Embed Size (px)
Citation preview

399
AACN Advanced Critical Care
Volume 19, Number 4, pp.399–411
© 2008, AACN
Pressure Modes of Mechanical VentilationThe Good, the Bad, and the Ugly
Suzanne M. Burns, RN, MSN, RRT, ACNP, CCRN, FAAN, FCCM, FAANP
Numerous pressure modes are currently
available on ventilators. The application of
microprocessor technology has resulted in
sophisticated mode options that are very
responsive to patient-initiated efforts, yet
little is known about how to use the modes or
their effect on patient outcomes. This article
describes a wide variety of pressure modes
including traditional modes such as pressure
support and pressure-controlled ventilation
in addition to less traditional new modes
such as airway pressure release ventilation,
biphasic positive airway pressure, Pressure
Augmentation (Bear 1000, Viasys Healthcare,
Yorba Linda, California), Volume Support
(Maquet, Bridgewater, New Jersey), Pressure
Regulated Volume Control (Maquet, Bridge-
water, New Jersey), Volume Ventilation Plus
(Puritan Bennett, Boulder, Colorado), Adap-
tive Support Ventilation (Hamilton Medical,
Switzerland), and Proportional Assist Ventila-
tion (Dräger Medical, Richmond Hill, Ontario,
Canada). The “good, the bad, and the ugly”
issues surrounding the application, evaluation,
and outcomes of the modes are discussed.
Keywords: advanced pressure modes,
mechanical ventilation, pressure modes of
ventilation
A B S T R A C T
who manage the patients and are charged witheducating others about the application andassessment of the modes, are unsure of whenand how best to use them.
Confusion related to mode application is, inpart, a result of the manufacturer-selected modenames that are often different from one anotherdespite the fact that the modes may functionquite similarly and are iterations, albeit moresophisticated and purportedly improved ver-sions, of traditional modes. This distressing factis further complicated by the tendency of theventilators to have numerous other parametersettings available for adjustment that have little
Mechanical ventilator modes have becomeprogressively more sophisticated with
the advent of microprocessor-controlled tech-nology. The ability of engineers and scientists todevelop ventilators that respond rapidly topatient-initiated breaths and cycle extremelyquickly between ventilatory phases hasresulted in modes that are very attractive foruse with some of our most critically illpatients.1 Unfortunately, the best use of themodes, especially as they relate to the manage-ment of the critically ill patient with respira-tory failure, has not been clearly elucidated. Inthe past, volume modes of ventilation were thestandard, but now a wide variety of pressuremodes have emerged and are in use. Many ofthe modes are complicated, and despite apaucity of clinical trials that demonstrate theirefficacy, proponents suggest their superiority.Understandably, bedside clinicians and APNs,
Suzanne M. Burns is a Professor of Nursing in the Acute
and Specialty Care Program, School of Nursing, and an
APN 2, Medical Intensive Care Unit, University of Virginia
Health System, Box 800782, Charlottesville, VA 22903
AACN1904_399–411 22/10/08 11:34 PM Page 399

BURNS AACN Advanced Cri t ical Care
400
demonstrated scientific effect on patient out-comes. Thus clinicians often feel underedu-cated about the modes and the best use of thesame. This is unfortunate because understand-ing the modes is essential if optimal care is tobe ensured.
The purpose of this article is to describeselected pressure modes and the science relatedto their efficacy and use. When possible, themodes are classified in categories to better illus-trate the similarities and important differencesbetween the modes. This article discusses bothtraditional and nontraditional pressure modeoptions such as pressure support ventilation(PSV), pressure control (PCV) and pressure-controlled inverse-ratio ventilation (PC-IRV),airway pressure release ventilation (APRV),biphasic positive airway pressure, volume-assured pressure modes (ie, Pressure Augmen-tation, Volume Support [VS] [Maquet,Bridgewater, New Jersey], Pressure RegulatedVolume Control [Maquet, Bridgewater, NewJersey], and Volume Ventilation Plus [PuritanBennett, Boulder, Colorado]), automatic tubecompensation (although not really a mode perse, some use it as such), Adaptive Support Ven-tilation (Hamilton Medical, Switzerland), andproportional assist ventilation (PAV). The useof the modes from the acute to the weaningstages of ventilation is discussed as applicable.
Throughout this article, selected specificventilator mode names are referenced as repre-sentative examples of mode options in aneffort to help clarify similarities and differ-ences. It is not the intention of the author toprovide an exhaustive list of those available onall ventilators today but rather to provideinformation to the reader so that ventilator
pressure modes and their application might bebetter understood.
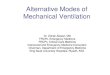
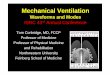
Pressure Mode Characteristics:An OverviewTraditional volume modes of ventilation, mostnotably assist control (AC) and synchronizedintermittent mandatory ventilation (SIMV),although still widely used are becoming lesspopular than pressure modes. In contrast tovolume modes, pressure modes were initiallyconfigured to ensure that a clinician-selectedinspiratory pressure level (IPL) was providedon a breath-to-breath basis, volume variedwith each breath. All pressure modes are asso-ciated with a “decelerating” flow pattern dur-ing inspiration. This decelerating flow patternrepresents the speed of the gas, which is ini-tially very high but gradually lowers as thechest fills. This characteristic flow pattern isconsidered more physiologic than that associ-ated with volume-based ventilation and maycontribute to better gas distribution as well(Figures 1 and 2).2 In part, it is the deceleratingflow pattern that has driven the developmentof newer and more sophisticated pressuremodes of ventilation.
In many of the earlier ventilator models, theselection of a pressure mode required that theclinician select the mode (ie, PSV or PCV) andthe desired pressure level. With these pressuremodes, pressure is stable and volume is variabledependent on compliance (lungs and chest wall)and resistance (airways). However, some newerpressure modes require that the clinician selectfirst the mode (which may or may not have“pressure” in the title) and then the relatedparameters that further define the characteristics
Figure 1: Square flow waveform: Volume breath, where the path from A to B represents insipiration, the
path from B to C represents expiration, D represents end-insipiration, and E indicates peak expiratory flow.
Abbreviations: INSP, inspiration; EXP, expiration; V., flow; L/min, liters per minute; S, seconds. Used with
permission from Nellcor Puritan Bennett LLC, Boulder, Colorado, part of Covidien (formerly Tyco Healthcare).
AACN1904_399–411 22/10/08 11:34 PM Page 400

VOLUME 19 • NUMBER 4 • OCTOBER–DECEMBER 2008 PRESSURE MODES OF MECHANICAL VENTILATION
401
of the mode such as the desired tidal volume(VT). In addition, many of the new modes whileproviding a decelerating flow pattern, asdescribed above, may sacrifice pressure limita-tion in an effort to ensure the desired volume. Instill other pressure modes, variations in bothvolume and pressure are allowed with patient-initiated breaths during the inspiratory and expi-ratory (I/E) ventilator respiratory cycles.Descriptions of these and other selected pressuremodes follow and are summarized in Table 1.
Pressure Support VentilationDescriptionPressure support ventilation is a mode of ven-tilation that augments or supports a sponta-neous inspiration with a clinician-selectedpressure level. The mode is a popular andcommonly used mode of ventilation. Althoughinitially proposed to be a mode for weaning,PSV is also used to ventilate less stable condi-tions. This mode is available on virtually allventilators for use as a stand-alone mode or incombination with others. It is relatively easy toapply and manage because it requires fewparameter adjustments.
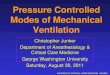
Once the clinician selects a PSV level, thepressure rises rapidly to a plateau (the selectedpressure) and the pressure is maintainedthroughout inspiration (Figure 3). Termina-tion of inspiration occurs when flow dimin-ishes to one fourth of the original flow (ordepending on the ventilator, some predeter-mined diminution of flow). Because this is aspontaneous breathing mode, no rate is set,and the patient controls the inspiratory time
(Ti), respiratory frequency (f x), and VT witheach breath. The work of breathing associatedwith the mode is dependent, in large part, onthe selected pressure level. Higher levels mayprovide nearly total ventilatory support,3,4 andthe level can be adjusted gradually to providefor graded endurance-training intervals.4,5
Pressure support ventilation is often usedin conjunction with other modes such asSIMV. When combined with SIMV, it is usedto offset the work of breathing associatedwith spontaneous breathing through artificialairways and circuits.6 Thus the adjustment ofthe PSV level provides either more or lesswork accordingly. There is some evidence thatthe combination of SIMV and PSV when usedas a mode for weaning may contribute tolonger weaning times.7 In addition, very highlevels of PSV, especially in patients withobstructive disease conditions, may increasethe incidence of auto–positive end-expiratorypressure (auto–PEEP) and ineffective patientefforts to trigger the ventilator.8
ParametersParameters used to set PSV include PSV level,sensitivity, positive end-expiratory pressure(PEEP), and the fraction of inspired oxygen(FIO2).
Pressure Control and Pressure-Controlled Inverse-Ratio VentilationDescriptionModes with “control” or “mandatory” in thetitle suggest that the mode has a set respiratoryfrequency (fx) and, by extension, a preselectedTi for the mandatory breaths. Pressure controlventilation is one such mode. When the modewas first introduced, it was proposed for use inpatients with acute respiratory distress syn-drome (ARDS). The goal of the mode was tocontrol the airway pressure (it was unclear atthe time if peak, plateau, or mean pressurescontributed to lung injury) and optimize gasdistribution by means of the decelerating flowpattern. It could be used with traditional I/Eratios or the ratios could be inverse, thus thename inverse-ratio ventilation.9–12 Because thelungs of patients with ARDS are noncompli-ant, stiff, and prone to collapse, investigatorshypothesized that by changing the I/E ratiosfrom the traditional 1:2, 1:3 patterns to inverseratios (ie, 1:1, 2:1, 3:1, 4:1), the ARDS lungmight be “kept open”—essentially what wenow refer to as “recruitment”—and prevented
Figure 2: Decelerating flow waveform: Pressure
breath. Abbreviations: INSP, inspiration; EXP,
expiration; V., flow; L/min, liters per minute; S,
seconds. Used with permission from Nellcor
Puritan Bennett LLC, Boulder, Colorado, part of
Covidien (formerly Tyco Healthcare).
AACN1904_399–411 22/10/08 11:34 PM Page 401

BURNS AACN Advanced Cri t ical Care
402
Table 1: Examples of Pressure Modes and Parameters
Mode Name
Pressure support
Pressure control
ventilation
Pressure-controlled
inverse-ratio
ventilation
Airway pressure
release ventilation
Volume-assured
pressure modes
(1–5 below)
1. Pressure
augmentation
(Bear 1000)
2. Volume Support
(Siemens)
3. Pressure
Regulated
Control
(Siemens)
Main Parameters
Pressure support level, sensitivity,
FIO2, and PEEP
Inspiratory pressure level, fx, Ti,
sensitivity, FIO2, and PEEP
As for pressure control ventilation,
but an inverse inspiratory/
expiratory ratio is attained by
lengthening the T i. Inverse ratios
include 1:1, 2:1, 3:1, and 4:1.
Pressure high: high CPAP level;
pressure low: generally 0–5 cm
H2O; time high; time low, and
FIO2.
These modes provide pressure
breaths with a volume guarantee.
Spontaneous mode: VT, sensitivity,
FIO2, and PEEP
Control mode: As per spontaneous
mode plus fx and Ti
VT, sensitivity, FIo2, and PEEP
fx and Ti set in addition to those set
for VS.
Comments
Often, pressure is arbitrarily selected
(eg, 10–20 cm H2O) and then adjusted
up or down to attain the desired tidal
volume. Some use the plateau
pressure if transitioning from volume
ventilation as a starting point.
Variants of pressure control
ventilation include volume-assured
pressure options and some other
modes such as airway pressure
release ventilation and BiLevel
ventilation. They are listed below.
Some ventilators allow for the
inspiratory/expiratory ratio to be
selected.
Generally, the CPAP level is adjusted
to ensure adequate oxygenation,
and the fx of the releases are
increased or decreased to meet
ventilation goals. VT is a variable
dependent on the CPAP level,
compliance and resistance of the
patient, and the patient's
spontaneous effort.
These modes are ventilator specific.
Although the similarities are
greater than the differences, they
are called by different names.
Often, the names suggest that the
mode is a volume mode, yet a
decelerating flow pattern
(associated with pressure
ventilation) is always provided.
This mode starts the breath as a
pressure breath. If calculations
automatically done by the ventilator
determine that the desired VT will
not be attained, the ventilator
provides the remainder of the
breath as a volume breath. This
changes both the flow pattern and
the pressure level of the breath.
The pressure level is automatically
adjusted to attain the desired VT. If
control of pressure is desired, it
must be carefully monitored.
As with VS. The difference is that this
is a control mode. However,
spontaneous breaths may also occur.
(continues)
AACN1904_399–411 22/10/08 11:34 PM Page 402

VOLUME 19 • NUMBER 4 • OCTOBER–DECEMBER 2008 PRESSURE MODES OF MECHANICAL VENTILATION
403
Table 1: Examples of Pressure Modes and Parameters (Continued)
Mode Name
4. Volume Support
(Puritan Bennett
840)
5. Volume Control
Plus (Puritan
Bennett 840)
BiLevel Positive
Airway Pressure
(Puritan Bennett
840) (other forms
of this exist by
different
manufacturers)
Adaptive Support
Ventilation (Galileo
and Raphael
[Hamilton Medical])
Automatic tube
compensation
Proportional assist
ventilation
Main Parameters
VT, sensitivity, FIO2, and PEEP
fx and Ti are set in addition to those
set for VS.
PEEPH, PEEPL, fx, and Ti
Body weight, %MinVol, and high
pressure limit
Endotracheal tube internal diameter
and percent compensation
Proportional pressure support
(Drager Medical, Richmond Hill,
Ontario, Canada): PEEP, FIO2, percent
volume assist, and flow assist
Proportional assist ventilation plus
(Puritan Bennett, now Covidien)
PEEP, FIO2, and percent support
Comments
This mode is one option in a
category called Volume Ventilation
Plus. This is the spontaneous
breathing option in this category
and is similar to VS above.
This mode is also a mode option
listed in the category called
Volume Ventilation Plus. To access
this mode, the user selects the
synchronized intermittent
mandatory ventilation or assist
control (both control modes) and
then selects volume control plus.
For some clinicians, this is
confusing because it appears that
the patient is on 2 different modes
versus Volume Control Plus.
If additional support is desired for
patient-initiated breathing, PSUPP
may be selected as well. Attention
to VT is important because the
patient can augment VT
significantly with supported
spontaneous breaths.
Once basic settings are selected,
adaptive support ventilation is
started and %MinVol is adjusted if
indicated. Spontaneous breathing
is automatically encouraged and
when the inspiratory pressure
(PINSP
) is consistently 0 and fx
control (rate) is 0, extubation may
be considered.
This is not a mode but rather a
pressure option to offset the work
associated with tube resistance. It
can be combined with other
modes or used alone as in a CPAP
weaning trial.
Depending on the ventilator, the
amount of “assist” to be provided
is determined by the clinician,
and different parameters are
selected to do so. Default percent
support numbers are recommen-
ded, but the clinician must
determine the timing of reduc-
tions of the same.
Abbreviations: CPAP, continuous positive airway pressure; FIO2, fraction of inspired oxygen; fx, respiratory frequency; PEEP, positive end-expiratory pressure; PEEPH, PEEP High; PEEPL, PEEP Low; %MinVol, minute volume; PSUPP, pressure support; Ti, inspiratory time; VS, volumesupport.
AACN1904_399–411 22/10/08 11:34 PM Page 403

BURNS AACN Advanced Cri t ical Care
404
from “derecruiting” during the expiratoryphase of ventilation.9–13 Although the idea wasright on target with what we now know aboutrecruiting a lung with ARDS, studies did notdemonstrate an improvement in mortality. Thisis in part because the assessment of lungrecruitment often focused on the effect of themode on oxygenation versus lung protec-tion;9–12 tidal volumes and pressure levels werenot controlled nor was the effect of PEEPand/or auto-PEEP induced by the inverseratios.14 Recent studies have demonstrated thatlow-VT ventilation15 and the use of relativelyhigh levels of PEEP are necessary to prevent“volu-trauma” and repetitive opening injurysecondary to inadequate lung recruitment.13
The studies have shown that the appropriateapplication of the protective lung strategiesdoes decrease mortality in these patients.
Earlier iterations of PCV modes did not allowfor adequate flow delivery during a patient-initiated breath. Patient-initiated breathing, andeven patient movement in some cases, resultedin oxygen desaturation. Sedation and neuromus-cular blockade were frequently necessary toensure control. Ventilator manufacturers havesubsequently addressed this and other relatedissues by designing and introducing modalitiesthat allow for adequate flow delivery for sponta-neous breathing during control breaths.
ParametersPressure control ventilation parameters includepressure level (often called inspiratory pressurelevel to distinguish it from PSV), fx, Ti, FIO2,PEEP, and sensitivity (ie, pressure or flow-trig-gering). If PC-IRV is desired, the same parame-ters are adjusted, but Ti is lengthened to attainthe desired I/E ratio.
Airway Pressure Release VentilationDescriptionAirway pressure release ventilation is a modethat allows for spontaneous breathing at a pre-
set continuous positive airway pressure (CPAP)level and that is interrupted at a clinician-deter-mined fx by a short (1- to 1.5-second) pressurerelease (to a lower baseline or to zero pressure).The mode is designed for spontaneously breath-ing patients such as those with ARDS whorequire a high level of pressure to effectivelyrecruit alveoli. In the case of APRV, this CPAPlevel is often in the 15 to 20 cm H2O range. Theshort “releases” assist with CO2 elimination(they allow for more uniform emptying of alve-oli with different time constants) and areincreased or decreased accordingly. Derecruit-ment of alveoli occurs if the fx releases aregreater than 1.5 to 2.0 seconds in duration. Theshort airway pressure releases are the hallmarkof APRV and set it apart from PCV and biphasicventilation (there are many ventilator-specificnames for this mode option; see below) in thatthere is no true conventional expiratory phase.This may be considered a form of PC-IRV inthat the idea is to encourage lung recruitment byprolonging inspiration at a set pressure whilepreventing derecruitment with a very short pres-sure release.16–19 The mode appears to be as safeand effective as conventional volume or PCventilation16–22 with the additional advantage ofallowing spontaneous breathing throughout allphases of the respiratory cycle, thus obviatingthe need for heavy sedation and paralyticagents.21,23 In the past, the use of sedation infu-sions and paralytic agents has been recom-mended to ensure patient-ventilator synchronyespecially with the use of some traditional con-trol modes of ventilation. Studies have demon-strated that this practice is associated withnegative clinical outcomes such as increased ven-tilator duration, longer critical care unit and hos-pital lengths of stay,24–26 and other morbidities(eg, ventilator-associated pneumonia, gastroin-testinal bleeding, deep-vein thrombosis, andbacteremia) and thus is to be discouraged.27 Inreality, the spontaneous breathing pattern ofpatients on this mode of ventilation is often very
Figure 3: Square pressure waveform: Pressure breath.
AACN1904_399–411 22/10/08 11:34 PM Page 404

VOLUME 19 • NUMBER 4 • OCTOBER–DECEMBER 2008 PRESSURE MODES OF MECHANICAL VENTILATION
405
rapid. Although generally a “rapid-shallow”breathing pattern heralds fatigue, it is unknownwhether this is true in a fully recruited(distended) lung.
ParametersAirway pressure release ventilation parametersinclude the pressure high (PHIGH), which is thehigh CPAP level; pressure low (PLOW), which isgenerally 0–5; the time high (THIGH); the timelow (TLOW); and FIO2. Generally, the CPAP levelis adjusted to ensure adequate oxygenation,and fx of the releases are increased ordecreased to meet ventilation goals. Tidal vol-ume is a variable dependent on the CPAP level,compliance and resistance of the patient, andthe patient’s spontaneous effort.
Biphasic modesBiLevel Positive Airway Pressure (PuritanBennett 840 [Puritan Bennett, Boulder, Col-orado]);28 Bi-Vent (Servo I [Maquet, Inc.,Bridgewater, New Jersey]);29 BIPAP (Evita XL[Dräger Medical, Inc., Telford, Pennsylva-nia]);30 DuoPAP (Galileo [Hamilton Medical,Reno, Nevada]);31 Biphasic (AVEA [ViasysHealthcare, Yorba Linda, California]).32
DescriptionBiphasic modes are similar to PCV and APRVin that the clinician selects IPL and PEEP levelsas well as fx and Ti (in the case of APRV the lowlevel is very short, as previously described). Butunlike conventional PCV, the modes allow forunrestricted spontaneous breathing during theI/E cycles. The modes employ an active exhala-tion valve that vents excess flow during thepatient’s spontaneous breathing while main-taining the pressure level of the control breaths.Names for what would conventionally becalled IPL and PEEP vary with the ventilator.For example, with the Puritan Bennett model,the high pressure level is referred to as PEEPHigh (PEEPH), which is the same as IPL in tra-ditional PCV, and PEEP Low (PEEPL), which isPEEP in traditional PCV. Spontaneous breath-ing at both levels can be augmented with PS(PSUPP) or tube compensation (described below)dependent on the ventilator. Tidal volume isdependent on the PEEPH and PEEPL levels andresistance and compliance of the lung and chestwall, however, is augmented by the patient’sspontaneous breathing at the high level. Thismay make the attainment of a lung protectiverange of VT (ie, 6 mL/kg) difficult. Plus, as noted
earlier, breathing patterns at the 2 levels of highand low support vary and are often rapid.Dependent on the specific ventilator, APRVand biphasic modes may be accessed via thesame mode parameters. Time in inspirationand expiration distinguishes the distinct mode.Some ventilators call this THIGH and TLOW.However, as noted earlier, with APRV, therelease time to the PEEPL level is very short.
Although biphasic ventilation is oftenconsidered a form of PCV, studies have soughtto determine whether the mode decreases thework of breathing using PSV as the comparisonmode. Two studies comparing PSV to biphasicdefined the work of breathing by measuring the pressure-time product.33,34 Interestingly,although the work of breathing was increasedin BiLevel in comparison with PSV, theincreased work of breathing did not translateinto an increased oxygen consumption orcarbon dioxide production.34 As noted in thestudies on APRV, the ability to breathe sponta-neously throughout the respiratory cycle with-out adversely affecting oxygenation may be adistinct advantage because rapid breathing pat-terns associated with desaturation of oxygensuggests ventilator tolerance and the need foranalgesics and sedatives.21,23 In another study ofadult cardiac surgery patients, the use of bipha-sic ventilation was compared with controlledvolume ventilation and intermittent mandatoryventilation. The biphasic group required signifi-cantly less analgesics and sedatives.35 A 70%reduction in neuromuscular blockade and a30% reduction of benzodiazepine use wererequired to maintain a bispectral index level of70 in the patients.
ParametersParameters for setting biphasic modes varybetween ventilators but include PEEPH, PEEPL,fx, and Ti. If additional support is desired forpatient-initiated breathing, PSUPP may be selectedas well. In other ventilators, the high and lowlevels may be defined by IPL and PEEP, and I/Etimes as THIGH or TLOW, as described for APRV.
Volume-Assured Pressure ModesDescriptionVolume-assured pressure modes are modes thatcombine PSV with a decelerating flow patternand a guaranteed volume.36 The modes weredeveloped to ensure that the desirable charac-teristics of pressure ventilation were availablefor use without sacrificing volume (especially
AACN1904_399–411 22/10/08 11:34 PM Page 405

BURNS AACN Advanced Cri t ical Care
406
in the case of unstable patients or with changesin patients’ conditions). Early reports suggestedthat in patients with acute respiratory failure,the mode resulted in lower workload and ven-tilatory drive, better patient-ventilator syn-chrony, and less auto-PEEP while ensuring adesired VT.36 This category includes numerousmodes developed for specific ventilators. Themodes, while bearing different names, are simi-lar as are many of the parameters required toapply the modes.
Pressure Augmentation (Bear 1000 [Viasys Healthcare, Yorba Linda, California])37
With this ventilator mode, the breath starts asa pressure breath, but if the calculatedmechanical properties of the airways, lung,and thorax predict that the patient will notattain the desired VT, the ventilator willdeliver the rest of the breath as a volumebreath (Figure 4). Thus, if the desired volumeis set inappropriately high, the goal of pres-sure breath delivery (decelerating flow) is lostas is the limitation of pressure. It is importantthat when using the mode, the clinician moni-tor transitions between pressure breath deliv-ery and volume breath delivery. One way todo this is to observe the respiratory wave-forms (see Figure 4). If the clinician observesfrequent transitions from pressure breathdelivery to volume breath delivery, thecause(s) should be identified.
ParametersBoth spontaneous and control modes areavailable. They are distinguished by the selec-tion of ventilator parameters. Spontaneousmode parameters include VT, sensitivity, FIO2,
and PEEP. For a control mode, the clinicianmust also set fx and Ti.
Volume Support, Pressure Regulated Control (Maquet, Bridgewater, New Jersey)29
This ventilator manufacturer distinguishes thespontaneous breathing mode from the controlmode by using distinctly different names.Volume Support is a spontaneous breathingmode that adjusts the pressure level automati-cally (on the basis of lung mechanics) to attainthe clinician-selected VT. Once the clinicianselects the VS, the ventilator provides a testbreath and then adjusts the pressure level in 3cm H2O increments, with each subsequentbreath to ensure the desired volume (Figure 5).Pressure Regulated Volume Control (PRVC) issimilar, but as noted in the name, it is a controloption that means that in addition to theparameters selected for VS, the clinician mustset fx and Ti. The patient may initiate a sponta-neous breath between the control breaths andreceive a pressure breath. In this way, it is verysimilar in design to the pressure mode calledpressure assist/control.
ParametersVolume Support requires a set VT, sensitivity,FIO2, and PEEP. Pressure Regulated VolumeControl requires that fx and Ti be set in addi-tion to those set for VS.
Volume Ventilation Plus (Puritan Bennett 840 [Puritan Bennett, Boulder, Colorado)38
This manufacturer has 2 volume-guaranteedpressure modes that are classified under acategory called Volume Ventilation Plus,
Figure 4: Pressure waveform of pressure augmentation: When desired tidal volume cannot be delivered,
the ventilator supplies the remainder of the breath as a volume breath. A indicates beginning pressure
breath (square pressure waveform), and B, volume delivery (accelerating pressure waveform).
AACN1904_399–411 22/10/08 11:34 PM Page 406

VOLUME 19 • NUMBER 4 • OCTOBER–DECEMBER 2008 PRESSURE MODES OF MECHANICAL VENTILATION
407
which includes VS and Volume Control Plus(VC�). Although both sound like volumemodes, they are not. Instead, they are, likethe others discussed in this category, pressuremodes that guarantee a volume. They can bepatient or ventilator initiated. Volume Sup-port is described as a spontaneous mode thatdelivers a desired volume as a pressure breath(pressure is automatically adjusted breath bybreath to ensure VT). Volume Control Plus isthe mandatory option, and thus, fx and Ti areset. This manufacturer has integrated anactive exhalation valve into the mechanics ofthe ventilator that allows for the patient’sspontaneous breathing (excess flow is ventedand patient-ventilator synchrony enhanced)while maintaining the pressure level of thecontrol breaths. This function is not cliniciancontrolled.
ParametersVolume Support requires that VT, sensitivity,FIO2, and PEEP be set. Volume Control Plusrequires that fx and Ti be set in addition tothose set for VS (similar to PRVC describedearlier). To access this mode, the user selectsthe SIMV or AC (both control modes) andthen selects VC�. For some clinicians, this isconfusing because it appears that the patient ison 2 different modes (ie, PC and SIMV) versusVC�. The difference between the settings ofSIMV and AC is how the spontaneous breathsare delivered. In the SIMV mode, the VT andTi are patient determined versus in the ACmode, where the spontaneously initiatedbreaths receive the pressure required to attainthe desired VT.
Automatic Tube CompensationDescriptionAutomatic tube compensation (ATC) is notreally a mode but rather a ventilatory adjunct
available on many current ventilators that isdesigned to overcome the work of breathingimposed by the artificial airway. To that end,ATC adjusts the pressure (proportional totube resistance) required to provide a vari-able fast inspiratory flow during spontaneousbreathing. Automatic tube compensation isincreased during inspiration and loweredduring expiration, thus decreasing the workof breathing secondary to tube resistance.
The accuracy of ATC in compensating fortube resistance has been studied using amechanical model with 4 ventilators. Theauthors used a prototype model as the criterionstandard and compared results to ATC modelscurrently employed by newer ventilators.39 Thestudy found that the tube-related inspiratorywork of breathing was significantly decreasedbut the expiratory work of breathing was not.They found that the adapted and simplifiedATC systems on the newer ventilators wereinferior to the original prototypes.
Although this option does appear to bepotentially quite useful to decrease the workimposed by artificial airways, there is much tobe learned especially about how it works incombination with other modes of ventilation.Use of the option may increase auto-PEEP ifobstructive disease is present.
ParametersThe clinician enters the internal diameter sizeof the endotracheal tube and the desired per-centage of compensation.
Adaptive Support Ventilation(Galileo and Raphael [HamiltonMedical, Bonaduz, Switzerland])40
DescriptionAdaptive Support Ventilation (ASV) may beone of the most unique ventilator modesavailable today. Referred to by the ventilator
Figure 5: Pressure waveform of volume support: The pressure is increased in increments with each
breath to attain the desired tidal volume.
AACN1904_399–411 22/10/08 11:34 PM Page 407

BURNS AACN Advanced Cri t ical Care
408
manufacturer as “intelligent ventilation,” themode is designed to assess lung mechanics on abreath-to-breath basis (controlled-loop ventila-tion) for spontaneous and control settings.40 Itachieves an optimal VT by automatically adjust-ing the mandatory respiratory fx and inspiratorypressure. The working concept with this modeis that the patient will breathe at an fx and VT
that minimizes elastic and resistive loads. In allmodes, the opportunity for spontaneousbreathing is promoted (the user does not haveto switch back and forth from one mode toanother to encourage spontaneous breathingbecause this is automatically done). Thus theinteractions required by the clinician are few.The manufacturer suggests that this aspect of“intelligent ventilation” may decrease thepotential for operator error and save time—both desirable outcomes of any ventilator sys-tem. Built into the mode are algorithms that are“lung protective.” The protective strategies aredesigned to minimize auto-PEEP and preventapnea, tachypnea, excessive dead space, andexcessively large breaths.40
Outcomes associated with ASV are favor-able.41,42 In a study of 36 cardiac surgerypatients, randomly assigned to either ASV- orSIMV-protocolized weaning, weaning timewas significantly less with ASV.41 In addition,in a preliminary study of 10 patients early inthe weaning phase, ASV was compared withSIMV plus PSV to determine the mode’s effecton respiratory central drive, arterial bloodgases, sternocleidomastoid electromyographicactivity and hemodynamics.42 Adaptive Sup-port Ventilation performed comparably toSIMV plus PSV in most measures, with theexception of sternocleidomastoid activity,which was significantly less than with the useof PSV. The results suggest that ASV is aseffective as conventional ventilation and thatthe work of breathing may be decreased withthe mode.
ParametersParameters in this mode are very differentfrom those in most modes but include very fewsettings. They are ideal body weight, %MinVol(minute volume), and high pressure limit. Oncethese are set, ASV is started, and %MinVol isadjusted if indicated.
Proportional Assist VentilationProportional Pressure Support (PPS) (DrägerMedical, Richmond Hill, Ontario, Canada),43
Proportional Assist Ventilation Plus (PAV�)(Puritan Bennett, Boulder, Colorado).44
DescriptionFirst introduced in the early 1990s,45 the con-cept with Proportional Assist Ventilation(PAV) is to prevent fatiguing workloadswhile still allowing the patient to sponta-neously breathe. To that end, current PAVmodes take measurements throughout theI/E cycle and then automatically adjust thepressure, flow, and volume proportionally tooffset the resistance and elastance of thesystem with each inspiration (patient andcircuit). Recognizing that inspiratory effortis a reflection of ventilatory demand, PAVmay provide a more physiologic breathingpattern. Different names for the modes areprovided by specific manufacturers, andparameters that require adjustment varysomewhat between the ventilators.
Studies testing the effect of PAV on variablesof interest have yielded mixed results. In astudy of 12 patients with acute respiratoryfailure,46 the authors sought to determinewhether PAV would provide better compensa-tion to an increased ventilatory demand thanPSV. Results suggest that the effect of PAValone, and of PAV with ATC, on cardiorespira-tory function and inspiratory muscle unloadingwas not significantly different from that ofPSV. In another study,47 14 ventilator-depend-ent patients were monitored on PSV and PAV.Despite some differences noted in breathingpatterns between the modes, no difference wasnoted in gas exchange or other variables ofinterest. Reports of volunteers’ subjectiveassessment of comfort on PAV and PSV48 notedthat although PAV was more comfortable, bothmodes were uncomfortable at high levels ofsupport. And finally, in sleeping patients,49 PAVwas associated with fewer patient-ventilatorasynchronies and arousals compared withPSV. Although it is tempting to draw conclu-sions about potential uses of PAV, especially asa weaning mode similar to PSV, an editorial onthe topic50 cautions that it should not besimply investigated as a weaning modality butalso as a mode that may be used in sickerpatients as well. They note that this mode, likeothers discussed previously, allows for morepatient control and, ultimately, perhaps betteroutcomes in these patients. Studies are stillrequired to help us determine the use of PAV indifferent populations.
AACN1904_399–411 22/10/08 11:34 PM Page 408

VOLUME 19 • NUMBER 4 • OCTOBER–DECEMBER 2008 PRESSURE MODES OF MECHANICAL VENTILATION
409
ParametersProportional Pressure Support (PPS) (DrägerMedical, Richmond Hill, Ontario, Canada)includes PEEP, FIO2, volume assist, and flowassist (eg, volume and flow assist are set in per-centage [%]; if set at 80%, that is how muchsupport will be provided during the breath).Proportional Assist Plus (PAV�) (PuritanBennett, Boulder, Colorado) requires that a“% support” setting be adjusted (again thehigher the level, the more the support).
What we know about pressure modes:the good, the bad, and the uglyThe new pressure modes of ventilation appearto be safe and as effective as conventionalmodes, although more studies are required indifferent populations and conditions beforedefinitive recommendations can be made as totheir use in practice. They are attractive foruse for a number of reasons. The associateddecelerating flow pattern is desirable, and themodes provide us with many different poten-tial uses in a wide variety of conditions fromthe acute phase to the weaning phase. Themicroprocessor technology supporting themodes ensures faster flow responses and,subsequently, the ability of the patient to par-ticipate in breathing potentially without nega-tively affecting oxygenation, ventilation, andthe work of breathing. In addition, this fea-ture of patient participation, even with highlevels of support, suggests that the applicationof at least some of the modes may obviate theneed for heavy use of analgesics and sedatives,which we know compromise other outcomessuch as ventilator duration and the intensivecare unit and hospital lengths of stay.
To date, however, no studies demonstratethe superiority of the modes in any patientpopulation. Most of the studies are not ran-domized controlled trials and suffer from thedeficiencies of design, small sample size, andlimited trial duration in selected categories ofpatients. And, although the modes do allowfor much improved patient ventilator interac-tion, much has yet to be learned about theeffect of the modes on work of breathing,especially during the acute phase of respira-tory failure when unloading the respiratorymuscles has traditionally been the goal tooffset fatigue. Does a fatiguing pattern ofbreathing result in respiratory failure if the lung is optimally recruited and how bestdo we use the modes to recruit the lung?
Studies are needed to help us determine suchoutcomes.
The sophistication of the new pressuremodes and the profusion of the same, althoughcommendable from a technology perspective,have provided us with a bit of a conundrum.Unfortunately, the mode names are often con-fusing, and the application is complicated inmany cases. This is indeed an issue becausesuch complicated use of names and parametersleads to increased variation in practice and thepotential for error. As studies using protocolsfor sedation management and weaning trialshave demonstrated, decreasing practice varia-tion does improve outcomes.24,25,51 It is alsoclear that the more complex the protocol theharder it is to attain compliance.52,53 It is unlikelythat decreased variation related to the use ofthe current new complex pressure modes willbe easily accomplished. In the experience ofthis author, even the product user manuals aresomewhat difficult to navigate. The modes aresophisticated and often require numerousparameter adjustments (ASV is an exception).Some modes are activated using settings thathave names that are not descriptive of theactual mode but are necessary to activateselected characteristics of the mode (eg, PC-SIMV). This makes the education of clini-cians a challenge and is often hard to accom-plish in busy critical care units. Even moreconcerning is the reality that in many criticalcare units across the country, standardizationof ventilators does not occur; instead, a pot-pourri of ventilators exists in the units, whichmeans that clinicians must learn a wide varietyof modes. Anecdotally, clinicians report thatmany of the modes available on ventilatorstoday are not used; perhaps this is due to thelearning curve that may be quite steep.
Do we need these “better” modes to be socomplex? Is “better” really “better”? Muchlike respiratory waveforms and other digitaldisplays available on ventilators today, the newpressure modes potentially could be used toimprove the care we provide. Many are elegantand have been designed to correct problemsidentified by clinicians in the past (flowresponse time, etc). But, often they are under-stood by only a handful of clinicians; too often,the bedside nurse is the least informed andrelies on the understanding of the physician orrespiratory therapist. This is unfortunate andmuch like a pilot flying without a copilot; it is amistake waiting to happen. Until the modes are
AACN1904_399–411 22/10/08 11:34 PM Page 409

BURNS AACN Advanced Cri t ical Care
410
better understood and easier to apply by allclinicians who care for the patients, we maynot be doing our patients a service by usingthem. Simple may indeed be better.
As we consider the requirements necessaryto care for patients during a mass casualty ordisaster event, one of the major requirementsof ventilators and other equipment is that theyare easy to use by professionals with a mini-mum amount of training. Certainly, the auto-matic external defibrillator is an example ofone such technology that years ago wasunthinkable. From the perspective of thisauthor, clinicians should advocate for ventila-tor technology that is safe and user-friendlyand requires little clinician decision makingand interaction (basically adapts ventilation tothe requirements of the patient). The idea of“intelligent ventilation” as promoted withASV is indeed attractive and to be encouraged.
For clinicians like APNs who must orderthe modes, it is important that the approach tothe same be one that is logical and safe. Thefirst step is to decide on the goal of ventilation.If it is lung protection, then the science relatedto lung protection dictates that VT be con-trolled and that attention to lung recruitmentwith PEEP be ensured. The mode of ventila-tion to attain the goal should be one that thepractitioner understands so that the parame-ters are selected appropriately and the patientis monitored to ensure the attainment of thegoal. In weaning patients, spontaneous breath-ing trials are well tested and generally can beaccomplished with CPAP, T-piece, and/or PSV.These methods are readily understood andrequire little in the way of complicated param-eter setting. Understanding the availablemodes on specific ventilators in one’s worksetting is essential if we are to provide qualitysafe care.
SummaryMany new pressure modes exist on ventilatorstoday; however, little evidence exists as to theirefficacy or superiority. Until additional studiesare done testing the modes in a wide variety ofpatient populations and conditions, recom-mendations for the best use of the modes willbe difficult to make. Inherent issues related tothe modes continue to be the complexity of themodes and the profusion of names that makeunderstanding and application difficult. Whenall is said and done, simple and familiar mayindeed be better.
References
1. Orlando R. Ventilators: how clever, how complex? [edi-torial]. Crit Care Med. 2003:2704–2705.
2. MacIntyre NR. Effects of initial flow rate and breath ter-mination criteria on pressure support ventilation. Chest.1991;99:134–138.
3. Brochard L, Harf A, Lorino H, Lemaire F. Inspiratory pres-sure support prevents diaphragmatic fatigue duringweaning from mechanical ventilation. Am Rev RespirDis. 1989;139:513–521.
4. MacIntyre NR. Ventilatory muscles and mechanicalventilatory support. Crit Care Med. 1997;25:1106–1107.
5. O’Kroy JA, Coast JR. Effects of flow and resistive train-ing on respiratory muscle endurance and strength.Respiration. 1993;60:279–283.
6. Fiastro JF, Habib MP, Quan SF. Pressure support com-pensation for inspiratory work due to endotrachealtubes and demand continuous positive airway pressure.Chest. 1988;93:499–505.
7. Esteban A, Alia I, Ibanez J, Benito S, Tobin MJ. Modes ofmechanical ventilation and weaning a national survey ofSpanish hospital. Chest. 1994;106:1188–1193.
8. Vittacca M, Bianchi L, Zanotti E, et al. Assessment ofphysiologic variables and subjective comfort under dif-ferent levels of pressure support ventilation. Chest.2004;126:851–859.
9. Cole AGH, Weller SF, Sykes MK. Inverse ratio ventilationcompared with PEEP in adult respiratory failure. Inten-sive Care Med. 1984;10:227–232.
10. Gurevich MJ, Van Dyke J, Young ES, Jackson K.Improved oxygenation and lower peak airway pressurein severe adult respiratory distress syndrome: treat-ment with inverse ratio ventilation. Chest. 1986;89:211–213.
11. Tharratt RS, Allen RP, Albertson TE. Pressure controlledinverse ratio ventilation in severe adult respiratory fail-ure. Chest. 1988;94:755–762.
12. Abraham E, Yoshira G. Cardiorespiratory effects of pres-sure controlled ventilation in severe respiratory failure.Chest. 1990;98:1445–1449.
13. Amato MBP, Barbas CSV, Medeiros DM, et al. Effect of aprotective-ventilation strategy on mortality in the acuterespiratory distress syndrome. N Engl J Med. 1998;338:347–354.
14. Kacmarek RM, Hess D. Pressure-controlled inverse-ratioventilation: panacea or auto-PEEP? [editorial]. RespirCare. 1990;35:945–948.
15. The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared withtraditional tidal volumes for acute lung injury and theacute respiratory distress syndrome. N Engl J Med.2000;342:1301–1308.
16. Downs JB, Stock MC. Airway pressure release ventila-tion: a new concept of ventilatory support. Crit CareMed. 1987;15:459–461.
17. Stock MC, Downs JB, Frolicher DA. Airway pressurerelease ventilation. Crit Care Med. 1987;15:462–466.
18. Garner W, Downs JB, Stock MC, Rasanen J. Airwaypressure release ventilation (APRV): a human trial.Chest. 1988;94:779–781.
19. Habashi NM. Other approaches to open-lung ventila-tion: airway pressure release ventilation. Crit Care Med.2005;33:S228–S240.
20. Cane RD, Peruzzi WT, Shapiro BA. Airway pressurerelease ventilation in severe acute respiratory failure.Chest. 1991;100:460–463.
21. Putensen C, Zech S, Wrigge H, et al. Long term effects ofspontaneous breathing during ventilatory support inpatients with acute lung injury. Am Rev Respir Crit CareMed. 2001;164:43–49.
22. Frawley PM, Habashi NM. Airway pressure release ven-tilation and pediatrics: theory and practice. Crit CareNurs Clin N Am. 2004;16:337–348.
23. Kaplan LJ, Bailey H, Formosa V. Airway pressure releaseventilation increases cardiac performance in patients
AACN1904_399–411 22/10/08 11:34 PM Page 410

VOLUME 19 • NUMBER 4 • OCTOBER–DECEMBER 2008 PRESSURE MODES OF MECHANICAL VENTILATION
411
with acute lung injury/adult respiratory distress syn-drome. Crit Care. 2001;5:221–226.
24. Kollef MH, Shapiro SD, Silver, et al. A randomized, con-trolled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Crit CareMed. 1997;25:567–574.
25. Brook AD, Ahrens TS, Schaff R, et al. Effect of a nurs-ing-implemented sedation protocol on the duration ofmechanical ventilation. Crit Care Med. 1999;27:2609–2615.
26. Kress JP, Pohlman O’Connor MF, Hall JB. Daily interrup-tion of sedative infusions in critically ill patients under-going mechanical ventilation. N Engl J Med. 2000;342:1471–1477.
27. Schweickert WD, Gehlbach BK, Pohlman AS, Hall JB,Kress JP. Daily interruption of sedative infusions andcomplications of critical illness in mechanically venti-lated patients. Crit Care Med. 2004;32:1272–1276.
28. Puritan Bennett Product Web site. http://www.puritanbennett.com/prod/Product.aspx?S1�VEN&S2�&id/289. Accessed January 2, 2008.
29. Maquet Product Web site. http://www.maquet.com/ p r o d u c t P a g e . a s p x ? m 1 �1 1 2 5 9 9 7 7 4 4 9 5 & m 2�12808545902&m3�105584076919&productGroupID�112808545902&productConfigID�105584076919&languageID�1&titleCountryID�224. Accessed January2, 2008
30. Dräger Product Web site. http://www.draeger.com/MT/internet/pdf/CareAreas/CriticalCare/cc_bipap_book_en.pdf. Accessed January 2, 2008.
31. Hamilton Product Web site. http://www.med1online.com/documents/Hamilton_Products_Galileo_Classic_Specs.pdf. Accessed January 2, 2008
32. Viasys Healthcare Web site. http://www.viasyshealthcare.com/prod_serv/downloads/284_Avea_Comp_Spec_Sheet.pdf. Accessed January 2, 2008
33. Calzia E, Lindner KH, Witt S, et al. Pressure time productand work of breathing during biphasic continuous posi-tive airway pressure and assisted spontaneous breath-ing. Am J Respir Crit Care Med. 1994;150:904–910.
34. Staudinger T, Kordova H, Roggla M, et al. Comparison ofoxygen cost of breathing with pressure support ventila-tion and biphasic intermittent positive airway pressureventilation. Crit Care Med. 1998;26:1518–1522.
35. Rathgeber J, Schorn B, Falk V, Kazmaier S, Speigel T,Burchardi H. The influence of controlled mandatory ven-tilation (CMV), intermittent mandatory ventilation (IMV)and biphasic intermittent positive airway pressure(BIPAP) on duration of intubation and consumption ofanalgesics and sedatives. A prospective analysis in 596patients following adult cardiac surgery. Eur J Anaesthiol.1997;14:576–582.
36. Amato MBP, Barbas CSV, Bonassa J, Saldiva PHN, ZinWA, de Carvalho RR. Volume-assured pressure supportventilation (VAPSV): a new approach for reducing mus-cle workload during acute respiratory failure. Chest.1992;102:1225–1234.
37. Viasys Healthcare Web site. http://www.viasyshealthcare.com/about/about_viasys.aspx?config�ab_main.Accessed January 2, 2008
38. Puritan Bennett Product Web site. http://www.puritanbennett.com/prod/Product.aspx?S1�VEN&S2�SOF&id�292. Accessed January 2, 2008
39. Elsasser S, Guttmann J, Stocker R, Mols G, Prieve HJ,Haberthur C. Accuracy of automatic tube compensationin new-generation mechanical ventilators. Crit CareMed. 2003;31:2619–2626.
40. http://www.hamilton-medical.com/GALILEO-ventilators.37.0.html. Accessed January 2, 2008.
41. Sulzer CF, Chiolero R, Chassot PG, Mueller XM. Adap-tive support ventilation for fast tracheal extubationafter cardiac surgery: a randomized controlled study.Anesthesiology. 2001;95:1339–1345.
42. Tassaux D, Dalmas E, Gratadour P, Jolliet P. Patient-ventilaor interactions during partial ventilatory support:a preliminary study comparing the effects of adaptivesupport ventilation with synchronized intermittentmandatory ventilation plus inspiratory pressure sup-port. Crit Care Med. 2002;30:801–807.
43. http://www.draeger.com/MT/internet/pdf/CareAreas/CriticalCare/cc_evita_atcpps_br_en.pdf. Accessed January2, 2008
44. http://www.puritanbennett.com/educ/List.aspx?S1�QUI&S2�VEN Accessed January 2, 2008
45. Younes M. Proportional Assist Ventilation, Principlesand Practice of Mechanical Ventilation. New York, NY:McGraw-Hill; 1994.
46. Varelmann D, Wrigge H, Zinserling J, Muders T, HeringR, Putensen C. Proportional assist versus pressure sup-port ventilation in patients with acute respiratory failure:cardiorespiratory responses to artificially increased ven-tilatory demand. Crit Care Med. 2005;33:1968–1975.
47. Giannouli E, Webster K, Roberts D, Younes M. Responseof ventilator-dependent patients to different levels ofpressure support and proportional assist. Am J RespirCrit Care Med. 1999;159:1716–1725.
48. Mols G, von Ungern-Sternberg B, Rohr E, Haverthur C,Geiger K, Guttmann J. Respiratory comfort and breath-ing pattern during volume proportional assist ventila-tion and pressure support ventilation: a study onvolunteers with artificially reduced compliance. CritCare Med. 200;28:1940–1946.
49. Bosma K, Ferreyra G, Ambrogio C, et al. Patient-ventila-tor interaction and sleep in mechanically ventilatedpatients: pressure support versus proportional assistventilation. Crit Care Med. 2007;35:1048–1054.
50. Carlon GC, Combs AH. Mechanical ventilators and respira-tory centers [editorial]. Crit Care Med. 2000;28:2154–2156.
51. Ely EW, Baker AM, Dunagan DP, et al. Effect on the dura-tion of mechanical ventilation of identifying patientscapable of breathing spontaneously. N Engl J Med.1996;335:1964–1969.
52. Oeyen SG, Hoste EA, Roosens CD, Decruyenaere JM,Blot SI. Adherence to and efficacy and safety of aninsulin protocol in the critically ill: a prospective obser-vational study. Am J Crit Care. 2007;16:599–608.
53. Malesker MA, Foral PA, McPhillips AC, Christensen KJ,Chang JA, Hillerman DE. An efficiency evaluation of pro-tocols for tight glycemic control in intensive care units.Am J Crit Care. 2007;16:589–598.
AACN1904_399–411 22/10/08 11:34 PM Page 411
















![Dual controlled modes of mechanical ventilation [onarılmış]](https://img.pdfslide.us/doc/110x75/5871a5ac1a28abda6a8b471f/dual-controlled-modes-of-mechanical-ventilation-onarilmis.jpg)






