Embed Size (px)
Citation preview
Prof. Dr. /
Khaled ElhayesPREPROSTHETIC
SURGERY
Prof. Dr.
Khaled Atef Elhayes Prof. Oral Maxillofacial Surgery
Faculty of Oral & Dental Medicine
Cairo University
4th Year
Prof.
Dr.
/ Kha
led E
lhaye
s
Definition: It’s corrective and preventive operations performed before denture construction andplacement to create proper support, stability and retention for prosthetic appliance.
* Ideal requirement for edentulous ridge:1- Adequate bone support: No v-shape ridge (should be U-shape). No sharp edge No bone irregularities. No bony undercuts No bony exostosis.
2- Adequate keratinized attached mucosal coverage: No flabby ridge. No hypertrophy. Adequate Vestibular depth. No high frenum or muscle attachment. No scar bands. No ulceration.
3- Good relationship between maxilla & mandible in antero-posterior, transverse andvertical dimensions.
4- Offering protection to neurovascular bundle*and sinus.
5- Freedom from pathosis.
* Objectives (Aim) of Preprosthetic surgery:1. Restore normal masticatory function.2. Restore esthetics.3. Restore ideal bone support with broad ridge form.4. Adequate palatal vault form.5. Restore Proper S.T support.6. Adequate vestibular depth.7. Restore proper inter-arch relation ship.8. Offering protection to neurovascular bundle.9. Remove any pathosis.
Factors affecting bone resorption:1- Local factors:a. Long standing denture wearing. b. Traumac. Previous dento-alveolar surgery.
PreProsthetIC s U r G e ry
1
Prof. D
r. / K
haled
Elha
yes
(42) — CHAPTER (3)
2- Systemic factors:a) Hormonal disease: as diabetes mellitus, hyperparathyroidism.b) Osteoporosis.c) Nutritional deficiency.
*Complications of Edentulous Bone Loss:1. Effect on bone
Loss of alveolar bone. Loss of basal bone and increase risk of basal bone fracture.
2. Effect on soft tissue Hypertrophy and flabby ridge High ms. Attachment and Decrease sulcus depth.
3. Increase inter-arch relation ship.4. ↓ Denture retention and stability 5. ↑ Patient discomfort.
Preoverative Patient EvaluationI- History:
• Chief complaint.• Patient Esthetic and functional goals .• Patient expectation of surgical ttt.• Psychological adaptability toward P.D and C.D.
II- Clinical examination (Intra-oral or Extra-oral):• Bony tissue (ridge hight, width and contour).• Soft tissue: quality, flabby ridge, scars,….etc.• Vestibular depth and ms attachment.• Inter-arch relationships.• Existing teeth relations..
III- Radiographic Examination:By panorama to denote:
• Pathological lesions• Remaining roots.• Impactions.• Pathosis.• Pneumatization of the sinus.
2
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (43)
IV- Laboratory investigation:• Blood sugar level.• Parathyroid hormones.• Serum calcium and phosphate levels.• Alkaline phosphatase enzyme.
Classifications of surgical procedures
I. Preventive surgical procedures:1. Routine measures during extraction2. Alveoloplasty Vs alveolotomy and alveolectomy.
II. Corrective surgical procedures: A) hard tissue abnormality:1- Torus palatinus.2. Torus mandibularis.3. Bony enlarged maxillary tuberosity.4- Mylohyoid ridge (lingual balcony).5- Bony prominence and bony undercuts.6- Correction of knife edge ridge.
B) soft tissue abnormality: 1- Labial frenum2- Lingual frenum.3- Fibrous enlarged Maxillary tuberosity.4- Flabby ridge.5- Denture fissuratum.6- Inflammatory papillary hyperplasia of the palate. C) Surgical correction of flat ridge:1- Relative ridge hightening (vestibuloplasty).
Submucosal vestibuloplasty.Secondary epithalization vestibuloplasty.Grafted vestibuloplasty.
2-Absolute ridge hightening ( ridge augmentation).3
Prof. D
r. / K
haled
Elha
yes
(44) — CHAPTER (3)
I. Preventive surgical procedures:
1. Routine measures during extraction:Aim: promote healing and preserve shape of alveolar ridge.
• Treat any gingival inflammation before extraction. Remove any projecting interseptal bone . Remove loose pieces of alveolar bone. Squeeze the bony socket to avoid undercuts and for better healing. Loosely tied suture if necessary
2. Alveoloplasty:Definitions:Alveoloplasty: It’s surgical contouring of alveolar ridge.Alveolotomy: it’s cutting into the alveolar process.
e.g. during removal of remaining root, cyst,……Alveolectomy: it’s complete surgical excision of alveolar bonee.g. neoplasm or radiotherapy.
Indications: Remove bone irregularities or undercutsTechniques:
A- Recontouring of rough and sharp bone edges
1. Paraperiosteal infiltration anesthesia.2. crestal incision using BP blade NO.15.3. Reflection of mucoperisosteum using mucoperiosteal elevator.4. Trimming sharp bony edges using bone rongeur.5. Filing & irrigation.6. Remove excess soft tissue.7. Suturing. (interrupted suture)
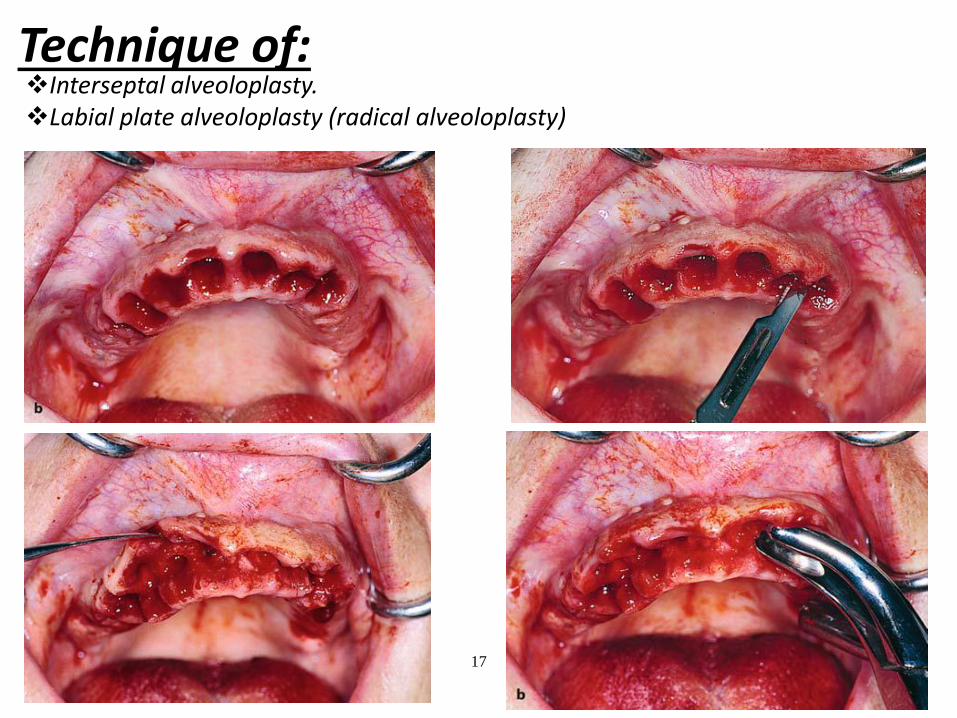
B- Alveloplasty for multiple teeth extraction:i- Interseptal alveoloplasty1. L.A.2. Gingival incision around the teeth (vertical releasing incisions may be used)3. Reflection of mucoperisosteum using mucoperiosteal elevator.
4
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (45)
4. Teeth extraction.5. Cutting interseptal bone by rongeur.6. bony groove may be done in the labial plate followed by green stick fracture to
yield labial plate toward the lingual plate by compression 7. Filing & irrigation.8. Remove excess soft tissue.9. Suturing (interrupted suture)
ii- Labial plate alveoloplasty (radical alveoloplasty):Indication: maxillary prognathism
Technique:1. Paraperiosteal infiltration anesthesia.2. Gingival incision extending one tooth distal 3. on either sides using lancet NO.15.4. Reflection of mucoperisosteum using mucoperiosteal elevator.5. Teeth extraction.6. Cutting labial plate of bone and interseptal bone using bone rongeur.7. Trimming of the palatal bone and beveling is done.8. Filing & irrigation.9. Remove excess soft tissue.10. suturing ( interrupted suture)11. Now labial mucoperiosteum rests on palatal bone.
5
Prof. D
r. / K
haled
Elha
yes
(46) — CHAPTER (3)
II. Corrective surgical procedures:
A) Hard tissue abnormality:
Exostoses
Exostoses are generally bony protuberances, which develop in various areas of the jaw. They are not considered real neoplasms, but dysplastic exophytic lesions. The etiology of these lesions remains unknown, even though evidence suggests that genetic and environmental factors determine their development. Exostoses are classified into three types: (1) torus palatinus, (2) torus mandibularis, and (3) multiple exostoses.
Torus Palatinus
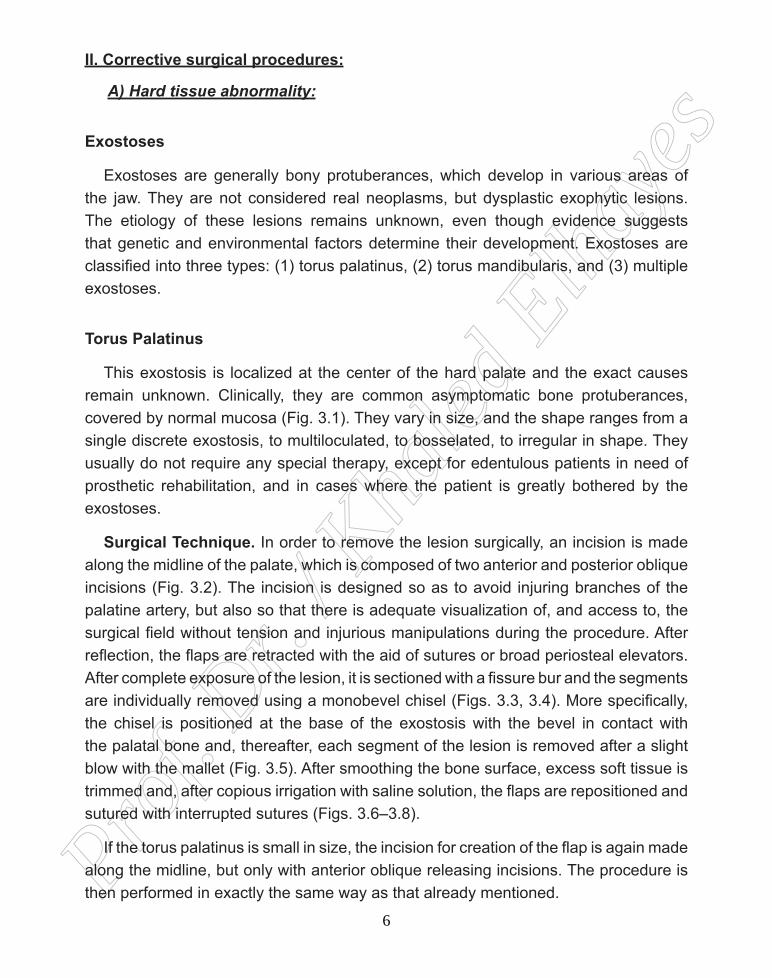
This exostosis is localized at the center of the hard palate and the exact causes remain unknown. Clinically, they are common asymptomatic bone protuberances, covered by normal mucosa (Fig. 3.1). They vary in size, and the shape ranges from a single discrete exostosis, to multiloculated, to bosselated, to irregular in shape. They usually do not require any special therapy, except for edentulous patients in need of prosthetic rehabilitation, and in cases where the patient is greatly bothered by the exostoses.
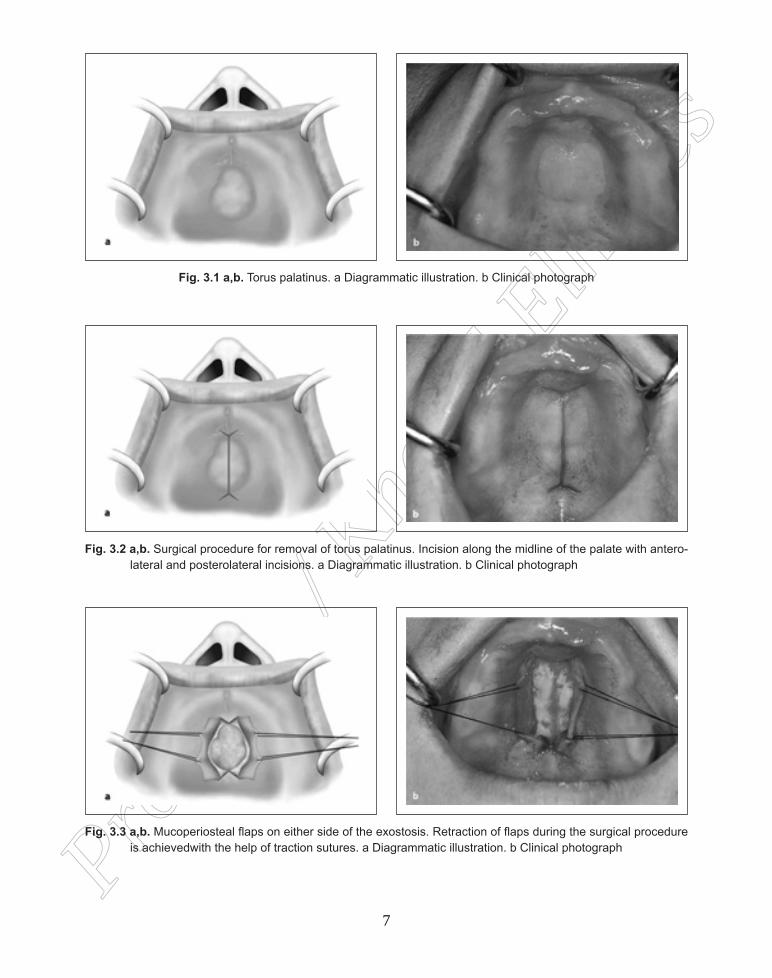
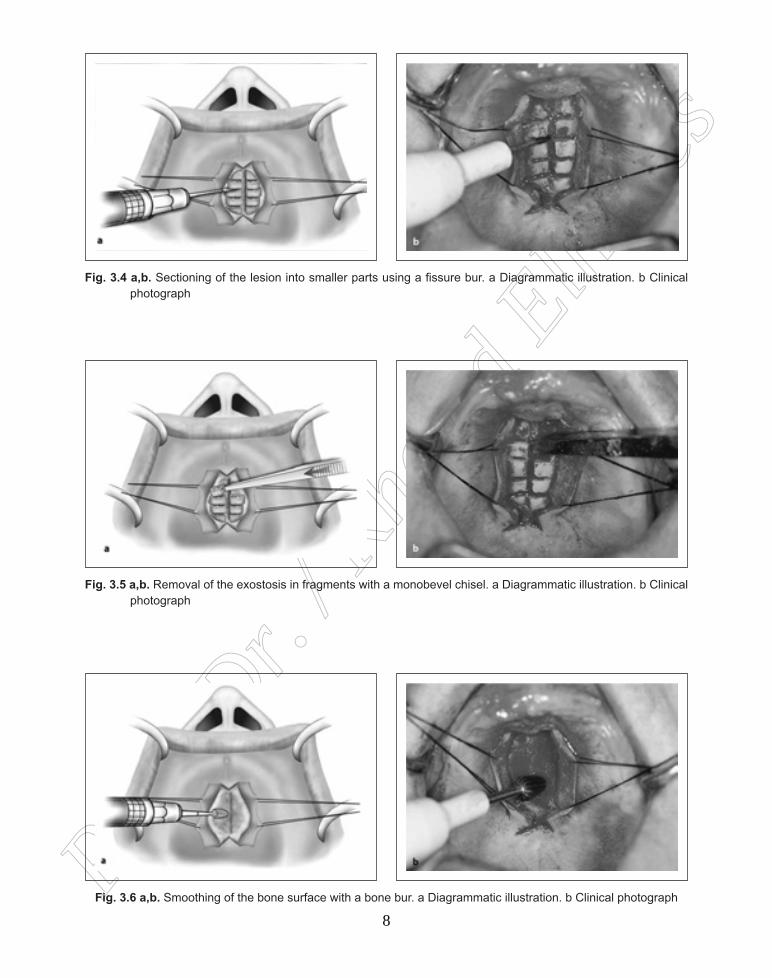
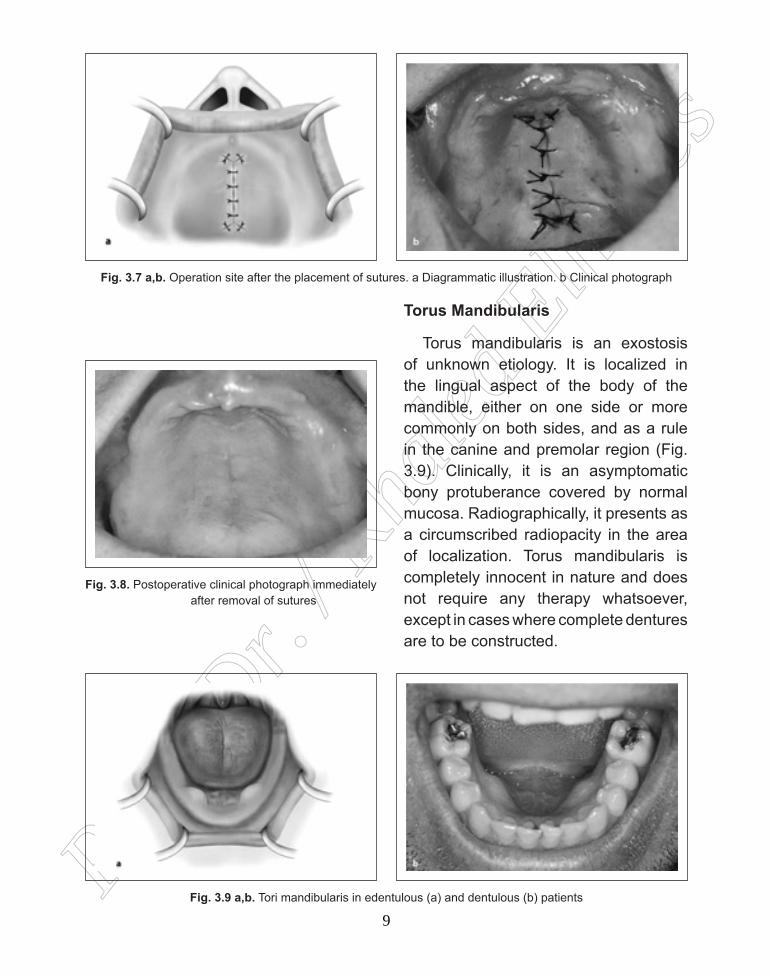
Surgical Technique. In order to remove the lesion surgically, an incision is made along the midline of the palate, which is composed of two anterior and posterior oblique incisions (Fig. 3.2). The incision is designed so as to avoid injuring branches of the palatine artery, but also so that there is adequate visualization of, and access to, the surgical field without tension and injurious manipulations during the procedure. After reflection, the flaps are retracted with the aid of sutures or broad periosteal elevators. After complete exposure of the lesion, it is sectioned with a fissure bur and the segments are individually removed using a monobevel chisel (Figs. 3.3, 3.4). More specifically, the chisel is positioned at the base of the exostosis with the bevel in contact with the palatal bone and, thereafter, each segment of the lesion is removed after a slight blow with the mallet (Fig. 3.5). After smoothing the bone surface, excess soft tissue is trimmed and, after copious irrigation with saline solution, the flaps are repositioned and sutured with interrupted sutures (Figs. 3.6–3.8).
If the torus palatinus is small in size, the incision for creation of the flap is again made along the midline, but only with anterior oblique releasing incisions. The procedure is then performed in exactly the same way as that already mentioned.
6
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (47)
Fig. 3.1 a,b. Torus palatinus. a Diagrammatic illustration. b Clinical photograph
Fig. 3.2 a,b. Surgical procedure for removal of torus palatinus. Incision along the midline of the palate with antero-lateral and posterolateral incisions. a Diagrammatic illustration. b Clinical photograph
Fig. 3.3 a,b. Mucoperiosteal flaps on either side of the exostosis. Retraction of flaps during the surgical procedure is achievedwith the help of traction sutures. a Diagrammatic illustration. b Clinical photograph
7
Prof. D
r. / K
haled
Elha
yes
(48) — CHAPTER (3)
Fig. 3.4 a,b. Sectioning of the lesion into smaller parts using a fissure bur. a Diagrammatic illustration. b Clinical photograph
Fig. 3.5 a,b. Removal of the exostosis in fragments with a monobevel chisel. a Diagrammatic illustration. b Clinical photograph
Fig. 3.6 a,b. Smoothing of the bone surface with a bone bur. a Diagrammatic illustration. b Clinical photograph
8
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (49)
Fig. 3.7 a,b. Operation site after the placement of sutures. a Diagrammatic illustration. b Clinical photograph
Fig. 3.8. Postoperative clinical photograph immediately after removal of sutures
Fig. 3.9 a,b. Tori mandibularis in edentulous (a) and dentulous (b) patients
Torus Mandibularis
Torus mandibularis is an exostosis of unknown etiology. It is localized in the lingual aspect of the body of the mandible, either on one side or more commonly on both sides, and as a rule in the canine and premolar region (Fig. 3.9). Clinically, it is an asymptomatic bony protuberance covered by normal mucosa. Radiographically, it presents as a circumscribed radiopacity in the area of localization. Torus mandibularis is completely innocent in nature and does not require any therapy whatsoever, except in cases where complete dentures are to be constructed.
9
Prof. D
r. / K
haled
Elha
yes
(50) — CHAPTER (3)
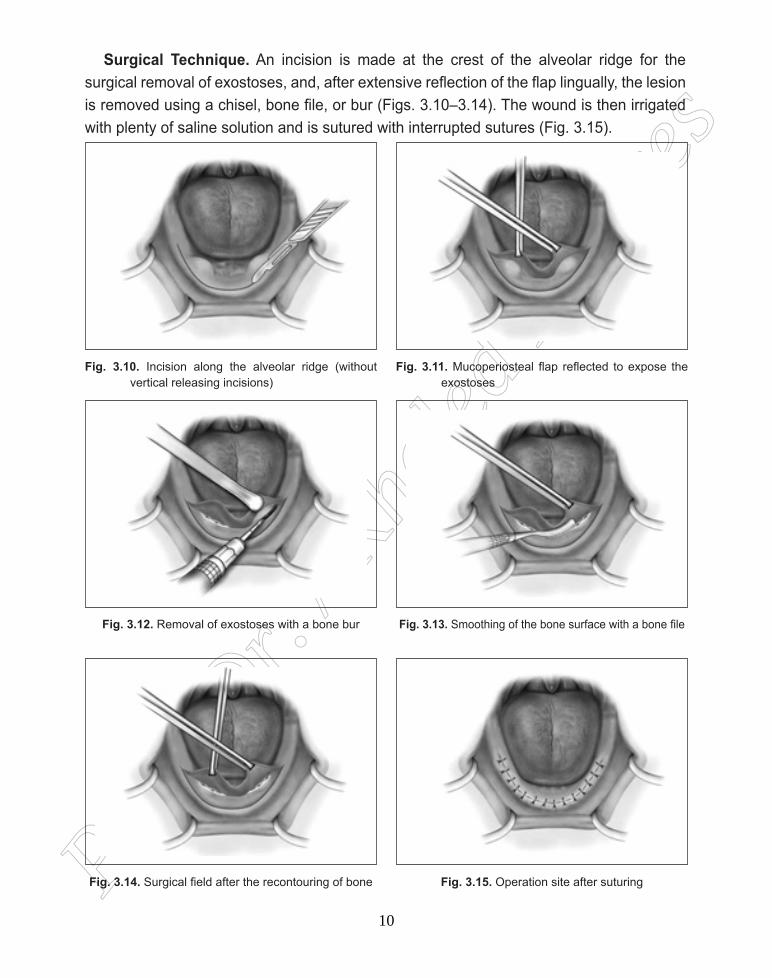
Surgical Technique. An incision is made at the crest of the alveolar ridge for the surgical removal of exostoses, and, after extensive reflection of the flap lingually, the lesion is removed using a chisel, bone file, or bur (Figs. 3.10–3.14). The wound is then irrigated with plenty of saline solution and is sutured with interrupted sutures (Fig. 3.15).
Fig. 3.10. Incision along the alveolar ridge (without vertical releasing incisions)
Fig. 3.12. Removal of exostoses with a bone bur
Fig. 3.14. Surgical field after the recontouring of bone
Fig. 3.11. Mucoperiosteal flap reflected to expose the exostoses
Fig. 3.13. Smoothing of the bone surface with a bone file
Fig. 3.15. Operation site after suturing
10
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (51)
3- Bony enlarged maxillary tuberosity:Tuberosity reduction May be enlarged buccally, palatally or vertically. Unilateral or bilateral. Could be associated with pneumatized sinus.
Indication for removal: 1. If causes injury to the overling soft tissue or coronoid process.2. If interfere with Denture Fittness and retention.3. Encroach inter-arch space and interfere with denture construction..
Technique: Pre-operative radiograph is mandatory to look for sinus floor approximation andpreventing Oro-antral Communication
1. L.A (infiltration buccally and palatally) or Posterior superior alveolar and greater palatine nerve block2. Crestal incision using B.P blade No 15 and incision is extended posterior to tuberosity using B.P blade No 123. Reflection buccally or palatally.4. Bone removal by surgical burs or bone rongeur 5. Filing and irrigation.6. Remove excess tissue.7. Suturing by interrupted or continuous suturing.
4- Mylohyoid ridge reduction “lingual Balcony”- It’s a prominent Internal oblique ridge due to alveolar bone resorption.Indications: 1- Interfere with denture retention and stability due to inadequate denture flange extension2- Soft tissue pain due to denture flange compression.Technique
1- Anesthesia : ( inferior alveolar + lingual nerve block) .2- crestal incision extending from area of 3 → 8.3- Reflection by mucoperiosteal elevator lingually.4- Mylohyooid Muscle is detached by electrosurgery for haemostasis.5- Bone removal using surgical bur & chisel.6- Smoothening of any sharp edges using large bur & irrigation7- Remove excess tissue.8- Suturing 3/0 black silk
11
Prof. D
r. / K
haled
Elha
yes
(52) — CHAPTER (3)
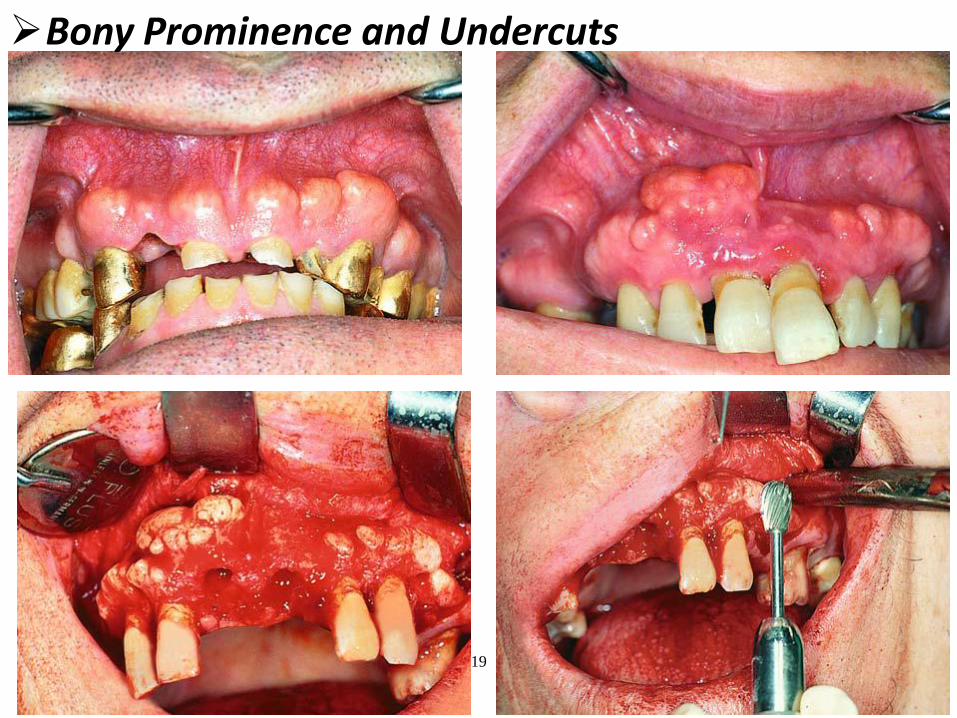
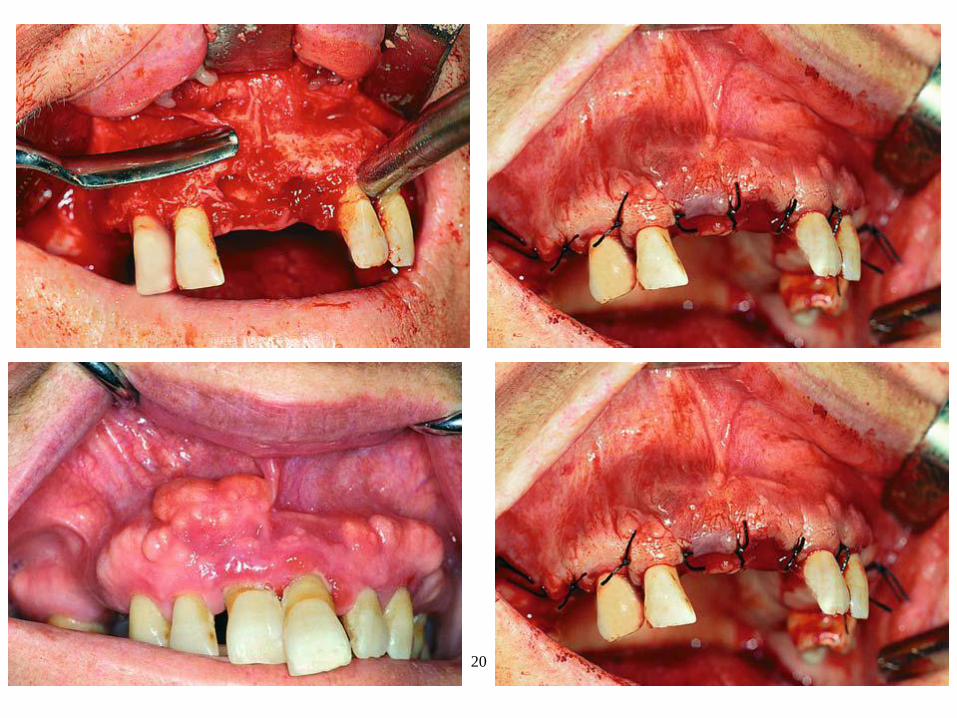
5- Bony prominence and bony undercuts:Indications: a. Causing soft tissue irritation.b. Interfere with denture .Technique:1- LA.2- Crestal incision using B.P blade NO 15.3- Reflection labially and slightly lingually using mucoperiosteal elevator.4- Remove bony prominence by bone rongeur, chisels or surgical burs.5- Filing & irrigation.6- remove excess soft tissue.7- Suturing: interrupted or continuous sutures by 3/0 black silk.
6- Knife-edge ridge: Indication: a. Causing soft tissue irritation.b. interfere with denture seating, retention and stability. Technique:1- Local anesthesia.2- Crestal incision using B.P blade NO 15.3- Reflection labially and slightly lingually using mucoperiosteal elevator.4- Remove bony irregularity by bone rongeur, bone file.5- Filing & irrigation.6- Remove excess soft tissue.7- Suturing by 3/0 black silk.
B) Soft tissue abnormality:
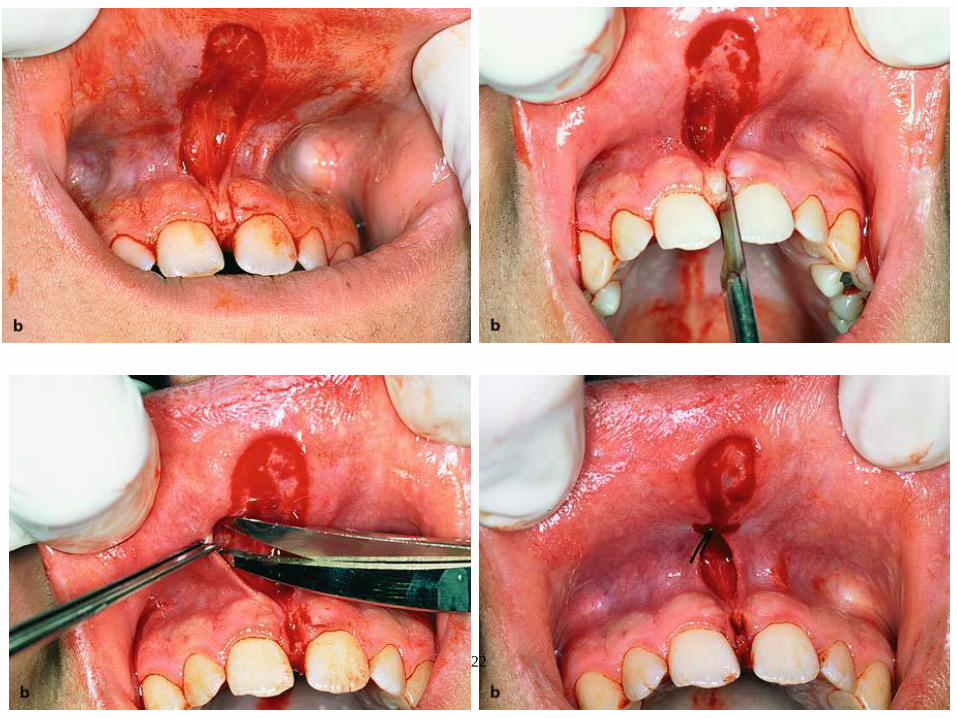
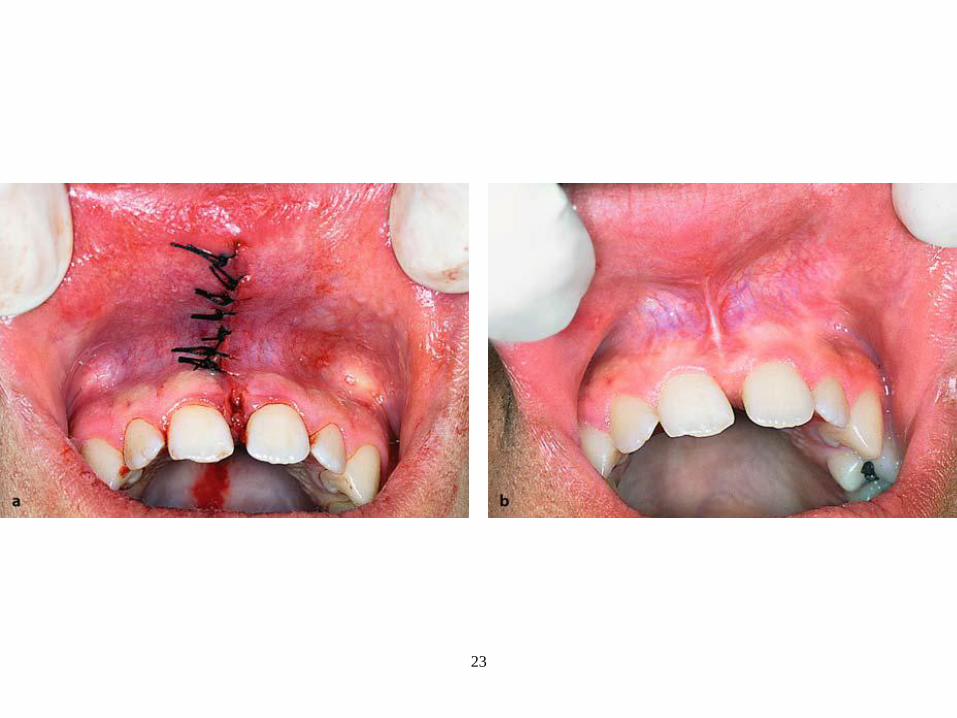
1- labial frenum (labial frenectomy)
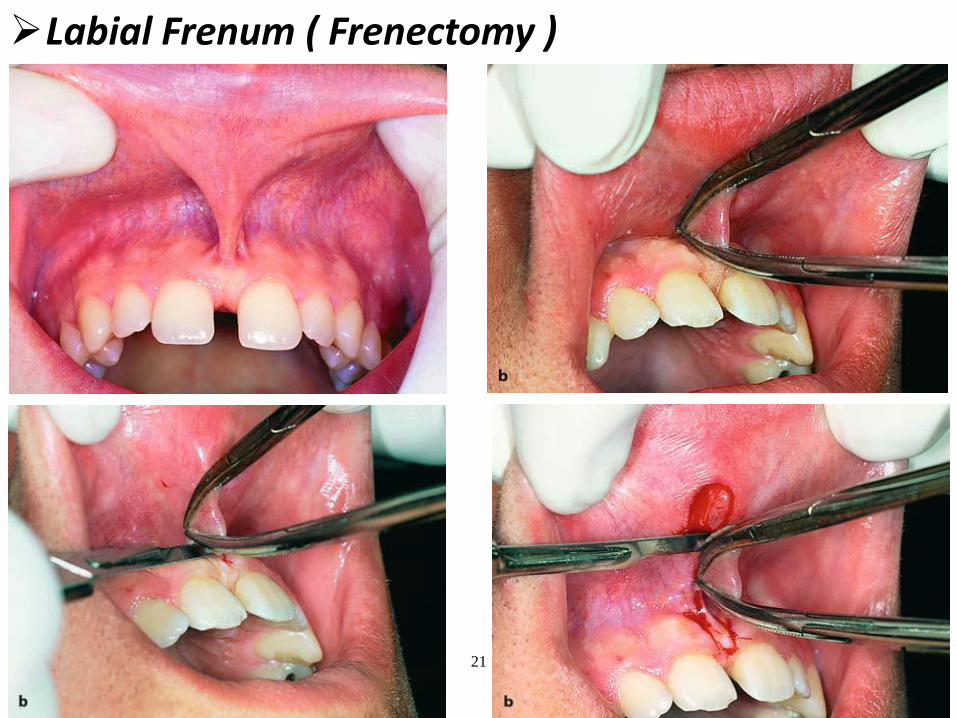
Definitions:Labial frenum: it’s a fibrous C.T band covered with mucosa rarely muscular in nature. It may be attached to alveolar crest of incisive papilla.Frenectomy: it’s Surgical excision of labial Frenum.
Indication:a.interfere with denture retentionb. cause pain and ulceration to S.T c. in case of diastema
12
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (53)
Techniques:1- Sub-mucosal anesthesia. 2- Raise the lip by finger. 3- Grasp the frenum by 2 artery forceps (2 haemostats).
1st // to the lip mucosa up to the mucolabial fold. 2nd // to labial surface of the alveolar Ridge up to the mucolabial fold perpendicular to each other.
4- Incision is done by lancet 11 from outside the haemostatsà diamond shape wound
5- Undermined wound edges. 6- suturing with 3/0 black silk
1st suture pass from the depth of the vestibule to the underlying periosteum interrupted sutures are done fot the rest of incision
7- Surgical pack or dressing could be placed
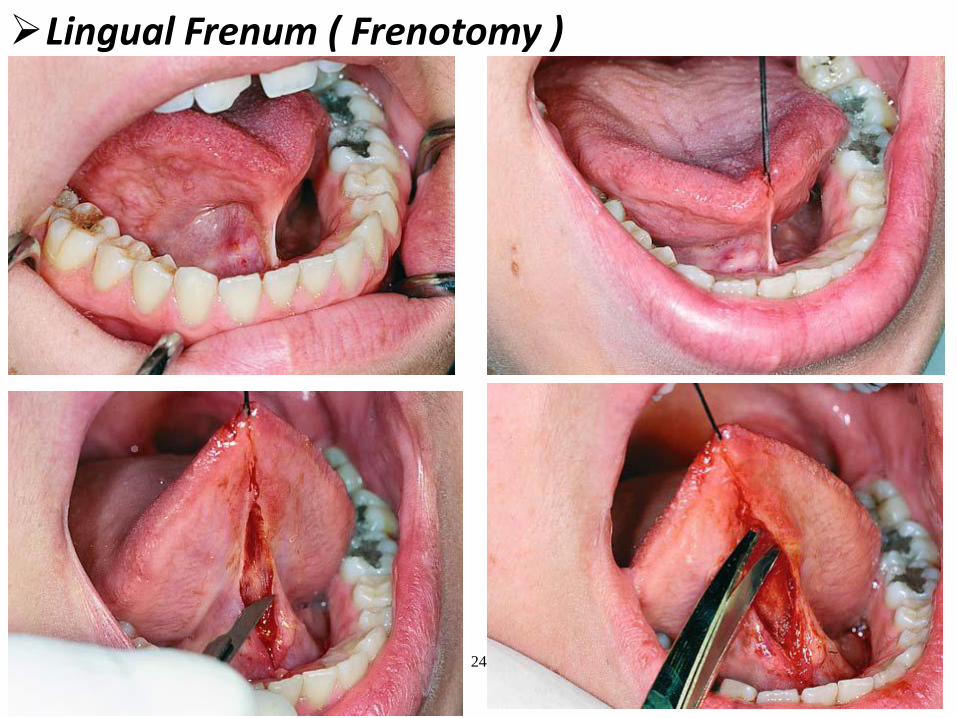
2- lingual frenum (ankyloglossia or tongue tie) “lingual frenotomy or ankylotomy”Definitions: Lingual frenum: it’s mucosal fold rarely muscular in nature.Ankyloglossia: it’s a congenital condition where the lingual frenum is very short or
attached to tip of the tongue. May be partial or complete.Ankylotomy: it’s the surgical excision of ling. Frenum.
Indications:a. Interfere with denture retention.b. Periodontal problems due to inability to clean foods.c. Interfere with tongue movement& speech.
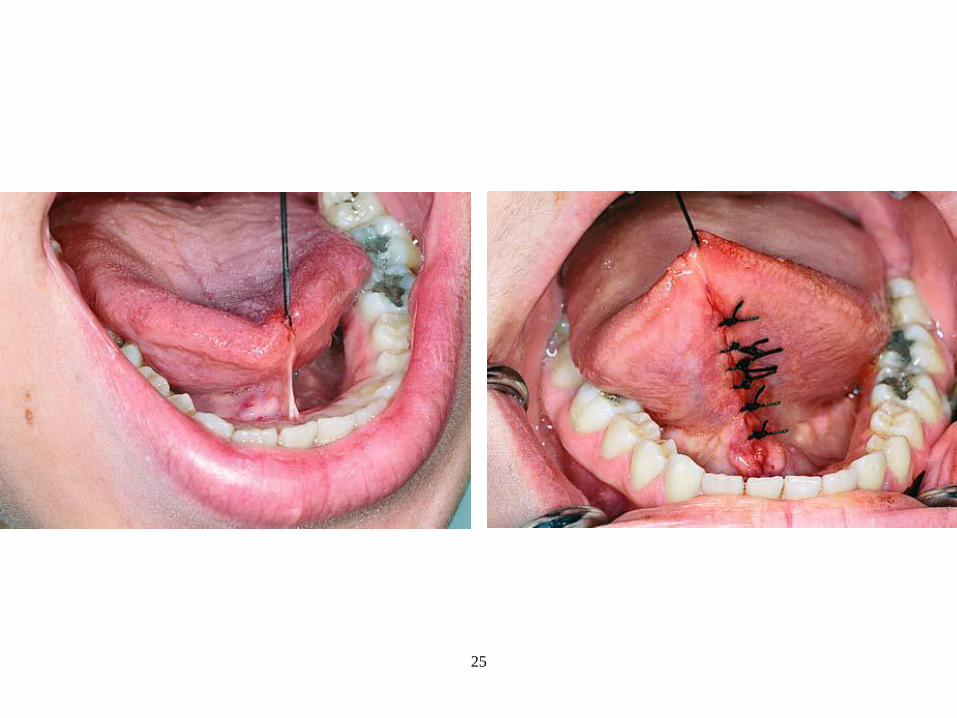
Technique: 1. Anesthesia is bilateral ling. Nerve block+ Infiltration ( for Haemostasis). 2. Pull the tongue by tongue forceps or suture (in midline 1 inch from the tip).3. Cut by scissor midway between Floor of mouth& ventral surface of tongue (avoid
injury to duct of submandibular S.G or lingual vessels) Till tip the tongue touches the palatal surface of maxillary anterior teeth while mouth is opened.
4. Undermined wound edges (avoid injury to sublingual veins).5. Suturing with 3/0 black silk interrupted sutures.
13
Prof. D
r. / K
haled
Elha
yes
(54) — CHAPTER (3)
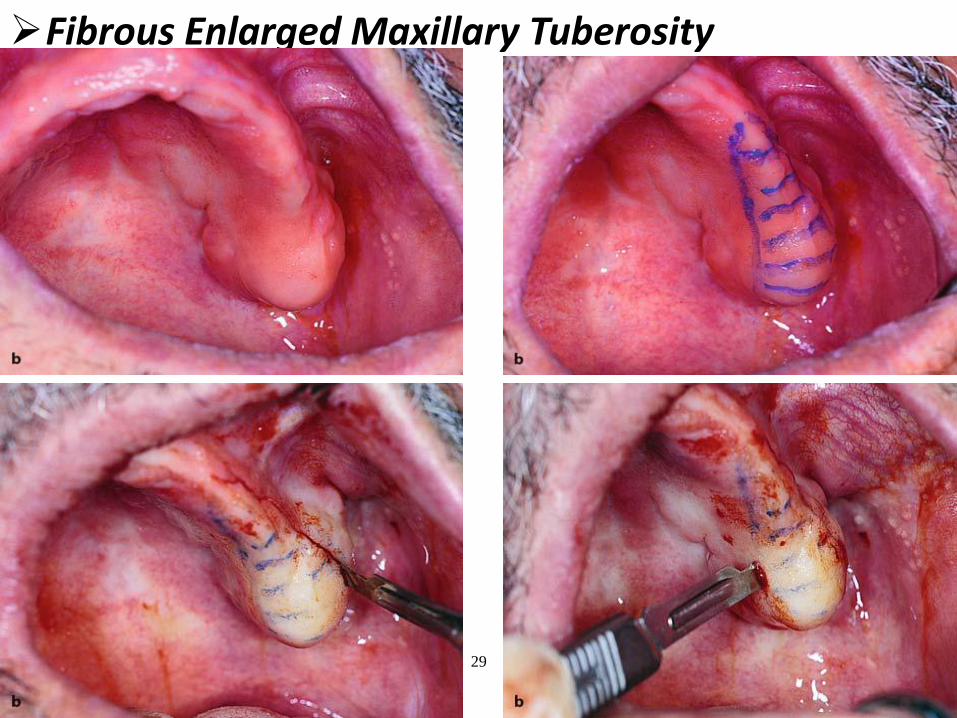
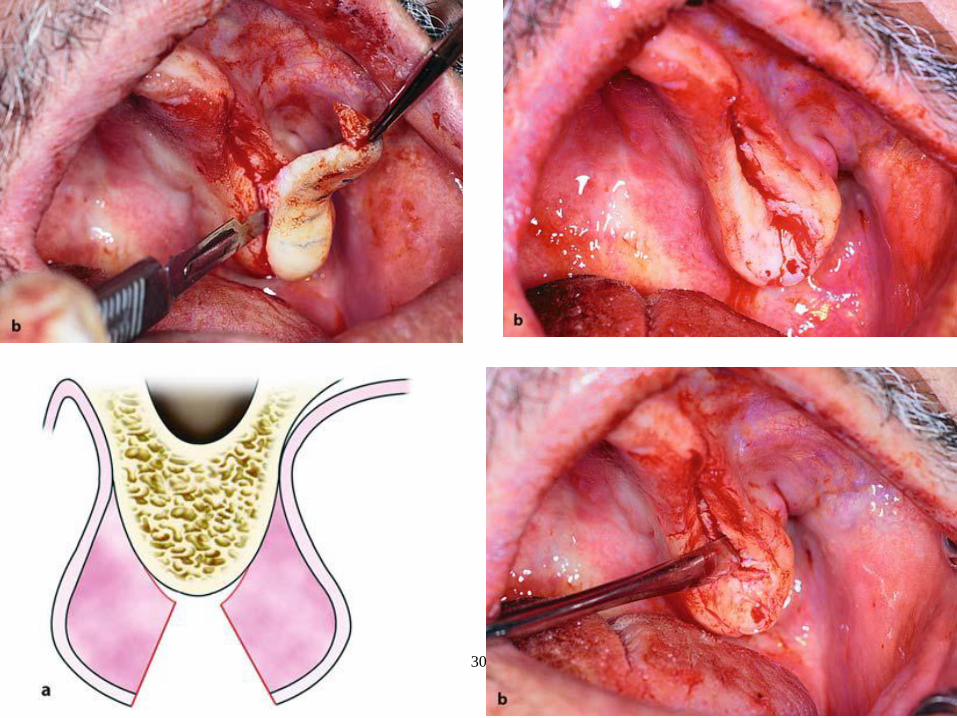
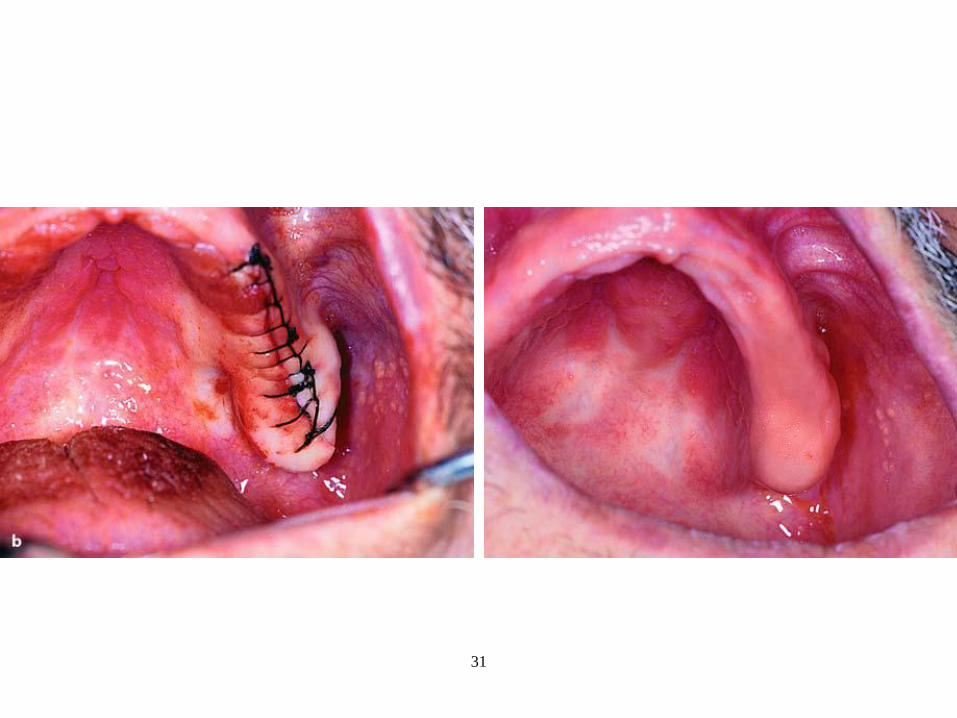
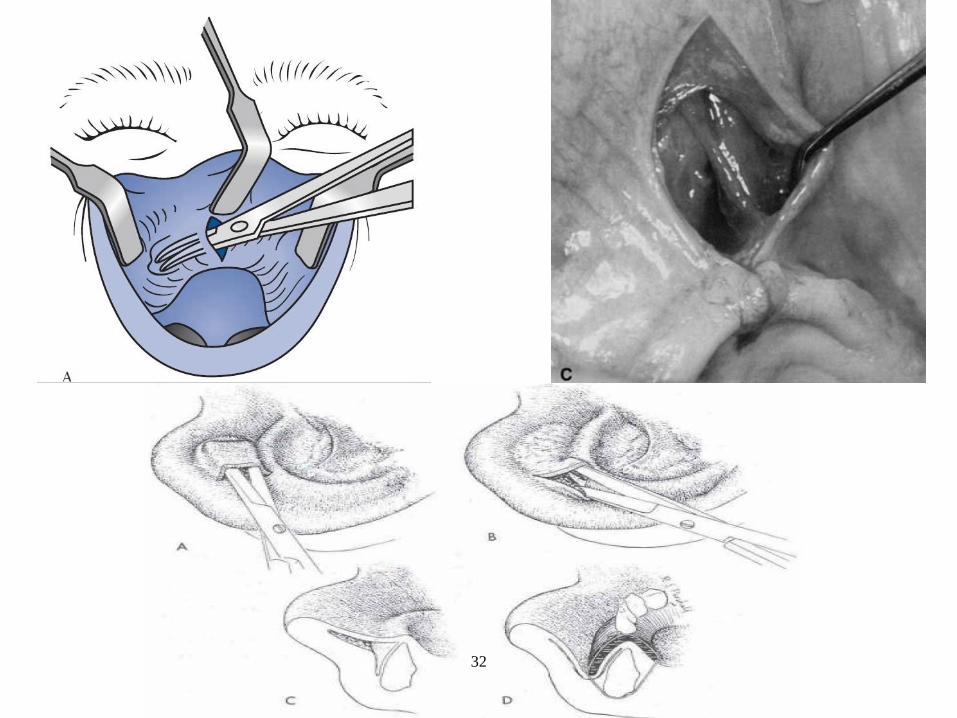
3- Fibrous tissue enlarged maxillary tuberosity:it could be enlarged: - 2ry to periodontal disease of maxillary molar - over erupted 8Indications: 1. If cause soft tissue irritation 2. Encroach inter-arch space and interfere with denture constructionTechnique:1- Paraperiosteal infiltration anesthesia buccally and palatally.2- Elliptical v-shaped incision by B.P blade 153- Grasp the tissue by Allis forceps and separate it from its origin by mucoperiosteal elevator.5- Undermined wound edges to provide tension free closure. 6- Suturing with 3/0 black silk interrupted or continuous suture.
4- Flabby ridge:Definition: it’s a redundant pendulous ridge that lacks bony support. Etiology:
1. traumatic occlusion (Single upper denture). 2. Ill fitting denture.3. Inflammatory hyperplasia.4. Severe bone resorption.
Technique: denture should be removed 7-10 days before surg. To ↓edema and inflammation.1- Paraperiosteal infiltration anesthesia.2- Grasp flabby tissue by multiple Allis forceps .3- Elliptical v-shape incision down to periosteum .4- separate it by mucoperiosteal elevator.5- undermined wound edges 6- Suturing with interrupted or continuous sutures.
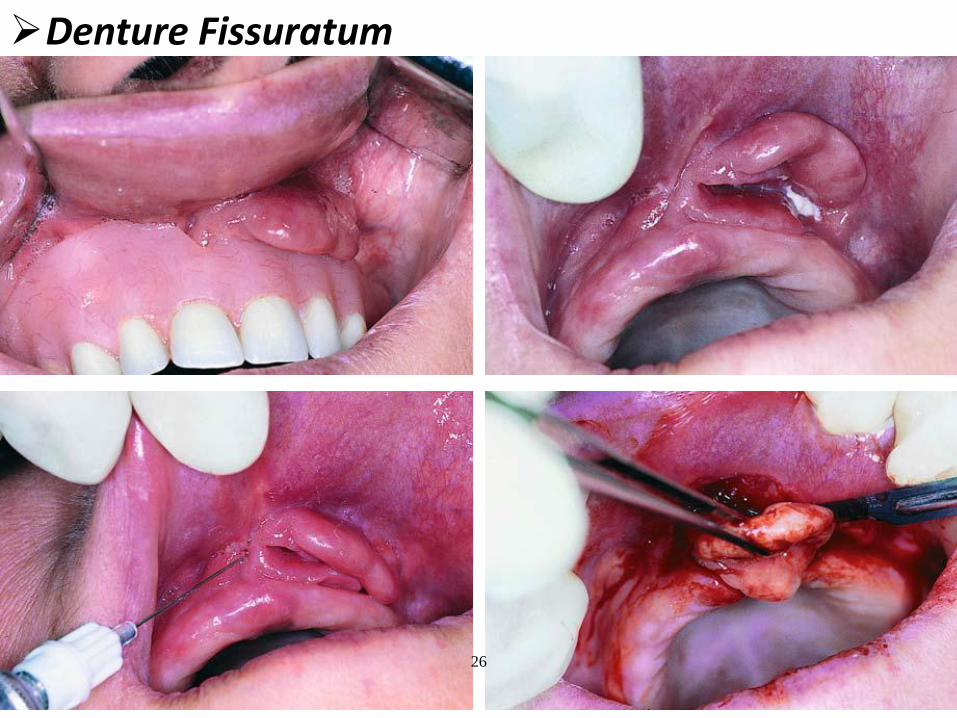
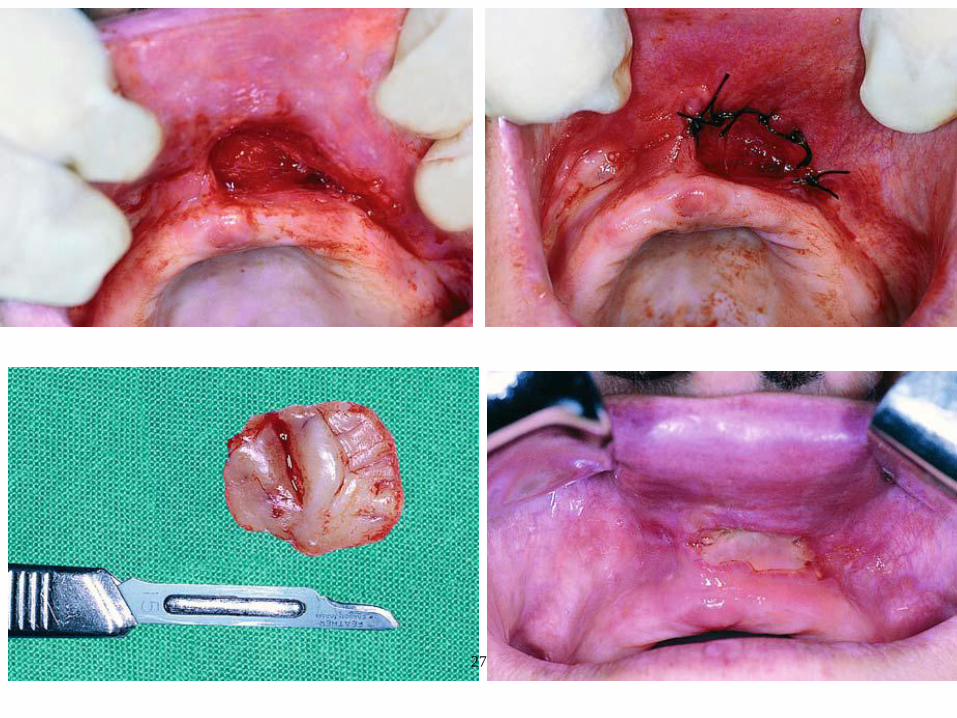
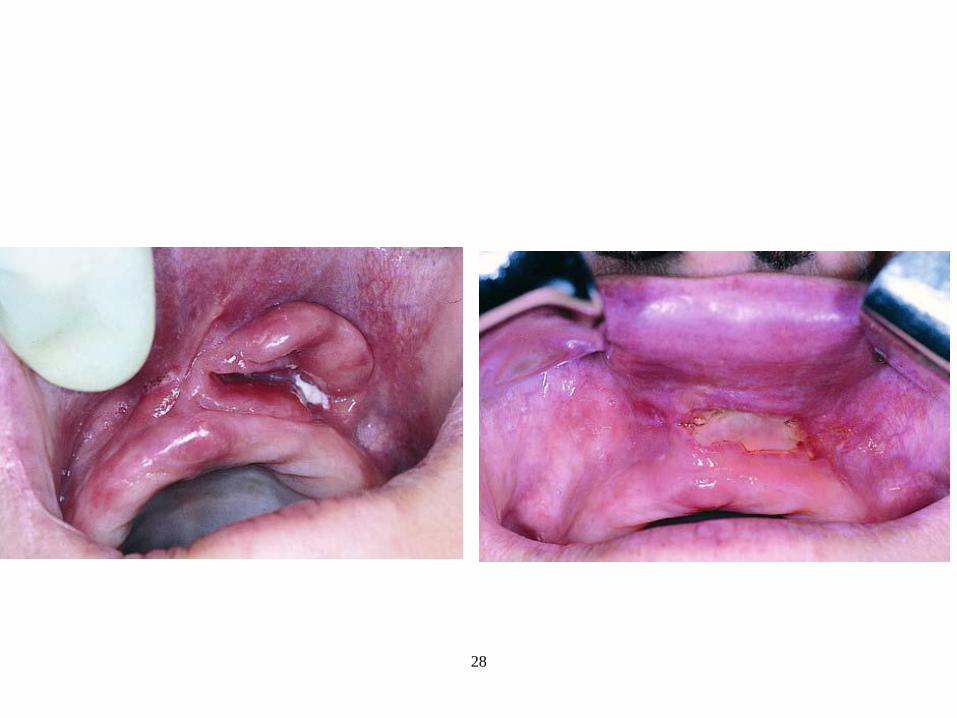
5- Denture fissuratum:Definition:It’s a hyperplastic inflammatory excess tissue present in the vestibule.It could be localized or generalizedEtiology: a. Over-extended or ill fitting denture→ ulcer→ granulation tissue→ fibrosis. b. Acute trauma.
14
Prof. D
r. / K
haled
Elha
yes
PREPROSTHETIC SURGERY — (55)
Management:a. early stage: reversible after relief of denture and use soft linerb. late stage: irreversible fibrosed tissue that should be removedTechnique:1- Infiltration Anesthesia in the vestibule. 2- Grasp tissue by Allis forceps or pickup.3- Supraperiosteal excision using scalpel.4- Undermined wound edges 5- Suturing with interrupted or continuous sutures.*N.B
if lesion is very large suturing will ↓sulcus depth So, raw area is packed to heal by 2ry intension or denture is lined with tissue conditioner. Biopsy could be done to exclude neoplastic nature.
C) Surgical Correction of Flat Ridge
Vestibuloplasty: Sulcus deepening or relative ridge heightening. Bone height ≥ 2cmRidge augmentation: Absolute ridge heightening. Bone height < 2cm
1. Vestibuloplasty: ( Sulcus deepening or relative ridge hightening)Defintion: surgical sulcus deepening i.e relative ridge hightening Etiology : Inadequate sulcus depth as a result of:
a. Moderate resorption (bone height is ≥ 2cm)b. High muscle attachment.c. Scar tissue in vestibule.
Indications:a. adequate bone height (≥ 2cm)b. High muscle attachment.
Techniques:
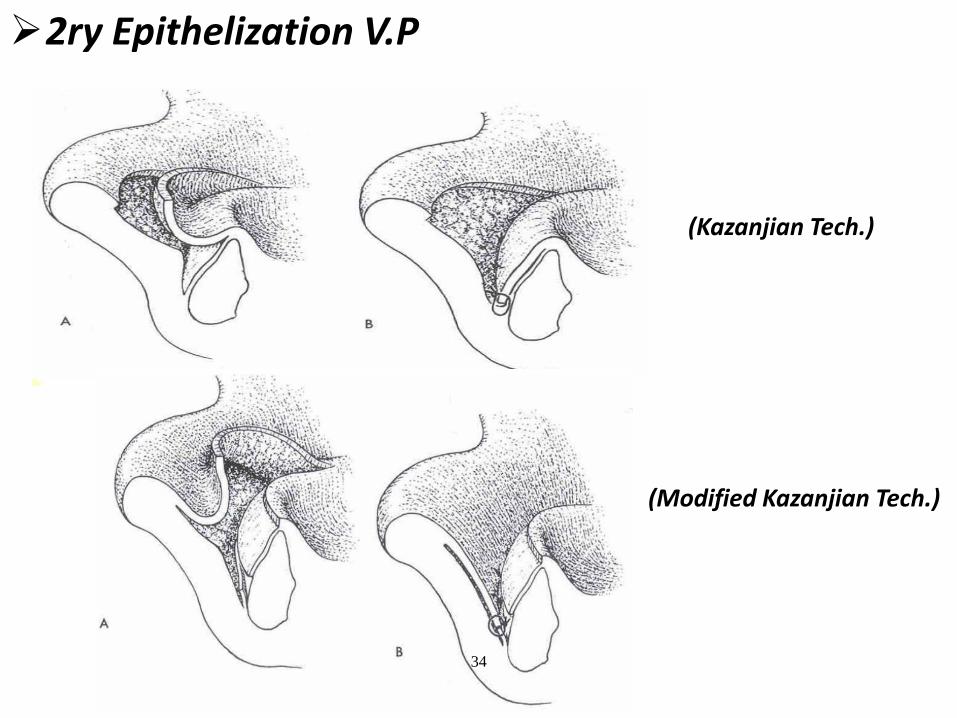
A- Secondary epithelization vestibuloplasty:Indications:
1. Moderate bone resorption ( ≥ 2cm. ).2. mucosa is not enough or not healthy (e.g. scar, hyperplastic or fibrosed)
Technique:1. Infiltration anesthesia 2. horizontal mucosal incision between Alveolar mucosa and attached gingiva labially.
15
Prof. D
r. / K
haled
Elha
yes
(56) — CHAPTER (3)
3. supra-periosteal dissection of mucosal flap & Cut high muscle attachment.4. Suture mucosa deeply to periosteum at the depth of vestibule.5. Bare periosteum is packed to heal by 2ry intension.
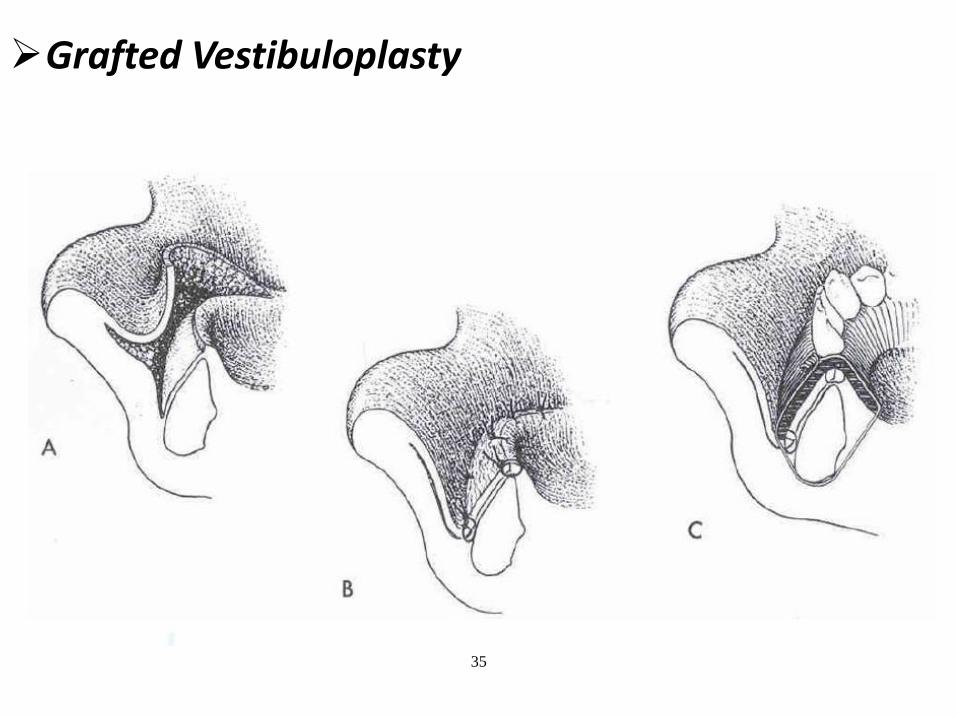
B- Mucosal graft vestibuloplasty:Mucosal grafts is taken from cheek or palate (from a pathologically free area), the graft is put over raw periosteum:Advantages:
a. Cover raw area of periosteum à↓wound regression. b. Better healing.
C- Skin graft vestibuloplasty:Indication: for larger area coverageRules for obtaining skin graft:a. from hairless area (inner thigh, buttock, lateral abdomen and medial side of forearm).b. thin graft (split thickness).c. recipient area should have good blood supply.d. complete hemostasis of the raw area before the graft is inserted.
Keys of success of skin graft:a. adequate vascularity of recipient site.b. adequate fixation of the graft.
2. Ridge Augmentation:
Definition: it’s absolute ridge hightening.Indication:
1. Severe atrophy in ridge, remaining bone height is < 2cm.2. High muscle attachment that can not be repositioned at lower level.
Techniques of ridge augmentation:Onlay bone graft:
Indication: To ↑height + ↑widthTecnique: -Rib or iliac crest grafts. Or - Hydroxy appatite augmentation through subperiosteal tunnellingDisadvantages: Resorbs fastly.
16
Prof. Dr. /
Khaled Elhayes
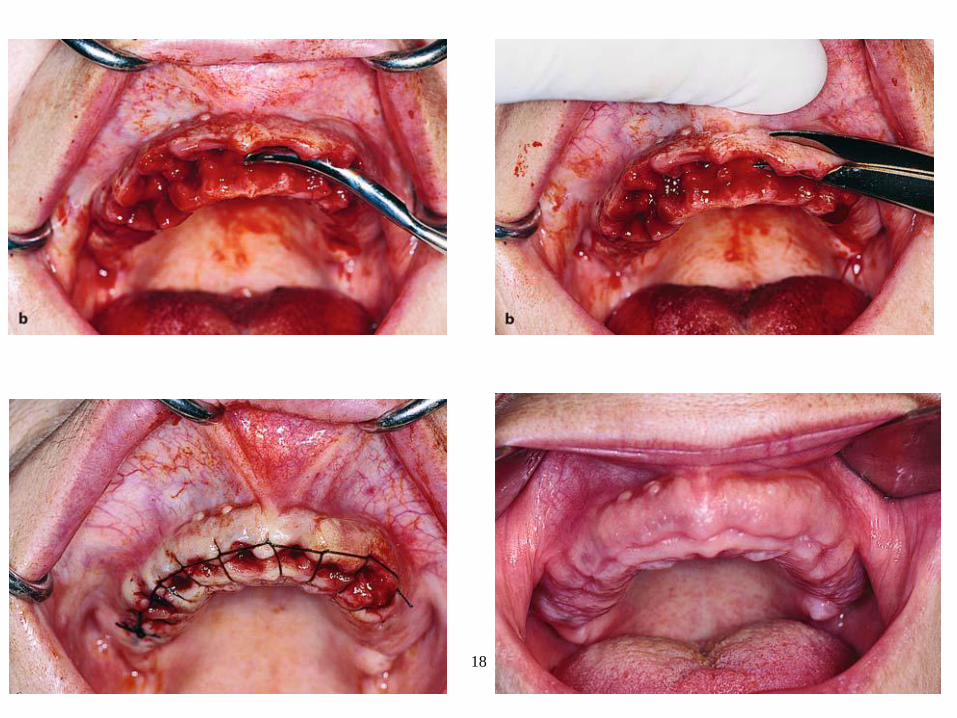
Technique of: Interseptal alveoloplasty. Labial plate alveoloplasty (radical alveoloplasty)
17
Prof. Dr. /
Khaled Elhayes
18
Prof. Dr. /
Khaled Elhayes
Bony Prominence and Undercuts
19
Prof. Dr. /
Khaled Elhayes
20
Prof. Dr. /
Khaled Elhayes
Labial Frenum ( Frenectomy )
21
Prof. Dr. /
Khaled Elhayes
22
Prof. Dr. /
Khaled Elhayes
23
Prof. Dr. /
Khaled Elhayes
Lingual Frenum ( Frenotomy )
24
Prof. Dr. /
Khaled Elhayes
25
Prof. Dr. /
Khaled Elhayes
Denture Fissuratum
26
Prof. Dr. /
Khaled Elhayes
27
Prof. Dr. /
Khaled Elhayes
28
Prof. Dr. /
Khaled Elhayes
Fibrous Enlarged Maxillary Tuberosity
29
Prof. Dr. /
Khaled Elhayes
30
Prof. Dr. /
Khaled Elhayes
31
Prof. Dr. /
Khaled Elhayes
32
Prof. Dr. /
Khaled Elhayes
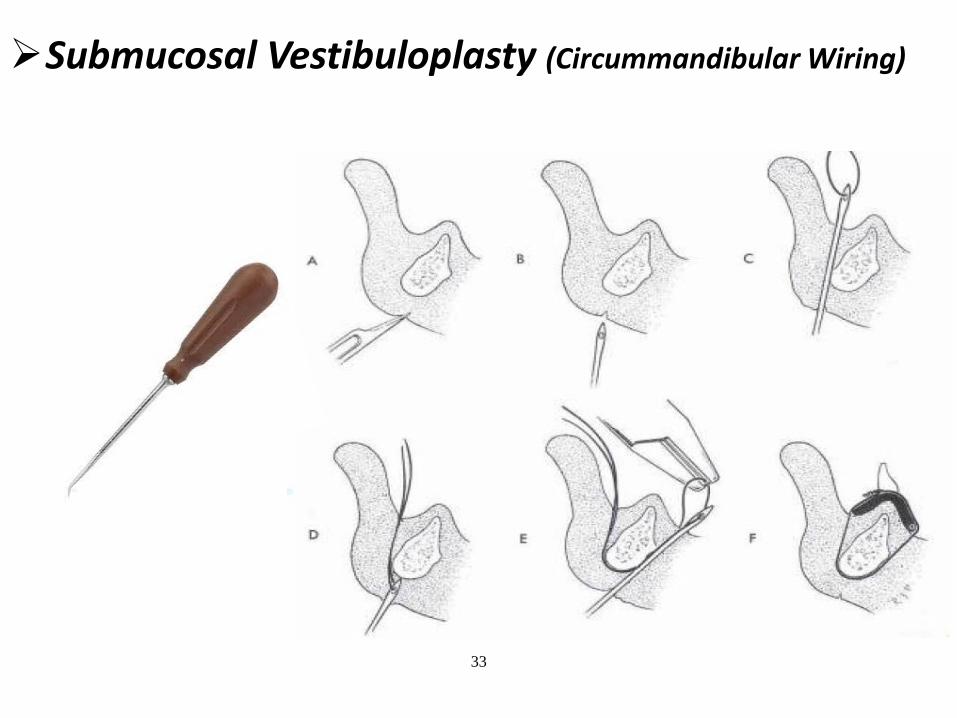
Submucosal Vestibuloplasty (Circummandibular Wiring)
33
Prof. Dr. /
Khaled Elhayes
2ry Epithelization V.P
(Kazanjian Tech.)
(Modified Kazanjian Tech.)
34
Prof. Dr. /
Khaled Elhayes
Grafted Vestibuloplasty
35
Prof. Dr. /
Khaled Elhayes
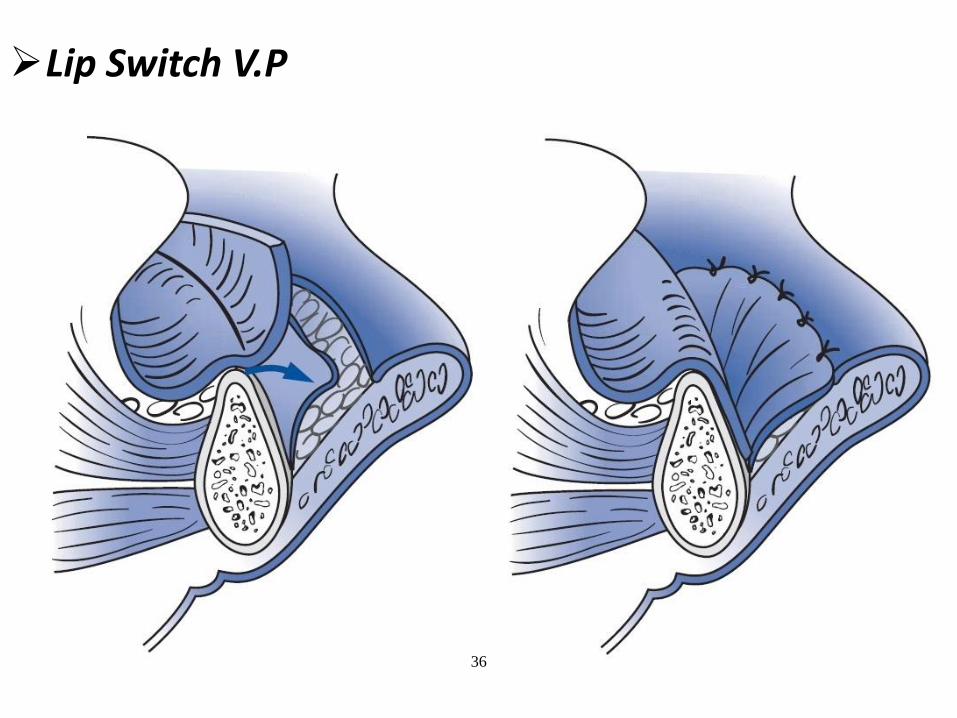
Lip Switch V.P
36