Embed Size (px)
Citation preview
VOL.1 NO.2 1988
PRESSURE SUPPORT AND FLOW BYGOOD NEWS FOR THE VENTILATED PATIENT
Heidi HughesRN ICRN CIG MedishieldNSW Ventilator Specialist
~} 1~9~sur'e SUPPOt~t and Flow By are twoof themost recent forms of mechanical ventllatorysupport. Although they work using differentmethods , theend result is the same; areduction in the patient's work of breathing.Pressure Support is currently found on mostof the current generation venttlatorsincluding thePuritan Bennett 7200A.Siemens Servo 900C, Bear 5. EngstromErIka. and the Ohmeda CPU-l .
Flow By is however unique to and currentlyeveueo le on only one of these ventilators, thePur1tan Bennett 7200A Microprocessorventilator. as opposed to the continuous flowCPAP system on other ventilators.
In this paper I shall discuss PressureSupport and Flow By in turn. covering basicprinciples, use of and potential clinicalapplications of each one. I shall bereferencing to thePB7200A as themajorityof myexperience with these two new modeshas been with this machine, and as statedpreviously. is the only machine capable ofFlow By in the form discussed here.
PRESSURE SUPPORT VENTILATION
Pressure Support Ventilation (PSV.) is aform of mechanical ventilatory support thataugments the patient's spontaneousventilatory effort with apreset amount(Clinician selected) of positive airwaypressure. This inspiratory pressure isgenerally delivered in asquare wave patternthat begins with apatient's inspiratoryeffort. and on thePB7200A. terminates wheneither 1) The patient pressure exceeds thepositivepressure settlng by 1.5cmH20, or
21
2) When inspiratory flow drops below5LPM.( 1,8)
PSV is similar in it's concept to some of theolder forms of pressure assisted ventilation ,e.g. IPPV, but differs from these modalitiesin that pressure and flow are servocontrolled with PSV and most venttletoesequipped todeliver PSV incorporatecomprehensive alarm systems. ( 1). The useof artificial airwaysand gas de11very circuitsin mechanical ventllation to control thepatient's airwayI cause a hIgh resistance togas flow thereby increasing the patient'swork of breathing.
Because patients With Cardiopulmonarydisease experience an increased work. ofbreathing (WOB) during weaning frommechanical ventilation, it would bereasonable to expect that gas deliverysystems that reduce the WOB may thereforefacilitate the weaning process. Thus bymatching the amount of PS to the resistanceto gas flow of the artificial airway. theinspiratory WOB on thepatient's behalf maybe greatly reduced.( 3) There arecurrentlytwo approaches to using PSV. The first is.touse a low level of PSV e.g. 5-1 O,emH20, toassist the spontaneous breeths'occurrtnqduring tMV. This level of P-SV promotespatient comfort and reduces the spontaneousbreathing workload imposed by demand flowsystems and high resistance endotrachealtubes which compromise muscle function andpatient comfort.
The ventilatory adjustments and weaningstrategy for this approach to PSV areessentially thesame as those for IMV and thismethod has been shown to greatly reduce theoxygen (Emends of the patient. ( 4.5)
The second approach is t.o use high levelor
COHFEDERATIOH OF AUSTRALIAN CRITICAL CARE NURSES JOURNAL
total PSV as a stand alone ventilatory mode.( 6)
In this approach. the level of inspiratorypressure is adjusted to provide a desired tidalvolume and minutevolume. This method isgenerally used in patients who are difficult towean because of ventilatory muscledysfunction but have spontaneous ventilatorydrives.( 4)
There are twoOOvantages to using PSV in thisw~.
1. Patient comfort is increased over thatwith IMV as the patient controls both theinspiratory and expiratory time of everybreath giving a regular pattern ofventilation with PSV supported breaths.
2. The magnitude and characteristics ofpatient work can be changed substantiallyby these higher levelsof PSV. Not onlydoes it reduce oxygen demands but it alsoreduces the pressureper volume changecharacteristics.
One other point to remember when usingPSV. is that most systems today have a fixed,rapid initial flowrate, thatm~ not betolerated by some patients. COnversely, tooslow a flowrate may not provide maximalpressure supporting effects. Therefore.foroptimal use of PSV an adjustable flowrate 1sreQuired.( 1)
The PB 7200A is capable of flowrates of up to120 LPM with supplemental flowrates of upto 180 LPM evetlenle, PressuresupportleveIs of + 1 to +30 cm H20are available.(Soon to be increased to + 1 to + 70 em H20. )
The mode is active in SIMV AND CPAP duringspontaneous demand breathing, and actual
22
delivered value is ctsplevec both digitally andon an analogue meter. Most of the ventilatorson themarket have varying levels of PSVavailable, and most use different algorlttlmsto calculate these levels.
Acalculated level of PSV may be obtained bythe followingequation:
PS Level =RSM XPSF /60
Where RSM =steuc rtecnemc Patlent AirwayResistance (cmH201 1/sec.)
PSF =Peak Spontaneous Flow ( 1/mtn.)60 =Conversion Factor between l/see and
l/min.
Please note these values arederived from theRespiratory Mechanics Manouvres eo le to beperformed on the PB 7200A. (8).
FLOW BY
Flow By is a form of ventilatory supportunique to the PB 7200A ventilator. asopposed to thecontinuous flow CPAP systemsavailable on some of theother ventilators onthe market. It 15designed to rmmrmze thetime delay between the patient's initiation ofan tnsotretorv effort and the supp Iy of gas tothe patient "wye"during spontaneousbreathing.
When the mode is invoked, the ventilatordelivers aconstant flow or gas through thepatient ctrcutt during exhalation. Thisconstant flow is known as the BASE FLOW andis cltructen selected. As 8 result, fresh gas 15
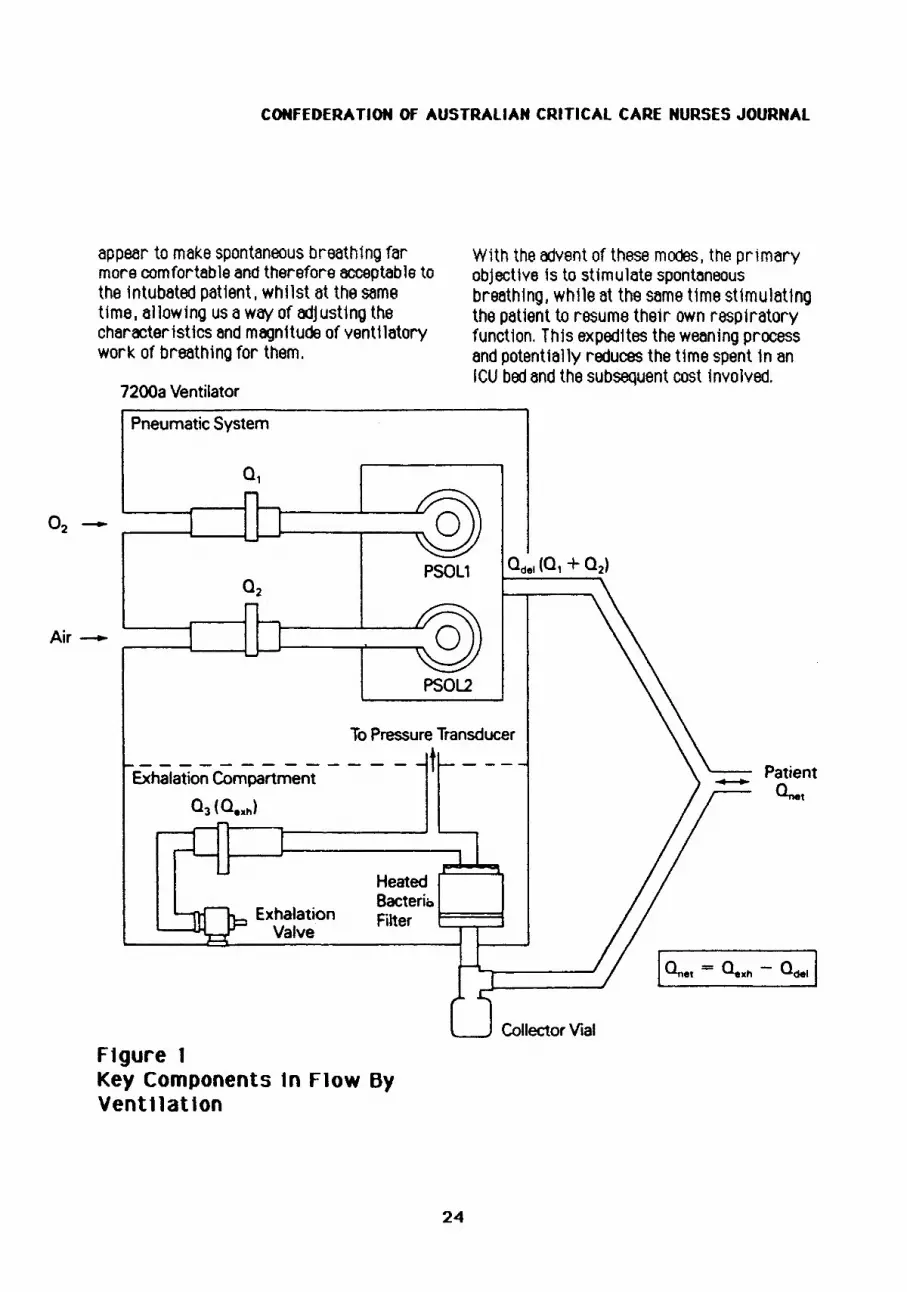
evat lable to the pat tent as soon as aninspiratory effort is initiated. The Flowsensors in the PB 7200A monitor the flowdelivered, (Ode]) I the now exhaled, (Qexh),and then computes the nat flow, (Qnel).
VOL.l NO.2 1988
Therefore Onet =Qexh - Qdel. (7) see figure1.
Base Flow is comprised of the combined flowthrough theoxygen and air sensors. The flowis mixed and travels into the patient circuit,(Odel). Thus just prior to inspiration Odelequals the base flow.
Net Flow or FLOW SENSITIVITY, is the rateofflow inhaled by the patient which will triggerinspiration from the ventilator. e.g. we setabase flow of20 LPM and a flow sensitivity of2LPM. When the exneletton flow sensordetects a drop of 2LPM from the 20LPM baseflow 1t is prOViding, it calculates that thepatient has commenced inspiration. Themachine then drops it's base flow down to5LPM and normal inspiratory flow occurs.When exhalation is detected the machine thenrecommences base flow at the presetamount.
Base Flow can be set at between 5-20 LPMwith a possible supplemental flow ofup to180 LPM.
Flow sensitivitycan be set at between 1- 10LPM for best performances.
so WHAT HAPPENS DmING THEEXPIRATORY PHASE?
When the amount being exhaled exceeds theamount being delivered by the flowsensitivity, exhalation beg1ns. This is causedby patient exhalation. Once the exhalation 1sdetected, base flow is temporarily reduced to5 LPM to reduce expiratory resistance, andthe flow sensitivity sets itselfto3 LPN forinspiratory detection during this phase.Therefore, when the end of expiration Isdetected by the flow sensor, base flowresumes at the operator set level. Peep is
23
created by using the exhalation valve asaflow reliefvalve. (8)
It is interesting to note that:
Aflow sensitivity system is more responsivetopatient effort than a pressure sensitivitysystem, however for safety reasons, the PB7200A has a preset pressure sensitivity of3cm H20 toprovide a backup to the flowsens1t1vity trigger.
Therefore in theor1sing, a pressuresensitivity setting of 2 cm H20 couldpotentially mean the pat1ent has togenerate aflow of up to 100mlIsee to tnttietetnsplretton, With a flow sensitivity settingof 1LPM however, the patient only has todraw as little s 16ml/see flow to triooer themachine into the inspiratory cycle.
The Flow By option is available in SIMV andCPAP modes of ventnenon. Consequently I
once 1nspirat1on 1s sensed, the vent1latorswitches from base flow to normal delivery I
be 1t spontaneous or mandatory. Forspontaneous breath delivery, the flow ratedelivered, is thet flow rate required to .metntetn the pressure in the patient circuitat Peep. For a mandatory breath, after theflow sensitivity value is reached, the flow tsdelivered according to the operator set peakflow and waveform setting.
CONCLUSION
Thus is appears we have two 1nteresting newmodes of ventilatory support available. Onebeing pressure assisted and found on many ofthe current generation ventilators, the otherbeing volume assisted, and in the formdescribed, currentlyavailable on only one oft.he newer ventilators, Both these modes
CONFEDERATION OF AUSTRALIAN CRITICAL CARE NURSES JOURNAL
appear to make spontaneous breathing farmore comfortabte and thereforeacceptab1e tothe Intubated patient I whllst at thesametime. allowing us awftY of adjusting thecharacteristics and magnitUde of ventl1atorywork of breathing for them.
7200a Ventilator
With the advent of these modes, the primaryobjective ts to stimulate spontaneousbreathing, whl1e at thesame t1me stimulatingthe penent to resume their own respiratoryfunction. Th1s expedites theweaning processand potentially reduces the time spent 1n anleu bed and the subsequent cost involved.
PneumaticSystem
PatientQ".t
IOnet = °8llh - °del ICollector Vial
HeatedBacteriaFilter F===lExhalation
Valve
To PressureTransducer
------------- t ---Exhalation Compartment
0 3 (Q."h)
PSOL2
Air-
FIgure 1Key Components In Flow ByVentilatIon
24
VOl.. 1 NO.2 1988
REFERENCES
1. Macintyre, N.R. (1986). Pressuresupportventilation. Respiratory care31 .3.189- 190
2. Gibney, R.T .• Wilson. R.S. andPontopploen, H. (1982). Comparison ofWOB on high gas flow and demand valvecontinuous positive pressure systems.~ 6.692-695.
3. Field. 5.. Kelly. S.M. and Macklem, P.T.The oxygen cost of breathing in patientswith cardiorespiratory disease.Amerjcan Review of Respiratory Diseases126.9
4. Macintyre, N.R. (1986). PSVPotential clinical applications.Problems In pulmonary Diseose2.4.1-7
5. Kanak. R.. Fahey. P.J.•Wanderwarf. C.(1985). Oxygen cost of breathing.changes dependant upon mode ofventilation.~ 87.126-127
6. Prekesh.O.• Mey.S. (1985).Cardiopulmonary response to inspiratoryP.5. during spontaneous ventilation vsconventional ventilation.~ 88,403-408
7. Puritan Bennett Communications.(1986). Ventilation file - Flow by.~ 1-3.
8. Puritan Bennett Corporation. (1987).PB 7200A Operators ManualSupplements, Pressure Support andFlow By.
25