Embed Size (px)
Citation preview

Research in Developmental Disabilities 35 (2014) 3071–3080
Contents lists available at ScienceDirect
Research in Developmental Disabilities
Prevalence and factors associated with polypharmacy in
Victorian adults with intellectual disabilitySyed Imran Haider a,*, Zahid Ansari b, Loretta Vaughan a, Helen Matters c,Eric Emerson d
a Health Intelligence Unit, Victorian Government Department of Health, 50 Lonsdale Street, Melbourne, Victoria 3000, Australiab School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australiac Service Design and Implementation Group, Victorian Government Department of Human Services, 50 Lonsdale Street, Melbourne,
Victoria 3000, Australiad Centre for Disability Research & Policy, University of Sydney, Australia
A R T I C L E I N F O
Article history:
Received 6 June 2014
Received in revised form 28 July 2014
Accepted 29 July 2014
Available online
Keywords:
Intellectual disability
Developmental disability
Pharmacoepidemiology
Medicine use
Polypharmacy
A B S T R A C T
Although polypharmacy is a medication safety concern leading to increased risk of non-
adherence, adverse drug reaction and drug–drug interactions, polypharmacy and
associated risk factors has rarely been investigated involving people with ID at a
population level. The purpose of this paper is to analyze the prevalence of polypharmacy
and to evaluate the role of different factors associated with polypharmacy in a state-wide
representative population of adults with ID. In a population-based survey in Victoria,
Australia, 897 people with ID 18 years of age or older were selected by simple random
sampling. The data were collected from proxy respondents on behalf of people with ID.
Polypharmacy was defined as the concomitant use of five or more medications. The data
were weighted to reflect the age/sex/geographic distribution of the population. Results
revealed that more than 76% of adults with ID had used prescribed medicine and about 21%
were exposed to polypharmacy in the last two weeks. In both univariate and multivariate
analyses, polypharmacy was significantly associated with older age, unemployment and
inability to get help from family and friends if needed. After controlling for age, sex and
severity of intellectual disability, polypharmacy was associated with having a blood
pressure, blood cholesterol and blood glucose level check. Polypharmacy was also
associated with a greater number of visits to general practitioners, fair or poor reported
health status and inability to walk unaided. Subjects with epilepsy, diabetes, stroke,
osteoporosis and cancer had a higher probability of polypharmacy. None of the disease
inducing behaviors was associated with polypharmacy. This study highlights the need that
medication should be regularly reviewed overall in ID population and particularly when
polypharmacy exists.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Polypharmacy is a medication safety concern, as it is associated with the risk of developing adverse drug reactions,undesirable drug–drug interactions, hospitalization, medication non-adherence, poorer quality of life and of premature
* Corresponding author. Tel.: +61 3 90960000; fax: +61 3 90969176.
E-mail addresses: [email protected], [email protected] (S.I. Haider).
http://dx.doi.org/10.1016/j.ridd.2014.07.060
0891-4222/� 2014 Elsevier Ltd. All rights reserved.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–30803072
mortality (Lunsky & Elserafi, 2012; Passarelli, Jacob-Filho, & Figueras, 2005; Stortz, Lake, Cobigo, Ouellette-Kuntz, & Lunsky,2014; Straetmans, van Schrojenstein Lantman-de Valk, Schellevis, & Dinant, 2007). While polypharmacy may be necessaryfor the treatment of multiple co-morbid health conditions, in other cases it may represent inappropriate prescribing, whichitself represents a substantial clinical and economic burden for both patients and society (Simonson & Feinberg, 2005).
People with ID have high rates of premature mortality, morbidity and comorbidity (Emerson & Hatton, 2013; Havemanet al., 2010; Krahn & Fox, 2013; Hara, McCarthy, & Bouras, 2010; Oeseburg, Dijkstra, Groothoff, Reijneveld, & Jansen, 2011;Van Schrojenstein Lantman-de Valk, 2005). Given the high prevalence of comorbid conditions such as epilepsy, hyperactivitydisorder, schizophrenia, bipolar disorder, anxiety, depression, sleep disorders and gastrointestinal problems (Levy, Mandell,& Schultz, 2009; Mahan et al., 2010), people with ID are likely to be prescribed a variety of medicines and experiencepolypharmacy (Straetmans et al., 2007).
According to a recent review, there is a lack of consensus on the methods used to study polypharmacy includingmeasurements, definitions of polypharmacy, study samples and analytical methods (Stortz et al., 2014). Although there is noclear consensus on the definition of polypharmacy, one of the most commonly used definitions is the concurrent use of fiveor more drugs (Haider, Johnell, Weitoft, Thorslund, & Fastbom, 2009; Linjakumpu et al., 2002; Veehof, Stewart, Haaijer-Ruskamp, & Jong, 2000).
The prevalence of polypharmacy among people with ID varies considerably, ranging from 11% to 60% (Stortz et al., 2014).This variability in prevalence of polypharmacy may be due to different study methods and analytics used, makingcomparisons difficult across different studies. This evidence base may also be criticized on two important counts (Stortzet al., 2014). First, the majority of studies are based on small scale convenience or clinical-based samples, making it difficultto generalize the findings to the wider ID population. Second, there is a lack of studies examining factors associated withpolypharmacy to understand why the prevalence of polypharmacy differs within populations. For example, studies in peoplewho do not have ID have shown that factors associated with polypharmacy include older age, female gender, low education,institutional living, poor self-reported health, high number of visits to health professionals and dementia (Agostini, Han, &Tinetti, 2004; Haider, Johnell, Thorslund, & Fastbom, 2008; Haider et al., 2009; Jyrkka, Enlund, Korhonen, Sulkava, &Hartikainen, 2009; Pitkala, Strandberg, & Tilvis, 2001).
To our knowledge, no study has investigated polypharmacy (concurrent use of five or more drugs) and associated factorsin a representative ID population. The aims of this study were to describe the prevalence of medicine use and polypharmacy(defined in this study as use of five or more drugs) and to investigate the role of different factors associated withpolypharmacy in a representative population of people with intellectual disability living in the state of Victoria, Australia.
2. Methods
The design, data source, and sampling frame reflect the population based and cross sectional nature of the study.
2.1. Design and data source
The data used in this study were obtained from state-wide population health survey; the ‘Victorian Population HealthSurvey of people with an Intellectual Disability 20090 (VPHS-ID 2009). The VPHS-ID 2009 was the first population levelsurvey in Victoria, Australia for people with intellectual disability and was designed to provide information on the health andwellbeing of the population to inform policy and planning.
A public health model of the social determinants of health, provided the theoretical framework for the VPHS-ID andinformed the development of the questionnaire (Ansari, Carson, Ackland, Vaughan, & Serraglio, 2003). Essentially the modelpredicts that the underlying social determinants of health, which include socioeconomic determinants, psychosocial riskfactors and community and societal characteristics (social determinants), impact on the health of the individuals (healthoutcomes) both directly and indirectly via the healthcare system and disease-inducing behaviors (Ansari et al., 2003).
2.2. Sampling frame
The VPHS-ID 2009 was a cross sectional study conducted by the Victorian Department of Health with data collected fromproxy respondents between October and December 2009. The VPHS-ID 2009 sampling plan was designed to yield state-widerepresentative estimates that would generalize to all people with intellectual disability aged 18 years and over living inVictoria.
A full description of details about design, recruitment and representativeness of the sample, as well as diagnosticmethods, has been published elsewhere (Department of Health, 2008, 2011; Haider, Ansari, Vaughan, Matters, & Emerson,2013). An administrative database of people with ID who had previously sought assistance from the Victorian Department ofHuman Services was used as the sampling frame for the VPHS-ID 2009. The database contained information onapproximately 21,210 people aged 18 years and over who were listed on the administrative database and resided in Victoriaand had ID as either a primary or secondary condition (0.5% of the resident adult population of Victoria). 7106 recruitmentpackages were mailed to a randomly selected sample of people aged 18 years and over with ID. 897 people with ID, and theirproxy respondents agreed to participate, giving a response rate of 14% of people with whom contact was made. The overallparticipation rate defined as completed interviews divided by people who agreed to participate in the survey was 90.7%.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–3080 3073
Analysis weights were applied to the data so that estimates generalize to people with intellectual disability aged 18 yearsand over living in Victoria.
2.3. Data collection
The telephone interviews were conducted with proxy respondents on behalf of 897 people with ID. A proxy respondentwas someone who knew the person with ID well enough to answer detailed questions about that person’s health, wellbeingand daily routine. Proxy respondents included disability support workers, family members, close friends, advocates or casemanagers. Data on medicine use was collected by the trained telephone interviewers of a market research company who hadhad experience in interviewing carers and people with disabilities. The interviewers contacted the nominated proxyrespondent and scheduled a telephone interview. Pharmacist checked the quality of medicine use data. Interviews inlanguages other than English were undertaken where required (eight interviews). The interview questions were posted inadvance to proxy respondents to assist them in preparing for their telephone interviews. These questions also includedinstructions to gather medicines information used by the person with intellectual disability. Proxy respondents wereencouraged to discuss these questions with the person with intellectual disability to gather the latest information.
2.4. Measures and variables
During the interview information on the participants’ sociodemographic background, health and lifestyle includingasthma, diabetes, alcohol and tobacco consumption, fruit and vegetable consumption, physical activity, obesity, chronicdiseases and social networks were recorded.
In this study, medicine use refers to the use of prescribed medicine in the past two weeks. Most studies have definedpolypharmacy according to the number of medications taken by the patient (Haider et al., 2009; Linjakumpu et al., 2002;Veehof et al., 2000). For this study, polypharmacy was defined as the concurrent use of five or more prescribed medicines. Noinformation was collected about the name and dose of medicine used.
Age was categorized into three groups: 18–39 years (reference), 40–59 years, and 60 years and over. Type of residentialarea was stratified into metropolitan and rural.
Survey respondents were asked a series of questions about physical activity. A respondent was deemed to have engagedin sufficient physical activity if he/she had accrued 150 or more minutes of moderate intensity physical activity (such aswalking) on a regular basis over one week. This is the recommended threshold of physical activity according to the NationalPhysical Activity Guidelines for Australians (DoHA, 1999).
The body mass index (BMI) provides a measure of weight in relation to height and can be used to estimate levels ofunhealthy weight in a population. It is calculated as weight in kilograms divided by height in metres squared (WHO, 2000).BMI 25–<30 kg/m2 was classified as overweight and BMI �30 kg/m2 was classified as obese.
Survey respondents were asked about their average daily fruit and vegetable consumption. A respondent was deemed tohave met the Australian guidelines for fruit and vegetable consumption if they consumed at least two serves of fruit and fiveserves of vegetables per day (NHMRC, 2003).
Reported health was measured on a five point scale. For this study, reported health status was classified into the followingthree classes: excellent/very good, good, and fair/poor.
Respondents were also asked whether people with ID had at any time in their life been told by a doctor that they had anyof the following conditions: heart disease, epilepsy, depression, diabetes, stroke, osteoporosis, arthritis, cancer, currentasthma, vision impairment, and hearing impairment. These conditions were coded as present or absent.
Survey measures social capital using a cohesion-based approach and indicators used included: ability to get help fromfamily, friends or neighbors, ability to get care in an emergency and access to community resources.
2.5. Data analysis
The survey data were weighted to reflect the age, sex and geographic distribution of the population aged 18 years andolder, as estimated from the administrative database. In order to eliminate the effect that differences in age structure mayhave on estimates from different population groups, the estimates were age-standardized to the 2006 estimated residentialpopulation, using the direct method of age-standardization (ABS, 2006).
The data obtained from this study are expressed as proportions for prevalence estimates of drug use and polypharmacy.The significance of differences in prevalence estimates for polypharmacy was evaluated by determining whether the pointestimate lay within or outside the 95 percent confidence intervals (95% CI) of the relevant comparison estimate. Thereliability of estimates had been determined using relative standard errors (RSEs), with RSEs less than 25% deemed to bereliable for general use.
Logistic regression was performed to determine the factors associated with polypharmacy with either: (1) a singledependent variable and a single independent variable (simple logistic regression) reporting unadjusted odds ratios (OR) and95% confidence intervals (CI); or (2) with a single dependent variable and multiple independent variables (multiple logisticregression) reporting adjusted OR and 95% CI. In multiple logistic regression model adjustment was made for age, sex andseverity of ID. We were unable to adjust for all significant variables associated with polypharmacy at the univariate analyses
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–30803074
in a single logistic regression model due to small numbers, as the adjusted model does not converge well, leading to lack ofprecision in the estimates and their standard errors (wide 95% CIs). The Hosmer–Lemeshow goodness-of-fit statistic wasapplied to test the data’s fit to the model. In this study, p-values of<0.05 were considered statistically significant. Data wereanalyzed using Stata statistical software version 12.0 (StataCorp, College Station, Texas, USA).
The public health model of the social determinants of health provided the framework for reporting of results in this paper(Ansari et al., 2003).
2.6. Ethical standards
The Victorian Department of Human Services, Human Research Ethics Committee approved the survey method andquestionnaire content.
3. Results
3.1. Study population
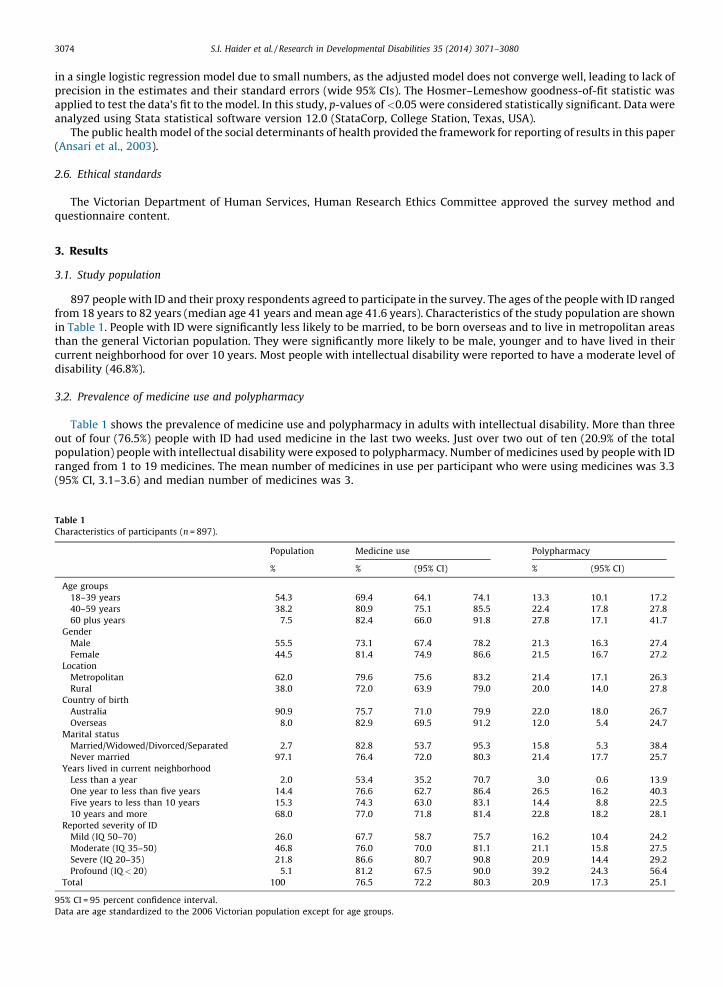
897 people with ID and their proxy respondents agreed to participate in the survey. The ages of the people with ID rangedfrom 18 years to 82 years (median age 41 years and mean age 41.6 years). Characteristics of the study population are shownin Table 1. People with ID were significantly less likely to be married, to be born overseas and to live in metropolitan areasthan the general Victorian population. They were significantly more likely to be male, younger and to have lived in theircurrent neighborhood for over 10 years. Most people with intellectual disability were reported to have a moderate level ofdisability (46.8%).
3.2. Prevalence of medicine use and polypharmacy
Table 1 shows the prevalence of medicine use and polypharmacy in adults with intellectual disability. More than threeout of four (76.5%) people with ID had used medicine in the last two weeks. Just over two out of ten (20.9% of the totalpopulation) people with intellectual disability were exposed to polypharmacy. Number of medicines used by people with IDranged from 1 to 19 medicines. The mean number of medicines in use per participant who were using medicines was 3.3(95% CI, 3.1–3.6) and median number of medicines was 3.
Table 1
Characteristics of participants (n = 897).
Population Medicine use Polypharmacy
% % (95% CI) % (95% CI)
Age groups
18–39 years 54.3 69.4 64.1 74.1 13.3 10.1 17.2
40–59 years 38.2 80.9 75.1 85.5 22.4 17.8 27.8
60 plus years 7.5 82.4 66.0 91.8 27.8 17.1 41.7
Gender
Male 55.5 73.1 67.4 78.2 21.3 16.3 27.4
Female 44.5 81.4 74.9 86.6 21.5 16.7 27.2
Location
Metropolitan 62.0 79.6 75.6 83.2 21.4 17.1 26.3
Rural 38.0 72.0 63.9 79.0 20.0 14.0 27.8
Country of birth
Australia 90.9 75.7 71.0 79.9 22.0 18.0 26.7
Overseas 8.0 82.9 69.5 91.2 12.0 5.4 24.7
Marital status
Married/Widowed/Divorced/Separated 2.7 82.8 53.7 95.3 15.8 5.3 38.4
Never married 97.1 76.4 72.0 80.3 21.4 17.7 25.7
Years lived in current neighborhood
Less than a year 2.0 53.4 35.2 70.7 3.0 0.6 13.9
One year to less than five years 14.4 76.6 62.7 86.4 26.5 16.2 40.3
Five years to less than 10 years 15.3 74.3 63.0 83.1 14.4 8.8 22.5
10 years and more 68.0 77.0 71.8 81.4 22.8 18.2 28.1
Reported severity of ID
Mild (IQ 50–70) 26.0 67.7 58.7 75.7 16.2 10.4 24.2
Moderate (IQ 35–50) 46.8 76.0 70.0 81.1 21.1 15.8 27.5
Severe (IQ 20–35) 21.8 86.6 80.7 90.8 20.9 14.4 29.2
Profound (IQ< 20) 5.1 81.2 67.5 90.0 39.2 24.3 56.4
Total 100 76.5 72.2 80.3 20.9 17.3 25.1
95% CI = 95 percent confidence interval.
Data are age standardized to the 2006 Victorian population except for age groups.
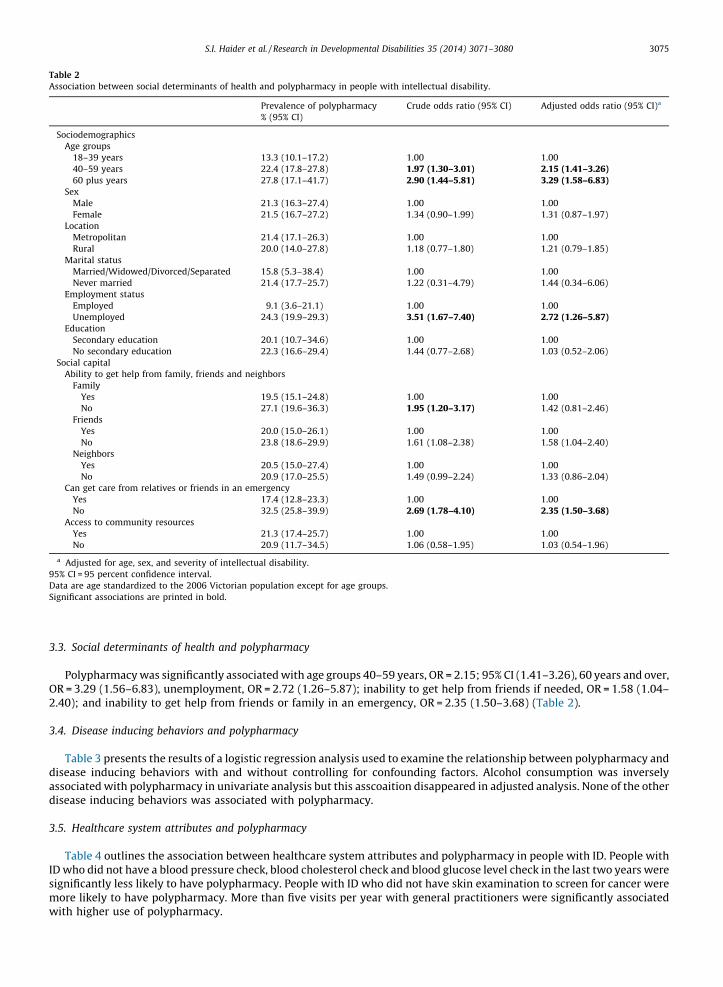
Table 2
Association between social determinants of health and polypharmacy in people with intellectual disability.
Prevalence of polypharmacy
% (95% CI)
Crude odds ratio (95% CI) Adjusted odds ratio (95% CI)a
Sociodemographics
Age groups
18–39 years 13.3 (10.1–17.2) 1.00 1.00
40–59 years 22.4 (17.8–27.8) 1.97 (1.30–3.01) 2.15 (1.41–3.26)60 plus years 27.8 (17.1–41.7) 2.90 (1.44–5.81) 3.29 (1.58–6.83)
Sex
Male 21.3 (16.3–27.4) 1.00 1.00
Female 21.5 (16.7–27.2) 1.34 (0.90–1.99) 1.31 (0.87–1.97)
Location
Metropolitan 21.4 (17.1–26.3) 1.00 1.00
Rural 20.0 (14.0–27.8) 1.18 (0.77–1.80) 1.21 (0.79–1.85)
Marital status
Married/Widowed/Divorced/Separated 15.8 (5.3–38.4) 1.00 1.00
Never married 21.4 (17.7–25.7) 1.22 (0.31–4.79) 1.44 (0.34–6.06)
Employment status
Employed 9.1 (3.6–21.1) 1.00 1.00
Unemployed 24.3 (19.9–29.3) 3.51 (1.67–7.40) 2.72 (1.26–5.87)Education
Secondary education 20.1 (10.7–34.6) 1.00 1.00
No secondary education 22.3 (16.6–29.4) 1.44 (0.77–2.68) 1.03 (0.52–2.06)
Social capital
Ability to get help from family, friends and neighbors
Family
Yes 19.5 (15.1–24.8) 1.00 1.00
No 27.1 (19.6–36.3) 1.95 (1.20–3.17) 1.42 (0.81–2.46)
Friends
Yes 20.0 (15.0–26.1) 1.00 1.00
No 23.8 (18.6–29.9) 1.61 (1.08–2.38) 1.58 (1.04–2.40)
Neighbors
Yes 20.5 (15.0–27.4) 1.00 1.00
No 20.9 (17.0–25.5) 1.49 (0.99–2.24) 1.33 (0.86–2.04)
Can get care from relatives or friends in an emergency
Yes 17.4 (12.8–23.3) 1.00 1.00
No 32.5 (25.8–39.9) 2.69 (1.78–4.10) 2.35 (1.50–3.68)Access to community resources
Yes 21.3 (17.4–25.7) 1.00 1.00
No 20.9 (11.7–34.5) 1.06 (0.58–1.95) 1.03 (0.54–1.96)
a Adjusted for age, sex, and severity of intellectual disability.
95% CI = 95 percent confidence interval.
Data are age standardized to the 2006 Victorian population except for age groups.
Significant associations are printed in bold.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–3080 3075
3.3. Social determinants of health and polypharmacy
Polypharmacy was significantly associated with age groups 40–59 years, OR = 2.15; 95% CI (1.41–3.26), 60 years and over,OR = 3.29 (1.56–6.83), unemployment, OR = 2.72 (1.26–5.87); inability to get help from friends if needed, OR = 1.58 (1.04–2.40); and inability to get help from friends or family in an emergency, OR = 2.35 (1.50–3.68) (Table 2).
3.4. Disease inducing behaviors and polypharmacy
Table 3 presents the results of a logistic regression analysis used to examine the relationship between polypharmacy anddisease inducing behaviors with and without controlling for confounding factors. Alcohol consumption was inverselyassociated with polypharmacy in univariate analysis but this asscoaition disappeared in adjusted analysis. None of the otherdisease inducing behaviors was associated with polypharmacy.
3.5. Healthcare system attributes and polypharmacy
Table 4 outlines the association between healthcare system attributes and polypharmacy in people with ID. People withID who did not have a blood pressure check, blood cholesterol check and blood glucose level check in the last two years weresignificantly less likely to have polypharmacy. People with ID who did not have skin examination to screen for cancer weremore likely to have polypharmacy. More than five visits per year with general practitioners were significantly associatedwith higher use of polypharmacy.
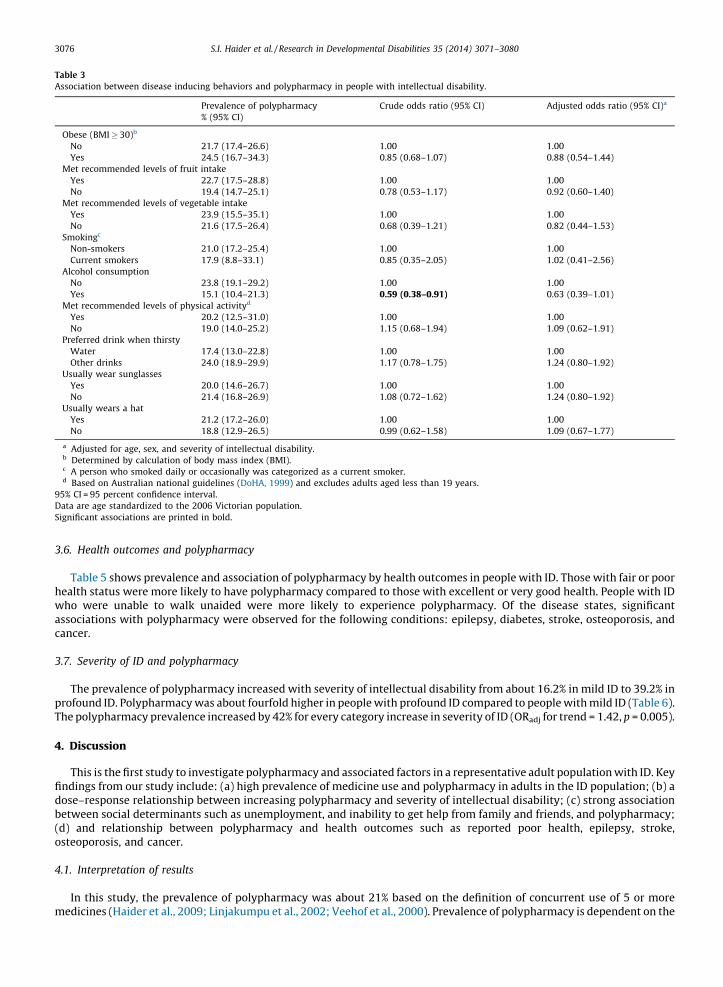
Table 3
Association between disease inducing behaviors and polypharmacy in people with intellectual disability.
Prevalence of polypharmacy
% (95% CI)
Crude odds ratio (95% CI) Adjusted odds ratio (95% CI)a
Obese (BMI� 30)b
No 21.7 (17.4–26.6) 1.00 1.00
Yes 24.5 (16.7–34.3) 0.85 (0.68–1.07) 0.88 (0.54–1.44)
Met recommended levels of fruit intake
Yes 22.7 (17.5–28.8) 1.00 1.00
No 19.4 (14.7–25.1) 0.78 (0.53–1.17) 0.92 (0.60–1.40)
Met recommended levels of vegetable intake
Yes 23.9 (15.5–35.1) 1.00 1.00
No 21.6 (17.5–26.4) 0.68 (0.39–1.21) 0.82 (0.44–1.53)
Smokingc
Non-smokers 21.0 (17.2–25.4) 1.00 1.00
Current smokers 17.9 (8.8–33.1) 0.85 (0.35–2.05) 1.02 (0.41–2.56)
Alcohol consumption
No 23.8 (19.1–29.2) 1.00 1.00
Yes 15.1 (10.4–21.3) 0.59 (0.38–0.91) 0.63 (0.39–1.01)
Met recommended levels of physical activityd
Yes 20.2 (12.5–31.0) 1.00 1.00
No 19.0 (14.0–25.2) 1.15 (0.68–1.94) 1.09 (0.62–1.91)
Preferred drink when thirsty
Water 17.4 (13.0–22.8) 1.00 1.00
Other drinks 24.0 (18.9–29.9) 1.17 (0.78–1.75) 1.24 (0.80–1.92)
Usually wear sunglasses
Yes 20.0 (14.6–26.7) 1.00 1.00
No 21.4 (16.8–26.9) 1.08 (0.72–1.62) 1.24 (0.80–1.92)
Usually wears a hat
Yes 21.2 (17.2–26.0) 1.00 1.00
No 18.8 (12.9–26.5) 0.99 (0.62–1.58) 1.09 (0.67–1.77)
a Adjusted for age, sex, and severity of intellectual disability.b Determined by calculation of body mass index (BMI).c A person who smoked daily or occasionally was categorized as a current smoker.d Based on Australian national guidelines (DoHA, 1999) and excludes adults aged less than 19 years.
95% CI = 95 percent confidence interval.
Data are age standardized to the 2006 Victorian population.
Significant associations are printed in bold.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–30803076
3.6. Health outcomes and polypharmacy
Table 5 shows prevalence and association of polypharmacy by health outcomes in people with ID. Those with fair or poorhealth status were more likely to have polypharmacy compared to those with excellent or very good health. People with IDwho were unable to walk unaided were more likely to experience polypharmacy. Of the disease states, significantassociations with polypharmacy were observed for the following conditions: epilepsy, diabetes, stroke, osteoporosis, andcancer.
3.7. Severity of ID and polypharmacy
The prevalence of polypharmacy increased with severity of intellectual disability from about 16.2% in mild ID to 39.2% inprofound ID. Polypharmacy was about fourfold higher in people with profound ID compared to people with mild ID (Table 6).The polypharmacy prevalence increased by 42% for every category increase in severity of ID (ORadj for trend = 1.42, p = 0.005).
4. Discussion
This is the first study to investigate polypharmacy and associated factors in a representative adult population with ID. Keyfindings from our study include: (a) high prevalence of medicine use and polypharmacy in adults in the ID population; (b) adose–response relationship between increasing polypharmacy and severity of intellectual disability; (c) strong associationbetween social determinants such as unemployment, and inability to get help from family and friends, and polypharmacy;(d) and relationship between polypharmacy and health outcomes such as reported poor health, epilepsy, stroke,osteoporosis, and cancer.
4.1. Interpretation of results
In this study, the prevalence of polypharmacy was about 21% based on the definition of concurrent use of 5 or moremedicines (Haider et al., 2009; Linjakumpu et al., 2002; Veehof et al., 2000). Prevalence of polypharmacy is dependent on the
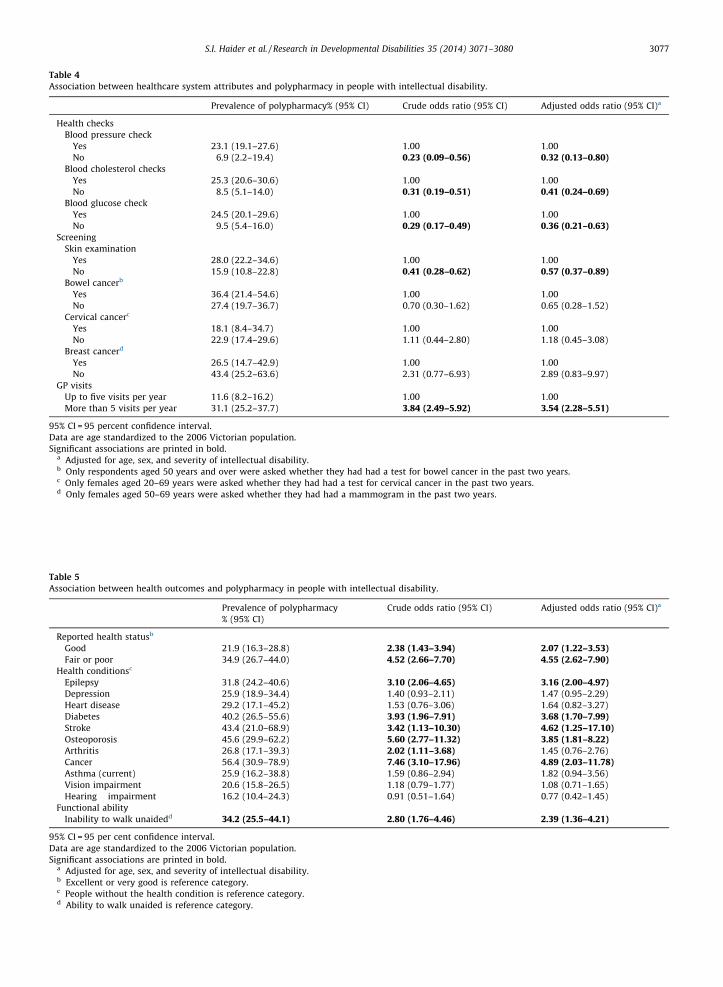
Table 4
Association between healthcare system attributes and polypharmacy in people with intellectual disability.
Prevalence of polypharmacy% (95% CI) Crude odds ratio (95% CI) Adjusted odds ratio (95% CI)a
Health checks
Blood pressure check
Yes 23.1 (19.1–27.6) 1.00 1.00
No 6.9 (2.2–19.4) 0.23 (0.09–0.56) 0.32 (0.13–0.80)Blood cholesterol checks
Yes 25.3 (20.6–30.6) 1.00 1.00
No 8.5 (5.1–14.0) 0.31 (0.19–0.51) 0.41 (0.24–0.69)Blood glucose check
Yes 24.5 (20.1–29.6) 1.00 1.00
No 9.5 (5.4–16.0) 0.29 (0.17–0.49) 0.36 (0.21–0.63)Screening
Skin examination
Yes 28.0 (22.2–34.6) 1.00 1.00
No 15.9 (10.8–22.8) 0.41 (0.28–0.62) 0.57 (0.37–0.89)Bowel cancerb
Yes 36.4 (21.4–54.6) 1.00 1.00
No 27.4 (19.7–36.7) 0.70 (0.30–1.62) 0.65 (0.28–1.52)
Cervical cancerc
Yes 18.1 (8.4–34.7) 1.00 1.00
No 22.9 (17.4–29.6) 1.11 (0.44–2.80) 1.18 (0.45–3.08)
Breast cancerd
Yes 26.5 (14.7–42.9) 1.00 1.00
No 43.4 (25.2–63.6) 2.31 (0.77–6.93) 2.89 (0.83–9.97)
GP visits
Up to five visits per year 11.6 (8.2–16.2) 1.00 1.00
More than 5 visits per year 31.1 (25.2–37.7) 3.84 (2.49–5.92) 3.54 (2.28–5.51)
95% CI = 95 percent confidence interval.
Data are age standardized to the 2006 Victorian population.
Significant associations are printed in bold.a Adjusted for age, sex, and severity of intellectual disability.b Only respondents aged 50 years and over were asked whether they had had a test for bowel cancer in the past two years.c Only females aged 20–69 years were asked whether they had had a test for cervical cancer in the past two years.d Only females aged 50–69 years were asked whether they had had a mammogram in the past two years.
Table 5
Association between health outcomes and polypharmacy in people with intellectual disability.
Prevalence of polypharmacy
% (95% CI)
Crude odds ratio (95% CI) Adjusted odds ratio (95% CI)a
Reported health statusb
Good 21.9 (16.3–28.8) 2.38 (1.43–3.94) 2.07 (1.22–3.53)Fair or poor 34.9 (26.7–44.0) 4.52 (2.66–7.70) 4.55 (2.62–7.90)
Health conditionsc
Epilepsy 31.8 (24.2–40.6) 3.10 (2.06–4.65) 3.16 (2.00–4.97)Depression 25.9 (18.9–34.4) 1.40 (0.93–2.11) 1.47 (0.95–2.29)
Heart disease 29.2 (17.1–45.2) 1.53 (0.76–3.06) 1.64 (0.82–3.27)
Diabetes 40.2 (26.5–55.6) 3.93 (1.96–7.91) 3.68 (1.70–7.99)Stroke 43.4 (21.0–68.9) 3.42 (1.13–10.30) 4.62 (1.25–17.10)Osteoporosis 45.6 (29.9–62.2) 5.60 (2.77–11.32) 3.85 (1.81–8.22)Arthritis 26.8 (17.1–39.3) 2.02 (1.11–3.68) 1.45 (0.76–2.76)
Cancer 56.4 (30.9–78.9) 7.46 (3.10–17.96) 4.89 (2.03–11.78)Asthma (current) 25.9 (16.2–38.8) 1.59 (0.86–2.94) 1.82 (0.94–3.56)
Vision impairment 20.6 (15.8–26.5) 1.18 (0.79–1.77) 1.08 (0.71–1.65)
Hearing impairment 16.2 (10.4–24.3) 0.91 (0.51–1.64) 0.77 (0.42–1.45)
Functional ability
Inability to walk unaidedd 34.2 (25.5–44.1) 2.80 (1.76–4.46) 2.39 (1.36–4.21)
95% CI = 95 per cent confidence interval.
Data are age standardized to the 2006 Victorian population.
Significant associations are printed in bold.a Adjusted for age, sex, and severity of intellectual disability.b Excellent or very good is reference category.c People without the health condition is reference category.d Ability to walk unaided is reference category.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–3080 3077
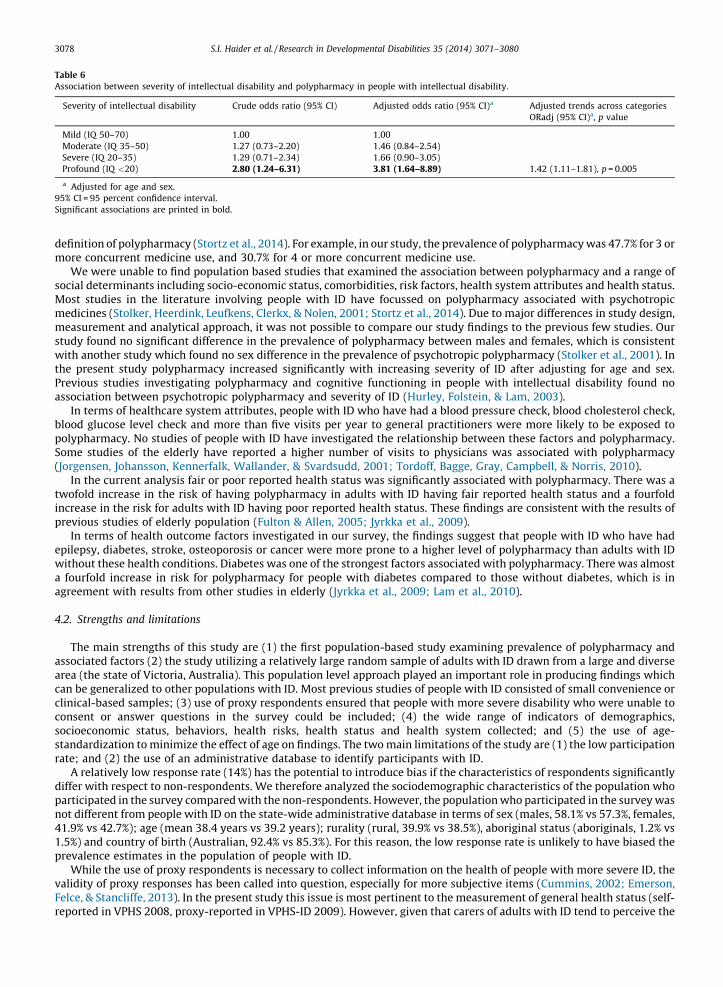
Table 6
Association between severity of intellectual disability and polypharmacy in people with intellectual disability.
Severity of intellectual disability Crude odds ratio (95% CI) Adjusted odds ratio (95% CI)a Adjusted trends across categories
ORadj (95% CI)a, p value
Mild (IQ 50–70) 1.00 1.00
Moderate (IQ 35–50) 1.27 (0.73–2.20) 1.46 (0.84–2.54)
Severe (IQ 20–35) 1.29 (0.71–2.34) 1.66 (0.90–3.05)
Profound (IQ <20) 2.80 (1.24–6.31) 3.81 (1.64–8.89) 1.42 (1.11–1.81), p = 0.005
a Adjusted for age and sex.
95% CI = 95 percent confidence interval.
Significant associations are printed in bold.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–30803078
definition of polypharmacy (Stortz et al., 2014). For example, in our study, the prevalence of polypharmacy was 47.7% for 3 ormore concurrent medicine use, and 30.7% for 4 or more concurrent medicine use.
We were unable to find population based studies that examined the association between polypharmacy and a range ofsocial determinants including socio-economic status, comorbidities, risk factors, health system attributes and health status.Most studies in the literature involving people with ID have focussed on polypharmacy associated with psychotropicmedicines (Stolker, Heerdink, Leufkens, Clerkx, & Nolen, 2001; Stortz et al., 2014). Due to major differences in study design,measurement and analytical approach, it was not possible to compare our study findings to the previous few studies. Ourstudy found no significant difference in the prevalence of polypharmacy between males and females, which is consistentwith another study which found no sex difference in the prevalence of psychotropic polypharmacy (Stolker et al., 2001). Inthe present study polypharmacy increased significantly with increasing severity of ID after adjusting for age and sex.Previous studies investigating polypharmacy and cognitive functioning in people with intellectual disability found noassociation between psychotropic polypharmacy and severity of ID (Hurley, Folstein, & Lam, 2003).
In terms of healthcare system attributes, people with ID who have had a blood pressure check, blood cholesterol check,blood glucose level check and more than five visits per year to general practitioners were more likely to be exposed topolypharmacy. No studies of people with ID have investigated the relationship between these factors and polypharmacy.Some studies of the elderly have reported a higher number of visits to physicians was associated with polypharmacy(Jorgensen, Johansson, Kennerfalk, Wallander, & Svardsudd, 2001; Tordoff, Bagge, Gray, Campbell, & Norris, 2010).
In the current analysis fair or poor reported health status was significantly associated with polypharmacy. There was atwofold increase in the risk of having polypharmacy in adults with ID having fair reported health status and a fourfoldincrease in the risk for adults with ID having poor reported health status. These findings are consistent with the results ofprevious studies of elderly population (Fulton & Allen, 2005; Jyrkka et al., 2009).
In terms of health outcome factors investigated in our survey, the findings suggest that people with ID who have hadepilepsy, diabetes, stroke, osteoporosis or cancer were more prone to a higher level of polypharmacy than adults with IDwithout these health conditions. Diabetes was one of the strongest factors associated with polypharmacy. There was almosta fourfold increase in risk for polypharmacy for people with diabetes compared to those without diabetes, which is inagreement with results from other studies in elderly (Jyrkka et al., 2009; Lam et al., 2010).
4.2. Strengths and limitations
The main strengths of this study are (1) the first population-based study examining prevalence of polypharmacy andassociated factors (2) the study utilizing a relatively large random sample of adults with ID drawn from a large and diversearea (the state of Victoria, Australia). This population level approach played an important role in producing findings whichcan be generalized to other populations with ID. Most previous studies of people with ID consisted of small convenience orclinical-based samples; (3) use of proxy respondents ensured that people with more severe disability who were unable toconsent or answer questions in the survey could be included; (4) the wide range of indicators of demographics,socioeconomic status, behaviors, health risks, health status and health system collected; and (5) the use of age-standardization to minimize the effect of age on findings. The two main limitations of the study are (1) the low participationrate; and (2) the use of an administrative database to identify participants with ID.
A relatively low response rate (14%) has the potential to introduce bias if the characteristics of respondents significantlydiffer with respect to non-respondents. We therefore analyzed the sociodemographic characteristics of the population whoparticipated in the survey compared with the non-respondents. However, the population who participated in the survey wasnot different from people with ID on the state-wide administrative database in terms of sex (males, 58.1% vs 57.3%, females,41.9% vs 42.7%); age (mean 38.4 years vs 39.2 years); rurality (rural, 39.9% vs 38.5%), aboriginal status (aboriginals, 1.2% vs1.5%) and country of birth (Australian, 92.4% vs 85.3%). For this reason, the low response rate is unlikely to have biased theprevalence estimates in the population of people with ID.
While the use of proxy respondents is necessary to collect information on the health of people with more severe ID, thevalidity of proxy responses has been called into question, especially for more subjective items (Cummins, 2002; Emerson,Felce, & Stancliffe, 2013). In the present study this issue is most pertinent to the measurement of general health status (self-reported in VPHS 2008, proxy-reported in VPHS-ID 2009). However, given that carers of adults with ID tend to perceive the

S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–3080 3079
person they care for to be healthier than suggested by the results of medical examination (Beange, McElduff, & Baker, 1995),it is likely that any bias associated with the use of proxy responses on this item will have underestimated the extent of theinequality in general health status between people with ID and the general Victorian population.
4.3. Conclusions and policy implications
We conclude that the estimated prevalence of medicine use and polypharmacy was high in the ID population. There is alack of national and international studies that have used population-based approaches to investigate prevalence ofpolypharmacy and a variety of factors for people with ID. This study fills a void in research in polypharmacy and associatedfactors, and provides a high quality and reliable data for planning service delivery in both the health and disability services;has direct application to evidence-based policy development and strategic planning across the government departments,disability service providers, health service providers and the wider community; and informs policy development andmedication safety and quality activities. Some population groups with ID may be exposed to higher levels of adverse effectsof medicines, while at the same time having impaired capacity to protect themselves from the harmful effects of thesemedicines.
The continuous monitoring of medicine use in people with ID through population-based surveys provides data toimprove safety and quality of medicines. The current study calls for a public health strategy that highlights and tacklepolypharmacy and inappropriate medicine use in ID population groups. Some studies recommend interventions to improvethe appropriateness of prescribing in patients with ID, such as training in pharmacotherapy for people with ID, developmentof intellectual disability medicine services, pharmacist involvement in patient care, and computerized decision support.There should also be an increased focus on non- pharmacological interventions. One such approach would be to build astrong communication between prescribers, patients and their carers. Because of a high proportion of people with ID havedifficulty understanding complex medication regimen, their caregivers’ involvement in decision-making relevant toprescribing can promote rational drug therapy (Valk & Walsh, 2008). People with ID and their carers’ education on the use ofmedication is important in ensuring compliance, recognizing side effects and maximizing efficacy. Finally we stress the needthat medications should be regularly reviewed overall in ID population and particularly when polypharmacy exists. Inaddition, we recommend further population based research focussing on the relationship between polypharmacy,inappropriate drug use, other drug related problems and associated risk factors.
Conflict of interest
There is no conflict of interest.
Funding
This project was financially supported by the Department of Human Services, Victoria, Australia.
Ethical standards
The Department of Health Human Research Ethics Committee, Victoria approved methodology and questionnairecontent of both surveys.
References
ABS (2006). Population by age and sex, Australian states and territories, Cat. No. 3201.0. Canberra: Australian Bureau of Statistics (ABS).Agostini, J. V., Han, L., & Tinetti, M. E. (2004). The relationship between number of medications and weight loss or impaired balance in older adults. Journal of
the American Geriatrics Society, 52, 1719–1723.Ansari, Z., Carson, N. J., Ackland, M. J., Vaughan, L., & Serraglio, A. (2003). A public health model of the social determinants of health. Sozial- und Praventivmedizin,
48, 242–251.Beange, H., McElduff, A., & Baker, W. (1995). Medical disorders of adults with mental retardation: A population study. American Journal of Mental Retardation, 99,
595–604.Cummins, R. (2002). Proxy responding for subjective well-being: A review. In L. M. Glidden (Ed.), International Review of Research in Mental Retardation (vol. 25, pp.
183–207). San Diego, CA: Academic Press.Department of Health (2008). The Victorian Population Health Survey (VPHS) – Selected findings. Melbourne, Victoria: Department of Health, State Government of
Victoria.Department of Health (2011). The Victorian Population Health Survey of people with an intellectual disability 2009. Melbourne, Victoria: Department of Health, State
Government of Victoria.DoHA (1999). National physical activity guidelines for Australians. Canberra: Commonwealth Department of Health and Aged Care.Emerson, E., Felce, D., & Stancliffe, R. J. (2013). Issues concerning self-report data and population-based data sets involving people with intellectual disabilities.
Intellectual and Developmental Disabilities, 51, 333–348.Emerson, E., & Hatton, C. (2013). Health inequalities and people with intellectual disabilities. Cambridge: Cambridge University Press.Fulton, M. M., & Allen, E. R. (2005). Polypharmacy in the elderly: A literature review. Journal of the American Academy of Nurse Practitioners, 17, 123–132.Haider, S. I., Ansari, Z., Vaughan, L., Matters, H., & Emerson, E. (2013). Health and wellbeing of Victorian adults with intellectual disability compared to the general
Victorian population. Research in Developmental Disabilities, 34, 4034–4042.Haider, S. I., Johnell, K., Thorslund, M., & Fastbom, J. (2008). Analysis of the association between polypharmacy and socioeconomic position among elderly aged�77 years in Sweden. Clinical Therapeutics, 30, 419–427.
S.I. Haider et al. / Research in Developmental Disabilities 35 (2014) 3071–30803080
Haider, S. I., Johnell, K., Weitoft, G. R., Thorslund, M., & Fastbom, J. (2009). The influence of educational level on polypharmacy and inappropriate drug use: Aregister-based study of more than 600,000 older people. Journal of the American Geriatrics Society, 57, 62–69.
Haveman, M., Heller, T., Lee, L., Maaskant, M., Shooshtari, S., & Strydom, A. (2010). Major health risks in aging persons with intellectual disabilities: An overview ofrecent studies. Journal of Policy and Practice in Intellectual Disabilities, 7, 59–69.
Hurley, A. D., Folstein, M., & Lam, N. (2003). Patients with and without intellectual disability seeking outpatient psychiatric services: Diagnoses and prescribingpattern. Journal of Intellectual Disability Research, 47, 39–50.
Jorgensen, T., Johansson, S., Kennerfalk, A., Wallander, M. A., & Svardsudd, K. (2001). Prescription drug use, diagnoses, and healthcare utilization among the elderly.Annals of Pharmacotherapy, 35, 1004–1009.
Jyrkka, J., Enlund, H., Korhonen, M. J., Sulkava, R., & Hartikainen, S. (2009). Patterns of drug use and factors associated with polypharmacy and excessivepolypharmacy in elderly persons: Results of the Kuopio 75+ study: A cross-sectional analysis. Drugs & Aging, 26, 493–503.
Krahn, G. L., & Fox, M. H. (2013). Health disparities of adults with intellectual disabilities: What do we know? what do we do?. Journal of Applied Research inIntellectual Disabilities. http://dx.doi.org/10.1111/jar.12067/abstract
Lam, D. P., Mak, C. F., Chan, S. M., Yao, R. W., Leung, S. S., & You, J. H. (2010). Polypharmacy and inappropriate prescribing in elderly Hong Kong Chinese patients.Journal of the American Geriatrics Society, 58, 203–205.
Levy, S. E., Mandell, D. S., & Schultz, R. T. (2009). Autism. Lancet, 374, 1627–1638.Linjakumpu, T., Hartikainen, S., Klaukka, T., Veijola, J., Kivela, S. L., & Isoaho, R. (2002). Use of medications and polypharmacy are increasing among the elderly.
Journal of Clinical Epidemiology, 55, 809–817.Lunsky, Y., & Elserafi, J. (2012). Antipsychotic medication prescription patterns in adults with developmental disabilities who have experienced psychiatric crisis.
Research in Developmental Disabilities, 33, 32–38.Mahan, S., Holloway, J., Bamburg, J. W., Hess, J. A., Fodstad, J. C., & Matson, J. L. (2010). An examination of psychotropic medication side effects: Does taking a
greater number of psychotropic medications from different classes affect presentation of side effects in adults with ID? Research in Developmental Disabilities,31, 1561–1569.
NHMRC (2003). Dietary guidelines for Australian adults. Canberra, Australia: National Health and Medical Research Council.O’Hara, J., McCarthy, J. E., & Bouras, N. (2010). Intellectual disability and ill health: A review of the evidence. Cambridge: Cambridge University Press.Oeseburg, B., Dijkstra, G. J., Groothoff, J. W., Reijneveld, S. A., & Jansen, D. E. M. C. (2011). Prevalence of chronic health conditions in children with intellectual
disability: A systematic literature review. Intellectual & Developmental Disabilities, 49, 59–85.Passarelli, M. C., Jacob-Filho, W., & Figueras, A. (2005). Adverse drug reactions in an elderly hospitalised population: Inappropriate prescription is a leading cause.
Drugs & Aging, 22, 767–777.Pitkala, K. H., Strandberg, T. E., & Tilvis, R. S. (2001). Is it possible to reduce polypharmacy in the elderly? A randomised, controlled trial. Drugs & Aging, 18, 143–149.Simonson, W., & Feinberg, J. L. (2005). Medication-related problems in the elderly: Defining the issues and identifying solutions. Drugs & Aging, 22, 559–569.Stolker, J. J., Heerdink, E. R., Leufkens, H. G., Clerkx, M. G., & Nolen, W. A. (2001). Determinants of multiple psychotropic drug use in patients with mild intellectual
disabilities or borderline intellectual functioning and psychiatric or behavioral disorders. General Hospital Psychiatry, 23, 345–349.Stortz, J. N., Lake, J. K., Cobigo, V., Ouellette-Kuntz, H. M., & Lunsky, Y. (2014). Lessons learned from our elders: How to study polypharmacy in populations with
intellectual and developmental disabilities. Intellectual and Developmental Disabilities, 52, 60–77.Straetmans, J. M. J. A. A., van Schrojenstein Lantman-de Valk, H. M. J., Schellevis, F. G., & Dinant, G.-J. (2007). Health problems of people with intellectual
disabilities: The impact for general practice. British Journal of General Practice, 57, 64–66.Tordoff, J. M., Bagge, M. L., Gray, A. R., Campbell, A. J., & Norris, P. T. (2010). Medicine-taking practices in community-dwelling people aged �75 years in New
Zealand. Age and Ageing, 39, 574–580.Valk, H.M.J.v.S.L.-d., & Walsh, P. N. (2008). Managing health problems in people with intellectual disabilities. British Medical Journal, 337, a2507.Van Schrojenstein Lantman-de Valk, H. (2005). Health in people with intellectual disabilities: Current knowledge and gaps in knowledge. Journal of Applied
Research in Intellectual Disabilities, 18, 325–333.Veehof, L., Stewart, R., Haaijer-Ruskamp, F., & Jong, B. M. (2000). The development of polypharmacy. A longitudinal study. Family Practice, 17, 261–267.WHO (2000). Obesity: Preventing and managing the global epidemic. Geneva, Switzerland: World Health Organization.