Embed Size (px)
Citation preview


Presenter Disclosure:
Maria van Harten has no potential for
conflict of interest with this presentation
Dr. Maria van Harten
Public Health Dentist
Dental Consultant
Oral Health
and
Lorde, Pen V, Varnish, and Taxes

Lorde
• 16yr old songstress from New Zealand
• Critical of mainstream culture & artists
• Songs referring to teeth:
– Royals
– Team
– White Teeth Teens

Obsession with teeth?
• Clean teeth, white teeth, jewels between
teeth, teeth cut on wedding rings
• Songs refer to class divides
• Oral health just like general health occurs on
a gradient – amplified by non-universal dental
care “system”

Canary in the coalmine
Through CASE MANAGEMENT
Individual FOR HEALTH ISSUES
– Diabetes, obesity, mental illness, substance
dependencies
Through SCHOOL-BASED SCREENING
Community FOR SOCIAL ISSUES
– Immigration, poverty, unemployment

Pen V
DRUGS OF CHOICE
Tooth Pain
– “Throbbing”: OTC ibuprofen max dosage NOT
acetominophen
– “Dull, achy”: OTC acetominophen
Tooth abscess and/or cellulitis PEN V
≤ 12yrs: 25-50mg/kg q6-8h for 7d, max 3g/d
>12yrs: 500mg q6h for 7d
Or Clindamycin 8-25mg/kg in 3-4 doses for 5d (≤ 12yrs), 300mg q12h for 7d (>12yrs)

Focus of infection
Drugs offer temporary relief
Treatment options:
– Fill tooth (restoration)
– Remove tooth (extract)
– Do nothing, endure pain, wait for tooth death;
repeated cellulitis, abscess, drainage
Focus of infection must be removed for resolution!

How did we get here?
– Dental disease is preventable!
– No such thing as “weak teeth” unless hypoplastic
conditions happen during tooth development

Caries prevention

Fluoride varnish

Fluoride varnish
• Applied at primary medical care visits can
reduce decay rates by one-third
• Controlled substance but not controlled act
• Especially for high-risk and generationally
low-income families
– Inexpensive preventive measure to curb future
high costs to publicly funded programs
– Lack of access to care is persistent challenge
Why can’t OHIP reimburse physicians?

Fluoride varnish in London & Middlesex County
• Private dental offices – Majority don’t see children <3yrs of age ? Too late
• Health Unit programs – School-screening begins in kindergarten ? Too late
– PrevOH program ? Can’t access without hardship
– Pilot project with HBHC program ? Voluntary
– Pilot project at high-risk schools ? Buy-in from schools
Why can’t OHIP reimburse physicians?

What does this have to do with taxes?
Canadian Centre for Policy Alternatives’ Putting our money where our mouth is: the future of dental care in Canada (2011).
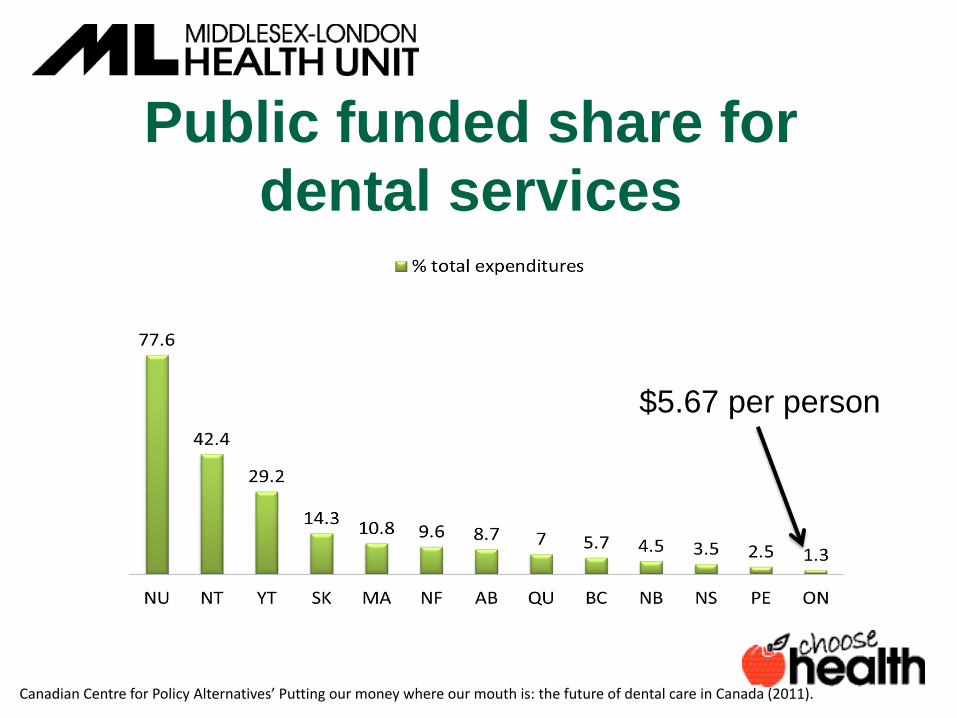
Public funded share for dental services
$5.67 per person
Canadian Centre for Policy Alternatives’ Putting our money where our mouth is: the future of dental care in Canada (2011).

IntelliHEALTH Ontario (2012).

Referring to Health Unit for dental
• Children & youth 17 years of age and younger who • Have no access to private insurance • Cannot afford dental care
• We may be able to offer no-cost coverage for care • We see eligible children at the 50 King Dental Clinic
for some services
• We see OW adults and parents of HSO children at the 50 King Dental Clinic for cleanings only

Publicly funded care
WHO HAS PUBLIC DENTAL COVERAGE • First Nations people with band card (NIHB) • OW adults (breadth depends on municipality) • OW child-dependents (emergency, preventive, treatment) • Ontario Disability Support Plan recipients • Children and youth whose parents declare financial
hardship • Children and youth whose parents prove AFNI is lower
than threshold income for Healthy Smiles Ontario
WHO DOES NOT HAVE PUBLIC DENTAL COVERAGE • Working adults and seniors • Non-resident low income children and youth
Aug2016

Thanks for your attention
Artwork by
Adriana van Harten