Embed Size (px)
Citation preview

Prevalence, mortality and socio-economic outcome in Turner syndrome
Claus H. GravholtDepartment of Endocrinology and Internal MedicineDepartment of Molecular MedicineAarhus University HospitalDenmark

Who am I?
• I started working with Turner syndrome already in medschool in the last millenium
• I am an adult endocrinologist working with rarer endocrine conditions
• I have performed numerous studies in kids, adolescents and adults with Turner syndrome
• Also used epidemiology, genetics, cardiology, MR radiology and more
• I am also the father of 5 kids

What is Turner syndrome in 2014?
• Decreased final height, >95%• Gonadal dysgenesis
– no puberty– infertility– chronic estrogen insufficiency– androgen insufficiency
• Endocrine disturbances• Psychosocial problems• Physical abnormalities• And much more………………………….

The heart?Socio-economic conditions?
Diagnosis? Mortality and morbidity?

Genetics

SHOX – part of an explanation!
short 4th metacarpal cubitus valgus Madelung deformity mesomelic growth high arched palate micrognathia sensorineural deafness dysproportionality of skeletal size
Consequence:

Height, skeletal anomalies
Height, gonads, lesserphysical features
Viability
Gonadal dysgenesis
SHOX(ZFX)
(USP9X)
(RPS4X)
(DIAPH2)
p
q
Gene (candidate)Phenotype
Critical regions for TS phenotype on the X chromosome
X

SHOX effects
Ottesen et al, Am J Med Genet, 152A: 1206-1212, 2010
Marchini et al, Hum Mol Genet, 16:3081-3087, 2007
SHOX – homeodomain transcription factorNPPB is a transcriptional target – encodesBNP, which is known as a cardiac and natriuretichormoneInvolved in growth of hypertrophic chondrocytes
Clement-Jones et al, Hum Mol Genet, 9:695-702, 2000
SHOX2SHOX SOX9
X chromosome inactivation (XCI)
• In each cell either the paternal or the maternal X is inactivated
• Initiation of XIC is controlled by Xist• X chromosome: ~1100 genes• Y chromosome: ~100 genes
Heard and Disteche, Genes Dev 20:1848, 2006

Early letality – placental factor
Urbach et al, PloS ONE 4:e4175, 2009
CSF2RAColony-stimulatingfactor 2 receptoralpha
Encodes the α subunit of the receptor of the granulocyte-macrophagecolony-stimulatingfactor
Essential for normal placental development

When are patients diagnosed? And how many are eligible for GH?
Delay in diagnosis / years
80706050403020100
120
100
80
60
40
20
0
Range = 0-86 yearsMedian = 15 years
N = 746
Number
Stochholm et al, J Clin Endocrinol Metab, 2006

Age at diagnosis – effect of karyotype
Age at Diagnosis
0 20 40 60 80
Number
0
20
40
60
80
100
120
140
160
180
45,XIsochromosome XqOther karyotypes
Median age at diagnosis:45,X: 13.3 (95% CI: 12.1 - 14.2) yearsIso Xq: 14.2 (12.4 - 16.2) yearsOther karyotypes: 19.1 (17.8 - 21.9) years
Stochholm et al, J Clin Endocrinol Metab, 2006

Prevalence of TS – closing the gap?
Year
1970 1975 1980 1985 1990 1995 2000
Observed andexpectednumber of TSdiagnoses
0
200
400
600
800
1000
1200
1400
1600
Stochholm et al, J Clin Endocrinol Metab, 2006

How good are we at diagnosis?
• Median age - 1999:• 15.1 years (14.5-15.8) range 0-85.5
• Median age - 2008:• 15.1 years (14.5-15.9) range 0-85.5
Stochholm et al, J Clin Endocrinol Metab, 2006Stochholm et al, unpublished data

Swedish data on diagnosis
Age at diagnosis Stigmata• 45,X 9.6 10.1• 45,X/46,XX 17.6 6.4• Isochromosome 11.6 9.3• X-marker 11.0 9.6• Y-marker 14.6 9.6• Ring chromosome 8.7 9.2
• N=126El-Mansoury et al, Clin Endocrinol, 66:744-751, 2007

How many suffer from TS?
• 50 per 100,000 females• About 1300 in Denmark• 125,500 in EU
• 78,000 in USA
• 5500 in Australia – about 1300 in Sydney

Europe
• Denmark: 900/5,400,000, expected 1350 – relative percentage: 67%
• Sweden: 900/9,000,000, expected 2250– relative percentage: 40%
• UK: 5000/62,000,000, expected 15500– relative percentage: 32%

Rate of abortion
• 2008: 28 prenatally diagnosed / 20 abortions• 2009: 15 prenatally diagnosed / 13 abortions• 2010: 20 prenatally diagnosed / 18 abortions• 2011: 26 prenatally diagnosed / 20 abortions
• 2008-2011: 89 / 71 = 80% abortion rate
Viuff et al., unpublished data

Prenatal conditonsNuchal Fold vs Gestational age in Turner syndrome
Gestational age /days
75 80 85 90 95 100
Nu
ch
al fo
ld /
mm
0
2
4
6
8
10
12
14
16
45,X Controls (mean)95%CI45,X - diagnosed postnatally Viuff et al., unpublished data
Mortality in TS
British registry study of 400 TS and 62 deaths RR: 4.2 (95% CI 3.2 – 5.4) Causes: nervous, cardiovascular, digestive and
genitourinary systems Specific causes: epilepsy, IHD, aortic dissection,
pneumonia, cong. heart disease No gonadoblastoma deaths Bias: ascertainment, cause of mortality
Swerdlow et al., Ann Hum Genet, 65:177-188, 2001

Mortality in TS SMR – 2.86 (95% CI 2.26 – 3.62) Endocrine diseases, SMR: 5.68 Coronary diseases, SMR: 3.47 Congenital anomalies, SMR: 24.09 No increased cancer mortality
1970-1979, SMR: 4.68 1980-1989, SMR: 2.86 1990-1999, SMR: 2.49, test for trend p=0.08
Stochholm et al, J Clin Endocrinol Metab, 2006

Mortality in TS
Age
0 20 40 60 80
Survival
0.0
0.2
0.4
0.6
0.8
1.0
45,X
Isochromosomes
Otherkaryotypes
Backgroundpopulation
Stochholm et al, J Clin Endocrinol Metab, 2006

Mortality
Schoemaker et al, JCEM (2008).

Mortality
Schoemaker et al, JCEM (2008).

Quality of life and socio-economy

• TS persons– Quality of life Normal
– Higher education Increased– Married Fewer– Health problems Increased
– Children ?– Income ?– Retirement ?
Turner syndrome - questionnaires
Carel 2005, Verlinde 2004, Naess 2009, Bannink 2006, Cunnif 1995

Material and methods
• Danish Cytogenetic Central Registry
• 997 Turner syndrome persons identified
• 94.883 controls (age and gender)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Materials and methods
• Statistics Denmark– Cohabitation– Income– Education– Children– Retirement
– Mortality
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Statistical approach
• Hazard ratios– Total
– Before the diagnosis Turner syndrome– After the diagnosis Turner syndrome
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Cohabitation
• First partner
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Age (years)
20 30 40 50 60 70
Proportion with partner
0.0
0.2
0.4
0.6
0.8
1.0
p<0.001
Turner
Controls
HR: 0.4 (0.4-0.5)
Cohabitation
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Children
• First child
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Children
Age (years)
20 30 40 50
Proportion with firstchild
0.0
0.2
0.4
0.6
0.8
1.0
Controls
Others
45,X
45,X/46,XX
HR: 0.2 (0.2-0.2)p<0.001
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Income
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Income
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Retirement
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Retirement
Age (years)
20 30 40 50 60 70
Proportion retired
0.0
0.2
0.4
0.6
0.8
1.0
p<0.001
ControlsTurner
HR: 1.8 (1.5-2.2)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Retirement
Age (years)
20 30 40 50 60 70
Proportion retired
0.0
0.2
0.4
0.6
0.8
1.0
p<0.001
ControlsTurner
HR: 1.8 (1.5-2.2)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Education
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
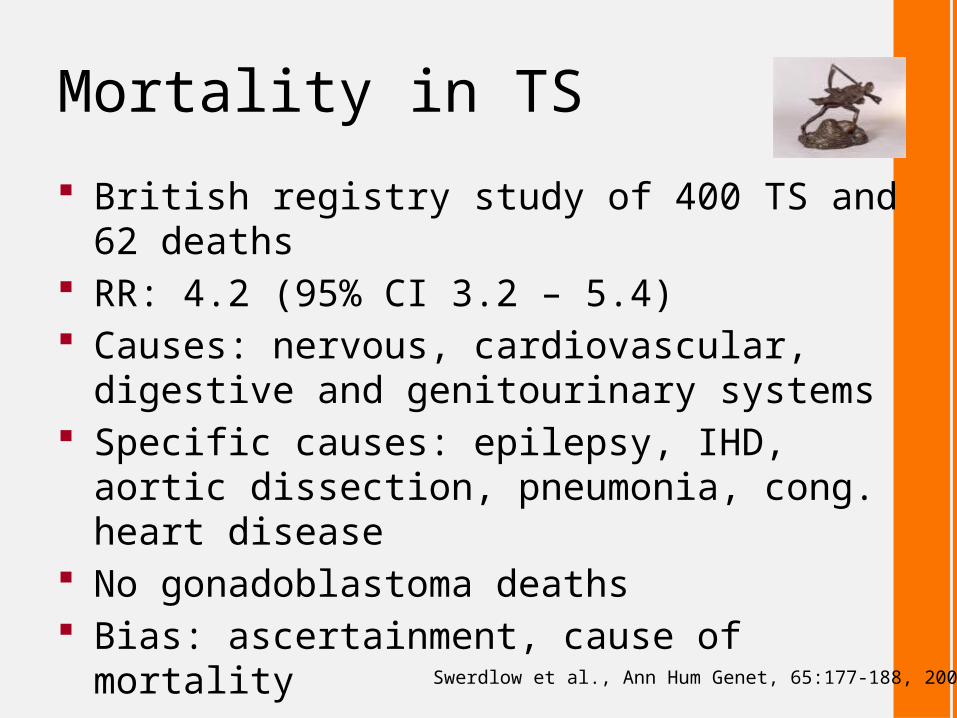
Education
• Hazard ratios– Total 1.0 (0.9-1.2)
– Before the diagnosis 0.9 (0.7-1.1)– After the diagnosis 1.1 (0.9-1.3)
Controls Turner syndrome p-value controls compared to all TS
Number with at least one higher
education (%)
16,018(32.5)
193(34.5)
0.98

Mortality
Hazard ratio, log scale
1 10 100 1000
ICD-10 chapter
Trauma (10/393)
Symptoms not elsewhere classified (2/267)
Congenital anomalies and genetic disorders (15/21)
Diseases in the perinatal period (2/0)
Diseases of the genitourinary system (2/68)
Diseases of the musculoskeletal system (1/40)
Diseases of the skin (1/5)
Diseases of the digestive system (3/244)
Diseases of the respiratory system (3/432)
Diseases of the cardiovascular stystem (35/1,869)
Diseases of the nervous system (4/116)
Psychiatric diaseases (2/126)
Endocrine, nutritional and metabolic diseases (6/153)
Malignant neoplasms (22/1,647)
Infectious and parasitic diseases (1/50)
Total (114/6,035)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Mortality
• Hazard ratios– Total 3.2 (2.6-3.8)
– Adjusted education and retirement 2.9 (2.4-3.6)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

Conclusion
• Divergent socio-economic profile with little impact on the increased mortality
• No major differences between karyotype groups• The reason for the reported high quality of life may be due to a
”coping” mechanism• Note: number of mothers• Note income• Note education
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012

US Turner syndrome women
• N=240 females
Gould et al, J Women Health, 22:230, 2013

The heart in TS
Mortensen et al, Endocrine Reviews, 33:677-714, 2012

Congenital malformations
• 70-80% of a given Turner syndrome population will have a congenital malformation!
Matura et al, Circulation, 116:1663, 2007; Mortensen et al, Cardiol Young, 20:191, 2010

Summary
• Epidemiology tells us a lot about Turner syndrome
• However, only scant data on GH and HRT and long term outcome
• How to interfere with hypertension, heart disease and other disease?
• Continued studies are necessary

Turner syndrome clinics
o Dedicatedo Multi disciplinaryo Anchored in one departmento Implementation of international guidelines on
a national basiso … but a still a need for further research on a
number of issues!

Recommendation
• Screening – everybody at diagnosis– Evaluation by cardiologist– Full investigation including blood pressure– Echocardiography, especially in younger girls– MRI and Echo in older girls and adults
• Continuous monitoring – follow-up dependent of clinical situation– Re-evaluation at transition, before pregnancy,
hypertension, etc.– Or every 5-10 year
Clinical Practice Guideline, J Clin Endocrinol Metab, 92:10-25, 2007

Pregnancy work-up
• Pre-pregnancy screening:– MRI af the heart and great vessels– Hypertension– Hypothyreosis, diabetes, vitamin D, celiac disease
• During pregnancy:– Echocardiography in first and last trimester, MRI if
necessary, hypothyreosis, diabetes, vitamin D• After pregnancy:
– hypothyreosis, diabetes, vitamin D

Adult medical follow-up
o Blood pressure, heart auskultation and echocardiography, MRI
o Thyroid status, coeliac screeno Body composition status (BMI<25), including
physical exercise and diet instructiono Blood sugar, lipid profile, and liver enzymeso Osteoporosis surveillanceo Otological examinationo Urinary screening

Treatment
o Female sex steroid substitution with natural estrogens (17β-estradiol) and gestagens
o Male sex steroid substitution ?o GH substitution ?o Tight control of blood pressure (beta-blocker or
other drugs?)o Prevention of obesity and other lifestyle diseaseso Regular visits in outpatient clinics (internal
medicine, gynaecology or other specialists with an interest in the syndrome)

Information bookAvailable on the internet – http://www.medical-research.dk/turner-know-your-body/

Take-home message
Turner syndrome is often diagnosed late (or never)
Metabolic disease is frequentHypothyroidism is seen in 50%Type 2 diabetes is frequentHRT can prevent osteoporosisHeart disease is frequentThe natural history is still not unravelledMorbidity and mortality is clearly increased