Embed Size (px)
Citation preview

Preparing for the case
Lee Benson MD FSCAIThe Hospital for Sick Children,
Toronto, Canada

No Disclosures

Ask yourself these questions as youprepare for the catheterization
Why is the case being done?-pre-operative information:-hemodynamics –PVRI, LVED-morphology or intervention
Is the case elective, emergent or urgent?
Is this the right timing for the procedure?
Is the child stable enough for the procedure?if non-elective…is transportation an issue…
ECMO

Has the child & family been prepared for the procedure…………do they understand the risks and benefits?
Have you obtained consent & spoken to the family directlybefore the procedure?
Is the nursing staff & anesthesia prepared for the case?
Is the child appropriately sedated and stable?
Have you determined the best approach …vascular access?
Ask yourself these questions as youprepare for the catheterization

Precatheterization Conference
-reduces possibility that information will be missed
-identifies therapeutic procedures & equipment needed
-time to review echocardiograms, CXR, prior cath’s..etc
-time to develop a procedural plan

History & Physical Examination
Prior historybleeding disorderallergy to drugscontrast reactions
Intercurrent illness or recent feverdepends on how elective the case:e.g. infant in CHF…..may not find a 2 week period where theyare fever free …….in general avoid cath if temp ≥380C(likely to become bacteremic)
General history & physical examination
-specific questions relating totechnical aspects of the case

History & Physical Examination
Last menstrual period or possible pregnancymust have a very compiling reason to exposeher to radiation
Prior catheterizations or cardiac operations particular attention to unsuccessful cath’s or operations that effect vascular access

Physical examination*right & left thoracotomy scars
e.g. classical Blalock-Taussig shunts, Glenn anastomosis,precluding access to the heart from the arms
-vertical cut down from groin bypassvessels usually repaired
Extensive scar tissue, makes passage of sheaths & dilators difficult & often require staged dilation…sometimes with balloons
*groin or antecubital fossa scarsprevious vascular cut downs may make percutaneous studydifficult
-saphenous vein cut down: migrates distally,enter distal to scar proximal to inguinalligament

Abdominal, thoracic or neck vein distention infants with prolonged ICU stays (indwelling central lines) Mustard, Senning or Fontan repairs can develop caval or baffle obstruction
Peripheral arterial pulses CoA the most common but not only arterial lesion that may limit arterial access…..e.g. subclavian artery isolation

Medical & psychological preparation for cardiac catheterization
Precatheterization preparation
*Preparation is individualized……no hard & fast rules
*Begins when decision made to perform the procedure
*All patients beyond infancy need a general explanationregardless of sedation/GA. Describe that portion of theprocedure that they will be aware
*Never say ‘nothing will hurt’ …….makes the child moredistressed & uncooperative. Do not let them think it’sjust like an ‘office visit’

Medical & psychological preparation for cardiac catheterization
Precatheterization preparation
*Exact details depends on the age/understanding/interestof the child…tailored at the time of the interview
*Be truthful, not all the gruesome details……leads to > anxiety
*-information:young children pre-procedure tests,
the inevitable ‘needle’,premeds/sedation given
older child length of procedure, stay in PAR, stay in hospital,any special issues: IV lines, Foley’s

Medical & psychological preparation for cardiac catheterization
Precatheterization preparation
* older patient more detail/explanationtailored to patient & family
*Emphasize the reason for the cath, not only technical details or risks
*Full details make you ‘medicolegally’ more comfortable………………….but only worsens anxiety for the child

Medical & psychological preparation for cardiac catheterization
Precatheterization preparation
Those in a decision making position, informed consent shouldinclude:
1- the diagnosis2- the nature of the procedure3-the risks4-the alternatives5-the risks of not doing the procedure6-the benefits

Medical & psychological preparation for cardiac catheterization
The risks:
Data from 11,073 children catheterized (last 10 yr) looking at complications withinthe first 24 h after catheterization
Complications occurred in 7.3%.....~1% major (stroke, perforation, permanentarterial thrombosis, seizures) & ~6% minor with vascular complications(hematoma, transient vessel occlusion)
25 children died within 24 h (0.23% of total case numbers)
Independent risk factors:young patient age (<6 months)male genderinpatient statusyear of catheterization

Medical & psychological preparation for cardiac catheterization
Precatheterization preparation
*No infant/most all children do not need sedation the nightbefore the study
*Occasionally, an adolescent/ACHD-or-parent is very apprehensive …….mild sedative is reasonable
*In addition to explanation & psychological preparation……there are administrative issues that must be addressed:i.e., when and where to come to the hospital, NPO etc

Medical & psychological preparation for cardiac catheterization
Precatheterization preparation
*What are the arrangements for any pre-cath testing?
*Instructions for bathing…no shaving…EMLA cream 1-2 hours before case at home
*What time to come to hospital before the procedure

Medical & psychological preparation for cardiac catheterization
Nutritional & fluid requirements
*NPO after midnight not necessary2 hours NPO for clear fluids4 hours for breast milk or formula <6 months 6 hours food or formula >6 months
Assure that they take fluids 6 hours before the study ……….but remember…in the (polycythemic) infant ….start IV to maintain hydration, as study may be delayed …..….Lactated Ringers/NS or 5%dextrose/0.25NS
*Remember, infants/small children empty their stomachs faster than older children become dehydrated/hypoglycemic

Medical & psychological preparation for cardiac catheterization
Immediate pre-cath preparation
*EMLA cream (home) 1-2 hours before case, on all possible access sites
*Careful IV starts…avoid multiple attempts
*The combative child (for IV start): monitor ECG/BPketamine………1-2 mg/kg IMmidazolam…..0.25mg/kg IN
Very anxious……………0.2 – 0.6 mg/kg PO (30 minutes before IV)

Medical & psychological preparation for cardiac catheterization
Immediate pre-cath preparationSpecial situations
*Polycythemia (Hct>65%):increased risk of catheffects hemodynamics
If Hgb >200 g/l, while increases oxygen carrying capacity ..…decreased CO, leading to reduced oxygen delivery to tissues…………risk of thrombosis & embolization…perform coagulation studies/platelet count
Anemia:decreases oxygen carrying capacity, falsely increases CO,
worsening CHF……exacerbated during the cath (blood loss/fluids)Correct any Hgb <80 g/l……….if can’t………….cancel case

Medical & psychological preparation for cardiac catheterization
Pre-medication*Goal: a calm, sleepy & cooperative child, before they enter the lab. Give medication in work up room, PO/IN/IM/IV
When GA is not used, all children need some sedation in addition local analgesia…good combination is fentanyl & midazolam
Fentanyl…..1-3 µg/kg IV, can repeat every 30 minutes…analgesia/sedation……..anaesthetic dose….5-10 µg/kg IV, 1-10 µg/kg/hr infusion
Midazolam….0.05-0.2 mg/kg IV, over 2 – 4 minutes ….0.2-0.3 mg/kg IN; 0.2-1 mg/kg 30 minutes prior to case PO ….0.07-0.1 mg/kg IM 30 minutes before cases
Monitor ECG, saturation, BP

Medical & psychological preparation for cardiac catheterization
*Under-sedation results in an uncooperative, anxious, hyperventilating, straining, moving, crying child….....both cruel to them and the staff
Today GA frequently used, as most catheterizations are performed for interventional indications
and a time out!

Medical & psychological preparation for cardiac catheterization
The anaesthetists will have their own checklist……………..….communication with them before the case is essential
Provide information so they can make an anaesthetic plan
nature of the procedurecardiac anatomyrecent echofunctional statusCHF?risk of ABE

Nurses role in preparation forcatheterization procedure
?

Nurses role in preparation forcatheterization procedure
*Nursing supervises an OPD pre-catheterization clinic
*Families are meet by their assigned nurse & an explanationis given to the families of the expectations for the day & administrative issues for the procedure day
*Pre-ordered tests are obtained (echo, ECG, CXR within 6 months),
but no routine tests (SS in appropriate populations)
*Test results are reviewed & discussed by the cardiology team &
communicated to the children & their family prior to discharge home

Nurses role in preparation forcatheterization procedure
The Clinic Nurse is responsible for performing a comprehensiveassessment for each child seen in pre-cath clinic, including:
vital signs, height, weight, chest assessment, infectious disease & medication checklist
Responsible for coordinating appropriate consultations (i.e. anesthesia consultation & thrombosis consultation)
Arranging a meeting between the children/family with the cardiologist performing the procedure

Nurses role in preparation forcatheterization procedure
The clinic nurse is responsible for educating the patient & their families on:
-the arrival time on the day of the procedure
-feeding instructions
-expectations before & after the catheterization
-provide information on research studies
-post catheterization site care upon discharge
-addressing questions & concerns of the children &
their families

Trends in the catheterization laboratoryCase Load: The CDIUCase Load: The CDIU
The Hospital for Sick Children 1969-2008The Hospital for Sick Children 1969-2008

Understand the indications for catheterization

On June 25th, 1876, General George Armstrong On June 25th, 1876, General George Armstrong
CusterCuster
received information that a significant number of received information that a significant number of
Indians were gathering at Little Big Horn. Without Indians were gathering at Little Big Horn. Without
analyzing the facts, he decided to ride out with 250 analyzing the facts, he decided to ride out with 250
men to ‘surround’ almost 3000 Indians ………….men to ‘surround’ almost 3000 Indians ………….
this was a serious mistakethis was a serious mistake.
Analyze the facts before making a decision

THANK YOU

Understand the timing of the studyElective
preparation for surgery,*primarily hemodynamic questions such as PAP, PVR, VEDP*anatomical questions such as pulmonary artery morphology……..complimenting
MRI/echo*preoperative intervention……collateral
occlusion

Understand the timing of the studyElective
*interventional (e.g. CoA, PDA, ASD, severe butnon-critical PS, AS)
*EP ablation
Emergent or urgent*post-operative
anatomical & hemodynamic questionsinterventional procedures
*hemodynamic (e.g. critical PS, AS, BAS, pulmonary atresia/IVS)

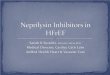
Understand the risks
*Cardiac catheterization in the immediate post-operative ICU period
*Between 2004 & 2007, 49 children (~3% of cardiac surgeries),
underwent 62 catheterizations before discharge from the ICU
*Median age at surgery was 167 days & time
to catheterization 8.5 days
*Overall mortality was high (43%)
*Delay to catheterization, especially>2 to 3 weeks & a splinted sternum were risk factors for death
*Re-operation after a non-interventionalcatheterization predicted worse survival(p<0.001)
Diagnostic catheter leading to re-operation
Intervention or diagnostic catheter

Probability of disease being present%
Mort
alit
y o
f ca
thete
riza
tion (
%)
Neither cathNor operate
Catheterize
Operate withoutcatheterization
MaCartney Br Heart J 1984
Understand the risksCompeting risks vs. other non-invasive testing





![Benson Lecture Inpla[1] Phil Benson](https://img.pdfslide.us/doc/110x75/5549e849b4c90518488b4ca4/benson-lecture-inpla1-phil-benson.jpg)












![George Benson - The Best of George Benson[1]](https://img.pdfslide.us/doc/110x75/5695cf541a28ab9b028d9c4a/george-benson-the-best-of-george-benson1.jpg)







