Embed Size (px)
Citation preview
Presented by:
Wendy Talbot, MPH, CHCA
January 16, 2008
Overview of 2007
Performance Measure Validation Findings and HEDIS Results

Presentation Overview
I. Performance Measure Validationa. Process
b. Findings and Recommendations
c. Questions
II. HEDIS Resultsa. Results and Recommendations by
Dimension of Care
b. 2008 HEDIS Changes
c. Questions

Performance Measure Validation
Objectives– Evaluate accuracy of
data collected– Determine the extent to
which each measure calculated followed established specifications
– Utilize process consistent with CMS protocol

• NCQA-licensed audit organization• Pre-on-site call/meeting• BAT review• AHCA-specific measure set validation• Source code/certified software review• Primary source review• Convenience sample validation (if applicable)• Medical Record Review• Health Plan Quality Indicator Data File Review
Validation Activities
Validation Activities Findings• Used a certified software vendor:
– 10 out of 12 HMOs
• Convenience sample validation: – 4 HMOs had a convenience sample– 3 HMOs were exempt– Was not specified in final audit report whether one
was required or performed for 5 HMOs
• Medical record review validation– 11 HMOs– 1 HMO did not use the hybrid method
• All other validation activities were fulfilled

Audit Findings• R = Report
– Reportable rate or numeric result for HEDIS measures
• NA = Not Applicable– The HMO followed the specifications but the
denominator was too small to report a valid rate (<30)
• NB = No Benefit– The HMO did not offer the health benefits required
by the measure
• NR = Not Report– The HMO calculated the measure but the rate was
materially biased or the HMO chose not to report the measure

Audit Findings• Breast Cancer Screening
– 42-51 Years• R = 10 HMOs• NA = 2 HMOs
– 52-69 Years• R = 10 HMOs• NA = 2 HMOs
– Combined• R = 10 HMOs• NA = 2 HMOs
• Timeliness of Prenatal Care• R = 11 HMOs• NR = 1 HMO
Audit Findings• Cervical Cancer Screening
• R = 12 HMOs
• Chlamydia Screening– 16-20 Years
• R = 11 HMOs• NA = 1 HMO
– 21-25 Years• R = 11 HMOs• NA = 1 HMO
– Combined• R = 12 HMOs

Audit Findings• Appropriate Medications for People with
Asthma– 5-9 Years
• R = 9 HMOs• NA = 3 HMOs
– 10-17 Years• R = 8 HMOs• NA = 4 HMOs
– 18-56 Years• R = 8 HMOs• NA = 4 HMOs
– Combined• R = 10 HMOs• NA = 2 HMOs

Audit Findings• Comprehensive Diabetes Care
– LDL-C Screening• R = 10 HMOs• NA = 2 HMOs
– LDL-C Testing• R = 10 HMOs• NA = 2 HMOs
– Eye Exams• R = 9 HMOs• NA = 2 HMOs• NR = 1 HMO
– Nephropathy• R = 10 HMOs• NA = 2 HMOs

Audit Findings• Controlling High Blood Pressure
– 18-45 Years• R = 7 HMOs• NA = 1 HMO• NR = 4 HMOs
– 46-85 Years• R = 7 HMOs• NA = 1 HMO• NR = 4 HMOs
– Combined• R = 7 HMOs• NA = 1 HMO• NR = 4 HMOs

IS Standards
• IS 1.0—Sound Coding Methods for Medical Data• IS 2.0—Data Capture, Transfer, & Entry—Medical Data• IS 3.0—Data Capture, Transfer, and Entry—Membership
Data• IS 4.0—Data Capture, Transfer, and Entry—Practitioner
Data• IS 5.0—Data Integration Required to Meet the Demands
of Accurate HEDIS Reporting• IS 6.0—Control Procedures that Support HEDIS
Reporting Integrity
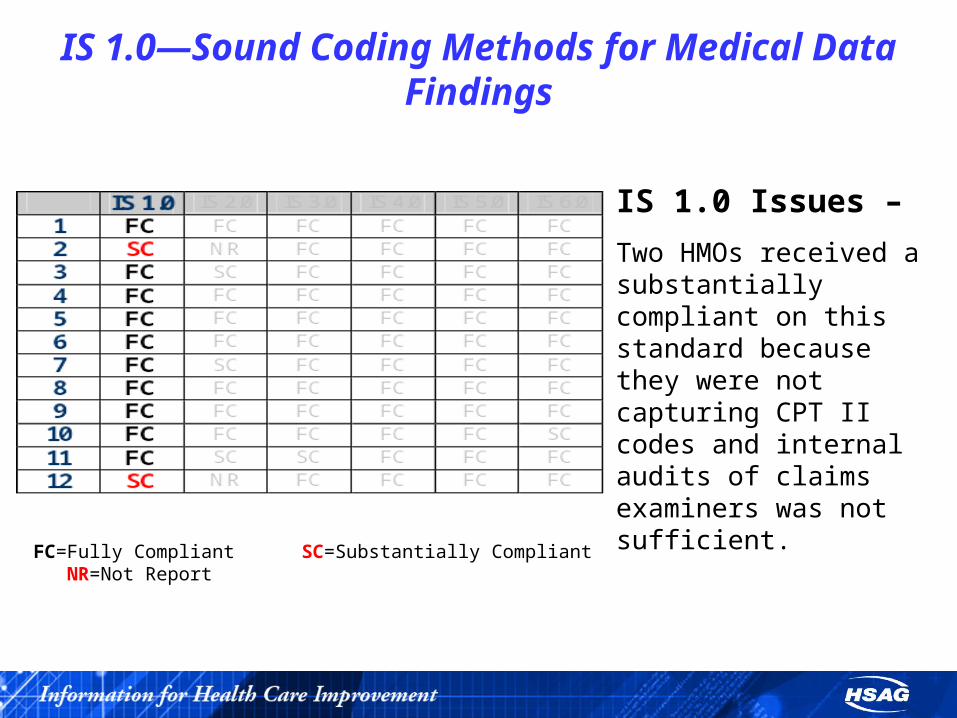
IS 1.0—Sound Coding Methods for Medical DataFindings
IS 1.0 Issues –
Two HMOs received a substantially compliant on this standard because they were not capturing CPT II codes and internal audits of claims examiners was not sufficient.
FC=Fully Compliant SC=Substantially Compliant NR=Not Report

IS 2.0—Data Capture, Transfer, & Entry—Medical Data
Findings
IS 2.0 Issues –
Three HMOs received a substantially compliant on this standard due to issues with data entry processes and data transmissions.
Two HMOs received a not report for this standard due to problems identified with their medical record process.
FC=Fully Compliant SC=Substantially Compliant NR=Not Report

IS 3.0—Data Capture, Transfer, and Entry—Membership Data
Findings
IS 3.0 Issues –
One HMO received a substantially compliant on this standard because there were no policies and procedures in place for receiving Medicaid enrollment files.
FC=Fully Compliant SC=Substantially Compliant NR=Not Report

IS 4.0—Data Capture, Transfer, and Entry—Practitioner Data
Findings
IS 4.0 Issues -
No issues, all HMOs were fully compliant with this standard.
FC=Fully Compliant SC=Substantially Compliant NR=Not Report

IS 5.0—Data Integration Required to Meet the Demands of Accurate HEDIS Reporting
Findings
IS 5.0 Issues -
No issues, all HMOs were fully compliant with this standard.
FC=Fully Compliant SC=Substantially Compliant NR=Not Report

IS 6.0—Control Procedures that Support HEDIS Reporting Integrity
Findings
IS 6.0 Issues –
One HMO received a substantially compliant on this standard because NCQA specifications were not followed for sample size production and over-sample
percentages.
FC=Fully Compliant SC=Substantially Compliant NR=Not Report

Recommendations—HMOs
• Monitor all vendors who are contracted to work with data; specifically medical record vendors
• Develop and implement policies and procedure for data entry validation, regardless of the amount of manual data entry performed
• Develop procedures to ensure all data files are consistent and accurate

Recommendations—AHCA• Require a predetermined file
layout for submitting data• Consider using the NCQA IDSS
data submission tool• Have HMOs submit Final Audit
reports and Audit Designation reports to AHCA as soon as they receive them to eliminate confusion in the reporting process
• Have auditors validate the actual data files being submitted to AHCA

QUESTIONS?

Florida Medicaid HEDIS 2007 Results

Dimensions of Care
• Women’s Care
• Living with Illness
AnalyticsComparative– Florida 2007 weighted average compared
to the national 2006 Medicaid 50th percentile
– Florida 2007 weighted averages compared to Florida 2006 weighted averages (when applicable)
Distribution– Range of MHP reported rates

Distribution Graphs
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Measure 1 Measure 2
Highest Plan Rate Weighted Average Lowest Plan Rate
Highest Rate
Lowest Rate
FL Weighted Average
HighOutlier
LowOutlier

Florida 2007 Results Compared to National Benchmarks
0
5
6
3
0
1
0
1
2
3
4
5
6
7
0 TO 10 10 TO 25 25 TO 50 50 TO 75 75 TO 90 90 TO 100
2006 National Medicaid Percentile Range
Nu
mb
er o
f W
eig
hte
d A
vera
ge
Rat
es

Women’s Care

Women’s Care• 2007 Measures
– Breast Cancer Screening• Ages 42-51 Years• Ages 52-69 Years• Combined
– Cervical Cancer Screening– Chlamydia Screening
• Ages 16-20 Years• Ages 21-25 Years• Combined
– Prenatal and Postpartum Care• Timeliness of Prenatal Care

Women’s Care
• In 2006, only Breast Cancer Screening and Chlamydia Screening were reported by the HMOs.
• Starting in 2007:– Breast Cancer Screening measure was
reported in three cohorts and the lower age limit was raised to 40 years of age
– The lower age limit for Cervical Cancer Screening was raised to 21 years of age

Women’s Care
Overall performance for the Women’s Care dimension continued to be below average to average.

Women’s Care• Breast Cancer Screening—Ages 52-69 Years
findings:– 10 HMOs reported a rate for this measure; two
HMOs were unable to report rates due to insufficient sample sizes
– Nine had rates below the national HEDIS 2006 50th percentile
– Four of the HMOs had rates below the low performance level (LPL)
– The 2007 Florida Medicaid weighted average decreased by 1 percentage point compared to the 2006 weighted average

Women’s Care
• Cervical Cancer Screening findings:– 12 HMOs reported a rate for this measure– All 12 HMOs’ rates were below the national
HEDIS 2006 50th percentile– 10 of the HMOs reported rates below the
LPL– The 2007 weighted average of 55.8
percent was below the LPL of 59.7 percent

Women’s Care
• Chlamydia Screening in Women—Combined findings:– 12 HMOs reported a rate for this measure– Four HMOs reported rates above the
national HEDIS 2006 50th percentile– Two HMOs reported rates below the LPL– The 2007 weighted average was 1.5
percentage points below the 2006 weighted average

Women’s Care
• Timeliness to Prenatal Care findings:– 11 HMOs reported a rate for this measure;
one HMO reported an NR for the measure– All 11 of the HMOs reported rates below
the LPL– The 2007 weighted average of 63.4
percent was below the LPL of 74.2 percent

Women’s CareRange of 2007 Rates
0%
10%
20%
30%
40%
50%
60%
70%
80%
Breast CancerScreening, 42-51
Years
Breast CancerScreening, 52-69
Years
Breast CancerScreening,Combined
Cervical CancerScreening
ChlamydiaScreening, 16-20
Years
ChlamydiaScreening, 21-25
Years
ChlamydiaScreening,Combined
Timeliness ofPrenatal Care
Highest Plan Rate FL Weighted Average Lowest Plan Rate

Women’s Care
• Improvement efforts to be considered for the Breast Cancer Screening measure include:– Increase efforts to target younger women
for mammograms– Educate on the importance of early
detection– Work to ensure complete administrative
data

Women’s Care
• Improvement efforts to consider for the Cervical Cancer Screening and Chlamydia Screening measures include:– Educate women on the importance of
screening– Identify barriers to accessing care and
services
Women’s Care
• Improvement efforts to consider for the Timeliness to Prenatal Care measure include:– Ensure complete data through the use of
medical record review, especially for plans that utilize global billing for maternity services
– Educate on the importance of prenatal care
Women’s Care
• Missed opportunities could be examined to identify barriers to improvement and target specific interventions
• High performing HMOs should share best practices with other HMOs

Living with Illness

Living with Illness• 2007 Measures:
– Use of Appropriate Medications for People with Asthma
• Ages 5-9 Years• Ages 10-17 Years• Ages 18-56 Years• Combined
– Comprehensive Diabetes Care• LDL-C Screening• LDL-C Controlled• Eye Exams• Medical Attention for Diabetic Nephropathy
– Controlling High Blood Pressure• Ages 18-52 Years• Ages 46-85 Years• Combined

Living with Illness
• In 2006, only Use of Appropriate Medications of People with Asthma was reported by the HMOs
• Starting in 2007:– Controlling High Blood Pressure measure
was reported in three cohorts and the lower age limit was decreased to 18 years of age
– There were changes to several indicators in the Comprehensive Diabetes Care measure

Living with Illness
The overall statewide results in the Living With Illness dimension were average to below average, with the exception of Comprehensive Diabetes Care—Medical Attention for Diabetic Nephropathy, which was above average.

• Appropriate Use of Medications for People with Asthma—Combined findings:– Nine HMOs reported a rate for this
measure; three HMOs had an insufficient sample size to report the measure
– Four HMOs reported rates above the national HEDIS 2006 50th percentile
– One HMO reported a rate below the LPL
Living with Illness

Living with Illness
• Comprehensive Diabetes Care findings:– LDL-C Screening
• No HMOs reported rates above the national HEDIS 50th percentile
• Eight of the 10 HMOs reported a rate below the LPL
– LDL-C Testing• One HMO reported a rate above the national
HEDIS 50th percentile• Two of the 10 HMOs reported a rate below the
LPL

Living with Illness
• Comprehensive Diabetes Care findings continued:– Eye Exams
• No HMOs reported a rate above the national HEDIS 50th percentile
• Two if the nine HMOs reported a rate below the LPL
– Medical Attention for Diabetic Nephropathy• Eight of the 10 HMOs reported a rate above the
HPL• One HMO reported a rate below the LPL

Living with Illness
• Controlling High Blood Pressure—Ages 46-85 Years findings:– Seven HMOs reported a rate for this
measure; one had an insufficient sample size to report the measure, and four reported an NR
– None of the HMOs reported a rate above the LPL

Living with IllnessRange of 2007 Rates
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Diabetes Care-Eye Exam Diabetes Care-LDL Screening Diabetes Care-LDL level <100 Diabetes Care-Nephropathy
Highest Plan Rate FL Weighted Average Lowest Plan Rate

Living with IllnessRange of 2007 Rates, cont.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Asthma, 5-9Years
Asthma, 10-17Years
Asthma, 18-56Years
Asthma,Combined Rate
Controlling HighBlood Pressure,
16-45 Years
Controlling HighBlood Pressure,
46-85 Years
Controlling HighBlood Pressure,
Combined
Highest Plan Rate FL Weighted Average Lowest Plan Rate

Living with Illness
• Improvement efforts to consider for Appropriate Medications for People with Asthma include:– Ensure pharmacy data are complete– Educate providers on the guidelines of
asthma treatment

Living with Illness
• Improvement efforts to consider for Comprehensive Diabetes Care include:– Educate members on the importance of
diabetes management care– Ensure vendor data, such as lab and
pharmacy, are complete– Work to improve administrative data to
minimize the burden of medical record review

Living with Illness
• Improvement efforts to consider for Controlling High Blood Pressure include:– Changes were made to the 2007 technical
specifications, HMOs should ensure all changes were implemented
– Monitor medical record review processes to ensure the measure is being captured according to specifications

Living with Illness
• Missed opportunities could be examined to identify barriers to improvement and target specific interventions
• High performing HMOs should share best practices with other HMOs

Changes to HEDIS 2008

Summary of Changes in HEDIS 2008
• New HEDIS measures
• Changes to existing measures
• Retired measures

HEDIS 2008 New Measures
• Lead Screening in Children (LSC)
• Pharmacotherapy Management of COPD Exacerbation (PCE)
• RRU – Cardiovascular Conditions (RCA)
• RRU – Uncomplicated Hypertension (RHY)
• RRU – COPD (RCO)

Changes to Existing Measures
• Childhood Immunization Status (CIS) – clarified numerator evidence for antigen compliance
• Persistence of Beta-Blocker Treatment After A Heart Attack (PBH) – decreased lower age limit to 18 years of age

Changes to Existing Measures, cont’d
• Avoidance of Antibiotic Treatment in Adults with Acute Bronchitis (AAB) – Inverted the measure rate so that a higher rate is better, and renamed the measure formerly called Inappropriate Antibiotic Treatment for Adults with Acute Bronchitis
• Use of High-Risk Medications in the Elderly (DAE) – renamed measure that was formally called Drugs to be Avoided in the Elderly

Retired Measures
• Adolescent Immunization Status
• Beta-Blocker Treatment After a Heart Attack
• Discharges and ALOS – Maternity
• Births and ALOS – Newborns
• Mental Health Utilization – Inpatient Discharges and ALOS
• Chemical Dependency Utilization – Inpatient Discharges and ALOS

Questions?

2007-2008 Focused Study
Behavioral Health Prior Authorizations
Peggy Ketterer, RN, BSN, CHCAExecutive Director, State and Corporate Services
Marilea Rose, RN, BAAssociate Director, State and Corporate Services
The purpose of the study is to determine:
• How behavioral health authorization processes vary between MCOs
• How medical necessity criterion vary between MCOs
• How timeliness of authorizations vary across MCOs

Who will participate in the study?
•HMOs
•PSNs
•PMHPs

Focused Study Activity
Step 1: Procure behavioral health information from MCOs
• 25 out of 26 MCOs have submitted behavioral health documents
• HSAG has completed a cursory review and in process of requesting additional information from MCOs

Focused Study Activity
Step 2: Conduct desk review
• HSAG is currently compiling and categorizing MCO survey responses
• HSAG conducted informal interviews with a limited number of providers to gather preliminary information regarding potential barriers

Focused Study Activity
Step 3: Evaluate self-reported timeliness of authorization
• Data submission file layout for timeliness data is being designed
• HSAG is preparing MCO data request letter
• HSAG is finalizing MCO instructions for calculating timeliness indicators

Focused Study Activity
Step 3: Evaluate self-reported timeliness of authorization (cont’d)
Key Dates:
• Data request letters will be sent to the MCOs on 1/31/08
• Timeliness data is due back to HSAG on 3/7/08

Focused Study Activity
Step 4: Report Preparation
• Report outline is being drafted
• HSAG will present findings, summary of common practices
• HSAG will provide recommendations for improvement of the process, consider standardization

Questions and Answers

Upcoming EQR ActivitiesContract Year Two
2:45 p.m. – 3:30 p.m.
Peggy Ketterer, RN, BSN, CHCAExecutive Director, EQRO Services

Upcoming EQR activities
MARK YOUR CALENDARS!!!!The next EQR Quarterly Meetings
are scheduled as follows:Wednesday, March 26, 2008 (Webinar)
Wednesday, June 18, 2008 (AHCA Offices)
Wednesday, September 24, 2008 (Webinar)

Performance Improvement Projects (PIPs)
• PIP validation process is targeted for completion in March, 2008.
• MCOs will be given the opportunity to review HSAG’s completed PIP tool and summary grid and provide feedback and comments.

Performance Improvement Projects (PIPs)
• Collaborative PIPs – HMOs/PSNs• The well-child visits collaborative PIP is on
two separate tracks: reform and non-reform plans. Non-reform plans have collected baseline data and are completing the causal/barrier analysis and intervention planning phase. Reform plans will be collecting baseline data (HEDIS® 2008), available June, 2008.
HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA)

Performance Improvement Projects (PIPs)
• Collaborative PIPs – PMHPs• Topic: Follow-up Within 7 Days After an
Acute Care Discharge for a Mental Health Diagnosis.
• PMHPs will be collecting baseline data on calendar year 2007, which will be available in June, 2008.
Performance Improvement Projects (PIPs)
• Collaborative PIPs – NHDPs• Topic: Retention Rate• NHDPs will begin collecting baseline data
quarterly and will prepare a 2008 calendar year roll-up rate.

Performance Measures
Non-reform HMOs:
• Validation of Performance Measures Report is targeted to be finalized in January, 2008.
• HEDIS 2007 Strategic Analysis Report will be provided to AHCA as a draft in January, 2008. The report is targeted to be finalized in March, 2008.

Performance Measures
Reform HMOs/PSNs:
• HEDIS 2008 data will be analyzed and reported on during the next contract year (2008-2009).

Performance Measures
PMHPs:
• PMHPs will be collecting and reporting performance measure data on calendar year 2007 to AHCA in July, 2008.
• HSAG will conduct the validation of performance measures activities concurrently during the data collection and reporting cycle.

Performance Measures
NHDPs:
• NHDPs have begun to collect performance measure data quarterly (Jan – Mar 2008).
• HSAG will conduct the validation of performance measures activity in the early part of the next contract year (2008-2009).

Focused StudyBehavioral Health Authorizations
• HMOs, PSNs, and PMHPs have completed the MCO survey document describing their authorization processes.
• HSAG will forward a request for timeliness data to the participating MCOs on January 31, 2008. Timeliness data should be submitted to HSAG by March 7, 2008.
• Draft focused study report is targeted for submission to AHCA in May, 2008.

Upcoming EQR activities
•Quarterly EQR meetings (webinar and onsite at AHCA offices in Tallahassee)
•Other meetings (including Collaborative PIP meetings and technical assistance sessions) will be scheduled in conjunction with the quarterly meetings

QUESTIONS???
THANK YOU FOR YOUR PARTICIPATION!