Embed Size (px)
Citation preview
JEADV
(2002)
16
, 625–627
© 2002 European Academy of Dermatology and Venereology
625
CAS E REPO R T
Blackwell Science, Ltd
Pretibial myxoedema associated with Hashimoto’s thyroiditis
SP
Cannavò,†*
F
Borgia,†
M
Vaccaro,†
F
Guarneri,†
E
Magliolo,‡
B
Guarneri†
†
Institute of Dermatology,
‡
Department of Human Pathology, University of Messina, Italy.
*
Corresponding author, Institute of Dermatology, University
Hospital, Via Consolare Valeria, Gazzi, 98125 Messina, Italy, tel. +39 90/2212891; fax +39 90/2927691; E-mail: [email protected]
ABSTRACT
Pretibial myxoedema is a cutaneous mucinosis typically associated with Graves’ disease, although it mayalso develop in subjects with non-thyrotoxic thyroid pathologies. This report presents a rare case of pretibialmyxoedema occurring in a 58-year-old woman with biopsy-proven Hashimoto’s thyroiditis. The hypotheticalpathogenetic link between the two disorders is discussed with particular attention to the role of thyroidstimulating hormone receptor antibodies.
Key words:
glycosaminoglycans, myxoedema, thyroid diseases, thyroid stimulating hormone receptor antibodies
Received: 2 January 2001, accepted 28 February 2002
Introduction
Pretibial myxoedema (PTM) is a rare form of cutaneous
mucinosis, characterized by mucin deposition in the preti-
bial skin; the pathogenesis is still unknown and treatment is
frequently unsatisfactory. It is considered an autoimmune
complication or association of Graves’ disease, although it may
develop in subjects with non-thyrotoxic thyroid disorders; in
particular, only a few cases of PTM associated with chronic
lymphocytic thyroiditis have been reported.
We report a rare case of PTM following onset of Hashimoto’s
thyroiditis, confirmed by thyroid biopsy, and discuss the
hypothetical pathogenetic link between these two diseases.
Case report
In 1997, a 58-year-old woman developed tenderness of the
thyroid gland and diffuse goitre. A clinical diagnosis of
thyroiditis was made in an Endocrinological Department. For
this reason, in July 1998, she was subjected to thyroid biopsy;
the thyroid specimen revealed atrophy of the parenchymal cells
and diffuse lymphocytic infiltration, showing chronic lym-
phocytic thyroiditis. Since then, the woman has been receiving
supplemental levothyroxine, 50–200 mg daily. Results of periodic
thyroid function tests show alternate patterns of hypothyroidism
and euthyroidism.
In November 1998, the woman developed exophthalmos
with ocular pain, lacrimation and photophobia. Four months
later, slowly growing skin papules and oedema were noted on
the lower part of her legs. These symptoms gradually worsened
and she was referred to the Institute of Dermatology, University
of Messina (Italy) in March 2000.
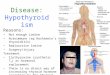
Clinical examination revealed reddish, indurated, non-
pitting plaques with an ‘orange peel-like’ appearance on both
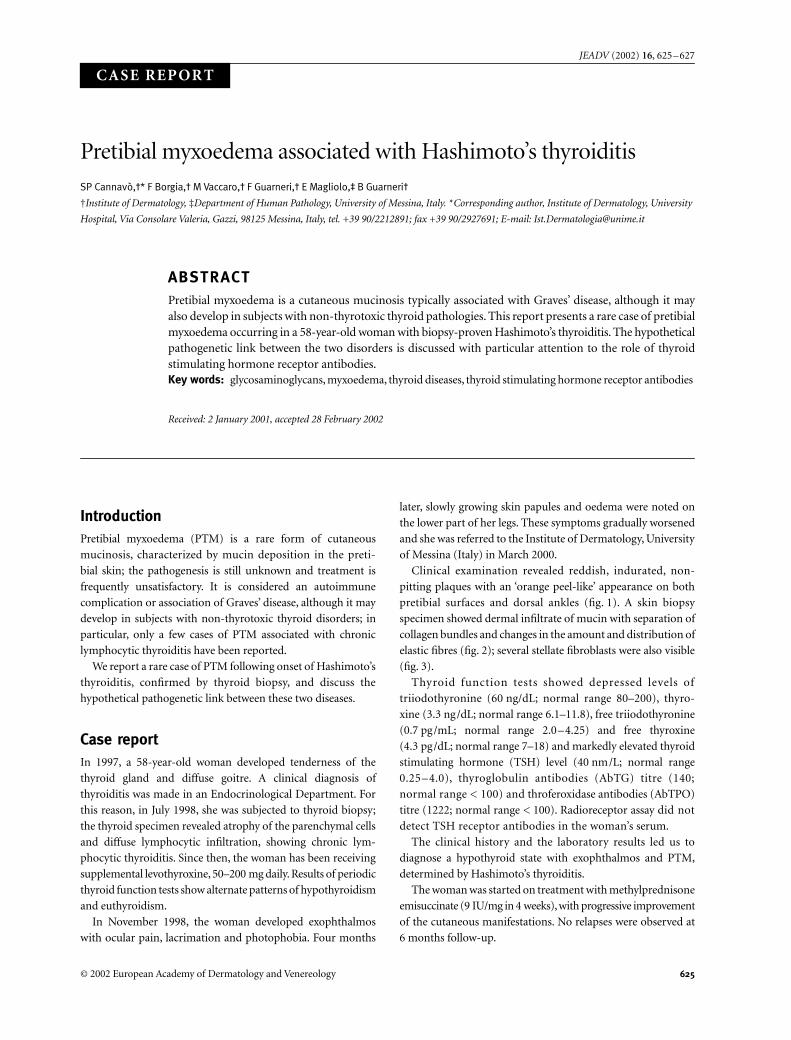
pretibial surfaces and dorsal ankles (fig. 1). A skin biopsy
specimen showed dermal infiltrate of mucin with separation of
collagen bundles and changes in the amount and distribution of
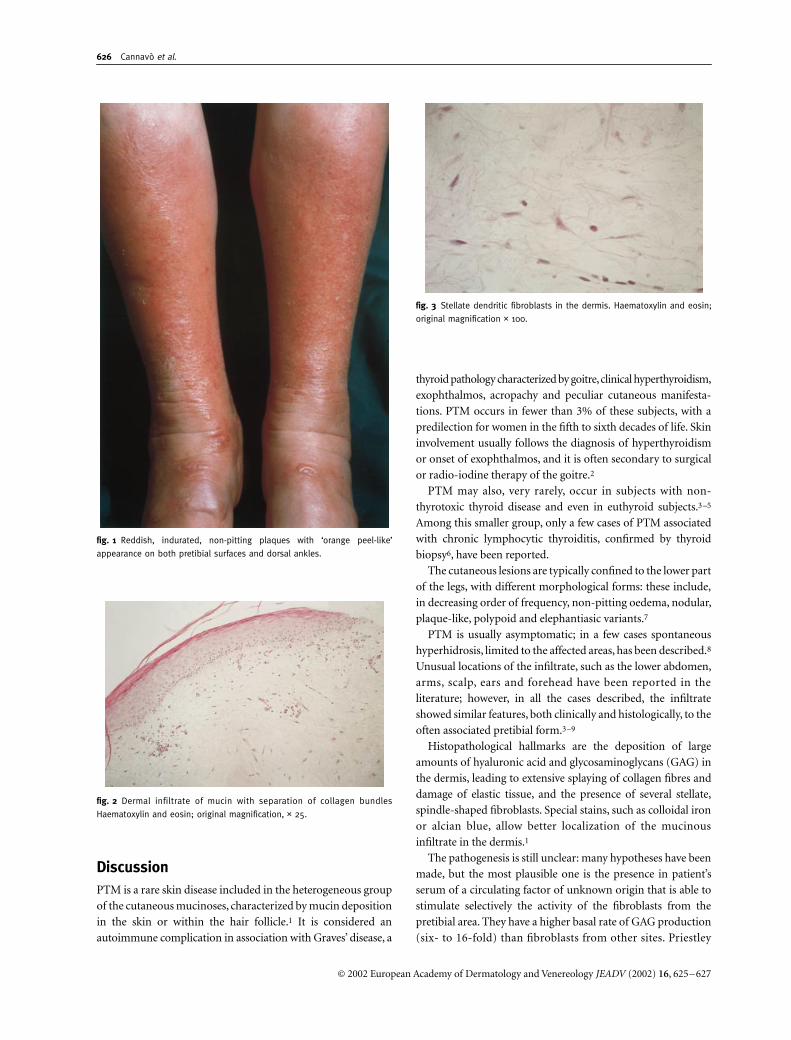
elastic fibres (fig. 2); several stellate fibroblasts were also visible
(fig. 3).
Thyroid function tests showed depressed levels of
triiodothyronine (60 ng/dL; normal range 80–200), thyro-
xine (3.3 ng/dL; normal range 6.1–11.8), free triiodothyronine
(0.7 pg/mL; normal range 2.0–4.25) and free thyroxine
(4.3 pg/dL; normal range 7–18) and markedly elevated thyroid
stimulating hormone (TSH) level (40 nm/L; normal range
0.25–4.0), thyroglobulin antibodies (AbTG) titre (140;
normal range < 100) and throferoxidase antibodies (AbTPO)
titre (1222; normal range < 100). Radioreceptor assay did not
detect TSH receptor antibodies in the woman’s serum.
The clinical history and the laboratory results led us to
diagnose a hypothyroid state with exophthalmos and PTM,
determined by Hashimoto’s thyroiditis.
The woman was started on treatment with methylprednisone
emisuccinate (9 IU/mg in 4 weeks), with progressive improvement
of the cutaneous manifestations. No relapses were observed at
6 months follow-up.
JDV_532.fm Page 625 Friday, October 25, 2002 8:42 PM
626
Cannavò
et al
.
© 2002 European Academy of Dermatology and Venereology
JEADV
(2002)
16
, 625–627
Discussion
PTM is a rare skin disease included in the heterogeneous group
of the cutaneous mucinoses, characterized by mucin deposition
in the skin or within the hair follicle.
1
It is considered an
autoimmune complication in association with Graves’ disease, a
thyroid pathology characterized by goitre, clinical hyperthyroidism,
exophthalmos, acropachy and peculiar cutaneous manifesta-
tions. PTM occurs in fewer than 3% of these subjects, with a
predilection for women in the fifth to sixth decades of life. Skin
involvement usually follows the diagnosis of hyperthyroidism
or onset of exophthalmos, and it is often secondary to surgical
or radio-iodine therapy of the goitre.
2
PTM may also, very rarely, occur in subjects with non-
thyrotoxic thyroid disease and even in euthyroid subjects.
3–5
Among this smaller group, only a few cases of PTM associated
with chronic lymphocytic thyroiditis, confirmed by thyroid
biopsy
6
, have been reported.
The cutaneous lesions are typically confined to the lower part
of the legs, with different morphological forms: these include,
in decreasing order of frequency, non-pitting oedema, nodular,
plaque-like, polypoid and elephantiasic variants.
7
PTM is usually asymptomatic; in a few cases spontaneous
hyperhidrosis, limited to the affected areas, has been described.
8
Unusual locations of the infiltrate, such as the lower abdomen,
arms, scalp, ears and forehead have been reported in the
literature; however, in all the cases described, the infiltrate
showed similar features, both clinically and histologically, to the
often associated pretibial form.
3–9
Histopathological hallmarks are the deposition of large
amounts of hyaluronic acid and glycosaminoglycans (GAG) in
the dermis, leading to extensive splaying of collagen fibres and
damage of elastic tissue, and the presence of several stellate,
spindle-shaped fibroblasts. Special stains, such as colloidal iron
or alcian blue, allow better localization of the mucinous
infiltrate in the dermis.
1
The pathogenesis is still unclear: many hypotheses have been
made, but the most plausible one is the presence in patient’s
serum of a circulating factor of unknown origin that is able to
stimulate selectively the activity of the fibroblasts from the
pretibial area. They have a higher basal rate of GAG production
(six- to 16-fold) than fibroblasts from other sites. Priestley
fig. 1 Reddish, indurated, non-pitting plaques with ‘orange peel-like’
appearance on both pretibial surfaces and dorsal ankles.
fig. 2 Dermal infiltrate of mucin with separation of collagen bundles
Haematoxylin and eosin; original magnification, × 25.
fig. 3 Stellate dendritic fibroblasts in the dermis. Haematoxylin and eosin;
original magnification × 100.
JDV_532.fm Page 626 Friday, October 25, 2002 8:42 PM

Pretibial myxoedema and Hashimoto’s thyroiditis
627
© 2002 European Academy of Dermatology and Venereology
JEADV
(2002)
16
, 625–627
et al
.’s experiments
10
demonstrated that sera from affected
subjects can stimulate the proliferation and GAG metabolism
of fibroblasts
in vitro
, regardless of their site of origin (pretibial
or other sites) and status (both patient and control). The lack
of site specificity does not permit an explanation of the
predominant localization of the mucinous infiltrate; it may
be due to an increased quantitative, rather than qualitative
response to stimulation.
Even the nature of the stimulating factor is still unknown:
first, long-acting thyroid stimulator and, then, insulin-like
growth factor 1 have been considered as the causative agents of
PTM, but their role has never been clearly demonstrated.
Recently, attention has been focused on the TSH receptor
antibodies. Chang
et al
.
11
have demonstrated that subjects
with Graves’ disease and PTM have high titres of TSH receptor
antibodies in their serum; moreover, the presence of TSH and
TSH receptor antibody-binding sites on fibroblasts derived
from the affected skin and the detection, within the pretibial
tissue, of RNA encoding non-variant human TSH receptor,
suggest the existence of a common antigenic site and seem
to provide evidence for the central pathogenetic role of
this autoantigen in both thyroidal and extrathyroidal
manifestations.
12
The woman in our case showed typical skin features of PTM
associated with chronic lymphocytic thyroiditis and exophthalmos;
the parallel course of both cutaneous and endocrinological
manifestations and the good response to corticosteroid therapy
confirm the presence of a close pathogenetic link between the
two diseases.
On the contrary, the absence of circulating TSH receptor
antibodies, as observed in our case, strongly suggests the
existence of a different autoimmune mechanism responsible
for such cutaneous features in subjects with Hashimoto’s
thyroiditis.
References
1 Rongioletti F, Rebora A. Les mucinoses cutanèes.
Ann Dermatol
Venereol
1993;
120
: 75–87.
2 Kriss JP. Pathogenesis and treatment of pretibial myxedema.
Endocrinol Metab Clin North Am
1987;
16
: 409–415.
3 Forgie JC, Highet AS, Kelly SA. Myxedematous infiltrate of the
forehead in treated hypothyroidism.
Clin Exp Dermatol
1994;
19
:
168–169.
4 Lynch PJ, Maize JC, Sisson JC. Pretibial myxoedema and
nonthyrotoxic thyroid disease.
Arch Dermatol
1973;
107
: 107–111.
5 Srebrnik A, Ophir J, Brenner S. Euthyroid pretibial myxedema.
Int
J Dermatol
1992;
31
: 431–432.
6 Horiuchi Y. Pretibial myxedema associated with chronic thyroiditis.
Arch Dermatol
1985;
121
: 451.
7 Fatourechi V, Pajouhi M, Fransway AF. Dermopathy of Graves
disease (pretibial myxedema). Review of 150 cases.
Medicine
1994;
73
: 1–7.
8 Gitter DG, Sato K. Localized hyperhidrosis in pretibial myxedema.
J Am Acad Dermatol
1990;
23
: 250–254.
9 Noppakun N, Bancheun K, Chandaprasert S. Unusual locations of
localized myxedema in Graves’ disease. Report of three cases.
Arch
Dermatol
1986;
122
: 85–88.
10 Priestley GC, Aldridge RD, Sime PJ, Wilson D. Skin fibroblast
activity in pretibial myxoedema and the effect of octreotide
in vitro
.
Br J Dermatol
1994;
131
: 52–56.
11 Chang TC, Wu SL, Hsiao YL
et al.
TSH and TSH receptor
antibody-binding sites in fibroblasts of pretibial myxedema are
related to the extracellular domain of entire TSH receptor.
Clin
Immunol Immunopathol
1994;
71
: 113–120.
12 Stadlmayr W, Spitzweg C, Bichlmair AM, Heufelder AE. TSH
receptor transcripts and TSH receptor-like immunoreactivity in
orbital and pretibial fibroblasts of patients with Graves’
ophthalmopathy and pretibial myxoedema.
Thyroid
1997;
7
: 3–12.
Visit the EADV website at: www.eadv.org
JDV_532.fm Page 627 Friday, October 25, 2002 8:42 PM
![The best hashimoto's diet [how to reduce your antibodies and autoimmunity with these 5 diets]](https://img.pdfslide.us/doc/110x75/58a7585f1a28ab217e8b4819/the-best-hashimotos-diet-how-to-reduce-your-antibodies-and-autoimmunity.jpg)