Embed Size (px)
Citation preview

Management of Management of PreeclampsiaPreeclampsia
Preventing Maternal Mortality and Preventing Maternal Mortality and Morbidity.Morbidity.

What is preeclampsia?What is preeclampsia?
►►Hypertension arising after 20 weeks Hypertension arising after 20 weeks gestation accompanied by evidence of gestation accompanied by evidence of dysfunction in another organ systemdysfunction in another organ system
Most commonly proteinuria (>0.3g/day equiv)Most commonly proteinuria (>0.3g/day equiv)
May also involve other systems/fetusMay also involve other systems/fetus►►NeurologicalNeurological►►LiverLiver►►Placental functionPlacental function►►HaematologicalHaematological
SOMANZ guidelinesSOMANZ guidelines

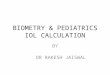
Deaths from preeclampsia Deaths from preeclampsia ––
UK UK confidential enquiry.confidential enquiry.
0
5
10
15
20
25
30
85-87 88-90 91-93 94-96 97-99 00-02 2003-05
absolute number
rate/ milliondeliveries

What type of deaths and are they What type of deaths and are they preventable?preventable?
►► Three major causes are intracerebral Three major causes are intracerebral haemorrhage, cerebral infarction and multiorgan haemorrhage, cerebral infarction and multiorgan failure (including pulmonary oedema).failure (including pulmonary oedema).
►► 13/18 deaths in the UK related to preeclampsia 13/18 deaths in the UK related to preeclampsia were felt to have remediable factorswere felt to have remediable factors
8 deaths felt to have involved major substandard care 8 deaths felt to have involved major substandard care
Blood pressure management was highlightedBlood pressure management was highlighted


Timely and accurate diagnosisTimely and accurate diagnosis
►► Antenatal screening for preeclampsia Antenatal screening for preeclampsia ––
requires requires access to antenatal care.access to antenatal care.
►► Recognition of hypertension and proteinuriaRecognition of hypertension and proteinuria►► Appropriate next investigationsAppropriate next investigations
Recognising the rare preeclampsia like conditions that Recognising the rare preeclampsia like conditions that require alternative management.require alternative management.
Recognising atypical preeclampsiaRecognising atypical preeclampsia

Avoiding disaster Avoiding disaster ––
right place, right right place, right time, right person.time, right person.
►►
Admission to hospital for initial assessment and planning.Admission to hospital for initial assessment and planning.
Unpredictability of disease courseUnpredictability of disease course
Assess severity, rate of progression and allows for acute Assess severity, rate of progression and allows for acute intervention for fulminating diseaseintervention for fulminating disease
►►
Not delaying admission and assessmentNot delaying admission and assessment
►►
Experienced clinician determining diagnosis and instituting Experienced clinician determining diagnosis and instituting managementmanagement
Requires senior staff led services and appropriate clinical stafRequires senior staff led services and appropriate clinical staff f education.education.

The definitive management of The definitive management of preeclampsiapreeclampsia
is delivery!!!is delivery!!!
►► Reasonable evidence now that delivery is indicated Reasonable evidence now that delivery is indicated for all women who have for all women who have preeclampsiapreeclampsia
at >37/40 at >37/40
completed weeks.completed weeks.
►► All women with severe, rapidly progressive All women with severe, rapidly progressive preeclampsiapreeclampsia
should be delivered in a timely should be delivered in a timely
fashion. Those remote from term need fashion. Those remote from term need multidisciplinary, senior team management.multidisciplinary, senior team management.
Include obstetrician, Include obstetrician, anaethetistanaethetist, physician, midwifery , physician, midwifery and and paediatricpaediatric
staff.staff.

HYPITAT trialHYPITAT trial
►►
Lancet 2009; 374: 979Lancet 2009; 374: 979--8888
►►
Singleton pregnancy, >36 weeks gestation with nonSingleton pregnancy, >36 weeks gestation with non--severe severe preeclampsiapreeclampsia
or gestational hypertensionor gestational hypertension
RandomisedRandomised
to IOL to IOL vsvs
expectant management (delivery when severe expectant management (delivery when severe maternal or fetal disease evident)maternal or fetal disease evident)
Poor maternal outcome higher in expectant management group (44% Poor maternal outcome higher in expectant management group (44% vsvs 31%).31%).
Neonatal outcome unchangedNeonatal outcome unchanged
Lower CS rate in IOL groupLower CS rate in IOL group
►►
Low numbers in <37 week group Low numbers in <37 week group ––
but gave good support to but gave good support to immediate IOL for women over 37 weeks with any form of new onsetimmediate IOL for women over 37 weeks with any form of new onset
hypertensive disease in pregnancy.hypertensive disease in pregnancy.

When to deliver?When to deliver?
►► >37 weeks>37 weeks►► Uncontrolled BPUncontrolled BP►► Deteriorating platelet Deteriorating platelet
count, count, LFTsLFTs, renal , renal functionfunction
►► Neurological symptoms Neurological symptoms or or eclampsiaeclampsia
►► Pulmonary Pulmonary oedemaoedema►► Placental abruptionPlacental abruption
►► Severe IUGRSevere IUGR►► NonNon--reassuring fetal reassuring fetal
statusstatus

Severe Severe preeclampsiapreeclampsia
►► Right place/right personRight place/right person
HDU level care with 1:1 nursing/midwifery care and HDU level care with 1:1 nursing/midwifery care and senior clinician roundsenior clinician round
►► Expectant management in remote from term Expectant management in remote from term patients (<28/40)patients (<28/40)
Any progression of maternal disease must initiate Any progression of maternal disease must initiate delivery.delivery.
Neonatal steroids are important BUT maternal wellbeing Neonatal steroids are important BUT maternal wellbeing must take precedence.must take precedence.

What sort of monitoring?What sort of monitoring?
►► If initially stable and less than 36 weeksIf initially stable and less than 36 weeks
Twice weekly bloodsTwice weekly bloods
Regular assessment of fetal/maternal wellbeing Regular assessment of fetal/maternal wellbeing ––
daily daily roundsrounds
Outpatient monitoring Outpatient monitoring ––►► for mild disease but need compliant patient and for mild disease but need compliant patient and organisedorganised
day day
stay unitstay unit
Repeat estimations of Repeat estimations of proteinuriaproteinuria
levels, once they are levels, once they are abnormal, not clinically useful abnormal, not clinically useful ––
PCR reasonably reliable PCR reasonably reliable
and can avoid 24 hour collection.and can avoid 24 hour collection.

Preventing disastrous BP eventsPreventing disastrous BP events
►► Management of Blood PressureManagement of Blood Pressure
Aim <159/99 in all womenAim <159/99 in all women►►Lower in women with low booking BPLower in women with low booking BP
Agents used to treat less important than achieving the Agents used to treat less important than achieving the result requiredresult required►►Aim to reach target BP inside one hourAim to reach target BP inside one hour
Team need to be familiar with iv/SL therapyTeam need to be familiar with iv/SL therapy
Invasive monitoring of BP useful for severe Invasive monitoring of BP useful for severe preeclampsiapreeclampsia
only if facilities/nursing staff available.only if facilities/nursing staff available.
Stay with the patient!!!!Stay with the patient!!!!

Management of acute severe Management of acute severe hypertension hypertension --
somanzsomanz
DoseDose RouteRoute Onset of Onset of actionaction
LabetololLabetolol 2020--50mg50mg iv bolus over iv bolus over 2 min2 min
5min, repeat 5min, repeat 15mins15mins
NifedipineNifedipine 55--10mg cap10mg cap
1010--20mg20mg
tabtab
OralOral
OralOral
1010--20mins, 20mins, repeat 30minsrepeat 30mins2020--30mins, 30mins, repeat 45 repeat 45 minsmins
HydralazineHydralazine 55--10mg10mg iv bolusiv bolus 20 20 minsmins, repeat , repeat 30mins30mins
DiazoxideDiazoxide 1515--45mg, max 45mg, max 300mg300mg
iv rapid bolusiv rapid bolus 33--5mins, repeat 5mins, repeat 10mins10mins

EclampsiaEclampsia
preventionprevention
►► Combination of BP control and prophylactic Combination of BP control and prophylactic medicationmedication
Magnesium Magnesium sulphatesulphate
drug of choicedrug of choice
►►Consider in all women with severe Consider in all women with severe preeclampsiapreeclampsia►►Risks of Risks of overtreatmentovertreatment
espesp
if renal failureif renal failure
►► Important for those with headache, high BP or any neurological Important for those with headache, high BP or any neurological signs/symptoms.signs/symptoms.
PhenytoinPhenytoin
for those with contraindication to MgSO4for those with contraindication to MgSO4
For mild For mild preeclampsiapreeclampsia
––
NNT = 100 to prevent one NNT = 100 to prevent one
seizure. Decision analysis suggests reasonable to both seizure. Decision analysis suggests reasonable to both treat or not treat.treat or not treat.

Avoiding pulmonary Avoiding pulmonary oedemaoedema
►► Careful management of iv fluids, fluid balance.Careful management of iv fluids, fluid balance.
►► Assessment of clinical fluid status on regular basisAssessment of clinical fluid status on regular basis
O2 saturation monitoring, CXR if neededO2 saturation monitoring, CXR if needed
►► Particular caution in patients withParticular caution in patients with
ObesityObesity
Heart diseaseHeart disease
Respiratory infection/conditions.Respiratory infection/conditions.
Renal diseaseRenal disease

Post partum carePost partum care
►►Often neglectedOften neglected►►Expect the following to happenExpect the following to happen
Worsening of BP over 2Worsening of BP over 2--3 days3 days
Third space fluid returning to circulationThird space fluid returning to circulation
Transient worsening of low platelets, raised Transient worsening of low platelets, raised LFTsLFTs
High risk of High risk of thromboembolismthromboembolism

ConclusionsConclusions
►►Avoid disaster with Avoid disaster with preeclampsiapreeclampsia
RecogniseRecognise
diseasedisease
Right place, right person, timely managementRight place, right person, timely management
Understand the high risks in severe Understand the high risks in severe preeclampsiapreeclampsia
Multidisciplinary team approach to careMultidisciplinary team approach to care
Post natal review.Post natal review.
►►Read the SOMANZ guidelines!!!Read the SOMANZ guidelines!!!