Embed Size (px)
Citation preview

Pressure Ulcer Prevention & Management
Presented by
Carol Compas, RN, BSNProject Manager (AFMC)
Jeff Edwards,RNMDS/RAI Coordinator (OLTC)

Outline
• Background
• Pressure Ulcer Prevention
• Pressure Ulcer Treatment and Monitoring
• Publicly reported PU Quality Measure
• Partnering with the QIO to improve PU care

Pressure Ulcers
• Definition• Any lesion caused by unrelieved pressure
resulting in damage of underlying tissue (AHCPR, 1994).
– Can occur anywhere on body

Healing of Pressure Ulcers• Pressure Ulcer Staging (depth & tissue type)
– Stage I Persistent redness (culturally sensitive)
– Stage II Partial thickness skin loss– Stage III Full thickness skin loss
(subcutaneous)– Stage IV Full thickness skin loss (fascia)– *NPUAP does not endorse reverse
staging;however, the current RAI guidelines mandate reverse staging

Pressure Ulcer Stages

Pressure Ulcer Causes
• Prolonged pressure
– duration and intensity of pressure
– location of pressure on body
– extended pressure that blocks flow to the tissue between the source of pressure & the bone
• Shear• Friction

Pressure Ulcer
• Pressure Ulcer Etiology• pressure exerted by bony prominences on
the body that stop capillary flow to the tissues.
• Deprives tissues of oxygen and nutrients causing cell death.
• Pressure greater than 32mmHg exerted by bony prominences to disrupt blood flow.

Pressure Ulcer Etiology
• Function of both time and pressure (hyperbolic curve)-70mmHg pressure for two hours produces irreversible injury-greater pressure takes less time-lower pressure takes more time-obese may be much lower; emaciated may be much higher-turning schedules must be individualized!!!!

Most Common Sites
• Sacrum (tail bone)- most common site-Semi-fowlers’ position-Slouching in bed or chair-higher risk in tube fed or incontinent pts.
• Heels- 2nd most common-Immobile or numb legs-Leg traction-Higher risk with PVD & diabetes neuropathy

Other Bony Prominences
• Trochanter (hip bone)
-Side lying
-Highest risk contractured residents
-Ulcers on lateral foot rather than heel itself
• Ischium (sitting erect bone)
-highest risk paraplegics

Pressure Ulcers from other sources of pressure
• Boots/boot straps
• Heel protectors/protector straps
• Oxygen tubing
• Stockings
• Any device that can lead to pressure induced ischemia on the skin

Morbidity & Mortality
• Pain
• Infection
• Quality of life
• Death
• Cost

Mortality
• 40% die per year• 60% die within 1 year after hospital discharge
sources: Thomas DR JAGS 1996; 44:1435.
Brandeis GH JAMA 1990;264:2905-9.

Pain with Pressure Ulcers
• 59% report some degree of pain
• Only 2% receive pain medication within 4 hours of dressing change
• 45% report pain as distressing or horrible

KEY Pressure Ulcer Risk Factors
• Impaired bed or chair mobility
• Urinary incontinence
• Fecal incontinence
• Poor nutritional status
• History of pressure ulcer
• PVD or Diabetes Mellitus
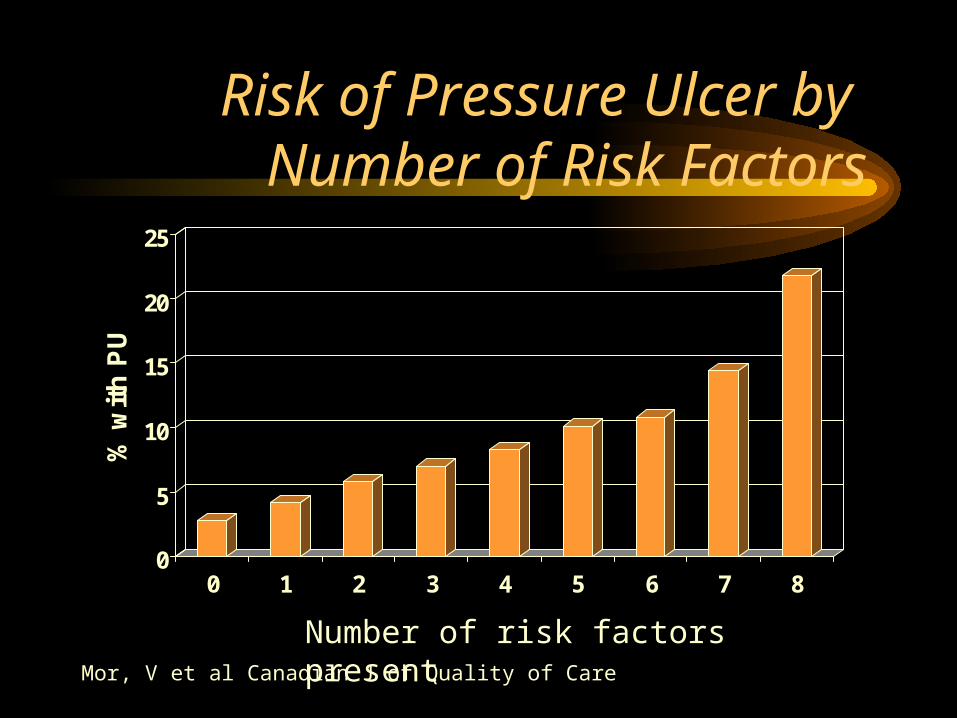
Risk of Pressure Ulcer by Number of Risk Factors
0
5
10
15
20
25
% w
ith
PU
0 1 2 3 4 5 6 7 8
Number of risk factors presentMor, V et al Canadian J of Quality of Care
Admission Assessment for Risk Factors
• Mobility status• Urinary continence • Bowel continence• Feeding assistance
needed
• Pressure ulcer history
• Recent weight loss• Height & weight• Skin exam

Impact of Risk Assessments
• Implementation of risk assessment reduced development of new pressure ulcers each year in one hospital
18.7% 13.1% 11.7% 6.4%
Source: Bergstrom N. Nurs Clin North Am 1995;30:539-551.

Impact of Risk Assessments
• Implementation of Braden scale reduced new pressure ulcers over 6 months in high risk patients
32.6% 9.1% Source: Horn ., Clinical Practice Improvement. Faulkner & Gray Inc. 1994

Plan of Care to AddressRisk Factors
• Skin Care
• Pressure Reduction
• Incontinence Care
• Nutritional Interventions

General Skin Care
• Daily skin inspections for high-risk individuals
• Skin cleansing
• Minimize drying & cracking
• Minimize excess moisture
• Avoid massage

Protect skin from moisture
• Cleanse skin with warm water & mild soap
• Cleanse skin after soiling
• Use non-alcohol based moisturizers
• Use skin protectants or barriers
• Do not massage over bony prominences
• Institute bowel or bladder training programs
• Use briefs or absorbent underpads

Pressure Reduction
• Rehabilitation to improve mobility• Repositioning schedule (individualized)
– Minimum turn Q2 hours in beds– Minimum shift Q1 hour in chair (15 mins)– Heel relief
• Positioning• Pressure reduction devices
– Beds– wheelchairs/chairs

Support Surface Selection
• No one support surface ever has been shown to be the best for all users
• Bed- consider the # of body surfaces available for support
• Wheelchair- cushions are fundamentally different than horizontal support surfaces
• Effectiveness is judged directly & indirectly-Direct- clinical outcomes-Indirect- interface pressure/IP, blood flow, etc. (never use 32 mmHg as the safe threshold for IP)

Pressure Reduction Helpful Hints
• Static Devices– Air, gel, water, foam and combinations
• No statistical significant differences have been noted between static devices
– Key to static devices• Foam density of 1.3lbs/cubic foot• 3 inches for solid foam, 4 inches for convoluted• Ability to assume variety of positions without bearing
weight• Remember wear and tear factor (average life of foam
overlay is 1 - 2 years).

Pressure Reduction Helpful Hints Cont’d
• Dynamic Surfaces– Alternating, low air loss and air fluidized– effective in maintaining < capillary closure
pressures.– Few studies demonstrate variances
between dynamic surfaces.– Must be operational (check instructions)

Pressure Reduction Helpful Hints Cont’d
• Key to selection– Inability to assume variety of positions
without bearing weight on pressure ulcer– “Bottoming out”– Absence of healing (wide variance on
stages)– Resident has Stage IIIs and Stage IVs on
multiple turning surfaces– Check Heels!

Pressure, friction and shear reduction
• Reduce pressure over bony prominences• Individualized bed turning (min. q 2hrs)• Individualized chair repositioning (min. q1hr)• HOB < 30 degrees• Avoid positioning directly on great trochanter• Float heels off bed• Check devices for “bottoming out”• Avoid mechanical injury- use slide boards, turn sheet,
trapeze, corn starch• Increase mobility/Consult PT/OT

Encourage optimal nutrition and fluid intake
• Conduct nutritional consultation• Consider resident preferences and special
needs• Provide assistance and adequate time• Offer snacks and fluids between meals• Consider administration of vitamins &/or
protein supplements• Assess lab values

Risk Assessment upon admission
Admission interventions for each selected risk factor
Admit & daily skin exams documented for at-risk population
QualityImprovement/
Monitor Program
RiskEarly
Care Plan
Daily skin check
Pressure Ulcer Prevention

Pressure Ulcer Monitoring and Treatment

Description of Ulcers
• Stage Ulcer• Location• Size• Wound bed • Granulation tissue
• Necrotic tissue• Wound edges• Drainage• Infection• Pain

Healing of Pressure Ulcers
• Pressure Ulcer Staging – Stage I Persistent erythema (culturally
sensitive)– Stage II Partial thickness skin loss– Stage III Full thickness skin loss
(subcutaneous)– Stage IV Full thickness skin loss (fascia)*NPUAP does not endorse reverse staging;
however, the current RAI guideline does

Identification
• Consider risk factors that are present-Shortness of breath, weight loss, inability to eat, orthopedic surgery (hip, knee) diabetes
• Consider if patient cannot move voluntarily-Bedridden, chair ridden, coma, restrained, desaturation with movement, traction, pain
• Consider the pattern of ulcer development-High risk? Or acquired, trapped in one place for extended time?

Identification
• Consider location of the ulcer
-Bony prominence, in location of medical devices• Descriptions (photographs)
-crater like ulcers common
-do not rely on the use of staging, many people stage wounds of any etiology
• Do not rely on the use of staging terms as evidence that a wound is a pressure ulcer

Management of Ulcers
• Wound Care– debridement
– wound cleansing– dressings– adjuvant therapies
• Pressure reduction
• Risk factors addressed– Continence care
– Nutritional improvement– Mobility
• Consider operative repair

Monitoring of Ulcers
• Maintain communication with treating physician• Physician and nursing documentation should
correlate• Reassess ulcer weekly (skin daily)
– PUSH Tool – see sample
• Re-evaluate plan of care – if wound deteriorates– if no healing in 2-4 weeks

Healing the Heels Hints
• Heel Pressure Ulcers– Account for 20% of all pressure ulcers– Easier to acquire, challenging to heal
• Pressure relief on heels?– Moisturize heels– pillows– semipermeable membrane dressing for
pre-Stage I– Hydrocolloid for Stage I

Healing the Heels Cont’d
• Heel protector boots (check warranty, check wear and tears, usual heel protector last 1 year!)
• Heel lift suspension (usually last 1-2 yrs)
• “Good fitting” sneakers with cushion pads
• Heels can be vulnerable independent of support surfaces on bed/wheelchair

Wound Cleansing
• Completed with each dressing change• Clean with saline or water
– do not use skin cleansers or antiseptic agents
– use appropriate irrigation pressure

Wound Cleansing
• Completed at each dressing change• Clean with saline or water
-Saline is considered the most appropriate solution-Literature also supports use of tap water if quality
• No skin cleansers or anti-septics• Use appropriate irrigation pressure between 4-15
psi-35cc syringe with 19-gauge cath. (delivers 8 psi)
->15 psi may drive wound fluid & debris into wound
• Consider availability, ease of use and cost

Wound Dressings
• Keep wound bed moist
• Keep surrounding tissue clean & dry
• Eliminate dead space
• Do not use antiseptic agents

Types of Dressings
• Gauze• Transparent films• Hydrocolloid• Hydrogel
• Alginates• Foam• Composite

Keys to Selecting Dressings
• Must use clinical judgement
• Keeps ulcer bed continuously moist
• Keeps surrounding periulcer skin dry
• Controls exudate without dessicating (drying out) ulcer bed
• Caregiver time

Debridement Techniques
• All wounds with necrotic tissue should be debrided (except eschar on heels) as necrotic tissue delays wound healing and predisposes to infection.
• Sharp • Mechanical (including dextranomers)
– initial form of debridement
• Enzymatic• Autolytic

Bacterial Infection
• Clinically Infected– redness of the skin around – purulent drainage– foul odor– edema
• All wounds colonize!

Helpful Hints to Prevent Infection
• Sterile vs. Clean Technique– Wounds are not sterile– Assure wound care products/dressing supplies
do not become contaminated during storage and use
• To Swab or not to Swab?– Has little value in determining whether wound
is infected, not currently recommended

Monitor Nutritional Status
• Track percent meals consumed
• Monitor changes in weight
• Monitor protein intake (< 90% RDA)
• Consider laboratory tests

Nutritional Interventions
• Supplements
• Feeding assistance programs
• Feeding assistance devices
• Vitamins & minerals

Assessment upon admission
Admission treatment order based on current standards or product guidelines
Weekly ulcer assessments
QualityImprovement/
Monitor Program
Admit assessment
Treatment Plan
WeeklyRe-assess
Pressure Ulcer Treatment

Section M. Skin Condition
• Skin Ulcer Definition-Local loss of epidermis and variable levels of dermis and subcutaneous tissue, or in the case of Stage I pressure ulcers, persistent area of skin redness.Skin ulcers that may develop because of injury, circulatory problems, pressure, or in association with other diseases.
Section M. Skin Condition
• M1 Ulcer -Due to any cause-7 Day look back
• Intent is to record the number of ulcers, of any type at each ulcer stage, on any part of the body
• M2 Type of Ulcer (only 2 choices)a. Pressure Ulcerb. Stasis Ulcer

Regulatory Compliance• F271- “At the time each
resident is admitted, the facility must have physician orders for the resident’s immediate care”
• “Orders at a min. should include routine care to maintain or improve functional abilities until staff can conduct a comprehensive assessment and develop a care plan”

Regulatory Compliance
• F281- The services provided must meet professional standards of quality
• “Professional standards of quality” means services that are provided according to accepted standards of clinical practice
• Standards published by a professional organization• Pressure ulcer specific- AMDA & AHCPR • Manufacturer guidelines count as standards! • Ensure product is used accordingly

Regulatory Compliance
• F272- “The scope of the RAI does not limit the facility’s responsibility to assess & address all care”
• “The facility is responsible for addressing the residents’ needs from the moment of admission”

Regulatory Compliance
• F314- “A resident who enters the facility does not develop pressure sores unless clinical condition demonstrates that they were unavoidable”
• “A resident having pressure sores receives necessary treatment & services to promote healing, prevent infection and prevent new sores form developing”

Was the ulcer avoidable?
• Avoidable: ulcers develop when all appropriate care was given, or in residents who cannot move, will not move, will not be fed, etc…
• Documentation must support appropriate care, inability to move (e.g. unstable spinal cord injury), noncompliance, advanced directives
• Support surfaces & pain control often are other aspects of determining if appropriate care was given

Investigative ProtocolTask 5c, 6
• Conduct a review of the assessment and care plan noting the facility’s interventions
• Observe care delivery to determine if the interventions have been implemented, such as: -incontinence care with frequency to keep skin clean & dry-repositioning and evaluation of skin condition-nutritional interventions-treatment interventions-changes in skin condition & healing

Investigative Protocol
• Note: Regardless of the timing of the assessment, the facility is required to develop and implement a care plan to meet the needs of the resident
• Evaluation of the assessment identified conditions that may put the resident at-risk for development such as:-Diabetes-Peripheral Vascular Disease-COPD

Investigative Protocol
• All related information and documentation will be reviewed to look for evidence of identified causes of the condition or problem
• Inquiry should include interviews with appropriate staff, who by level of training and knowledge of the resident, should be able to provide information about the causes of a resident’s condition or problem

Investigative Protocol
• Determination if the facility developed a care plan with interventions for the prevention of the development of an ulcer
• Determination if an interdisciplinary care plan was developed for the conditions identified
• Review documented interventions, such as pressure relieving devices, nutritional interventions and other measures, developed to provide an aggressive program of prevention and/or treatment

Case Scenario I
• 78 year old CVA immobile resident is admitted with recent weight loss. She is admitted on a regular diet and consumes <25% of each meal. She has a Stage I reddened area on her left heel and excoriated perineal area from urinary & bowel incontinence.

Case Scenario I
• Is she at-risk of developing a pressure ulcer?• Does she have a stage I pressure ulcer?• If so, how should it be coded on the MDS?• What should be considered for her plan of care?• When should the plan of care be implemented?• Who should implement the plan of care?

Case Scenario II
• 85 year old diabetic man was admitted to the facility with skin tear on his right shin that resulted from the stretcher transfer. His sacral area is reddened and he has a Stage 3 pressure ulcer on his left hip. His previous diet was regular with BID Ensure which he consumed between 25-50% . He is continent of bowel only.

Case Scenario II
• How many ulcers will be coded on M1?
• Where should the ulcers be coded on the MDS?
• What physician orders are needed for the resident’s immediate care upon admission?