Embed Size (px)
Citation preview

Presented by Nike Neuvenheim, MPA
Sr. Program Coordinator, Disease Control and Prevention Program
April 10, 2018: Presentation to Washington County Public Health Advisory Council


Vaccines are among the most cost-effective clinical preventive services and are a core component of any preventive services package.
Childhood immunization programs provide a very high return on investment.
For example, for each birth cohort vaccinated with the routine immunization schedule (this includes DTap, Td, Hib, Polio, MMR, Hep B, and varicella vaccines), society:
• Saves 33,000 lives• Prevents 14 million cases of disease• Reduces direct health care costs by $9.9 billion• Saves $33.4 billion in indirect costs

Despite progress, approximately 42,000 adults and 300 children in the United States die each year from vaccine-preventable diseases.*
Communities with pockets of unvaccinated and under vaccinated populations are at increased risk for outbreaks of vaccine-preventable diseases.
In 2008, imported measles resulted in 140 reported cases—nearly a 3-fold increase over the previous year. The emergence of new or replacement strains of vaccine-preventable disease can result in a significant increase in serious illnesses and death.
*This includes influenza, but does not include deaths due to 2009 H1N1.
Source: Office of Disease Promotion and Health Prevention, Healthy People 2020

MMR: 2016-2017 MMR: 2015-2016
Source: Centers for Disease Control and Prevention

Source: Centers for Disease Control and Prevention
2015-2016:


Various surveys founds high exemption clusters associated with some of the
following:
• Both high and lower socioeconomic status clusters – survey results were
contradictory.
• Lifestyle categorized as “alternative living”, which includes veganism or
vegetarianism, organic gardening, and use of natural healing remedies.
• Sociodemographic composition of the school and surrounding community
also predicted exemption rates. Higher exemption rates were associated
with higher proportion of Whites, higher percentage of college
graduates, higher median household income, and lower percentage of
families in poverty at the census tract, zip code, or school district level.

• More exemptions in rural than in urban school districts, and exemption
rates were higher, and increased faster, among private than public
schools.
• Perceptions of information provision and sufficiency were correlated
with exemption preferences. Parents who did not believe that they had
enough immunization information were more likely to believe that states
should grant exemptions on the basis of religious and personal beliefs and
that parents should be allowed to obtain exemptions for their child even if
it raised the risk of disease for everyone else. However, evidence was
inconsistent regarding access to information.
Source: American Public Health Association: Nonmedical Exemptions from School Immunization Requirements: A Systematic Review. November 2014


OAR 333-050-0020, Purpose and Intent
(1) The purpose of these rules is to implement Oregon
Revised Statutes (ORS) 433.235 through 433.284, which
require evidence of immunization, a medical or nonmedical
exemption, or immunity documentation for each child as a
condition of attendance in any school or facility, and which
require exclusion from school or facility attendance until such
requirements are met.

2222----17 months 17 months 17 months 17 months entering Child entering Child entering Child entering Child Care or Early Care or Early Care or Early Care or Early
Education Education Education Education
18 months or 18 months or 18 months or 18 months or older entering older entering older entering older entering
Preschool.Preschool.Preschool.Preschool. Child Child Child Child Care, or Head Care, or Head Care, or Head Care, or Head
Start Start Start Start Kindergarten or Kindergarten or Kindergarten or Kindergarten or
Grades 1Grades 1Grades 1Grades 1----6666 GradesGradesGradesGrades 7777----9999 Grades 10Grades 10Grades 10Grades 10----12 12 12 12
Check with healthcare provider or school/facility 4 DTAP 5 DTAP 5 DTAP/1 Tdap 5 DTAP/1Tdap
3 Polio 4 Polio 4 Polio 4 Polio
1 Varicella 1 Varicella 1 Varicella 1 Varicella
1 MMR 2 MMR 2 MMR 2 MMR
3 Hepatitis B 3 Hepatitis B 3 Hepatitis B 3 Hepatitis B
2 Hepatitis A 2 Hepatitis A 2 Hepatitis A --
3 or 4 Hib -- -- --
DTAP: DTAP: DTAP: DTAP: DiptheriaDiptheriaDiptheriaDiptheria////TetnusTetnusTetnusTetnus/Pertussis/Pertussis/Pertussis/PertussisMMR: MMR: MMR: MMR: MeaselsMeaselsMeaselsMeasels, Mumps and Rubella, Mumps and Rubella, Mumps and Rubella, Mumps and Rubella

Within 30 days
of the start of
school share
immunization
rates
January 17,
2018: Primary
Review
Summary
(PRS) forms 1
& 2 are due to
the County
February 7,
2018:
Exclusion
orders are
mailed to
parents and
schools by
County
February 21,
2018:
Exclusion Day
March 5,
2018: Primary
Review
Summary
(PRS) forms
updated page
2, 3 and 4 due
to the County
March 23,
2018: Share
immunization
rates
“Primary Review Summary” : a form provided or approved by Primary Review Summary” : a form provided or approved by Primary Review Summary” : a form provided or approved by Primary Review Summary” : a form provided or approved by the Public Health Division to school and facilities for enclosure the Public Health Division to school and facilities for enclosure the Public Health Division to school and facilities for enclosure the Public Health Division to school and facilities for enclosure with records forwarded to the local health department for with records forwarded to the local health department for with records forwarded to the local health department for with records forwarded to the local health department for secondary review and follow up. OAR 333secondary review and follow up. OAR 333secondary review and follow up. OAR 333secondary review and follow up. OAR 333----050050050050----0010001000100010

508 Washington County Sites
(children’s facilities and schools)
Total Enrollment: 113,967
Children Not Counted: 3,501
(spend a majority of their time at another site)
Adjusted Enrollment: 110,466
(total enrollment minus children not counted)
Medical Exemptions: 207
Nonmedical Exemptions: 3,485
Source: Immunization Record Information System (IRIS)

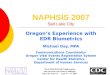
Total Issued 2017-2018
Totaled Issued 2016-2017
Students Excluded 2017-
2018
2858
3825
433
289 351
44
Washington County Exclusion Orders Issued
and Students Excluded
Incomplete/Insufficient No Record
Source: Immunization Record Information System (IRIS)
Decrease in Orders Issued Between
2016/2017 and 2017/2018
Incomplete/Insufficient: 25% decrease
No record: 17% decrease

AdjustedAdjustedAdjustedAdjustedEnrollEnrollEnrollEnroll NMENMENMENME % % % % D/T/PD/T/PD/T/PD/T/P %%%% MeaslesMeaslesMeaslesMeasles %%%% HepHepHepHep AAAA %%%% AllAllAllAll %%%%
Kindergarten 7,021 385 5.5% 225 3.2% 285 4.1% 255 3.6% 144 2.1%
7th Grade 7,325 205 2.8% 170 2.3% 122 1.7% 134 1.8% 71 1.0
Children’s Facilities 12,546 641 5.1% 331 2.6% 424 3.4% 460 3.7% 240 1.9%
Full School (K-12) 94,338 3,104 3.3% 2,052 2.2% 2,149 2.3% 1,840 2.5% 1,213 1.3%
Source: Immunization Record Information System (IRIS)

Why Share?
Senate Bill 895, passed in 2015, requires schools and child care facilities to have their immunization and exemption rates available at their main offices, on their websites, and for parents on paper
or electronic format.
When to Share?
30 days after the start of school AND 30 days after Exclusion Day
The online sharing of local-level data with the public contributes to transparency in public health by placing information about the risk
for vaccine preventable diseases in the hands of parents and communities.


� In collaboration with the Oregon Health Authority - Oregon
Immunization Program, promote AFIX (Assessment,
Feedback, Incentives and eXchange) a quality improvement
program supporting Vaccine for Children providers.
� Use local-level vaccination data to identify clusters of low
vaccination coverage, and develop and implement an
effective outreach program.
� Increase public health messaging focused on adherence to
recommended immunization schedule targeted towards
prenatal period and throughout infancy.

� Strengthen collaborative partnerships with Washington
County School Districts, School-Based Health Care
Centers, and safety net clinics.
� Reduce school exclusion orders and nonmedical
exemptions through an increased presence at back to
school events and through a targeted media campaign.

As Washington County Public Health (WCPH) continues
to address nonmedical exemptions prevalence and
trends in Washington County what combination of
targeted approaches would have the greatest impact?

As WCPH strengthens and develops partnerships at the
state and local-level among policy makers, educational
institutions and childcare facilities, non-profit
organizations and the public – what partnerships do you
believe would enable us to have the greatest impact on
vaccine hesitancy and adherence to the recommended
immunization schedules?

Using a health equity lens, are there specific
disenfranchised groups WCPH should work closely with
or organizations we should partner with that are closely
associated with these groups?










![Valve terminal MPA-S - Festo USA · Pneumatic components description Valveterminalwith MPA-Spneumatics Type: MPA-FB MPA-CPI MPA-MPM-…and MPA-ASI-… 534241 1309f [8028624] Valve](https://img.pdfslide.us/doc/110x75/5c5bd85409d3f236368c6efe/valve-terminal-mpa-s-festo-usa-pneumatic-components-description-valveterminalwith.jpg)