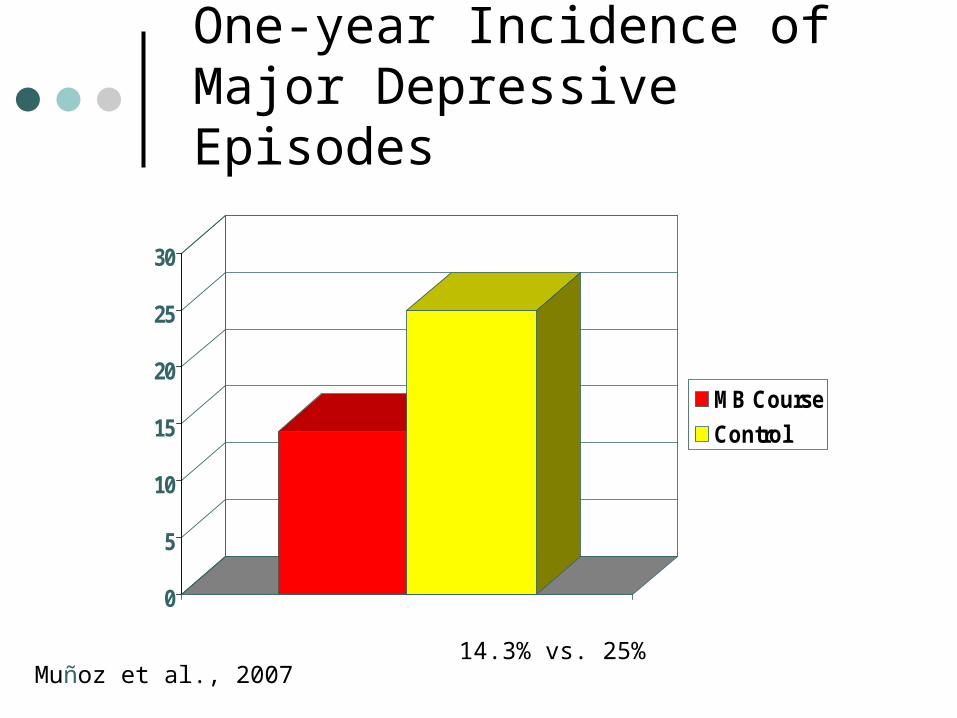
One-year Incidence of Major Depressive Episodes
0
5
10
15
20
25
30
MB Course
Control
14.3% vs. 25%Muñoz et al., 2007

The Mothers and Babies: Mood and Health Project
Goal: Reduce the onset of major depressive episodes by teaching women mood regulation skills and education regarding parenting and child development.Focus on mothers-to-be, with the long-term
aim of reducing depression risk in infants.

Usual Care
Positive thoughts Social support Pleasant activities
prenatal care
Depressive sxMDE incidence
Maternal efficacyMaternal & infant healthMother-child interaction
Maternal EfficacyMaternal & infant health
MEDIATING VARIABLES OUTCOME
Mothers & Babies Course
Randomized Controlled Trial

Community Partners
The Mary’s Center for Maternal and Child Care
The Center for Life at Providence Hospital

The Mothers and Babies Course
• 8 sessions during pregnancy
• 3 booster sessions (6 weeks, 4 & 12 months PP)
• Cognitive Behavioral Theory
• Relevant perinatal topics• Emphasis on a New
Latino sample

Eligibility Criteria
Demographics: 18 and 35 years of age < 24 weeks gestation No smoking, alcohol, substance use
High risk for Depression: History of Depression 110
(50.0%) CES-D ≥ 16 49
(22.3%) Dep Hx & CES-D ≥ 16 61 (27.7%)

Center staff administered Screening Interviews
n = 516 (68.3%)
Not eligible n = 446
(59.0%)
Eligible n = 310
(41.0%)
Randomized n = 220
(71.0%)
Intervention N = 112 (50.9%)
Usual Care N = 108 (49.1%)
Not randomizedn = 90 (29.0%)
Not interested/too busy n=23Past gestation n=14Work conflict n=15Unable to contact n=26Miscarriage n=8Other n=4
Research staff administered Screening Interviews n = 240 (31.7%)
No dep hx n=137CESD <16 n=310Demographic n=319Current depression n=39
Figure 1: Recruitment
Contacts with potential participants by center staff N = 553
Contacts with potential participants by research staff N=1,349

M (SD)
Age 25.4 (4.6)
Education (years) 8.9 (4.0)
Marital Status Married/Cohabitating Single Separated Widowed
63.5%30.0% 6.0% 0.5%
First Pregnancy 40.9%
Weeks gestation 17.6 (6.6)
Demographics I (N = 220)

Birthplace El Salvador
Mexico
Honduras
Guatemala
Other
54.5%
15.5%
10.9%
10.0%
1.4%
7.7%
Years in U.S. M (SD) 4.3 (4.7)
At least 1 child living in home country
30.9%
Demographics II

Intervention AttendanceN = 112
Class attendance 0 classes attended: 12.5%
Classes attended: M = 5.2 SD = 3.2 (1-8)

Pregnancy
Depressive Symptoms (BDI-II)N = 63 completers
15.6
12.1
5.0
7.58.2
4.6
6.3
8.4
11.9
15.2
0
2
4
6
8
10
12
14
16
18
T1 T2 T3 T4 T5
Intervention(N=32)
Usual Care (N=31)
PostpartumNote: All group differences N.S.

Incidence of Major Depressive Episodes (MDEs) from Baseline to One-year Postpartum
0
2
4
6
8
10
Intervention
Usual Care
3.1%
12.9%
Note: ns

Summary
Preliminary findings from first 63 completers: No differences in the levels of depressive
symptoms between groupsTrend for a difference in MDEs between
groups Feasible to screen and conduct a
preventive group intervention with low-income, pregnant Latinas.

Practice & Policy Implications
Need to integrate mental health prevention into perinatal care
Include ongoing screening and follow-up of high-risk groups
Prevention is important and worthwhile• Decrease stigma• Two-generational approach

Research Team
Co-PI: Deborah Perry (Johns Hopkins University) Coordinator: Adriana Ortiz Research Staff:- Glorimar Ortiz - Carina Viera- Laila Hochhausen - Katherine
Ulrich- Marta Genovez - Swati Singh- Michelle Mackenzie - Julie Wallick- Former staff:
H. Avillán, W. Bamatter, M.L. Berbery, M. Firmino Castillo, A. Chapman, S. Choi, L. Chowdhary, L. Cohen R. Craig, L. DiCesare, M. Hernandez, L. Jacob, L. Matherne, C. Reyes, J. Roman, K. Schaefer, A. Tsega, M. Janes, X. Sheng, C. Quiñonez, M. Vera

www.gwu.edu/[email protected]
DHHS/HRSA/MCHB/Division of Research, Training and EducationR40 MC 02497
Community Partners:
The Mary’s Center for Maternal and Child Care
The Center for Life at Providence Hospital