Embed Size (px)
Citation preview
21/09/2017
1
Chronic Kidney Disease -
General management and standard of care
part 1
Prof Michel Jadoul
Cliniques universitaires Saint-Luc
Université Catholique de Louvain
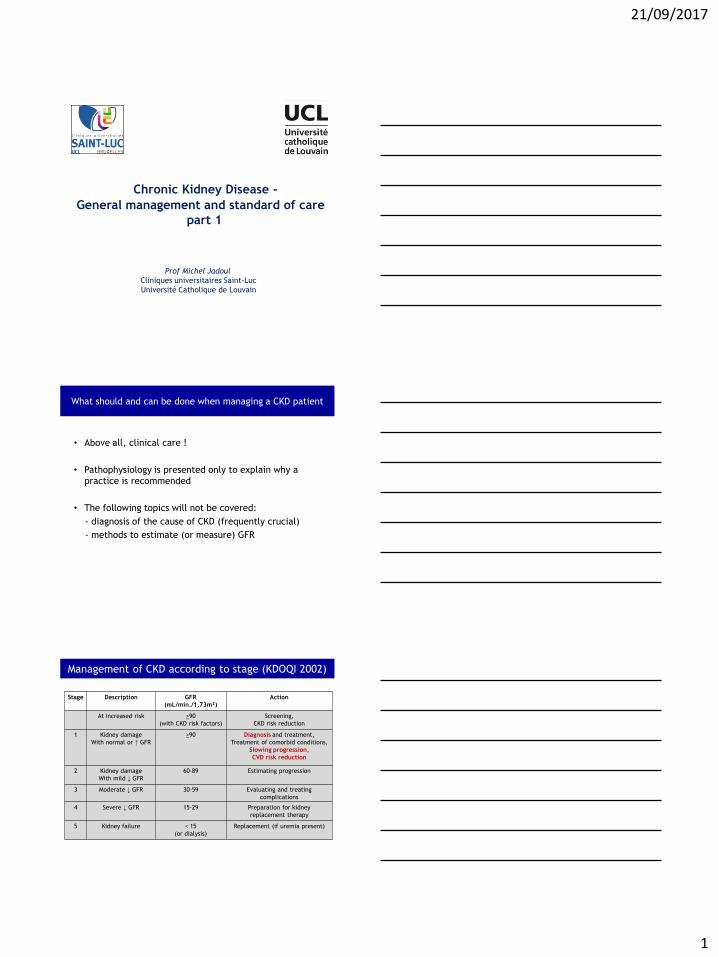
• Above all, clinical care !
• Pathophysiology is presented only to explain why a
practice is recommended
• The following topics will not be covered:
- diagnosis of the cause of CKD (frequently crucial)
- methods to estimate (or measure) GFR
What should and can be done when managing a CKD patient
Stage Description GFR
(mL/min./1,73m²)
Action
At increased risk >90
(with CKD risk factors)
Screening,
CKD risk reduction
1 Kidney damage
With normal or ↑ GFR
>90
Diagnosis and treatment,
Treatment of comorbid conditions,
Slowing progression,
CVD risk reduction
2 Kidney damage
With mild ↓ GFR
60-89 Estimating progression
3 Moderate ↓ GFR 30-59 Evaluating and treating
complications
4 Severe ↓ GFR 15-29 Preparation for kidney
replacement therapy
5 Kidney failure < 15
(or dialysis)
Replacement (if uremia present)
Management of CKD according to stage (KDOQI 2002)
21/09/2017
2
KDIGO CKD Guidelines 2012
Section 1: Definition and classification of CKD
Section 2: Definition, identification and prediction of CKD progression
Section 3: Management of progression and complications of CKD
Section 4: Other Complications of CKD: CVD, medication dosing,
patient safety, infections, hospitalizations, and caveats for
investigating complications of CKD
Section 5: Referral to specialists and models of care
21/09/2017
3
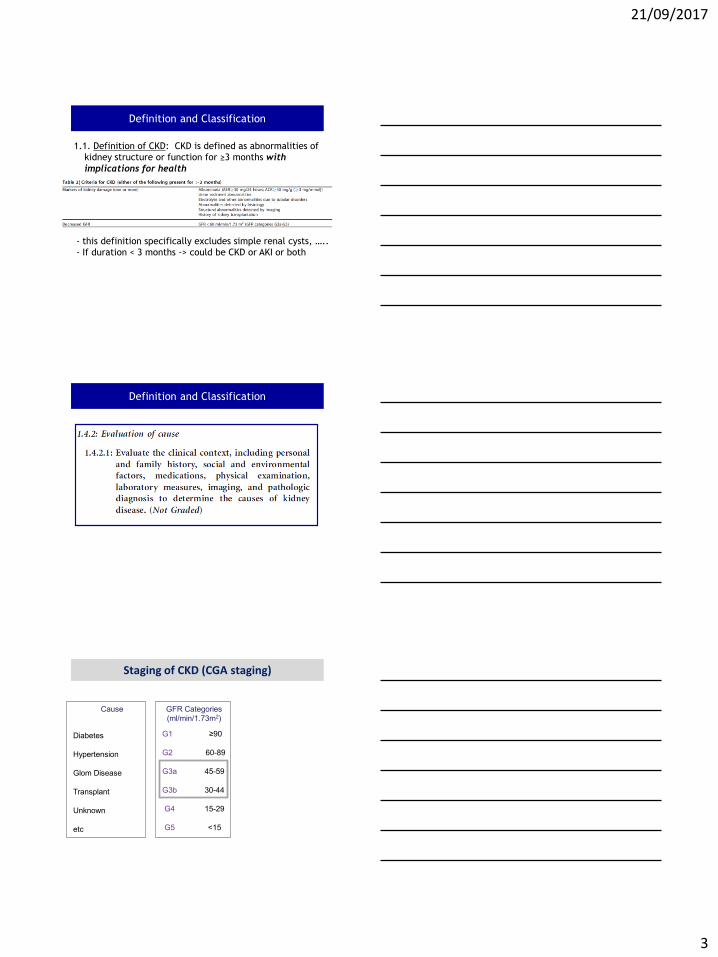
Definition and Classification
1.1. Definition of CKD: CKD is defined as abnormalities of
kidney structure or function for ≥3 months with
implications for health
- this definition specifically excludes simple renal cysts, …..
- If duration < 3 months -> could be CKD or AKI or both
Definition and Classification
Cause GFR Categories
(ml/min/1.73m2)
Albuminuria Categories
(ACR, mg/g)
Diabetes G1 ≥90
A1
<30
Hypertension G2 60-89
Glom Disease G3a 45-59
A2
30-299
Transplant G3b 30-44
Unknown G4 15-29
A3
≥300
etc G5 <15
Tigette OK
N to midly increased
Moderately increased
Severly increased
Staging of CKD (CGA staging)
21/09/2017
4
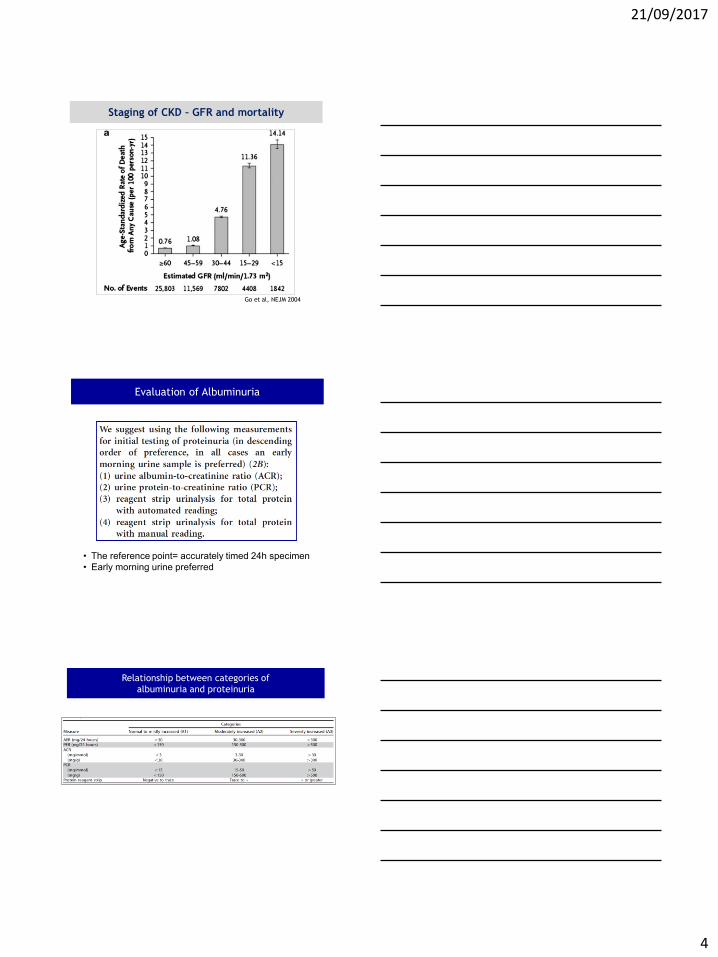
Go et al, NEJM 2004
Staging of CKD – GFR and mortality
• The reference point= accurately timed 24h specimen
• Early morning urine preferred
Evaluation of Albuminuria
Relationship between categories of
albuminuria and proteinuria
21/09/2017
5
Cause GFR Categories
(ml/min/1.73m2)
Albuminuria Categories
(ACR, mg/g)
Diabetes G1 ≥90
A1
<30
Hypertension G2 60-89
Glom Disease G3a 45-59
A2
30-299
Transplant G3b 30-44
Unknown G4 15-29
A3
≥300
etc G5 <15
N to mildly increased
Dipstick neg to trace
Moderately increased
Dipstick trace to +
Severely increased
Dipstick > +
Staging of CKD (CGA staging)
Prognostic value of GFR and albuminuria:
Cohorts and Subjects of CKD Consortium
• Community based populations – With ACR data, 14 studies, n=105,872
– With dipstick data, 10 studies, n=1,239,447
• Populations at increased CVD risk (HTN, diab, CV) – 10 studies, n=266,975
• CKD cohorts – 14 studies, n= 21,688
45 cohorts in total, >1.5 million subjects
Collaborative meta-analysis
Major publications: Lancet, KI, JAMA
Prognostic value of GFR and albuminuria:
Cohorts and Subjects of CKD Consortium
• Community based populations – With ACR data, 14 studies, n=105,872
– With dipstick data, 10 studies, n=1,239,447
• Populations at increased CVD risk (HTN, diab, CV) – 10 studies, n=266,975
• CKD cohorts – 14 studies, n= 21,688
45 cohorts in total, >1.5 million subjects
Collaborative meta-analysis
Major publications: Lancet, KI, JAMA
Matsushita et al, Lancet 2010
21/09/2017
6
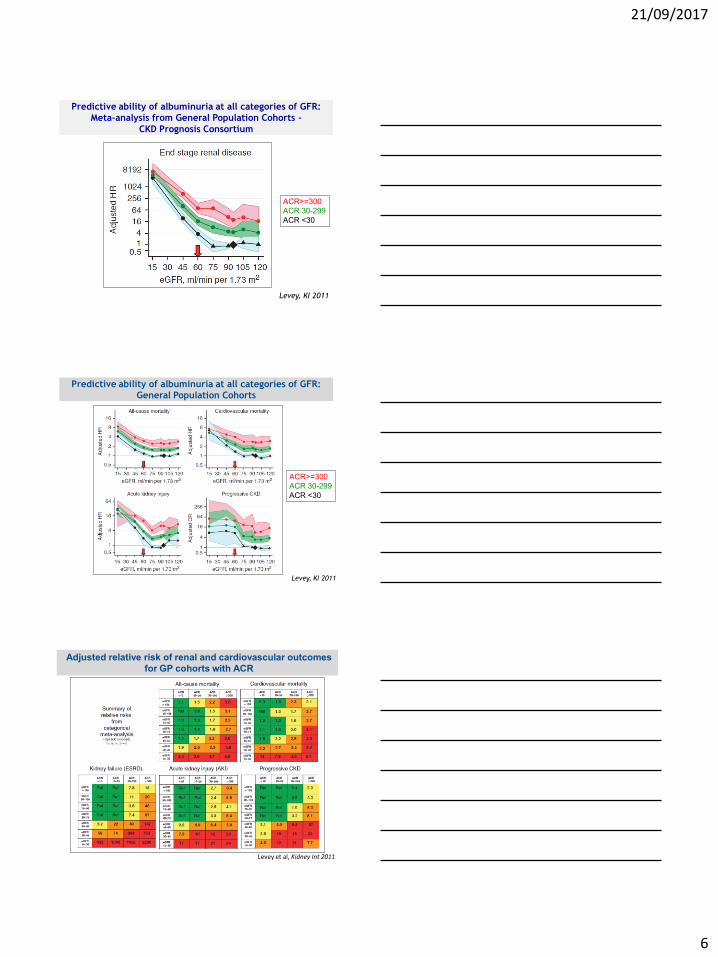
Predictive ability of albuminuria at all categories of GFR:
Meta-analysis from General Population Cohorts -
CKD Prognosis Consortium
Levey, KI 2011
ACR>=300
ACR 30-299
ACR <30
Predictive ability of albuminuria at all categories of GFR:
General Population Cohorts
ACR>=300
ACR 30-299
ACR <30
Levey, KI 2011
Adjusted relative risk of renal and cardiovascular outcomes
for GP cohorts with ACR
Levey et al, Kidney Int 2011
21/09/2017
7
KDIGO CKD Guidelines 2012
Section 1: Definition and classification of CKD
Section 2: Definition, identification and prediction of CKD progression
Section 3: Management of progression and complications of CKD
Section 4: Other Complications of CKD: CVD, medication dosing,
patient safety, infections, hospitalizations, and caveats for
investigating complications of CKD
Section 5: Referral to specialists and models of care
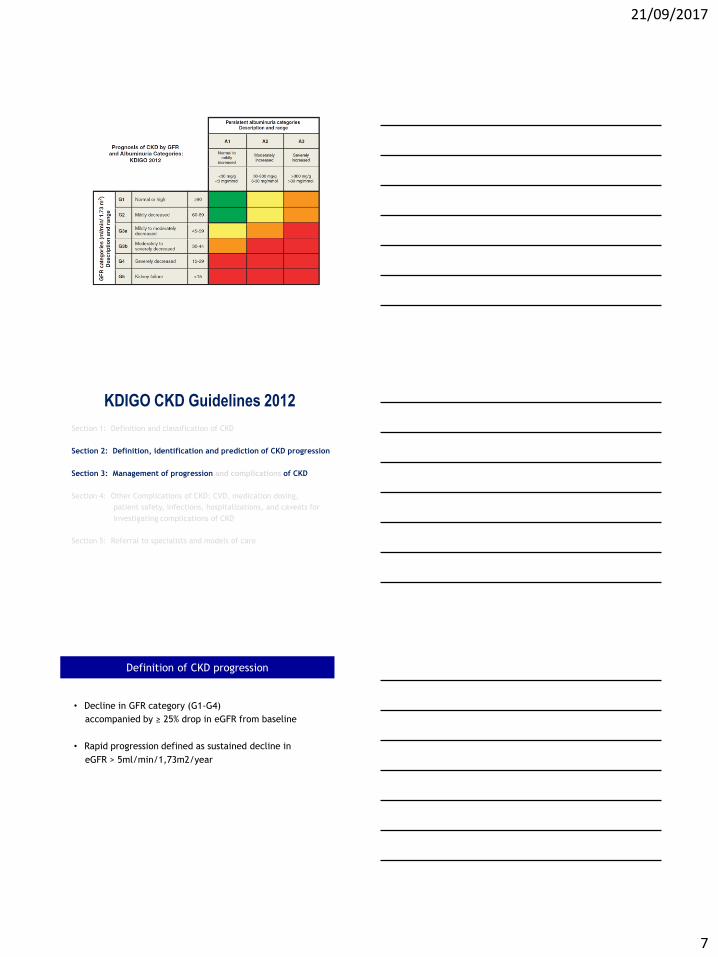
Definition of CKD progression
• Decline in GFR category (G1-G4)
accompanied by ≥ 25% drop in eGFR from baseline
• Rapid progression defined as sustained decline in
eGFR > 5ml/min/1,73m2/year
21/09/2017
8
• Cause of CKD
• Level of GFR
• Level of albuminuria
• Age
• Gender
• Elevated BP
• Hyperglycemia
• Dyslipidemia
• Smoking
• Obesity
• History of CVD
• Ongoing exposure to nephrotoxic agents
Predictors of progression of CKD
Anemia, acidosis, bone metabolism, hyperuricemia….
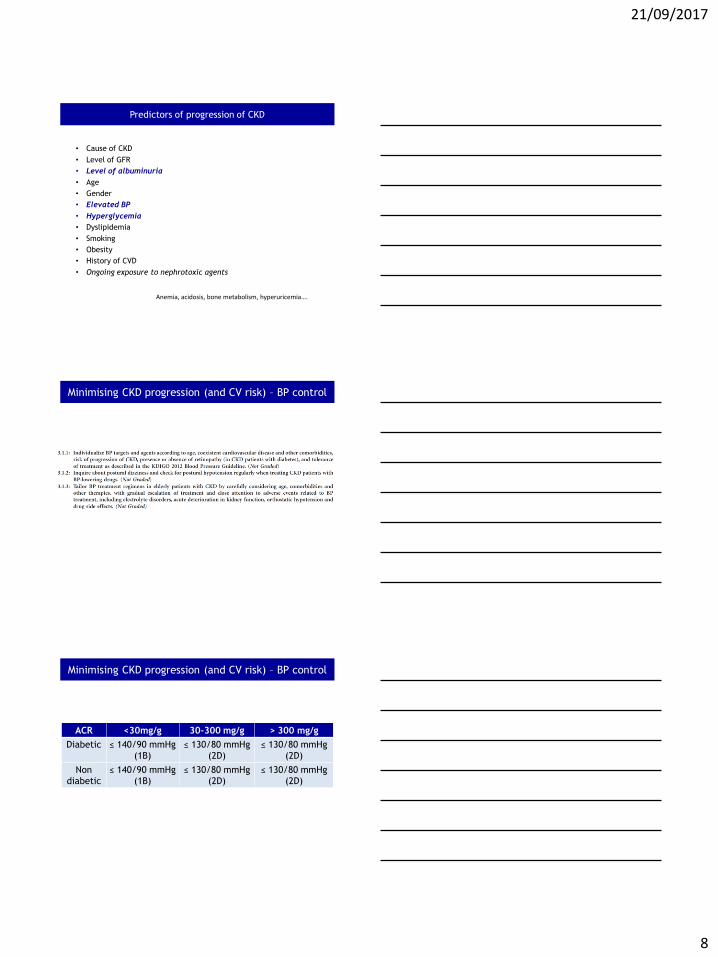
Minimising CKD progression (and CV risk) – BP control
ACR <30mg/g 30-300 mg/g > 300 mg/g
Diabetic ≤ 140/90 mmHg
(1B)
≤ 130/80 mmHg
(2D)
≤ 130/80 mmHg
(2D)
Non
diabetic
≤ 140/90 mmHg
(1B)
≤ 130/80 mmHg
(2D)
≤ 130/80 mmHg
(2D)
Minimising CKD progression (and CV risk) – BP control
21/09/2017
9
21/09/2017
10
21/09/2017
11
21/09/2017
12
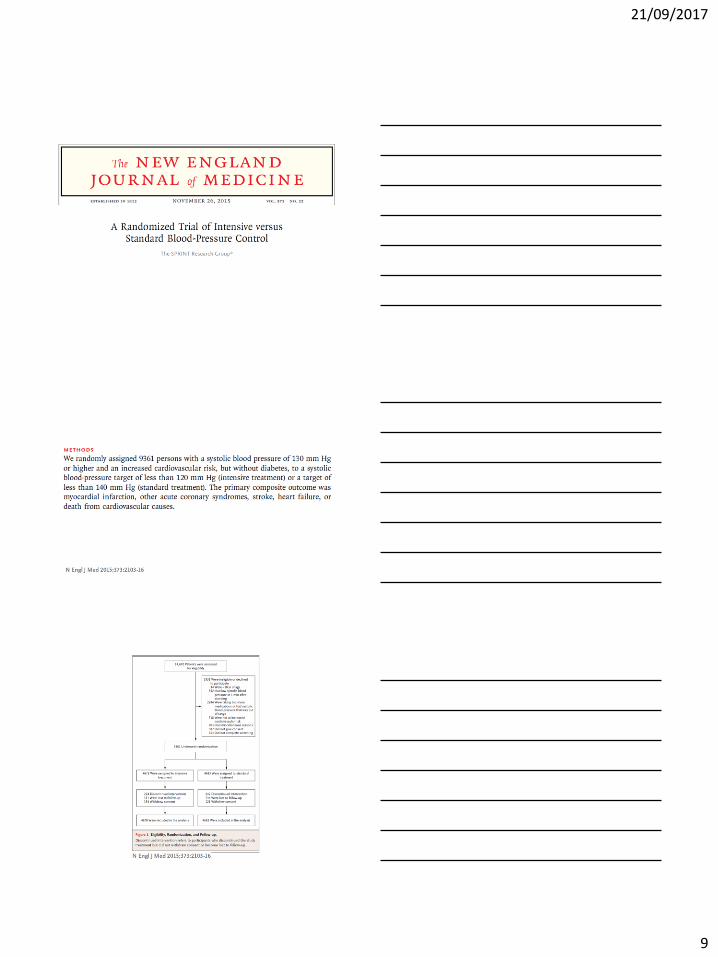
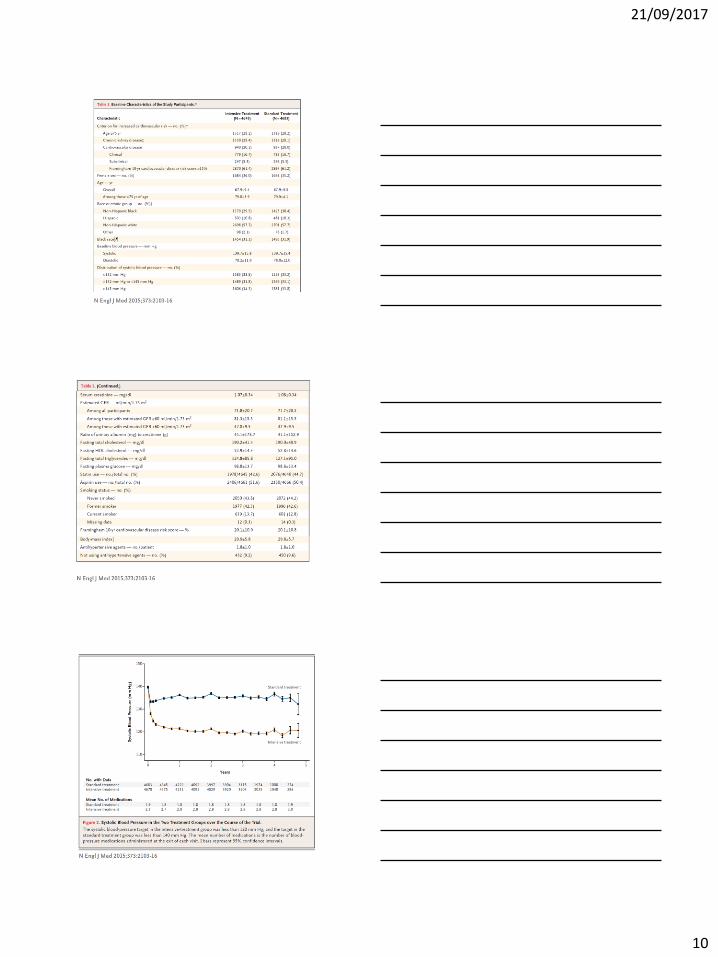
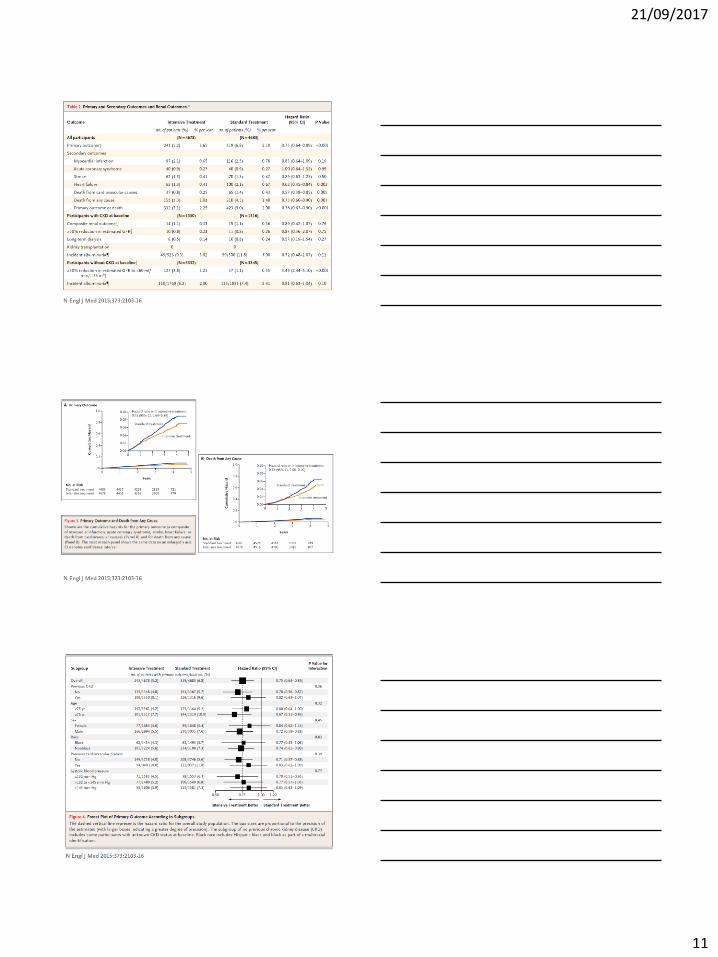
Managing hypertension in CKD patients : a marathon, not a SPRINT !
• SPRINT= CV trail , with a significant proportion of pts with mild-moderate CKD
• SPRINT = NOT A TYPICAL CKD TRIAL
• Standard versus more intensive antiHT therapy in pts with pre-existing CVD or at high CV risk (including the elderly)
• Subjects with advanced CKD or >1g proteinuria were excluded from SPRINT
• Do not generalize ……
Chertow et al JASN 2016; Rocco and Cheung Kidney Int 2016
• KDIGO Blood pressure Guideline currently under revision
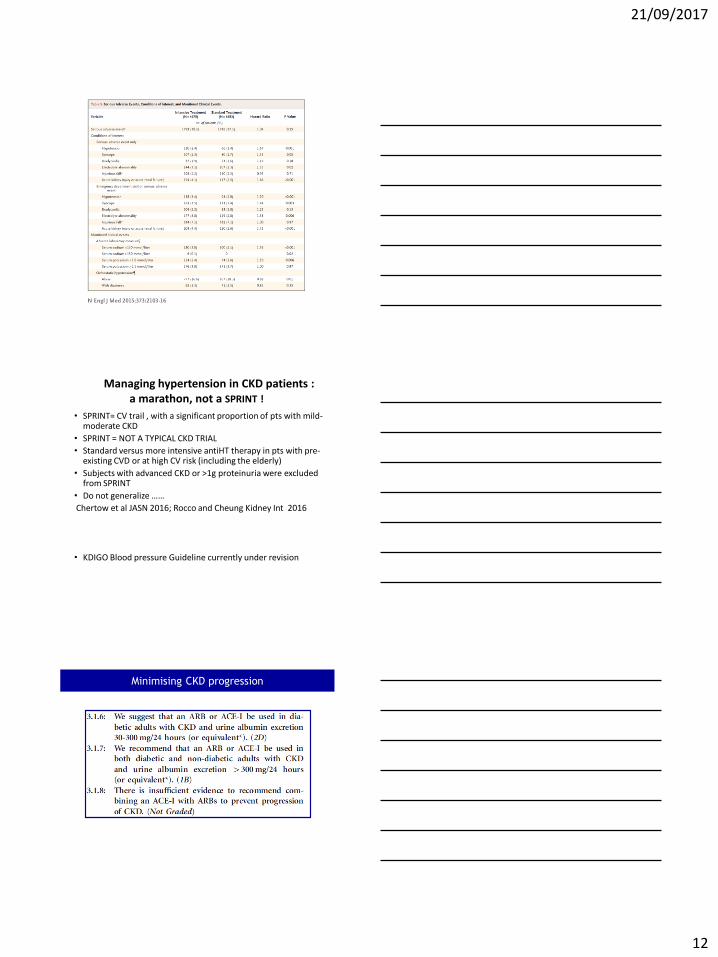
Minimising CKD progression
21/09/2017
13
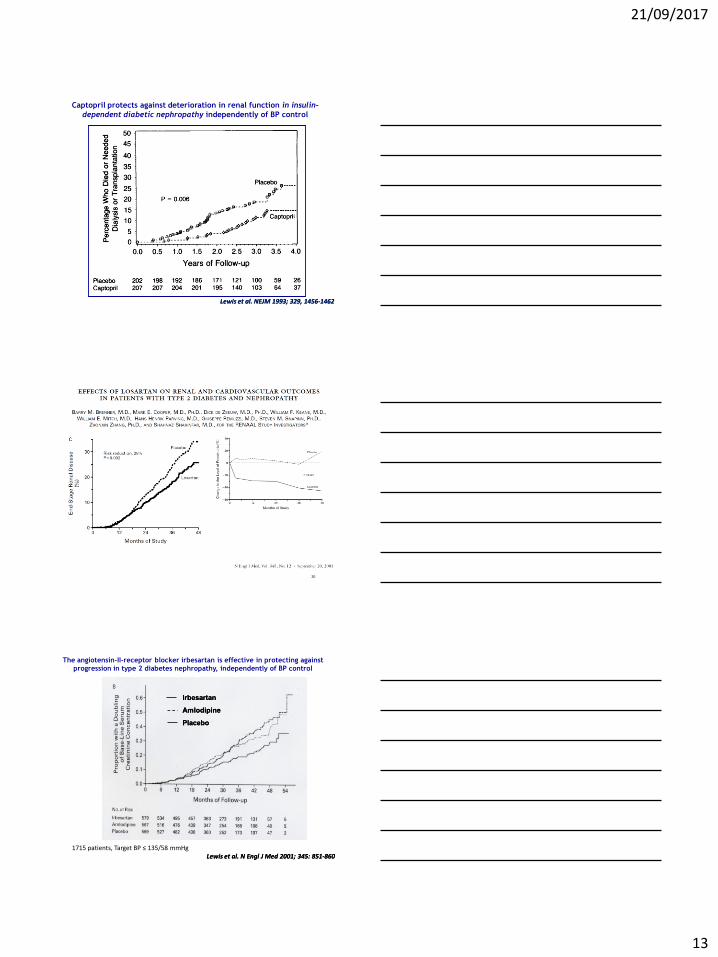
Lewis et al. NEJM 1993; 329, 1456Lewis et al. NEJM 1993; 329, 1456--14621462
Captopril protects against deterioration in renal function in insulin-
dependent diabetic nephropathy independently of BP control
20
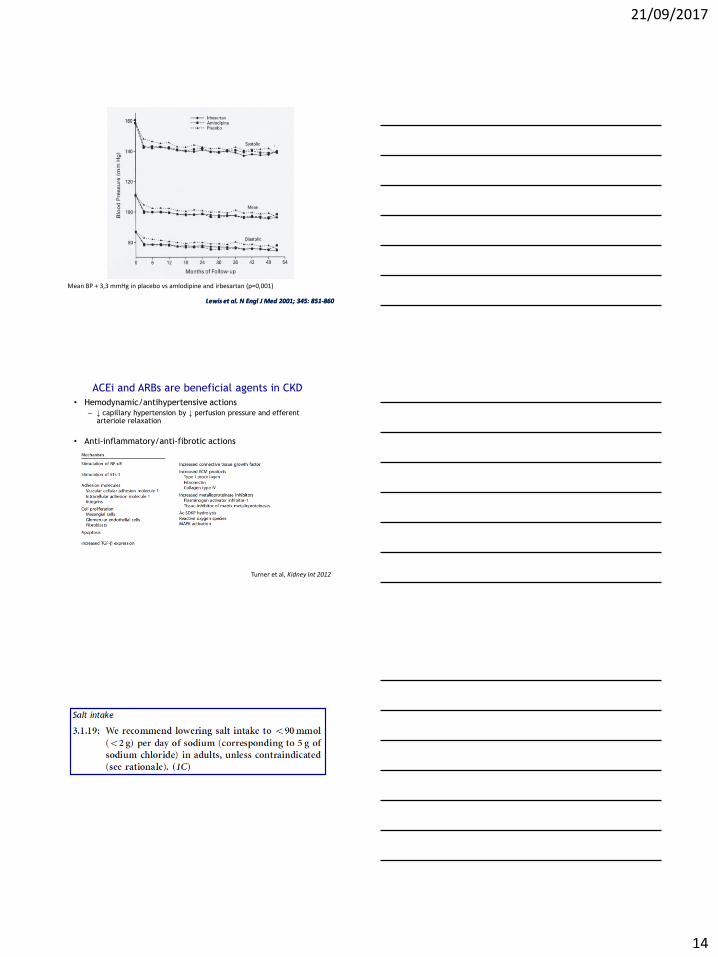
Lewis et al. N Lewis et al. N EnglEngl J Med 2001; 345: 851J Med 2001; 345: 851--860860
IrbesartanIrbesartan
AmlodipineAmlodipine
PlaceboPlacebo
The angiotensin-II-receptor blocker irbesartan is effective in protecting against
progression in type 2 diabetes nephropathy, independently of BP control
1715 patients, Target BP ≤ 135/58 mmHg
21/09/2017
14
Lewis et al. N Lewis et al. N EnglEngl J Med 2001; 345: 851J Med 2001; 345: 851--860860
Mean BP + 3,3 mmHg in placebo vs amlodipine and irbesartan (p=0,001)
ACEi and ARBs are beneficial agents in CKD
• Hemodynamic/antihypertensive actions – ↓ capillary hypertension by ↓ perfusion pressure and efferent
arteriole relaxation
• Anti-inflammatory/anti-fibrotic actions
Turner et al, Kidney Int 2012
21/09/2017
15
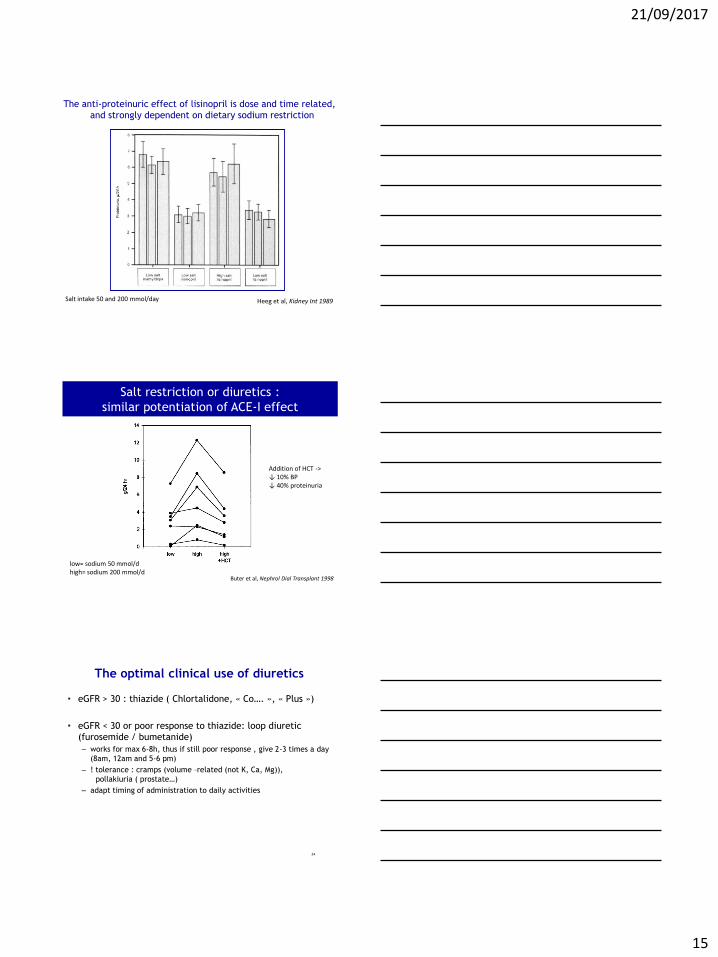
Heeg et al, Kidney Int 1989
The anti-proteinuric effect of lisinopril is dose and time related,
and strongly dependent on dietary sodium restriction
Salt intake 50 and 200 mmol/day
Salt restriction or diuretics :
similar potentiation of ACE-I effect
Buter et al, Nephrol Dial Transplant 1998
low= sodium 50 mmol/d high= sodium 200 mmol/d
Addition of HCT -> ↓ 10% BP ↓ 40% proteinuria
The optimal clinical use of diuretics
• eGFR > 30 : thiazide ( Chlortalidone, « Co…. », « Plus »)
• eGFR < 30 or poor response to thiazide: loop diuretic
(furosemide / bumetanide)
– works for max 6-8h, thus if still poor response , give 2-3 times a day
(8am, 12am and 5-6 pm)
– ! tolerance : cramps (volume –related (not K, Ca, Mg)),
pollakiuria ( prostate…)
– adapt timing of administration to daily activities
24
21/09/2017
16
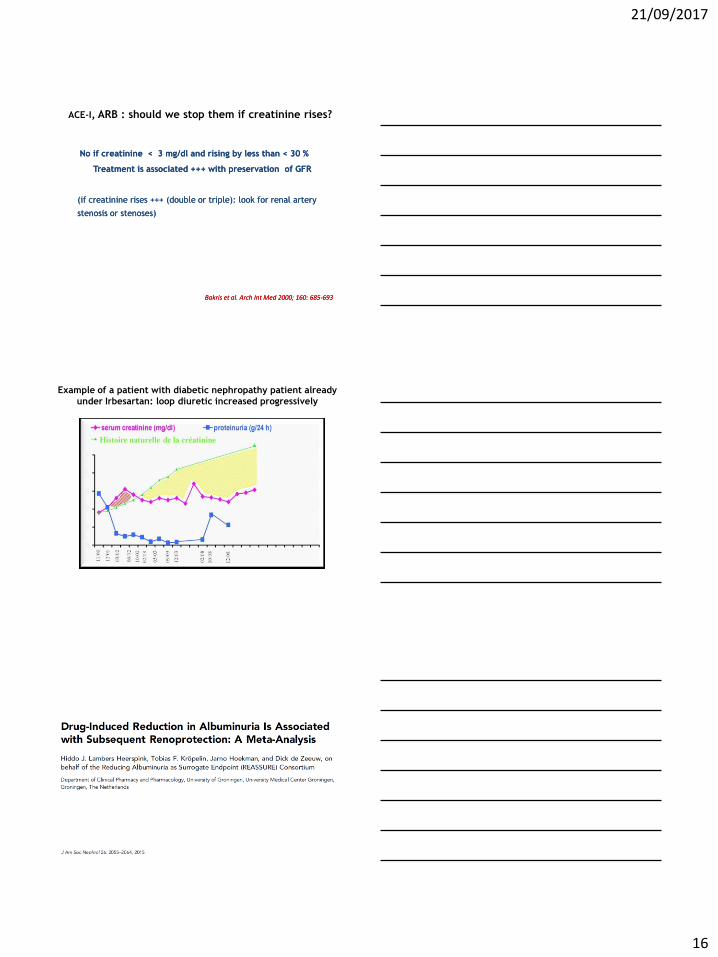
ACE-I, ARB : should we stop them if creatinine rises?
No if creatinine < 3 mg/dl and rising by less than < 30 %No if creatinine < 3 mg/dl and rising by less than < 30 %
Treatment is associated +++ with preservation of GFRTreatment is associated +++ with preservation of GFR
(if creatinine rises +++ (double or triple): look for renal artery (if creatinine rises +++ (double or triple): look for renal artery
stenosis or stenosis or stenosesstenoses))
BakrisBakris et al. Arch et al. Arch IntInt Med 2000; 160: 685Med 2000; 160: 685--693693
Example of a patient with diabetic nephropathy patient already
under Irbesartan: loop diuretic increased progressively
21/09/2017
17
Hyperkalemia with ACE inhibitors /
angiotensin II receptor antagonist / aliskiren (I)
Is it true hyperkalemia? (to avoid stopping valuable drug because of a laboratory error)
• Time between blood sampling and analysis?
• Hemolysis?
• Confirmed (precautions), severe? (> 5.8 mmol/l)
Dietary ? • Salt substitute
• (Dry) fruit, bananas, chocolate, instant coffee,....
28
Correct any acidosis (Vichy 1-2 glasses/d)
ACE inhibitor + angiotensin II receptor or aliskiren:
stop or reduce 1 of the 2
ACE inhibitor (angiotensin II receptor ) + spironolactone:
stop or reduce spironolactone
ACE inhibitor or angiotensin II receptor or aliskiren monotherapy:
dose - add Furosemide
If persistence, add calcium kayexalate 15 g/2 days per os
Awaiting newer K binders (Patiromer, ZS-9)
29
Hyperkalemia with ACE inhibitors /
angiotensin II receptor antagonist / aliskiren (I)
21/09/2017
18
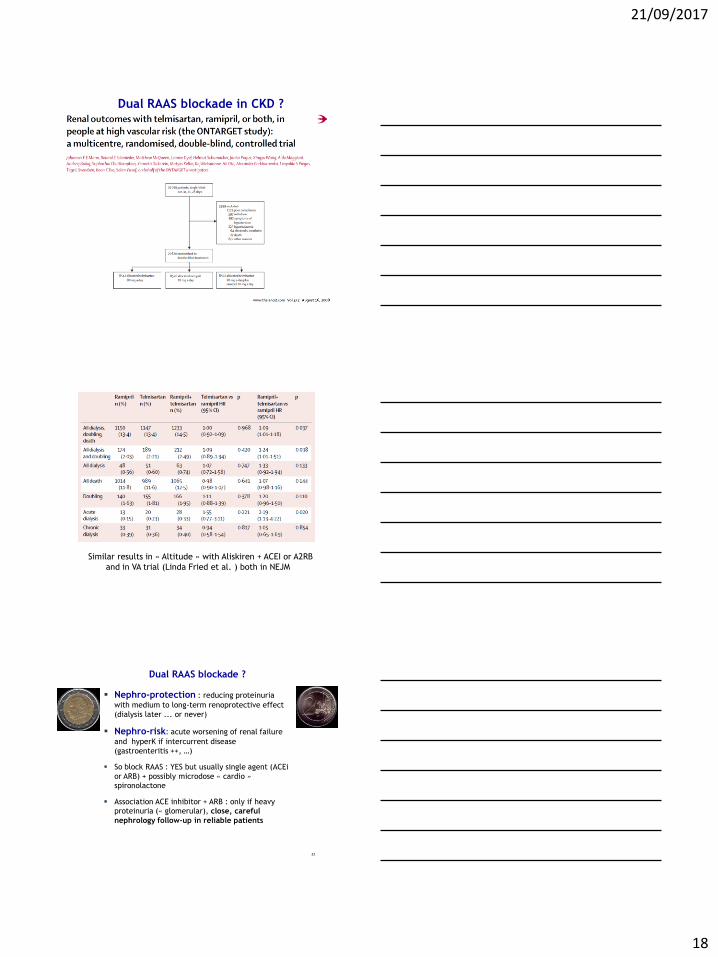
Dual RAAS blockade in CKD ?
Similar results in « Altitude » with Aliskiren + ACEI or A2RB
and in VA trial (Linda Fried et al. ) both in NEJM
Dual RAAS blockade ?
Nephro-protection : reducing proteinuria
with medium to long-term renoprotective effect
(dialysis later ... or never)
Nephro-risk: acute worsening of renal failure
and hyperK if intercurrent disease
(gastroenteritis ++, …)
So block RAAS : YES but usually single agent (ACEi
or ARB) + possibly microdose « cardio »
spironolactone
Association ACE inhibitor + ARB : only if heavy
proteinuria (« glomerular), close, careful
nephrology follow-up in reliable patients
32
21/09/2017
19
Rationale:
If BP and proteinuria are well controlled, the slope of CKD
progression will not change much with lower protein intake
In > 65 y old patients, potential for malnutrition !
Protein intake
Glycemic control
Lifestyle measures
21/09/2017
20
KDIGO CKD Guidelines 2012
Section 1: Definition and classification of CKD
Section 2: Definition, identification and prediction of CKD progression
Section 3: Management of progression and complications of CKD
Section 4: Other Complications of CKD: CVD, medication dosing,
patient safety, infections, hospitalizations, and caveats for
investigating complications of CKD
Section 5: Referral to specialists and models of care
• Strong and independent associations between GFR and albuminuria
categories and risk of CVD in people with CKD
• Cardiovascular risk in CKD is multifactorial
• Cardiovascular disease is more frequent and severe, often not
recognised and undertreated in patients with CKD
• Patients with CKD should be considered amongst the highest risk
groups for CVD
• To prevent progression of CKD is to prevent CVD
Classical CV risk factors
Not modifiable Modifiable but no proven benefit
Modifiable with clinical benefit
Older age Uric acid Smoking
Male gender Homocysteine Obesity
Ethnicity Hypertension
Lp (a) Diabetes
HDL cholesterol LDL cholesterol
Physical activity
37
21/09/2017
21
38
21/09/2017
22
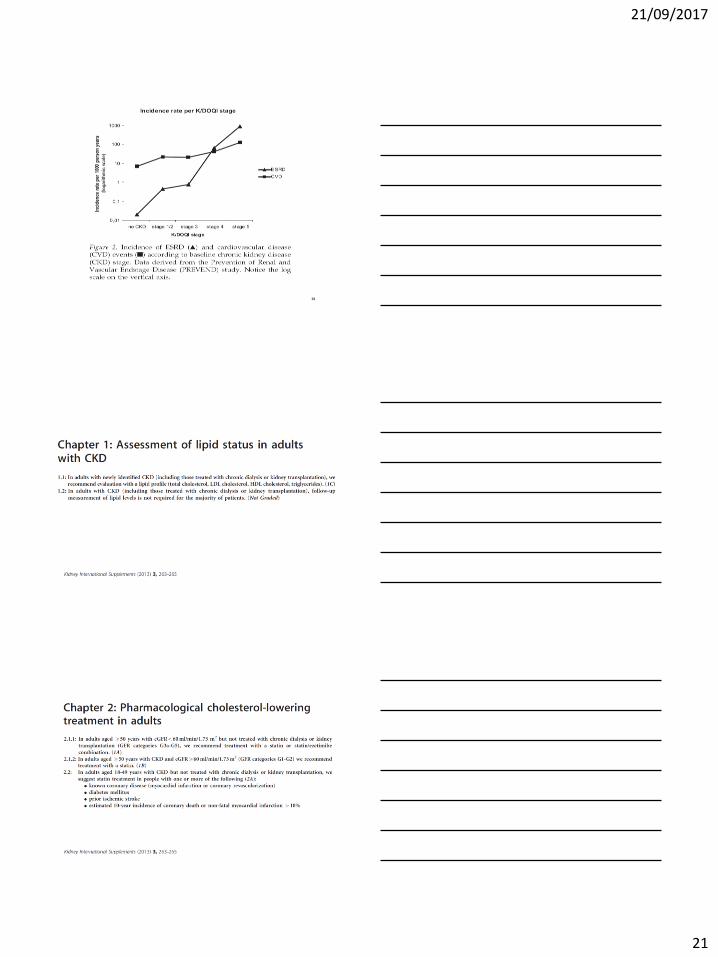
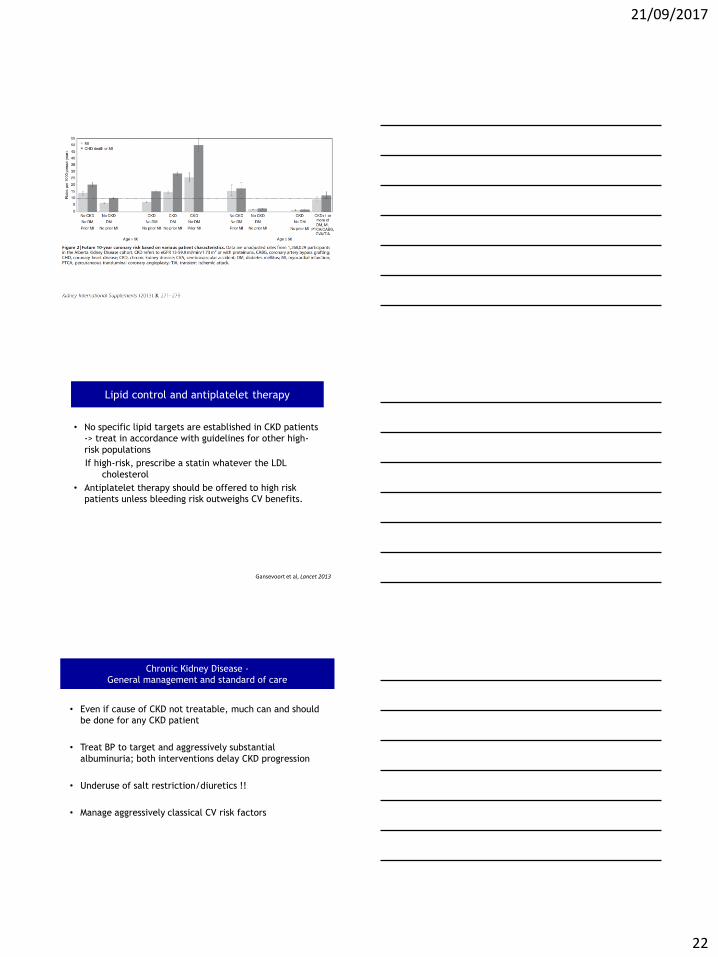
Lipid control and antiplatelet therapy
• No specific lipid targets are established in CKD patients
-> treat in accordance with guidelines for other high-
risk populations
If high-risk, prescribe a statin whatever the LDL
cholesterol
• Antiplatelet therapy should be offered to high risk
patients unless bleeding risk outweighs CV benefits.
Gansevoort et al, Lancet 2013
• Even if cause of CKD not treatable, much can and should
be done for any CKD patient
• Treat BP to target and aggressively substantial
albuminuria; both interventions delay CKD progression
• Underuse of salt restriction/diuretics !!
• Manage aggressively classical CV risk factors
Chronic Kidney Disease -
General management and standard of care
21/09/2017
23
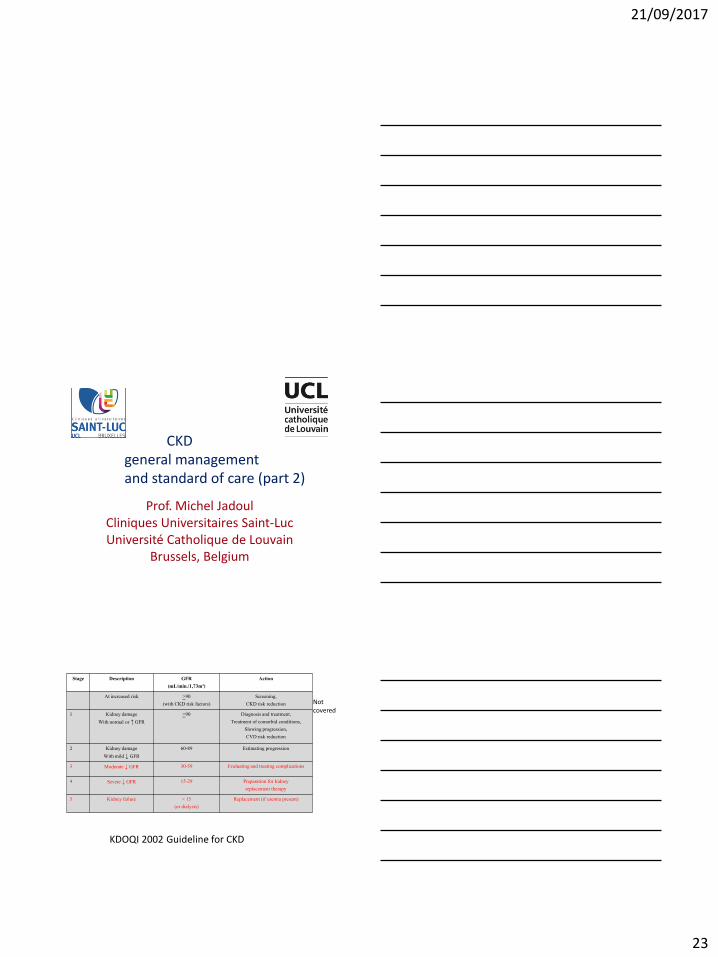
CKD general management and standard of care (part 2)
Prof. Michel Jadoul Cliniques Universitaires Saint-Luc Université Catholique de Louvain
Brussels, Belgium
Stage Description GFR (mL/min./1,73m²)
Action
At increased risk >90 (with CKD risk factors)
Screening, CKD risk reduction
1 Kidney damage
With normal or ↑ GFR
>90
Diagnosis and treatment, Treatment of comorbid conditions,
Slowing progression, CVD risk reduction
2 Kidney damage
With mild ↓ GFR
60-89 Estimating progression
3 Moderate ↓ GFR 30-59 Evaluating and treating complications
4 Severe ↓ GFR 15-29 Preparation for kidney replacement therapy
5 Kidney failure < 15 (or dialysis)
Replacement (if uremia present)
KDOQI 2002 Guideline for CKD
Not covered
21/09/2017
24
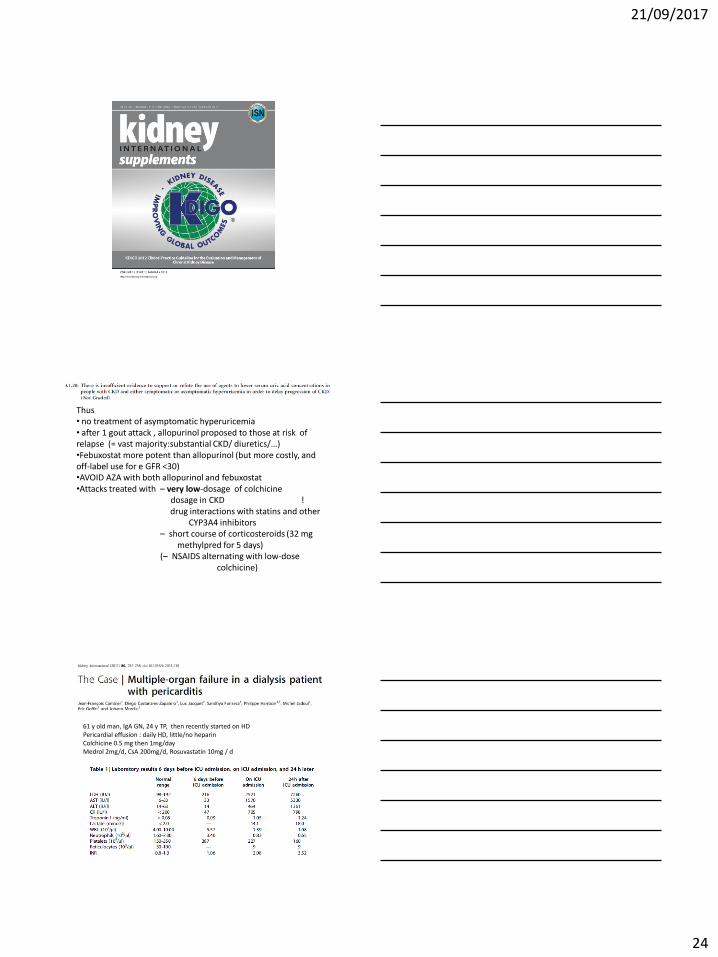
Thus • no treatment of asymptomatic hyperuricemia • after 1 gout attack , allopurinol proposed to those at risk of relapse (= vast majority:substantial CKD/ diuretics/…) •Febuxostat more potent than allopurinol (but more costly, and off-label use for e GFR <30) •AVOID AZA with both allopurinol and febuxostat •Attacks treated with – very low-dosage of colchicine dosage in CKD ! drug interactions with statins and other CYP3A4 inhibitors – short course of corticosteroids (32 mg methylpred for 5 days) (– NSAIDS alternating with low-dose colchicine)
61 y old man, IgA GN, 24 y TP, then recently started on HD Pericardial effusion : daily HD, little/no heparin Colchicine 0.5 mg then 1mg/day Medrol 2mg/d, CsA 200mg/d, Rosuvastatin 10mg / d
21/09/2017
25
Refractory shock … and death
Colchicine largely eliminated by the liver, somewhat by kidney Metabolism inhibited by some CCB, CNI, antifungals, macrolides , some statins ….. Here CsA + rosuvastatin + colchicine for some weeks = deadly combination Thus use lowest possible colchicine dosage, for very short period and beware of drug interactions
Drug dosage in CKDDrug dosage in CKD
•• StartingStarting dosagedosage
** aimaim: : therapeutictherapeutic bloodblood levellevel : ex. : ex. vancomycinvancomycin
** functionfunction of distribution volume of distribution volume (V , or (V , or weightweight and and drugdrug distribution distribution bloodblood/tissues)/tissues)
** thusthus normal in CKD (or normal in CKD (or eveneven increasedincreased if if oedemaoedema +++)+++)
•• Maintenance dosage Maintenance dosage
** eliminatedeliminated by by liverliver : : littlelittle or no change or no change ((metabolitesmetabolites !) !)
** eliminatedeliminated by by kidneykidney : : increaseincrease intervalinterval or or reducereduce dosagedosage
Drug dosage in CKD (II)Drug dosage in CKD (II)
21/09/2017
26
Maintenance dosage unchanged in CKD
•• CalciumCalcium--channelchannel blockersblockers , , metoprololmetoprolol
•• Nitrates Nitrates
•• Standard (Standard (unfractionatedunfractionated) ) heparinheparin, AVK, AVK
•• ClonidineClonidine, , guanfacineguanfacine, , moxonidinemoxonidine
•• DoxycyclineDoxycycline, , oxacillineoxacilline, , rifampicinrifampicin
•• StatinsStatins
•• PPIPPI
•• CorticosteroidsCorticosteroids , all«, all« steroidssteroids » » (OP,…)(OP,…)
•• cyclosporine, cyclosporine, tacrolimustacrolimus
Maintenance dosage reduced in CKD
•• SotatolSotatol :class III :class III effecteffect, QT , QT prologationprologation, , suddensudden deathdeath!!
•• LMW LMW heparinsheparins
•• ColchicineColchicine
•• Allopurinol Allopurinol
•• MethotrexateMethotrexate……
•• Lithium …Lithium …
•• Morphine Morphine derivativesderivatives ( ( codeinecodeine, morphine, , morphine, fentanylfentanyl,….),….)
•• DigoxineDigoxine
•• GanciclovirGanciclovir, acyclovir ,…, acyclovir ,…
•• ManyMany othersothers ………………….………………….
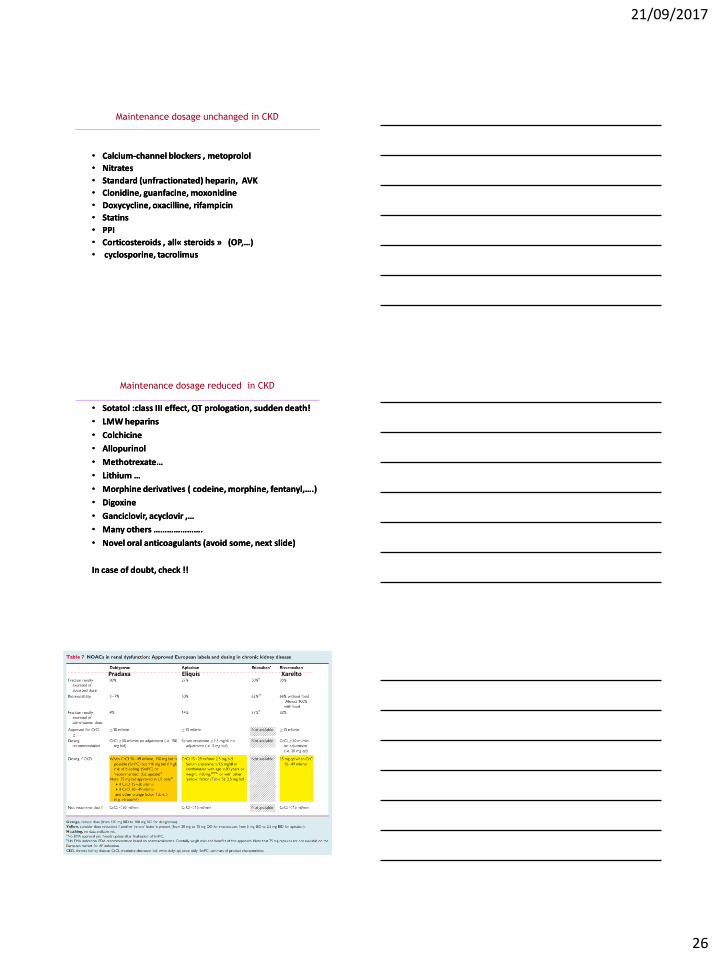
•• NovelNovel oral anticoagulants (oral anticoagulants (avoidavoid somesome, , nextnext slideslide))
In case of In case of doubtdoubt, check !!, check !!
Pradaxa Eliquis Xarelto
21/09/2017
27
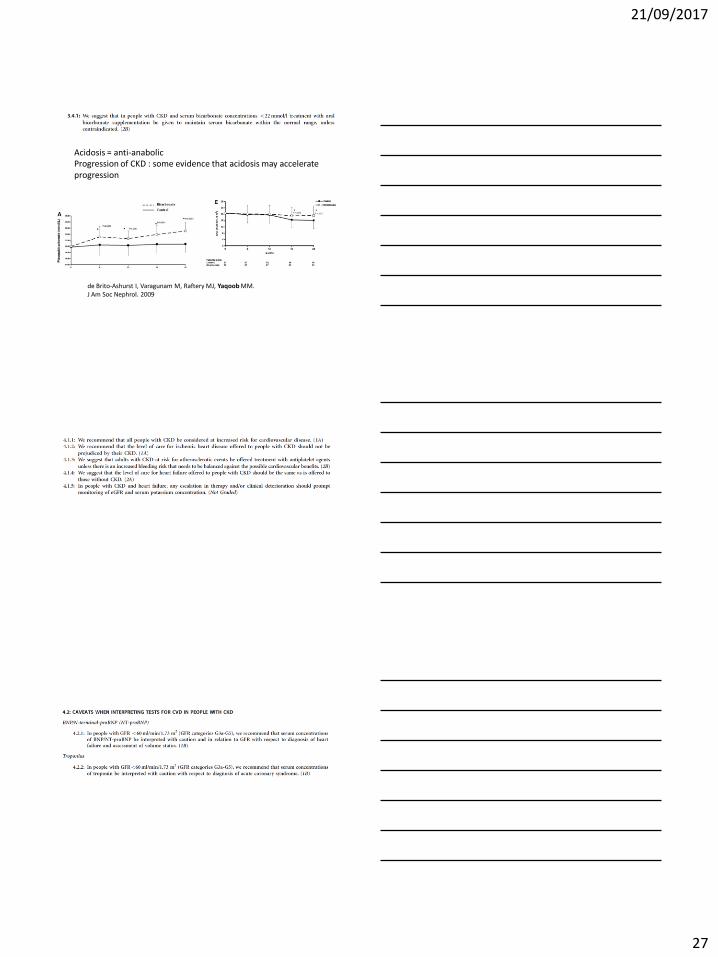
Acidosis = anti-anabolic Progression of CKD : some evidence that acidosis may accelerate progression
de Brito-Ashurst I, Varagunam M, Raftery MJ, Yaqoob MM. J Am Soc Nephrol. 2009
21/09/2017
28
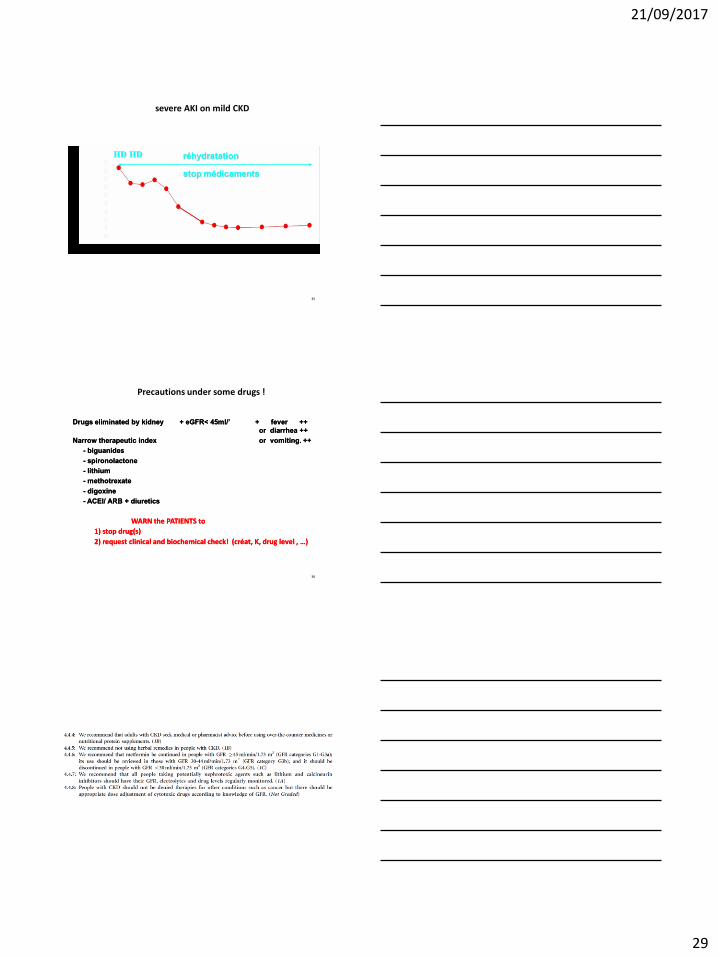
Mrs V - 82 y old type 2 Diabetes II - Hypertension Admitted in emergency room on 26/09/2004 : vomiting- unwell Home treatment: Zestril 20 mg/j, Aldactazine 1/j, Glucophage 850 mg 2/j, Selozok 100 mg/j, Glurenorm 3/j
Clinically : BP 120/80, dehydrated
Bio: pH 7.06
Bicarbonate: 6, Lactate: 7.7 (nl < 1.3)
K: 8.4
urée: 164
créat.: 8.4
Hb: 10.7
34
21/09/2017
29
severe AKI on mild CKD
35
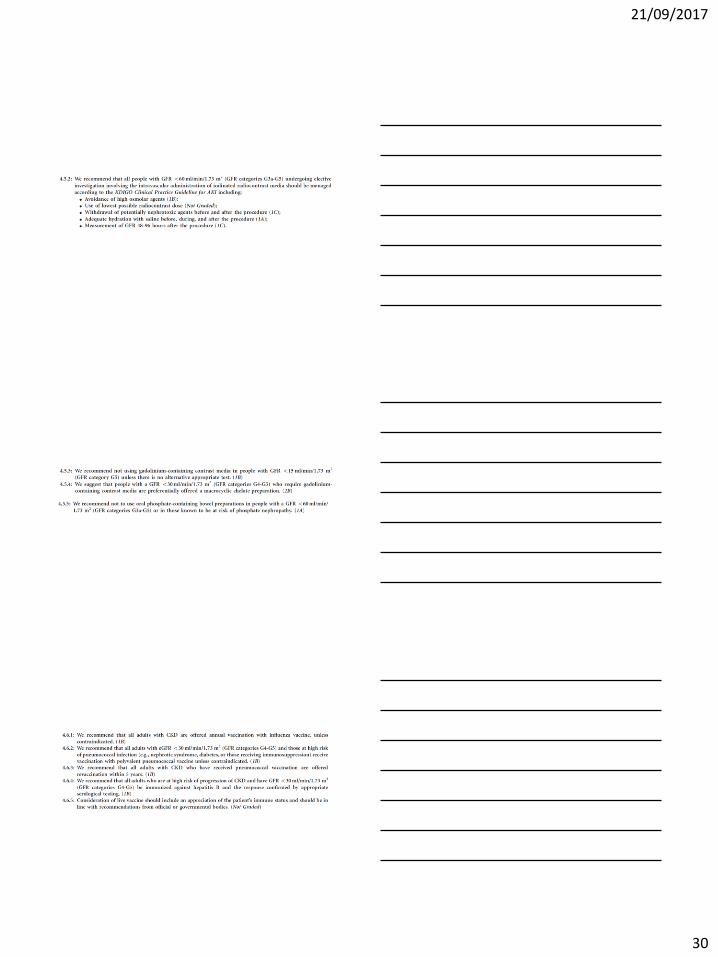
WARN the PATIENTS to WARN the PATIENTS to
1) stop drug(s)1) stop drug(s)
22) request clinical ) request clinical and biochemical check! (and biochemical check! (créatcréat, K, drug level , …), K, drug level , …)
Drugs eliminated by kidneyDrugs eliminated by kidney + + eGFReGFR< 45ml/’ + fever ++ < 45ml/’ + fever ++
or or diarrheadiarrhea ++++
Narrow therapeutic indexNarrow therapeutic index or vomiting. or vomiting. ++++
-- biguanidesbiguanides
-- spironolactonespironolactone
-- lithiumlithium
-- methotrexatemethotrexate
-- digoxinedigoxine
-- ACEI/ ARB + diureticsACEI/ ARB + diuretics
Precautions under some drugs !
36
21/09/2017
30
21/09/2017
31
21/09/2017
32
« End-stage » or « terminal » renal disease
• Does not equal to (quasi)- death sentence
• Human species is adaptative
• Anxiety will usually be reduced by adequate information, rather than increased
• Any patient with advanced CKD knows about a single patient, very sick, who died rapidly after dialysis start
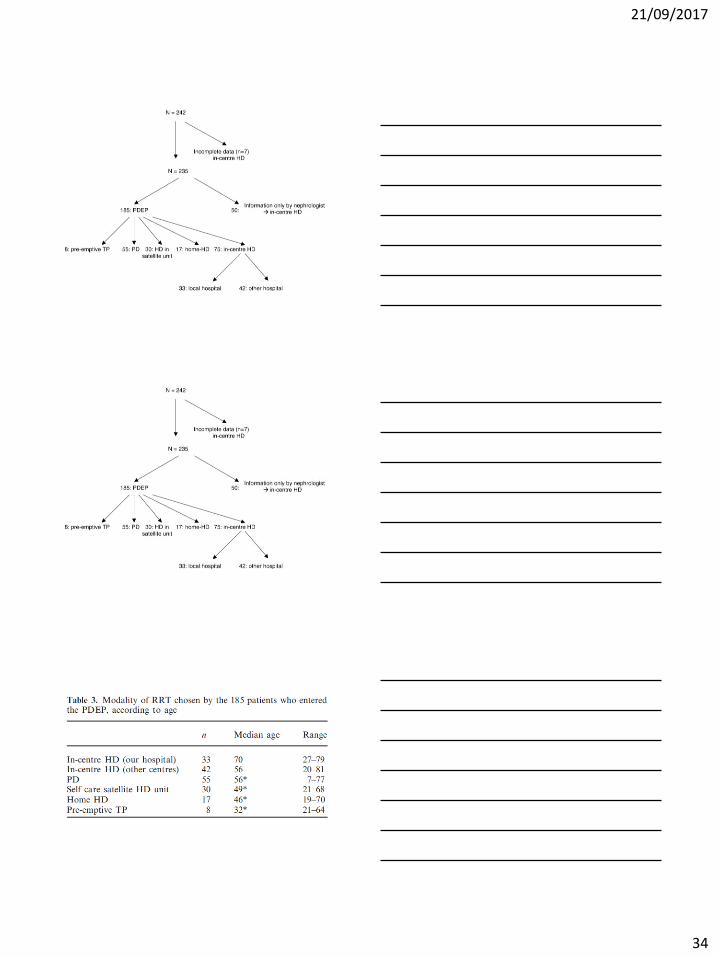
ESRD treatment Modalities
• Transplantation, including preemptive , both living and deceased -donor
• Haemodialysis – In-centre – Self care satellite (1984) – Home HD (1970) , with partner or solo or with
nurse ( partly reimbursed 2003) – Satellite non-self care (2006, 2012)
• PD (1978) – CAPD – APD
• Conservative treatment
PDEP Programme (1)
• Nephrologist initiates discussion and briefly (30 minutes) explains the various RRT modalities
• Suggests appointment with self-care team
• Indicates which modalities are “reasonable” in the particular patient (written form)
e.g. Crohn’s disease and extensive abdominal surgery : no PD
21/09/2017
33
PDEP Programme (2)
• Information provided by nurses in charge of self-care dialysis (median >20 years in unit)
• Individual (preferably with family)
• In-house Video with further details on modalities and videos of patients on all modalities
• Questions/answers : job, timing, eating, sleeping, holidays, travelling, sexual,...
PDEP Programme (3)
• Next outpatient nephrology clinic : further discussion with nephrologist
• Brochures
• Contact with experienced patients
• Sometimes video and Q/A second time with team
( repeating = important)
• Should be started early enough (slope of eGFR), human brain complex , and opinions may change
• Preference(s) of patient crucial ! (except gross CI)
• Adherence to treatment better if “self- choice “
Experience 1994-2000
21/09/2017
34
21/09/2017
35
CLINIQUES UNIVERSITAIRES SAINT-LUC 104
Khosla S and Melton L. N Engl J Med 2007;356:2293-2300
Lifestyle Measures Recommended for Patients with Osteopenia
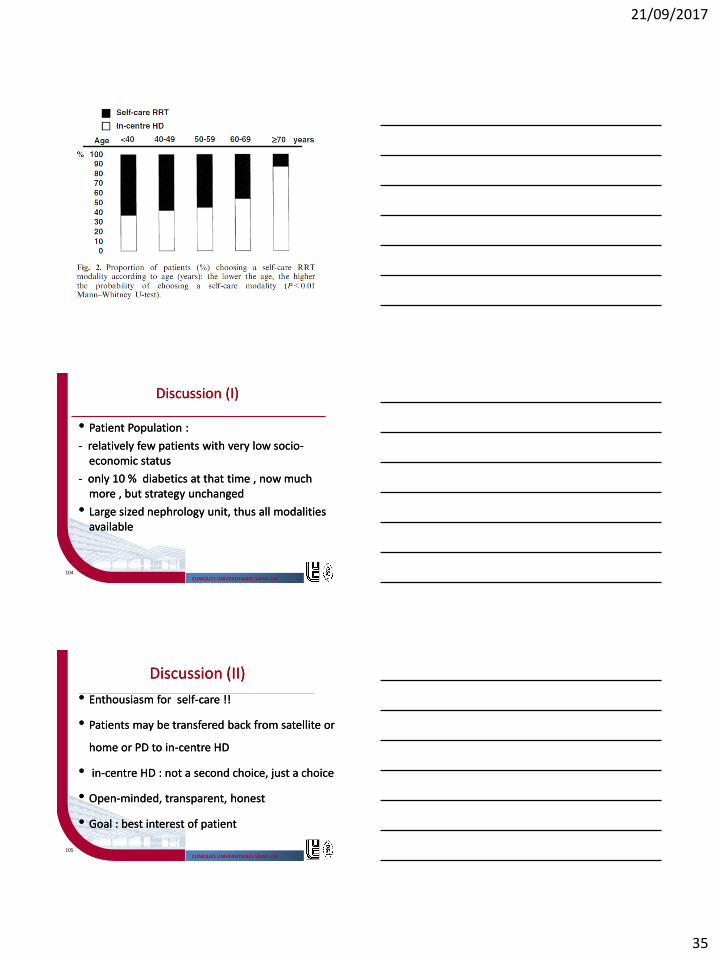
Discussion (I)Discussion (I)
•• Patient Population :Patient Population :
-- relatively few patients with very low sociorelatively few patients with very low socio--economic status economic status
-- only 10 % diabetics at that time , now much only 10 % diabetics at that time , now much more , but strategy unchanged more , but strategy unchanged
•• Large sized nephrology unit, thus all modalities Large sized nephrology unit, thus all modalities availableavailable
CLINIQUES UNIVERSITAIRES SAINT-LUC 105
Khosla S and Melton L. N Engl J Med 2007;356:2293-2300
Lifestyle Measures Recommended for Patients with Osteopenia
Discussion (II)Discussion (II)
•• EnthousiasmEnthousiasm for selffor self--care !!care !!
•• Patients may be Patients may be transferedtransfered back from satellite or back from satellite or
home or PD to inhome or PD to in--centre HDcentre HD
•• inin--centre HD : not a second choice, just a choicecentre HD : not a second choice, just a choice
•• OpenOpen--minded, transparent, honest minded, transparent, honest
•• Goal : best interest of patient Goal : best interest of patient
21/09/2017
36
CLINIQUES UNIVERSITAIRES SAINT-LUC 106
Khosla S and Melton L. N Engl J Med 2007;356:2293-2300
Lifestyle Measures Recommended for Patients with Osteopenia
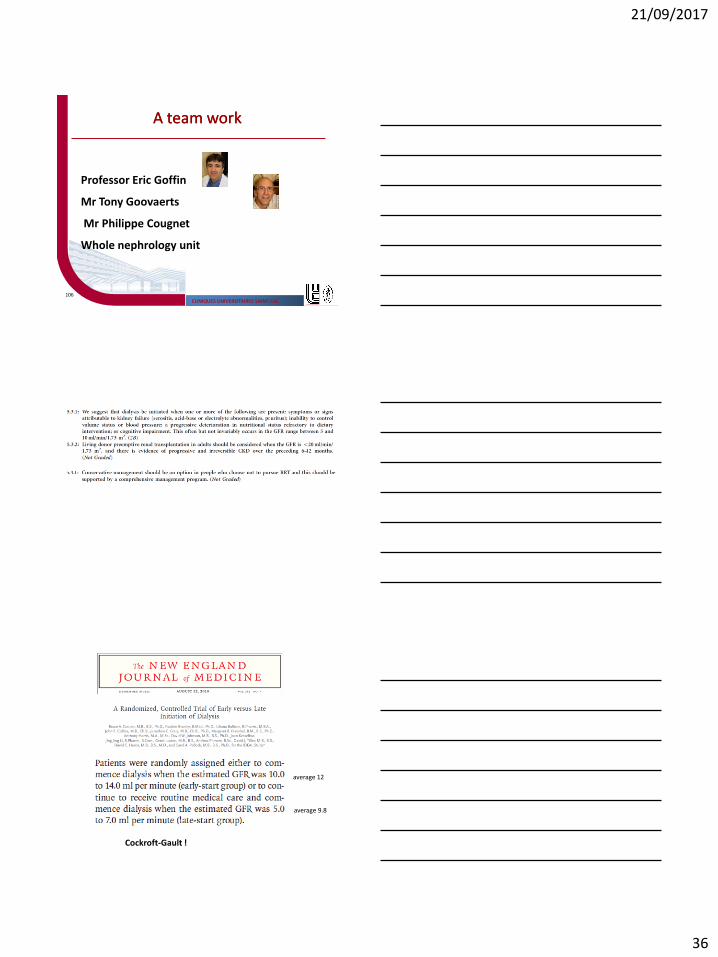
A team workA team work
Professor Eric Goffin
Mr Tony Goovaerts
Mr Philippe Cougnet
Whole nephrology unit
average 12
average 9.8
Cockroft-Gault !
21/09/2017
37
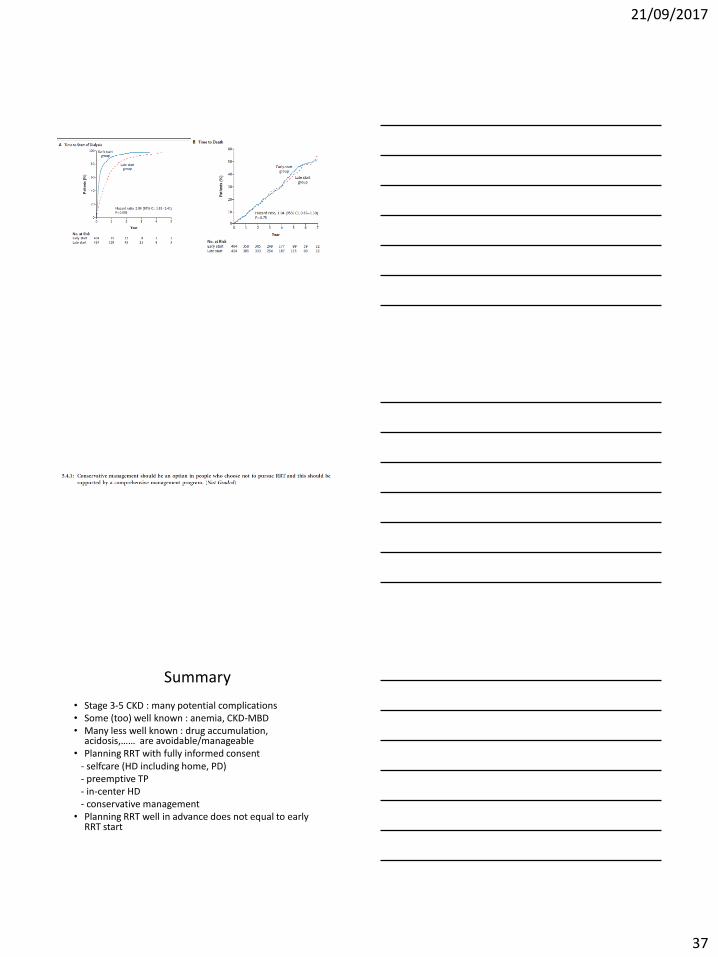
Summary
• Stage 3-5 CKD : many potential complications • Some (too) well known : anemia, CKD-MBD • Many less well known : drug accumulation,
acidosis,…… are avoidable/manageable • Planning RRT with fully informed consent - selfcare (HD including home, PD) - preemptive TP - in-center HD - conservative management • Planning RRT well in advance does not equal to early
RRT start





























