Embed Size (px)
Citation preview

PREVALENCE OF PREOPERATIVE ANEMIA AND TRANSFUSION
PRACTICE IN ADULT ELECTIVE NON-CARDIAC SURGERY: A
PROSPECTIVE SINGLE CENTRE 3 MONTHS AUDIT
VANESSA LOUIS LIONEL LOUIS
DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF THE
REQUIREMENTS FOR THE DEGREE OF MASTER OF
ANESTHESIOLOGY
DEPARTMENT OF ANESTHESIOLOGY
UNIVERSITY OF MALAYA
KUALA LUMPUR
2018
Univers
ity of
Mala
ya

ii
UNIVERSITY OF MALAYA
ORIGINAL LITERARY WORK DECLARATION
Name of candidate: Vanessa Louis Lionel Louis
Registration/Matrics No: MGE140015
Name of Degree: Masters of Anesthesiology
Title of Project Paper/Research Report/Dissertation/ Thesis (“this work”):
Prevalance of Anemia and Transfusion Practice in Adult Elective Non Cardiac
Surgery: A Prospective Single Centre 3 Months Audit
Field of Study:
I do solemnly and sincerely declare that:
(1) I am the sole author/writer of this Work;
(2) This Work is original;
(3) Any use of any work in which copyright exists was done by way of
fair dealing and for permitted purposes and any excerpt or extract from,
or reference to or reproduction of any copyright work has been
disclosed expressly and sufficiently and the title of the Work and its
authorship have been acknowledged in this Work;
(4) I do not have any actual knowledge nor do I ought reasonably to know
that the making of this work constitutes an infringement of any copyright
work;
(5) I hereby assign all and every rights in the copyright to this Work to
the University of Malaya (“UM”), who henceforth shall be owner
of the copyright in this Work and that any reproduction or use in any form
or by any means whatsoever is prohibited without the written consent of
UM having been first had and obtained;
(6) I am fully aware that if in the course of making this Work I have
infringed any copyright whether intentionally or otherwise, I may be
subject to legal action or any other action as may be determined by UM
Candidate’s Signature Date:
Subscribed and solemnly declared before,
Witness’s Signature Date:
Name:
Designation :
Univers
ity of
Mala
ya

iii
ABSTRACT
Background
Anemia is defined as a condition in which the red blood cells or the oxygen
carrying capacity is insufficient to meet the physiological needs. According to WHO
sex based criteria, anemia is diagnosed as less than 13 g/dl for men and less than 12
g/dl for women. We audited patients undergoing elective non cardiac surgeries in our
hospital setting to see the prevalence of anemia, the timing of detection of anemia and
the type of anemia. We also wanted to audit the incidence of transfusion preoperatively,
intraoperatively and post operatively and the transfusion trigger. We also looked into
the complications of blood transfusion and the morbidity and mortality including length
of hospital stay, any death within hospitalization and the 30 day mortality. Elective
procedures likely to be associated with high transfusion use were audited which
included : gynaecological, colorectal, urological and arthroplasty surgeries.
Methods
Our audit was a prospective single centre audit over the period of 3 months,
from December 2017 up to mid March 2018 at the University Malaya Medical Centre,
Kuala Lumpur and got a total of 306 patients. Patients that were included were all
patients above the age of 18 in the following elective gynaecological,
colorectal, urological and arthroplasty surgeries. Pregnant patients, any patients with
American Society of Anaesthesiologists score 6 and all cancelled operations were
excluded. Relevant data was extracted from the Hospital EMR (Electronic Medical
Records). Data that was collected included patients characteristics and comorbiditites,
type of operation and surgical discipline, selected laboratory investigations eg
hemoglobin level, perioperative data for blood loss, blood transfusion, autologous
Univers
ity of
Mala
ya

iv
techniques, post operative transfusion and complications of blood transfusion. We also
measured the mortality and morbidity including length of hospital stay, death within
hospitalization and the 30 days mortality as a secondary outcome for the audit.
Results
Our audit revealed that out of the 306 patients, according to the anemia
definition of hb<13 for males and hb<12 for females, a total of 126 patients
were anemic, 52 were males and 74 females. Out of the 126 anemic patients, 33.3%
had their anemias detected only 1-6 days prior to surgery and none of the anemic
patients had a complete blood profile to determine the type of anemia. As for the
transfusion practice, 17 anemic patients received preoperative blood transfusion, 14
received intraoperative transfusion and 14 also received postoperative transfusion, and
our study showed that persons who were anemic were more likely to receive blood
transfusions. Morbidity and mortality of our study revealed that patients were anemia
experienced more complications compared to those were not anemic, anemic patients
were significantly associated with infections (p value: 0.0024) and cardiac
complications (p value: 0.011) during their postoperative stay in the hospital.
There was also significant difference in median for their length of stay in hospital
between patients who were anemic (4 days) and patient who were not anemic (2 days).
Conclusion
A larger population of patients should have been audited over a longer duration
of time to determine a better incidence and prevalence of anemia, transfusion practices
and morbidity and mortality in our centre. From our study, it shows that incidence and
prevalence of anemia is significant in our population and they show a higher need for
Univers
ity of
Mala
ya

v
blood transfusion. Also those anemic patients had more postoperative complications
and longer hospital stays. It is important to note these findings so that we can work our
way towards the formation of a patient blood management protocol for our centre.
Univers
ity of
Mala
ya

vi
ABSTRAK
Latar belakang
Anemia ditakrifkan sebagai suatu keadaan di mana sel darah merah atau kapasiti
penyimpanan oksigen tidak mencukupi untuk memenuhi keperluan fisiologi. Menurut
kriteria berdasarkan seks WHO, anemia didiagnosis kurang dari 13 g / dl untuk lelaki
dan kurang daripada 12 g / dl untuk wanita. Kami telah mengaudit pesakit yang
menjalani pembedahan bukan jantung elektif di hospital kami untuk melihat kelaziman
anemia, masa pengesanan anemia dan jenis anemia. Kami juga ingin mengaudit
kejadian transfusi sebelum pembedahan,semasa pembedahan dan selepas pembedahan
dan pencetus transfusi. Kami juga melihat komplikasi pemindahan darah dan morbiditi
dan mortaliti termasuk tempoh penginapan hospital, mana-mana kematian di hospital
dan kematian dalam tempoh 30 hari. Prosedur elektif yang mungkin dikaitkan dengan
penggunaan pemindahan darah yang tinggi telah diaudit dan termasuk: pembedahan
ginekologi, kolorektal, urologi dan pembedahan sendi tulang.
Metodologi
Pengauditan kami adalah prospektif pusat audit tunggal dalam tempoh 3 bulan,
dari Disember 2017 hingga pertengahan Mac 2018 di Pusat Perubatan Universiti
Malaya, Kuala Lumpur dan mendapat sejumlah 306 pesakit. Pesakit yang dimasukkan
adalah semua pesakit yang berumur diatas 18 tahun dalam pembedahan elektif
ginekologi, pembedahan kolorektal, urologi dan pembedahan sendi tulang. Pesakit
hamil, mana-mana pesakit dengan Persatuan Anaesthesiologi Amerika skor 6 dan
semua pembedahan yang dibatalkan dikecualikan. Data yang berkaitan telah diekstrak
dari Hospital EMR (Rekod Perubatan Elektronik). Data yang dikumpulkan termasuk
Univers
ity of
Mala
ya

vii
ciri-ciri pesakit dan komorbiditit, jenis pebedahan dan disiplin pembedahan,
penyiasatan makmal terpilih seperti paras hemoglobin, data perioperatif untuk
kehilangan darah, pemindahan darah, teknik autologous, transfusi pasca operasi dan
komplikasi pemindahan darah. Kami juga mengukur kematian dan morbiditi termasuk
tempoh penginapan hospital, kematian dalam hospital dan kematian 30 hari sebagai
hasil menengah untuk audit.
Keputusan
Audit kami mendedahkan bahawa daripada 306 pesakit, menurut anemia
definisi hb <13 untuk lelaki dan hb <12 untuk perempuan, sejumlah 126 pesakit
didiagnosa anemia, 52 adalah lelaki dan 74 perempuan. Daripada 126 pesakit anemia,
33.3% mempunyai anemia yang dikesan hanya 1-6 hari sebelum pembedahan dan tidak
ada pesakit anemia yang mempunyai profil darah lengkap untuk menentukan jenis
anemia. Bagi amalan transfusi, 17 pesakit anemia mendapat pemindahan darah sebelum
pembedahan, 14 menerima pemindahan ketika pembedahan dan 14 juga menerima
transfusi selepas pembedahan, dan kajian kami menunjukkan bahawa pesakit yang
mengalami anemia lebih cenderung menerima pemindahan darah. Morbiditi dan
kematian kajian kami mendedahkan bahawa pesakit anemia mengalami komplikasi
yang lebih tinggi berbanding dengan yang tidak didiagnosa anemia.
Pesakit anemia juga menunjukkan lebih cenderung mengalami jangkitan (p nilai:
0.0024) dan komplikasi jantung (p nilai: 0.011) semasa mereka berada di hospital
selepas pembedahan. Terdapat perbezaan yang signifikan dalam median untuk tempoh
tinggal mereka di hospital antara pesakit yang mengalami anemia (4 hari) dan pesakit
yang tidak anemia (2 hari).
Univers
ity of
Mala
ya

viii
Kesimpulan
Populasi pesakit yang lebih besar sepatutnya telah diaudit sepanjang tempoh
yang lebih lama untuk menentukan kejadian yang lebih baik dan kelaziman anemia,
amalan transfusi dan morbiditi dan mortaliti di pusat kami. Dari kajian kami, ia
menunjukkan bahawa kejadian dan kelaziman anemia adalah penting dalam populasi
kita dan mereka menunjukkan keperluan yang lebih tinggi untuk pemindahan darah.
Juga pesakit anemia mempunyai lebih banyak komplikasi selepas pembedahan dan
tinggal di hospital lebih banyak hari. Adalah penting untuk perhatikan penemuan ini
supaya kita boleh melakukan perjalanan ke arah pembentukan protokol pengurusan
darah pesakit untuk pusat kami.
Univers
ity of
Mala
ya

ix
ACKNOWLEDGEMENTS
I would like to take this opportunity to first thank God for placing me exactly
where I am today, because without Him I am nothing. I am overjoyed that He gave me
the opportunity to be in the Masters programme and is still seeing me through my
studies and my raising of a family
I would also like to thank my two supervisors Dr Carolyn Yim and Dr Chloe
Ng who tirelessly helped throughout this process, who gave me so much of advice and
who patiently guided me through the audit and my thesis writing. Their dedication,
effort and time is deeply appreciated and I will be forever indebted to them.
I wouldn’t be where I am today if not for my father, mother and sisters who has
always prayed for me and helped give me motivation to carry on. My heartfelt gratitude
to them for all they are to me.
A huge thank you also to my dear husband Yohen who has helped me with my
thesis and encouraged me not to give up and who has supported and sacrificed a lot so
that I can finish my masters programme.
To my babies Everly and Micah, you are the reason for everything. I love u two
deeply.
And last but certainly not the least, I would like to take this opportunity to thank
all the patients involved in this audit, as without them this will not be possible.
Univers
ity of
Mala
ya

x
TABLE OF CONTENTS
Abstract…………………………………………………………………….....iii
Abstrak…………………………………………………………………...…...vi
Acknowledgements………………………………………………………...…ix
Table of Contents………………………………………………………………x
List of Figures…………………………………………………………..……..xi
List of Tables…………………………………………………………………xii
List of Symbols and Abbreviations………………………………......………xiii
List of Appendices……………………………………………………...……xiv
CHAPTER 1 : INTRODUCTION……………………………………………..1
CHAPTER 2 : LITERATURE REVIEW……………………………….……..3
CHAPTER 3 : METHODOLOGY…………………………………………….6
CHAPTER 4 : RESULTS………………………………………………...……8
CHAPTER 5 : DISCUSSION…………………………………………….…..15
CHAPTER 6 : CONCLUSION………………………………………………17
References……………………………………………………………..……..18
Appendix……………………………………………………………………20
Univers
ity of
Mala
ya

xi
LIST OF FIGURES AND TABLES
TABLE 1………………………………………………………………………………8
TABLE 2.…………………………………………………………………………….11
TABLE 3……………………………………………………………………………..12
TABLE 4……………………………………………………………………………..14
FIGURE 1……………………………………………………………………………...9
FIGURE 2……………………………………………………………………………...9
FIGURE 3…………………………………………………………………………….10
FIGURE 4…………………………………………………………………………….10
Univers
ity of
Mala
ya

xii
LIST OF SYMBOLS AND ABBREVIATIONS
WHO : World Health Organization
HB : Hemoglobin
EMR : Electronic Medical Record
UMMC : University Malaya Medical Centre
PBM : Patient Blood Management
ASA : American Society of Anaesthesiologists
HIV : Human Immunodeficiency Virus
USA : United States of America
Univers
ity of
Mala
ya

xiii
LIST OF APPENDICES
APPENDIX A……………………………………………………….……….20
Univers
ity of
Mala
ya

1
CHAPTER 1: INTRODUCTION
According to WHO, anemia is defined as a condition where the number of red
blood cells or their oxygen carrying capacity is unable due to insufficiency so as to meet
the basic physiological needs which varies with a person’s age, gender, altitude, smoking,
behavior and pregnancy [1]. Iron deficiency anemia is the most common cause of anemia
globally [1]. For men hemoglobin <13 g/dl is anemia and for women hemoglobin levels
less than 12 g/dl is anemic. Table 1.1 shows the hemoglobin levels to diagnose anemia at
sea level.
Each year more than 230million patients undergo surgery world wide[4].Anemia
is the most common hematological problem in the preoperative patient and often, it is a
sign of an underlying disease or condition that could affect the surgical outcome[5].
Consequently, blood transfusions are commonly given perioperatively to anemic patients.
Perioperatively, anemia can be encountered at anytime. Patients hospitalized for
surgery may have an underlying anemia or blood loss during surgery can cause anemia
[2]. The etiology of preoperative anemia may be multifactorial and complex. Nutritional
deficiencies and some drugs may contribute to reduced red blood cell production [3].
There are many other causes for preoperative anemia for example activation of the
immune system by underlying processes as well as certain inflammatory cytokines that
can decrease RBC half life due to dyserythropoiesis[3]. Repeated diagnostic
phlebotomies, gastrointestinal or genitourinary blood loss, coagulopathies and
hemodilution can also contribute to development of anemia.
Many studies have shown that preoperative anemia is associated with poorer
patient outcomes (length of hospital stay, post operative complications and
death)[3].Transfusion outcomes include higher mortality, more ischemic complications,
Univers
ity of
Mala
ya

2
organ dysfunction, infections, delayed wound healing and increased length of hospital
stay[6].
The concept of patient blood management was introduced to promote best practice
in the timely detection and management of preoperative anemia[4].
Our audits primary outcome was to find out the prevalence of anemia among
patients who are scheduled for elective non-cardiac surgery, timing of detection of anemia
and the type of anemia. Our secondary outcome was to see the incidence of transfusion
preoperatively, intra operatively, post operatively and the transfusion trigger. We also
looked into complications of blood transfusion and morbidity and mortality including
length of hospital stay, death within hospitalization and 30 days mortality in our centre
UMMC in the span of 3 months.
The information from this audit is planned to be used to come up with a PBM
protocol which is defined as a timely application of evidence based medicine and surgical
concepts designed to maintain hemoglobin concentration, optimize hemostasis and
minimize blood loss in an attempt to improve patient outcome for our centre.
Univers
ity of
Mala
ya

3
CHAPTER 2: LITERATURE REVIEW
There is so much importance in finding out the prevalence of preoperative anemia
as it can show its correlation with increase in mortality or morbidity preoperatively, effects
of transfusion, transfusion practices and could also be used as a foundation for the
planning of a PBM protocol and many others. Anemia is defined by WHO as Hb < 13g/dl
in non pregnant females and Hb< 12g/dl in males. According to Klein et al (2016) there
is considerable evidence that preoperative anemia is associated with poor surgical
outcomes in non cardiac surgical patients[7].
Beattie et al (2009) undertook a single centre retrospective cohort study to
determine the independent association between preoperative anemia and mortality after
non-cardiac surgery. Data were collected on 7760 consecutive adult patients from March
2003 to June 2006. All patients receiving patient-controlled analgesia, patient-controlled
epidural anesthesia, epidural, and intravenous pain management were included,
comprising virtually all patients having major surgery. Patients having emergent surgery
were excluded. For patients who underwent more than one relevant procedure during the
study period, only their initial surgery was included for analysis. Transplantation and
cardiac surgery cases were excluded. They found that preoperative anemia was a highly
prevalent condition that was strongly and independently associated with postoperative
mortality. Fully one-third of patients who presented for non emergent surgery had a
hemoglobin concentration that the World Health Organization would define as anemia.
They noted that patients with preoperative anemia had more than two-fold greater odds of
dying within 90 days of surgery[8]
Carson JL et al(1996) did a retrospective cohort study on the effect of anemia and
cardiovascular disease on surgical mortality and morbidity. The primary outcome was 30-
day mortality and the secondary outcome was 30-day mortality or in-hospital 30-day
Univers
ity of
Mala
ya

4
morbidity. Cardiovascular disease was defined as a history of angina, myocardial
infarction, congestive heart failure, or peripheral vascular disease. Findings were the 30-
day mortality was 3.2%. The mortality was 1.3% in patients with preoperative hemoglobin
12 g/dL or greater and 33.3% in patients with preoperative hemoglobin less than 6 g/dL.
The increase in risk of death associated with low preoperative hemoglobin was more
pronounced in patients with cardiovascular disease than in patients without. The effect of
blood loss on mortality was larger in patients with low preoperative hemoglobin than in
those with a higher preoperative hemoglobin. The results were similar in analyses of
postoperative hemoglobin and 30-day mortality or in-hospital morbidity[9].
C bernard et al(2009) conducted a study entitled intraoperative transfusion of 1u
to 2u packed red blood cells is associated with increased 30 day mortality, surgical site
infection, pneumonia and sepsis in general surgery patients. The results showed that 1u
RBC significantly increased risk of 30 day mortality, composite morbidity, pneumonia
and sepsis/shock. Transfusion of 2u increased risk for these outcomes plus surgical site
infection.
W Scott Beattie et al (2009) conducted an observational study to measure the
prevalence of anemia and assess the relationship between preoperative anemia and
postoperative mortality[11] The results of the study showed that preoperative anemia was
common and equal between genders and was associated with a 5 fold increase in post
operative mortality and was concluded that although anemia increases mortality
independent of transfusion, it is associated with increased in requirement for transfusion
which is also then associated with increased mortality.
Univers
ity of
Mala
ya

5
According to a single institution, large case controlled study conducted by Jessica
Viola et al in 2015 to examine the association between preoperative anemia and adverse
outcomes following total joint arthroplasty, anemic patients had a higher rate of
complications namely cardiovascular [12]. The study confirmed that patients with
preoperative anemia are likely to exhibit a higher incidence of post operative
complications following total joint arthroplasty.
Gregory MT Hare et al [2013] wrote an article entitled risks of anemia and related
management strategies: can perioperative blood management improve patient safety? The
conclusion of the article was that ongoing initiatives to treat anemias and optimize patient
blood management may improve patient outcomes.
Univers
ity of
Mala
ya

6
CHAPTER 3: METHODOLOGY
We undertook a prospective single center audit over the period of 3 months from
December 2017 to March 2018. The subjects were patients undergoing elective non-
cardiac surgery, which included the gynecology, urology, colorectal, and arthroplasty
disciplines of surgery. Since this was an observational study without any intervention,
consent from patients was not required.
Inclusion criteria were patients aged above 18 years old undergoing surgery in the
gynecology, urology, colorectal and arthroplasty disciplines.
Exclusion criteria was any cancellation of surgery, pregnant patients and patients
with ASA score 6
All patients who were eligible for the audit was identified through the daily
elective operation list, relevant data was extracted from the hospital EMR and the patients
were followed up through the hospital admission period up to 30 days post operation.
Patient’s characteristics and comorbidities, name of operation and surgical
category, selected laboratory investigations (hemoglobin level, hematocrit, red blood cell
indices, serum ferritin etc) are recorded.
Perioperative data for allogeneic blood transfusion, transfusion trigger, blood loss,
anesthetic technique and involvement of autologous technique are recorded. All
information was added onto a paper case report form.
Complications of blood transfusion eg: febrile reaction, hemolytic reaction
(acute/delayed), transfusion associated circulatory overload, transfusion related acute lung
Univers
ity of
Mala
ya

7
injury, transfusion related bacterial sepsis (contamination) and transfusion transmitted
infection like hepatitis, HIV etc was recorded
Secondary outcome measured the 30 days mortality and morbidities which
included events affecting the cardiovascular system (acute coronary syndromes, cardiac
arrest necessitating cardiopulmonary resuscitation), respiratory system (pneumonia,
ventilator support more than 48hrs, unplanned intubation), vascular/thrombotic
complications (deep vein thrombosis or pulmonary embolism), renal system (acute or
progressive renal failure), neurological system (stroke) , infection, hemorrhage and
duration of hospital stay.
Data were analyzed using SPSS version 21.00 (Chicago, IL, USA). Numerical
variable were presented using mean and standard deviation if the data were normally
skewed; while median and interquartile range were used to present skewed numerical data.
Categorical variables were presented using frequency and percentage. Pearson Chi-square
was used to test the association between anemic status and the incidence of peri-operative
blood transfusion. In order to test the association between anemic status and patients’
outcomes (morbidity and mortality), several analyses such as Pearson Chi-Square, Fisher
Exact test and Mann Whitney U test were employed. Level of significance is set at p <
0.05.
CHAPTER 4: RESULTS
Univers
ity of
Mala
ya

8
A total number of 306 patients were recruited in our study from December 2017
to March 2018. Table 1 shows the characteristics of the study population. Out of the 306
patients, 126 patients were anemic. The majority of patients belonged to the middle age
group with mean age of 56 years old. The anemic patients at 57.34 years old and the non-
anemic patients at 55.45 years old. In our study there were 106 male patients, where 52
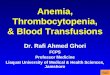
were anemic and 200 female patients where 74 were anemic. Figure 1 shows a pie chart
on the gender distribution among all the patients. Out of the 126 anemic patients 58.7%
were females. This could also be due to the fact that most of our patients were from the
gynecology discipline, a total number of 145 out of the 306 patients (47.1%). 7.8% of
patients were from the arthroplasty discipline, 10.4% from colorectal and 34.1% form the
urology discipline. Figure 2 depicts the different disciplines covered. Most of the patients
were from ASA 2 category (59.7%) and out of the 306 patients, 208 patients were seen
preoperatively in our anesthesia clinic and 98 patients were not seen as shown on Figure
4.
Table 1: Characteristics of study population (n=306)
SD: standard deviation
All
(n=306)
Anemia
(n=126)
Non-anemic
(n=180)
Age, Mean (SD) 56.23 (16.33) 57.34 (17.69) 55.45 (15.31)
Gender
Male
Female
106 (34.4)
200 (64.9)
52 (41.3)
74 (58.7)
54 (30.0)
126 (70.0)
Discipline
Gynecology
Arthroplasty
Colorectal
Urology
145 (47.1)
24 (7.8)
32 (10.4)
105 (34.1)
50 (39.7)
8 (6.3)
19 (15.1)
49 (38.9)
95 (52.8)
16 (8.9)
13 (7.2)
56 (31.1)
ASA
I
II
III
74 (24.0)
184 (59.7)
48 (15.6)
27 (21.4)
72 (57.1)
27 (21.4)
47 (26.1)
112 (62.2)
21 (11.7)
Pre-op anesthesia
assessment
Yes
No
208 (67.5)
98 (31.8)
76 (60.3)
50 (39.7)
132 (73.3)
48 (26.7)
Univers
ity of
Mala
ya

9
Figure 2: Pie chart based on the different disciplines (n=306)
47%
8%11%
34%
Discipline
Gynaecology
DJR
Colorectal
Urology
Univers
ity of
Mala
ya

10
Univers
ity of
Mala
ya

11
The time of detection for the anemic status of the patients were computed.
Majority of the anemic patients were detected one to six days prior to surgery (33.3%),
mostly during the pre-operative assessment after hospitalization. There were 28 (22.2%)
of patients detected with anemia 7-13 days prior to surgery, followed by 30 (23.8%)
patients detected 14-20 days prior to surgery, 8 patients were detected 21-27 days prior to
surgery, 3 patients detected 35 to 41 days prior to surgery and 11 patients detected more
than 42 days prior to surgery. Table 2 shows the time of detection of anemia.
Table 2: Time of detection of anemia (n=126)
Variable Frequency (%)
Time of detection
1-6 days prior surgery
7-13 days prior surgery
14-20 days prior surgery
21-27 days prior surgery
28-34 days prior surgery
35-41 days prior surgery
≥ 42 days prior surgery
42 (33.3)
28 (22.2)
30 (23.8)
8 (6.3)
4 (3.2)
3 (2.4)
11 (8.7)
From our audit, we also wanted to determine if the anemic patients were
investigated to determine the type of anemia they had, however all the anemic patients did
not have a complete blood profile to determine their type of anemia for example not all
were investigated if they had thalassemia, vitamin b12 deficiency, folate deficiency or
iron deficiency anemia.
For the incidence of pre-operative, intra-operative and post operative transfusion,
Pearson Chi-square was used in this study after assumption checking and found met and
showed that most of the patients did not receive blood transfusion pre-operatively
(94.2%), intra-operatively (92.5%) and post-operatively (93.8%). However, there was
more incidence on the need of blood transfusion intra-operatively compared to pre-
Univers
ity of
Mala
ya

12
operation and post-operation. There were 23 cases on blood transfusion intra-operatively,
18 cases pre-operatively and 19 cases post operatively.
Pearson Chi-square was used to test the association on the anemic status of
patients and the need of blood transfusion. Results were significant for all phases: pre-
operation (p value: <0.001), intra-operation (p value: 0.046) and post-operation (p value:
0.003). Patients who were anemic were more likely to receive blood transfusion compared
to patients who were not anemic. These findings are depicted in table 3
Table 3: Incidence of pre-operative, intra-operative and post-operative transfusion
(N=306)
Variable All
(n=306)
Anemia
(n=126)
Non-anemic
(n=180)
p-value
Pre-op
Yes
No
18 (5.8)
290 (94.2)
17 (13.5)
109 (86.5)
1 (0.6)
179 (99.4)
<0.001
Intra-op
Yes
No
23 (7.5)
285 (92.5)
14 (11.1)
112 (88.9)
9 (5.0)
171 (95.0)
0.046
Post-op
Yes
No
19 (6.2)
289 (93.8)
14 (11.1)
112 (88.9)
5 (2.8)
175 (97.2)
0.003
Pearson’s Chi square
Another outcome from the study that we wanted to analyze were the complications
of blood transfusion, however out of all the patients who received transfusion, none of
them developed any documented complications towards blood transfusion.
As for the morbidity, mortality and length of hospital stay, assumption checking
was done before the analysis as well. Mann-Whitney U test was used in this study, as the
normality assumption was not met. Expected count was checked before the decision was
made whether to use Pearson Chi-square or Fisher Exact test. Pearson Chi-square was
used when the expected count more than five is more than 20% of the cell while Fisher
Exact test was used when the expected count less than five is more than 20% of the cell.
Univers
ity of
Mala
ya

13
The morbidity and mortality of the patients were computed in Table 4. In general, patients
who has anemia experience more complications compared to patients who were not
anemic. There were 3 anemic patients who passed away, and one patient who was not
anemic died during hospitalization.
Pearson Chi-square and Fisher Exact test were used to test the association
between the anemic status and patient’s outcome (complications, death during
hospitalization and mortality within 30 days). Mann-Whitney U test was used to test the
difference in hospital stay among patients who were and were not anemic. Anemic status
of patients was significantly associated with infections (p value: 0.0024), and cardiac
complications (p value: 0.011). While for the length of stay, there were significant
difference in median between patients who were anemic (4 days) and patient who were
not anemic (2 days) (p value: 0.003). Hence, anemic patients tend to have longer hospital
stays according to our audit.
Univers
ity of
Mala
ya

14
Table 4: Morbidity and mortality of study population (n=306)
Variable All
(n=306)
Anemia
(n=126) Non-anemic
(n=180) p-value
Complication
Infection
Yes
No
Cardiac
Yes
No
Respiratory
Yes
No
Gastrointestinal
Yes
No
Renal
Yes
No
Other
Yes
No
18 (5.8)
285 (92.5)
5 (1.6)
298 (96.8)
8 (2.6)
294 (95.5)
3 (1.0)
300 (97.4)
11 (3.6)
292 (94.8)
11 (3.6)
292 (94.8)
12 (9.5)
113 (89.7)
5 (4.0)
120 (95.2)
6 (4.8)
118 (93.7)
3 (2.4)
122 (96.8)
8 (6.3)
117 (92.9)
7 (5.6)
118 (93.7)
6 (3.3)
172 (95.6)
0 (0.0)
178 (98.9)
2 (1.1)
176 (97.8)
0 (0.0)
178 (98.9)
3 (1.7)
175 (97.2)
4 (2.2)
174 (96.7)
0.024c
0.011d
0.068d
0.069d
0.056d
0.210d
Length of hospitalization 4.00 (4.00) 4.00 (7.00) 3.00 (3.00) 0.003e
Death during
hospitalization
Yes
No
4 (1.3)
298 (96.8)
3 (2.4)
121 (96.0)
1 (0.6)
177 (98.3)
0.309d
Mortality within 30 days
Yes
No
4 (1.3)
297 (96.4)
3 (2.4)
120 (95.2)
1 (0.6)
177 (98.3)
0.308d
aMedian (IQR); bFrequency (%); cPearson Chi-Square test; dFisher Exact test; eMann-
Whitney U test
Univers
ity of
Mala
ya

15
CHAPTER 5: DISCUSSION
From our study, it showed that out of the 306 patients, 126 patients were anemic
equating to about 41.7%. Out of the 126 patients, 74 females. This could have been due
to the fact that the largest group of patients was from the gynecology discipline, which
were all female patients. It was also shown that 98 out of the total 306 patients were not
seen in the anesthesia clinic for preoperative assessment and 50 of those not seen were
anemic. It was also revealed that out of all the anemic patients most of them were only
detected to have anemia 1-6 days prior to their surgery, only 11 were detected more than
42 days prior to surgery. The results also showed patients who were anemic were more
likely to receive blood transfusions compared to patients who were not anemic. Also the
anemic patients experienced more complications and out of the 4 patients who passed
away, 3 of them were anemic. Anemic patients also were showed to have a longer duration
of hospital stay.
From this results, some of the improvements that could have been done were, a
larger population of patients should have been audited over a longer duration of time to
determine a better incidence and prevalence of anemia, transfusion practices and
morbidity and mortality in our center and also other disciplines could also have been
included. This would give us a bigger sample and more accurate and better results could
have been seen.
We could also advice all disciplines to send all patients going for operations for
preoperative assessment so that earlier detection of anemia could happen. It is vital to
detect and treat anemia as we could see in the results that anemic patients have more
complications and longer duration of hospital stay which will then require more hospital
resources being used. Anemic patients were also found to have more complications
Univers
ity of
Mala
ya

16
compared to the non anemic ones, thus the importance of detecting anemia earlier and
treating it.
More thorough investigations need to be done to determine the cause of anemia,
from our study out of 126 anemic patients, none of them had a full blood workout to
determine the cause of their anemia.
From our study and its results we can see the importance of detecting anemia and
treating it as many lives could be saved as preoperative anemia was associated with poorer
patient outcomes. This study can be used as a stepping stone to the development of a
patient blood management protocol for UMMC and would need cooperation from all
disciplines to work together and help detect and come up with the proper treatment for
preoperative anemia.
Univers
ity of
Mala
ya

17
CHAPTER 6: CONCLUSION
Anemia is one of the most common hematological problems preoperatively and
has been shown to affect the surgical outcome. It is of grave importance to detect anemia
preoperatively and to manage it accordingly to reduce the incidence of intraoperative
transfusion, which can lead to poorer surgical outcomes, which then predisposes the
patients to longer hospital stay and more healthcare resources being used.
A larger population of patients should have been audited over a long duration of
time to determine a better incidence and prevalence of anemia, transfusion practices and
morbidity and mortality in our center. From our study, it shows that incidence and
prevalence of anemia is significant in our non-cardiac surgical patients and they show a
higher need for blood transfusion. Also those anemic patients had more postoperative
complications and longer hospital stays.
It is important to note these findings as it showed increase in hospital mortality
and worse outcomes in anemic patients. Using the results of this study, we can come up
with a patient blood management protocol to help in the management and treatment of
preoperative anemia, which can then reduce mortality and reduce usage of hospital
resources.
Univers
ity of
Malaya

18
REFERENCES
Beattie, W., Karkouti, K., Wijeysundera, D. N., & Tait, G. (2009). Risk Associated with
Preoperative Anemia in Noncardiac Surgery. Anesthesiolgoy, 110(3), 574-581.
Doi” 10.1097/aln.0b013e31819878d3
Bernard, A., Davenport, D., Chang, P., Vaughan, T., & Zwschenberger, J. (2009).
Intraoperative Transfusion of 1 U to 2 U Packed Red Blood Cells Is Associated
with Increased 30-Day Mortality, Surgical-Site Infection, Pneumonia, and Sepsis
in General Surgery Patients. Journal of the American College of Surgeons, 208(5),
931-937.e2. doi: 10.1016/j.jamcollsurg.2008.11.019
Carson, J., Duff, A., Poses, R., Berlin, J., Spence, R., & Trout, R. et al. (1996). Effect of
anaemia and cardiovascular disease on surgical mortality and morbidity. The
Lancet, 348(9034), 1055-1060. Doi: 10.1016/s0140-6736(96)04330-9
Hare, G., Freedman, J., & David Mazer, C. (2013). Review article: Risks of anemia and
related management strategies: can perioperative blood management improve
patient safety? Canadian Journal of Anesthesia/Journal Canadien D’anesthesie,
60(2), 168-175. Doi: 10.1007/s12630-012-9861-y
Klein, A., Collier, T., Brar, M., Evans, C., Hallward, G., Fletcher, S., & Richards, T.
(2016). The incidence and importance of anaemia in patients undergoing cardiac
surgery in the UK - the first Association of Cardiothoracic Anaesthetists national
audit. Anaesthesia, 71(6), 627-635. Doi: 10.1111/anae.13423
Manuel Munoz, Susana Gomez-Ramirez. Pre-operative anaemia: prevalence,
consequences and approaches to management. Blood Transfus.2015 Jul; 13(3):
370-379
Organization, W. (2019). Haemoglobin concentrations for the diagnosis of anaemia and
assessment of severity. Retrieved from
http://apps.who.int/iris/handle/10665/85839
Patel, M., & Carson, J. (2009). Anemia in the Preoperative Patient. Medical Clinics of
North America, 93(5), 1095-1104. doi: 10.1016/j.mcna.2009.05.007
Shander, A., Knight, K., Thurer, R., Adamson, J., & Spence, R. (2004). Prevalence and
outcomes of anemia in surgery: a systematic review of the literature. The
American Journal of Medicine, 116(7), 58-69. doi:
10.1016/j.amjmed.2003.12.013
Spahn, D., Theusinger, O., & Hofmann, A. (2012). Patient blood management is a win-
win: a wake-up call. British Journal of Anaesthesia, 108(6), 889-892. doi:
10.1093/bja/aes166
Univers
ity of
Mala
ya

19
Viola, J., Gomez, M., Restrepo, C., Maltenfort, M., & Parvizi, J. (2015). Preoperative
Anemia Increases Postoperative Complications and Mortality Following Total
Joint Arthroplasty. The Journal of Arthroplasty, 30(5), 846-848. doi:
10.1016/j.arth.2014.12.026
Univers
ity of
Mala
ya