Embed Size (px)
Citation preview

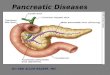
CT & MRI imaging Of
sellar ¶sellar lesions

The sella turcica is a central cup depression within the sphenoid bone. The bony sella , AP diameter is 15 mm and the Depth is 13 mm. The sellar content is pituitary gland, stalk and CSF.

CT technique, axial and coronal images with 2 mm space and thickness is from 1.5 to 3 mm, FOV is 16 cm. Contrast enhancement is mandatory.

MR technique include, sagittal T1WI, Axial T1, T2WI, Coronal T1 and T2WI The slice thickness is 1-3 mm and the interval is 0.5-1 mm or no gap interval. The FOV is 16-20 cm.

Anatomic approach for differential diagnosis.In order to analyze a sellar or parasellar mass on MRI we use the following anatomic approach: First identify the pituitary gland and sella turcica. Then determine the epicenter of the lesion and whether it is in the sella or above, below or lateral to the sella. If it is in the sella, determine whether or not the sella is enlarged. Once the location of the mass is clear, analyze the signal intensity patterns: is the lesion cystic or solid? Does it contain any abnormal vessels? Are there any calcifications? And so on. Finally establish a Differential Diagnosis.

Pituitary gland On a coronal section through the brain the reference structure is the pituitary gland which lies in the sella turcica.
It is usually larger in females than in males - in females the superior border tends to be convex, whereas in males it is usually concave. The most common abnormalities that arise in the pituitary gland are pituitary adenoma, cyst, Rathke's cleft cyst and craniopharyngioma.

Pituitary stalk The next structure to identify is the pituitary stalk. This is a vertically oriented structure which connects the pituitary gland to the brain. It is thinner at the bottom and thicker at the top. Embryologically, it is also derived from Rathke's cleft epithelium and therefore the pathologies, which can arise in the pituitary gland can also arise in the stalk. There are a few unusual things to be considered in children, such as germinomas and eosinophilic granulomas. In adults metastases and occasionally lymphoma can arise in the pituitary stalk.

Optic chiasm Another major structure in the suprasellar cistern is the optic chiasm.
It is an extension of the brain and looks like the number 8 lying on its side. It is glial tissue - therefore the most common tumors to originate here are glioma.
In the US and Europe another frequent pathology in this region is demylinating disease - particularly multiple sclerosis. This can also be associated with some swelling of the optic chiasm.

Hypothalamus Further cephalad lies the base of the brain, which at this location is the hypothalamus. Anatomically the hypothalamus forms the lateral walls and floor of the third ventricle. The most common pathologies to arise here are gliomas - in children hamartomas, germinomas and eosinophilic granuloma.

Carotid artery A very important structure in this area is the internal carotid artery. It runs a complex anatomic course as it passes through the skull base shaped like an S on lateral views. It passes through the cavernous sinus. The segment cranial to this is known as the supracavernous segment. This bifurcates into the anterior cerebral artery, which passes cranially to the optic chiasm, and the middle cerebral artery, which runs laterally. Aneurysms and ectasias are pathologies that can arise here. One must also be aware of congenital variations in the course of the internal carotid Sometimes it is very medially positioned and can actually lie in the midline.

Cavernous sinus The cavernous sinus is a paired complex of venous channels. In the lateral wall of the sinus run nerve III (oculomotorius), IV (trochlearis), V1 and V2 (trigeminus). The sixth cranial nerve (abducens) runs more medially and is located caudal to the carotid artery. The most common pathologies occurring in the cavernous sinus include schwannomas arising from the cranial nerves and inflammation, which can lead to thrombosis. This is known as cavernous sinus thrombophlebitis. Carotid-cavernous fistulas are fistulous communications between the carotid artery and the veins of the cavernous sinus.

Meninges The meninges cover the cavernous sinus. They are thicker laterally and superiorly than medially and inferiorly. The most common tumor to arise from the meninges is of course the meningioma. Dural metastasis is the second most common tumor to arise here. Also inflammatory pathologies occur in the basal meninges - the most common infection being tuberculous meningitis. Of the non-infectious inflammatory pathologies sarcoidosis is the commonest.

Sphenoid sinus Inferior to the pituitary gland lies the sphenoid sinus. This structure contains air and is lined by mucosa and bone.Posterior to the sphenoid sinus lies the clivus (not shown on this coronal section through the brain). Pathology that arises in this area includes carcinomas arising from the mucosa of the sphenoid sinus - squamous cell carcinoma and adenoid cystic carcinoma are the most common. Chordomas arise in the clivus and chondrosarcomas and osteosarcomas also occur in this area.Metastases can occur anywhere. Bacterial or fungal inflammatory processes in the sphenoid sinus can spread Intracranially via the cavernous sinus.

Normal pituitary gland (coronal and sagittal scans). Maximum normal height of the gland is Elster,s rule of 6,8,10 and 12. 6mm for infant and childhood, 8mm for men and postmenapausal women, 10 mm for women in childbearing age and 12 mm for women
in late pregnancy and post-partum women

Non enhanced sagittal MRI study can differentiate between the anterior and posterior portion of the gland by the signal characteristic.


Empty sella shows infundibulum(Arrow head), and the pituitary gland(Arrow), ICA(internal carotid artery), OC(optic chiasm).

Multislices enhanced CT Scan of the empty sella at coronal and sagittal images.Empty sella considered as a normal variant.

Intra-sellar arachnoidal cyst resulting in an “empty-sella” (coronal and sagittal imaging). No displacement of the stalk.

Pituitary micro and macroadenoma.
• The pituitary adenomas is by far the most common lesions, accounting for approximately one third to one half of the sellar and juxtasellar masses.
• The microadenoma is less than 10 mm and the macroadenoma is more than 10 mm.
• Pathologic study indicate microadenomas are 400 times more common than macroadenoma. Microadenoma at autopsy is
8-27%.• Macroadenoma: Imaging based studies report macroadenoma are twice
as frequent as microadenoma.

After the bolus injection of Gadolinium (Gadopentetate dimeglumine or Magnevist), 10 sets of images each consisting of three anatomic sections through the pituitary gland were acquired using T1 weighted Turbo Spin Echo sequence of 3 mm slice thickness with no intersection gap. This technique yields an imaging time 16 seconds per set and a total time of 2 minutes 40 seconds.The enhancement first occurs in the pituitary stalk, then in the pituitary tuft (the junction point of the stalk and the gland) and finally there is centrifugal opacification of the entire anterior lobe. Within 30-60 seconds, the entire gland shows homogeneous enhancement. The maximum image contrast between the normal pituitary tissue and microadenomas is attained about 30-60 seconds after the bolus. Most microadenomas appear as relatively non-enhancing (dark) lesions within an intensely enhancing pituitary gland. The peak enhancement of the pituitary adenomas occurs at 60-200 seconds, usually after the marked enhancement of the normal pituitary gland and persists for a longer duration. Delayed scan 30-60 minutes after contrast administration may demonstrate a reversal of the image contrast obtained at 30-60 seconds on dynamic scanning. This is because the contrast from the normal pituitary gland fades but diffuses into the microadenomas which stands out as a hyperintense focus. The addition of multiple sequences taken of the pituitary region gives an excellent picture of blood supply to the pituitary. So, the early enhancement of microadenoma long before anterior lobe attributes microadenomas having direct arterial blood supply similar to the posterior pituitary gland.



Dynamic MRI contrast images in coronal plane showing a superior contour convexity with a small nodule Figure 3b: Zoomed images of dynamic MRI, showing the same adenomatous nodule. Note the size of the nodule, which measured two mm.

Coronal T1 and T2WI show microadenoma along the right aspect of the gland which appears bright at the T2WI.

Post-contrast coronal T1WI shows hypointense microadenoma along the right aspect of the gland. Delayed sagittal images after 10 minutes shows enhancing microadenoma is more clear.




These images show a classic case: on T1 a lesion about 3-4 mm in diameter, slightly hypointense compared to normal pituitary tissue, located in the pituitary gland. On T2, the lesion is slightly hyperintense. The sensitivity of an unenhanced MRI scan for detecting pituitary microadenomas is about 70%.

On an unenhanced scan, approximately 70% of all pituitary macroadenoma can be detected. If you give gadolinium, you can reduce the false-negative rate from 30% to 15%.
As mentioned earlier, this usually does not affect patient management.

Coronal T1 and T2-weighted images and T1-weighted images before and after gadolinium. In this patient the lesion in the pituitary gland is only detectable after the administration of intravenous contrast. The differential diagnosis: pituitary microadenoma or Rathke's cleft cyst.

Cystic rounded lesion within the gland which appears of low signal at the T1WI and of bright signal at the T2WI. No contrast uptake within the lesion at the enhanced study, related to cystic
microadenoma. The stalk is deviated to the right side.

A case of pituitary cyst with their characteristic signal appearance and no contrast uptake seen at the enhanced T1WI.

By definition, pituitary macroadenoma are adenomas over 10mm in size. They tend to be soft, solid lesions, often with areas of necrosis or hemorrhage as they get bigger. As they grow, they first expand the sella turcica and then grow upwards. In this example of a pituitary macroadenoma there is suprasellar extension with elevation and compression of the optic chiasm. Because they are soft tumors, they usually indent at the diaphragma sellae, giving them a 'snowman' configuration. This is one feature that can help distinguish between a pituitary macroadenoma and a meningioma. Another feature which can help differentiate them is enlargement of the sella turcica - this generally only occurs with pituitary macroadenoma that originate in the sella.

Macroadenoma with supra and para-sellar extension. Any sellar mass you must comment on its extension, involvement of the cavernous sinus, infra-sellar sphenoid extension and intra-tumoral hemorrhage.

On the left another example of a pituitary macroadenoma. The lesion starts in the sella, which is enlarged, and extends into the suprasellar cistern.
Note the classic 'snowman' configuration caused by constriction by the diaphragma sellae. Notice the blood-fluid level, indicating hemorrhage

The usefulness of observing the inclination of the diaphragmatic leaflets was referred to earlier. On the T2-weighted images on the right you can see that the leaflets are displaced upwards by this
macroadenoma which started in the sella and is growing upwards. A lesion originating above the sella and growing downwards would push the leaflets in the other
direction (this can be seen with meningiomas for example).

Usually the diagnosis of a macroadenoma is straightforward.

Aggressive pituitary adenomas are the most common lesions of the skull base with destruction and extension to the sphenoid sinus.

Acute hemorrhage of a pituitary macroadenoma, with enlargement of the bony pituitary fossa and compression of the optic chiasm (coronal and sagittal scans).

Rathke's cleft cyst (coronal T2-, coronal and sagittal T1-weighted scans).Rathke's cleft cyst arise from the craniopharyngeal duct (Rathke's, s pouch) (An epithelial
structures connect nasopharynx with the 3rd ventricle , involutes during fetal life).

Rathke's cleft cyst

Rathke's cleft cyst(Pre and post-contrast images).

These T1, T2 and T1-weighted images after gadolinium demonstrate another Rathke's cleft cyst located in the pituitary gland. Unlike the normal pituitary tissue and pituitary stalk it does not enhance after the administration of intravenous contrast. The normal pituitary tissue is compressed and displaced far to the left. It is important to recognize this as it could be mistaken for an enhancing component of the cystic mass.

Rathke's cyst with sellar and supra-sellar component.

Post-operative changes with defect along the sellar floor associated with marginal wall enhancement of pituitary abscess.

D.D of supra-sellar hot spot, Ectopic posterior lobe on non-enhanced T1-weighted images Gerinoma, Lipoma, Thrombosed aneurysm and dermoid.

Craniopharyngioma. Adamantanous occur in children and the papillary in old age.

Adamantinomatous and papillary craniopharyngioma.

Supra-sellar calcified mass lesion at CT images with invasion of the ethmoid, sphenoid sinuses with posterior fossa extension as well as frontal lobe extension and eggshell calcification. MRI shows non-homogenous enhancement, with invasion to the posterior fossa, both para-sellar area and posterior ethmoid sinuses.

In over 50% of cases Craniopharyngioma have a pathognomonic appearance. On these unenhanced and enhanced T1-weighted sagittal images, a compressed pituitary gland can
be identified. There is a large intrasellar and suprasellar mass with cystic and enhancing components as well as calcifications. These findings in a child are virtually pathognomonic for Craniopharyngioma
(perhaps with only a dermoid in the differential diagnosis).

.
•

Figure 13: Sagittal T1 weighted unenhanced (A) and coronal enhanced (B) images showing a partially cystic craniopharyngioma. This is a large complex suprasellar mass which extends down into the pituitary fossa and up to deform the third ventricle. It is of mixed signal intensity and the solid components enhance after contrast. (B) There are patchy areas of high signal before contrast (A) which represent the cystic components with a high protein/ lipid content.


Meningioma of the planum sphenoidale with “dural tail” (axial, coronal and sagittal scans).The pituitary gland and the meningioma can be identified, even at the pre-contrast images.

Supra-sellar meningioma with the epicenter of the lesion above the sella.

Sagittal images of the same case (Suprasellar meningioma) with the epicenter of the lesion above the sella.

Supra-sellar meningioma with intra-sellar extension.

Figure11 A and B: Coronal (A) enhanced T1 weighted image and sagittal (B) enhanced T1 weighted images. There is a suprasellar meningioma which appears to be arising from the planum sphenoidale and is seen extending along the floor of the anterior cranial fossa where a dural tail (arrow) is visible. The pituitary gland itself appears normal and a cleft of CSF is visible between the meningioma and the pituitary tissue. The meningioma is displacing and possibly involving the optic nerves anterior to the chiasm.

A Coronal T1 weighted enhanced image of a left cavernous sinus meningioma. There is expansion of the left cavernous sinus (arrows) and some concentric narrowing of the left cavernous carotid artery (compare to the right carotid ).

Right para-sellar partially thrombosed aneurysm.

Aneurysm of right para-sellar region with partially thrombosed aneurysm.

Enhanced and non-enhanced study of right para-sellar aneurysm.

The mass is predominantly black and there is a large flow artifact running in the phase-encoding direction. These findings correspond to rapid blood flow, and the mass must therefore be an aneurysm

Angiogram of the same patient. It demonstrates that the flow in the aneurysm is not laminar, but that it swirls, gradually filling the lumen with contrast.

Para-ophthalmic “giant aneurysm” of the right internal carotid artery (coronal T2-, axial T2/FLAIR-weighted images, TOF-MRA).

Carotid cavernous fistula in a 16years old boy presented with exophthalmous and objective tinnitus.

MRA demonstrate right carotid cavernous fistula(Arrow) with dilated superior ophthalmic vein and 3D reconstructed images showing CC fistula.

Intracranial intra-sellar kissing carotid arteries.

These are CT images of hamartoma suspended from the floor of the third ventricle. It does not enhance after the administration of intravenous contrast. Hamartoma masses of dysplastic found exclusively in young children and the most common
location is floor of the 3rd ventricle.

MR images of a similar small nodule suspended from the floor of the third ventricle.

The best images to see hamartomas on are enhanced sagittal T1-weighted MR images. Here you can see the non-enhancing hamartomas attached to the tuber cinereum between the pituitary stalk and mamillary body. There really is no differential diagnosis. The hamartoma is a congenital neoplastic heterotopias and usually present with precious puberty at child and gelastic seizures at adult.

Glioma can occur in any part of the brain and the optic chiasm is a common location, particularly in patients with neurofibromatosis type 1. This enhanced CT shows an example of an optic nerve glioma in a patient with neurofibromatosis. There is a suprasellar mass which is indistinguishable from the optic chiasm.

These consecutive coronal and axial enhanced MR-images show the mass at the optic chiasm and the swollen optic nerves with enhancement at the post-contrast study.

This is another example of a right-sided optic nerve glioma with enhancement after gadolinium. Note the normal pituitary gland and stalk.

Intra-sellar Lipoma (coronal and sagittal scans).

Hypophysitis with thickening of the pituitary stalk in combination with an intense contrast enhancement (coronal and sagittal imaging).

Right para-and suprasellar dermoid cyst.

Rupture supra-sellar dermoid cyst with hyperintense speckles at the cortical sulci and fat fluid level at the ventricles.


Right para-sellar arachnoid cyst.

T1 weighted enhanced images show thickening of the pituitary stalk and nodular enhancement of the Rt. Side of the chiasm(arrow) in a patient with neurosarcoid.

Hypophysitis sagittal and coronal post-contrast study shows markedly thickened pituitary stalk.

Sagittal enhanced T1WI show a well defined enhancing mass within the pituitary stalk. The pituitary gland is normal, as is the hypothalamus. This was a granular cell tumour.

Histiocytosis involving the pituitary infundibulum. Sagittal pre and post-contrast study absent posterior pituitary spot with thickened stalk on post-contrast images.

Hypothalamic glioma at pre and post-contrast study and the presentation is diabetes insipedus.

T2 and T1WI, pre and post-contrast study show hyperintense mass filling the inferior recesses of the 3rd ventricle and extending down along the infundibulum into pituitary fossa. It demonstrate homogenous
contrast uptake. The pineal body is also involved, related to supra-sellar germinoma.

The following case concerns a 9-year-old male with a history of headache, nausea and vomiting. Sagittal T1 images before and after intravenous contrast show a mass in the midline, on the floor of the third ventricle. The mass enhances after gadolinium. Continue with next images. Sagittal T2 and T1WI . This is a Germinoma.

Figure 16: Sagittal (A) and (B) T1 weighted enhanced images of two different germinomas. (A) demonstrates a large homogeneously enhancing soft tissue mass within the suprasellar region involving the upper aspect of the pituitary stalk and the hypothalamic region with a second separate mass visible in the region of the pineal gland -this is typical of a germinoma. (B) demonstrates a much smaller lesion in the region of the upper aspect of the stalk and hypothalamus (arrow).

Trigeminal lipoma with right side facial neuralgia with right para-sellar component at the axial CT Scan and the coronal T1WI.

Trigeminal schwanoma is the 2nd one after acoustic neuroma. The diagnostic landmark is dumble shaped configuration and involvement of the Meckels cave .Trigeminal neuroma, axial T2, T1WI, pre and post-contrast images with extension through the skull foramina and the right para-sellar component.

Parasellar chordoma (coronal, axial and sagittal scans) with characteristic bright fluid signal at the T2WI.

Chordomas are the most common lesions of the clivus, also a favored location for metastases and chondrosarcomas. his patient has a normal pituitary gland. Posterior to this is a large, fungating mass positioned at the level of the clivus. The CT shows some calcifications in this area. The differential diagnosis for this mass would be chondroma or chondrosarcoma. Chordomas tend to occur in the midline, whereas condrosarcomas
tend to occur off the midline.

Axial T2 and axial enhanced T1WI of chondrosarcoma. This shows the typical bubby high T2 signal and involve the right side of the pituitary fossa, the Rt. Cavernous sinus and
the extends into the Rt. Middle cranial fossa.

The patient on the left is a patient with lung cancer who presented with a sixth cranial nerve palsy. The abnormality is in the clivus, which should have a high signal intensity on this sagittal T1-weighted image (as in the image on the left). A low signal intensity means the normal fatty marrow has been replaced by some other tissue. In this case by tumor metastasis. Also lymphomas, myelomas or diffuse bone abnormalities can give this appearance. Therefore always
take a minute to look at the clivus.

Coronal enhanced T1WI show a diffusely enlarged pituitary gland with bilateral enlargement of the cavernous sinuses and some thickening of the stalk, this was metastatic disease with breast carcinoma.

So again in order to analyze a sellar or parasellar mass on MRI we use the following anatomic approach: First identify the pituitary gland and sella turcica. Then determine the epicenter of the lesion and whether it is in the sella or above, below or lateral to the sella. If it is in the sella, determine whether or not the sella is enlarged. Once the location of the mass is clear, analyze the signal intensity patterns: is the lesion cystic or solid? Does it contain any abnormal vessels? Are there any calcifications? And so on. Finally establish a Differential Diagnosis.

Quiz Case.1 Dynamic enhanced MRI study show, CSC Hem.

Q 2,AHMA.

2 G.

Rosai–Dorfmann disease is a lymphoproliferative disorder of male predominance that rarely involves the central nervous system. Scanty citations of RD involving isolated cranial and spinal compartments of central nervous system are noted in the literature, combined involvement of the two being extremely rare. Extensive involvement of both compartments in a female child is highlighted in this case report with a short review of the available literature.

A rare case of posterior fossa CP, and account for 1-4%, CT and MR images show PFCP, arising from the sellar region and extending to the posterior fossa, and CT show calcification of the lesion and MRI show cystic lesion with brain stem compression.

![Presentation1.pptx%20 flash[1]](https://img.pdfslide.us/doc/110x75/553b80ea4a795951348b46c1/presentation1pptx20-flash1.jpg)
![Presentation1.pptx [repaired]](https://img.pdfslide.us/doc/110x75/58a9e64c1a28ab36018b4839/presentation1pptx-repaired-58ac0f71a4da9.jpg)