Embed Size (px)
Citation preview

Commentaries
Preparing School Personnel to Assist Students with Life-Threatening Food Allergies Genevieve H. Hay, Thomas B. Harper Ill Frances H. Courson
nowledge of life-threatening food allergies and prep- K aration for allergic reactions will enable school personnel to better respond to a student who has had a severe allergic reaction. While the mortality rate for food allergy reactions is low and most students do not experience life-threatening reactions, there can be dis- astrous exceptions. School personnel may work with a child with the potential for a severe allergic reaction, such as previous severe or life-threatening reactions.
Foods can and do cause anaphylaxis in some individ- uals and fatal cases do occur, but they are probably underreported. Recently, six cases of fatal food-induced anaphylaxis in children were reported.' Four of these fatalities occurred at school, indicating the critical need for school personnel to be knowledgeable about food- induced anaphylaxis.
A severe, life-threatening allergic reaction, known as anaphylaxis, occurs when an allergic reaction - usually to a food, medication, or insect sting - causes suf- ficient quantities of chemical mediators (such as histamine) to be released from mast cells scattered throughout the body. These mediators are released into the blood stream and produce leakage of fluid from blood vessels (causing hives and swelling), itching, contraction of smooth muscle, bronchospasm (asthma), diarrhea, low blood pressure and shock, and at times cardiac rhythm disturbances and death. Death from anaphylaxis occurs most commonly from upper airway swelling leading to asphyxia. Because symptoms can develop quickly, usually within 20-30 minutes after exposure, proceeding rapidly to overt clinical symptoms, schools must have an emergency plan for dealing with life-threatening allergic food reactions.
Several factors may contribute to fatal allergic reactions to foods. Parents, children, and teachers often deny allergic symptoms. Even when an allergy problem is acknowledged, understanding the potential severity of the reaction may not be understood. As a result, a tendency develops to deny or minimize symptoms or to rely solely on oral antihistamine for treatment of an evolving severe reaction. Individuals who recognize
Genevieve H. Hay, PhD, Assistant Professor; and Frances H. Courson, PhD, School of Education, University of Charleston. Charleston, SC 29424; and Thomas B. Harper III, MD, Clinical Assistant Professor, Dept. of Pediatrics, Medical University of South Carolina, 44 E. Markfield Road, Charleston. SC 29407. This article was submitted October 8, 1993. and revised and accepted forpublica- tion January 31. 1994.
that severe food allergic reactions require immediate intervention tend to be better prepared when a possible life-threatening reaction
A critical factor linked to the food anaphylaxis deaths has been failure to administer epinephrine promptly.'S2 In one study of fatal and near-fatal food reactions in children, five of six fatalities occurred in public places. Four incidents occurred at school. In each fatal case, epinephrine was administered only after severe symptoms developed. In seven cases occurring in private homes, epinephrine was given prior to develop- ment of life-threatening symptoms, preventing a fatality in all seven patients.'
PREPARATION OF SCHOOL PERSONNEL Given the higher incidence of food-related anaphy-
laxis in public places, teachers and school personnel should be aware of and prepared to deal with severe food allergy reactions.' Educators must be aware that appropriately documented food allergies are real and can be potentially life-threatening for children.J-6 The American Academy of Pediatrics' Committee on School Health recommends that schools be equipped to treat anaphylaxis in students.2J
The parent of a child with a life-threatening food allergy usually will contact the teacher and school nurse to explain the condition, answer questions, and sign a medical release form. Once a child has been identified with a severe food allergy, the school should develop a procedure for alerting teachers working with the stu-
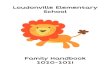
Figure 1 Eplnephrlne (Admnalln) Admlnittratlon
Epl-Pen@ is epinephrine in a disposable springloaded selt-injectable syringe with a concealed needle. It is available by prescription only. Children over the age of seven can be taught to sen-administer in an emergency.
DlNctlOIIS 1) Pull oft the gray safety cap. (This prepares the injector to be trigwred.) 2) Place the black tip on thigh, at a right angle to the leg. (Can administer
through clothes.) 3) Ress hard (and constrain the individual, if necessary) into thigh until Autw
In]eclor mechanism functions, and hold in place for 15 seconds (counting slowly). Do not release pressure when the Epi-Pen' clicks - keep light on outer thigh. Remove unit. Massage injection area for 10 seconds.'O
'Periodically check the expiration date on the medication' and whether it has berome discolored.'o
4) Dispose of Epi-Pen@ unit in a sate place."
__ ~~
Journal of School Health March 1994, Vol. 64, No. 3 119

Figure 2 Medical Release Formla
Medhtlon F m Student: School: Grade: Address: Date: Parents: Home Phone:
Work Phone:
To Authorlzed School Personnel: I hereby request and authorize you to give:
to: as prescribed by Doctor , and I release school personnel from
liability should reactions result from medications. In case of an anaphylactic reaction, follow-up care and transportation are to be as lollows:
(dose and medication)
(Parent’s Signature) . . . . . . . . . . * * * . . To Authorized Schwl Personnel: I prescribe
reasons stated:
to be given to
by school personnel during school hours for (dose and medication)
. MD (Physician’s Signature)
dent. A prominent notation on the child’s health record should indicate a potentially life-threatening food allergy.
Teachers and other school personnel can be prepar- ed to deal with food allergic reactions by being trained to administer CPR and first aid. School personnel should keep phone numbers of the nearest medical facility and should know how quickly an EMS team can respond to a medical emergency in the school.6
School personnel should know where appropriate medications are stored, the correct dosage, and how to administer the medications (Figure 1). Epinephrine (adrenalin), usually in the form of a self-administered automatic device such as an Epi-Pen,@ should be sup- plied by the parent and should be available at all times. This device should be brought on class trips or any out- ings involving the child at risk.’J Training kits, as well as other helpful materials and literature, are available from The Food Allergy Network, a national food allergy support group.
Once the emergency plan is in effect, authority should be delegated to include who gets and administers the medication, who calls the emergency medical serv- ices, parents, and physician, and who will stay with the child having the reaction. The child experiencing the reaction should not be left alone if at all possible.
Liability is a major concern of school personnel. Though Good Samaritan laws exist in fewer than 20 states,2 school personnel may obtain an effective medi- cal release form (Figure 2) from the child’s physician indicating the necessity of immediate treatment, what medications to give, and releasing school personnel from liability if a reaction occurs from administered medication( s).
THERAPY FOR ANAPHYLAXIS Anaphylaxis, a medical emergency, requires prompt
and appropriate therapy. Deaths have occurred because of delays in initiating therapy, particularly in a school or restaurant environment where lack of knowledge and concerns for liability have delayed initiation of therapy until well into a reaction.lsg School personnel must have a working knowledge of early treatment for anaphylaxis because their contributions may be the difference be- tween life and death for a specific child.
Actual treatment for a child with potential anaphy- laxis begins with anticipation and preventive planning, coordinated with parent, teacher, and dietary person- nel. Suspected food allergy should be confirmed by an allergist, and avoidance measures should be undertaken including avoidance of the specific food and all foods containing components of this food, such as avoiding casein or whey products in a milk-allergic child.
Treatment of anaphylactic reactions is sequential and should begin with identification of the event and prompt administration of epinephrine. Though antihis- tamines may be of some use with mild hives, gener- alized reactions with hives, swelling, flushing and dif- ficulty swallowing or breathing should be treated promptly with epinephrine. In children with previous food reactions, an epinephrine injective device (prefer- ably Epi-Pen or Epi-PenJr.@ ) should be immediately available to the teacher, nurse, or other school person- nel.
Once the reaction is identified and prompt adminis- tration of epinephrine has taken place, additional medi- cation administration should be deferred to EMS per- sonnel or to physicians in an emergency room. In order of appropriate sequence, the following calls should be made: 1) emergency medical services (911), 2) parent, and 3) child’s physician if phone number is available. Under no circumstance should the child having an anaphylactic reaction be transported by school person- nel to an emergency facility unless no emergency trans-
~ ~ ~~
120 Journal of School Health March 1994. Vol. 64. No. 3

port services are available in the community. Prompt therapy with epinephrine at the school site and inter- vention of emergency medical services at the site and during transport are mainstays of therapy to reverse a potentially life-threatening anaphylactic reaction.
CONCLUSION When contemplating the seriousness of potential
life-threatening food allergic reactions in school chil- ~
Resources
OrQanlzations
1) The Food Allergy Network 4744 Holy Ave. Fairfax, VA 22030 703/691-3179 Publishes a bimonthly newsletter.
1125 15th St., NW, Suite 502 Washington, D.C. 20036
2) Asthma and Allergy Foundation of America
Hotlines
1) The American Academy of Allergy and Immunology
To order a Medic Alert necklace or bracelet:
1-800-842-ASMA
Medic Alert Foundation P.O. Box 1009 Turlock, CA 95381
dren, attitude of school personnel may be the single most important factor for ensuring fair and proper treatment of these children. School personnel must listen carefully to parents of children with severe food allergies and obtain the necessary medical information. If school personnel are open, knowledgeble, and under- standing, they can successfully respond to emergency life-threatening food reactions.
References 1 . Sampson HA. Mendelson L, Rosa JP. Fatal and near-fatal
anaphylactic reactions to food in children and adolescents. N Engl J Med. 1992;327(6):380-384.
2. Yunginger J. Lethal food allergy in children. N Engl J Med. 1992;327(6):421.
3. Bochner BS, Lichtenstein LM. Anaphylaxis. N Engl J Med.
4. Galvin ES, Kcim RE, Conway TP. Children and allergies: Some effects and treatment. Children Today. 1983;13:31-33.
5 . Staudenmayer H. Convincing others food allergies are real. Food Allergy News. 1993;2(4):1,7.
6. Munoz-Furlong A. Planning ahead. Food Allergy News. 1993;2(4): 3.
7. Golden D, Graft D, Schwartz H, Bock A. Draft position state- ment - Use epinephrine in the treatment of anaphylaxis. News and Notes. 1993;3:6-7.
8. Munoz-Furlong A, Sampson HA. Just One Little Bite Can Hurt! Important Facts About Anaphylaxis. Fairfax, Va: The Food Allergy Network; 1992;6.
9. Yunghga J, Swcency KO, Sturner WQ, et al. Fatal food- induced anaphylaxis. JAMA. 1988;260(10):1450-1452.
10. Committee Report from the Adverse Reactions to Food Com- mittee of the American Academy of Allergy and Immunology. The treatment in school of children who have food allergies. JAIlergy Clin Immunol. 1991;87:749-751.
1991;324(25): 1785-1790.
A S H A P A R T N E R S +
Platinum Endowment Partner + McGovern Fund for the Behavioral Sciences, 6969 Brompton, Houston, TX 770s
Gold Endowment Partner + +
Consumer Health Care Division of Pfizer, Inc., New York, NY 10017 Tambrands, Inc., One Marcus Ave., Lake Success, NY 11042
Silver Endowment Partner + + + + +
Center for Injury Research and Control, University of Pittsburgh, MUH, Room NE560,200 Lothrop St., Pittsburgh, PA 15213 Dept. of Health Science Education, University of Florida, Gainesville, FL 32611 Dept. of Health Studies, The University of Alabama, TuscaloosB, AL 354874312 Mosby-Year Book, Inc., 11830 Westline Industrial Drive, St. Louis, MO 63146 School of Education, University of Pittsburgh, 5T01 Forbes Quadrangle, Pittsburgh, PA 15260
Sustaining Partner + +
Health Education Dept., University of Utah, Salt Lake City, UT 84112 School Health Supply Company, P.O. Box 409, Addison, IL 60101
Century Partner + +
Commercial Press, Inc., 115 S. Depeyster St., Kent, OH 44240 Mead Johnson Laboratories, P.O. Box 4500, Princeton, NJ 085434500
Journal of School Health March 1994, Vol. 64, No. 3 121












![Food & Formula Reference Guide [FFRG] · 8. Severe food allergies requiring an elemental formula 9. Life threatening disorders, disease and medical conditions that impair ingestion,](https://img.pdfslide.us/doc/110x75/5f68600c00640326c54dd526/food-formula-reference-guide-ffrg-8-severe-food-allergies-requiring-an.jpg)














