Embed Size (px)
Citation preview

Presented by: Jean Yoo-Campbell, Matthew Konerman, Monica Konerman, Jean Yoo Campbell, Christian Gocke, Eunpi Cho
Donald Lynch
Faculty Advisor: Dr. Fred Brancati
Bass N.M., et. al. N Engl J Med 2010; 362:1071-1081

Study Outline
Hypothesis: Rifaximin can prevent episodes of acute hepatic encephalopathy
Study Design: Randomized Control Trial (double-blind, placebo-controlled)
Setting: Multi-center in US, Canada, Russia Participants: 299 patients in remission from
recurrent hepatic encephalopathy secondary to chronic liver disease Inclusion: Age >18, >2 eps of HE in previous 6 months,
remission at enrollement, MELD <25 Exclusion: liver transplant expected w/in 1 month, GI
bleed, TIPSS, Cr >2.0, Hg <8, electrolyte abnormality, infection, active SBP, respiratory insufficiency

Study Outline Data Collection: Conn score & Asterixis grade
during clinic visits and phone interviews Conn: 1 = trivial lack of awareness, 2 = lethargy or apathy,
3 = somnolence to semistupor, 4 = coma Asterixis grade: 0 = no tremor, 1 = few flaps, 2 = occasional
flap, 3 = frequent flaps, 4 = continuous flaps Data Analysis: Efficacy data through intention-to-
treat; Kaplan-Meier, Cox proportional-hazards Outcome: time to breakthrough HE episode, time
to HE hospitalization, safety

Background• Hepatic encephalopathy is a complication of hepatic
cirrhosis • HE based on clinical diagnosis of 1) impaired mental
status (def by Conn score) and 2) impaired neuromotor function (hyperreflexia, rigidity, myoclonus and asterixis)
• Current standard of care is treatment with lactulose, nonabsorbable disaccharides (Sharma et al demonstrated lactulose effective in preventing HE compared to placebo)
Sharma BC, Sharma P, Agrawal A, Sarin SK. Secondary prophylaxis of hepatic encephalopathy: an open-label randomized controlled trial of lactulose versus placebo. Gastroenterology 2009;137:885-91, 91 e1.

Rifaximin• Also reduces ammonia by decreasing the ammonia-
producing enteric bacteria w/o toxicity other Abx• Min absorbed in gut, broad spectrum• H/o randomized studies that demonstrated rifaximin
was more effective than nonabsorbable disaccharides and equal or better than other Abx for treatment of HE
• Unknown efficacy for prevention of HE (until now…)

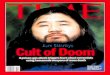
ResultsOver a 6-month period, patients treated
with rifaximin (550mg bid) maintained remission from hepatic encephalopathy more effectively than placebo.
Patients in the rifaximin group also had longer time to HE related hospitalization.


Subgroup Analysis
Bass NM et al. N Engl J Med 2010;362:1071-1081

Adverse Events, According to Study Group
Bass NM et al. N Engl J Med 2010;362:1071-1081

Conclusions/Implications First RCT addressing prevention with rifaximin Rifaximin is effective in preventing first breakthrough
episode of HE Patients already on lactulose 50% relative risk reduction
Similar safety profiles Reduce cost, frequency of hospitalizations
Seen in retrospective chart reviews already Small number needed to treat

Rifaximin in Hepatic Encephalopathy: Strengths Randomized, double-blind, placebo-controlled trial is the gold
standard for evaluating a drug (protects against many potential biases)
Kaplan-Meier Time-to-Event analysis most appropriate for this data set
Included more concrete secondary endpoint of “hospitalizations involving hepatic encephalopathy”
Included comparison of adverse effects between groups, demonstrating that Rifaximin may be better tolerated than antibiotics used previously for hepatic encephalopathy

Rifaximin in Hepatic Encephalopathy: Weaknesses Soft Primary Outcome Measure: Episodes of Hepatic Encephalopathy
Conn score and asterixis grade are subjective measures Study not powered to assess impact on mortality
Concomitant use of lactulose not well characterized Mean doses similar between groups but titration of doses unclear
True placebo not used in this study --- proper interpretation is that rifaximin + lactulose is more effective at preventing HE than only lactulose
Inclusion/Exclusion criteria limits generalizability of results Excluded patients with recent GI bleed, chronic renal insufficiency, anemia, etc.
Involvement of Salix Pharmaceuticals does encourage more investigation into study’s methods (i.e., how was randomization performed?, etc.)

Discussion Points Can we generalize this to our patients?
Sicker patients/higher MELD less exclusions like “intercurrent infection”
How long do you stay on rifaximin? Does it continue to prevent HE after a few months or do
you get gut resistance? What about frequency of HE while still on rifaximin (ie,
are you protected similarly for 2nd, 3rd episodes?) Can rifaximin be used alone to prevent HE?
Compare lactulose to rifaximin in preventing over long periods