Embed Size (px)
Citation preview

At age 23, this medical student presented with a multicystic mass in the right ovary. The patient had
an apparently unrelated clinical history of tumours in other organs
Case

RSO MacroscopyMulticystic ovary 6 X 8 X 6cmCysts varying from 0.3-3cmOcassional solid yellow areaContralateral ovary normal








p53

What is this lesion?
Is it sensu stricto neoplastic?
Multifocal coexisting with normal follicles
Contralateral ovary is normal
Papillary projections, angiogenesis

What is this lesion?
Is it a granulosa cell lesion?:
All cell markers present: InhA, CLRT, dot keratins

Inh A

CAM 5.2

AAT

CAM 5.2
Calretinin
Inhibin
Melan A

What is this lesion?
Can granulosa cells be so atypical ?
Similar atypia can be found in
juvenile granulosa cell tumours


Surprise !!!!!

AGE SITE HISTOLOGIC TYPELOCAL
RECURRENCE
METAST. TREATMENT
10 Lt tibia Telangiectatic Osteosarcoma 6 months Pulmonar
yAmputation andchemotherapy
15 Lt breast Fibroadenoma - - Local excision
18 Bothbreasts
Rt.Malignant Phyllodes tumour
Lt. Phyllodes tumour3 & 5 years -
Extensive local excision followed
by bilateral mastectomy at
25yrs
21 Skin (nose) Reticulohistiocytoma Local excision
23 Lt breast Intraductal Carcinoma - - Local excision
23 RT OVARY
GRANULOSA CELL LESION - - RSO

Possibility of mutational syndrome ??
Li-Fraumeni syndrome ?
Clinical considerations

Autosomal dominant familial disorderMultiple primary neoplasmsYoung patients < 45 yrs70% germline mutation of exons 5-8 of p53

Associations (usual):Sarcomas Breast CancerCNS tumoursAdrenocortical CarcinomaLeukaemia
Li-Fraumeni Syndrome

Patient’s Blood:P53 gene mutation @ exon 10 [exons
5-8 no change] T insertion in codon 336 (ATG to TAT) generating a stop codon in the oligomerization domain of the protein (E336X).
Genetic analysis

E336X
P53
E336XE336X

Family: (Parents, 2 siblings, uncle): P53 gene normal
Tumour tissue: T insertion (ATG to TAT) in codon 237 of exon 7
Genetic analysis

Multifocal intrafollicular granulosa
cell tumor of the ovary associated
with an unusual exon 10, codon 336
[non familial] germline p53 mutation
Case 2 Diagnosis


F o l l o w u p

24 Retroperit. Well differentiated Liposarcoma - - Local excision
24 Rt breast Invasive ductal Carcinoma
3 axillary nodes
Rt mastectomy and axillary dissection
25 Myometrium Leiomyomas - - TAH-LSO
25 Endometrium
Intramucosal endometrioid
adenocarcinoma with atypical hyperplasia
- - TAH-LSO
AGE SITE HISTOLOGIC TYPELOCAL
RECURRENCE
METASTAST. TREATMENT

25 Iliac bone. Leiomyosarcoma - - Biopsy
AGE SITE HISTOLOGIC TYPELOCAL
RECURRENCE
METASTAST. TREATMENT


In childhood malignant adrenocortical tumor where a similar mutation occurs in the same dimerization domain of TP53, exon 10 codon 337, an altered apoptotic function may be responsible for tumorigenesis. Varley et al, 2003

Epithelial ovarian Ca.Teratoma, YST, DysgerminomaEndometrial CaCervical CaLeiomyomas
Li-Fraumeni Syndrome and the female genital
tract
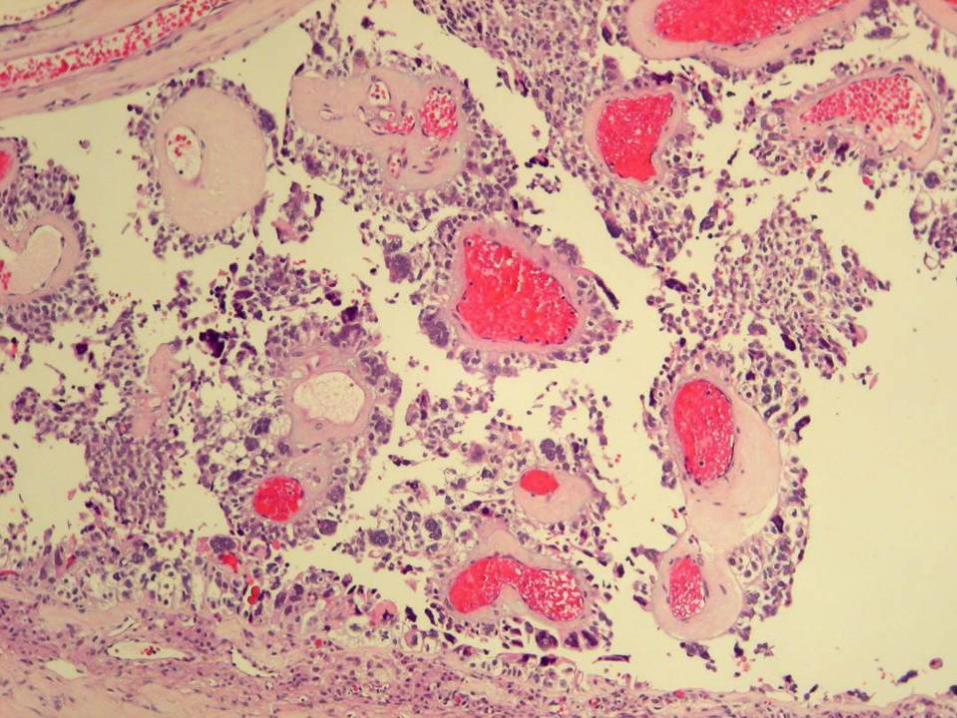
Exon 10 mutation most unusual
Cellular appearance of the previous mesenchymal
tumours was identical (atypia, globules: continuum?)
Li Fraumeni Syndrome does not include any sex
cord stromal tumours of the ovary
Granulosa Cell Tu. are asociated with mesenchymal
tumours (Ollier, Mafucci, etc....)
Pertinent questions

6 year old girlMultiple right side
enchondromas in phalanxes, scapula, pelvis, femur, tibia, tarsal bones
Spontaneous fracture in femur
Vaginal bleeding Precocious pseudopuberty 12cm right ovarian tumour
Ollier’s Disease associated to JGCT
Velasco et al, Cancer 62:222-225; 1988

Case has typical clinical presentation of a full blown LFS
In LFS there is usually a relationship between the type of mutation (mutational genotype) and the number and type of cancers and age of presentation (tumor phenotype)
Childhood malignant adrenocortical tumor is characteristically associated with LFS and usually involves mutations at exon 10 at “hot spot” 337 only. Here mutation was at codon 336
Mutation occurred in a domain which is characteristically related to the childhood malignant adrenocortical tumor reported in Brazilian children with LFS, a neoplasm with which it shares a common embryogenesis.
More pertinent questions
Velasco A, Alonso A, Blanco A, Nogales FF. Ollier's disease associated with ovarian juvenile granulosa cell tumor. Report of a case and literature review. Cancer 1988; 62:222-225.
Kleihues P et al. Tumors associated with p53 germline mutations. A synopsis of 91 families. Am J. Pathol 150:1-13, 1997
Varley JM et al. Are there low-penetrance TP53 Alleles? evidence from childhood adrenocortical tumors. Am J Hum Genet 1999;55:995-1006
Ribeiro RC, et al . An inherited p53 mutation that contributes in a tissue-specific manner to pediatric adrenal cortical carcinoma. PNAS 2001;98:9330-9335
Varley JM. Germline TP53 mutations and Li-Fraumeni syndrome. Hum Mutat 2003;21:313-320.
www.iarc.fr/P53/Germline.html
References



![The Ovary of the Teleost Fish Xenotoca Eiseni (Goodeidae ... · the ovary, called a gonoduct, connects the ovary to the exterior by a gonopore [7]. These unique features of the ovary](https://img.pdfslide.us/doc/110x75/5f5082c1c1cb78272c63e522/the-ovary-of-the-teleost-fish-xenotoca-eiseni-goodeidae-the-ovary-called-a.jpg)